Mar 18, 2026

Before you move your injection day forward by two full days, there is one number you need to know. Seventy-two. That is the minimum number of hours the FDA requires between tirzepatide doses, and taking your shot two days early puts you right at the edge of that boundary. Maybe even past it.
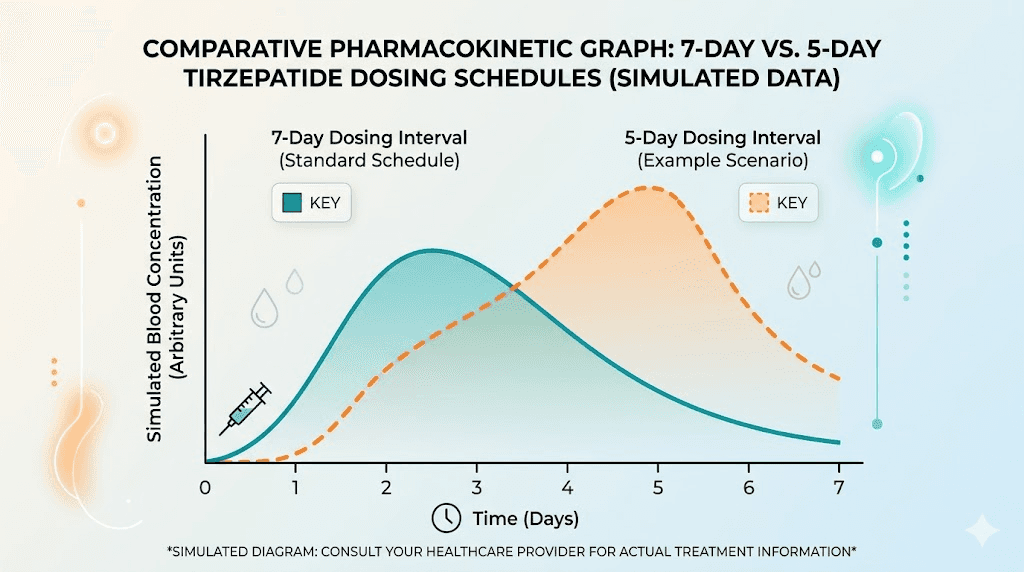
Here is what makes this question different from simply taking tirzepatide a day early. One day early gives you a comfortable six-day gap. Two days early? That shrinks your window to five days, roughly 120 hours. Still technically above the 72-hour minimum. But the math changes depending on when you injected your last dose, what time of day you normally inject, and whether you are accounting for the full picture or just counting calendar days.
This matters because tirzepatide has a half-life of approximately five days. When you shorten the interval between doses, you increase the overlap of drug concentrations in your system. That overlap is exactly what the 72-hour rule is designed to prevent. Too much overlap means more gastrointestinal side effects, stronger appetite suppression than intended, and in rare cases, complications that require medical attention.
This guide breaks down exactly what happens pharmacologically when you take tirzepatide two days ahead of schedule, how to calculate whether your specific timing is safe, what side effects to watch for, and how to properly adjust your injection schedule without putting yourself at risk.
SeekPeptides has compiled every guideline, clinical data point, and practical scenario you need to make an informed decision.
The 72-hour rule and why it exists
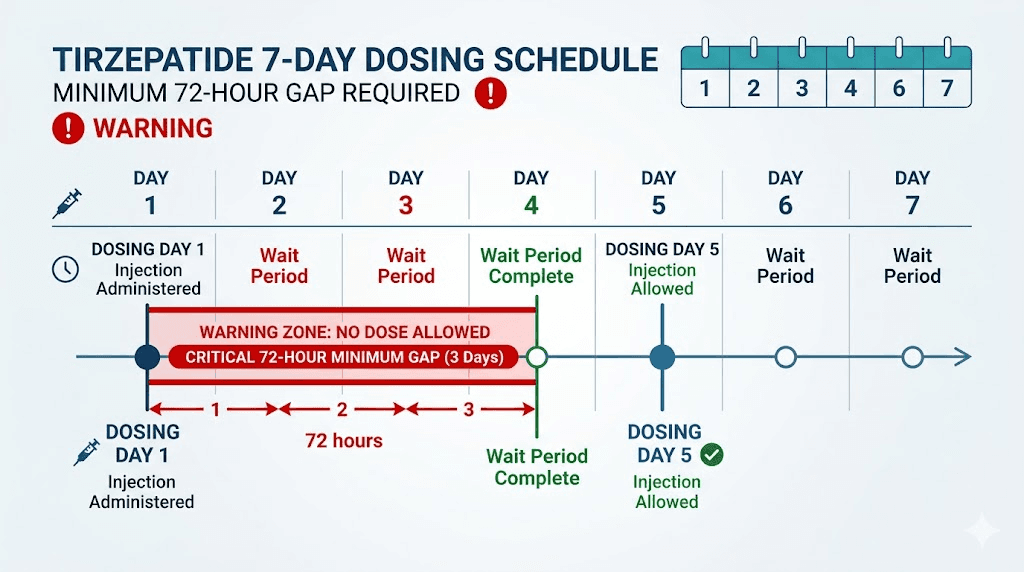
The FDA prescribing information for both Mounjaro and Zepbound states one requirement clearly. Doses must be separated by at least 72 hours. Three full days. This is not a suggestion or a best practice. It is the minimum safe interval established through clinical trials involving thousands of participants.
Why 72 hours specifically?
Tirzepatide is a dual GIP and GLP-1 receptor agonist with a long pharmacological half-life. After you inject a dose, the drug reaches peak plasma concentration within 8 to 72 hours. From there, it takes approximately five days for your body to eliminate half of the active compound. At the standard seven-day interval, roughly 30 to 40 percent of the previous dose remains circulating when you inject again. This creates a predictable steady-state concentration that your body adapts to over the first four weeks of treatment.
Shorten that interval, and the math shifts. More drug accumulates. Side effects intensify. The dose-response curve that your healthcare provider carefully calibrated when setting your starting dose no longer applies in the same way.
The 72-hour minimum prevents what pharmacologists call supratherapeutic drug levels, concentrations that exceed the intended therapeutic range. At those elevated levels, the gastrointestinal effects that many people already find challenging can become significantly worse.
Two days early vs one day early: understanding the difference
Taking tirzepatide one day early means injecting on day six instead of day seven. That leaves a 144-hour gap between doses. Well above the 72-hour minimum. No safety concerns at all.
Two days early is different.
Injecting on day five instead of day seven leaves a 120-hour gap. Still above 72 hours. Still technically within the safe window. But the margin shrinks considerably, and the amount of drug remaining from your previous dose is meaningfully higher than it would be at the standard seven-day mark.
Here is how the numbers break down at different intervals, assuming a standard weekly dose:
Timing | Hours between doses | Approximate drug remaining from previous dose | Safety status |
|---|---|---|---|
On schedule (day 7) | 168 hours | 30-40% | Standard |
1 day early (day 6) | 144 hours | 35-45% | Safe |
2 days early (day 5) | 120 hours | 40-55% | Within limits but elevated |
3 days early (day 4) | 96 hours | 50-65% | Borderline, not recommended |
4 days early (day 3) | 72 hours | 60-75% | Absolute minimum |
At the two-day-early mark, you have roughly 40 to 55 percent of your previous dose still active. That is 10 to 15 percentage points higher than the steady-state level your body has adapted to. For most people on lower doses like 2.5 mg or 5 mg, this increased overlap may cause only mild additional nausea. For those on higher doses like 10 mg or 15 mg, the effects can be more pronounced.
Tirzepatide pharmacokinetics: what your body does with each dose
Understanding why dose timing matters requires a basic grasp of how tirzepatide moves through your body. The pharmacokinetics are not complicated, but they explain everything about why the 72-hour rule exists and what happens when you compress your dosing schedule.
Absorption phase
After subcutaneous injection, tirzepatide absorbs slowly from the injection site. Peak plasma concentrations arrive anywhere from 8 to 72 hours post-injection, with most people hitting peak levels around 24 to 48 hours. This slow absorption is by design. The drug binds to albumin in the blood, creating a depot effect that extends its duration of action.
Where you inject matters too. The abdomen typically provides the most consistent absorption rates. The thigh can be slightly slower. Either way, the drug enters circulation gradually rather than all at once.
Distribution and binding
Once absorbed, tirzepatide binds extensively to plasma albumin, with approximately 99 percent protein binding. This high binding rate is what gives the drug its long half-life. Only unbound drug is pharmacologically active, so the albumin-bound reservoir acts as a slow-release mechanism that maintains therapeutic levels between weekly doses.
The volume of distribution is approximately 10.3 liters, which means the drug stays primarily in the bloodstream rather than distributing widely into tissues. This concentration in plasma is relevant because it means earlier dosing creates a more immediate spike in active drug levels than it would for a drug that distributes broadly into fat or muscle tissue.
Elimination and the five-day half-life
Tirzepatide has a terminal half-life of approximately five days (120 hours). This means that five days after injection, half of the drug remains. After ten days, roughly a quarter remains. After fifteen days, about an eighth.
At steady state, which is reached after approximately four weeks of weekly dosing, the accumulation ratio is about 1.6-fold compared to a single dose. This means your trough level (the lowest point before your next injection) is significantly higher than it was during your first few weeks of treatment.
When you take a dose two days early, you are injecting at a point where your drug levels are still relatively high. Instead of the normal trough, you are closer to the mid-decline phase. The new dose stacks on top of higher residual levels, temporarily pushing your peak concentration above the steady-state range your body has calibrated to.
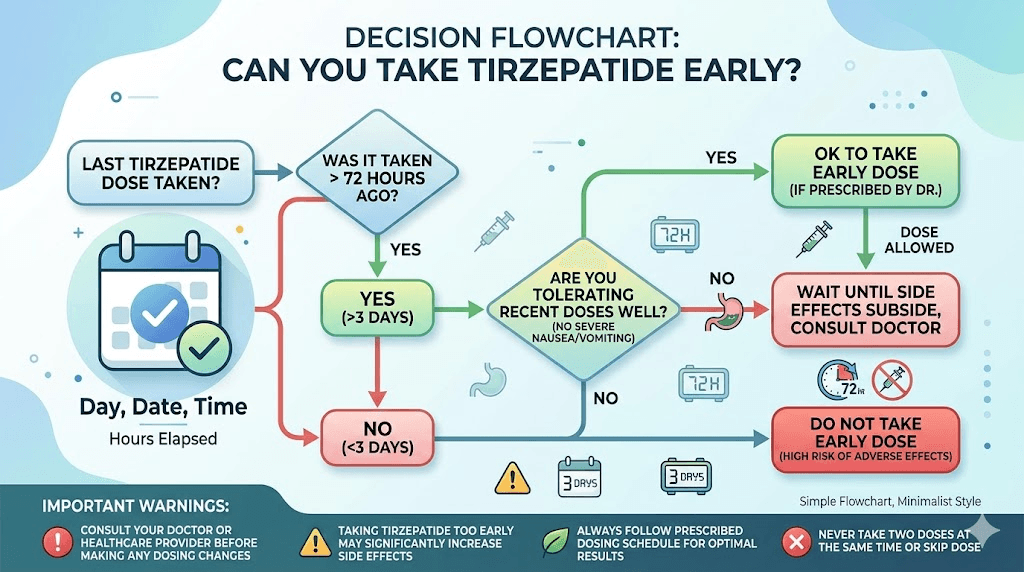
What happens when you take tirzepatide 2 days early
The short answer: for most people at lower to moderate doses, taking tirzepatide two days early on a single occasion is unlikely to cause serious harm. You remain above the 72-hour minimum. Your drug levels will be elevated but not dramatically so.
The longer answer involves what you might actually feel.
Increased gastrointestinal effects
Tirzepatide works partly by slowing gastric emptying, the rate at which food moves from your stomach into your small intestine. This delayed emptying is what creates the prolonged feeling of fullness that helps with weight loss. But it is also what causes constipation, bloating, nausea, and diarrhea in many users.
At higher drug concentrations, gastric emptying slows even further. Clinical trial data shows that nausea affects approximately 20 percent of tirzepatide users at standard dosing intervals. Vomiting occurs in about 9 percent. These rates were established with proper seven-day spacing.
With compressed dosing, the GI effects can intensify temporarily. Many users report that taking a dose even slightly early leads to a day or two of stronger nausea than they normally experience. The effect is typically self-limiting, resolving as drug levels return to their normal range.
Stronger appetite suppression
If you are already experiencing significant appetite suppression at your current dose, taking it two days early can push that suppression into uncomfortable territory. Some people report having essentially no desire to eat for 48 to 72 hours after an early dose, which can lead to inadequate nutrition and fatigue.
This is why maintaining proper nutrition matters even more when your dosing schedule shifts. Having a solid meal plan and knowing what to eat on tirzepatide becomes critical during periods of intensified appetite suppression.
Potential blood sugar effects
For people using tirzepatide for type 2 diabetes management, the blood sugar implications of early dosing are more significant. Higher drug concentrations mean stronger glucose-lowering effects. If you are also taking insulin or sulfonylureas, the combined effect can increase hypoglycemia risk.
This is one reason the FDA specifically warns against doses closer than 72 hours. The glucose-lowering effect of tirzepatide is dose-dependent, and temporarily elevated levels can drop blood sugar below safe ranges, especially overnight or between meals.
Injection site considerations
An often-overlooked factor is injection site reactions. When you inject sooner than usual, the previous injection site may not have fully recovered. Using the same general area can increase the risk of redness, itching, and irritation. Always rotate your injection site, especially when adjusting your schedule. If you normally inject in the abdomen, switch to the thigh, or vice versa.
How to calculate your exact gap between doses
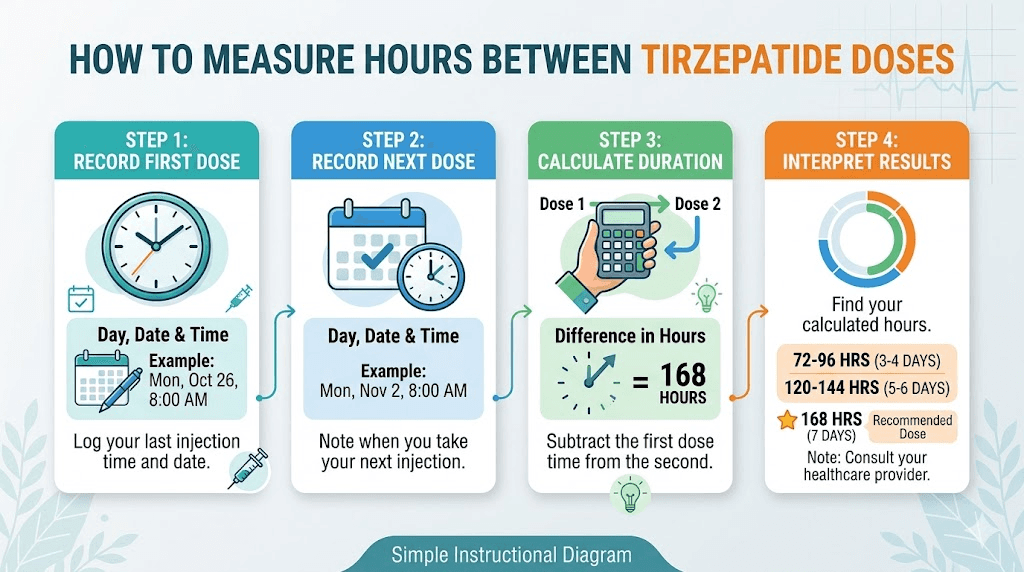
Calendar days can be misleading. What matters is actual hours between injections. Here is how to figure out whether your specific timing falls within safe parameters.
Step 1: note your exact injection time
If you injected your last dose on Monday at 8 AM, your clock starts at Monday 8 AM. Not Monday midnight. Not Monday generally. The exact time matters when you are working with compressed schedules.
Step 2: calculate 72 hours forward
From Monday at 8 AM, 72 hours lands on Thursday at 8 AM. That is your absolute earliest safe injection time. Anything before Thursday 8 AM violates the 72-hour minimum.
Step 3: calculate your proposed early injection time
If your next dose is normally scheduled for Wednesday the following week at 8 AM, and you want to take it on Monday at 8 AM instead (two days early), your gap is: Wednesday 8 AM minus five days equals Saturday 8 AM of the previous week. Wait. Let me simplify this.
Here is the clearer version. You injected on Wednesday at 8 AM. Your next dose is the following Wednesday. You want to inject on Monday instead. Wednesday 8 AM to Monday 8 AM is 120 hours (five full days). That is well above 72 hours. Safe.
But if you injected on Wednesday at 8 PM and want to inject on Monday at 8 AM, your gap is only 108 hours. Still safe, but the margin narrows.
Step 4: account for steady-state effects
If you have been on tirzepatide for more than four weeks, you are at steady state. Your body has accumulated drug to a predictable level. Any shortening of the interval adds to that accumulated load. A single two-day-early dose will not dramatically change your steady-state levels, but doing it repeatedly will shift your effective average concentration upward over time.
Use the GLP-1 plotter tool to visualize how dose timing affects your drug levels. These calculators model the pharmacokinetic curve and show exactly where your concentration sits at any point between doses.
Safe ways to permanently change your tirzepatide injection day
Sometimes you do not just need a one-time early dose. You need to permanently move your injection day. Maybe your work schedule changed. Maybe you realized that injecting at a different time reduces your side effects. Maybe travel plans demand a new routine. Whatever the reason, there is a right way to do it.
The forward shift method (moving your day earlier)
To move your injection day earlier in the week, you simply take your next dose on the new preferred day, ensuring at least 72 hours have passed since your last injection. Then continue on the new day going forward.
Example: you currently inject on Sundays and want to switch to Fridays.
Inject on Sunday as normal
Wait until Friday (five days later, 120 hours)
Inject on Friday
Continue every Friday going forward
That initial five-day gap is shorter than your usual seven days, but it is well above the 72-hour minimum. After one cycle, your body adjusts and you are back to a consistent weekly rhythm on the new day.
The backward shift method (moving your day later)
Moving your injection day later is actually easier from a safety perspective. You simply wait a few extra days. Your drug levels will drop slightly lower than usual during the extended interval, but this is not dangerous. You might notice a slight return of appetite or reduced efficacy for a day or two.
Example: switching from Wednesday to Saturday.
Inject on Wednesday as normal
Wait until Saturday (ten days later)
Inject on Saturday
Continue every Saturday
The ten-day gap means your drug levels will be lower when you resume, but a single longer interval does not undo your progress. Your weight loss trajectory continues once regular dosing resumes.
When time of day matters
Many people ask about the best time to take their tirzepatide shot. Research suggests that evening injections may reduce nausea by 15 to 20 percent because GI side effects peak one to three hours post-injection and you sleep through the worst of them. If you are changing your injection day, consider also optimizing your injection time.
Some users find that injecting at night produces fewer daytime side effects overall. Others prefer morning injections so they can monitor for any reactions during waking hours. There is no pharmacological reason one time is better than another in terms of drug efficacy. The long half-life ensures consistent drug levels regardless of injection time.
The missed dose protocol: what the FDA actually says
Understanding the missed dose protocol helps put the "two days early" question in perspective. The FDA guidelines work in both directions, covering both late and early dosing scenarios.
If you miss a dose by less than 4 days (96 hours)
Take the missed dose as soon as you remember. Then return to your regular weekly schedule. You do not need to adjust your dose or skip the following week.
This 96-hour window is important because it tells us something about the drug manufacturer safety margin. If you can safely take a dose up to four days late (making the gap as long as eleven days), the pharmacological profile clearly supports some flexibility in timing.
If you miss a dose by more than 4 days
Skip the missed dose entirely. Take your next dose on the regularly scheduled day. Do not double up. Taking two doses close together to "catch up" is never recommended and significantly increases the risk of severe side effects.
What this tells us about early dosing
The missed dose guidelines reveal that the acceptable dosing window ranges from a minimum of 72 hours to a maximum of roughly 11 days (168 + 96 hours). Your normal seven-day interval sits comfortably in the middle. Taking a dose two days early (120 hours) puts you within the acceptable range but closer to the lower boundary.
The key takeaway: occasional two-day-early dosing is pharmacologically tolerable, but it should not become your regular pattern. Repeated compression of the dosing interval effectively increases your average weekly drug exposure beyond what was prescribed.
Common scheduling scenarios and exactly what to do
Real life does not follow perfect seven-day cycles. Here are the most common scenarios people encounter and the safest approach for each one.
Scenario 1: upcoming travel requires early injection
You normally inject on Wednesdays, but you are flying internationally on Tuesday and do not want to deal with traveling with tirzepatide through airport security. Can you inject on Monday instead?
Answer: Yes. Monday to the following Wednesday is 120 hours. Above the 72-hour minimum. Inject Monday, skip your Wednesday dose, and resume the following Wednesday. Or, if you prefer, inject Monday and make Monday your new injection day going forward.
Scenario 2: you forgot and need to get back on schedule
You normally inject on Fridays. You forgot last Friday and remembered on Sunday. Now you want to take Sunday's late dose but also get back to Fridays next week.
Answer: Take the dose Sunday. Then wait until the following Friday (five days later, 120 hours). That gets you back on your Friday schedule with one slightly short interval that remains above the 72-hour minimum.
Scenario 3: upcoming surgery
Your surgeon wants you to stop tirzepatide before a procedure because of the gastroparesis risk during anesthesia. You want to take one last dose before your medication break.
Answer: Many surgeons recommend stopping GLP-1 medications two to three weeks before surgery due to delayed gastric emptying concerns. If you are planning around surgery, discuss the exact timing with your surgical team. Taking a dose early to squeeze one more in before your break is generally acceptable if you maintain the 72-hour minimum, but always confirm with your prescriber.
Scenario 4: you want to align with your partner or friend
Some people on GLP-1 medications prefer to inject on the same day as someone they know for accountability and support. Moving your injection day forward by one or two days to match another person is safe as a one-time adjustment, provided you respect the 72-hour gap.
Scenario 5: dose escalation timing
You are about to increase from 5 mg to 7.5 mg. Should you take the higher dose early to start seeing results sooner?
Answer: No. Dose escalation already increases your drug exposure. Combining a higher dose with a shortened interval compounds the increase. Always start a new dose on your regular schedule day. The standard protocol calls for dose increases every four weeks at minimum, and rushing this process is one of the most common reasons people experience severe headaches, fatigue, and intense nausea.
Side effects to watch for after taking tirzepatide early
If you have already taken your dose two days early, or you plan to, here is what to monitor in the 24 to 72 hours following injection.
Mild side effects (expected, manageable)
These are intensified versions of normal tirzepatide side effects and do not require medical attention unless they become severe or persistent.
Nausea: May be stronger than usual. Eat small, bland meals. Avoid fatty or fried foods. See our guide on foods to avoid on tirzepatide
Bloating and fullness: Slower gastric emptying at higher concentrations means food sits longer in your stomach
Constipation: Drink extra water and consider fiber supplementation
Decreased appetite: More pronounced than normal. Make sure you are still eating adequate protein
Fatigue: Common with elevated drug levels. Rest as needed
Sulfur burps: May increase in frequency or intensity
Moderate side effects (worth monitoring)
Headaches: Can indicate dehydration or blood sugar fluctuations. Stay hydrated. See tirzepatide headache treatment options
Diarrhea: If persistent for more than 48 hours, contact your provider
Body aches and muscle pain: Occasionally reported with higher concentrations
Dry mouth: Stay well-hydrated throughout the day
Insomnia or sleep disruption: May occur with elevated drug levels
Serious side effects (seek medical attention)
These are rare but possible, especially at supratherapeutic concentrations.
Severe, persistent vomiting: If you cannot keep fluids down for more than 24 hours
Signs of pancreatitis: Severe abdominal pain radiating to the back, often with vomiting
Hypoglycemia symptoms: Shakiness, confusion, sweating, rapid heartbeat. Particularly relevant if you take other diabetes medications
Severe injection site reaction: Extensive redness, swelling, or warmth at the injection site. See our injection site reaction treatment guide
Gallbladder symptoms: Upper right abdominal pain, especially after eating
The vast majority of people who take a single dose two days early will experience only the mild category of side effects, if any. The serious side effects listed above are extremely uncommon with a single compressed interval and are more associated with chronic overdosing or underlying medical conditions.
If you do experience side effects after an early dose, remember that they are temporary. The elevated drug levels that cause them will decline over the following days as normal elimination continues. Taking over-the-counter anti-nausea medication, staying well-hydrated, and resting can help manage the acute phase. Do not compensate by skipping your next scheduled dose unless a healthcare provider specifically instructs you to do so. One compressed interval followed by one normal interval will quickly return your drug levels to their usual steady-state range.
What the clinical trial data tells us about dose timing
The pivotal SURMOUNT and SURPASS clinical trials that led to tirzepatide approval provide the best data on dosing consistency and outcomes.
SURMOUNT-1 results
In this 72-week obesity trial, participants receiving tirzepatide achieved remarkable weight loss results:
5 mg dose: 85% achieved at least 5% weight reduction, with average weight loss of 15%
10 mg dose: 89% achieved at least 5% weight reduction, with average weight loss of 19%
15 mg dose: 91% achieved at least 5% weight reduction, with average weight loss of 21%
These results were achieved with consistent weekly dosing. The trial protocol allowed for minor schedule adjustments (the 72-hour minimum), and the results reflect real-world adherence patterns where participants occasionally shifted their injection days.
What the data tells us about irregular dosing
While the trials were designed around strict weekly dosing, adherence data shows that not every participant hit their exact injection day every single week. The built-in pharmacological buffer (the five-day half-life) provides some protection against minor timing variations.
However, no trial specifically studied the effects of routinely shortened intervals. The safety data applies to occasional timing variations, not to systematic early dosing. If you find yourself consistently wanting to inject early, it may signal that your dose needs adjustment. Talk to your prescriber about whether a dose increase is appropriate.
Why you might feel the urge to dose early
Before we go further, it is worth examining why someone would want to take their tirzepatide before the scheduled day. Understanding the underlying reason helps determine the right solution.
Appetite returning before injection day
This is the most common reason. By day five or six, the appetite-suppressing effects start to wane. Food thoughts return. Cravings resurface. The temptation to inject early is strong because you remember how good those first few days after injection feel.
If appetite consistently returns well before your next dose, this may indicate that your current dose is not fully effective for the seven-day interval. Rather than dosing early, discuss a dose increase with your provider. The tirzepatide escalation protocol allows increases of 2.5 mg every four weeks up to the maximum dose.
In the meantime, managing hunger on tirzepatide involves nutritional strategies. High-protein meals, adequate fiber, and proper hydration can extend the appetite-suppressing effect. Your diet plan matters as much as the medication itself.
Weight loss plateau
Some people hit a plateau where tirzepatide stops working as well as it did initially. The instinct is to increase frequency rather than dose. This is not the right approach. Plateaus are normal and are better addressed through dose optimization, dietary adjustments, or exercise modifications. Taking the medication more frequently does not meaningfully improve outcomes and increases side effect risk.
If your weight loss has stalled, review your overall approach. Are you eating enough protein? Are you exercising? Sometimes the issue is not the medication at all but the surrounding habits.
Scheduling convenience
This is the most legitimate reason to take a dose early. Life happens. Vacations, work events, medical procedures, or simply wanting a different injection day. These are all valid reasons to shift your schedule, and a single two-day-early dose is a perfectly reasonable way to make the transition.
Splitting doses and alternative scheduling approaches
Some users ask about splitting their tirzepatide dose into two smaller injections per week instead of one larger weekly dose. The theory is that more frequent, smaller doses provide steadier drug levels with fewer side effect peaks.
The case for dose splitting
Split dosing has anecdotal support in online communities. The logic makes pharmacological sense: two half-doses separated by 3.5 days each would theoretically produce a flatter drug concentration curve with lower peaks and higher troughs. This could reduce GI side effects while maintaining efficacy.
However, split dosing is not FDA-approved. The clinical trials studied once-weekly injection only. Compounded formulations may have different concentration profiles that make precise splitting more feasible, but the approach remains off-label.
Microdosing as an alternative
Another approach gaining attention is microdosing tirzepatide. Rather than taking a full dose early, some users take smaller supplemental doses between their regular weekly injections. The microdosing chart and schedule guides outline various approaches people have used.
This strategy is particularly popular among those using compounded formulations where syringe dosing allows for precise volume measurements. The compound dosage charts make it relatively straightforward to calculate fractional doses.
Both split dosing and microdosing should only be undertaken with guidance from a healthcare provider. Self-adjusting your medication regimen carries risks even when the total weekly dose remains the same.
How tirzepatide compares to semaglutide on dosing flexibility
If you are considering switching medications or are curious about the differences in side effect profiles, the dosing flexibility comparison is relevant.
Semaglutide (Ozempic, Wegovy) has a similar half-life of approximately seven days, slightly longer than tirzepatide's five days. This means semaglutide levels remain more stable between doses, and the consequences of early dosing may be marginally less pronounced. The 72-hour minimum applies to both medications, but the longer half-life of semaglutide means the steady-state trough is proportionally higher, leaving less room for drug level variation.
Both medications use the same basic protocol for schedule changes and missed doses. The key differences are in their receptor profiles (tirzepatide targets both GIP and GLP-1 receptors, while semaglutide targets GLP-1 only) and their dose conversion ratios.
If you are evaluating both options, the dosage comparison chart provides a side-by-side analysis. For those alternating between medications or switching, understanding the pharmacokinetic differences is essential for safe transitions.
Special populations and considerations
Certain groups need to exercise extra caution when adjusting their tirzepatide dosing schedule.
People with type 2 diabetes
The blood sugar effects of compressed dosing are more clinically significant for diabetic patients than for those using tirzepatide purely for weight management. If you take tirzepatide alongside other glucose-lowering medications, taking your dose early creates a period of enhanced glucose reduction that can tip you into hypoglycemia. Monitor your blood sugar more frequently around any schedule change.
Older adults
Drug clearance slows with age. If you are over 65, the effective half-life of tirzepatide may be slightly longer than the population average of five days. This means drug accumulation from early dosing could be more pronounced. The 72-hour minimum remains the same, but the practical margin of safety may be narrower.
People with kidney impairment
While tirzepatide is not primarily cleared by the kidneys, renal function affects overall drug metabolism. If you have kidney disease, discuss any schedule changes with your prescriber before making adjustments. The standard 72-hour minimum may not provide the same safety margin.
Breastfeeding
If you are using tirzepatide while breastfeeding, any increase in drug concentration could theoretically affect what passes into breast milk. The data on tirzepatide in breast milk is limited. Maintaining the standard seven-day interval is particularly important in this situation.
People taking supplements or combination therapies
Many tirzepatide users take supplements alongside their medication. Common combinations include vitamin B12, glycine, niacinamide, and levocarnitine. Some compounded formulations already include these additives, such as tirzepatide with glycine and B12 or tirzepatide with methylcobalamin.
When you take a dose early, the interactions between tirzepatide and these supplements may shift slightly. B12 absorption, for instance, can be affected by the degree of gastric emptying delay. This is unlikely to be clinically significant for a single early dose, but it is worth noting if you rely on your tirzepatide combination for B12 supplementation.
If you are combining tirzepatide with other medications like phentermine or metformin, the compressed dosing interval may affect how these drugs interact. Always consult your prescriber about timing adjustments when you are on combination therapy.
Compounded tirzepatide and dosing flexibility
A significant portion of tirzepatide users obtain their medication from compounding pharmacies. The dosing flexibility considerations apply equally to compounded formulations, but there are some additional factors to consider.
Concentration differences
Compounded tirzepatide comes in various concentrations. A 10 mg vial reconstituted in different volumes of bacteriostatic water produces different concentrations. When measuring doses with an insulin syringe, the unit measurements correspond to specific milligram amounts based on your reconstitution ratio.
This matters for early dosing because the precision of your measurement affects how much drug you are actually injecting. If you use our compounded tirzepatide dosage calculator, you can verify that your intended dose matches your actual injection volume.
Stability considerations
When you take a dose early, it means your vial runs out sooner. Make sure you have enough supply to cover the shortened interval. Running out of medication mid-cycle because you dosed early is worse than the slight inconvenience of waiting the full seven days.
Check your tirzepatide shelf life and storage guidelines to ensure your medication remains potent through any schedule adjustments. Reconstituted tirzepatide should be stored in the refrigerator and used within the timeframe specified by your compounding pharmacy.
Building a consistent injection routine
The best way to avoid the "should I take it early?" dilemma is to build a routine that you can maintain consistently. Here are evidence-based strategies.
Choose the right day
Pick a day that works for your lifestyle every single week. The best day to take tirzepatide is the one you will not need to change. For many people, this means avoiding days that frequently conflict with travel, social events, or irregular schedules.
Weekdays work well for people with consistent work schedules. Weekends work for those whose weekdays vary. Some people even choose their injection day based on when they experience the most side effects, scheduling it so that the peak GI discomfort falls on their least active day.
Set reminders
Phone alarms are the simplest and most effective tool. Set one for the morning of your injection day and another for the evening if you tend to procrastinate. Some people use medication tracking apps that provide persistent reminders until the dose is logged.
Prepare your supplies in advance
If you use compounded tirzepatide, having your supplies ready reduces friction. Know your reconstitution process, have your syringes ready, and keep your bacteriostatic water stocked. The more seamless the injection process, the less likely you are to delay and then feel pressured to dose early the following week.
Plan around known disruptions
If you know a vacation, work trip, or medical procedure is coming, adjust your schedule proactively. A planned, deliberate two-day-early dose with full awareness of the 72-hour rule is infinitely safer than a last-minute panicked injection.
For travel, review our guide on traveling with tirzepatide well in advance. Proper storage during travel and temperature management are just as important as dose timing.
When to call your healthcare provider
Most dose timing adjustments do not require a provider consultation. But certain situations warrant professional guidance before you make changes.
Call your provider if:
You want to make early dosing a regular pattern (this may indicate dose optimization is needed)
You are on other diabetes medications and plan to shift your schedule
You experienced severe side effects after a previous early dose
You are considering splitting your dose or microdosing
You have kidney, liver, or gallbladder conditions
You are pregnant, planning pregnancy, or breastfeeding
You plan to stop tirzepatide soon and want guidance on tapering
You do not need to call for:
A single one-time early dose that maintains the 72-hour minimum
A permanent schedule change that respects the 72-hour transition gap
Taking your dose a few hours early or late on your regular injection day
Long-term dosing consistency and weight loss outcomes
Research consistently shows that dosing consistency correlates with better weight loss outcomes. The tirzepatide weight loss timeline follows a predictable pattern when dosing is consistent: steady loss during the escalation phase, accelerated loss at therapeutic doses, and eventual stabilization at a new set point.
Irregular dosing disrupts this pattern. Shortened intervals cause side effect spikes that may lead to missed meals and inconsistent nutrition. Lengthened intervals (forgetting doses) reduce the average drug exposure and can stall progress.
The users who see the best before-and-after results are overwhelmingly those who maintain a consistent weekly schedule. Minor one-time adjustments (like taking a dose two days early for travel) have negligible impact on long-term outcomes. But habitual inconsistency accumulates.
For those in the early stages of treatment, the first month on tirzepatide sets the trajectory. Establishing a rock-solid dosing routine during this period pays dividends throughout your treatment.
SeekPeptides members track their dosing consistency alongside their results, giving them visibility into how schedule adherence affects their individual progress over time.
What real users experience when dosing early
Clinical trial data only tells part of the story. Real-world experiences from people who have taken their tirzepatide early provide practical insights that controlled studies do not capture.
The "day 5 nausea spike" pattern
One of the most consistently reported experiences among people who dose two days early is a temporary nausea spike that feels similar to when they first started the medication. This makes pharmacological sense. The elevated peak concentration after a shortened interval mimics what happens during dose escalation, when your body encounters higher drug levels than it has adapted to.
For most people, this nausea resolves within 12 to 24 hours as the peak passes and levels begin to decline. The pattern is particularly noticeable in people taking 7.5 mg or higher, where the absolute increase in peak concentration is more significant. Those on 2.5 mg starting doses often report no noticeable difference when dosing a couple of days early, likely because the absolute drug levels remain relatively low even with the compressed interval.
Enhanced appetite suppression window
A commonly reported benefit of early dosing is a temporary period of enhanced appetite control. Because the new dose stacks on top of higher residual levels, the appetite-suppressing effect during the first 48 to 72 hours after injection can be noticeably stronger. Some people actually time early doses strategically before holidays, vacations, or social events where they know food temptation will be high.
This is not a recommended practice. But it illustrates an important point about the pharmacology. The drug does not distinguish between "therapeutic" appetite suppression and "too much" appetite suppression. When drug levels run higher than normal, everything intensifies proportionally, both the desired effects and the unwanted ones.
The rebound when returning to normal schedule
Perhaps the most underappreciated aspect of early dosing is what happens the following week when you return to your regular seven-day interval. After a five-day gap, your next seven-day gap feels longer by comparison.
Your drug levels at trough will be lower than they were on your compressed schedule.
Some people report a noticeable return of appetite or reduced efficacy in the final day or two before their next scheduled dose.
This rebound is temporary and resolves after one to two normal cycles. But it can be psychologically frustrating, especially if you are watching the scale daily. Understanding that this is a pharmacokinetic artifact, not a sign that the medication has stopped working, helps manage expectations. If you find yourself in this situation, our guide on managing hunger on tirzepatide provides practical nutritional strategies.
Impact on weight tracking
Early dosing can create confusing weight fluctuations in the days following the compressed dose. The enhanced GI effects may cause temporary water weight shifts, while the stronger appetite suppression can lead to reduced food intake that shows up as an artificially steep drop on the scale.
Neither of these reflects actual fat loss or gain.
If you track your weight daily, understand that readings in the 48 to 72 hours after an early dose may not reflect your true trajectory. Weekly or biweekly averages provide a more accurate picture. The before-and-after trajectory smooths out these short-term fluctuations when viewed over weeks rather than days.
Oral and sublingual tirzepatide: does dosing flexibility differ?
With the growing availability of oral tirzepatide formulations, some users wonder whether the 72-hour rule applies equally to non-injectable versions.
Oral tirzepatide (tablets)
The tablet form of tirzepatide has a different absorption profile than the subcutaneous injection. Oral bioavailability is lower, meaning a higher dose is needed to achieve equivalent blood levels. However, once absorbed, the drug behaves identically in the bloodstream. The same five-day half-life applies, and the same 72-hour minimum between doses should be observed.
The orally disintegrating tablet (ODT) format absorbs through the oral mucosa and GI tract. Absorption timing may differ slightly from standard tablets, but the elimination kinetics remain the same. Whether you use injectable, tablet, or ODT formulations, the dose timing guidelines are consistent.
Sublingual tirzepatide
Sublingual formulations, including tirzepatide drops and sublingual dosing protocols, absorb through the tissue under the tongue. This can provide faster initial absorption compared to subcutaneous injection, but the overall pharmacokinetic profile once the drug reaches systemic circulation is the same.
Faster absorption actually makes the 72-hour rule more important for sublingual formulations, not less. The quicker peak means that early dosing creates a sharper spike in drug levels compared to the gradual rise seen with subcutaneous injection. If you use a sublingual formulation, be especially careful about maintaining adequate spacing between doses.
Managing nutrition during a compressed dosing interval
If you have decided to take your tirzepatide two days early, or if you have already done so, optimizing your nutrition during the period of elevated drug levels helps minimize side effects and maintain your energy.
The first 24 hours after an early dose
This is when GI effects peak. Your stomach is emptying more slowly than usual, and nausea risk is highest.
What to eat:
Small portions every 2 to 3 hours instead of large meals
Lean protein sources: chicken breast, white fish, egg whites, Greek yogurt
Simple carbohydrates that digest easily: rice, toast, crackers
Room-temperature or cool foods (heat intensifies nausea)
What to avoid:
High-fat foods (slow digestion even further)
Fried or greasy items
Large portions of any food
Carbonated drinks (increase bloating)
Spicy foods (irritate already-sensitive GI lining)
For a comprehensive breakdown, our foods to avoid on tirzepatide guide covers everything in detail. The principles are the same as normal tirzepatide dietary guidance, just more important to follow strictly during periods of elevated drug levels.
Hours 24 through 72
As the acute peak passes, appetite typically returns gradually. This is a good time to focus on nutrient density. Your body has been running on reduced intake, and the nutrients you consume now matter more than volume.
Prioritize protein above all else. Adequate protein intake prevents muscle loss during weight loss, supports immune function, and helps maintain energy levels. Aim for 80 to 120 grams per day depending on your body weight and activity level. Our tirzepatide meal plan provides specific meal ideas designed around the appetite patterns of GLP-1 medication users.
Hydration is equally critical. Tirzepatide can cause mild dehydration even at normal doses, and the intensified effects of an early dose amplify this. Aim for at least 64 ounces of water daily, more if you experience diarrhea or vomiting. Adding electrolytes can help if you are struggling to maintain hydration.
The role of supplements
Taking the right supplements during a compressed dosing interval helps offset the nutritional gaps that reduced food intake creates. Key supplements to consider include:
Vitamin B12: GLP-1 medications can reduce B12 absorption over time. This effect may be temporarily enhanced with higher drug concentrations
Magnesium: Supports muscle function and reduces cramping, which some users report after early dosing
Fiber supplement: Helps manage both constipation and the alternating GI symptoms that compressed dosing can trigger
Electrolytes: Sodium, potassium, and magnesium replacement if GI symptoms cause fluid loss
If your tirzepatide formulation already includes B12 (as in compounded tirzepatide with B12), the early dose delivers more B12 as well, which is not harmful but is worth noting for tracking purposes.
Exercise considerations after early dosing
Physical activity interacts with tirzepatide in ways that become more relevant when drug levels are elevated.
The blood sugar factor
Exercise lowers blood glucose independently of medication. When combined with higher-than-normal tirzepatide levels, the glucose-lowering effect is amplified. This is especially relevant for morning exercisers who inject in the evening. If you took your dose two days early and plan to exercise the next day, monitor for signs of low blood sugar: shakiness, confusion, excessive sweating, or sudden weakness.
This concern is more acute for people with type 2 diabetes who take other glucose-lowering medications alongside tirzepatide. But even non-diabetic users can experience exercise-induced hypoglycemia-like symptoms when drug levels peak above their usual range.
GI comfort and exercise timing
Intense exercise during the nausea window (first 12 to 24 hours post-injection) is uncomfortable at normal drug levels and potentially worse after an early dose. High-impact activities like running, jumping, or heavy lifting can exacerbate nausea and increase the risk of vomiting.
Lower-intensity exercise like walking, light cycling, or yoga is generally well-tolerated even with elevated drug levels. If you normally exercise on your injection day, consider shifting your workout to the afternoon or evening rather than the morning, giving the acute peak time to pass.
Performance impacts
Some users report reduced exercise performance for one to two days after any tirzepatide injection, with the effect being more pronounced after early dosing. This likely relates to reduced caloric intake, mild dehydration, and the metabolic shifts that higher drug concentrations create. Do not push through intense training sessions if your body signals that it needs rest. One or two lighter workout days will not derail your fitness goals.
Other GLP-1 medications and their dosing flexibility
Understanding how other medications in the same class handle dose timing provides useful context for tirzepatide users.
Semaglutide (Ozempic, Wegovy)
Semaglutide has a slightly longer half-life of approximately seven days compared to tirzepatide five-day half-life. The same 72-hour minimum between doses applies. Because of the longer half-life, semaglutide drug levels remain more stable between doses, and the percentage increase from early dosing is proportionally smaller. Users who find tirzepatide dose timing challenging sometimes explore switching to semaglutide for its slightly more forgiving pharmacokinetic profile.
The conversion between the two medications is not straightforward because they target different receptor combinations. Any switch should be managed by a healthcare provider.
Retatrutide
Retatrutide, the newer triple receptor agonist targeting GIP, GLP-1, and glucagon receptors, has a different pharmacokinetic profile. Users curious about this medication can review the retatrutide vs tirzepatide comparison and the retatrutide dosing schedule for details on its timing requirements.
For those considering a transition, our guide on switching from tirzepatide to retatrutide covers the pharmacokinetic considerations of changing between medications with different half-lives and receptor profiles.
The broader GLP-1 landscape
Whether you are on tirzepatide, semaglutide, or considering newer options like orforglipron, survodutide, or cagrisema, the fundamental principle remains the same. These are long-acting medications designed for once-weekly administration. Respecting the prescribed dosing interval is essential for safety and efficacy across the entire class.
SeekPeptides provides detailed comparison guides for every major GLP-1 medication, helping you understand the differences in pharmacology, side effects, and dosing requirements so you can make informed decisions about your research protocol.
Tracking your dose timing for better outcomes
One of the most effective strategies for maintaining dosing consistency is keeping a simple injection log. This does not need to be complicated. A notes app on your phone, a spreadsheet, or even a wall calendar with injection dates and times marked serves the purpose. The goal is creating a record that removes guesswork from your dosing decisions.
What to track
At minimum, record the exact date and time of each injection. This gives you a definitive answer whenever the question "when was my last dose?" arises. No more trying to remember if it was Tuesday morning or Monday night. No more counting calendar days incorrectly because you forgot the exact timing.
Beyond the basics, tracking a few additional data points provides valuable insight into your tirzepatide experience over time:
Dose amount: Especially important if you are on compounded tirzepatide where doses are measured in units rather than pre-filled pens
Injection site: Rotating between abdomen, thigh, and upper arm sites helps prevent tissue irritation
Side effects: Rate your nausea, energy, and appetite on a simple 1 to 5 scale each day for the first 48 hours post-injection
Any schedule deviation: Note if you dosed early or late and by how many hours
Over time, this data reveals patterns. You might notice that evening injections consistently produce fewer side effects for you. Or that injecting in the thigh leads to more injection site reactions than the abdomen. Or that your appetite typically returns around day five, suggesting your dose may need adjustment.
Using dose tracking to plan schedule changes
When you have a clear injection log, planning an early dose becomes precise rather than approximate. You can calculate the exact hour gap before deciding whether to inject. You can identify whether your proposed timing falls within the safe 72-hour-plus window or whether you need to adjust your plan.
The GLP-1 plotter tools available online take this a step further by modeling your drug concentration curve based on your specific dose, timing, and history. These visual tools make it immediately obvious whether an early dose will push your peak concentration significantly above your normal range or whether the impact will be minimal.
For people managing complex schedules with frequent travel, shift work, or irregular routines, a dose tracking system is not optional. It is essential. The 72-hour rule only works as a safety guardrail when you know exactly when your last dose was administered. Guessing is how people accidentally dose at 60 or 65 hours instead of the 72 they intended.
The bottom line on taking tirzepatide 2 days early
Taking tirzepatide two days early is generally safe as a one-time event if you maintain at least 72 hours (three full days) between doses. The 120-hour gap that a two-day-early dose creates is well above the minimum safe interval. You may experience temporarily intensified side effects, particularly GI symptoms, but these are typically mild and self-limiting.
What you should not do is make early dosing a habit. Repeated compression of the dosing interval increases your average drug exposure beyond what was prescribed, elevates side effect risk, and disrupts the steady-state pharmacokinetics that your body has adapted to. If you consistently feel the urge to dose early because your appetite returns or your effects wane before day seven, talk to your prescriber about a dose adjustment instead.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
Frequently asked questions
Is it safe to take tirzepatide 2 days early every week?
No. While a single two-day-early dose is safe (maintaining the 72-hour minimum), doing this every week effectively shortens your dosing interval to five days. This increases your average drug exposure by roughly 15 to 20 percent above what your prescribed dose was designed to deliver. If you consistently want to inject early, ask your provider about a dose adjustment rather than increasing frequency.
What is the minimum time between tirzepatide doses?
The FDA-mandated minimum is 72 hours (three days). This applies to all tirzepatide formulations including Mounjaro, Zepbound, and compounded versions. Taking doses closer than 72 hours apart increases the risk of side effects and is never recommended.
I took my tirzepatide 2 days early by accident. What should I do?
If at least 72 hours had passed since your previous dose, you are fine. Resume your normal schedule on your next injection day (seven days from the early dose, not seven days from your original schedule). If less than 72 hours had passed, monitor for intensified side effects and contact your healthcare provider if you experience severe nausea, vomiting, or signs of hypoglycemia.
Can I take tirzepatide 3 days early?
Taking it three days early creates a 96-hour gap between doses. This is above the 72-hour minimum and technically safe for a one-time occurrence. However, the side effect increase is more noticeable at a four-day interval than a five-day interval. Proceed with extra caution and do not make this a regular practice.
Does taking tirzepatide early make it work faster for weight loss?
No. Taking doses closer together does not accelerate weight loss. The rate at which tirzepatide works depends on your dose level, diet, exercise, and individual metabolism. Shortening the interval only increases side effects without meaningfully improving the drug's efficacy. Trust the prescribed weekly schedule for optimal results.
Should I eat differently if I took my dose early?
If you are experiencing stronger appetite suppression or nausea after an early dose, focus on small, frequent, protein-rich meals. Avoid large portions and high-fat foods that worsen GI symptoms. Our tirzepatide meal plan and food guide provide specific recommendations for managing nutrition during periods of intense appetite suppression.
Does the 72-hour rule apply to compounded tirzepatide too?
Yes. The pharmacological properties of tirzepatide are the same regardless of whether it comes from a brand-name product or a compounding pharmacy. The 72-hour minimum between doses applies universally. The same dosage calculations and safety guidelines govern all formulations.
Can I take tirzepatide and semaglutide in the same week?
This is a separate question from early dosing and involves combining two GLP-1 medications. Our guide on taking semaglutide and tirzepatide together covers this topic in detail. In short, combining these medications is not standard practice and carries significant safety considerations.
What if I need to take tirzepatide early because of a holiday or event?
This is one of the most legitimate reasons to adjust your schedule. If a holiday, wedding, vacation, or other event falls on your regular injection day and you prefer to inject beforehand, moving the dose forward by one or two days is acceptable as long as you maintain the 72-hour minimum. Plan ahead rather than deciding last minute, and prepare your injection supplies in advance. Check our travel guide for tips on managing tirzepatide around trips and events.
Will taking tirzepatide 2 days early affect my period?
GLP-1 medications including tirzepatide can affect menstrual cycles in some women. A single early dose is unlikely to cause additional menstrual disruption beyond what the medication already does at steady state. However, if you notice changes in cycle timing, flow, or symptoms after adjusting your dose schedule, mention this to your healthcare provider. The hormonal effects of tirzepatide are still being studied, and individual responses vary significantly.
Can I drink alcohol if I took my tirzepatide early?
Alcohol and tirzepatide are not a great combination even at normal drug levels. Alcohol can worsen nausea, increase dehydration, and affect blood sugar regulation. With elevated drug concentrations after early dosing, these interactions may be more pronounced. If you plan to drink, wait at least 24 to 48 hours after injection and keep consumption moderate. Our guide on drinking on tirzepatide covers the full spectrum of considerations, and our best alcohol choices article helps you minimize GI discomfort if you do choose to drink.
I take compounded tirzepatide from a pharmacy. Does the 72-hour rule still apply?
Absolutely. Whether you use brand-name Mounjaro, Zepbound, or compounded formulations from pharmacies like Empower, Southend, or any other compounder, the active ingredient is the same. The pharmacokinetics do not change based on the source. The 72-hour minimum applies equally to all tirzepatide formulations.
Should I lower my dose if I am taking tirzepatide early?
For a one-time early dose, reducing the amount is generally unnecessary if you maintain at least 72 hours between injections. However, if you anticipate needing to compress your schedule regularly, discuss a slight dose reduction with your prescriber to offset the higher average drug exposure. This is especially relevant for people already on higher doses like 12.5 mg or 15 mg where the absolute increase in peak concentration from early dosing is more substantial.
How does this apply if I am also taking berberine or other supplements?
Supplements like berberine have their own glucose-lowering effects. When combined with elevated tirzepatide levels from early dosing, the blood sugar impact can be additive. If you take berberine, metformin, or other supplements that affect glucose metabolism, be especially watchful for hypoglycemia-like symptoms after an early dose. Consider skipping your berberine dose on the day you inject early and the following day to reduce the combined effect.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your injection timing stay precise, your side effects stay manageable, and your progress stay consistent.