Feb 28, 2026

Some people stop semaglutide overnight and feel fine for weeks. Others watch their appetite roar back within days, their weight climb within months, and their blood sugar spiral if they have type 2 diabetes. Same medication. Completely different outcomes. The difference is not luck. It is not genetics, not willpower, not some mysterious metabolic advantage. It comes down to how you stop, when you stop, and what you do in the weeks that follow.
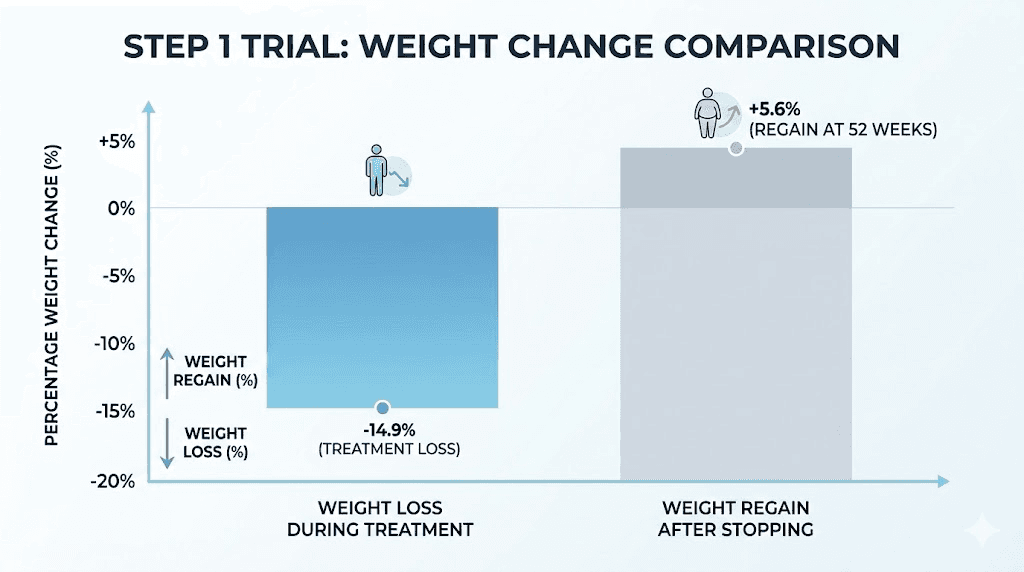
The short answer to the question everyone asks is yes, you can stop semaglutide cold turkey. The medication is not addictive. It does not create chemical dependency. There is no dangerous withdrawal syndrome waiting on the other side. But safe and smart are two very different things. The STEP 1 trial extension study showed that participants who stopped semaglutide regained two-thirds of their lost weight within a single year. Two-thirds. That is not a minor setback. That is most of your progress, gone. And it did not have to happen that way.
This guide covers everything you need to know about stopping semaglutide abruptly. The hour-by-hour and week-by-week timeline of what changes in your body. The actual clinical data on weight regain and cardiometabolic rebound. Three proven tapering protocols that protect your results. Strategies for maintaining your nutrition, your exercise habits, and your metabolic health long after your last injection. Whether you are stopping by choice, because of side effects, or because your prescription ran out, the information here will help you make the transition without losing what you have built.
What happens when you stop semaglutide cold turkey
Understanding what happens inside your body after your last dose is the single most important thing you can do before quitting. Not because the changes are dangerous, but because knowing the timeline removes the panic. When your appetite surges at day ten, you will know it is the medication clearing your system, not some personal failing. When your weight ticks up at week six, you will know it matches the clinical data exactly. Knowledge turns surprises into expected events. And expected events are manageable events.
The first 48 hours
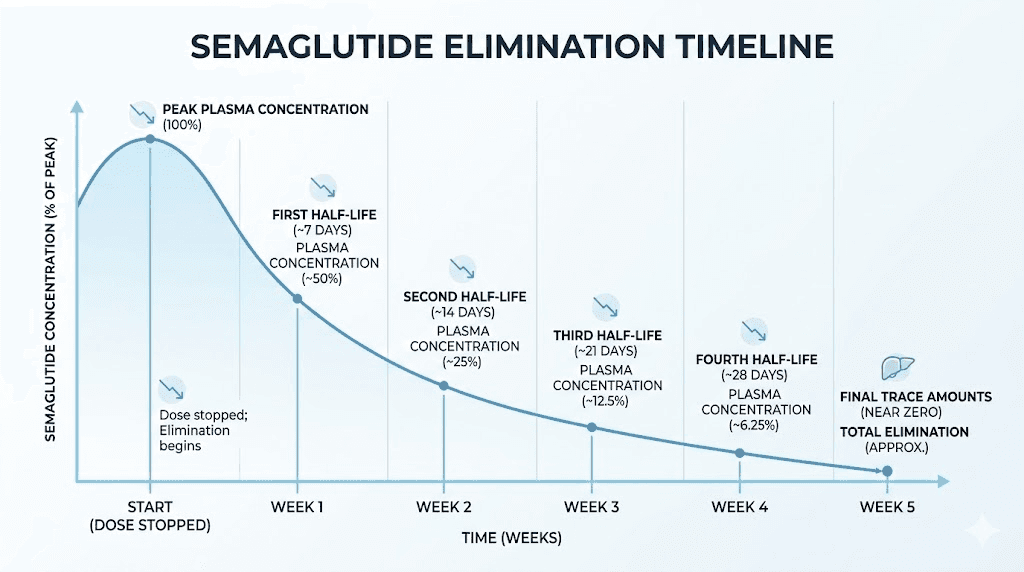
Nothing dramatic happens in the first two days after your last injection. Semaglutide has a half-life of approximately seven days, which means the medication is still working at near-full capacity during this window. Your appetite stays suppressed. Your gastric emptying stays slowed. Your blood sugar regulation, if you have diabetes, remains supported. Most people notice absolutely nothing different during this period.
This is both reassuring and deceptive.
Reassuring because there is no abrupt cliff. Deceptive because it creates false confidence. Some people interpret these first quiet days as evidence that stopping will be easy, that their body has somehow learned new habits that will persist without pharmacological support. The research does not support that interpretation. The medication is simply still present in your bloodstream, doing what it has been doing all along. The real changes begin when drug levels start to meaningfully decline.
Week one changes
By the end of the first week, your body has eliminated roughly half of the remaining semaglutide. If your last dose was the standard 2.4 mg for weight management, you now have approximately 1.2 mg still circulating. That is enough to maintain partial appetite suppression and some degree of gastric slowing, but the effects are noticeably weaker.
Most people describe the first week as subtle. A slight increase in food thoughts. Meals that previously felt satisfying now leave a hint of wanting more. The portion sizes that felt natural on the medication start feeling smaller. These shifts are real, physiological, and completely expected. Your GLP-1 receptors are receiving less stimulation. Your hypothalamus is recalibrating hunger signals. Your gut is beginning to speed up its emptying process.
For people using semaglutide to manage type 2 diabetes, the first week may also bring mild fasting blood glucose increases. Studies show readings can climb 20 to 30 mg/dL in the initial two weeks after stopping. This is not a crisis, but it does require monitoring, especially if you take other diabetes medications that may need adjustment.
Weeks two through four
This is when the real transition happens. By week two, semaglutide levels have dropped to roughly 25% of your last therapeutic dose. By week three, you are at about 12%. By week four, the medication is functionally gone from your system, with only trace amounts remaining.
The appetite return is the most noticeable change. Most patients report significant hunger increases between days 7 and 14 after their final dose. This is not psychological. The medication was directly suppressing hunger signals in your brain, slowing stomach emptying to keep you feeling full longer, and modulating reward pathways that influence food cravings. All of those mechanisms are now fading.
Gastric emptying speeds back up during this window. If you experienced constipation on semaglutide, you may notice it resolving. If you dealt with bloating, that typically improves too. Some people experience temporary digestive irregularity as their system readjusts to processing food at normal speed. Loose stools, mild cramping, or intermittent nausea can occur but usually resolve within one to two weeks.
The fatigue some people experienced while on semaglutide often lifts during this period. Energy levels frequently improve. For some, this feels like a genuine positive of stopping. For others, the increased energy comes packaged with increased appetite, creating a frustrating combination of feeling better physically while struggling more with food.
Month two and beyond
By month two, semaglutide has been completely cleared from your body for at least two to three weeks. Your systems are now operating entirely on their own biology. Appetite has fully returned to pre-medication baseline for most people. Gastric emptying has normalized. Blood sugar regulation is dependent entirely on your own insulin production and any other medications you take.
This is where the weight regain data becomes relevant. The STEP 1 trial extension tracked participants for a full year after discontinuation and found an average regain of 11.6 percentage points of body weight. If someone lost 17% of their body weight on semaglutide, they regained roughly two-thirds of that loss, ending up with a net loss of about 5.6% from their original starting weight. That pattern held remarkably consistent across the study population.
But here is the critical nuance. That study involved abrupt discontinuation with no structured maintenance plan. No tapering. No specific dietary protocol. No targeted exercise program. Real-world data from clinical practices, where patients often implement maintenance strategies, shows more variable outcomes. Some people maintain most of their loss. Others regain more than the trial averages. The determining factor is almost always what the person does after stopping, not whether they stopped.
Is it safe to stop semaglutide suddenly
Let us separate two questions that often get confused. Is it medically safe to stop semaglutide cold turkey? Yes, for most people. Is it the best approach for preserving your results? Almost never. Safety and optimization are different conversations, and understanding both matters.
For weight loss patients
If you are taking semaglutide exclusively for weight management and do not have type 2 diabetes, stopping cold turkey is medically safe. The medication does not create physical dependency. There is no withdrawal syndrome comparable to opioids, benzodiazepines, or even caffeine. Your body will not go into crisis. No emergency room visit will be needed.
What you will experience is the gradual return of the symptoms that led you to semaglutide in the first place. Increased appetite. Stronger food cravings. Faster gastric emptying that makes meals less satisfying. These are not withdrawal symptoms in the medical sense. They are the reemergence of your baseline physiology once the medication is no longer masking it.
The appetite suppression that semaglutide provided was pharmacological, not behavioral. When the pharmacology stops, the suppression stops. This is an important distinction because it sets realistic expectations. You are not failing if your appetite returns. Your biology is simply reasserting itself.
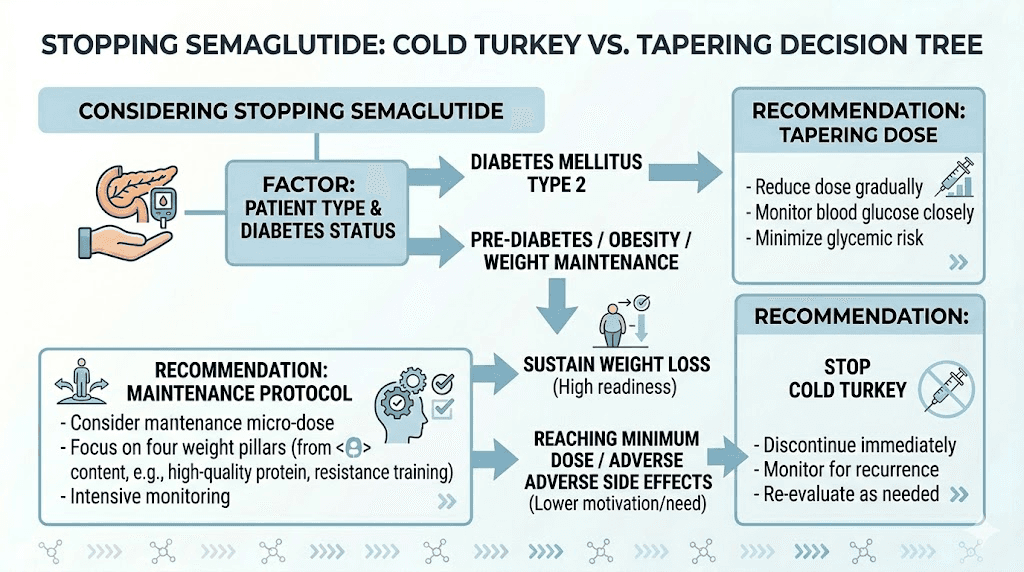
For type 2 diabetes patients
The safety calculus changes significantly for people using semaglutide to manage type 2 diabetes. Abrupt discontinuation can cause meaningful blood glucose elevations. Fasting readings may increase by 20 to 30 mg/dL in the first two weeks, with continued deterioration over the following months. HbA1c levels that improved on semaglutide will gradually drift upward toward pre-treatment values.
This does not mean cold turkey stopping is impossible for diabetes patients. It means it requires medical coordination. Your healthcare provider may need to adjust other diabetes medications, increase insulin doses, or add a different GLP-1 receptor agonist to fill the gap. The key word is coordination. Stopping semaglutide without telling your doctor and without monitoring your blood sugar is the scenario that creates real risk.
Dangerous blood sugar spikes are most likely in patients who rely heavily on semaglutide as their primary glucose-lowering medication. If you take semaglutide alongside metformin, insulin, or other diabetes drugs, the transition is typically smoother because those other medications continue working. If semaglutide is your only glucose-lowering therapy, stopping abruptly requires immediate medical oversight.
When cold turkey stopping is dangerous
There are specific situations where stopping semaglutide without medical guidance crosses from suboptimal into genuinely risky.
Uncontrolled type 2 diabetes with semaglutide as primary therapy. If your HbA1c was above 9% before starting and semaglutide brought it down to target range, abrupt removal can cause rapid glycemic deterioration that may require emergency intervention.
Active kidney disease complicated by diabetes. Blood sugar spikes after stopping semaglutide can accelerate kidney damage in patients with existing renal complications.
Pregnancy planning. If you become pregnant while semaglutide is still in your system, there are potential risks to fetal development. Semaglutide should be stopped at least two months before planned conception. But this should be a planned, medically supervised transition, not an abrupt stop.
Post-surgical patients. If you recently had surgery and are scheduled to resume semaglutide after surgery, the timing and method of stopping and restarting should be coordinated with your surgical team.
The science of semaglutide elimination
Understanding the pharmacokinetics of semaglutide removal helps explain why the transition off the medication follows such a predictable pattern. This is not about memorizing numbers. It is about understanding why your body responds the way it does, so you can plan accordingly.
Half-life and clearance timeline
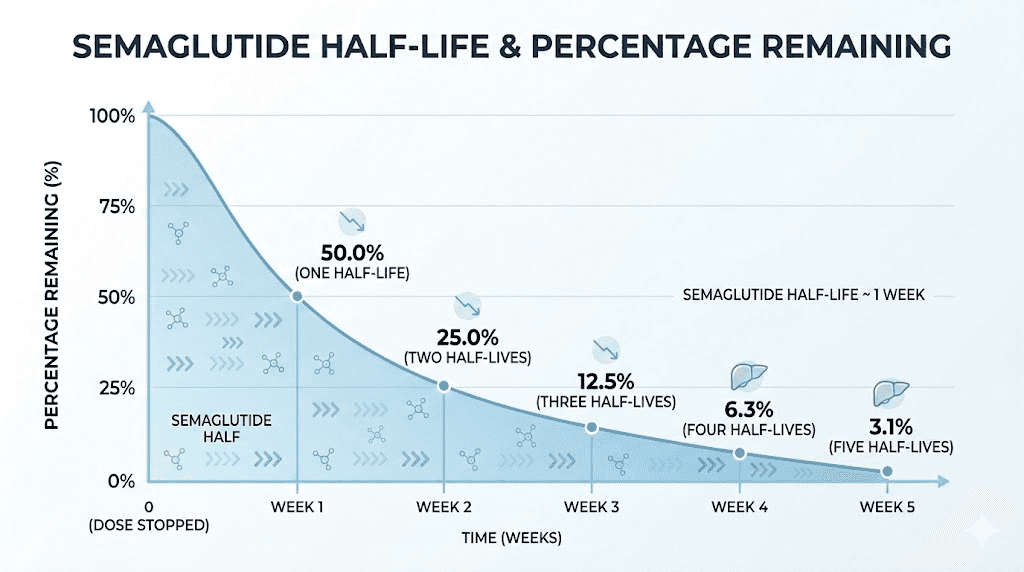
Semaglutide has a terminal elimination half-life of approximately seven days, or 168 hours. This means that every seven days after your last injection, the amount of active semaglutide in your bloodstream drops by roughly half. The math is straightforward.
After one week, 50% remains. After two weeks, 25%. After three weeks, 12.5%. After four weeks, about 6%. After five weeks, approximately 3%, which is considered functionally eliminated. The medication is gone. Your body is on its own.
This five-week clearance window is why some people feel fine for the first week or two after stopping and then notice changes accelerating. The decline is exponential, not linear. You lose the same fraction each week, but the absolute amount decreases faster as levels get lower. The difference between 100% and 50% is barely noticeable for most people. The difference between 25% and 12.5% is where the appetite return becomes real. And the drop from 12.5% to functional zero is when the full force of your pre-medication biology reasserts itself.
There is no way to speed up this elimination process. Semaglutide is metabolized through standard protein degradation pathways and excreted via urine and feces. Exercise, hydration, saunas, and supplements do not meaningfully accelerate clearance. The seven-day half-life is the seven-day half-life.
How your body readjusts
The readjustment process involves multiple systems recalibrating simultaneously. Your hypothalamus, the brain region that regulates hunger, has been receiving amplified GLP-1 signals for months or years. When those signals diminish, it takes time for new equilibrium to establish. Some researchers describe this as a neurological readjustment period that can take 8 to 12 weeks to fully stabilize.
Your digestive system readjusts faster. Gastric emptying rate typically normalizes within two to three weeks of stopping. This is why digestive symptoms tend to resolve more quickly than appetite and weight changes. The mechanical aspects of digestion recover before the neurological aspects of hunger regulation.
Metabolic rate changes are more complex. Weight loss on semaglutide, like all weight loss, comes with some degree of metabolic adaptation. Your body burns fewer calories at the lower weight than it did at the higher weight. This metabolic adaptation does not fully reverse when you stop semaglutide, which creates an asymmetric challenge. Your appetite returns to pre-medication levels, but your metabolic rate stays adapted to the lower weight, creating a gap between what your body wants to eat and what it actually needs.
Why appetite returns at different speeds
Not everyone experiences appetite return on the same timeline, and the reasons are both biological and behavioral.
Duration of treatment matters. People who took semaglutide for longer periods sometimes report a more gradual appetite return compared to those who stopped after just a few months. The theory is that longer treatment allows more behavioral adaptation, things like smaller portion preferences, reduced snacking, and changed food reward responses, that partially persist even after the medication clears.
Dose at discontinuation also plays a role. Someone stopping from 2.4 mg has more medication to clear than someone who had already tapered to 1.0 mg. The higher the final dose, the longer the clearance period, and the more dramatic the transition can feel when levels finally drop below the therapeutic threshold.
Individual variation in GLP-1 receptor sensitivity means some people feel changes earlier than others. Genetics, gut microbiome composition, and baseline metabolic health all influence how quickly your brain registers the loss of exogenous GLP-1 stimulation. There is no way to predict exactly when a specific individual will notice the shift, but the two-week mark is the most commonly reported turning point.
Weight regain after stopping semaglutide: what the research shows
The weight regain conversation deserves more nuance than it usually gets. Headlines scream that people gain everything back. Online forums insist that semaglutide is pointless if you cannot take it forever. Neither extreme reflects the full picture. The data tells a more complicated and more hopeful story than either side suggests.
STEP 1 trial extension data
The STEP 1 trial remains the most cited study on semaglutide discontinuation outcomes. Here is what actually happened.
During the 68-week treatment phase, participants on semaglutide 2.4 mg lost an average of 17.3% of their body weight. That is substantial. For a 220-pound person, that represents roughly 38 pounds of weight loss.
After treatment was discontinued at week 68, all lifestyle intervention also stopped. This is a critical detail that often gets overlooked. Participants were not just taken off the medication. They were also removed from the structured support system. No more counseling. No more dietary guidance. No more regular check-ins. Everything stopped simultaneously.
By week 120, one year after discontinuation, participants had regained an average of 11.6 percentage points. Their net weight loss from baseline was 5.6%. For our 220-pound example, that means they went from losing 38 pounds to keeping about 12 pounds off.
The cardiometabolic improvements followed a similar pattern. Improvements in blood pressure, waist circumference, lipid profiles, and C-reactive protein levels achieved during treatment largely reverted toward baseline after stopping. However, they did not fully return to pre-treatment levels in all cases, suggesting some lasting benefit even after regain.
Real-world data vs clinical trials
Clinical trials create artificial conditions that do not reflect how people actually manage their medication transitions. In the STEP 1 extension, everything stopped at once, medication and lifestyle support, with no tapering, no maintenance plan, and no ongoing care. In real clinical practice, the situation is very different.
Real-world data from Epic Research, analyzing outcomes for patients who stopped semaglutide or liraglutide in standard clinical settings, found more encouraging results. More than half of patients maintained their weight loss at one year. The key difference was that real-world patients often continued pursuing weight management through other means, including switching to alternative medications, working with dietitians, maintaining exercise programs, or implementing structured maintenance protocols.
A weight regain meta-analysis published in eClinicalMedicine found that the average weight regained after stopping semaglutide was 5.63 kg with a 5.81% body weight increase. This is significant but less catastrophic than the headlines suggest, particularly when combined with active maintenance strategies.
The takeaway is not that regain is unavoidable. It is that unmanaged discontinuation produces the worst outcomes, and managed transitions produce substantially better ones.
Why some people regain more than others
Several factors predict who regains more and who maintains more of their loss.
Amount of weight lost during treatment. People who lost more on semaglutide tend to regain a larger absolute amount but maintain a higher percentage of their total loss. Losing 40 pounds and regaining 25 still leaves you 15 pounds lighter. Losing 15 pounds and regaining 12 leaves you only 3 pounds lighter. The math favors those who responded most strongly to treatment.
Duration of treatment before stopping. Longer treatment periods allow more time for behavioral adaptation and metabolic adjustment. People who used semaglutide for 12 or more months before stopping tend to maintain more than those who stopped after just a few months.
Exercise habits established during treatment. Research consistently shows that people who established regular resistance training during their semaglutide treatment maintained more lean mass and regained less fat after stopping. The muscle preserved during weight loss acts as a metabolic buffer against regain.
Having a structured maintenance plan. People who transitioned from semaglutide to a specific dietary and exercise protocol maintained dramatically more of their loss than those who simply stopped and hoped for the best.
Psychological readiness. Those who stopped by choice, on their own timeline, with realistic expectations, fared better than those who stopped abruptly due to insurance changes, supply shortages, or financial constraints. Planned transitions outperform forced ones every time.
Cold turkey vs tapering: which approach works better
The debate between abrupt discontinuation and gradual tapering is not just academic. It has practical implications for your weight, your comfort during the transition, and your long-term outcomes. Both approaches have legitimate proponents, and the evidence favors tapering for most people, though not all.
The case for stopping abruptly
There are situations where cold turkey makes sense.
Severe side effects. If you are experiencing serious adverse reactions like persistent vomiting, significant sleep disruption, or concerning laboratory changes, your doctor may recommend immediate discontinuation rather than prolonging exposure.
Planned pregnancy. Since semaglutide should be cleared from the body at least two months before conception, some providers prefer a clean stop rather than an extended taper that delays the clearance window.
Simplicity. Some patients and providers prefer the straightforward approach. You stop. You manage the transition. You move on. No complicated dose adjustments, no drawn-out process, no pharmacy coordination for smaller doses.
Cost. If you are paying out of pocket and can no longer afford the medication, continuing at reduced doses may not be financially viable. A clean stop may be the only realistic option.
The case for gradual tapering
The evidence favoring tapering is growing. A study highlighted by Medscape found that individuals who gradually reduced their semaglutide dose to zero over approximately nine weeks while receiving coaching on exercise and diet maintained their weight loss. Some actually lost an additional 1.5% of body weight during the taper period. The gradual reduction allowed their behavioral adaptations to solidify while the medication slowly withdrew its support.
Tapering offers several advantages over cold turkey. The appetite return is more gradual, giving you time to adjust your eating patterns consciously rather than reactively. Blood sugar changes are more modest, reducing the risk of glycemic complications in diabetes patients. The psychological transition is gentler, as you are not going from full support to zero support overnight.
For people who are anxious about stopping, tapering also provides a sense of control. Each dose reduction is a step you can evaluate. If a particular reduction feels too aggressive, you can hold at that dose longer before reducing again. This flexibility simply does not exist with cold turkey.
Three tapering protocols that work
While there is no officially established tapering protocol for semaglutide, clinical experience has produced three approaches that healthcare providers commonly use.
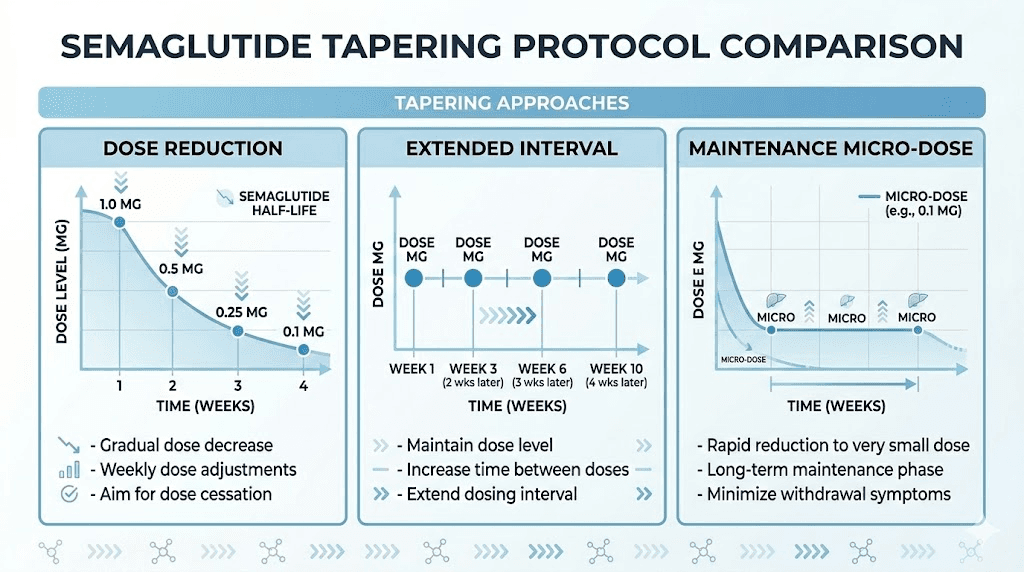
Dose reduction taper. This involves stepping down through the standard dose tiers in reverse. From 2.4 mg to 1.7 mg for two to four weeks, then to 1.0 mg for two to four weeks, then to 0.5 mg for two to four weeks, then to 0.25 mg for two to four weeks before stopping completely. Total taper duration is 8 to 16 weeks depending on how long you hold each step.
Extended interval taper. Instead of reducing the dose, you extend the time between injections. Move from weekly to every 10 days for two to three doses, then every two weeks for two to three doses, then every three weeks for one to two doses, then stop. This approach gradually reduces your average daily exposure while maintaining some peak drug levels.
Maintenance micro-dose. Some clinicians use a very small maintenance dose, typically 0.25 mg, administered every two weeks for an extended period. This is enough to provide mild ongoing GLP-1 stimulation at a fraction of the therapeutic cost, while you solidify behavioral changes and exercise habits. This is not technically tapering to zero but rather transitioning to long-term low-dose maintenance.
How to taper off semaglutide safely
If you have decided that tapering is the right approach, and for most people it is, here is how to execute each protocol safely. These are general frameworks. Your healthcare provider should customize any tapering plan to your specific situation, medical history, and treatment goals.
Protocol 1: dose reduction taper
This is the most commonly recommended approach and the one most pharmacies can easily accommodate since it uses standard dose formulations.
Starting from 2.4 mg weekly:
Weeks 1 to 3: reduce to 1.7 mg weekly
Weeks 4 to 6: reduce to 1.0 mg weekly
Weeks 7 to 9: reduce to 0.5 mg weekly
Weeks 10 to 12: reduce to 0.25 mg weekly
Week 13: discontinue
At each step, monitor your appetite, weight, and energy levels. If any reduction feels particularly challenging, hold at that dose for an extra one to two weeks before stepping down again. The goal is not speed. It is a smooth transition that allows your biology and behavior to stay aligned.
If you are using compounded semaglutide, your prescriber can dial in custom doses between the standard tiers, which may allow for even smoother transitions. Compounded formulations offer flexibility that brand-name pens do not.
Protocol 2: extended interval taper
This approach works well for people who want to maintain their current dose strength but reduce frequency. It is simpler in some ways because you keep injecting the same amount, just less often.
Starting from any stable weekly dose:
Weeks 1 to 3: inject every 10 days instead of every 7
Weeks 4 to 6: inject every 14 days
Weeks 7 to 9: inject every 21 days
Week 10: final injection
Week 13 onward: fully discontinued
The advantage of this method is that each injection still provides the familiar peak of medication activity you are used to. The troughs between injections get longer, which gives your body increasingly longer windows of minimal GLP-1 support. Many people find this approach feels more natural than reducing doses, because the individual injection experiences remain consistent.
The drawback is that the extended intervals create more pronounced cycles of appetite suppression and appetite return. You may notice hunger increasing toward the end of each extended interval. Planning higher-protein, higher-fiber meals around these periods can help bridge the gap. Reviewing your nutrition strategy before starting this protocol is essential.
Protocol 3: maintenance micro-dose
This protocol is less about tapering and more about transitioning from therapeutic dosing to maintenance dosing. It is best suited for people who want to keep some pharmaceutical support while they build sustainable habits.
Transition schedule:
Weeks 1 to 4: reduce from therapeutic dose to 0.25 mg weekly
Weeks 5 to 12: 0.25 mg every two weeks
Weeks 13 to 24: reassess, continue micro-dosing or discontinue based on results
At 0.25 mg every two weeks, you are receiving roughly one-twentieth of the standard therapeutic exposure. This is enough to provide mild GLP-1 receptor stimulation, which may help blunt the most aggressive appetite return, without the full side effect profile or cost of therapeutic dosing. Some clinicians use this as a long-term bridge for patients who are not ready for complete discontinuation but cannot or do not want to continue full-dose treatment.
The evidence for micro-dosing is limited to clinical observation rather than randomized trials, but the theoretical basis is sound. Even small amounts of GLP-1 receptor stimulation can influence satiety signaling, and the dose is low enough that side effects are minimal. Discuss this option with your prescriber to determine if it fits your situation.
Which protocol fits your situation
Choosing between these three protocols depends on several factors.
If you have type 2 diabetes, the dose reduction taper is generally preferred because it provides the most predictable and gradual glycemic transition. Extended intervals create blood sugar fluctuations that complicate diabetes management.
If you are stopping due to side effects, a faster taper or even cold turkey may be appropriate. There is no benefit in prolonging exposure to a medication that is causing you harm.
If you are stopping by choice and want to maximize result preservation, the maintenance micro-dose approach offers the gentlest transition. It gives you months of partial support while you solidify the lifestyle changes that will maintain your results independently.
If cost is the primary driver, cold turkey or a brief dose reduction taper of four to six weeks may be the most realistic option. A shorter taper still provides meaningful benefit over abrupt discontinuation.
Maintaining your results after semaglutide
Stopping semaglutide without a maintenance plan is like building a house and removing the foundation before the cement dries. The structure might hold temporarily, but it is vulnerable to the first strong wind. Your maintenance plan is the new foundation. And it needs to be in place before you stop, not after.
Maintenance after GLP-1 medications follows similar principles regardless of which specific medication you were taking. The core challenge is the same. Your appetite returns. Your metabolism has adapted to a lower weight. The caloric gap between what your body wants and what it needs is real and persistent. Closing that gap requires deliberate, sustained effort across several domains.
The protein and fiber foundation
If you implement only one nutritional change before stopping semaglutide, make it this one. Increase your protein intake to 1.0 to 1.2 grams per kilogram of body weight per day, and ensure you are consuming 25 to 35 grams of fiber daily. These two macronutrients are the most powerful dietary tools for managing appetite without pharmaceutical support.
Protein promotes satiety through multiple mechanisms. It triggers cholecystokinin release, delays gastric emptying naturally, and requires more energy to digest than carbohydrates or fats. A high-protein meal can reduce subsequent caloric intake by 10 to 15% compared to an isocaloric high-carbohydrate meal.
Fiber works through volume. It adds bulk to meals without adding significant calories, physically expanding the stomach and triggering stretch receptors that signal fullness. Soluble fiber also forms a gel in the gut that slows nutrient absorption, creating a more sustained satiety signal. Together, protein and fiber recreate some of what semaglutide was doing pharmacologically, just through food rather than injection.
Building your meal plan around these priorities before you stop semaglutide gives your body time to adapt to the new eating pattern while still having pharmaceutical support. Start increasing protein and fiber at least four to six weeks before your planned discontinuation date.
Resistance training as your metabolic anchor
Weight loss on semaglutide includes some loss of lean body mass. This is true for all weight loss, not just medication-assisted weight loss. But the lean mass loss means your resting metabolic rate has decreased beyond what weight loss alone would predict. Resistance training is the single most effective intervention for counteracting this metabolic decline.
The recommendation is straightforward. Two to four sessions per week of progressive resistance training, focusing on compound movements that recruit large muscle groups. Squats, deadlifts, rows, presses, and their variations. The goal is not bodybuilding. The goal is preserving and rebuilding the metabolically active tissue that keeps your calorie burn higher.
Studies show that at least 150 minutes of moderate-intensity physical activity per week can help sustain weight loss maintenance. But the type of activity matters. Cardiovascular exercise is valuable for heart health and caloric expenditure, but resistance training specifically protects against the metabolic adaptation that drives regain. Ideally, your program includes both, with a minimum of two dedicated strength sessions per week.
Start this before you stop semaglutide, not after. Building the exercise habit while you still have appetite suppression supporting your recovery and energy balance is significantly easier than starting from scratch when your appetite has returned in full force.
Behavioral strategies that prevent regain
The behavioral component of maintenance is often underestimated. Semaglutide does not just reduce appetite. It changes your relationship with food. Meals become less urgent. Cravings become less compelling. The constant background noise of food thoughts quiets down. When the medication stops, all of that noise returns.
Four behavioral strategies have the strongest evidence for preventing regain.
Food journaling. Tracking what you eat, even loosely, creates awareness that substitutes for the automatic appetite reduction semaglutide provided. You do not need to count every calorie. Even a simple daily food log increases dietary awareness enough to prevent the unconscious overconsumption that drives most regain.
Meal planning and preparation. Having planned meals eliminates the decision fatigue that leads to impulsive eating when appetite returns. If your meals are already prepared and portioned, the returning hunger drives you toward the planned food rather than toward whatever is most convenient and most caloric.
Mindful eating practices. When you stop semaglutide, you need to replace its automatic appetite control with conscious appetite management. Eating slowly. Putting your fork down between bites. Checking in with fullness cues during meals rather than after. These practices are not gimmicks. They are practical tools for recognizing satiety without pharmaceutical amplification of those signals.
Regular weigh-ins. Weekly self-weighing is consistently associated with better weight maintenance outcomes. It provides early warning of regain trends, allowing you to adjust behavior before small gains become large ones. The key is treating the number as data, not judgment. A two-pound increase is a signal to tighten up, not a reason for self-criticism.
When to consider restarting
There is no shame in restarting semaglutide if you find that maintenance without it is not sustainable. Obesity is a chronic medical condition, and chronic conditions often require ongoing treatment. You would not expect a person with high blood pressure to stop their medication and maintain normal blood pressure through willpower alone. The same logic applies to weight management medications.
The American Association of Clinical Endocrinology and multiple obesity medicine professional societies now explicitly recognize that long-term pharmacotherapy may be necessary for weight maintenance. If you attempted a structured discontinuation with tapering, dietary optimization, and regular exercise, and you are still experiencing significant regain, restarting is a reasonable and medically supported option.
If you do restart, the good news is that most patients respond well to re-treatment. Response timelines on re-initiation are typically similar to the initial treatment course, though some patients respond even faster the second time because they already know what dietary and behavioral adjustments work best for them.
Blood sugar management after stopping semaglutide
This section is specifically for people who take semaglutide for type 2 diabetes or prediabetes. If you use it exclusively for weight management without a diabetes diagnosis, blood sugar changes after stopping are typically minimal and self-resolving. But if you have diabetes, this section deserves your full attention.
What happens to blood glucose
Semaglutide improves blood sugar through multiple mechanisms. It stimulates insulin secretion when glucose is elevated. It suppresses glucagon, which prevents your liver from releasing excess sugar. It slows gastric emptying, which blunts post-meal glucose spikes. And it promotes weight loss, which improves insulin sensitivity independently.
When you stop the medication, all of these mechanisms stop. The result is predictable. Fasting blood glucose starts climbing within the first week, typically increasing 20 to 30 mg/dL in the first two weeks. Post-meal spikes become more pronounced as gastric emptying normalizes. HbA1c levels begin drifting upward, with meaningful increases visible at the three-month mark.
The cardiometabolic data from the STEP 1 extension tells the same story. Blood pressure improvements achieved during treatment largely reverted toward baseline after stopping. Lipid improvements followed a similar pattern. C-reactive protein, a marker of inflammation, also trended back toward pre-treatment levels.
Monitoring schedule
If you have type 2 diabetes and stop semaglutide, whether cold turkey or through tapering, you need an intensified monitoring schedule for at least the first 12 weeks.
Weeks 1 to 4: Check fasting blood glucose daily. Check post-meal glucose (two hours after your largest meal) at least three times per week. Contact your provider if fasting readings consistently exceed 180 mg/dL or post-meal readings exceed 250 mg/dL.
Weeks 5 to 8: You can reduce to fasting glucose checks three to four times per week if levels are stable. Continue post-meal checks twice weekly.
Week 12: Get an HbA1c test. This gives you the most accurate picture of how your average blood sugar has changed since stopping. Compare it to your most recent on-treatment HbA1c to assess the actual impact of discontinuation.
Ongoing: Resume your pre-semaglutide monitoring schedule, or whatever schedule your healthcare provider recommends based on your current control.
Medication adjustments to expect
Your provider will likely need to adjust your other diabetes medications when you stop semaglutide. The most common adjustments include increasing metformin to maximum tolerated dose if you are not already there, adding or increasing sulfonylurea therapy if needed, adjusting insulin doses upward, or switching to a different GLP-1 receptor agonist like liraglutide or dulaglutide.
If you are considering stopping semaglutide and transitioning to a different GLP-1 medication, discuss the differences between available options with your prescriber. Switching to tirzepatide or another GLP-1 agonist may provide continued blood sugar benefits while addressing whatever issue prompted the switch.
Do not adjust your own diabetes medications without medical guidance. The interaction between multiple glucose-lowering drugs is complex, and incorrect adjustments can cause dangerous hypoglycemia. This is the one area where stopping semaglutide truly requires professional oversight rather than self-management.
Side effects and symptoms after quitting semaglutide
Let us be precise about language here. Semaglutide does not cause withdrawal in the medical sense of that term. Withdrawal implies physical dependency, tolerance, and a specific syndrome of symptoms caused by the absence of the drug. Semaglutide does not produce any of these. What it does produce is a rebound, the return of the original symptoms that the medication was treating. This distinction matters because it changes how you think about and manage what happens after stopping.
Appetite and hunger changes
The return of appetite is the most universally reported change after stopping semaglutide. It manifests differently for different people. Some experience it as a general increase in food interest, thinking about meals more often, noticing food smells more acutely, finding portions less satisfying. Others experience it as intense, specific cravings for high-calorie foods that were easy to resist while on the medication.
The timeline is relatively consistent. Mild increases in appetite during weeks one and two. Moderate increases during weeks two through four. Full return to pre-medication appetite levels by weeks four through eight. Some people report a temporary overshoot, where appetite feels stronger than it was before starting semaglutide, during weeks six through ten. This usually normalizes by month three.
The overshoot phenomenon may be related to neurological rebound. Your GLP-1 receptors have been chronically stimulated by supraphysiological doses of semaglutide. When that stimulation is removed, there may be a temporary period of relative undersensitivity to your own natural GLP-1, which manifests as heightened hunger. This is not yet well-characterized in the literature, but it is consistently reported in clinical practice.
Digestive shifts
Semaglutide slows gastric emptying significantly. When it clears your system, gastric emptying speeds back up. This transition can cause temporary digestive symptoms in both directions.
If you experienced constipation on semaglutide, the return to normal gastric motility often brings relief. Bowel movements become more regular and more comfortable. This is one of the genuinely positive changes after stopping.
If you adjusted to the slow gastric emptying and ate accordingly, the sudden normalization can temporarily cause bloating, loose stools, or increased gas as your system readjusts to processing food at its natural pace. These symptoms are typically mild and resolve within one to three weeks.
Some people experience temporary nausea during the transition. This is ironic, since nausea is also a common side effect of starting semaglutide. The mechanism is different, though. Startup nausea comes from the medication slowing your digestive system. Stopping nausea comes from blood sugar fluctuations and rapid changes in gut motility. Both are temporary.
Energy and mood changes
Energy changes after stopping semaglutide are mixed and individual. Many people report increased energy as the medication clears. Semaglutide-related fatigue is a recognized side effect, and its resolution can feel genuinely rejuvenating. Physical energy improves. Mental fog lifts. Exercise feels less effortful.
Mood changes are more variable. Some people feel better after stopping, particularly if they experienced mood changes, anxiety, or emotional blunting while on the medication. Others feel worse, particularly if the weight they begin to regain triggers frustration, self-criticism, or anxiety about losing their progress.
The psychological aspect of stopping should not be minimized. If you lost significant weight on semaglutide and your self-image improved, watching the scale trend upward can be genuinely distressing. Having realistic expectations, a solid maintenance plan, and support from a healthcare provider or counselor can make this transition significantly less challenging emotionally.
What is normal vs what needs medical attention
Most symptoms after stopping semaglutide are temporary and self-resolving. However, certain situations warrant immediate medical contact.
Contact your provider if you experience fasting blood glucose consistently above 200 mg/dL if you have diabetes. Contact them for severe or persistent nausea lasting more than two weeks. Report unexplained abdominal pain, especially if it is severe or accompanied by vomiting. Seek attention for symptoms of dehydration like dizziness, dark urine, or rapid heart rate. And reach out for any symptom that feels significantly different from what you expected based on this guide or your provider pre-discussion.
General appetite increase, mild digestive changes, gradual weight gain, and temporary mood shifts are all within the normal range of post-discontinuation experiences. They are unpleasant but not dangerous. They are manageable with the strategies outlined throughout this guide.
Who should NOT stop semaglutide cold turkey
While cold turkey is medically safe for most people, certain populations benefit strongly from a structured taper rather than abrupt discontinuation. If you fall into any of these categories, talk to your provider about a tapering plan rather than stopping on your own.
Diabetes patients on combination therapy
If you take semaglutide alongside insulin, sulfonylureas, or other glucose-lowering medications, stopping abruptly without adjusting those other medications can create unpredictable blood sugar patterns. In some cases, the other medications may need to be increased when semaglutide stops. In others, the combination may need to be restructured entirely. This is too complex for self-management and requires prescriber involvement.
The risk here is not semaglutide withdrawal. It is the medication gap. When you remove one component of a multi-drug diabetes regimen, the remaining components may not be sufficient. Getting ahead of this gap through planned tapering and proactive medication adjustment is significantly safer than reacting to high blood sugars after they have already occurred.
People with significant remaining weight to lose
If you are stopping semaglutide before reaching your weight loss goal, the risk of regain is particularly high. You are stopping before the full behavioral adaptation that comes with extended treatment has had time to develop. You may not have established the exercise habits, dietary patterns, or psychological coping mechanisms needed to maintain your partial loss.
In this situation, tapering rather than cold turkey gives you a longer runway to build those habits. Each step down in dose provides weeks of partial support while you strengthen your independent maintenance skills. If you find during the taper that you cannot maintain at a given step, that information is valuable. It might indicate that continued treatment at a lower maintenance dose is more appropriate than full discontinuation.
Those without a maintenance plan
Stopping semaglutide without a maintenance plan is the single biggest predictor of maximum regain. If you have not established a specific dietary protocol, an exercise routine, a monitoring schedule, and ideally professional support, you are not ready to stop. This is not judgment. It is data. The research is unambiguous on this point.
Before stopping, you should be able to answer these questions concretely. What is your daily protein target? What does your weekly exercise schedule look like? How often will you weigh yourself? What is your plan if the scale increases by more than five pounds? Who is your professional support, a dietitian, a trainer, a counselor? If any of these answers are vague, spend another four to eight weeks building those structures before initiating discontinuation.
SeekPeptides members access comprehensive protocol guides for managing treatment duration, tapering strategies, and post-medication maintenance. The transition off semaglutide is one of the most commonly discussed topics in the community, and having access to experienced perspectives during this phase can make the difference between maintaining your results and losing them.
Building your personal discontinuation plan
A good discontinuation plan is specific, structured, and starts before your last dose. Vague intentions to eat better and exercise more are not plans. They are wishes. And wishes do not outperform pharmacology. Your plan needs to be concrete enough that you could hand it to someone else and they could follow it.
Four weeks before stopping
Begin increasing protein intake to target levels. Start or intensify a resistance training program. Establish a food journaling practice, even a simple one. Get baseline measurements: weight, waist circumference, blood pressure, and fasting blood glucose if you have diabetes. Schedule follow-up appointments for weeks 4, 8, and 12 after your planned stop date.
This is also the time to prepare mentally. Read the research on outcomes after stopping. Set realistic expectations. Acknowledge that some weight regain is normal and does not represent failure. Identify your emotional triggers around food and weight and develop specific strategies for managing them without pharmaceutical support.
The day you stop (or begin tapering)
Record your current weight, waist circumference, and how you feel. Take a photo if that motivates you. Write down your protein target, your exercise schedule, and your monitoring plan. Put your follow-up appointments in your calendar. Tell someone what you are doing, a partner, a friend, your healthcare provider, your trainer. Accountability makes maintenance significantly more likely.
Remove high-calorie, low-nutrition trigger foods from your home. Stock your kitchen with high-protein, high-fiber options that you genuinely enjoy eating. Preparation is not paranoia. It is strategy. Your appetite is going to increase, and when it does, you want your environment to support your goals rather than undermine them.
Weeks one through four after stopping
Monitor your weight weekly. Not daily, as daily fluctuations create unnecessary anxiety. Weekly provides trend data without noise. Continue your exercise program even when motivation dips, and it will dip. Stick to your meal plan even when hunger increases, and it will increase.
Expect the appetite return around days 7 to 14. Do not panic. It is pharmacologically predictable. Increase meal frequency to four to five smaller meals per day if three larger meals are not satisfying. Prioritize protein at every eating occasion. Stay hydrated, as thirst can masquerade as hunger, especially during this transition.
Check in with your provider if you have diabetes. Share your blood glucose data. Make any medication adjustments they recommend promptly rather than waiting.
Months two through six
This is the critical maintenance window. Most regain that is going to happen occurs during this period. Continue weekly weigh-ins. Maintain your exercise program. If you notice a trend of more than five pounds of regain, tighten your dietary protocol rather than waiting to see if it resolves on its own. Early intervention beats late reaction every time.
Consider working with a registered dietitian during this period if you are not already. The transition from medication-supported weight management to self-directed weight management is a specific skill set that professionals can help you develop. This is not about willpower. It is about strategy and support.
At the six-month mark, you will have a clear picture of your long-term trajectory. If you have maintained within five to ten pounds of your stopping weight, your maintenance plan is working. If regain has been more significant, it is time to discuss options with your provider, which may include restarting semaglutide, switching to a different medication, or intensifying behavioral support.
The role of SeekPeptides in your semaglutide journey
Navigating semaglutide discontinuation does not have to be a solo project. SeekPeptides provides comprehensive resources for every phase of the GLP-1 journey, from initial dosing through long-term maintenance and discontinuation planning. Members access detailed dosage calculators, evidence-based protocols, and a community of researchers who have navigated these exact transitions.
The peptide calculator tools help with precise dosing during tapering, ensuring you know exactly how much medication you are administering at each step-down. The reconstitution calculator ensures accuracy if you are working with compounded formulations that require custom dilution for taper doses.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
Comparing semaglutide discontinuation to other GLP-1 medications
If you are considering stopping semaglutide, understanding how its discontinuation compares to other GLP-1 receptor agonists provides useful context. Not all GLP-1 medications produce the same rebound effects, and knowing the differences can inform your decision.
Semaglutide vs liraglutide discontinuation
A meta-analysis comparing GLP-1 discontinuation outcomes found that semaglutide is associated with more pronounced rebound in body weight and systolic blood pressure compared to liraglutide. This makes sense pharmacologically. Semaglutide produces greater weight loss during treatment, which means there is more potential weight to regain. The higher the peak, the further the potential fall.
Liraglutide has a shorter half-life, approximately 13 hours compared to semaglutide seven-day half-life. This means liraglutide clears the body faster after stopping, approximately two to three days versus five weeks. The shorter clearance means the transition is compressed but more intense. Appetite returns faster but the total adjustment period is shorter.
Semaglutide vs tirzepatide discontinuation
Tirzepatide, which works on both GIP and GLP-1 receptors, produces even greater weight loss than semaglutide during treatment. Early discontinuation data suggests similar patterns of regain, with participants regaining a substantial portion of lost weight after stopping. The dual-mechanism nature of tirzepatide means discontinuation involves the loss of two receptor pathways rather than one, which may make the transition feel more dramatic.
If you are thinking about switching between these medications rather than stopping entirely, understanding the conversion dosing is important. Some patients find that switching to a different GLP-1 from one that was causing side effects allows them to continue treatment rather than discontinuing the class entirely.
The broader GLP-1 discontinuation landscape
Across all GLP-1 receptor agonists, the pattern is consistent. These medications treat the symptoms of obesity and diabetes while they are active. When they are removed, the underlying condition reasserts itself to varying degrees. This is not a flaw of the medications. It is a reflection of the chronic nature of the conditions they treat.
Understanding this helps frame the discontinuation conversation properly. Stopping semaglutide is not quitting a crutch. It is choosing to manage a chronic condition through alternative means. Sometimes those alternative means are sufficient. Sometimes they are not. And there is no moral dimension to either outcome. The question is purely practical: what approach gives you the best health outcomes?
Frequently asked questions
Can I stop semaglutide cold turkey if I only took it for a few weeks?
Yes. If you have only been on semaglutide for a few weeks and are still at a low dose like 0.25 mg or 0.5 mg, cold turkey is perfectly safe and tapering is unnecessary. The medication has not been in your system long enough to produce significant rebound effects. You may notice a mild appetite increase but it will be far less dramatic than someone stopping after months of treatment at full therapeutic dose.
How long after stopping semaglutide will my appetite return?
Most people notice meaningful appetite increases between days 7 and 14 after their last injection, with full return to pre-medication appetite levels by weeks four through eight. The timeline depends on your final dose, duration of treatment, and individual biology. Some people experience a temporary overshoot where appetite feels even stronger than before starting, but this usually normalizes by month three.
Will I definitely gain weight back after stopping semaglutide?
Not necessarily. The STEP 1 trial showed an average regain of two-thirds of lost weight, but that study involved no maintenance plan after stopping. Real-world data is more encouraging, with more than half of patients maintaining weight loss at one year when they implement structured nutrition plans, exercise programs, and monitoring. Your maintenance strategy determines your outcome far more than the act of stopping itself.
Is semaglutide addictive?
No. Semaglutide does not create chemical dependency, physical tolerance, or withdrawal syndrome. It is not classified as a controlled substance. The changes you experience after stopping are rebound effects, the return of pre-existing conditions, not withdrawal from an addictive substance. This distinction is medically important.
Can I switch from semaglutide to another GLP-1 instead of stopping?
Yes. Switching to tirzepatide, liraglutide, or another GLP-1 receptor agonist is a common strategy for people who want to change medications without losing the benefits of GLP-1 therapy. The dosage conversion between medications requires medical guidance to get right, as the potencies and mechanisms are not identical.
Should I stop semaglutide before surgery?
Most surgical guidelines now recommend stopping semaglutide before elective surgery due to its effect on gastric emptying and anesthesia risk. The American Society of Anesthesiologists suggests stopping at least one week before surgery, though some surgeons prefer two to three weeks. Always discuss timing with your surgical team, as recommendations vary based on the type of procedure.
Can I take supplements to help with the transition off semaglutide?
Some people find that berberine provides mild appetite-suppressing and blood sugar-lowering effects that can help bridge the transition. Fiber supplements can increase satiety. Protein supplements help meet increased protein targets. None of these replace semaglutide effect, but they can provide modest support during the adjustment period. Discuss any supplements with your provider, especially if you have diabetes.
What if I accidentally missed a dose but was not planning to stop?
A single missed dose is not the same as stopping cold turkey. Semaglutide seven-day half-life means one missed weekly injection reduces your levels but does not eliminate them. Take your next dose as scheduled. If you miss two or more consecutive doses and were at a higher dose, your provider may recommend re-titrating up from a lower dose to avoid reintroduction side effects.
How long does semaglutide stay in your system after stopping?
Approximately five weeks. Semaglutide has a half-life of about seven days, and it takes roughly five half-lives for a medication to be considered fully eliminated. You will still have trace amounts at five weeks, but they are below the threshold for meaningful clinical effect. Full clearance to undetectable levels takes about seven weeks.
Can I stop and restart semaglutide multiple times?
Yes, but repeated stop-start cycles are not ideal. Each restart typically requires re-titration from the lowest dose, which means weeks of subtherapeutic dosing before you return to an effective level. The startup side effects like nausea often return with each restart. If you find yourself stopping and restarting repeatedly, it may be worth discussing consistent long-term treatment at a lower maintenance dose with your provider instead.
External resources
STEP 1 Trial Extension: Weight Regain After Semaglutide Withdrawal (PubMed)
Metabolic Rebound After GLP-1 Receptor Agonist Discontinuation (eClinicalMedicine/The Lancet)
Real-World Weight Loss Maintenance After GLP-1 Discontinuation (Epic Research)
What to Expect When You Stop Taking Semaglutide (Banner Health)
In case I do not see you, good afternoon, good evening, and good night. May your transitions stay smooth, your results stay lasting, and your health stay on track.