Mar 16, 2026

You are wasting peptide. Probably 15 to 20 percent of every vial. And the worst part is you do not even know it is happening. With a tirzepatide 60 mg vial sitting in your refrigerator right now, every miscalculated reconstitution, every imprecise syringe draw, every extra day past the stability window is costing you money and compromising your results.
This is not a small problem when you are working with a vial that contains enough peptide for four to twenty-four weeks of research, depending on your dose. The 60 mg format is the most cost-effective option available in the compounded tirzepatide market. But it is also the most unforgiving. Get the reconstitution wrong and you are guessing at every dose. Get the storage wrong and the peptide degrades before you finish the vial. Get the math wrong and you either underdose for weeks or burn through an expensive vial in half the expected time.
This guide covers everything you need to know about the tirzepatide 60 mg vial. From the exact reconstitution protocols to precise dosing charts for every concentration, from storage rules that actually preserve potency to cost-per-dose calculations that show you exactly what you are spending.
Whether you are new to compounded tirzepatide or switching from a smaller vial size, this is your complete reference.
SeekPeptides members have been asking about the 60 mg format more than any other vial size. The reason is simple. It offers the best value per milligram, but only if you handle it correctly.
What is the tirzepatide 60 mg vial?
The tirzepatide 60 mg vial is a lyophilized (freeze-dried) powder containing 60 milligrams of tirzepatide peptide. It arrives as a white to off-white cake or powder inside a sealed glass vial with a rubber stopper and aluminum crimp cap. Before you can use it, you must reconstitute it with bacteriostatic water to create an injectable solution.
Think of it this way. The powder is stable. It can survive shipping, brief temperature fluctuations, and months of storage. Once you add water, the clock starts ticking.
The 60 mg format is not an FDA-approved product. It is a compounded formulation, meaning it comes from compounding pharmacies that prepare it using bulk tirzepatide powder. This is the same active ingredient found in the branded version, but the final product has not undergone the same regulatory testing process. That distinction matters for understanding what you are working with.
How the 60 mg vial compares to other sizes
Compounded tirzepatide comes in several vial sizes. The most common are 5 mg, 10 mg, 15 mg, 30 mg, and 60 mg. Here is how they compare:
Vial Size | Weeks at 2.5 mg/week | Weeks at 5 mg/week | Weeks at 10 mg/week | Weeks at 15 mg/week | Best For |
|---|---|---|---|---|---|
5 mg | 2 | 1 | 0.5 | 0.3 | Trial doses |
10 mg | 4 | 2 | 1 | 0.7 | Starting out |
30 mg | 12 | 6 | 3 | 2 | Mid-range |
60 mg | 24 | 12 | 6 | 4 | Best value |
The math is straightforward. A 60 mg vial at the starting dose of 2.5 mg per week lasts 24 weeks. That is nearly six months from a single vial. At the maximum recommended dose of 15 mg per week, it still provides four full weeks of dosing. No other vial size comes close to that duration at the lower end of the dosing range.
But here is the catch. Once reconstituted, the solution has a limited shelf life. Most protocols recommend using the vial within 28 days, though some sources extend that to 60 days under ideal refrigeration. If you are on a low dose, you may not use the entire vial before it expires. This is the primary consideration when choosing the 60 mg format.
Reconstitution protocol for the 60 mg vial
Reconstitution is the single most important step. Get it right and every dose is precise. Get it wrong and you are guessing for the life of the vial.
The process itself is simple. You add a measured amount of bacteriostatic water (BAC water) to the vial of lyophilized powder, allow it to dissolve, and store the resulting solution in your refrigerator. The amount of water you add determines the concentration, which determines how much liquid you draw for each dose.
Choosing your concentration
This is where most people make their first mistake. They add water without thinking about what concentration they actually need. The concentration you choose affects everything: how easy it is to measure doses, how much liquid you inject each time, and whether your doses fall on convenient syringe markings.
Here are the common concentration options for a 60 mg vial:
Desired Concentration | BAC Water to Add | Volume per 2.5 mg Dose | Volume per 5 mg Dose | Volume per 10 mg Dose | Volume per 15 mg Dose |
|---|---|---|---|---|---|
5 mg/mL | 12 mL | 0.50 mL (50 units) | 1.00 mL (100 units) | 2.00 mL | 3.00 mL |
10 mg/mL | 6 mL | 0.25 mL (25 units) | 0.50 mL (50 units) | 1.00 mL (100 units) | 1.50 mL |
15 mg/mL | 4 mL | 0.17 mL (17 units) | 0.33 mL (33 units) | 0.67 mL (67 units) | 1.00 mL (100 units) |
20 mg/mL | 3 mL | 0.125 mL (12.5 units) | 0.25 mL (25 units) | 0.50 mL (50 units) | 0.75 mL (75 units) |
The formula is: Total peptide (mg) / Desired concentration (mg/mL) = Volume of BAC water (mL)
For most researchers, 10 mg/mL is the sweet spot. It provides convenient syringe measurements at common doses and keeps injection volumes manageable. The peptide reconstitution calculator on SeekPeptides can help you determine the exact amount for your target concentration.
At 5 mg/mL, the doses land on round numbers that are easy to measure on a standard insulin syringe. But the injection volume at higher doses gets large. A 15 mg dose at 5 mg/mL requires 3 mL of liquid, which is uncomfortable and may need to be split into two injections.
At 20 mg/mL, the injection volumes are tiny. A 2.5 mg dose is only 12.5 units. That level of precision requires a syringe with half-unit markings, and even small measurement errors translate to significant dosing variations.
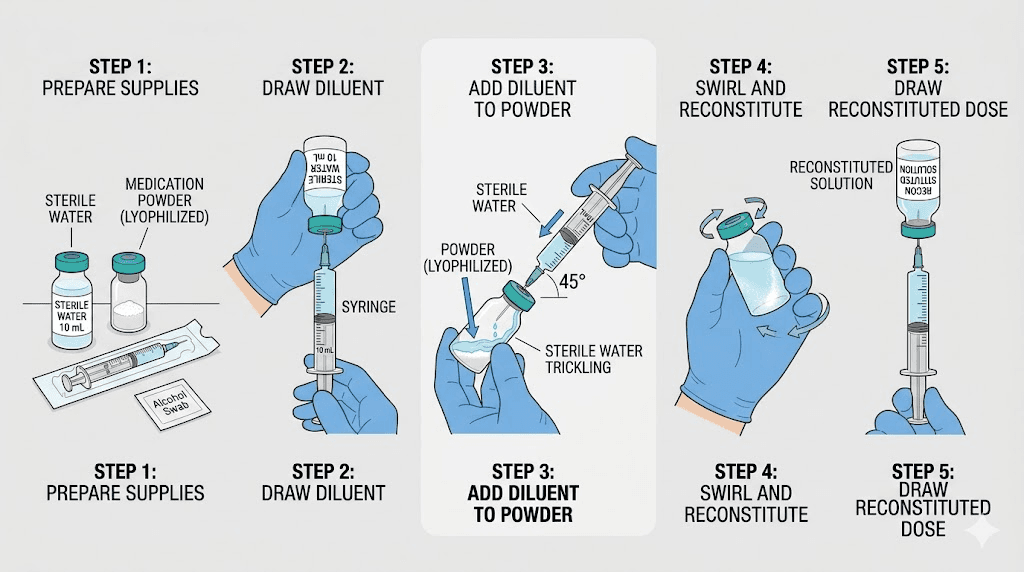
Step-by-step reconstitution process
Before you begin, gather everything you need. Do not start the process and then realize you forgot the alcohol swabs.
Materials required:
Tirzepatide 60 mg lyophilized vial
Bacteriostatic water (0.9% benzyl alcohol)
Sterile syringe (3 mL or 5 mL, depending on water volume)
Drawing needle (18-21 gauge)
Alcohol swabs
Clean workspace
Step 1: Wash your hands thoroughly with soap and water. This sounds basic. Skip it and you risk contaminating a vial worth hundreds of dollars.
Step 2: Allow the tirzepatide vial to reach room temperature. Cold vials dissolve more slowly and can cause the powder to clump. Give it 15 to 20 minutes on a clean surface.
Step 3: Wipe the rubber stopper of both the tirzepatide vial and the BAC water vial with an alcohol swab. Let them air dry for 30 seconds.
Step 4: Draw your calculated volume of BAC water into the syringe. For a 10 mg/mL concentration, that is exactly 6 mL. For 5 mg/mL, it is 12 mL. Double-check this number. There is no fixing a wrong concentration after the fact.
Step 5: Insert the needle through the rubber stopper of the tirzepatide vial. Angle the needle so the tip touches the inside wall of the glass, not the powder directly. Slowly depress the plunger, letting the water trickle down the side of the vial. This is critical. Blasting water directly onto the lyophilized cake can damage the peptide structure and create foam that takes hours to clear.
Step 6: Once all the water is in the vial, remove the needle. Do not shake the vial. Vigorous shaking denatures the peptide, breaking the molecular bonds that make it functional. Instead, gently roll the vial between your palms for 30 to 60 seconds. Some researchers prefer to simply set the vial in the refrigerator and let it dissolve on its own over 15 to 30 minutes.
Step 7: Once the solution is completely clear with no visible particles or cloudiness, it is ready for use. If you see undissolved powder, continue gentle rolling. If cloudiness persists after an hour, there may be a quality issue with the peptide.
Step 8: Label the vial immediately. Write the date, the concentration (e.g., 10 mg/mL), and the total volume. You will thank yourself in two weeks when you cannot remember when you mixed it.
The entire process takes about 5 minutes of active work, plus 15 to 30 minutes of passive dissolution time. If you have reconstituted semaglutide or other peptides before, this process is identical.
Dosing chart for the 60 mg vial
Once your vial is reconstituted, you need to know exactly how much liquid to draw for each dose. This depends on two things: your target dose in milligrams and the concentration you created during reconstitution.
The standard tirzepatide dosing protocol follows a titration schedule. You start low and increase gradually every four weeks. The recommended schedule from clinical trials is:
Weeks 1-4: 2.5 mg once weekly
Weeks 5-8: 5 mg once weekly
Weeks 9-12: 7.5 mg once weekly
Weeks 13-16: 10 mg once weekly
Weeks 17-20: 12.5 mg once weekly
Week 21+: 15 mg once weekly (maximum dose)
Not everyone follows this exact schedule. Some researchers use microdosing protocols at lower amounts. Others titrate more slowly to minimize side effects. The key is that your syringe measurements must be accurate regardless of which protocol you follow.
Dosing chart at 10 mg/mL concentration (6 mL BAC water)
This is the most common concentration for the 60 mg vial. Here is exactly what to draw on an insulin syringe:
Dose (mg) | Volume (mL) | Insulin Syringe Units | Number of Doses in Vial |
|---|---|---|---|
1 mg | 0.10 | 10 units | 60 doses |
2.5 mg | 0.25 | 25 units | 24 doses |
5 mg | 0.50 | 50 units | 12 doses |
7.5 mg | 0.75 | 75 units | 8 doses |
10 mg | 1.00 | 100 units | 6 doses |
12.5 mg | 1.25 | N/A (use 1.5 mL syringe) | 4.8 doses |
15 mg | 1.50 | N/A (use 1.5 mL syringe) | 4 doses |
Notice something important. At 10 mg/mL, doses up to 10 mg fit perfectly in a standard 1 mL (100 unit) insulin syringe. Doses above 10 mg require a larger syringe or splitting the dose into two injections.
For those using the compounded tirzepatide dosage calculator, these numbers should match exactly. If they do not, recheck your reconstitution volume.
Dosing chart at 5 mg/mL concentration (12 mL BAC water)
If you prefer larger, easier-to-measure volumes:
Dose (mg) | Volume (mL) | Insulin Syringe Units | Number of Doses in Vial |
|---|---|---|---|
2.5 mg | 0.50 | 50 units | 24 doses |
5 mg | 1.00 | 100 units | 12 doses |
7.5 mg | 1.50 | N/A | 8 doses |
10 mg | 2.00 | N/A | 6 doses |
15 mg | 3.00 | N/A | 4 doses |
The advantage here is measurement precision. Drawing 50 units for a 2.5 mg dose is much easier than drawing 25 units. The disadvantage is larger injection volumes, which some people find uncomfortable. Anything over 1 mL can sting or leave a noticeable subcutaneous bump at the injection site.
Dosing chart at 20 mg/mL concentration (3 mL BAC water)
For those who want minimal injection volumes:
Dose (mg) | Volume (mL) | Insulin Syringe Units | Number of Doses in Vial |
|---|---|---|---|
2.5 mg | 0.125 | 12.5 units | 24 doses |
5 mg | 0.25 | 25 units | 12 doses |
7.5 mg | 0.375 | 37.5 units | 8 doses |
10 mg | 0.50 | 50 units | 6 doses |
15 mg | 0.75 | 75 units | 4 doses |
This concentration is popular with experienced researchers who are comfortable with precise measurements. The small volumes mean less liquid to inject, which can reduce injection site reactions. But the margin for error shrinks dramatically. Half a unit off at 20 mg/mL equals 1 mg of tirzepatide. At 5 mg/mL, that same half-unit error is only 0.25 mg.
Choose your concentration based on your comfort level with syringe precision and your tolerance for injection volume. There is no universally correct answer.

How long does a 60 mg vial last?
This question has two answers. How long the vial lasts in terms of doses, and how long it lasts in terms of stability. Both matter.
Duration by dose
The number of weeks your vial lasts depends entirely on your weekly dose:
Weekly Dose | Doses per Vial | Duration (Weeks) | Duration (Months) |
|---|---|---|---|
2.5 mg | 24 | 24 | ~6 months |
5 mg | 12 | 12 | ~3 months |
7.5 mg | 8 | 8 | ~2 months |
10 mg | 6 | 6 | ~1.5 months |
12.5 mg | 4.8 | 4.8 | ~5 weeks |
15 mg | 4 | 4 | ~1 month |
If you follow the standard titration schedule starting at 2.5 mg and increasing every four weeks, a single 60 mg vial provides:
Weeks 1-4 at 2.5 mg = 10 mg used
Weeks 5-8 at 5 mg = 20 mg used
Weeks 9-12 at 7.5 mg = 30 mg used
Total: 60 mg consumed over 12 weeks
That is three full months of a complete titration protocol from one vial. Conveniently, one vial takes you from the starting dose through 7.5 mg. You would then need a second vial to continue titrating to 10 mg and above.
Stability after reconstitution
Here is where the 60 mg vial creates a challenge. Once reconstituted, the peptide solution has a finite shelf life.
Conservative estimate: 28 days refrigerated at 2-8 degrees Celsius (36-46 degrees Fahrenheit)
Extended estimate: Up to 60 days under ideal storage conditions
At low doses, the math does not work. If you are taking 2.5 mg per week, you need 24 weeks to use the entire vial. But the solution only lasts 4 to 8 weeks. You would use 10 to 20 mg of the 60 mg before the solution degrades, wasting 40 to 50 mg of peptide.
This is the fundamental problem with the 60 mg vial for low-dose users.
Solutions:
Use a higher concentration with smaller reconstitution volume, which does not actually solve the stability issue since the same amount of time passes
Start at a higher dose point if your protocol allows (only if you have already titrated up with a smaller vial)
Consider aliquoting into smaller sterile vials and freezing portions for later use (reduces contamination risk to the main vial)
Share the reconstitution timing with your dosing schedule, only reconstituting when you are at a dose where you will use the vial within 28-60 days
For researchers at 10 mg or 15 mg weekly, the 60 mg vial is perfect. You will use the entire contents within 4 to 6 weeks, well within the stability window. This is why the 60 mg format is most popular among those who have already titrated to maintenance doses.
For detailed information on how long a vial of tirzepatide lasts, check our dedicated guide that covers storage variables and stability testing.
Storage requirements for the 60 mg vial
Storage mistakes are the second most common way people waste their tirzepatide. The peptide is remarkably stable in lyophilized form but becomes sensitive once reconstituted.
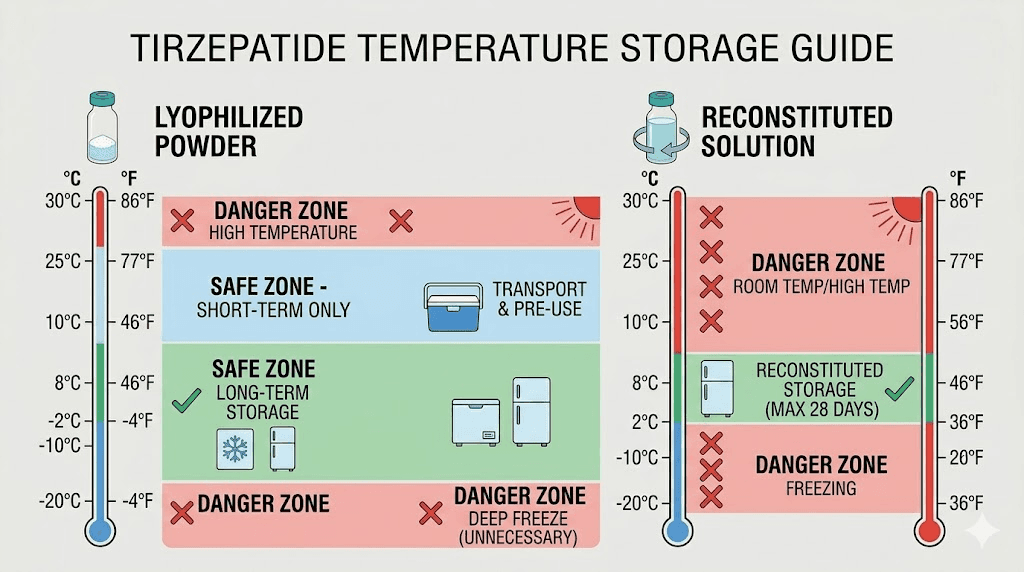
Before reconstitution (powder form)
Lyophilized tirzepatide is surprisingly durable. Store it:
Temperature: Room temperature is acceptable for short-term storage (weeks). Refrigeration (2-8 degrees C) is preferred for long-term storage (months)
Light: Keep away from direct sunlight and UV exposure. Store in the original box or a dark drawer
Humidity: Avoid humid environments. The powder can absorb moisture, which starts the degradation process before you even add water
Duration: Properly stored lyophilized tirzepatide can last 12 to 24 months. Check the expiration date from your compounding pharmacy
If your vial arrives warm from shipping, do not panic. Brief temperature excursions during transit rarely damage lyophilized peptides. The freeze-drying process specifically makes them resistant to temperature fluctuations. Refrigerate upon arrival and allow the vial to stabilize for a few hours before reconstituting.
After reconstitution (liquid form)
Once water hits the powder, the rules change completely.
Temperature: Refrigerate immediately at 2-8 degrees C (36-46 degrees F). Not the freezer. Not the counter. The refrigerator, specifically the main compartment where temperatures are most stable. Avoid the door shelves where temperatures fluctuate with opening and closing
Light: Continue protecting from light. Some researchers wrap the vial in aluminum foil for additional protection
Duration: Use within 28 days (conservative) to 60 days (extended). Mark the reconstitution date on the vial
Handling: Always use a new, sterile needle each time you draw a dose. Never touch the rubber stopper with your fingers after swabbing. Minimize the number of needle punctures through the stopper
Refrigeration is non-negotiable after reconstitution. Leaving the vial at room temperature for even a few hours accelerates degradation. If you accidentally leave it out of the fridge, brief exposures (under 2 hours) are generally tolerable. Longer than that, and you should evaluate whether the peptide is still viable.
Freezing reconstituted tirzepatide is a debated topic. Some researchers freeze aliquots successfully. Others report reduced potency after freeze-thaw cycles. If you choose to freeze portions, use sterile vials, freeze only once (no repeated freeze-thaw), and expect some potency loss.
Cost analysis: is the 60 mg vial worth it?
The 60 mg vial costs more upfront than smaller sizes. But the per-milligram cost is almost always lower. Here is how the economics typically break down.
Prices vary significantly between compounding pharmacies and vendors. These are representative ranges based on current market conditions:
Vial Size | Typical Price Range | Cost per mg | Cost per Week at 10 mg |
|---|---|---|---|
5 mg | $30 - $60 | $6.00 - $12.00 | $60 - $120 |
10 mg | $45 - $90 | $4.50 - $9.00 | $45 - $90 |
30 mg | $100 - $200 | $3.33 - $6.67 | $33 - $67 |
60 mg | $150 - $300 | $2.50 - $5.00 | $25 - $50 |
The savings are substantial. At the high end, switching from a 5 mg vial to a 60 mg vial can cut your per-milligram cost by more than half. Over a 20-week titration protocol using 150 mg of total peptide, that difference adds up to hundreds of dollars.
But the savings only materialize if you use the entire vial. Wasting 30 mg of a 60 mg vial because it expired before you could use it is worse than buying two 15 mg vials and using them completely. The peptide cost calculator can help you model different scenarios based on your specific dosing plan.
Factor in the cost of supplies too. Each vial requires the same reconstitution supplies regardless of size: BAC water, syringes, needles, alcohol swabs. Using one 60 mg vial instead of six 10 mg vials means fewer supply purchases and less waste.
When the 60 mg vial makes financial sense
You are at a maintenance dose of 7.5 mg or higher (you will use the vial within the stability window)
You have already titrated using smaller vials and know your target dose
You are comfortable with reconstitution and precise syringe measurements
You can store the vial properly for the entire duration
When smaller vials make more sense
You are just starting tirzepatide and do not know your dose yet
You are microdosing at very low amounts (1-2.5 mg)
You want to test a new vendor or batch before committing to a large purchase
Your storage conditions are not ideal (unreliable refrigeration, travel)
Syringe selection and measurement precision
The syringe you use matters more than most people realize. A wrong syringe choice can introduce 10 to 20 percent dosing errors on every injection.
Insulin syringes vs tuberculin syringes
For subcutaneous tirzepatide injections, you have two main options:
Insulin syringes (U-100): These are marked in units from 0 to 100, where 100 units = 1 mL. They come in three sizes: 0.3 mL (30 units), 0.5 mL (50 units), and 1 mL (100 units). The needles are typically 29-31 gauge, which is thin enough for comfortable subcutaneous injection. For most tirzepatide dosing, the 1 mL insulin syringe is ideal.
Tuberculin syringes: These are marked in mL with 0.01 mL gradations. They are available in 1 mL and 3 mL sizes. They offer more flexibility for larger volumes but the needles are typically thicker (25-27 gauge) and they require a separate needle attachment.
For the 60 mg vial reconstituted at 10 mg/mL, an insulin syringe works perfectly for doses up to 10 mg (100 units). For the 12.5 mg and 15 mg doses, you either need a tuberculin syringe or must split the dose across two injections.
Measurement tips for accuracy
Small errors compound over time. Drawing 23 units instead of 25 units every week means you are getting 2.3 mg instead of 2.5 mg. Over 24 weeks, you will have 4.8 mg of peptide left in a vial you thought was empty. That leftover is wasted money.
To improve accuracy:
Hold the syringe at eye level when checking the measurement. Looking down at an angle makes the meniscus appear higher or lower than it actually is
Draw past your target by a few units, then push the plunger back to the exact mark. This clears any air from the needle hub
Tap out air bubbles before measuring. Air in the syringe displaces liquid and reduces your actual dose
Use the right syringe size for your dose. A 0.3 mL syringe has larger markings and better precision for doses under 30 units than a 1 mL syringe does
These details matter. Experienced researchers on SeekPeptides consistently report that measurement precision is the single biggest factor in getting consistent results from their protocols.
Injection technique for the 60 mg vial
The injection process is the same regardless of vial size. But since the 60 mg vial will be your primary supply for weeks or months, developing good technique from the start prevents problems down the road.
Preferred injection sites
Subcutaneous injection means the needle goes into the fat layer between the skin and muscle. The most common sites for tirzepatide are:
Abdomen (2 inches away from the navel, rotating sides)
Front of thighs (upper third, alternating legs)
Back of upper arms (harder to self-administer)
Rotate injection sites with every dose. Injecting repeatedly in the same spot can cause lipohypertrophy (hardened fat deposits) that interfere with absorption. The abdomen generally provides the most consistent absorption rate, which is why many protocols recommend it as the primary site.
For a detailed walkthrough, see our guide on how to inject tirzepatide with a syringe.
Minimizing injection site reactions
Some people experience redness, swelling, or itching at the injection site. This is more common with larger injection volumes, which is relevant if you reconstituted your 60 mg vial at a lower concentration like 5 mg/mL.
To reduce reactions:
Allow the solution to warm to room temperature for 5 to 10 minutes before injecting (cold solution stings more)
Inject slowly over 5 to 10 seconds rather than pushing the plunger quickly
Apply gentle pressure with a cotton ball after withdrawing the needle (do not rub)
Consider using a higher concentration to reduce injection volume
If injection site reactions persist, switching to a different anatomical site or adjusting your reconstitution concentration may help. Persistent or worsening reactions warrant consulting a healthcare provider.

The titration schedule with a 60 mg vial
Planning your titration schedule around the 60 mg vial is important for avoiding waste. Here is how a standard protocol maps onto this vial size.
Full titration using one 60 mg vial
Starting from 2.5 mg and titrating up:
Week | Weekly Dose | Cumulative mg Used | Remaining in Vial |
|---|---|---|---|
1-4 | 2.5 mg | 10 mg | 50 mg |
5-8 | 5 mg | 30 mg | 30 mg |
9-12 | 7.5 mg | 60 mg | 0 mg |
A single 60 mg vial covers exactly 12 weeks of standard titration from 2.5 mg through 7.5 mg. That is elegant. No waste, no leftover. But it only works if the reconstituted solution remains stable for the full 12 weeks.
Since most stability estimates cap out at 28 to 60 days, you would need to either:
Reconstitute the full 60 mg and accept potential degradation in weeks 9-12
Consider reconstituting only a portion of the powder (not recommended as it is nearly impossible to accurately divide lyophilized powder)
Accept that stability may extend beyond the conservative 28-day estimate, especially with proper BAC water use and refrigeration
Many experienced researchers report viable solution quality at 8 to 10 weeks when using bacteriostatic water and maintaining strict refrigeration. The benzyl alcohol preservative in BAC water provides ongoing antimicrobial protection that extends usable life well beyond what sterile water would allow.
Maintenance dosing with 60 mg vials
Once you have titrated to your target dose, the 60 mg vial becomes straightforward:
Maintenance Dose | Weeks per Vial | Vials per Year |
|---|---|---|
5 mg/week | 12 | 4.3 |
7.5 mg/week | 8 | 6.5 |
10 mg/week | 6 | 8.7 |
12.5 mg/week | 4.8 | 10.8 |
15 mg/week | 4 | 13 |
At a 10 mg maintenance dose, you need roughly 9 vials per year. At 15 mg, you need 13. This long-term view helps with budgeting and ordering. Many vendors offer bulk discounts on larger orders, which further reduces the per-milligram cost of the 60 mg format.
Common mistakes with the 60 mg vial
After reviewing thousands of questions from researchers, these are the errors that come up again and again. Every one of them is preventable.
Mistake 1: wrong reconstitution volume
This is the most common and most consequential error. Adding 3 mL of water when you meant to add 6 mL creates a concentration twice as strong as intended. Every subsequent dose is double what you think it is. Some researchers have experienced significant gastrointestinal side effects because they were unknowingly taking twice their target dose.
Prevention: Calculate your water volume before you start. Write it down. Verify it. Then measure carefully using a syringe marked in mL.
Mistake 2: shaking the vial
Vigorous shaking creates foam and can denature the peptide. Denatured tirzepatide is less effective or completely inactive. You cannot tell by looking at the solution whether it has been damaged this way.
Prevention: Gentle rolling only. Or let it dissolve passively in the refrigerator.
Mistake 3: using sterile water instead of bacteriostatic water
Sterile water contains no preservative. Once you puncture the vial with a needle, bacteria can enter. Without the benzyl alcohol in BAC water, bacterial growth can begin within hours. With multiple needle punctures over weeks, the contamination risk multiplies.
BAC water is not optional for a multi-dose vial. The 60 mg vial will be punctured dozens of times over its life. Bacteriostatic water is the only appropriate choice.
Mistake 4: storing at room temperature
Some researchers leave their vial on the bathroom counter or bedroom nightstand for convenience. Room temperature storage cuts the usable life of reconstituted tirzepatide dramatically. Peptides degrade faster in warm environments, and the 60 mg vial is too expensive to treat casually.
Prevention: Refrigerator. Always. No exceptions. Keep a cold storage solution if you need portability.
Mistake 5: not labeling the vial
Week 3, you look at the vial and cannot remember when you reconstituted it. Was it 2 weeks ago or 4 weeks ago? Was the concentration 10 mg/mL or 5 mg/mL? Without a label, you are guessing. And guessing with peptides means inaccurate dosing or using degraded solution.
Prevention: Label immediately after reconstitution. Date, concentration, total volume. Every time.
Mistake 6: dead volume loss
Every time you draw from the vial with a syringe, a small amount of liquid stays trapped in the needle hub and dead space. Over 24 draws from a vial, this can add up to 0.5 to 1.0 mL of solution, depending on your syringe type. At 10 mg/mL, that is 5 to 10 mg of wasted tirzepatide.
Prevention: Use low dead-space syringes designed to minimize waste. Draw slowly and ensure you are pulling the full intended volume. Some researchers add a small overage of BAC water during reconstitution to account for dead volume loss, but this changes the concentration slightly and requires careful math.
Side effects and what to expect at different doses
The 60 mg vial does not change the side effect profile. You experience the same effects whether your dose comes from a 5 mg vial or a 60 mg vial. But since the 60 mg format enables longer continuous use, understanding the side effect timeline is especially relevant.
Common side effects by dose tier
Dose Range | Common Side Effects | Frequency | Typical Duration |
|---|---|---|---|
2.5 mg | Mild nausea, decreased appetite | 30-40% of users | First 1-2 weeks |
5 mg | Nausea, mild diarrhea, reduced appetite | 40-50% | First 1-2 weeks after dose increase |
7.5-10 mg | Nausea, diarrhea, constipation, fatigue | 50-60% | First 2-3 weeks after dose increase |
12.5-15 mg | Nausea, GI disturbance, fatigue, headaches | 55-65% | First 2-4 weeks, may persist |
Most side effects follow a predictable pattern. They appear after each dose increase, peak during the first week at the new dose, and gradually subside over 2 to 4 weeks. This is why the titration protocol spaces increases by 4 weeks, to give your body time to adjust before the next step up.
If you experience persistent fatigue, it usually resolves as your body adapts. Constipation can be managed with increased fiber and hydration. Headaches are often related to reduced caloric intake and dehydration rather than the peptide itself.
For more on what to anticipate, see what to expect after your first dose of tirzepatide.
When to slow the titration
Not everyone should follow the standard 4-week titration. With a 60 mg vial, you have enough peptide to extend the titration timeline without worrying about running out. Slower titration is worth considering if:
Nausea persists beyond 2 weeks at your current dose
You experience significant GI symptoms that interfere with daily function
Your body aches or muscle pain are severe
You are losing weight faster than 1 to 2 percent of body weight per week (too-rapid weight loss increases muscle loss risk)
Some researchers use a 6 or 8-week interval between dose increases instead of the standard 4 weeks. The 60 mg vial easily accommodates this extended schedule. In fact, slower titration is one of the best uses of the 60 mg format because you have plenty of peptide to take your time finding the optimal dose.
Comparing tirzepatide 60 mg to semaglutide vials
Many researchers have experience with compounded semaglutide and wonder how the 60 mg tirzepatide vial compares. The reconstitution process is identical, but there are important differences.
Factor | Tirzepatide 60 mg | Semaglutide 10 mg |
|---|---|---|
Active mechanism | Dual GIP/GLP-1 agonist | GLP-1 agonist only |
Max weekly dose | 15 mg | 2.4 mg |
Weeks per vial at starting dose | 24 (at 2.5 mg) | 40 (at 0.25 mg) |
Weeks per vial at max dose | 4 (at 15 mg) | 4.2 (at 2.4 mg) |
Reconstitution | Identical process | Identical process |
Storage | 28-60 days refrigerated | 28-56 days refrigerated |
Weight loss (clinical trials) | Up to 20.9% at 15 mg | Up to 14.9% at 2.4 mg |
Tirzepatide consistently outperforms semaglutide in head-to-head comparisons for weight reduction. The SURMOUNT-1 trial showed up to 20.9% body weight reduction with 15 mg tirzepatide over 72 weeks, compared to roughly 15% with semaglutide in the STEP trials. For a detailed comparison, see semaglutide vs tirzepatide.
If you are considering switching between the two, the conversion chart can help you determine equivalent doses. The process of reconstituting and storing semaglutide vials is virtually identical to what you have learned here for the 60 mg tirzepatide.
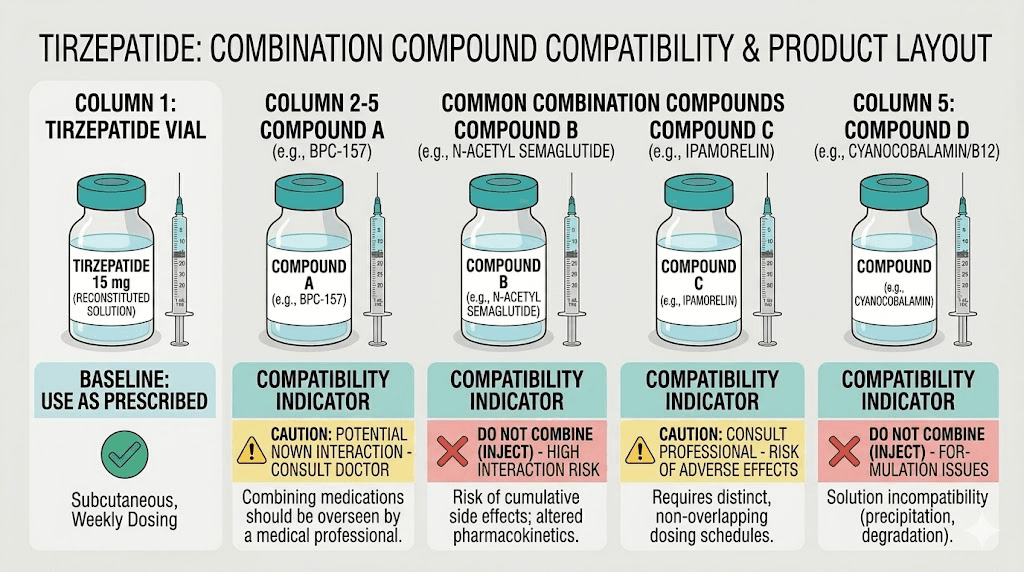
Combining tirzepatide with other compounds
Some researchers use their 60 mg tirzepatide alongside other compounds. This is where things get complicated, and where having a larger vial supply simplifies logistics.
Common combinations
Tirzepatide with B12 is the most popular combination. Some compounding pharmacies even offer pre-mixed tirzepatide with glycine and B12 formulations. When using a standalone 60 mg vial, you would administer B12 as a separate injection.
Tirzepatide with glycine is another common pairing. Glycine may help reduce injection site reactions and improve tolerability for some users.
Tirzepatide with levocarnitine combines the appetite-suppressing effects of tirzepatide with the fat-metabolism support of L-carnitine.
Tirzepatide with niacinamide adds a B3 vitamin component that some researchers believe supports metabolic function during weight loss.
AOD-9604 with tirzepatide combines two different fat-loss mechanisms, though this stack requires separate vials and careful timing.
For comprehensive guidance on combining compounds, SeekPeptides members get access to detailed stacking calculators and protocol databases that account for interactions and timing.
What not to combine
Never combine tirzepatide with semaglutide or other GLP-1 agonists simultaneously. They share the same receptor pathway, and doubling up dramatically increases the risk of severe gastrointestinal side effects without proportional benefit.
If you are thinking about adding phentermine to tirzepatide, understand that this combination has limited research support and the cardiovascular implications are not well studied.
Vendor considerations for the 60 mg format
Not all 60 mg vials are created equal. The compounding pharmacy and vendor you choose directly affects the quality, purity, and potency of your peptide.
What to look for in a vendor
Third-party testing: Legitimate vendors provide Certificates of Analysis (COA) from independent labs showing purity above 98% and accurate peptide content
503B pharmacy status indicates the pharmacy operates under FDA oversight with more stringent quality controls than 503A pharmacies
Proper shipping: The vial should arrive in insulated packaging. Lyophilized powder is temperature-resistant, but extreme heat or cold during multi-day shipping can still cause issues
Accurate labeling: The vial should clearly state the peptide content (60 mg), lot number, expiration date, and storage instructions
Reputation: Check reviews and community feedback. Peptide forums and trusted communities often have firsthand vendor experience
Several popular vendors have been reviewed extensively. You can find detailed analyses of providers like Empower Pharmacy, Peptide Sciences, and many others in the SeekPeptides review database.
Red flags
No COA available or refuses to provide one
Prices significantly below market range (quality testing is expensive)
Vials arrive without proper labels or lot numbers
The powder looks discolored or has a strange odor after reconstitution
The solution remains cloudy after 30 minutes of gentle mixing
With the bulk tirzepatide market growing rapidly, counterfeit and under-dosed products do exist. The 60 mg vial represents a significant financial investment. Spending the extra time to verify your vendor is worth it.
Troubleshooting the 60 mg vial
Even with perfect technique, issues arise. Here is how to handle the most common problems.
The powder will not dissolve
If the lyophilized cake refuses to dissolve after 30 minutes of gentle rolling:
Make sure the BAC water reached the powder. Sometimes the water pools on one side without contacting the cake
Allow the vial to sit at room temperature (not refrigerated) for 30 minutes. Cold temperatures slow dissolution
Continue gentle rolling every 5 minutes
If still undissolved after 2 hours, the peptide may have been compromised during manufacturing or shipping
Cloudy or discolored solution
Clear and colorless is the standard for properly reconstituted tirzepatide. Slight turbidity immediately after mixing is normal and should clear within minutes. Persistent cloudiness, yellow tint, or visible particles indicate potential degradation or contamination. Do not use a solution that does not clear. The color of tirzepatide should be transparent after reconstitution.
Results plateauing
If you have been using the same 60 mg vial for several weeks and notice reduced effectiveness, consider whether the solution has been reconstituted for too long. Peptide degradation does not announce itself. The solution looks the same. It just works less.
If you are within the stability window and still experiencing a plateau, it may be time to evaluate other factors like diet, sleep, and exercise. A structured eating plan can significantly improve outcomes.
Side effects suddenly worsening
If side effects intensify mid-vial without a dose change, check your concentration math. A common scenario: you think you reconstituted at 10 mg/mL but actually used 5 mL instead of 6 mL of water, creating a 12 mg/mL solution. Every dose has been 20% higher than intended. This compounds over weeks.
Recheck your math. Recalculate your volume per dose. Consider whether a measurement error during reconstitution could explain the change.
Advanced protocols with the 60 mg vial
Beyond standard titration, the 60 mg vial supports several advanced dosing strategies that smaller vials cannot practically accommodate.
Split dosing
Instead of one weekly injection, some researchers split their dose across two injections per week. For example, 10 mg per week becomes 5 mg on Monday and 5 mg on Thursday. This approach can reduce peak-related side effects like nausea while maintaining the same total weekly dose.
With a 60 mg vial, split dosing means twice as many needle punctures through the stopper. Use BAC water (not sterile water) and proper aseptic technique to minimize contamination risk.
Microdosing
The microdosing approach uses much lower amounts, often 0.5 to 1.5 mg per dose, for specific applications like inflammation management. At these low doses, a 60 mg vial could theoretically last 40 to 120 weeks. Obviously, stability limits prevent that. But the 60 mg format is still cost-effective for microdosing if you aliquot portions for freezing and reconstitute fresh batches as needed.
For a complete microdose schedule, check the dedicated guide.
Extended titration
Some researchers prefer a very gradual titration: increasing by 1.25 mg every 4 weeks instead of the standard 2.5 mg. This results in a 32-week titration from 2.5 mg to 15 mg, using approximately 140 mg of total peptide. Two to three 60 mg vials cover the entire extended protocol with excellent cost efficiency.
The tirzepatide 60 mg vial for different goals
Your goal influences how you should approach the 60 mg vial.
Weight loss protocols
For weight loss, the standard titration to 10-15 mg per week is the most studied approach. The SURMOUNT-1 trial demonstrated that participants on 15 mg tirzepatide lost an average of 20.9% of their body weight over 72 weeks. That level of reduction is unprecedented for any weight management intervention.
The 60 mg vial supports a full weight loss protocol without the hassle of switching vials mid-titration. Combined with a proper diet plan and the right supplements, this format provides a convenient and cost-effective foundation.
Track your progress with the tirzepatide weight loss timeline to set realistic expectations for each phase of treatment.
Metabolic health protocols
Beyond weight loss, tirzepatide shows benefits for blood sugar regulation, insulin sensitivity, and cardiovascular risk markers. These applications often use lower maintenance doses (5-10 mg), making the 60 mg vial last even longer.
Researchers interested in the benefits beyond weight loss often find that the 60 mg format provides enough supply to experiment with dosing variations while maintaining a consistent peptide source.
Transitioning from other GLP-1 compounds
If you are switching from semaglutide or transitioning to retatrutide, the 60 mg tirzepatide vial gives you enough supply to manage a proper crossover protocol. Use the semaglutide to tirzepatide conversion chart or the reverse conversion chart to find your equivalent starting dose.
Frequently asked questions
How much bacteriostatic water do I add to a 60 mg tirzepatide vial?
The amount depends on your desired concentration. For 10 mg/mL, add 6 mL. For 5 mg/mL, add 12 mL. For 20 mg/mL, add 3 mL. Use the formula: 60 mg divided by your target concentration equals the required volume. The reconstitution calculator can verify your math.
How many doses are in a 60 mg vial?
At 2.5 mg per dose, you get 24 doses. At 5 mg, 12 doses. At 10 mg, 6 doses. At 15 mg, 4 doses. The number of doses is simply 60 divided by your dose in milligrams. See the dosage in units guide for syringe-specific conversions.
Is the 60 mg vial FDA approved?
No. The 60 mg vial is a compounded product. FDA-approved tirzepatide comes as pre-filled injection pens in fixed doses of 2.5 mg through 15 mg. The compounded 60 mg format offers cost savings but does not carry the same regulatory oversight. Learn about the differences in our compounded tirzepatide guide.
Can I travel with a 60 mg vial?
Yes, with proper precautions. Keep it refrigerated using a travel cooler and avoid temperature extremes. Carry documentation from your healthcare provider or pharmacy. Airport security generally allows medical injectables with proper documentation. Lyophilized (unreconstituted) vials are easier to travel with since they do not require refrigeration.
What if I miss a dose from my 60 mg vial?
If you miss a dose by 1-3 days, take it as soon as you remember and resume your regular schedule. If more than 3 days have passed, skip the missed dose and take the next scheduled dose. Do not double up. The vial itself is not affected by a missed dose, you simply have more solution remaining.
Does the 60 mg vial expire faster than smaller vials?
In lyophilized form, no. The expiration date depends on manufacturing conditions, not vial size. Once reconstituted, the stability is the same regardless of whether you mixed a 10 mg vial or a 60 mg vial. The difference is that you are more likely to have unused solution in the 60 mg vial if you are on a low dose. Check our guide on tirzepatide expiration for details.
Can I mix two partially used 60 mg vials together?
No. Never combine the contents of two vials. Even if both are the same concentration and from the same manufacturer, combining introduces contamination risk and makes it impossible to track the reconstitution date for the mixed solution. Use each vial independently.
What is the best time of day to inject from the 60 mg vial?
Most researchers inject in the morning or evening, choosing a consistent time each week. The best time to take tirzepatide depends on your individual response. If nausea is a concern, evening injection allows you to sleep through the initial wave. If you prefer to plan your meals around appetite suppression, morning injection may work better.
External resources
For researchers serious about optimizing their tirzepatide protocols, SeekPeptides offers comprehensive dosing calculators, reconstitution guides, and a community of experienced researchers who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your reconstitution stay precise, your vials stay potent, and your protocols stay consistent.