Mar 10, 2026

What if the medication you are worried about is actually helping the problem you think it is causing? That is the question facing thousands of men who start tirzepatide for weight loss and immediately begin searching whether it will wreck their sexual health. The fear is understandable. You are injecting a powerful peptide that changes your appetite, your metabolism, your energy levels, and seemingly everything about how your body functions. Of course you want to know what it does below the belt.
Here is the short answer. No.
Tirzepatide does not cause erectile dysfunction in most men. The emerging research actually points in the opposite direction. A 2025 retrospective cohort study published in the Journal of Diabetes Complications found that tirzepatide was associated with a significantly reduced risk of ED compared to three other diabetes medications. And a separate pilot study showed tirzepatide boosted testosterone levels in obese men more effectively than testosterone replacement therapy itself. Those are not small findings. Those are paradigm-shifting results that flip the entire concern on its head.
But the full story is more nuanced than a simple yes or no. Some men do experience temporary changes in libido during dose escalation. Others find that the nausea and fatigue common in early weeks dampens their interest in sex. And a handful of case reports describe sexual side effects that deserve serious examination. This guide breaks down every piece of evidence, every mechanism, every real-world experience, and every strategy for protecting your sexual health while using tirzepatide. By the end, you will know exactly what to expect, what to watch for, and what to do if problems arise.
SeekPeptides has analyzed the clinical data, community reports, and mechanistic research to create the most comprehensive resource available on this topic. Whether you are about to start tirzepatide, already on it and noticing changes, or researching for someone you care about, this guide covers it all.
What the clinical research says about tirzepatide and erectile dysfunction
The most important study to date on this topic comes from researchers at the University of South Florida. Published in the Journal of Diabetes Complications in 2025, this retrospective cohort study used the TriNetX global health research network to compare erectile dysfunction outcomes across four different medications. The study period ran from May 2022 to May 2025, capturing real-world data from thousands of male patients aged 18 to 70 with type 2 diabetes and no prior ED diagnosis.
The results were striking.
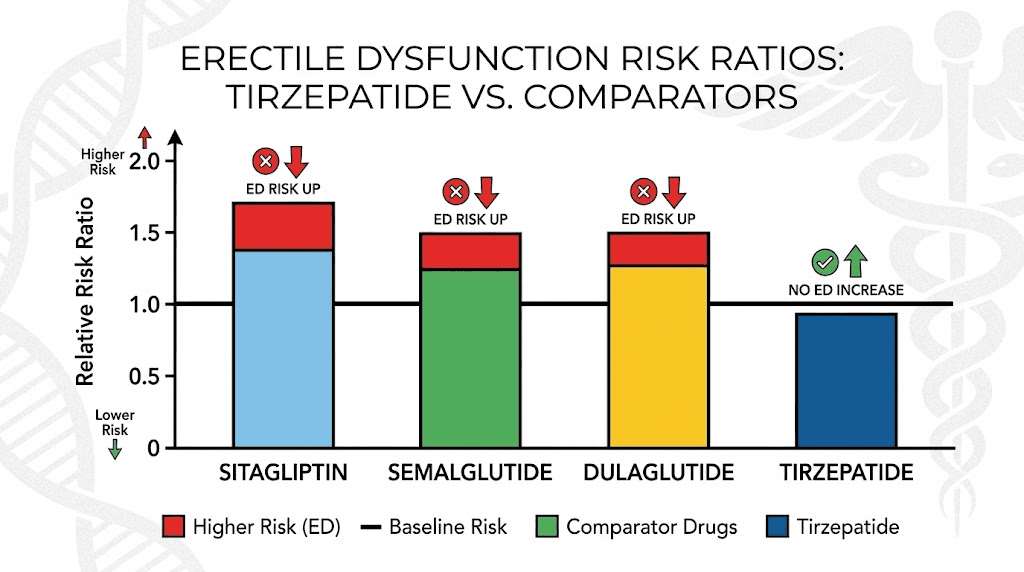
Tirzepatide was associated with a lower risk of ED compared to every medication it was tested against. When compared to sitagliptin, the risk ratio was 0.70. That means men on tirzepatide had a 30% lower chance of developing ED or needing a PDE-5 inhibitor prescription. Against injectable semaglutide, the risk ratio dropped to 0.67, representing a 33% reduction. And against dulaglutide, tirzepatide showed a risk ratio of 0.55, meaning a 45% lower risk of erectile dysfunction.
All three comparisons reached statistical significance with p-values below 0.001. These are not borderline results. These are robust, clinically meaningful differences that survived propensity score matching to control for confounding variables like age, BMI, comorbidities, and medication history.
But context matters. This was a retrospective study, not a randomized controlled trial. The researchers themselves noted that randomized trials are needed to confirm these findings and explore potential mechanisms. Still, the direction of the evidence is clear. Tirzepatide does not appear to cause ED. If anything, it appears to protect against it.
Why tirzepatide might actually improve erectile function
The mechanisms behind this protective effect are not mysterious once you understand the biology. Erectile dysfunction is fundamentally a vascular and hormonal condition. Blood flow, nerve function, testosterone levels, and psychological factors all converge to determine erectile quality. Tirzepatide influences several of these pathways simultaneously.
First, weight loss. Obesity is one of the strongest independent risk factors for ED. Research published in the Journal of the American Medical Association showed that weight loss alone restored erectile function in over 30% of obese men who lost an average of just 33 pounds over two years. Tirzepatide produces weight loss of 15% to 25% of body weight in clinical trials, far exceeding the threshold shown to improve sexual function.
Second, testosterone. Excess body fat contains aromatase, an enzyme that converts testosterone into estradiol. The more fat you carry, the more testosterone gets converted to estrogen. One study found that an increase of just 4 inches in waist circumference was associated with a 75% chance of having clinically low testosterone. By reducing body fat, tirzepatide reverses this conversion and allows natural testosterone production to recover.
Third, insulin sensitivity. Type 2 diabetes and insulin resistance damage the endothelium, the inner lining of blood vessels responsible for producing nitric oxide. Nitric oxide is the molecule that triggers the vascular dilation required for erections. Tirzepatide dramatically improves insulin sensitivity, which in turn improves endothelial function and blood flow to every organ, including the penis.
Fourth, inflammation. Chronic low-grade inflammation associated with obesity damages blood vessels and nerves throughout the body. Tirzepatide reduces inflammatory markers, which supports better overall vascular health and nerve function.
The FAERS database analysis
A separate 2025 study examined the FDA Adverse Event Reporting System (FAERS) database for reports of male sexual dysfunction associated with GLP-1 receptor agonists. This cross-sectional analysis found some reports of sexual dysfunction linked to GLP-1 medications as a class, but the overall signal was weak and inconsistent.
The FAERS database has significant limitations. Anyone can submit a report, causation cannot be established from adverse event reports alone, and reporting bias affects the data substantially. Medications that receive more media attention about sexual side effects tend to generate more reports regardless of actual risk. The researchers concluded that while monitoring is appropriate, the current evidence does not support a causal link between tirzepatide and erectile dysfunction.
How tirzepatide affects testosterone levels in men
A groundbreaking pilot study published in Reproductive Biology and Endocrinology in 2025 provides the most direct evidence that tirzepatide positively affects male hormonal health. This controlled study examined 83 overweight men with metabolic hypogonadism, a condition where obesity suppresses the hormonal axis and leads to clinically low testosterone.
The study divided participants into three groups. One received tirzepatide. One received lifestyle modifications alone. And one received actual testosterone replacement therapy. After 8 weeks, the researchers measured a comprehensive panel of hormonal markers.
The tirzepatide group showed significantly higher serum levels of luteinizing hormone, follicle-stimulating hormone, sex hormone-binding globulin, total testosterone, free testosterone, and bioavailable testosterone compared to both other groups. They also showed significantly lower estradiol levels. In plain language, tirzepatide helped the body produce more of its own testosterone while simultaneously reducing the conversion of testosterone to estrogen.
Read that again. Tirzepatide outperformed actual testosterone replacement therapy for improving natural hormone production.
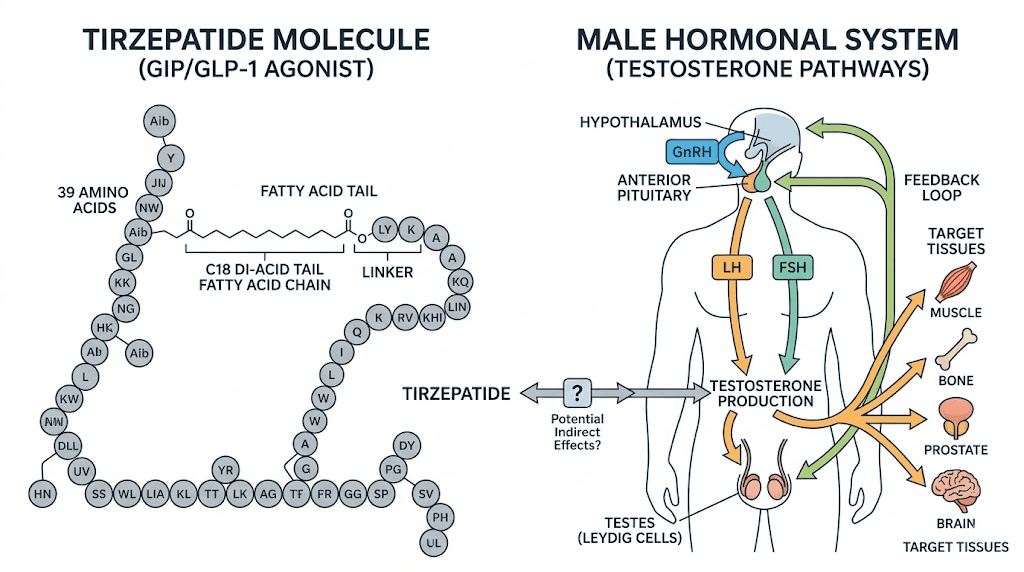
The mechanism is elegant in its simplicity. Excess adipose tissue produces aromatase, which converts testosterone to estradiol. This excess estradiol then suppresses gonadotropin-releasing hormone (GnRH) in the hypothalamus, which reduces LH and FSH output from the pituitary, which further reduces testosterone production from the testes. It is a vicious cycle that obesity perpetuates.
Tirzepatide breaks this cycle by rapidly reducing body fat. Less fat means less aromatase. Less aromatase means less testosterone-to-estrogen conversion. Less estrogen means the hypothalamus receives the signal to increase GnRH. More GnRH means more LH and FSH. More LH means the testes produce more testosterone. The entire hormonal axis resets toward healthy function.
Unlike exogenous testosterone replacement, which suppresses the hypothalamic-pituitary-gonadal axis and can impair fertility, tirzepatide works by restoring the natural production pathway. This is a critical distinction for younger men who may want to preserve fertility while addressing both weight and hormonal concerns.
What this means for men with low testosterone
If you are an overweight man with symptoms of low testosterone, fatigue, low libido, difficulty building muscle, brain fog, mood changes, tirzepatide may address the root cause rather than just the symptoms. Testosterone replacement therapy replaces the hormone but does not fix why levels are low. Tirzepatide, by driving significant fat loss, actually corrects the underlying metabolic dysfunction that suppressed testosterone in the first place.
This does not mean tirzepatide replaces TRT for all men. Men with primary hypogonadism, where the testes themselves are dysfunctional, will still need testosterone therapy. But for the millions of men with obesity-related secondary hypogonadism, tirzepatide offers a fundamentally different and potentially superior approach.
The 2025 systematic review and meta-analysis on GLP-1 receptor agonists and testosterone confirmed these findings at scale. Across multiple studies, GLP-1 RAs increased total testosterone and gonadotropins while reducing body weight. The improvements in erectile function correlated with hormonal improvements but also appeared to involve mechanisms independent of weight loss alone.
Temporary sexual side effects during dose escalation
While the long-term evidence favors improved sexual function, the short-term reality during the first weeks of tirzepatide treatment can be different. Understanding this distinction is crucial for managing expectations and avoiding premature concern.
During dose escalation, particularly in the first 4 to 8 weeks, many men experience gastrointestinal side effects that can indirectly affect sexual desire and performance. Nausea, reduced appetite, fatigue, and general malaise do not create an environment conducive to sexual interest. When you feel sick, sex drops down the priority list. This is normal. This is temporary. And this is not erectile dysfunction.
The distinction matters medically. True erectile dysfunction means the inability to achieve or maintain an erection sufficient for sexual activity despite adequate desire. What most men experience during tirzepatide dose escalation is reduced libido, decreased interest rather than decreased ability. These are fundamentally different conditions with different causes and different prognoses.
What happens during the first weeks
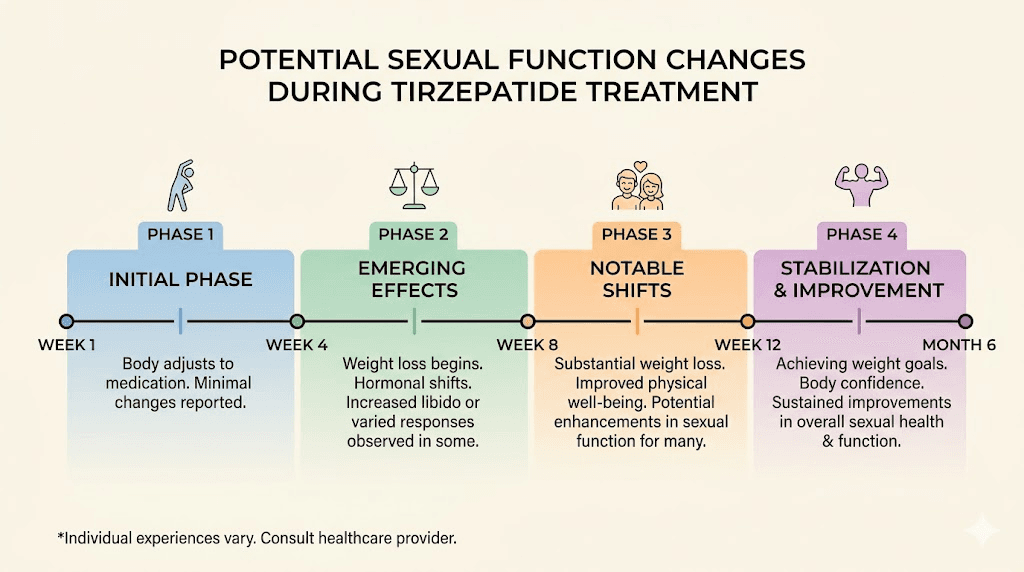
Week one through four on tirzepatide often involves the body adjusting to GLP-1 and GIP receptor activation. The gastrointestinal tract slows down. Appetite drops significantly. Some men report feeling unusually tired as their caloric intake decreases dramatically. Others experience nausea that peaks in the hours after injection and gradually fades over the following days.
During this adjustment period, sexual interest commonly decreases. This is a normal physiological response. The body is adapting to reduced caloric intake, shifting metabolic processes, and managing gastrointestinal changes. Sexual function is not a survival priority when the body is stressed, and the early days of GLP-1 therapy represent a form of metabolic stress that the body needs time to accommodate.
By weeks four through eight, most men report that gastrointestinal side effects have stabilized or resolved. As the body adapts and side effects diminish, sexual interest typically returns. Many men then begin to notice the positive effects of weight loss on their sexual health, including improved erection quality, increased stamina, and higher spontaneous desire.
The energy deficit factor
Caloric restriction, regardless of the method, temporarily reduces testosterone and libido. This is a well-documented physiological response that occurs with any significant diet change. When you consume substantially fewer calories than your body is accustomed to, reproductive hormones downregulate as the body prioritizes survival functions over reproductive ones.
Tirzepatide produces profound appetite suppression. Some men find their daily caloric intake drops by 40% to 60% in the early weeks. This dramatic reduction can temporarily lower testosterone and reduce sexual interest even before the metabolic benefits of weight loss begin to manifest.
The solution is not to panic. The solution is to ensure adequate protein intake (0.7 to 1 gram per pound of body weight), maintain basic nutritional adequacy with a well-designed meal plan, and give your body time to adapt. As weight loss progresses and the body establishes a new metabolic equilibrium, testosterone levels typically rise rather than fall, and sexual function improves.
The obesity and erectile dysfunction connection explained
To fully understand why tirzepatide is more likely to help ED than cause it, you need to understand the devastating relationship between obesity and erectile function. This is not a minor association. It is one of the strongest and most consistent findings in sexual medicine research.
Obese men are significantly more likely to develop ED than men of normal weight, even after controlling for age, diabetes status, cardiovascular disease, and medication use. The relationship is dose-dependent. The more excess weight a man carries, the higher his risk of erectile dysfunction.
Hormonal disruption from excess body fat
Adipose tissue is not inert storage. It is an active endocrine organ that produces hormones, inflammatory mediators, and enzymes that directly affect sexual function. The most important of these for erectile health is aromatase.
Aromatase converts circulating testosterone into estradiol. In lean men, this conversion occurs at a rate that maintains healthy hormonal balance. In obese men, the dramatically increased volume of adipose tissue produces excess aromatase, tipping the balance toward estrogen dominance. The resulting hormonal profile, low testosterone and elevated estradiol, directly impairs libido, erectile function, and sexual satisfaction.
But the hormonal damage extends beyond the testosterone-estrogen axis. Obesity increases cortisol production, which independently suppresses testosterone synthesis. It increases sex hormone-binding globulin in some contexts while paradoxically reducing it in others, creating unpredictable fluctuations in bioavailable testosterone. And it disrupts insulin signaling in ways that impair nitric oxide production, the chemical messenger essential for healthy erectile function.
Vascular damage from metabolic syndrome
Erectile function depends on healthy blood vessels. An erection requires rapid, significant blood flow into the penile corpora cavernosa, the spongy tissue that fills with blood during arousal. This process demands healthy endothelium, flexible arterial walls, and functional nitric oxide signaling.
Obesity and its associated conditions, insulin resistance, dyslipidemia, hypertension, and chronic inflammation, systematically damage every component of this vascular system. The endothelium loses its ability to produce adequate nitric oxide. Arterial walls stiffen and thicken. Small blood vessels, the very ones that supply the penis, narrow and become less responsive to vasodilatory signals.
This is why ED is often called the canary in the coal mine for cardiovascular disease. The penile arteries are among the smallest in the body, typically 1 to 2 millimeters in diameter. They are often the first to show signs of vascular damage. By the time a man develops ED from vascular causes, larger vessels in the heart and brain may already be compromised.
Tirzepatide addresses vascular ED at its root by reducing body fat, improving insulin sensitivity, lowering inflammatory markers, and improving lipid profiles. These metabolic improvements translate directly into better endothelial function and improved blood flow, including to the erectile tissue.
Psychological factors in obesity-related ED
The relationship between obesity and ED is not purely physical. Body image, self-confidence, and mood all play significant roles in sexual function. Many obese men experience depression, anxiety, and poor body image that directly impair sexual desire and performance. These psychological factors create a feedback loop where poor sexual performance increases anxiety, which further impairs performance.
Weight loss on tirzepatide addresses this psychological dimension powerfully. As men lose weight, body confidence improves. Clothes fit better. Energy increases. The physical transformation creates psychological momentum that extends into the bedroom.
Multiple studies have confirmed that weight loss, independent of the method used, improves sexual satisfaction scores, reduces performance anxiety, and increases sexual confidence. Tirzepatide produces the kind of dramatic, visible weight loss that transforms not just the body but the mindset.
GLP-1 receptor agonists and male sexual health: the broader evidence
Tirzepatide is not the only GLP-1 receptor agonist studied for effects on male sexual health. The broader class of GLP-1 RAs has generated an increasingly positive body of evidence, providing additional context for understanding tirzepatide specifically.
The European Congress of Endocrinology findings
A 1-year retrospective cohort study presented at the 26th European Congress of Endocrinology found that GLP-1 RAs added to metformin therapy significantly improved erectile function scores in men with type 2 diabetes and ED. The improvement occurred regardless of different background characteristics and testicular function, suggesting that the benefits are broadly applicable rather than limited to specific patient subsets.
The leading determinant of erectile function improvement was GLP-1 RA treatment itself, more so than changes in HbA1c, weight, or other metabolic parameters. This finding suggests that GLP-1 receptor agonists may have direct or indirect effects on erectile function beyond what can be explained by metabolic improvements alone.
Testosterone effects across the GLP-1 class
A 2025 systematic review and meta-analysis examining GLP-1 RA effects on testosterone found consistent increases in total testosterone across multiple agents and studies. The researchers noted that while weight loss likely drives much of the testosterone improvement, the lack of a significant association between the degree of weight loss and testosterone change in some analyses suggests additional mechanisms may be at work.
One proposed mechanism involves GLP-1 receptors in the hypothalamus and pituitary gland. GLP-1 signaling in these regions may directly stimulate gonadotropin release, enhancing natural testosterone production through central nervous system effects independent of weight loss. This hypothesis remains under investigation, but it would explain why GLP-1 RAs sometimes improve testosterone more than expected based on the degree of weight loss achieved.
Tirzepatide may have an advantage over pure GLP-1 RAs in this regard because it also activates GIP receptors. GIP (glucose-dependent insulinotropic polypeptide) has been identified in reproductive tissues, and GIP receptor activation may contribute to the hormonal benefits observed with tirzepatide. This dual mechanism could explain why the Cowart study found tirzepatide performed better than injectable semaglutide for ED risk reduction.
Important distinction: semaglutide versus tirzepatide
Not all GLP-1 medications are identical when it comes to sexual health. The FAERS analysis found that some reports of sexual dysfunction were more common with semaglutide than with tirzepatide. While the clinical significance of FAERS data is limited, the 2025 cohort study corroborates this difference by showing tirzepatide had a lower ED risk ratio than injectable semaglutide (0.67).
The reasons for this difference likely relate to the dual GLP-1/GIP mechanism of tirzepatide versus the pure GLP-1 action of semaglutide. Tirzepatide may produce more favorable hormonal changes, different gastrointestinal side effect profiles, or additional metabolic benefits through GIP receptor activation that contribute to better sexual health outcomes. For men particularly concerned about sexual function, this distinction may be relevant when choosing between GLP-1 therapies.
Real-world experiences: what men actually report
Clinical studies provide the foundation, but real-world experiences fill in the details that trials cannot capture. Online communities, patient forums, and clinical practice reports paint a nuanced picture of how tirzepatide affects male sexual function in everyday use.
The early weeks: temporary dip in desire
The most consistent report across communities like Reddit and patient forums is a temporary reduction in sexual desire during the first 2 to 6 weeks of treatment. Men describe this not as erectile dysfunction but as simply having less interest in sex. The pattern typically aligns with peak gastrointestinal side effects, particularly nausea and fatigue.
Common descriptions include feeling too nauseated to think about sex, being too tired in the evenings, and experiencing a general dampening of drive that lifts as side effects resolve. These experiences are consistent with the physiological effects of caloric restriction, GI disturbance, and metabolic adaptation rather than any direct effect on erectile tissue or hormonal function.
The turning point: weeks 6 through 12
Around the 6 to 12 week mark, many men report a notable improvement in sexual function that exceeds their pre-treatment baseline. The combination of weight loss, improved energy, better body image, and hormonal recovery creates what many describe as a sexual renaissance. Erection quality improves. Morning erections return or become more frequent. Spontaneous desire increases. Stamina during sexual activity improves.
These reports align perfectly with the clinical data. As body fat decreases, testosterone rises, estrogen falls, insulin sensitivity improves, and endothelial function recovers. The body is literally rebuilding its capacity for healthy sexual function from the ground up.
The long-term picture: sustained improvement
Men who have been on tirzepatide for 6 months or longer consistently report sustained improvements in sexual health. The initial dip is a distant memory. What remains is the accumulated benefit of significant weight loss, normalized hormones, improved cardiovascular fitness, and better psychological wellbeing.
Some men report that their sexual function at 30 to 50 pounds lighter is better than it has been in years or even decades. Others note that the improvement was gradual and took several months to fully manifest. A smaller group reports no change in sexual function, neither positive nor negative, which is also a perfectly normal outcome.
The rare negative experience
A small percentage of men do report persistent sexual difficulties while on tirzepatide. These cases typically involve one or more confounding factors: rapid weight loss exceeding 2 to 3 pounds per week, inadequate protein intake leading to muscle loss, concurrent use of medications known to affect sexual function (SSRIs, beta-blockers, antiandrogens), or pre-existing hormonal conditions unrelated to obesity.
When persistent sexual side effects occur on tirzepatide, they warrant medical evaluation. The cause is almost never the tirzepatide itself but rather an underlying condition that the medication has unmasked or a nutritional deficiency that excessive caloric restriction has created.
Specific mechanisms: how tirzepatide protects erectile function
Understanding the specific biological mechanisms helps explain why tirzepatide is protective rather than harmful for erectile function. Each mechanism represents a separate pathway through which this dual-agonist peptide improves the conditions necessary for healthy sexual function.
Nitric oxide pathway restoration
Nitric oxide (NO) is the master regulator of erectile function. Sexual arousal triggers the release of NO from endothelial cells and nerve endings in the penile tissue. NO activates guanylate cyclase, which produces cyclic GMP, which relaxes smooth muscle in the corpora cavernosa, which allows blood to flow in and create an erection. PDE-5 inhibitors like sildenafil work by preventing the breakdown of cyclic GMP, but they cannot compensate for inadequate NO production in the first place.
Insulin resistance, the hallmark metabolic derangement of obesity, directly impairs endothelial NO synthase (eNOS) activity. Less eNOS means less NO means weaker vasodilation means poorer erections. Tirzepatide dramatically improves insulin sensitivity, often moving HbA1c from diabetic ranges to near-normal within months. This improvement directly restores eNOS function and NO production.
Additionally, the reduction in inflammatory markers that tirzepatide produces (C-reactive protein, IL-6, TNF-alpha) further supports NO bioavailability. Chronic inflammation destroys NO before it can act on smooth muscle, a process called NO quenching. By reducing inflammation, tirzepatide preserves the NO that the body produces and allows it to function normally.
Adipose tissue remodeling
Not all fat is created equal when it comes to sexual health. Visceral fat, the deep abdominal fat that surrounds internal organs, is far more metabolically active and hormologically disruptive than subcutaneous fat. Visceral fat produces more aromatase, more inflammatory cytokines, and more adipokines that impair sexual function.
Tirzepatide preferentially reduces visceral fat. Clinical imaging studies show that the weight lost on tirzepatide comes disproportionately from the visceral compartment, the exact fat depot most responsible for hormonal disruption and vascular damage. This means that the sexual health benefits of tirzepatide-driven weight loss may be greater pound-for-pound than weight loss achieved through other methods that reduce subcutaneous and visceral fat equally.
Sympathetic nervous system normalization
Obesity is associated with chronic sympathetic nervous system overactivation, essentially a state of perpetual low-level fight-or-flight response. This sympathetic overdrive increases blood pressure, constricts peripheral blood vessels, and shifts the autonomic balance away from the parasympathetic tone necessary for sexual arousal and erectile function.
Weight loss on tirzepatide reduces sympathetic tone and restores autonomic balance. Blood pressure drops. Resting heart rate decreases. The body shifts from a state of chronic stress to a state of physiological calm that is much more conducive to healthy sexual function.
Sleep quality improvement
Obesity is strongly associated with obstructive sleep apnea (OSA), a condition that fragments sleep and causes intermittent hypoxia throughout the night. OSA is independently associated with erectile dysfunction through multiple mechanisms including testosterone suppression, sympathetic activation, endothelial damage, and daytime fatigue.
Weight loss on tirzepatide frequently resolves or significantly improves sleep apnea. Some men find that their CPAP pressure requirements decrease dramatically or that they no longer need CPAP at all. The improvement in sleep quality has cascading benefits for energy levels, mood, hormonal function, and sexual health.
Protecting your sexual health while on tirzepatide
Even though the evidence overwhelmingly suggests that tirzepatide improves rather than harms sexual function, there are practical steps men can take to optimize outcomes and minimize any temporary disruptions during the adjustment period.
Protein intake is non-negotiable
Inadequate protein intake during rapid weight loss is one of the most common causes of hormonal disruption and sexual health complaints. Protein provides the amino acid building blocks for hormone synthesis, neurotransmitter production, and muscle maintenance. When protein intake falls below 0.7 grams per pound of body weight during caloric restriction, the body starts breaking down muscle tissue and downregulating hormonal production.
Aim for 0.8 to 1.0 grams of protein per pound of goal body weight daily. This is challenging on tirzepatide because appetite suppression makes eating difficult. Prioritize protein at every meal. Use protein shakes, high-protein snacks, and nutrient-dense foods to hit your target. Consider tracking protein intake specifically during the first 3 months of treatment when appetite suppression is most severe.
Do not skip resistance training
Resistance exercise is one of the most potent natural testosterone boosters available. Compound movements like squats, deadlifts, bench presses, and rows stimulate testosterone release, improve insulin sensitivity, preserve lean mass during weight loss, and directly improve body composition.
Men on tirzepatide who engage in regular resistance training report better sexual health outcomes than those who do not exercise. The combination of pharmaceutical weight loss and structured exercise creates a synergistic effect on testosterone, body composition, cardiovascular fitness, and sexual function that exceeds what either intervention achieves alone.
Aim for 3 to 4 resistance training sessions per week, focusing on compound movements with progressive overload. If you are new to weight training, start with basic movements and gradually increase intensity. The goal is to send the signal that muscle is needed so the body preferentially burns fat rather than lean tissue during the weight loss process.
Manage dose escalation gradually
Rapid dose escalation increases the severity of gastrointestinal side effects, which increases the likelihood of temporary libido disruption. If sexual health is a priority concern, discuss with your prescriber the option of extending the time at each dose level before increasing.
The standard tirzepatide dosing schedule calls for dose increases every 4 weeks, but some clinicians allow 6 to 8 weeks at each dose if the patient is experiencing significant side effects. A slower titration means milder side effects, which means less disruption to daily life including sexual function.
Some men find that microdosing approaches or split dosing reduces gastrointestinal side effects while maintaining weight loss efficacy. Discuss these options with your healthcare provider if side effects are impacting your quality of life.
Ensure adequate micronutrient intake
Several micronutrients are essential for testosterone production and erectile function. When caloric intake drops significantly on tirzepatide, deficiencies can develop that independently impair sexual health.
Zinc is critical for testosterone synthesis. Zinc deficiency causes hypogonadism and ED in as little as 20 weeks. Ensure adequate intake through food (oysters, red meat, pumpkin seeds) or supplementation (30 to 50 mg daily).
Vitamin D deficiency is associated with low testosterone and ED. Most overweight individuals are vitamin D deficient to begin with, and reduced food intake can worsen this. Supplement with 2000 to 5000 IU daily based on blood levels.
Magnesium supports testosterone production, improves sleep quality, and reduces inflammation. Aim for 400 to 600 mg daily of magnesium glycinate or citrate, which are well-absorbed forms that also support GI motility.
B vitamins, particularly B12, are essential for nerve function and energy production. Many tirzepatide formulations already include B12 supplementation, but verify with your prescriber that your levels are adequate.
Monitor your hormones
If you are concerned about sexual health on tirzepatide, baseline and follow-up hormone testing provides objective data. Request the following labs before starting and then at 3 and 6 months:
Total testosterone (optimal: 500 to 900 ng/dL for most men)
Free testosterone (optimal: 15 to 25 pg/mL)
Estradiol (optimal: 20 to 40 pg/mL)
SHBG (reference: 10 to 57 nmol/L)
LH and FSH (reference: LH 1.8 to 8.6 mIU/mL, FSH 1.5 to 12.4 mIU/mL)
If testosterone is rising and estradiol is falling over time, the trajectory is positive regardless of how you feel in the short term. If testosterone remains suppressed or drops despite weight loss, that indicates an underlying condition that warrants further evaluation by an endocrinologist or urologist.
When to be concerned: red flags and when to seek help
While most men experience neutral or positive effects on sexual function from tirzepatide, certain situations warrant medical attention. Do not ignore these signals.
Persistent ED beyond 3 months
If erectile function has not returned to baseline or improved after 3 months on stable-dose tirzepatide, something else is going on. This timeline is generous enough to account for dose adjustment effects and early metabolic changes while being short enough to catch treatable conditions before they become entrenched.
Potential causes include pre-existing vascular ED that was present before tirzepatide but was attributed to the medication, medication interactions with drugs known to cause ED (SSRIs, beta-blockers, spironolactone, finasteride), severe nutritional deficiencies from inadequate intake, or undiagnosed conditions like depression or hypogonadism unrelated to obesity.
Complete loss of morning erections
Morning erections (nocturnal penile tumescence) are a useful marker of hormonal and vascular health. Healthy men experience 3 to 5 erections during sleep, typically resulting in a morning erection upon waking. The complete absence of morning erections for more than 2 to 3 weeks suggests a physiological rather than psychological cause and warrants investigation.
New onset of ED in previously healthy function
If you had excellent erectile function before starting tirzepatide and develop significant ED that does not resolve within 4 to 6 weeks, this is worth investigating even though tirzepatide is unlikely to be the direct cause. The rapid metabolic changes of early treatment can unmask pre-existing conditions or interact with other factors in unexpected ways.
Accompanying symptoms
ED accompanied by extreme fatigue, muscle wasting, depression, or cognitive changes suggests a hormonal problem that may require specific treatment. ED accompanied by chest pain, shortness of breath, or leg pain during exertion suggests cardiovascular disease that needs immediate evaluation. ED accompanied by genital numbness or tingling suggests a neurological issue.
In all of these cases, the appropriate response is medical evaluation rather than discontinuing tirzepatide, which is unlikely to be the cause and is probably helping through its metabolic benefits.
Tirzepatide versus other ED risk factors: putting it in perspective
To understand how minor any potential risk from tirzepatide is compared to other ED risk factors, consider the following comparisons:
Factor | Impact on ED risk | Modifiable? |
|---|---|---|
Obesity (BMI over 30) | 2 to 3 times higher risk | Yes, with weight loss |
Type 2 diabetes | 2 to 3 times higher risk | Partially |
Smoking | 1.5 to 2 times higher risk | Yes |
Sedentary lifestyle | 1.5 to 2 times higher risk | Yes |
Heavy alcohol use | 1.5 to 2 times higher risk | Yes |
Sleep apnea | 1.5 to 2 times higher risk | Yes, with treatment |
SSRI antidepressants | 25% to 73% incidence | Discuss with prescriber |
Beta-blockers | 15% to 25% incidence | Discuss with prescriber |
Tirzepatide | 30% to 45% LOWER risk vs alternatives | Beneficial |
The comparison is stark. Every major risk factor for ED is either caused by or worsened by obesity. Tirzepatide addresses the obesity itself, which addresses the root cause of most weight-related ED. It is like worrying about the fire extinguisher while the house is burning.
If you are overweight and experiencing ED, the most impactful thing you can do for your sexual health is lose weight. Tirzepatide happens to be one of the most effective weight loss interventions ever developed. The math is straightforward.
Combining tirzepatide with other approaches for optimal sexual health
For men who want to maximize the sexual health benefits of tirzepatide treatment, several complementary approaches can enhance outcomes.
PDE-5 inhibitors during the adjustment period
If you experience temporary erectile difficulties during dose escalation, PDE-5 inhibitors (sildenafil, tadalafil) can provide a bridge until the metabolic benefits of tirzepatide begin to manifest. There is no contraindication between tirzepatide and PDE-5 inhibitors. Many men use low-dose daily tadalafil (2.5 to 5 mg) during the first few months of treatment and then taper off as their natural function improves.
Discuss this option with your prescriber. It is a common and well-accepted practice that ensures sexual function is maintained during the transition period without creating dependence on the erectile medication long-term.
Cardiovascular exercise
Regular aerobic exercise improves endothelial function, reduces blood pressure, improves insulin sensitivity, and increases cardiovascular fitness. All of these benefits translate directly to improved erectile function. Aim for 150 minutes per week of moderate-intensity cardio (brisk walking, cycling, swimming) in addition to resistance training.
Exercise also directly improves mood and reduces anxiety, addressing the psychological components of ED. The combination of tirzepatide-driven weight loss and regular exercise produces cardiovascular improvements that exceed what either intervention achieves alone.
Sleep optimization
Poor sleep quality is both a cause and consequence of ED. Testosterone production peaks during deep sleep, and sleep deprivation directly suppresses testosterone levels. If you have sleep apnea, ensure it is being treated. If you have insomnia or poor sleep hygiene, address these issues proactively.
Prioritize 7 to 9 hours of quality sleep nightly. Maintain consistent sleep and wake times. Avoid screens for 1 hour before bed. Keep the bedroom cool (65 to 68 degrees Fahrenheit). Consider magnesium glycinate supplementation, which supports both sleep quality and testosterone production.
Stress management
Chronic psychological stress elevates cortisol, suppresses testosterone, and activates the sympathetic nervous system, all of which impair erectile function. The stress of managing a chronic condition, adjusting to medication side effects, and dealing with body changes can compound existing stressors.
Incorporate stress management techniques that work for you. Options include meditation, deep breathing exercises, time in nature, social connection, therapy, and adequate leisure time. The goal is to shift your autonomic nervous system toward parasympathetic dominance, the state in which sexual arousal and erectile function operate optimally.
Peptides that support sexual health
Some men combine tirzepatide with other peptides that specifically target sexual function. PT-141 (bremelanotide) is a melanocortin receptor agonist that directly increases sexual desire and arousal through central nervous system mechanisms. Unlike PDE-5 inhibitors, which affect blood flow, PT-141 affects the brain pathways involved in sexual motivation.
Other peptides that support complementary goals include kisspeptin, which stimulates the hypothalamic-pituitary-gonadal axis, and various growth hormone secretagogues that support body composition and recovery. Any combination protocol should be discussed with a knowledgeable healthcare provider to ensure safety and appropriate dosing.
The female partner perspective: tirzepatide and female sexual function
While this guide focuses on erectile dysfunction in men, it is worth briefly addressing the evidence on tirzepatide and female sexual function, as some partners may be taking the medication simultaneously.
A case report published in 2025 described a 36-year-old woman who developed sexual dysfunction while on tirzepatide. Her symptoms significantly improved when she stopped the medication and returned when she restarted it. This is currently the most notable published report of tirzepatide-induced sexual dysfunction in women.
However, one case report does not establish a pattern. Many women report improved sexual function on GLP-1 medications due to weight loss, improved body image, and hormonal changes. The relationship between tirzepatide and female sexual health requires significantly more research before conclusions can be drawn.
If a female partner experiences sexual dysfunction on tirzepatide, she should discuss it with her prescriber. As with men, the cause may be multifactorial and the medication may not be the primary driver.
Common myths about tirzepatide and erectile dysfunction
Several misconceptions circulate online about GLP-1 medications and sexual health. Addressing these directly helps separate fact from fiction.
Myth: GLP-1 medications destroy testosterone
This is the opposite of what the research shows. GLP-1 medications, including tirzepatide, are associated with increased testosterone in overweight men. The confusion likely stems from temporary libido reduction during dose escalation being misattributed to hormonal damage. In reality, testosterone levels typically rise steadily as weight decreases on tirzepatide treatment.
Myth: weight loss always causes ED
While extreme caloric restriction can temporarily suppress testosterone, moderate sustained weight loss consistently improves erectile function. The JAMA study showing 30% ED resolution with an average 33-pound weight loss is one of many demonstrating this benefit. The key is adequate nutrition (especially protein) during the weight loss process.
Myth: if you get ED on tirzepatide, you should stop immediately
Stopping tirzepatide to address ED is almost always the wrong approach. The weight regain that follows discontinuation will likely worsen the very metabolic conditions driving ED. A better strategy is to address the ED specifically (PDE-5 inhibitors, hormone testing, nutritional optimization) while continuing the medication that is improving overall metabolic health.
Myth: peptides and PDE-5 inhibitors cannot be combined
There is no pharmacological interaction between tirzepatide and PDE-5 inhibitors like sildenafil or tadalafil. These medications work through entirely different mechanisms and can be safely used together under medical supervision. Many clinicians routinely prescribe both for men managing weight loss and erectile function simultaneously.
Myth: younger men do not need to worry about ED on weight loss drugs
While younger men are less likely to have established vascular ED, the metabolic effects of obesity affect men of all ages. Young obese men frequently have suppressed testosterone, impaired insulin sensitivity, and subclinical endothelial dysfunction that affects erectile quality. Tirzepatide benefits men across age groups by addressing these underlying factors.
Practical protocol: maximizing sexual health on tirzepatide
Based on the clinical evidence and real-world experiences, here is a practical protocol for men who want to protect and improve their sexual health while using tirzepatide.
Before starting tirzepatide
Baseline labs: Total testosterone, free testosterone, estradiol, SHBG, LH, FSH, complete metabolic panel, lipid panel, HbA1c, vitamin D, zinc, B12.
Baseline function assessment: Honestly evaluate your current erectile function using the IIEF-5 questionnaire (International Index of Erectile Function). This gives you an objective score to compare against as treatment progresses.
Nutrition plan: Establish a high-protein eating strategy before starting. Have protein-rich foods and supplements ready for when appetite suppression kicks in. Identify your protein sources and calculate daily targets.
Exercise baseline: Start a resistance training program before beginning tirzepatide if you are not already training. Establish the habit and routine before adding the challenge of reduced appetite and potential fatigue.
First 4 weeks on tirzepatide
Expect: Reduced appetite, possible nausea, possible fatigue, possible temporary libido decrease.
Action: Focus on protein intake (minimum 0.8 g/lb goal body weight). Continue resistance training. Do not increase dose faster than your prescriber recommends. Stay hydrated. Take a quality multivitamin plus zinc, vitamin D, and magnesium.
Sexual health strategy: If libido dips, do not panic. If erectile function is needed, discuss low-dose tadalafil (2.5 to 5 mg daily) with your prescriber as a temporary bridge. Maintain intimacy and communication with your partner.
Weeks 4 through 12
Expect: Side effects stabilizing, weight loss becoming visible, energy beginning to improve, possible improvement in sexual function.
Action: Continue dose escalation per prescriber guidance. Maintain high protein intake. Increase exercise intensity gradually if tolerated. Follow the dosing schedule consistently.
Sexual health strategy: Most men notice improvement in this window. If function has not returned to baseline by week 12, request hormone testing. Compare results to your baseline labs.
Months 3 through 6
Expect: Significant weight loss (15 to 30+ pounds), improved metabolic markers, hormone levels trending positive, sexual function at or above baseline.
Action: Follow-up labs at 3 months. Adjust supplementation based on results. Continue resistance training. Consider reducing or discontinuing PDE-5 inhibitor if used temporarily.
Sexual health strategy: If testosterone has risen and erectile function has improved, you are on the right trajectory. If testosterone remains suppressed despite weight loss, discuss further evaluation with an endocrinologist. Consider checking for specialized peptide therapy options if additional support is desired.
Month 6 and beyond
Expect: Stable weight loss, normalized or improved metabolic markers, sustained improvement in sexual health for most men.
Action: Annual comprehensive labs. Maintain exercise and nutrition habits. Discuss long-term medication strategy with prescriber.
Sexual health strategy: Most men at this point have better sexual function than before starting tirzepatide. Continue monitoring and maintaining the lifestyle factors that support hormonal and vascular health. Long-term maintenance of weight loss is critical for sustaining the sexual health benefits.
Tirzepatide and fertility considerations
For men concerned about fertility in addition to erectile function, tirzepatide offers important advantages over other interventions. Unlike testosterone replacement therapy, which suppresses sperm production by shutting down the hypothalamic-pituitary-gonadal axis, tirzepatide actually enhances natural hormonal function.
The 2025 pilot study showed tirzepatide increased LH and FSH levels, the exact hormones that drive sperm production. This means that rather than impairing fertility, tirzepatide may improve it in obese men whose reproductive function is compromised by excess weight.
For men planning to conceive, tirzepatide may be a superior choice for weight management compared to testosterone therapy, anabolic steroids, or other interventions that suppress the HPG axis. However, the long-term effects of tirzepatide on sperm quality and fertility outcomes have not been studied in randomized trials, so discuss this with a reproductive specialist if fertility is a priority.
Some men on tirzepatide use enclomiphene concurrently to further support natural testosterone and gonadotropin production. This combination addresses both weight and hormonal optimization without compromising fertility, though it should be managed by a knowledgeable clinician.
Frequently asked questions
Does tirzepatide directly cause erectile dysfunction?
No. The current clinical evidence does not support a direct causal link between tirzepatide and erectile dysfunction. A 2025 retrospective cohort study found that tirzepatide was associated with a 30% to 45% lower risk of ED compared to sitagliptin, injectable semaglutide, and dulaglutide. The weight loss and metabolic improvements produced by tirzepatide generally improve the conditions necessary for healthy erectile function.
Why did my libido decrease after starting tirzepatide?
Temporary libido reduction during the first 2 to 6 weeks is common and typically results from gastrointestinal side effects (nausea, reduced appetite), significant caloric restriction, and metabolic adaptation. This is not erectile dysfunction but rather reduced desire caused by the body adjusting to the medication. Most men find that libido returns and often improves as side effects resolve and weight loss progresses.
Will tirzepatide increase my testosterone?
Most likely, yes, if you are overweight. The 2025 pilot study showed tirzepatide increased total testosterone, free testosterone, and bioavailable testosterone in obese men with metabolic hypogonadism, outperforming both lifestyle changes alone and testosterone replacement therapy. The primary mechanism is reduced aromatase activity from fat loss, which allows natural testosterone production to recover.
Can I take Viagra or Cialis with tirzepatide?
Yes. There is no pharmacological interaction between tirzepatide and PDE-5 inhibitors like sildenafil (Viagra) or tadalafil (Cialis). Many prescribers recommend low-dose daily tadalafil during the dose escalation period as a temporary bridge for men who experience reduced function. The medications work through entirely different mechanisms and can be safely combined under medical supervision.
Should I stop tirzepatide if I develop ED?
In almost all cases, no. Stopping tirzepatide will lead to weight regain, which will worsen the metabolic conditions that drive ED. A better approach is to address the ED specifically, through hormone testing, nutritional optimization, PDE-5 inhibitors, or other targeted interventions, while continuing the medication that is improving your overall metabolic health. Discuss any concerns with your healthcare provider before making changes.
How long until sexual function improves on tirzepatide?
Most men notice improvement in sexual function between weeks 6 and 12 of treatment, as gastrointestinal side effects resolve and the metabolic benefits of weight loss begin to manifest. Some men notice earlier improvement, while others require 3 to 6 months of sustained weight loss before significant changes become apparent. The trajectory typically mirrors the degree of weight loss achieved.
Is tirzepatide better than semaglutide for sexual health?
The limited comparative data suggests yes. The 2025 cohort study found tirzepatide had a lower ED risk ratio than injectable semaglutide (0.67, meaning 33% lower risk). The dual GLP-1/GIP mechanism of tirzepatide may produce more favorable hormonal effects than pure GLP-1 agonists. However, larger comparative studies are needed to confirm this difference.
Does tirzepatide affect female sexual function?
Evidence is very limited. One case report documented sexual dysfunction in a woman on tirzepatide that resolved upon discontinuation. However, many women report improved sexual function due to weight loss, better body image, and hormonal changes. The topic requires significantly more research before definitive conclusions can be drawn.
External resources
The Impact of GLP-1 Receptor Agonists on Erectile Function: Friend or Foe? - PMC
Association of tirzepatide with erectile dysfunction in people with type 2 diabetes - PubMed
Short-term impact of tirzepatide on metabolic hypogonadism and body composition - PMC
Obesity and Erectile Dysfunction: From Bench to Clinical Implication - PMC
Effect of Lifestyle Changes on Erectile Dysfunction in Obese Men - JAMA
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your testosterone stay optimal, your protocols stay effective, and your confidence stay unshakeable.