Feb 10, 2026
You are wasting 40% of your peptide every single time you get the water volume wrong. That is not an exaggeration. Hundreds of people reconstitute their 5mg semaglutide vial with the wrong amount of bacteriostatic water, draw up what they think is the correct dose, and inject a fraction of what they intended. Or worse, they inject far more than planned. The math errors compound over weeks, the dose escalation falls apart, and the vial runs out days before it should. All because nobody handed them a clear mixing chart before they started.
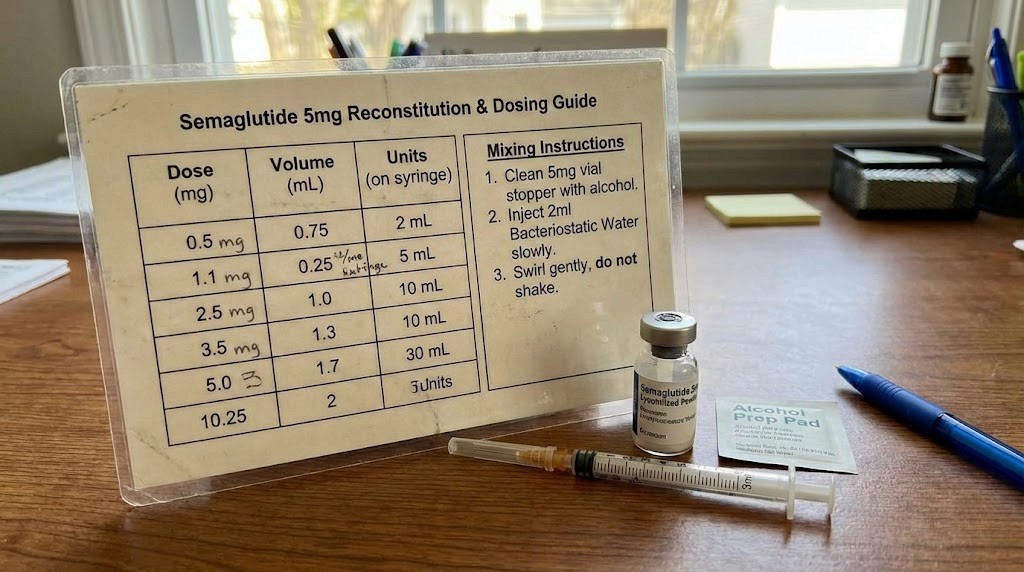
The 5mg semaglutide vial sits at the center of this confusion. It is not the 10mg vial that most generic mixing guides cover. It is not the pre-filled pen that pharmaceutical companies ship with instructions printed on the box. It is the research-grade lyophilized powder that arrives as a tiny white cake at the bottom of a small glass vial, and it demands precise reconstitution before a single dose can be drawn.
Here is what makes the 5mg vial uniquely tricky. The concentration you create depends entirely on how much bacteriostatic water you add. Add 1mL and you get 5mg per milliliter. Add 2mL and you get 2.5mg per milliliter. Add 2.5mL and you get 2mg per milliliter. Each concentration produces completely different syringe readings for the same milligram dose. Miss this distinction and every injection you draw will be wrong. This guide gives you every mixing chart, every syringe conversion, every dose calculation, and every step of the reconstitution process for the 5mg semaglutide vial. No guesswork. No wasted peptide. No math errors. Just the reference you keep open on your phone every time you mix a new vial.
Why the 5mg semaglutide vial requires its own mixing chart
Most reconstitution guides online focus on the 10mg vial. That makes sense from a volume standpoint, because 10mg is the more common research quantity for semaglutide. But the 5mg vial operates on entirely different math. The concentrations are different. The syringe readings are different. The number of doses per vial is different. Trying to use a general semaglutide mixing chart designed for 10mg will produce incorrect doses from a 5mg vial every single time.
Think about it this way. If you add 2mL of bacteriostatic water to a 10mg vial, you get 5mg/mL. If you add 2mL to a 5mg vial, you get 2.5mg/mL. Same water volume. Half the concentration. Someone following the 10mg chart with a 5mg vial would inject half their intended dose without realizing it. They would wonder why the peptide is not working. They would blame the product quality. They would post in forums about how their semaglutide must be fake.
The problem runs deeper than simple division, though.
Dose escalation schedules assume a specific concentration. When your semaglutide 5mg dosage chart says to inject 10 units for 0.25mg, that number only works at one specific concentration. Change the concentration and the unit count changes with it. This is where people get lost. They mix one concentration, follow a chart designed for another, and the entire protocol collapses before week two.
There is also the practical matter of injection volume. A 5mg vial mixed with 1mL of water produces a very concentrated solution. Your doses will be tiny, measured in just 5 or 10 units on an insulin syringe. That precision is difficult to achieve. A 5mg vial mixed with 2.5mL produces a more dilute solution. Your doses will be larger, easier to measure, but you will run through the vial faster because you are drawing more liquid each time.
The bacteriostatic water ratios for 10mg vials simply do not translate. You need dedicated charts for the 5mg vial, and that is exactly what the rest of this guide provides.
What you need before mixing semaglutide 5mg
Gather everything before you start. Once you puncture the bacteriostatic water vial and draw liquid into a syringe, you do not want to pause and search for an alcohol swab. Contamination happens during delays. Peptide degradation happens when reconstituted vials sit at room temperature while you look for supplies.
Here is what sits on your workspace before you begin.
The 5mg semaglutide vial. This is your lyophilized powder. It should be a white or off-white cake or powder at the bottom of the vial. If the powder looks discolored, clumped with moisture, or the vial seal appears compromised, do not use it. Quality matters, and peptide vial integrity determines whether your reconstitution will succeed.
Bacteriostatic water (BAC water). Not sterile water. Not saline. Bacteriostatic water specifically. It contains 0.9% benzyl alcohol, which prevents bacterial growth in the solution after mixing. This is critical because you will draw from the same vial multiple times over several weeks. Sterile water has no preservative, meaning bacteria can colonize the vial after the first needle puncture. For a multi-dose vial like semaglutide, bacteriostatic water is the only appropriate choice.
Insulin syringes (U-100). You need two types ideally. A 1mL syringe for measuring and adding the bacteriostatic water to the vial. And a 0.3mL or 0.5mL insulin syringe for drawing your individual doses. The smaller syringe has finer graduation marks, making it easier to measure doses precisely. Every syringe must be sterile and single-use. Learning how to calculate peptide dosages becomes much simpler when you have the right syringes.
Alcohol swabs. You will use these to sterilize the rubber stopper on both the semaglutide vial and the bacteriostatic water vial before each puncture. This is not optional. Skipping this step is one of the most common peptide mistakes beginners make.
A clean, flat workspace. A desk or countertop wiped down with isopropyl alcohol. Good lighting. No pets, no fans blowing dust around, no distractions. The reconstitution process takes about five minutes, but those five minutes require your full attention.
A permanent marker or label. After mixing, you will label the vial with the date of reconstitution and the concentration you created. This seems trivial until you have three vials in your refrigerator and cannot remember which one contains 2.5mg/mL and which contains 5mg/mL.
The peptide reconstitution calculator on SeekPeptides can help you double-check your math before you begin. Plug in 5mg as your peptide amount, enter your chosen water volume, and it will confirm the concentration and show you exactly how many units to draw for each dose. Having that confirmation before you start eliminates second-guessing during the process.
If you want a broader understanding of the mixing process for any peptide, the guide on how to mix peptides with bacteriostatic water covers the universal principles that apply across all peptides, not just semaglutide.
Semaglutide 5mg mixing chart: every concentration explained
This is the section you bookmarked this page for. Below you will find complete mixing charts for the three most practical concentrations you can create from a 5mg semaglutide vial. Each chart shows you the dose in milligrams, the volume in milliliters, and the number of units on a U-100 insulin syringe. The semaglutide syringe dosage conversion chart principles apply here, but the numbers are specific to the 5mg vial.
Pick your concentration based on your needs. Then use the corresponding chart for every dose you draw.
5mg + 1mL bacteriostatic water = 5mg/mL concentration
This is the most concentrated option. You are dissolving all 5mg of semaglutide into just 1 milliliter of water. The result is a potent solution where a tiny amount of liquid contains a significant dose. This concentration works well for people on lower doses who want to minimize injection volume. It also maximizes the number of doses you can pull from the vial because each dose uses very little liquid.
The downside is precision. At this concentration, the difference between 0.25mg and 0.5mg is only 5 units on your syringe. That is a small margin. You need steady hands, good eyesight, and a syringe with clear markings. A 0.3mL insulin syringe with half-unit markings is strongly recommended at this concentration.
Dose (mg) | Volume (mL) | Insulin syringe units (U-100) |
|---|---|---|
0.125mg | 0.025mL | 2.5 units |
0.25mg | 0.05mL | 5 units |
0.375mg | 0.075mL | 7.5 units |
0.5mg | 0.1mL | 10 units |
0.75mg | 0.15mL | 15 units |
1.0mg | 0.2mL | 20 units |
1.25mg | 0.25mL | 25 units |
1.5mg | 0.3mL | 30 units |
1.7mg | 0.34mL | 34 units |
2.0mg | 0.4mL | 40 units |
2.4mg | 0.48mL | 48 units |
At this concentration, a 0.25mg weekly dose uses only 5 units. That means your 5mg vial (containing 100 total units of liquid) could theoretically provide 20 doses at 0.25mg. That is 20 weeks from a single vial. However, reconstituted semaglutide should be used within 28 days of mixing, so you would not want to stretch a single reconstitution that far. The shelf life of compounded semaglutide in the fridge is a critical factor in your planning.
This concentration pairs well with the early stages of dose escalation where you are injecting 0.25mg or 0.5mg per week. The volumes stay small and manageable. Use the semaglutide dosage calculator to verify your numbers before each injection.
5mg + 2mL bacteriostatic water = 2.5mg/mL concentration
This is the most popular concentration for the 5mg vial. It balances precision with practicality. The doses are large enough to measure accurately on a standard insulin syringe but small enough that you still get a reasonable number of doses from each vial.
At 2.5mg per milliliter, the math stays clean. A 0.25mg dose equals exactly 10 units. A 0.5mg dose equals 20 units. A 1mg dose equals 40 units. These are easy numbers to find on any insulin syringe, which reduces the chance of measurement errors. If you are new to reconstituting peptides, this concentration offers the best combination of accuracy and simplicity.
Dose (mg) | Volume (mL) | Insulin syringe units (U-100) |
|---|---|---|
0.125mg | 0.05mL | 5 units |
0.25mg | 0.1mL | 10 units |
0.375mg | 0.15mL | 15 units |
0.5mg | 0.2mL | 20 units |
0.75mg | 0.3mL | 30 units |
1.0mg | 0.4mL | 40 units |
1.25mg | 0.5mL | 50 units |
1.5mg | 0.6mL | 60 units |
1.7mg | 0.68mL | 68 units |
2.0mg | 0.8mL | 80 units |
2.4mg | 0.96mL | 96 units |
Notice something important. At the 2.4mg dose, you are drawing 96 units out of 200 total units in the vial. That means a single 5mg vial at this concentration gives you roughly two doses at the maintenance level. For the early escalation phase at 0.25mg per week, you get 20 doses, though again the 28-day stability window means you should plan your reconstitution timing carefully.
This is the concentration that the peptide calculator defaults to for most semaglutide calculations. It represents the sweet spot where measuring accuracy meets dose flexibility. Whether you are just getting started with peptides or have been managing your own reconstitution for months, the 2.5mg/mL concentration from a 2mL water addition is the safest choice for consistent dosing.
5mg + 2.5mL bacteriostatic water = 2mg/mL concentration
This is the most dilute practical concentration for the 5mg vial. You get larger injection volumes, which some people prefer because they find larger volumes easier to measure and inject. The trade-off is that you use up the vial liquid faster.
At 2mg per milliliter, the dose-to-unit conversion changes again. Understanding how to calculate peptide dosages at different concentrations is essential for anyone managing their own reconstitution.
Dose (mg) | Volume (mL) | Insulin syringe units (U-100) |
|---|---|---|
0.125mg | 0.0625mL | 6.25 units |
0.25mg | 0.125mL | 12.5 units |
0.375mg | 0.1875mL | 18.75 units |
0.5mg | 0.25mL | 25 units |
0.75mg | 0.375mL | 37.5 units |
1.0mg | 0.5mL | 50 units |
1.25mg | 0.625mL | 62.5 units |
1.5mg | 0.75mL | 75 units |
1.7mg | 0.85mL | 85 units |
2.0mg | 1.0mL | 100 units |
2.4mg | 1.2mL | 120 units |
You will notice the math gets less clean with this concentration. Doses of 0.25mg require 12.5 units, which falls between the markings on most standard insulin syringes. This introduces measurement imprecision that compounds over time. Unless you have a specific reason to use 2.5mL of water, the 2mL option at 2.5mg/mL typically provides cleaner measurements.
Also note that the 2.4mg maintenance dose requires 120 units, which exceeds the capacity of a standard 1mL (100-unit) insulin syringe. At this concentration, higher doses physically cannot be drawn in a single syringe fill. You would need to split the dose across two injections, which is impractical and increases contamination risk.
For those tracking their peptide-based weight loss journey, keeping your concentration consistent across vials ensures your dose escalation stays on track. Switching concentrations between vials without updating your syringe readings is one of the fastest ways to derail progress.
Step-by-step reconstitution process for 5mg semaglutide
Charts only help if the mixing itself goes correctly. A perfect understanding of concentrations means nothing if bacteria enter the vial during reconstitution, or if the peptide degrades because you injected the water too forcefully. This section walks through every step of the physical process, from opening the packaging to storing the finished product.
Understanding the general principles of peptide reconstitution gives you a foundation. The steps below apply those principles specifically to the 5mg semaglutide vial.
Preparing your workspace
Wash your hands thoroughly with soap and water. Dry them with a clean paper towel, not a cloth towel that might harbor bacteria. Clear a section of counter or desk space. Wipe it down with isopropyl alcohol or a disinfectant wipe. Let it dry completely.
Lay out all your supplies: the 5mg semaglutide vial, the bacteriostatic water vial, your mixing syringe (1mL), your dosing syringes, alcohol swabs, and your label or marker. Everything should be within arm reach. You do not want to walk across the room mid-process with an uncapped syringe in one hand and an open vial in the other.
Check the semaglutide vial. The lyophilized powder should be a white or off-white puck at the bottom. It might look like a solid disc, or it might appear slightly crumbly. Both are normal. What is not normal: yellow discoloration, visible moisture inside the sealed vial, or a damaged crimp cap. If anything looks off, do not proceed. The peptide safety guide covers warning signs in detail.
Drawing bacteriostatic water
Decide your concentration first. For this walkthrough, we will use the most common option: 2mL of bacteriostatic water to create a 2.5mg/mL concentration. You can substitute 1mL or 2.5mL based on your chosen chart above.
Swab the top of the bacteriostatic water vial with an alcohol pad. Let it air dry for ten seconds. Do not blow on it or wave it around.
Remove your 1mL syringe from its sterile packaging. Pull the plunger back to the 2mL mark (if using a 3mL syringe) or fill a 1mL syringe twice. Push the needle through the rubber stopper of the bacteriostatic water vial. Turn the vial upside down. Slowly pull the plunger back until you reach exactly 2mL. Check for air bubbles. If you see large bubbles, push the water back into the vial and draw again slowly. Small bubbles at the top are acceptable; just push them back in with a gentle tap.
Remove the syringe from the water vial. Do not set it down. Proceed immediately to the next step.
Adding water to the vial
This is the most critical step. How you add the water determines whether the peptide survives intact.
Swab the top of the semaglutide vial with a fresh alcohol pad. Let it dry for ten seconds.
Insert the needle through the rubber stopper at a slight angle. Here is the crucial part: aim the needle tip at the glass wall of the vial, not directly at the powder. You want the water to trickle down the inside wall and gently flow onto the powder. Direct injection into the lyophilized cake can damage the peptide through physical force and rapid dissolution shock.
Push the plunger slowly. Very slowly. This should take 30 to 60 seconds for the full 2mL. Rushing creates turbulence inside the vial, which generates foam and can denature the peptide. Patience here protects your investment. Understanding how peptides work at the molecular level explains why gentle handling matters: the amino acid chain can unfold and lose function when subjected to physical stress.
Remove the syringe slowly after injecting all the water.
Dissolving the powder
Do not shake the vial. Never shake it. Shaking creates air bubbles, generates foam, and subjects the peptide to shear forces that can break the molecular structure.
Instead, hold the vial between your palms and gently roll it back and forth. Think of the motion you would use to roll a pencil between your hands. Slow, gentle, circular. You can also tip the vial at a slight angle and rotate it slowly, letting the water wash across the powder from different directions.
Semaglutide typically dissolves within 2 to 5 minutes of gentle swirling. The solution should become completely clear. No particles. No cloudiness. No clumps floating around. If you see undissolved powder after 10 minutes of gentle swirling, place the vial in the refrigerator for 30 minutes and try again. Sometimes cold temperatures help the dissolution process.
If the solution remains cloudy or contains visible particles after extended gentle mixing, the peptide may have degraded. Do not use it. The peptide storage guide explains the factors that cause degradation before and after reconstitution.
Labeling and storage
With a permanent marker, write three things on the vial or on a piece of tape attached to it. The date of reconstitution. The concentration (e.g., 2.5mg/mL). The peptide name (semaglutide 5mg). This takes ten seconds and prevents potentially dangerous mix-ups later.
Place the vial in your refrigerator immediately. The temperature should be between 2 and 8 degrees Celsius (36 to 46 degrees Fahrenheit). Not in the freezer. Not on the refrigerator door where temperatures fluctuate every time you open it. Ideally in the back of a shelf where temperature stays consistent. Learning how to store peptides after reconstitution properly can mean the difference between a vial that lasts the full 28 days and one that degrades in 10.
The reconstituted solution remains stable for 28 days under proper refrigeration. Mark your calendar. After 28 days, discard any remaining solution regardless of how much is left. Using expired reconstituted semaglutide risks both reduced efficacy and potential contamination. The question of whether you can use expired semaglutide has a clear answer: you should not.
Dose escalation schedule using a 5mg vial
Semaglutide is not a peptide you start at full dose. The GLP-1 receptor agonist mechanism, which activates anorexigenic neurons like POMC and CART while suppressing orexigenic neurons like NPY and AgRP, requires gradual introduction. Starting too high causes nausea, vomiting, and gastrointestinal distress that can make the entire experience miserable and lead people to quit before the peptide has a chance to work.
The standard dose escalation follows a predictable pattern. Each dose level lasts four weeks before increasing.
Phase | Weeks | Weekly dose | Doses from 5mg vial | Vial duration |
|---|---|---|---|---|
Initiation | 1-4 | 0.25mg | 20 doses | 20 weeks |
Escalation 1 | 5-8 | 0.5mg | 10 doses | 10 weeks |
Escalation 2 | 9-12 | 1.0mg | 5 doses | 5 weeks |
Escalation 3 | 13-16 | 1.7mg | ~2.9 doses | ~2.9 weeks |
Maintenance | 17+ | 2.4mg | ~2.1 doses | ~2.1 weeks |
Look at those numbers carefully. During the first four weeks at 0.25mg, a single 5mg vial contains enough semaglutide for 20 weekly doses. But the 28-day reconstitution shelf life means you cannot use all 20 doses from one mixing. You would reconstitute the vial, use four doses over four weeks (well within the 28-day window), and still have most of the liquid remaining. This is where planning becomes important.
At the 0.25mg initiation dose, you use only 1mg of the total 5mg over four weeks. That leaves 4mg unused when the 28-day clock expires. Some people choose to reconstitute with less water initially and plan their vial usage around the 28-day limit. Others accept the waste as the cost of proper protocol adherence.
By the time you reach the maintenance dose of 2.4mg per week, the math flips. A 5mg vial lasts roughly two weeks. You are going through vials much faster and need to plan your supply accordingly. Understanding how long you stay on semaglutide for weight loss helps you estimate the total number of vials you will need across your entire protocol.
Here is a practical planning table for the full escalation using 5mg vials.
Phase | Duration | Total semaglutide needed | 5mg vials needed |
|---|---|---|---|
0.25mg/week | 4 weeks | 1mg | 1 vial (4mg unused)* |
0.5mg/week | 4 weeks | 2mg | 1 vial (3mg unused)* |
1.0mg/week | 4 weeks | 4mg | 1 vial (1mg unused)* |
1.7mg/week | 4 weeks | 6.8mg | 2 vials |
2.4mg/week | ongoing | 2.4mg per week | 1 vial per ~2 weeks |
*Unused peptide within the 28-day window can continue to be used if properly stored. The "unused" column indicates peptide remaining after the 4-week escalation phase, not wasted peptide.
The question of how fast semaglutide works comes up frequently during the early escalation weeks. Most people notice appetite suppression within the first week or two. Significant weight changes typically appear by weeks 4 through 8. The GLP-1 mechanism takes time to fully engage the appetite regulatory pathways, and the gradual escalation ensures your body adjusts without overwhelming side effects.
For those interested in how this compares to other weight loss peptides, the escalation principle is similar across GLP-1 agonists, though the specific doses and timelines differ. The best peptides for weight loss all share this gradual titration approach to minimize side effects and maximize long-term adherence.
Insulin syringe unit conversion chart for 5mg semaglutide
Insulin syringes measure in units, not milligrams. This creates a translation problem that confuses almost everyone the first time they encounter it. The syringe does not know what peptide is inside it. It does not know the concentration. All it measures is volume, expressed as "units" where 100 units equals 1 milliliter on a standard U-100 insulin syringe.
So when someone asks "20 units of semaglutide is how many mg," the answer depends entirely on the concentration. At 5mg/mL (the 1mL reconstitution), 20 units equals 1mg. At 2.5mg/mL (the 2mL reconstitution), 20 units equals 0.5mg. Same number of units. Different milligram doses. This is why you must know your concentration before consulting any conversion chart.
Here is a comprehensive conversion table for all three concentrations side by side.
Syringe units (U-100) | Volume (mL) | Dose at 5mg/mL | Dose at 2.5mg/mL | Dose at 2mg/mL |
|---|---|---|---|---|
5 units | 0.05mL | 0.25mg | 0.125mg | 0.1mg |
10 units | 0.1mL | 0.5mg | 0.25mg | 0.2mg |
15 units | 0.15mL | 0.75mg | 0.375mg | 0.3mg |
20 units | 0.2mL | 1.0mg | 0.5mg | 0.4mg |
25 units | 0.25mL | 1.25mg | 0.625mg | 0.5mg |
30 units | 0.3mL | 1.5mg | 0.75mg | 0.6mg |
40 units | 0.4mL | 2.0mg | 1.0mg | 0.8mg |
50 units | 0.5mL | 2.5mg | 1.25mg | 1.0mg |
60 units | 0.6mL | 3.0mg | 1.5mg | 1.2mg |
68 units | 0.68mL | 3.4mg | 1.7mg | 1.36mg |
80 units | 0.8mL | 4.0mg | 2.0mg | 1.6mg |
96 units | 0.96mL | 4.8mg | 2.4mg | 1.92mg |
100 units | 1.0mL | 5.0mg | 2.5mg | 2.0mg |
The middle column, 2.5mg/mL, produces the cleanest numbers for standard dose escalation amounts. That is another reason why the 2mL reconstitution is the most recommended. At that concentration, every standard escalation dose (0.25mg, 0.5mg, 1.0mg, 1.7mg, 2.4mg) lands on or very near a clearly marked line on the insulin syringe.
If someone asks "how many mg is 40 units of semaglutide," you can now see the answer depends on concentration. At 2.5mg/mL, 40 units equals 1.0mg. At 5mg/mL, 40 units equals 2.0mg. Always know your concentration before interpreting any unit measurement.
How to read an insulin syringe correctly
A U-100 insulin syringe has markings along the barrel. The total capacity is either 0.3mL (30 units), 0.5mL (50 units), or 1.0mL (100 units). Each small line on a 1mL syringe represents 2 units. Each small line on a 0.3mL syringe represents 1 unit, and some models mark half-unit increments.
Hold the syringe at eye level. The plunger has a rubber gasket at the tip. Read the measurement at the top of the gasket, where it meets the barrel. Not the bottom of the gasket. Not the middle. The top edge where rubber meets air is your measurement point.
Common reading mistakes include counting the wrong line, reading from the bottom of the meniscus instead of the top, and confusing 0.3mL syringes with 1mL syringes. These errors are small on paper but significant in practice. Drawing 12 units instead of 10 units means a 20% dose error, and that kind of inconsistency accumulates over weeks of protocol adherence. The semaglutide syringe conversion chart helps, but physical syringe reading skill is something you develop with practice.
For precision at small doses, always use the smallest syringe that fits your dose. If you need 10 units, a 0.3mL syringe gives you finer gradations than a 1mL syringe. The marks are farther apart, easier to read, and the margin for error shrinks. This principle applies to all injectable peptides, not just semaglutide. The peptide injections guide covers syringe selection in more depth.
How many doses you get from one 5mg vial
Planning your peptide supply requires knowing exactly how many doses each vial provides at your current dose level. This varies dramatically across the escalation schedule. A person at the initiation dose gets 20 theoretical doses from one vial. A person at maintenance gets barely two.
The table below shows doses per vial at the 2.5mg/mL concentration (5mg + 2mL BAC water), which is the most common preparation.
Weekly dose | mL per dose | Units per dose | Total doses per vial | Weeks per vial |
|---|---|---|---|---|
0.125mg | 0.05mL | 5 units | 40 | 40 weeks* |
0.25mg | 0.1mL | 10 units | 20 | 20 weeks* |
0.5mg | 0.2mL | 20 units | 10 | 10 weeks* |
1.0mg | 0.4mL | 40 units | 5 | 5 weeks* |
1.7mg | 0.68mL | 68 units | 2.9 | ~2.9 weeks |
2.4mg | 0.96mL | 96 units | 2.08 | ~2 weeks |
*Subject to the 28-day reconstitution shelf life. Even if peptide remains in the vial, discard after 28 days.
The asterisks matter. At 0.25mg per week, the vial theoretically provides 20 weeks of doses. But you must discard the reconstituted solution after 28 days. That means you get 4 doses (4 weeks) from each reconstitution, then the remaining liquid should be discarded. You would need to work through the math of how much peptide you use within each 28-day window.
The peptide cost calculator factors in these variables to give you an accurate per-dose and per-week cost. Knowing how much peptides cost on a per-dose basis helps you budget realistically and avoid the surprise of running through vials faster than expected during higher dose phases.
For those planning their full protocol, the most cost-efficient approach during low-dose phases is to reconstitute with less water to create a more concentrated solution. At 5mg/mL (1mL of water), your injection volumes are smaller, and you use less liquid per dose. This means you can potentially get more doses out before the 28-day expiration hits. However, measuring precision at 5mg/mL is more challenging, so there is a trade-off between cost efficiency and dosing accuracy. The overall cost of peptide therapy varies based on how efficiently you manage your vials.
Storage and stability after mixing
Once you add bacteriostatic water to your 5mg semaglutide vial, the clock starts. The reconstituted solution is far more fragile than the lyophilized powder, and how you store it determines whether you get 28 days of potent, effective peptide or a degraded solution that loses efficacy by day 10.
Refrigeration requirements
Store the reconstituted vial at 2 to 8 degrees Celsius (36 to 46 degrees Fahrenheit). This is standard refrigerator temperature. Place the vial upright in the main body of the refrigerator, not on the door shelf. Door shelves experience temperature fluctuations every time you open the fridge. Those repeated warm-cold cycles accelerate degradation.
Does compounded semaglutide need to be refrigerated? Absolutely. Room temperature storage dramatically reduces shelf life and potency. Even a few hours at room temperature during a dose draw is acceptable, but returning the vial to the fridge promptly is essential.
Never expose the reconstituted solution to direct sunlight or fluorescent lighting for extended periods. Semaglutide, like many peptides, can degrade under UV exposure. Keep the vial in its box or wrap it in aluminum foil if your refrigerator has an internal light that stays on frequently.
The 28-day shelf life
Reconstituted semaglutide maintains its stability for 28 days under proper refrigeration. This is not a suggestion. It is the stability limit established through degradation studies. After 28 days, the peptide may have broken down to the point where the dose you draw no longer contains the milligrams you expect.
Understanding how long compounded semaglutide lasts in the fridge helps you plan your reconstitution timing. The ideal approach is to reconstitute a new vial only when you know you will use the contents within 28 days. At higher doses like 1.7mg or 2.4mg per week, this is easy since you deplete the vial in 2 to 3 weeks. At lower doses like 0.25mg per week, you will have leftover solution when the 28-day mark arrives.
The broader question of how long peptides last in the fridge varies by compound, but the 28-day guideline for reconstituted solutions is a safe standard across most research peptides.
Signs of degradation
A degraded solution may show visible changes: cloudiness, particles floating in the liquid, discoloration toward yellow or brown, or unusual odor. But degradation can also be invisible. The peptide chains break down silently, reducing potency without any outward sign.
This is why the 28-day rule exists as a hard boundary. You cannot smell or see a 30% potency loss. You can only notice it as reduced efficacy, reduced appetite suppression, or stalled progress. If your semaglutide seems to stop working mid-vial, temperature excursion or age-related degradation is a likely cause. The question of how long peptides last at room temperature provides more context on the degradation timeline outside refrigeration.
And no, you cannot solve this problem by reconstituting once and freezing portions for later. The question of whether peptides expire applies differently to lyophilized versus reconstituted forms. Lyophilized powder can last months or years when stored properly. Reconstituted solution is limited to 28 days regardless of storage method.
Common mixing mistakes and how to avoid them
Every mistake in this section costs you peptide, money, or both. Some mistakes are immediately obvious. Others hide for weeks, slowly undermining your protocol while you blame the product instead of the process. Learn them now so you do not learn them the expensive way.
Using the wrong water volume
This is mistake number one. Someone reads a chart designed for a 10mg vial, adds 2mL of water to their 5mg vial, and expects the same concentration. It will not be the same. The concentration will be exactly half. Every dose they draw will be half of what they intended. They will spend four weeks wondering why they feel no appetite suppression while injecting 0.125mg instead of 0.25mg.
The fix is simple. Confirm your vial size before consulting any chart. The charts in this guide are exclusively for 5mg vials. If you have a 10mg vial, you need the 10mg semaglutide mixing chart instead.
Shaking the vial
Shaking is intuitive. You shake orange juice. You shake protein shakes. You shake salad dressing. But you do not shake peptides. The shear forces generated by vigorous shaking can denature the semaglutide molecule. Denatured peptide does not bind to GLP-1 receptors. It becomes expensive, useless liquid.
Always swirl gently. Roll the vial between your palms. Tilt and rotate slowly. Patience protects potency.
Using the wrong syringe type
Not all syringes are U-100 insulin syringes. Some are U-40 (used for pet insulin dosing) where 40 units equals 1mL instead of 100 units. If you accidentally use a U-40 syringe with a U-100 chart, you will draw 2.5 times the intended dose. This is dangerous and surprisingly common among people who order syringes online without checking the specification.
Always verify: U-100 on the syringe packaging. 100 units equals 1mL. If the syringe says anything else, do not use it for this purpose. The peptide injection guide covers syringe selection details.
Contamination through poor technique
Every time a needle punctures the vial stopper, there is a contamination pathway. Failing to alcohol-swab the stopper before each entry introduces bacteria. Touching the needle tip to your fingers, the counter, or any non-sterile surface introduces bacteria. Using the same syringe for multiple dose draws introduces bacteria.
Use a fresh alcohol swab on the stopper before every entry. Use a fresh syringe for every dose draw. Never recap and reuse a syringe. These are basic sterile technique principles that become even more important with a multi-dose vial you will access repeatedly over 28 days. Avoiding common beginner peptide mistakes starts with consistent sterile practice.
Math errors during dose calculation
The formula is straightforward: dose in mg divided by concentration in mg/mL equals volume in mL to draw. Multiply by 100 to get insulin syringe units. But when you are doing this mental math at 6am before coffee, errors happen.
Use a calculator. Use the peptide reconstitution calculator. Print out the chart from this page and tape it to your refrigerator. Anything that removes the mental math from the process reduces your error rate. Understanding how to calculate peptide dosages is important for building your knowledge, but relying on verified charts for daily use is the safer practice.
Injecting water directly into the powder
Aim the needle at the glass wall, not the powder cake. A direct stream of water hitting the lyophilized peptide can cause localized high-concentration zones where the peptide partially dissolves and then re-aggregates. It can also physically break apart the powder cake in ways that make full dissolution harder. The wall-trickle method is gentler and produces a more uniform solution.
5mg semaglutide vs 10mg semaglutide mixing differences
Both vial sizes contain the same molecule. Semaglutide is semaglutide. The 94% structural homology to human GLP-1 is identical whether it comes from a 5mg or 10mg vial. What changes is the practical mixing math, the number of doses, and the cost efficiency.
Factor | 5mg vial | 10mg vial |
|---|---|---|
Peptide content | 5mg | 10mg |
Common water volume | 2mL | 2mL |
Resulting concentration | 2.5mg/mL | 5mg/mL |
Doses at 0.25mg | 20 | 40 |
Doses at 1.0mg | 5 | 10 |
Doses at 2.4mg | ~2 | ~4 |
28-day waste risk | Lower at high doses | Higher at low doses |
Best for | Early escalation, low doses | Maintenance, higher doses |
The key difference: if you add 2mL of water to both vials, you get 2.5mg/mL from the 5mg vial and 5mg/mL from the 10mg vial. The charts are completely different. The syringe readings for the same milligram dose are completely different. Mixing up which chart belongs to which vial size is one of the most dangerous reconstitution errors you can make.
The comprehensive semaglutide mixing chart covers both vial sizes, but if you specifically have a 10mg vial, the dedicated 10mg mixing chart provides focused reference tables.
When should you choose the 5mg vial over the 10mg? The 5mg vial makes the most sense during the early dose escalation phases (0.25mg and 0.5mg per week) where you will not use 10mg within the 28-day window. It also makes sense for people who want to test semaglutide with a smaller commitment before purchasing the larger vial. As you escalate to 1.7mg and above, the 10mg vial becomes more cost-effective because you use more peptide per week and the larger supply reduces reconstitution frequency.
Understanding what peptides are at a fundamental level helps you appreciate why vial size affects reconstitution planning. These are delicate molecules that require precise handling, and the math changes with every variable you adjust.
Injection technique after mixing
You have mixed the vial. The solution is clear. The label is on. Now you need to actually inject it. The quality of your injection technique affects how consistently the semaglutide absorbs and how comfortable the experience is over weeks and months of regular dosing.
Semaglutide is administered subcutaneously. That means the needle goes into the fat layer just beneath the skin, not into the muscle. Subcutaneous injection provides slow, steady absorption over hours, which matches the pharmacokinetic profile that makes once-weekly dosing effective. Understanding what a peptide injection involves removes much of the anxiety for first-timers.
Where to inject
Three primary sites for subcutaneous injection of semaglutide.
Abdomen. The most common site. Inject at least 2 inches (5 centimeters) away from the navel in any direction. The fatty tissue in the abdominal area provides consistent absorption and is easy to pinch for injection. Avoid areas with scars, bruises, stretch marks, or moles.
Thigh. The front or outer area of the upper thigh. Stay away from the inner thigh and knee area. Thigh injections can be slightly more painful than abdominal injections for some people due to less subcutaneous fat in the thigh compared to the abdomen.
Upper arm. The back of the upper arm, in the fatty area between the shoulder and elbow. This site is harder to self-inject because of the awkward angle, so some people have a partner assist with arm injections.
Rotation schedule
Do not inject in the same spot every week. Repeated injections in one location cause lipodystrophy, which is a change in the fat tissue under the skin that can appear as a lump or dent. It also reduces absorption consistency over time.
The recommended approach: rotate between your three injection sites (abdomen, right thigh, left thigh, right arm, left arm). Wait at least 4 weeks before returning to the same specific spot. Within each site, vary the exact injection point by at least 1 inch from the previous injection.
A simple system: Week 1, left abdomen. Week 2, right abdomen. Week 3, left thigh. Week 4, right thigh. Week 5, back to left abdomen but 1 inch from the Week 1 spot. This rotation ensures consistent absorption while protecting your tissue. The peptide injection pen guide covers rotation strategies in greater detail for those using pen-style injection devices.
Proper subcutaneous technique
Wash your hands. Swab the injection site with an alcohol pad. Let it dry completely; injecting through wet alcohol causes stinging.
Pinch a fold of skin and fat between your thumb and forefinger. This lifts the subcutaneous layer away from the muscle beneath. Insert the needle at a 45 to 90 degree angle (90 degrees if you have a good pinch of fat, 45 degrees if you are leaner at the injection site). Push the needle in smoothly, do not jab. Inject slowly, taking about 5 seconds to push the plunger fully. Hold the needle in place for 5 to 10 seconds after the plunger is fully depressed to allow the solution to disperse into the tissue.
Withdraw the needle and release the skin pinch. Do not rub the injection site. A small drop of blood at the injection point is normal and nothing to worry about. Apply light pressure with a clean cotton ball if needed.
Dispose of the syringe in a proper sharps container. Never recap and reuse needles. The list of injectable peptides all follow this same general injection technique, so mastering it once applies across your entire peptide toolkit.
Semaglutide 5mg mixing chart compared to tirzepatide mixing
If you are comparing GLP-1 agonists, you have likely looked at both semaglutide and tirzepatide. These two peptides dominate the weight loss peptide conversation, and their reconstitution processes share similarities while differing in important ways.
The semaglutide vs tirzepatide comparison covers the pharmacological differences in depth. Here, we focus on the mixing differences.
Tirzepatide is a dual GIP/GLP-1 receptor agonist, meaning it activates two incretin receptors instead of one. This dual mechanism does not change the reconstitution process, but it does change the dosing. Tirzepatide uses different milligram doses (2.5mg, 5mg, 7.5mg, 10mg, 12.5mg, 15mg) than semaglutide (0.25mg, 0.5mg, 1.0mg, 1.7mg, 2.4mg).
Because of these higher absolute doses, tirzepatide vials typically contain more peptide (5mg, 10mg, 15mg, or 30mg per vial). The tirzepatide reconstitution chart uses different water volumes and produces different concentrations than semaglutide charts.
Factor | Semaglutide 5mg | Tirzepatide 5mg |
|---|---|---|
Receptor targets | GLP-1 only | GIP + GLP-1 |
Typical starting dose | 0.25mg/week | 2.5mg/week |
Common reconstitution | 5mg + 2mL = 2.5mg/mL | 5mg + 1mL = 5mg/mL |
Doses at starting level | 20 doses | 2 doses |
Max dose | 2.4mg/week | 15mg/week |
Injection frequency | Once weekly | Once weekly |
The critical takeaway: do not use a semaglutide mixing chart for tirzepatide or vice versa. Even when the vial sizes are the same (both 5mg), the intended doses are completely different, and the resulting syringe readings have no overlap. A 0.25mg dose of semaglutide is therapeutic. A 0.25mg dose of tirzepatide is sub-therapeutic by an order of magnitude.
If you are considering tirzepatide, the tirzepatide reconstitution guide provides the same level of detail for that peptide as this guide provides for semaglutide. The tirzepatide dosage in units conversion follows similar principles but with different numbers entirely.
For those switching between the two, the semaglutide to tirzepatide dose conversion chart translates between the two dosing systems. The switching from semaglutide to tirzepatide dosage chart provides a week-by-week transition plan. The semaglutide vs tirzepatide comparison tool on SeekPeptides gives you a side-by-side look at both options.
When to adjust your concentration
Your mixing chart is not permanently locked once you choose a concentration. As you progress through the dose escalation, your ideal concentration may change. Recognizing when to switch prevents wasted peptide and improves dosing accuracy.
Signs you need a more concentrated solution
If your injection volume exceeds 0.5mL (50 units) at your current dose, you are drawing a large amount of liquid from each dose. Large injection volumes can cause more discomfort at the injection site and may absorb less consistently than smaller volumes. This happens when you use a dilute concentration (like 2mg/mL) and escalate to higher doses.
The fix: when you reconstitute your next vial, add less water. Moving from 2.5mL (2mg/mL) to 2mL (2.5mg/mL) or even 1mL (5mg/mL) reduces your injection volume while keeping the milligram dose identical.
Signs you need a more dilute solution
If your dose requires fewer than 5 units on the syringe, measurement precision becomes challenging. The difference between 4 units and 5 units represents a 20% dose variation. At very small volumes, even a steady-handed person struggles to hit the exact mark consistently.
The fix: add more water next time you reconstitute. Moving from 1mL (5mg/mL) to 2mL (2.5mg/mL) doubles your syringe reading for the same milligram dose, making precision easier.
Switching concentrations mid-protocol
You cannot change the concentration of an already-reconstituted vial. Adding more water later dilutes the solution but also introduces contamination risk and changes the benzyl alcohol concentration. If you want a different concentration, wait until your current vial is depleted or expired, then reconstitute the new vial with your preferred water volume.
When you do switch, update your chart immediately. Write the new concentration on the vial label. Recalculate your syringe readings. The semaglutide dosage calculator makes this recalculation instant.
People sometimes ask why they are not losing weight on semaglutide, and a surprising number of times the answer traces back to a concentration mismatch. They switched vials, changed their water volume without updating their chart, and have been injecting the wrong dose for weeks without realizing it. Understanding how long semaglutide takes to work requires knowing that you are actually receiving the correct dose in the first place.
The question of how long semaglutide takes to suppress appetite is closely tied to dose accuracy. If your concentration is off and you are underdosing, appetite suppression will be delayed or absent entirely. Proper reconstitution is not just about following steps. It is about ensuring every injection delivers exactly what you intend.
Frequently asked questions
How much bacteriostatic water do I add to 5mg semaglutide?
The most common volume is 2mL, which creates a concentration of 2.5mg/mL. This provides clean syringe readings for standard dose escalation amounts. You can also add 1mL for a 5mg/mL concentration (smaller injection volumes, harder to measure precisely) or 2.5mL for a 2mg/mL concentration (larger injection volumes, easier to measure but less convenient at high doses). The bacteriostatic water guide for peptides explains why BAC water specifically is the correct choice over other diluents. You can verify your chosen ratio using the free peptide reconstitution calculator.
How many units is 0.25mg of semaglutide?
It depends on your concentration. At 2.5mg/mL (5mg + 2mL water), 0.25mg equals 10 units. At 5mg/mL (5mg + 1mL water), 0.25mg equals 5 units. At 2mg/mL (5mg + 2.5mL water), 0.25mg equals 12.5 units. Always check the chart that matches your specific reconstitution before drawing any dose. The semaglutide reconstitution chart provides the full reference for all concentrations.
Can I use sterile water instead of bacteriostatic water?
Sterile water can technically dissolve the peptide, but it does not contain the 0.9% benzyl alcohol preservative found in bacteriostatic water. Without that preservative, bacteria can grow in the solution after the first needle puncture. Since a 5mg vial is a multi-dose vial that you will access multiple times over days or weeks, bacteriostatic water is the correct and safe choice. If you use sterile water, you should use the entire vial contents in one session, which is impractical for semaglutide dosing.
How long does mixed semaglutide last?
Reconstituted semaglutide lasts 28 days when stored properly at 2 to 8 degrees Celsius in a refrigerator. After 28 days, discard any remaining solution. The shelf life of reconstituted peptides in the fridge depends on proper storage practices and the type of diluent used. Bacteriostatic water maximizes this shelf life compared to sterile water or saline.
What if I added too much water?
If you added more water than intended, your concentration is lower than planned. Do not add more peptide or try to remove water. Instead, recalculate your concentration using the formula: peptide amount (5mg) divided by total water volume equals your new concentration. Then update your syringe readings accordingly. The peptide calculator can handle this recalculation instantly. Your peptide is not wasted. It is just more dilute, which means you draw more units per dose.
How do I know if my semaglutide is still good?
A properly reconstituted and stored solution should remain crystal clear throughout its 28-day life. Any cloudiness, visible particles, color change, or unusual smell indicates degradation. If the solution was clear yesterday and cloudy today, do not inject it. The most common cause of premature degradation is temperature excursion, either the vial warming to room temperature for too long or accidental freezing. Understanding whether you can use expired semaglutide also applies to solutions that show degradation signs before the 28-day mark.
Can I freeze reconstituted semaglutide?
No. Freezing reconstituted semaglutide damages the peptide structure. The formation of ice crystals within the solution physically disrupts the peptide chains, potentially reducing or eliminating potency. Lyophilized (freeze-dried) powder can tolerate cold temperatures because it has already been processed to survive the freeze-dry cycle. But once reconstituted, the peptide is in a fragile aqueous state that does not survive freezing. Always store between 2 and 8 degrees Celsius. Never place reconstituted peptides in the freezer. The peptide storage guide covers all storage do and do not guidelines.
What concentration is best for the 5mg vial?
For most people, 2.5mg/mL (achieved by adding 2mL of bacteriostatic water) is the best concentration. It provides clean syringe readings for all standard escalation doses, manageable injection volumes even at higher doses, and a good balance between measurement precision and practicality. The 5mg/mL option (1mL water) is better for very low doses where you want minimal injection volume. The 2mg/mL option (2.5mL water) is rarely the best choice due to uneven syringe readings and excessive volume at higher doses. Visit SeekPeptides for interactive tools that help you determine the optimal concentration for your specific dosing needs.
Beyond the mixing chart: building your full peptide knowledge
A mixing chart is a starting point. It tells you how much water to add and how many units to draw. But effective peptide use requires a broader foundation of knowledge that extends well beyond reconstitution.
Understanding the broader landscape of peptide dosage charts helps you see how semaglutide fits within the larger family of research peptides. Each peptide has its own dosing range, reconstitution requirements, and administration schedule. Semaglutide is weekly. Some peptides are daily. Some are twice daily. Some are cycled with weeks on and weeks off. The peptide dosing guide provides an overview of how different peptides are dosed and why.
If weight management is your primary goal, semaglutide is one of several peptides in the GLP-1 agonist category. The best peptide stack for weight loss might include complementary compounds that address different aspects of metabolism, appetite, and body composition. The peptide stack calculator helps you plan multi-peptide protocols while keeping dosing manageable.
Some people combine semaglutide with B12 supplementation. The semaglutide with B12 guide and the semaglutide B12 dosage chart cover that combination in detail. Others are exploring newer compounds like retatrutide or cagrilintide combined with semaglutide (the combination known as CagriSema). The amylin receptor agonist class represents yet another pathway being explored for weight management.
Whether you are using semaglutide alone or as part of a broader protocol, the reconstitution accuracy you build from this mixing chart carries forward to everything else. Getting the basics right, measuring carefully, storing properly, rotating injection sites, these habits protect your investment and your health across any peptide you work with. The complete peptide list gives you a comprehensive overview of what is available in the research peptide space.
For those exploring alternatives to traditional pharmaceutical weight loss options, the Ozempic alternatives guide covers the broader landscape. And if you want to understand how peptides compare across different delivery methods, the injectable vs oral peptides comparison explains the bioavailability and absorption differences between routes of administration.
The peptide cycle planning guide helps you map out long-term use, including when to take breaks and how to structure ongoing protocols. And if you are curious about whether you can cycle different peptides together or in sequence, that guide addresses the practical considerations.
Learning about peptide legality ensures you understand the regulatory landscape. And for those who prefer non-injectable options, nasal spray peptides and sublingual peptides offer alternative delivery methods for certain compounds (though semaglutide specifically is most effective via subcutaneous injection).
Understanding the distinction between research and pharmaceutical peptides also matters when sourcing your supplies. And for those exploring peptides beyond weight management, the peptides for fat loss page, peptides for muscle growth page, peptides for gut health page, and peptides for anti-aging page each cover the compounds most relevant to those goals.
The peptide stacks guide goes deeper into combining multiple peptides effectively. For weight-specific stacking, the peptide calculator for weight loss dosing helps you dial in the numbers. And for a broader overview of women-specific considerations, the peptides for weight loss in women guide addresses hormonal and physiological factors that influence protocol design.
The bioactive precision peptides for weight loss article explores the science behind targeted peptide approaches. And for anyone interested in accessing professional guidance, online peptide therapy is becoming an increasingly accessible option.
Understanding the GLP-3 receptor pathway is also relevant context, as the GLP-3 peptide overview explains the next frontier in incretin-based research. And for side-by-side dosing comparisons between semaglutide and tirzepatide, the tirzepatide vs semaglutide dosage chart lays out the differences clearly.
Additional tirzepatide resources include the tirzepatide compound dosage chart, the tirzepatide dose chart, the tirzepatide dosage chart in mL, and the microdosing tirzepatide chart for those exploring that compound alongside semaglutide.
The conversion guides for tirzepatide are equally important if you use both compounds: how many units is 5mg of tirzepatide, how many mg is 40 units of tirzepatide, and how many mg is 20 units of tirzepatide each address common conversion questions.
For the broader tirzepatide picture, the how fast tirzepatide works article, the tirzepatide dosing guide, and the tirzepatide dosing for weight loss in units round out the reference library. And the semaglutide to tirzepatide conversion chart and compound tirzepatide dosage chart are essential for anyone managing both peptides.
Lifestyle factors also affect your semaglutide results. The question of whether you can drink alcohol on semaglutide is one that comes up frequently. And understanding the compounded semaglutide landscape helps you make informed sourcing decisions.
For those curious about semaglutide withdrawal symptoms, that guide covers what happens when you stop and how to manage the transition. And understanding how long peptides take to work in general provides realistic expectations across compounds.
Finally, the peptide safety and risks overview should be required reading for anyone managing their own reconstitution. Safety is not just about sterile technique. It encompasses sourcing, storage, dosing accuracy, and knowing when to seek professional guidance. SeekPeptides members access comprehensive safety protocols, dosage guides, and interactive tools that make managing peptide protocols simpler and safer. If you are serious about doing this correctly, membership provides the structured knowledge base that turns scattered research into organized, actionable protocols.
The difference between lyophilized and liquid peptides is also worth understanding, as it directly affects reconstitution requirements. Lyophilized peptides like semaglutide require the mixing process covered in this guide, while liquid peptides arrive pre-reconstituted. Each format has trade-offs in shelf life, stability, and convenience.
External resources
PubMed Central: Semaglutide pharmacokinetics and dose-response relationship
PubMed: STEP 1 trial, semaglutide 2.4mg for weight management
In case I do not see you, good afternoon, good evening, and good night. May your reconstitutions stay precise, your concentrations stay accurate, and your results stay consistent.