Mar 5, 2026

What if the fatigue you feel on tirzepatide is not the drug failing you, but your cells running out of fuel? Most people starting a tirzepatide protocol expect the appetite suppression, the gradual weight loss, the occasional nausea. Nobody warns them about the energy crash. That deep, bone-level tiredness that settles in around week three or four and refuses to lift, no matter how much sleep you get or how many cups of coffee you pour down.
The reason is simpler than most people think. Rapid caloric restriction, the kind tirzepatide appetite suppression creates, depletes a molecule your mitochondria need to produce energy. That molecule is NAD+, nicotinamide adenine dinucleotide, and your body was already losing it at a rate of roughly 1-2% per year since your twenties. Add aggressive weight loss on top of that natural decline, and your cellular power plants start sputtering.
So can you take NAD+ and tirzepatide together?
Yes. There are no known contraindications between NAD+ supplements and tirzepatide. They work through completely different biological pathways, tirzepatide through GIP and GLP-1 receptors, NAD+ through sirtuin activation and mitochondrial function. But the absence of a contraindication does not mean you should combine them blindly. The details matter. The form of NAD+ you choose matters. The timing matters. The dosage matters. And the reasons you are combining them should guide every decision you make.
This guide covers everything researchers need to know about combining NAD+ with tirzepatide, from the molecular mechanisms that make this pairing logical to the specific protocols that minimize risk and maximize potential benefit. SeekPeptides has analyzed the available research, clinical observations, and community experiences to build the most comprehensive resource on this combination available anywhere.
What NAD+ actually does in your body
NAD+ is not a supplement trend. It is one of the most fundamental molecules in human biology, present in every single cell, required for over 500 enzymatic reactions. Without adequate NAD+ levels, your cells cannot convert food into usable energy, repair damaged DNA, regulate circadian rhythms, or maintain the inflammatory balance that keeps chronic disease at bay.
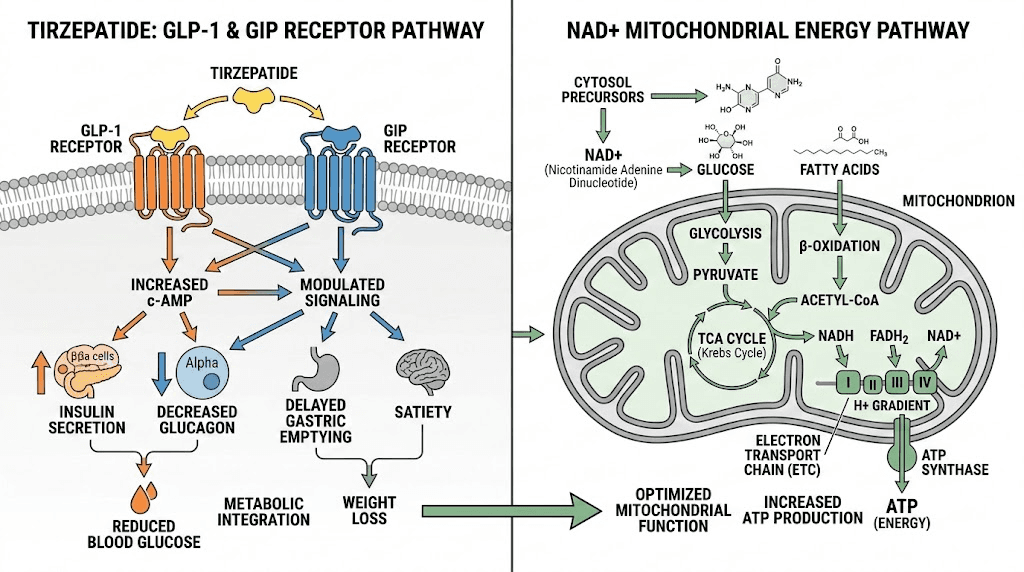
Think of NAD+ as the currency your cells spend to do work. Every time a mitochondrion converts glucose or fatty acids into ATP (the energy molecule your muscles, brain, and organs actually use), it needs NAD+ to complete the transaction. When NAD+ levels drop, the transaction slows down. Energy production drops. Cellular repair slows. Inflammation increases. You feel tired, foggy, and old.
Here is where it gets relevant to tirzepatide users. NAD+ levels decline naturally with age.
By age 50, most people have roughly half the NAD+ they had at 20. But caloric restriction, while beneficial in many ways, places additional demands on NAD+ dependent repair pathways. Your body is simultaneously trying to metabolize stored fat for fuel and repair tissues that were previously supported by a higher caloric intake. Both processes consume NAD+.
The result? An energy deficit that sleep alone cannot fix.
The three forms of NAD+ supplementation
You cannot simply swallow NAD+ and have it enter your cells. The molecule is too large to cross cell membranes efficiently when taken orally. Instead, most supplementation strategies use precursor molecules that your body converts into NAD+ after absorption. The three primary approaches each have distinct advantages and limitations that matter when combining with tirzepatide therapy.
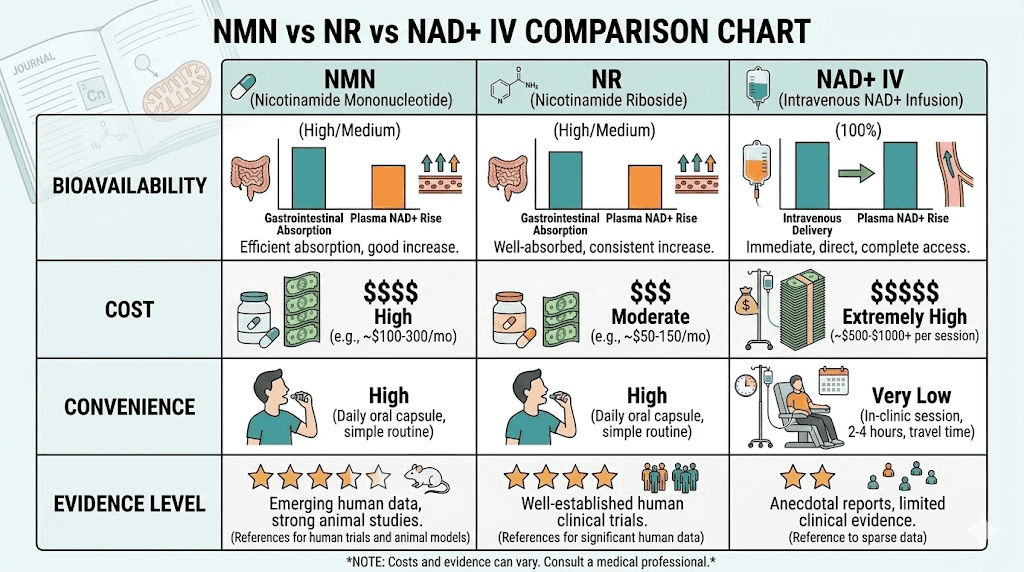
NMN (nicotinamide mononucleotide) is the precursor closest to NAD+ in the biosynthesis pathway. Research in mice shows that oral NMN is absorbed through a specific transporter (Slc12a8) in the small intestine, which means it enters the NAD+ pathway quickly. A key study published in Endocrinology found that NMN administration restored intestinal NAD+ levels and actually increased GLP-1 production in obese mice. That finding is particularly relevant for tirzepatide users because tirzepatide works partly through GLP-1 receptor activation, and higher endogenous GLP-1 levels could theoretically enhance that mechanism.
Typical NMN dosages in human studies range from 250mg to 1,200mg daily. Most researchers use 500-1,000mg.
NR (nicotinamide riboside) is another NAD+ precursor, one step further from NAD+ than NMN. NR has more human clinical trial data than NMN, with studies demonstrating it can raise blood NAD+ levels by 40-90% depending on dose. However, NR did not improve insulin sensitivity or increase GLP-1 secretion in the same mouse models where NMN succeeded. The difference may relate to the absence of the Slc12a8 transporter for NR in the intestinal lining, meaning NR must take a longer metabolic route to become NAD+.
Standard NR dosages range from 300mg to 1,000mg daily.
NAD+ IV infusions and subcutaneous injections bypass the digestive system entirely, delivering NAD+ directly into the bloodstream. Bioavailability approaches 100% with IV administration, compared to an estimated 10-40% for oral precursors. The drawback is cost ($100-700 per session depending on provider and location), inconvenience, and the fact that large-scale controlled trials comparing intracellular NAD+ levels after injection versus oral supplementation are still lacking. Some researchers question whether IV NAD+ actually enters cells or simply breaks down into precursor molecules in the bloodstream, effectively mimicking what oral supplementation achieves at much lower cost.
Why NAD+ levels matter more during weight loss
Weight loss is not just about burning calories. At the cellular level, rapid fat loss triggers a cascade of repair, recycling, and rebuilding processes that all depend on adequate NAD+ availability. Autophagy, the cellular cleanup process that removes damaged proteins and organelles, requires NAD+ dependent sirtuin activation. Metabolic adaptation, the shift from primarily glucose-burning to fat-burning metabolism, depends on mitochondrial efficiency that NAD+ regulates.
When you combine tirzepatide with aggressive caloric restriction (which happens naturally because the drug suppresses appetite so effectively), your NAD+ demands spike while your dietary NAD+ precursor intake drops. You are eating less food overall, which means less niacin, less tryptophan, less of the dietary building blocks your body uses to manufacture NAD+ internally.
This creates a perfect storm for fatigue, brain fog, and the frustrating energy crashes that many tirzepatide users report.
How tirzepatide works at the receptor level
Before understanding why NAD+ pairs well with tirzepatide, you need to understand what tirzepatide actually does. Unlike older GLP-1 agonists such as semaglutide, tirzepatide is a dual-agonist. It activates both the GIP (glucose-dependent insulinotropic polypeptide) receptor and the GLP-1 (glucagon-like peptide-1) receptor simultaneously. This dual action produces more potent effects on appetite, insulin sensitivity, and fat metabolism than either receptor alone.
The GLP-1 component slows gastric emptying, reduces appetite through hypothalamic signaling, and enhances insulin secretion in response to meals. The GIP component adds another layer of metabolic regulation, improving fat tissue metabolism and potentially contributing to the greater weight loss seen in clinical trials compared to semaglutide alone.
In the SURMOUNT-1 trial, tirzepatide produced average weight loss of 15-22.5% of body weight over 72 weeks depending on dose. That is substantially more than any previous GLP-1 monotherapy. But more weight loss means more metabolic stress, more cellular turnover, and consequently more demand on NAD+ dependent processes.
The tirzepatide weight loss timeline typically shows the fastest losses in months two through six, which coincides with the period when NAD+ depletion symptoms most commonly appear. This is not coincidence. It is biochemistry.
The tirzepatide side effect profile and NAD+ connection
Consider the most common tirzepatide side effects. Fatigue. Body aches. Sleep disruption. Brain fog. Headaches. Now consider the symptoms of NAD+ depletion. Fatigue. Muscle soreness. Poor sleep quality. Cognitive decline. Headaches.
The overlap is not subtle. While not every tirzepatide side effect is caused by NAD+ depletion (gastrointestinal effects like bloating, constipation, and diarrhea are related to the GLP-1 mechanism itself), the fatigue and cognitive symptoms may have a cellular energy component that NAD+ supplementation could theoretically address.
A poster presented at a recent obesity medicine conference (PMC12492188) examined the association between tirzepatide and fatigue, finding that energy-related complaints were among the most persistent non-GI side effects reported by patients. The study did not evaluate NAD+ levels, but the pattern fits the known biology.
The safety profile of combining NAD+ with tirzepatide
Let us be direct about what is known and what is not.
What is known: There are no documented drug interactions between NAD+ precursors (NMN or NR) and tirzepatide. They operate through entirely different biological systems. Tirzepatide binds to specific cell-surface receptors. NAD+ precursors are metabolized through well-characterized enzymatic pathways involving NAMPT, NMNAT, and other enzymes in the NAD+ salvage pathway. These systems do not compete for the same receptors, enzymes, or transporters in any way that would create a pharmacological conflict.
What is not known: No randomized controlled trial has specifically studied the combination of tirzepatide and NAD+ supplementation. The safety data comes from the individual safety profiles of each compound combined with the pharmacological logic that they do not interact. This is a reasonable basis for clinical decision-making, but it is not the same as direct evidence of combined safety.
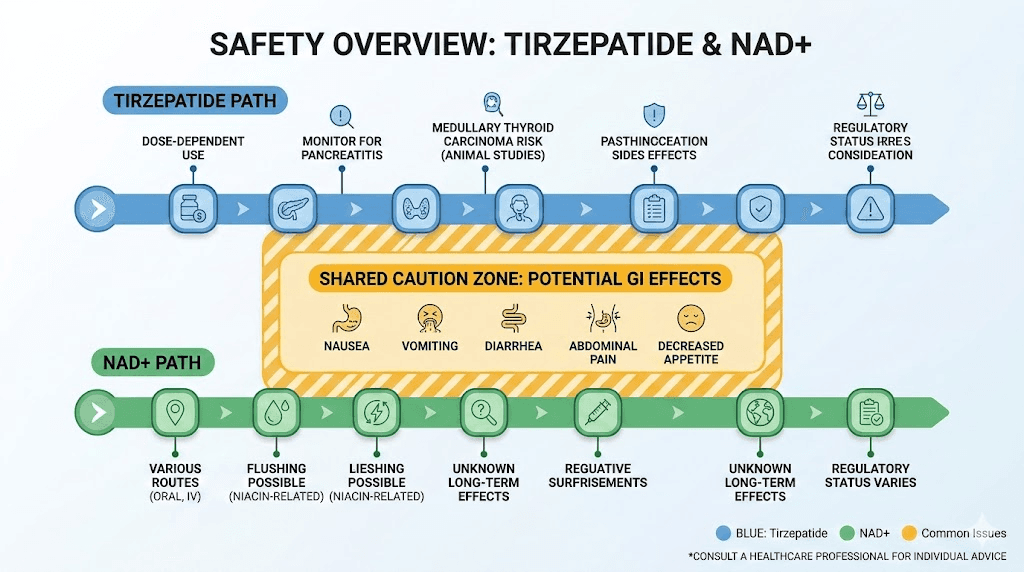
Both compounds share one potential concern. Gastrointestinal side effects.
Tirzepatide commonly causes nausea, especially during the first weeks of treatment and after dose escalations. NMN and NR can also cause mild GI discomfort in some users, particularly at higher doses. Taking both simultaneously could theoretically increase the gastrointestinal burden, though no systematic study has evaluated this.
The practical solution is simple. Separate them by timing. More on that in the protocol section below.
Who should exercise extra caution
While the combination appears safe for most healthy adults pursuing weight loss, certain groups should consult their healthcare provider before adding NAD+ supplementation to a tirzepatide protocol.
People with diabetes: Both tirzepatide and NAD+ precursors can affect blood glucose levels. Tirzepatide lowers glucose through enhanced insulin secretion. NMN has shown insulin-sensitizing effects in some studies. The combined effect could theoretically increase hypoglycemia risk, particularly in people on additional diabetes medications. If you are taking tirzepatide specifically for type 2 diabetes management alongside metformin or insulin, the medication interaction landscape becomes more complex and professional guidance is essential.
People on blood pressure medications: NMN may interact with medications affecting blood pressure through effects on vascular NAD+ metabolism. The clinical significance of this interaction is not fully characterized, but monitoring is prudent.
People with active cancer: NAD+ plays complex roles in cancer biology. While NAD+ depletion can impair healthy cell function, some cancer cells also depend on NAD+ for survival and proliferation. Adding NAD+ supplementation without oncologist guidance could theoretically support tumor metabolism. This is a theoretical concern, not a demonstrated risk, but caution is warranted.
People taking medications metabolized through cytochrome P450 enzymes: NMN may interact with the CYP450 enzyme system, though specific interactions have not been fully characterized in humans. If you take medications processed through these pathways (many common drugs including some statins, blood thinners, and antidepressants), discuss NAD+ supplementation with your prescribing physician.
Why researchers combine NAD+ with tirzepatide
Five specific reasons drive the growing interest in this combination. Each has a different evidence base, ranging from solid preclinical data to reasonable theoretical logic to early clinical observations.
Reason 1: fighting the energy crash
This is the most common reason people add NAD+ to their tirzepatide regimen. The fatigue that accompanies rapid weight loss on GLP-1 agonists is well documented and frequently reported in online communities. While some of this fatigue relates to reduced caloric intake (your body is simply receiving less fuel), a portion likely relates to impaired mitochondrial efficiency from declining NAD+ levels.
NAD+ supplementation addresses this by restoring the cofactor your mitochondria need to complete the electron transport chain, the final step in converting food (or stored fat) into ATP. When NAD+ levels are adequate, your mitochondria can process fatty acids more efficiently, potentially making the transition from glucose-dependent to fat-burning metabolism smoother and less fatiguing.
Users reporting on this combination frequently note improved energy within one to two weeks of adding NMN or NR supplementation. This timeline is consistent with the known pharmacokinetics of NAD+ precursor supplementation, where blood NAD+ levels begin rising within days and reach steady state within two to four weeks.
Compare this with other approaches to managing GLP-1 related fatigue. B12 supplementation helps if you have a deficiency but does not address the NAD+ pathway. Tirzepatide with B12 is a popular combination that supports methylation and red blood cell production, but B12 alone does not replenish cellular NAD+ stores. L-carnitine (tirzepatide with levocarnitine) supports fatty acid transport into mitochondria, which is complementary but targets a different step in energy production than NAD+.
For optimal energy support during tirzepatide therapy, some researchers layer multiple approaches. NAD+ precursor for mitochondrial efficiency. B12 for methylation support. L-carnitine for fatty acid transport. Glycine for collagen synthesis and sleep quality. This multi-target strategy addresses energy production from several angles simultaneously.
Reason 2: muscle preservation during rapid weight loss
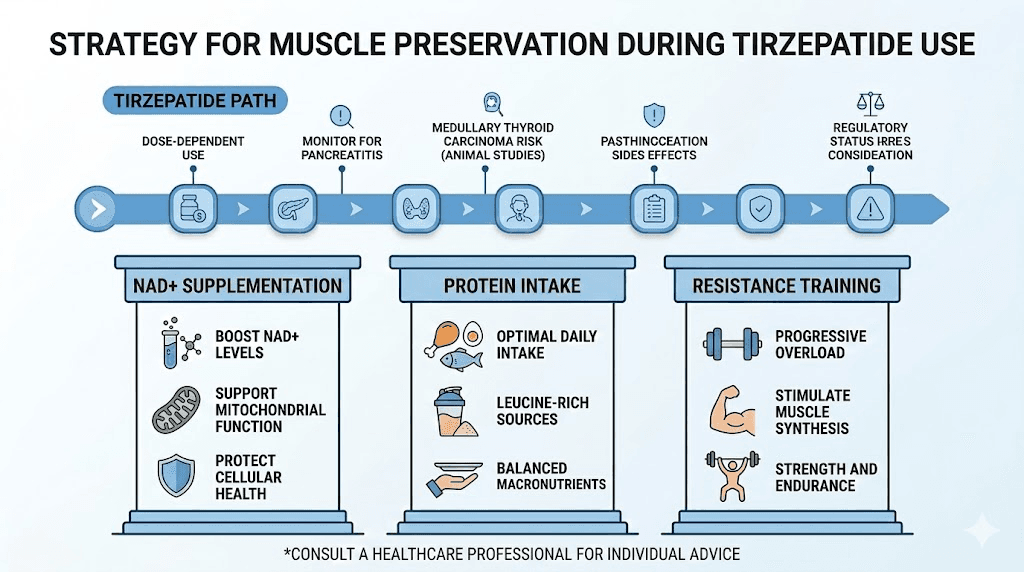
One of the most significant concerns with GLP-1 agonist therapy is muscle mass loss. Clinical trials consistently show that 20-40% of weight lost on tirzepatide comes from lean mass rather than fat. For someone losing 50 pounds, that means 10-20 pounds of muscle disappearing along with the fat. This muscle loss reduces metabolic rate, impairs physical function, and makes weight regain more likely after treatment ends.
NAD+ plays a critical role in muscle maintenance through several mechanisms. SIRT1, an NAD+ dependent enzyme, regulates muscle protein synthesis and mitochondrial biogenesis in skeletal muscle. SIRT3, another NAD+ dependent enzyme, protects mitochondrial function in muscle cells under metabolic stress. When NAD+ levels decline, these protective mechanisms weaken, potentially accelerating the muscle loss that caloric restriction already promotes.
Animal studies demonstrate that NMN supplementation preserves exercise capacity and muscle function in aged mice. A study in Cell Reports found that NMN enhanced mitochondrial oxidative metabolism in skeletal muscle and reversed age-associated physiological decline. While human data specifically on muscle preservation during GLP-1 therapy with NAD+ supplementation is lacking, the mechanistic logic is sound.
For researchers prioritizing lean mass retention, combining NAD+ supplementation with adequate protein intake (1.2-1.6g per kg body weight) and resistance training two to three times weekly creates a comprehensive muscle preservation strategy. The NAD+ supports mitochondrial health in the muscle cells, protein provides the building blocks for new muscle tissue, and resistance training signals the body to maintain muscle rather than break it down.
Reason 3: enhanced GLP-1 production
This is where the science gets genuinely interesting. A study published in Endocrinology (Oxford Academic, 2022) demonstrated that intestinal NAD+ biosynthesis directly regulates GLP-1 production. When researchers knocked out NAMPT (the rate-limiting enzyme in NAD+ production) in intestinal cells, GLP-1 secretion dropped significantly. When they restored NAD+ levels with NMN supplementation, GLP-1 production recovered.
The implications for tirzepatide users are significant. Tirzepatide activates GLP-1 receptors externally, mimicking what natural GLP-1 does. But your body also produces its own GLP-1 in response to meals, and this endogenous GLP-1 works alongside the synthetic agonist. If NMN supplementation increases your natural GLP-1 output, it could theoretically enhance the overall GLP-1 signaling environment, complementing what tirzepatide provides exogenously.
One important nuance: this GLP-1 enhancing effect was specific to NMN in the research. NR (nicotinamide riboside) did not produce the same increase in GLP-1 secretion, likely because the NMN-specific intestinal transporter Slc12a8 allows NMN to directly boost intestinal NAD+ levels in a way that NR cannot. If enhanced GLP-1 production is a primary goal, NMN may be the preferred precursor over NR for this specific application.
This research finding also adds context to the timeline of tirzepatide effects. If endogenous GLP-1 production is being supported by adequate NAD+ levels, the overall signaling environment may reach therapeutic thresholds faster than in someone with depleted NAD+.
Reason 4: metabolic flexibility
Metabolic flexibility refers to your body ability to switch efficiently between burning glucose and burning fat for fuel. People with poor metabolic flexibility get stuck in glucose-burning mode, struggling to access fat stores even during caloric restriction. This is one reason some people hit a tirzepatide plateau where weight loss stalls despite continued appetite suppression and adherence to their protocol.
NAD+ is central to metabolic flexibility. The sirtuins (SIRT1, SIRT3, SIRT6) that regulate the shift between glucose and fat metabolism all require NAD+ as a cofactor. When NAD+ levels are adequate, these sirtuins activate pathways that increase fatty acid oxidation, enhance mitochondrial fat burning, and improve insulin sensitivity. When NAD+ is depleted, the metabolic switch gets stuck.
Tirzepatide improves metabolic flexibility through its receptor-level effects on insulin sensitivity and fat tissue metabolism. NAD+ supplementation supports metabolic flexibility through intracellular enzyme activation. The two approaches work at different levels of the metabolic hierarchy, receptor signaling and intracellular enzyme activity, which means they complement rather than duplicate each other.
For people who have experienced a weight loss stall on tirzepatide, adding NAD+ supplementation is worth considering alongside other strategies like adjusting dietary composition, increasing physical activity, or discussing dose adjustments with their provider.
Reason 5: longevity and cellular repair
Many people taking tirzepatide are not just pursuing weight loss. They are pursuing healthier aging. The metabolic improvements tirzepatide produces, better insulin sensitivity, reduced visceral fat, lower inflammatory markers, align with longevity goals. NAD+ supplementation targets aging through a complementary pathway, supporting DNA repair, telomere maintenance, and cellular cleanup processes that protect against age-related disease.
The longevity peptide landscape is expanding rapidly, and the combination of metabolic optimization (via tirzepatide) with cellular repair optimization (via NAD+) represents a multi-target approach to healthy aging that addresses both macro-level body composition and micro-level cellular function.
Peptides for anti-aging research increasingly recognizes that no single intervention optimizes all aging pathways. The most promising approaches combine interventions that target different mechanisms, exactly what the tirzepatide plus NAD+ combination does.
NMN versus NR for tirzepatide users: which to choose
This is one of the most common questions from people considering NAD+ supplementation alongside their tirzepatide protocol. Both NMN and NR are legitimate NAD+ precursors with clinical data supporting their ability to raise blood NAD+ levels. But they are not interchangeable, and the differences matter.
Factor | NMN | NR |
|---|---|---|
GLP-1 production | Increased in studies | No effect observed |
Intestinal absorption | Direct via Slc12a8 transporter | Indirect, longer metabolic route |
Insulin sensitivity | Improved in prediabetic women | No significant change |
Human safety data | Safe up to 1,200mg daily | Safe up to 1,000mg daily |
NAD+ elevation | Significant increase | 40-90% increase depending on dose |
Cost (monthly) | $40-80 | $30-60 |
Regulatory status | Complex (FDA investigational drug designation in some markets) | Available as dietary supplement |
Best for tirzepatide users? | Yes, preferred for GLP-1 synergy | Good alternative if NMN unavailable |
For tirzepatide users specifically, NMN has the stronger theoretical case. The GLP-1 enhancing effect, the direct intestinal absorption pathway, and the insulin-sensitizing data in human studies all favor NMN over NR when the goal is complementing a GLP-1/GIP agonist.
That said, NR has more extensive long-term human safety data and wider regulatory acceptance as a dietary supplement. If NMN is unavailable or cost-prohibitive, NR remains a solid option for supporting cellular NAD+ levels during tirzepatide therapy.
One consideration that many guides overlook: the FDA has designated NMN as an investigational new drug in some regulatory contexts, which has complicated its availability as a dietary supplement. This regulatory landscape is evolving, and supplement availability may vary by region. Check current regulations in your area before purchasing.
Dosage protocols for combining NAD+ with tirzepatide
No clinical trial has established an optimal dosing protocol for this specific combination. The following protocols are derived from individual NAD+ supplementation studies, tirzepatide dosing guidelines, and clinical observations from practitioners who recommend both. They should be discussed with a qualified healthcare provider before implementation.
Protocol 1: conservative start (recommended for most people)
Goal: Address fatigue and support cellular energy during initial tirzepatide dose escalation
NAD+ component:
NMN 250mg once daily, taken in the morning with food
Maintain for 2-4 weeks to assess tolerance
If well tolerated, increase to 500mg daily
Tirzepatide component:
Follow standard escalation per provider guidance
Review our tirzepatide dose chart for reference
Timing:
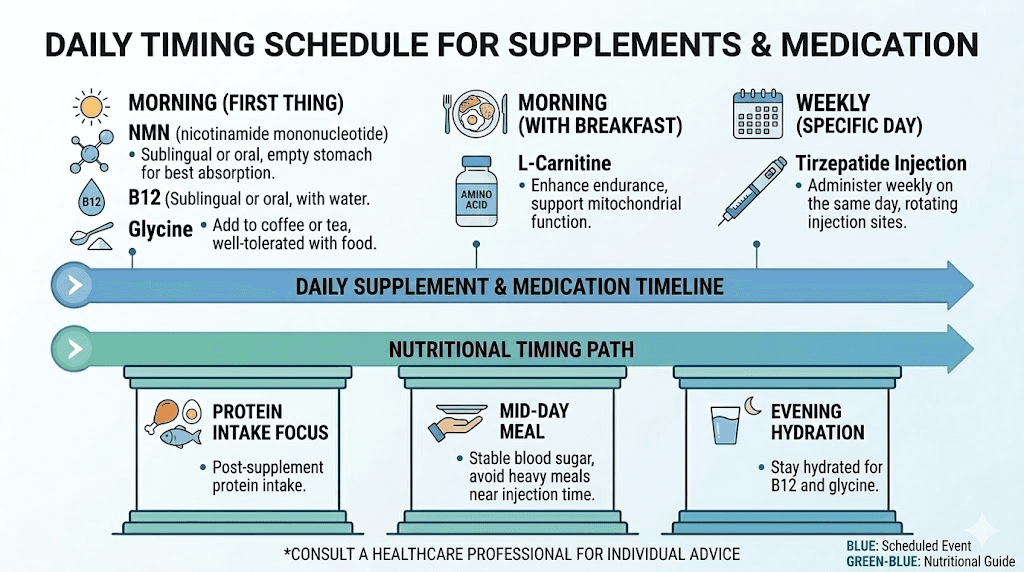
NMN: morning with breakfast
Tirzepatide injection: follow your normal schedule (see best time to take tirzepatide)
Separate NMN from tirzepatide by at least 2 hours to minimize combined GI effects
Duration: Ongoing throughout tirzepatide treatment
Expected timeline:
Week 1-2: Subtle improvement in baseline energy
Week 2-4: More noticeable energy stabilization, reduced brain fog
Week 4-8: Steady state NAD+ levels, consistent energy throughout the day
Protocol 2: moderate support (for active individuals)
Goal: Support energy, muscle preservation, and exercise recovery during tirzepatide therapy
NAD+ component:
NMN 500mg daily, split into two doses (250mg morning, 250mg early afternoon)
OR NMN 500mg morning + NR 300mg evening
Additional support:
L-carnitine 1,000-2,000mg daily for fatty acid transport
Protein intake 1.4-1.6g per kg body weight
Resistance training 2-3 sessions per week
Timing:
First NMN dose: morning with breakfast
Second NMN dose: early afternoon (before 3pm to avoid sleep disruption)
L-carnitine: 30 minutes before exercise
Tirzepatide: per normal schedule
This protocol targets the dual concerns of energy and lean mass preservation. The split NMN dosing maintains more consistent NAD+ levels throughout the day, while L-carnitine ensures the fatty acids being released from fat stores can actually reach the mitochondria for burning.
Protocol 3: comprehensive metabolic support
Goal: Maximum metabolic optimization for researchers pursuing aggressive weight loss with longevity benefits
NAD+ component:
NMN 750-1,000mg daily (split morning and early afternoon)
Periodic NAD+ IV or subcutaneous injection (optional, 1-2x monthly)
Complementary support stack:
B12 (methylcobalamin) 1,000-5,000mcg daily
B6 (pyridoxine) 50mg daily
Glycine 3-5g daily (evening, supports sleep and collagen)
L-carnitine 2,000mg daily
Magnesium glycinate 400mg daily (evening)
Omega-3 fatty acids 2-4g daily
Timing framework:
Morning: NMN 500mg + B12 + B6 with food
Early afternoon: NMN 250-500mg with food
Pre-workout: L-carnitine
Evening: Glycine + Magnesium (support sleep, which is critical for NAD+ dependent repair processes)
Tirzepatide: weekly injection per provider schedule
This comprehensive approach addresses energy production (NAD+, B vitamins), fatty acid metabolism (L-carnitine), tissue repair (glycine), neuromuscular function (magnesium), and inflammation (omega-3s). It is the most resource-intensive protocol but targets the broadest range of metabolic needs during aggressive weight loss.
Timing your NAD+ supplementation around tirzepatide injections
Getting the timing right can make the difference between a smooth experience and unnecessary GI distress. Here are the principles that guide effective scheduling.
NMN is best taken in the morning. NAD+ levels naturally follow a circadian rhythm, peaking during waking hours when metabolic demands are highest. Morning NMN supplementation aligns with this biological pattern and supports daytime energy production. Taking NMN late in the day could potentially interfere with sleep by keeping cellular energy machinery running when it should be winding down, which is why afternoon doses should be taken before 3pm.
Separate NMN from your tirzepatide injection day. If your tirzepatide injection day tends to cause nausea, consider taking a lower NMN dose that day or skipping the afternoon dose. The first 24-48 hours after injection are when GI effects peak, and you do not want to add any additional burden on your digestive system during this window.
Always take NMN with food. NMN on an empty stomach increases the likelihood of nausea and stomach discomfort. A small meal or snack is sufficient. This also applies if you are experiencing reduced appetite from tirzepatide, even a few bites of protein-rich food before your NMN dose can significantly reduce GI irritation.
Do not take NMN immediately before or after B3 (niacin) supplements. Both NMN and niacin feed into the NAD+ pathway, and flooding the system with both simultaneously can cause flushing, nausea, and discomfort. If your supplement stack includes a multivitamin with niacin, separate it from your NMN dose by at least two hours.
Weekly scheduling example
Here is how a typical week might look for someone on a standard tirzepatide protocol with NMN supplementation:
Monday (injection day): NMN 250mg morning only. Skip afternoon dose. Focus on hydration and easy-to-digest foods per your tirzepatide meal plan.
Tuesday (day after injection): NMN 250mg morning. Assess GI tolerance. If feeling well, resume afternoon dose.
Wednesday through Sunday: Full NMN protocol (250-500mg morning, optional 250mg early afternoon). Normal tirzepatide diet plan and supplement schedule.
This approach front-loads the most cautious supplementation around the injection window when GI sensitivity is highest, then allows full NAD+ support during the rest of the week when your body most benefits from sustained energy production.
Managing side effects when combining NAD+ and tirzepatide
Most people tolerate this combination well. But knowing what to watch for and how to respond prevents minor issues from becoming reasons to abandon a potentially beneficial protocol.
Increased nausea
If nausea worsens after adding NMN or NR, try these adjustments in order:
First, ensure you are taking NMN with food. Never on an empty stomach. Second, reduce the dose. Drop from 500mg to 250mg, or from 250mg to 125mg. Third, switch the form. Some people tolerate NR better than NMN, or vice versa. Fourth, switch the timing. Move the dose further from your tirzepatide injection day. If nausea persists despite all adjustments, discontinue the NAD+ supplement and discuss with your provider.
Standard tirzepatide GI management strategies also apply. Small, frequent meals. Avoiding high-fat foods around injection day. Staying well hydrated. Ginger supplements or tea for nausea relief.
Flushing and warmth
Some NAD+ precursors, particularly at higher doses, can cause a flushing sensation similar to niacin flush. This is more common with NR than NMN and typically subsides within 30-60 minutes. It is not dangerous but can be uncomfortable. Reducing the dose or splitting it into smaller portions throughout the day usually resolves flushing. Taking NAD+ with food also reduces flushing frequency.
Sleep disruption
NAD+ supports cellular energy production. Taking NMN too late in the day can interfere with the natural wind-down of metabolic activity that prepares your body for sleep. If you notice sleep difficulties after adding NAD+, move all doses to before 2pm. Add magnesium glycinate (400mg) and glycine (3g) in the evening to support sleep quality.
Headaches
Both NMN and tirzepatide can independently cause headaches. If headaches appear or worsen after combining them, hydration is the first intervention. Many headaches during GLP-1 therapy relate to inadequate fluid intake as appetite decreases. Aim for a minimum of 80 ounces of water daily. If headaches persist, reducing the NMN dose and using our tirzepatide headache treatment guide for additional strategies is recommended.
The research: what the studies actually show
Honesty about the evidence base matters. Here is what the research supports and where the gaps remain.
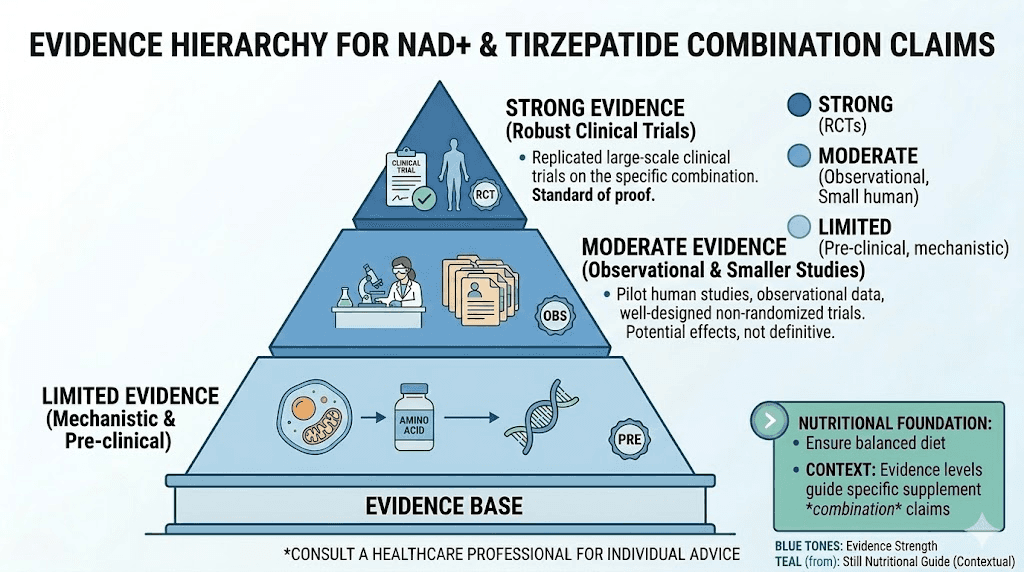
Strong evidence
NMN raises NAD+ levels in humans. Multiple clinical trials confirm that oral NMN supplementation at doses of 250-1,200mg daily significantly increases blood NAD+ levels. A systematic review in PMC10721522 evaluated the safety and antiaging effects of NMN in human clinical trials and found it well-tolerated with consistent NAD+ elevation.
NR raises NAD+ levels in humans. Similarly robust clinical data shows NR supplementation (300-1,000mg daily) increases blood NAD+ by 40-90%. Safety profiles are favorable across multiple trials.
NMN enhances GLP-1 production in mice. The Endocrinology study (2022) demonstrated that NMN administration restored GLP-1 secretion in obese mice by replenishing intestinal NAD+ levels through the Slc12a8 transporter.
NAD+ depletion contributes to age-related metabolic dysfunction. Decades of research confirm that declining NAD+ levels contribute to mitochondrial dysfunction, impaired DNA repair, and metabolic inflexibility with aging.
Moderate evidence
NMN improves insulin sensitivity in some populations. A study in prediabetic women showed NMN supplementation improved muscle insulin sensitivity. This aligns with the metabolic benefits of tirzepatide but the study was small.
NAD+ precursors preserve muscle function in animal models. Multiple rodent studies show NMN and NR improve exercise capacity and preserve muscle mitochondrial function. Human translation is promising but not confirmed.
Limited or theoretical evidence
Combined tirzepatide and NAD+ synergy. No clinical trial has tested this combination directly. The rationale is based on non-overlapping mechanisms and individual component safety data.
NAD+ supplementation reduces tirzepatide side effects. Anecdotal reports suggest improved energy and reduced fatigue, but no controlled study has evaluated this claim.
NAD+ enhances tirzepatide weight loss outcomes. Theoretical based on improved metabolic flexibility and GLP-1 production, but unconfirmed.
The evidence gap here is important. You are not taking two drugs with proven synergy supported by randomized controlled trials. You are taking two compounds with compatible mechanisms, individual safety data, and a reasonable biological rationale for combination. That is a meaningful distinction, and honest researchers should acknowledge it.
NAD+ IV therapy versus oral supplementation during tirzepatide treatment
Some clinics now offer NAD+ IV infusions alongside tirzepatide injections as a premium metabolic package. Is the additional cost justified?
NAD+ IV infusions deliver the molecule directly into your bloodstream, achieving roughly 100% bioavailability compared to the estimated 10-40% of oral precursors. The effects tend to be more immediately noticeable, with many recipients reporting improved mental clarity and energy within hours. Subcutaneous NAD+ injections offer a middle ground, with effects building over 12-24 hours.
But here is the nuance that expensive IV clinics rarely mention. Researchers remain uncertain whether IV NAD+ actually enters cells intact or whether it breaks down into NMN and NR in the bloodstream before being taken up by cells, essentially mimicking what oral supplementation achieves at a fraction of the cost. The controlled trials comparing intracellular NAD+ levels after IV versus oral administration have not been done.
What the cost comparison actually looks like:
Delivery method | Monthly cost | Convenience | Evidence quality | Speed of effect |
|---|---|---|---|---|
Oral NMN | $40-80 | High (daily pill) | Strong | 2-4 weeks to steady state |
Oral NR | $30-60 | High (daily pill) | Strong | 2-4 weeks to steady state |
SQ NAD+ injection | $150-300 | Moderate (self-injection) | Limited | 12-24 hours |
IV NAD+ infusion | $400-2,800 (1-4 sessions) | Low (clinic visit) | Limited | Hours |
For most tirzepatide users, oral NMN supplementation provides the best balance of cost, convenience, evidence base, and effectiveness. IV infusions may be worth considering for people who cannot tolerate oral supplements due to severe GI issues, or for those who want the immediate effect of IV delivery and have the budget to support it.
If you are already managing tirzepatide injection logistics, adding subcutaneous NAD+ injections requires separate injection sites and a different needle gauge, which some people find burdensome. Oral supplementation avoids this complexity entirely.
What happens when you stop NAD+ supplementation
A question many researchers overlook. If you add NAD+ during your tirzepatide treatment and then stop, what happens?
NAD+ supplementation does not create dependency. Your body continues producing NAD+ through its normal salvage and de novo pathways regardless of supplementation. When you stop taking NMN or NR, your blood NAD+ levels will gradually return to baseline over a period of one to two weeks. The timeframe depends on your age, diet, exercise habits, and overall metabolic health.
However, if you stop NAD+ supplementation while still on tirzepatide, you may notice the fatigue or energy decline returning if those symptoms were being managed by the NAD+ support. This does not mean you are dependent on the supplement. It means the underlying demand for NAD+ still exceeds your natural production capacity during active weight loss.
Most researchers plan their NAD+ supplementation to span the entire duration of their tirzepatide treatment, then taper off after reaching their goal weight and transitioning to a maintenance protocol. At maintenance, caloric intake stabilizes, weight loss slows or stops, and the extraordinary NAD+ demands of rapid fat loss decrease. Some people continue NAD+ supplementation indefinitely for its anti-aging benefits, regardless of tirzepatide status.
Diet considerations for maximizing NAD+ during tirzepatide therapy
Supplementation is one half of the equation. Diet is the other.
Your body produces NAD+ from dietary precursors, primarily tryptophan (found in turkey, chicken, eggs, dairy, and nuts) and niacin/B3 (found in meat, fish, legumes, and fortified grains). When tirzepatide suppresses your appetite and reduces your overall food intake, you are getting less of these precursors from diet. Smart food choices can partially offset this decline.
Foods that support NAD+ production:
Fatty fish (salmon, tuna, sardines): Rich in niacin and tryptophan
Chicken breast: One of the highest food sources of niacin
Turkey: High in tryptophan, a NAD+ precursor
Eggs: Contain both tryptophan and B vitamins
Green vegetables: Broccoli, edamame, and cucumber contain small amounts of NMN naturally
Avocado: Contains NMN along with healthy fats
Mushrooms: Some varieties contain NR
Building meals around these foods while following your tirzepatide diet plan provides a dietary foundation that supplementation can build upon. The goal is not to get all your NAD+ precursors from food (that would require impractically large quantities) but to ensure your baseline dietary intake supports rather than undermines your supplementation strategy.
Prioritize protein at every meal. This serves the dual purpose of supporting muscle preservation and providing amino acid precursors for NAD+ synthesis. Our best foods to eat on GLP-1 therapy guide provides comprehensive meal planning strategies that align well with NAD+ optimization.
Combining NAD+ with other tirzepatide support supplements
NAD+ does not exist in a vacuum. It works within a complex metabolic network where other nutrients and cofactors play supporting roles. Understanding how NAD+ interacts with the most common tirzepatide support supplements helps you build a coherent strategy rather than a random collection of pills.
NAD+ and B12
Tirzepatide with B12 is one of the most popular combinations, and for good reason. B12 supports methylation, red blood cell production, and neurological function, all processes that can be stressed during rapid weight loss. Adding NAD+ to this combination is complementary, not redundant. B12 and NAD+ participate in different metabolic pathways that converge on energy production. B12 supports the methylation cycle and folate metabolism. NAD+ supports the electron transport chain and sirtuin activity. Together, they address energy production from two different angles.
Many compounded tirzepatide formulations already include methylcobalamin (B12). If yours does, oral NMN supplementation adds the NAD+ component without requiring any changes to your existing protocol.
NAD+ and glycine
Glycine is a fascinating addition to NAD+ supplementation because it supports both NAD+ metabolism and independent health benefits. Research published in Cell Metabolism found that glycine and NAC (N-acetylcysteine) together can boost glutathione levels, the body master antioxidant, which is relevant because glutathione production also depends partly on NAD+ availability. Additionally, glycine taken at bedtime (3-5g) improves sleep quality, and quality sleep is when your body performs the majority of its NAD+ dependent repair processes.
The tirzepatide glycine B12 compound already combines two of these elements. Adding oral NMN creates a triple support system: NAD+ for mitochondrial energy, B12 for methylation, glycine for sleep and collagen synthesis.
NAD+ and niacinamide
Tirzepatide with niacinamide requires more careful consideration. Niacinamide (nicotinamide) is itself a NAD+ precursor, it converts to NAD+ through the salvage pathway. If you are already taking NMN, adding niacinamide may be redundant. High combined doses of multiple NAD+ precursors can cause GI discomfort and flushing. If your compounded tirzepatide includes niacinamide, you may want to start with a lower NMN dose (250mg or less) and adjust based on tolerance.
NAD+ and L-carnitine
This is one of the most synergistic pairings for tirzepatide users focused on fat loss. L-carnitine (levocarnitine) transports long-chain fatty acids into the mitochondria for oxidation. NAD+ ensures the mitochondria can actually process those fatty acids once they arrive. Without adequate NAD+, even perfect fatty acid delivery does not result in efficient fat burning. Without adequate L-carnitine, NAD+ replete mitochondria sit idle waiting for fuel that never arrives.
Together, they create a complete fat-burning pipeline: L-carnitine delivers the fuel, NAD+ ensures the engine can run.
NAD+ and tirzepatide for specific populations
Women over 40
Women in perimenopause and menopause experience accelerated NAD+ decline alongside hormonal changes that already complicate weight loss. Estrogen has protective effects on mitochondrial function, and as estrogen levels drop, mitochondrial efficiency decreases in parallel. Adding tirzepatide to this hormonal landscape produces weight loss but may intensify the fatigue and brain fog that perimenopausal women already struggle with.
NAD+ supplementation may be particularly beneficial for this group because it addresses the mitochondrial dysfunction directly, independent of hormonal status. Researchers in this demographic often report the most dramatic improvement in energy and cognitive clarity when adding NMN to their tirzepatide protocol.
Women considering tirzepatide should also review how the medication affects menstrual cycles and discuss the interaction with any hormone replacement therapy with their provider.
Men prioritizing body composition
Men are often more focused on preserving muscle mass during weight loss than achieving a specific number on the scale. The tirzepatide results in men show significant fat loss but also notable lean mass reduction in the absence of resistance training and nutritional optimization.
For men prioritizing body recomposition, the NAD+ plus tirzepatide combination makes particular sense when paired with progressive resistance training and high protein intake. NAD+ supports the muscle mitochondrial health needed for performance in the gym, protein provides the raw materials for muscle protein synthesis, and resistance training provides the stimulus that tells your body to prioritize muscle retention over muscle breakdown.
People over 60
Age-related NAD+ decline is most pronounced in older adults, and the combination of age-related depletion plus tirzepatide-induced caloric restriction creates the largest potential deficit. However, this group also has the most considerations around drug interactions and existing health conditions.
Starting with the conservative protocol (250mg NMN daily) and escalating slowly while monitoring for any changes in blood pressure, blood glucose, or medication effectiveness is the prudent approach. Tirzepatide effectiveness does not depend on NAD+ supplementation, so there is no urgency to start high.
People who have stalled on tirzepatide
Weight loss plateaus on tirzepatide are common and frustrating. After initial rapid loss, many people experience weeks or months where the scale barely moves despite continued appetite suppression and adherence to their protocol. Our guide on why tirzepatide stops working covers the major reasons, from metabolic adaptation to dose saturation.
NAD+ supplementation is worth trying during a plateau because improved metabolic flexibility (the ability to switch between glucose and fat burning) is one of the mechanisms that can restart stalled fat loss. If your mitochondria are running at reduced capacity due to NAD+ depletion, they are less efficient at burning fat even when caloric restriction is maintained. Restoring NAD+ levels may not break every plateau, but it addresses one potential contributing factor at relatively low cost and risk.
Other strategies to combine with NAD+ during a plateau include adjusting macronutrient ratios (more protein, less processed carbohydrate), increasing physical activity, considering microdosing approaches, or discussing dose adjustments with your provider.
Monitoring and blood work
If you are serious about optimizing the NAD+ and tirzepatide combination, periodic blood work provides objective feedback that subjective feelings cannot.
Baseline labs before starting NAD+ supplementation:
Comprehensive metabolic panel (CMP)
Fasting insulin and glucose
HbA1c
Complete blood count (CBC)
Lipid panel
Liver enzymes (AST, ALT)
Vitamin B12 and folate levels
Follow-up labs at 8-12 weeks:
Repeat all baseline labs
Note improvements in insulin sensitivity (fasting insulin, HOMA-IR)
Monitor liver enzymes (both tirzepatide and NMN are processed through the liver)
Check B12 levels if supplementing B12 alongside NAD+
NAD+ specific testing: Blood NAD+ levels can be measured through specialized labs, though this testing is not widely available or standardized. Companies like Jinfiniti offer intracellular NAD+ testing that may provide more clinically relevant data than serum levels. This testing is optional and not required for most users, but it can confirm whether your supplementation is actually raising NAD+ levels.
Your provider can help interpret these results in the context of your overall tirzepatide treatment progress and adjust your protocol accordingly.
Common mistakes when combining NAD+ with tirzepatide
Knowing what not to do is often as valuable as knowing what to do. These are the errors researchers most frequently make when adding NAD+ to their tirzepatide protocol.
Starting too high, too fast. Jumping to 1,000mg NMN on day one while also escalating your tirzepatide dose creates a confusing situation where any new side effect could come from either change. Start NMN at 250mg, wait two weeks, then increase. Never change both your tirzepatide dose and your NMN dose in the same week.
Taking NMN at night. NMN boosts cellular energy. Taking it before bed is like drinking coffee at 10pm. Your cells do not know it is bedtime. They just see more NAD+ and ramp up metabolic activity. All NMN doses should be taken before 3pm.
Ignoring protein intake. NAD+ supports muscle mitochondrial function, but mitochondria do not build muscle by themselves. Without adequate protein (minimum 1.2g per kg body weight), the dietary foundation for muscle preservation is missing, and NAD+ supplementation alone will not compensate.
Buying low-quality NMN supplements. The NAD+ precursor market has exploded with products of highly variable quality. Third-party testing for purity, potency, and contaminants is essential. Look for brands with certificates of analysis (COA) from independent labs. Sublingual NMN formulations may offer better absorption than standard capsules, though the evidence for this advantage is preliminary.
Expecting immediate results. NAD+ supplementation is not like caffeine. You will not feel a dramatic energy surge on day one. The benefits build over two to four weeks as cellular NAD+ levels reach steady state and mitochondrial function gradually improves. Patience matters.
Stacking too many NAD+ precursors. Taking NMN, NR, niacin, and niacinamide simultaneously does not produce four times the benefit. It produces GI distress and possibly liver strain. Choose one primary NAD+ precursor (NMN is recommended for tirzepatide users) and use it consistently. If your compounded tirzepatide includes niacinamide, account for this when determining your NMN dose.
What the online community reports
While anecdotal evidence is not scientific proof, community reports provide useful signal about real-world experiences. Across peptide forums, Reddit communities, and weight loss groups, several consistent themes emerge from people combining NAD+ with tirzepatide.
Energy improvement is the most consistently reported benefit. The majority of users who add NMN or NR to their tirzepatide protocol report improved baseline energy within two to three weeks. The descriptions vary from "I no longer need an afternoon nap" to "my brain fog finally lifted" to "I can exercise again without feeling destroyed afterward."
GI tolerance is generally good when timing is managed. Most reports of increased nausea come from people who started NMN at high doses immediately or who take it on an empty stomach. Those who follow a gradual introduction with food report no additional GI burden beyond what tirzepatide itself causes.
Exercise performance improvement is frequently mentioned. People who maintain fitness routines during tirzepatide therapy often report that adding NAD+ improves their workout energy and recovery. This aligns with the muscle mitochondria support mechanism and the energy-enhancing properties of NAD+ precursors.
Sleep quality reports are mixed. Some users report better sleep with NAD+ supplementation. Others report sleep disruption. The difference almost always correlates with timing, those who take NMN in the morning sleep well, those who take it in the afternoon or evening report restlessness. This reinforces the importance of the timing guidelines discussed earlier.
Weight loss acceleration is occasionally reported but inconsistent. Some users feel that adding NAD+ helped break a plateau or accelerated their rate of loss. Others see no difference in weight loss speed. This inconsistency suggests that NAD+ is not a direct weight loss accelerator but may help optimize the metabolic environment that tirzepatide works within.
Alternatives to NAD+ for tirzepatide energy support
NAD+ supplementation is not the only approach to managing energy during tirzepatide therapy. If NAD+ is not accessible, affordable, or well tolerated, several alternatives address the same underlying energy production pathways through different mechanisms.
CoQ10 (Coenzyme Q10): Like NAD+, CoQ10 is a critical component of the mitochondrial electron transport chain. It functions at a different step (Complex III) than NAD+ (Complex I), so the two are complementary rather than redundant. CoQ10 at 100-200mg daily may support mitochondrial energy production independently. It is widely available, well-tolerated, and inexpensive.
Creatine: Creatine supports rapid energy recycling (ATP regeneration) in high-demand tissues like muscle and brain. At 3-5g daily, creatine helps maintain exercise performance and cognitive function during caloric restriction. It does not replace NAD+ but addresses a related energy pathway.
Alpha-lipoic acid: This antioxidant supports mitochondrial function and has some evidence for improving insulin sensitivity. At 300-600mg daily, it may provide mild energy support and metabolic benefits that complement tirzepatide therapy.
Berberine activates AMPK, the same cellular energy sensor that sirtuins (NAD+ dependent enzymes) regulate. While berberine is more commonly discussed alongside semaglutide, some researchers use it with tirzepatide for its insulin-sensitizing and metabolic effects. Note that berberine can interact with various medications, so professional guidance is essential.
None of these alternatives fully replicate the NAD+ specific benefits (sirtuin activation, DNA repair support, circadian rhythm regulation), but they each address aspects of the energy production challenge that tirzepatide users face.
Frequently asked questions
Can I take NAD+ and tirzepatide on the same day?
Yes. There is no need to separate them by days. The key is separating them by hours within the same day. Take your NMN supplement in the morning with food, and schedule your tirzepatide injection at your normal time. A two-hour gap between NMN and the injection is sufficient to minimize any combined GI effects.
Will NAD+ make my tirzepatide work better?
There is no direct evidence that NAD+ enhances tirzepatide potency. However, by supporting mitochondrial function and potentially increasing endogenous GLP-1 production (with NMN specifically), NAD+ may optimize the metabolic environment in which tirzepatide operates. Think of it as tuning the engine rather than adding more fuel.
How long should I take NAD+ with tirzepatide?
Most researchers maintain NAD+ supplementation throughout their entire tirzepatide treatment period and taper off during the tirzepatide tapering phase. Some continue indefinitely for general longevity benefits. There is no medical reason to limit the duration, as NAD+ precursors have been shown safe in studies lasting up to 12 months.
Is NMN or NR better with tirzepatide?
For tirzepatide users specifically, NMN has the stronger theoretical case due to its demonstrated ability to enhance GLP-1 production through intestinal NAD+ restoration. NR is a reasonable alternative if NMN is unavailable. Both effectively raise NAD+ levels. See the comparison table in the NMN versus NR section above for a detailed breakdown.
Can NAD+ cause weight gain?
No. NAD+ supplementation has not been associated with weight gain in any clinical study. A meta-analysis of NAD+ precursor trials actually found modest reductions in BMI and increases in adiponectin (a hormone that supports fat metabolism). NAD+ supports fat burning at the cellular level, not fat storage.
Should I tell my doctor about taking NAD+ with tirzepatide?
Absolutely. Always inform your healthcare provider about all supplements you are taking alongside prescription or research medications. While NAD+ precursors are generally safe, your provider needs a complete picture of your supplementation to identify any potential interactions with your specific health profile and other medications.
Can I take NAD+ if my tirzepatide already contains B12 or niacinamide?
Yes, but with dosing adjustments. If your compounded tirzepatide includes B12, no NMN adjustment is needed as they work through different pathways. If it includes niacinamide, start with a lower NMN dose (250mg or less) since both feed into the NAD+ pathway, and monitor for GI tolerance before increasing.
Does NAD+ help with tirzepatide hair loss?
NAD+ supports cellular repair including in hair follicles, but there is no specific evidence that NAD+ prevents or reverses GLP-1 related hair loss. Hair loss during rapid weight loss is typically related to telogen effluvium from nutritional stress and caloric restriction. Ensuring adequate protein, biotin, iron, and zinc is more directly relevant to hair health than NAD+ supplementation.
Can I take NAD+ with semaglutide instead of tirzepatide?
Yes. The same principles apply to semaglutide users experiencing fatigue. NAD+ precursors work through cellular energy pathways that are independent of which GLP-1 receptor agonist you are using. The NMN advantage regarding GLP-1 production enhancement would apply equally to semaglutide users. See our semaglutide versus tirzepatide comparison for differences between the two medications.
For researchers serious about optimizing their peptide protocols, SeekPeptides provides the most comprehensive resource available, with evidence-based guides, dosing calculators, and a community of thousands who navigate these exact questions. SeekPeptides members access detailed protocols, stacking tools, and expert guidance for every stage of their research journey.
External resources
Safety and antiaging effects of NMN in human clinical trials (PMC)
Intestinal NAD+ biosynthesis regulates GLP-1 production (Oxford Academic)
NAD+ precursor supplementation and weight loss meta-analysis (PMC)
NMN characteristics and pharmacodynamic effects (Frontiers in Pharmacology)
In case I do not see you, good afternoon, good evening, and good night. May your mitochondria stay fueled, your energy stay steady, and your protocols stay optimized.