Feb 28, 2026

Of every ten people who start semaglutide for weight loss, roughly eight will lose at least 5% of their body weight. That is the clinical data. But the number that matters most to you, the one keeping you up at night, is simpler. How fast? How many pounds per week? When will you actually see results on the scale, in the mirror, in the way your clothes fit? The answer is not one number. It is a curve, and that curve looks different depending on a dozen factors that most guides completely ignore.
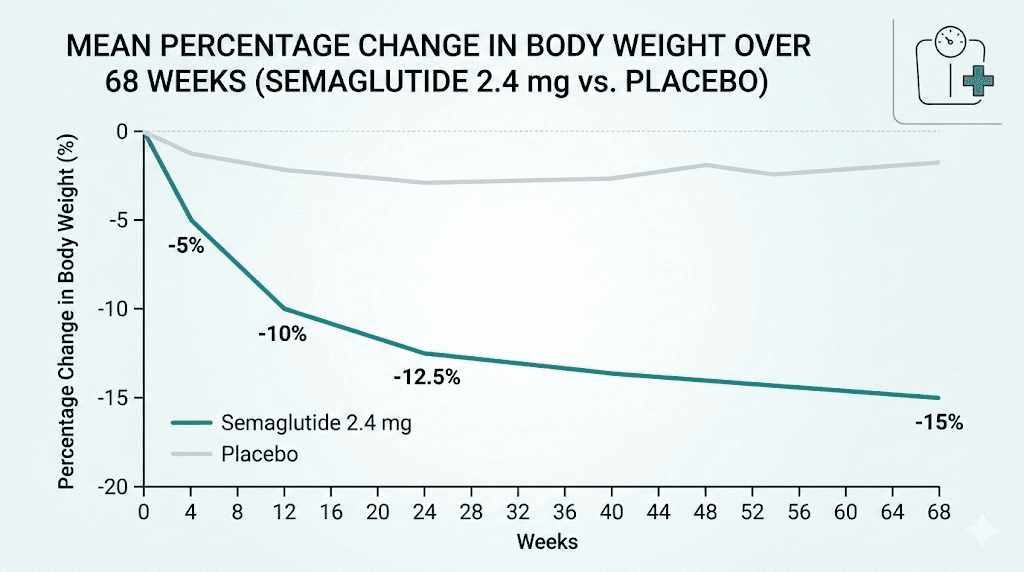
Here is what the research actually shows. In the landmark STEP 1 clinical trial, participants lost an average of 3.8% of their body weight in the first four weeks alone. By month three, that number climbed to 9.6%. By month six, 13.8%. And by the end of the 68-week study, the average weight loss reached 14.9% of starting body weight. For someone who weighs 220 pounds, that translates to roughly 33 pounds gone. Real pounds. Documented in a randomized, double-blind, placebo-controlled trial published in the New England Journal of Medicine.
But averages hide enormous variation. Some people lose weight rapidly from week one. Others see almost nothing for the first month, then experience a dramatic acceleration. And a significant minority, roughly 14% in clinical trials, do not achieve even 5% weight loss despite consistent use. Understanding where you are likely to fall on that spectrum requires looking beyond the headlines. This guide breaks down the complete semaglutide weight loss timeline, the factors that determine your personal rate of loss, and the strategies that separate the fastest responders from everyone else.
What the clinical trials actually show about semaglutide weight loss speed
Before looking at individual timelines, the trial data provides the foundation. Four major clinical trials, collectively known as the STEP program, enrolled thousands of participants and tracked their weight loss over periods ranging from 68 weeks to two full years. The results tell a consistent story about how semaglutide works over time.
STEP 1 trial results
The STEP 1 trial remains the gold standard. Published in the New England Journal of Medicine, it enrolled 1,961 adults with a BMI of 30 or higher (or 27 with at least one weight-related condition) who did not have diabetes. Participants received either semaglutide 2.4 mg once weekly or placebo, combined with lifestyle counseling.
The results were striking. At week 68, the semaglutide group lost an average of 14.9% of their body weight compared to just 2.4% in the placebo group. Breaking that down by milestone shows a clear pattern of rapid early loss that gradually decelerates.
Week 4 showed a 3.8% average reduction. Week 12 reached 9.6%. Week 24, roughly six months in, hit 13.8%. The curve continued climbing but at a slower rate, reaching its lowest point around week 60 before plateauing. The distribution matters too. A full 86.4% of participants on semaglutide achieved at least 5% weight loss. Nearly 70% hit 10% or more. And over half, roughly 51 to 64%, reached the 15% threshold that clinicians consider transformative for metabolic health.
STEP 5 trial: the two-year picture
The STEP 5 trial extended the observation window to 104 weeks, two full years on semaglutide. The long-term data paints an even more encouraging picture for sustained results.
At 6 months, participants lost an average of 13.4% of their starting weight. By 12 months, that figure reached 17.6%. At 18 months, 20.3%. And at the two-year mark, 20.4%. The plateau around weeks 60 to 68 that appeared in STEP 1 held here as well, with weight loss essentially stabilizing after the first year. But the critical finding was that the lost weight stayed off for those who continued treatment.
For practical purposes, these numbers translate to roughly 2% of body weight lost per month during the first six months, then approximately 1% per month during months six through twelve. After that, the rate drops to near zero as the body reaches a new equilibrium. Understanding this trajectory is essential for setting expectations, because early results do not always predict long-term outcomes.
Real-world data versus clinical trials
Clinical trial participants receive intensive lifestyle counseling, regular monitoring, and structured support that most real-world users do not get. So how do results compare outside the controlled environment?
A real-world analysis published in JAMA Network Open tracked patients initiating semaglutide 2.4 mg in clinical practice. The findings were encouraging. Mean weight loss reached approximately 12 to 15% at 12 months, slightly lower than clinical trials but still substantial. The difference was modest, suggesting that semaglutide delivers meaningful results even without the intensive support structure of a clinical trial.
Individual variation, however, was wider in real-world settings. Adherence to the proper dosing schedule played a significant role, as did dietary choices and physical activity levels. Users who combined semaglutide with structured diet plans and consistent exercise typically matched or exceeded clinical trial results.
Week-by-week semaglutide weight loss timeline
The clinical data provides averages, but what does the experience actually look like week by week? Understanding the typical progression helps set realistic expectations and prevents the frustration that causes many people to quit too early.
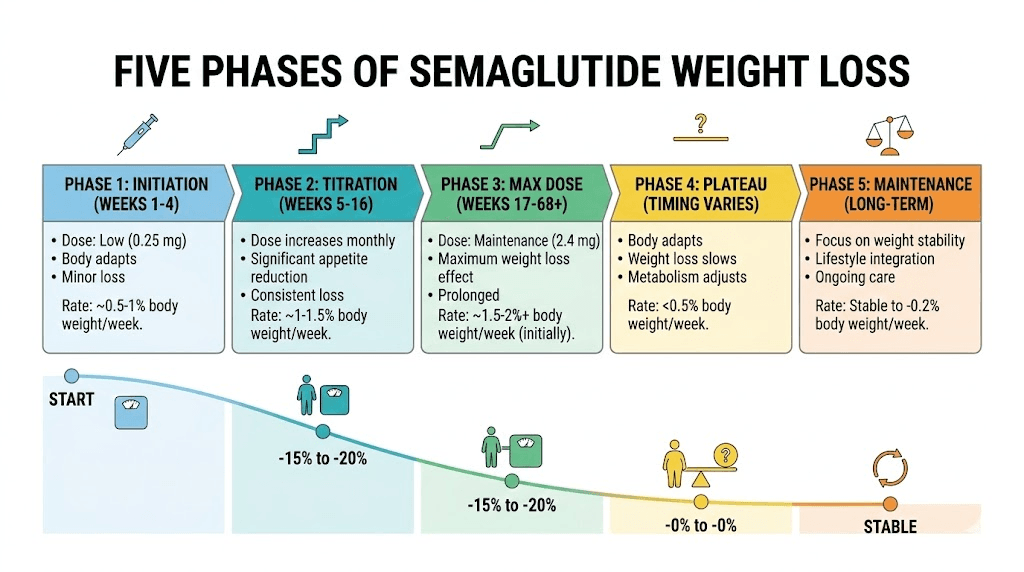
Week 1 to 2: the adjustment phase
Most people start semaglutide at 0.25 mg, the lowest dose in the escalation protocol. This is not the therapeutic dose for weight loss. It exists solely to allow your body to adjust to the medication and minimize gastrointestinal side effects.
Weight changes during this period are minimal and inconsistent. Some people lose 1 to 3 pounds from reduced appetite. Others see no change at all. A few might even gain a pound or two from water retention. Do not panic if the scale does not move.
What you will notice is different. Appetite begins to shift. Food becomes less interesting. The appetite suppression effect starts subtly, like background noise you barely register at first. Portions that once felt normal start feeling too large. Cravings for highly palatable foods, the salty, sweet, and fatty combinations that drive overeating, begin to quiet down.
Side effects during weeks one and two are usually mild. Bloating, mild nausea, and occasional constipation are the most common. These typically resolve within a few days of each injection.
Week 3 to 4: first measurable results
Still on 0.25 mg for the first four weeks (or transitioning to 0.5 mg at the end of week four), this is when the scale starts cooperating for most people. Average weight loss at the four-week mark sits around 3.8% of starting body weight based on STEP 1 data.
What does 3.8% look like in real numbers?
Starting weight 180 lbs: approximately 7 pounds lost
Starting weight 200 lbs: approximately 7 to 8 pounds lost
Starting weight 220 lbs: approximately 8 to 9 pounds lost
Starting weight 250 lbs: approximately 9 to 10 pounds lost
Starting weight 300 lbs: approximately 11 to 12 pounds lost
These numbers come from clinical trial averages. Your actual results will vary. But if you are within this ballpark by week four, you are on track. If you are seeing less, the therapeutic dose has not kicked in yet, and the real acceleration comes in the next phase.
This is also when many people check the one-month results data to benchmark their progress. Compare trends, not individual days. Weight fluctuates constantly from water retention, food volume, and hormonal shifts.
Month 2 to 3: the acceleration zone
This is where things get interesting. By month two, most users have escalated to 0.5 mg or 1.0 mg. The appetite suppression deepens. Caloric intake drops naturally without the white-knuckle willpower that diet attempts require. And the scale starts moving faster.
Clinical data shows approximately 9.6% body weight loss by week 12. That is a dramatic acceleration from the 3.8% at week four. The rate of loss during this window averages roughly 2 to 2.5% of body weight per month, the fastest sustained rate most people will experience on semaglutide.
In practical terms, someone who started at 220 pounds might be down 18 to 21 pounds by month three. Clothing fits noticeably differently. The face begins to look leaner. Energy levels often improve as the body carries less excess weight. Friends and family start commenting.
Side effects can intensify during dose escalations. Sulfur burping, nausea, and dizziness sometimes flare when moving to a higher dose. These typically settle within a week. If they do not, talk to your healthcare provider about splitting the dose or slowing the escalation.
The critical mistake during this phase is cutting calories too aggressively on top of the appetite suppression. Semaglutide already reduces your intake substantially. Combining it with an extreme caloric deficit leads to muscle loss, fatigue, nutritional deficiencies, and a metabolic slowdown that undermines long-term results. Eat enough. Prioritize protein. Trust the medication to handle the deficit.
Month 4 to 6: steady, significant loss
By month four, most people have reached or are approaching the 1.7 mg or 2.4 mg maintenance dose. The appetite suppression is at its peak. The metabolic benefits of GLP-1 receptor agonism, improved insulin sensitivity, reduced inflammation, better glucose regulation, are fully engaged.
Weight loss continues at a strong but slightly decelerating pace. The STEP 1 trial showed 13.8% average loss at week 24 (roughly six months). That means someone starting at 250 pounds would be down approximately 34 to 35 pounds. A person starting at 200 pounds would be down about 28 pounds.
The deceleration is normal and expected. It does not mean the medication stopped working. It means your body has adjusted to the lower caloric intake, your metabolic rate has recalibrated, and you are approaching the range where your body wants to stabilize. This is the same trajectory seen with every effective weight loss intervention, from surgery to pharmacotherapy to intensive lifestyle programs.
During this phase, non-scale victories often become more meaningful than the number. Improved blood pressure. Better sleep. Reduced joint pain. Higher energy. Improved blood markers. These changes happen whether the scale moves one pound or five in a given week. If you are not losing weight as expected during this window, specific strategies can help reignite progress.
Month 7 to 12: the gradual deceleration
Weight loss does not stop at six months. It continues. But the pace slows to approximately 1% of body weight per month, sometimes less. This is the long, steady tail of the semaglutide weight loss curve.
The STEP 5 trial documented this clearly. At 12 months, average weight loss reached 17.6%, up from 13.4% at six months. That additional 4.2 percentage points over six months represents real, meaningful progress, but the rate is roughly half what it was during months two through six.
This phase tests patience. The rapid initial drops that felt so motivating give way to slower, grindier progress. Some weeks the scale does not move at all. Others it drops suddenly. The pattern becomes less predictable, and many people interpret the slowdown as failure.
It is not failure. It is physiology.
Your body has lost a substantial amount of mass. Its caloric needs have dropped. The metabolic adaptations that evolved to prevent starvation are pushing back against further loss. The medication continues working, suppressing appetite and improving metabolic function, but it is fighting against a body that is increasingly resistant to further weight reduction.
This is also when questions about treatment duration become important. The evidence strongly supports continued use for weight maintenance, but the conversation with your healthcare provider should address your specific goals and health markers.
Beyond 12 months: the maintenance plateau
Around month 12 to 15, weight loss essentially plateaus for most people. The STEP 5 trial showed virtually identical weight loss at 18 months (20.3%) and 24 months (20.4%). The body has reached a new equilibrium.
This plateau is not a sign to stop. Discontinuing semaglutide leads to weight regain in most cases. The STEP 1 extension study found that participants who stopped semaglutide regained approximately two-thirds of their lost weight within one year. The medication is not a temporary fix. For most people, it is a long-term or potentially lifelong therapy, similar to blood pressure medication or statins.
Continued use maintains the weight loss and the metabolic improvements that came with it. The plateau is the goal, not a problem to solve. Reaching a stable, lower weight while maintaining your health markers is exactly what successful treatment looks like.
How much weight you can realistically expect to lose
Clinical trial averages are helpful. But you want to know what to expect for your body, at your weight, in your situation. Here is a framework for setting realistic expectations based on the data.
Weight loss by starting weight
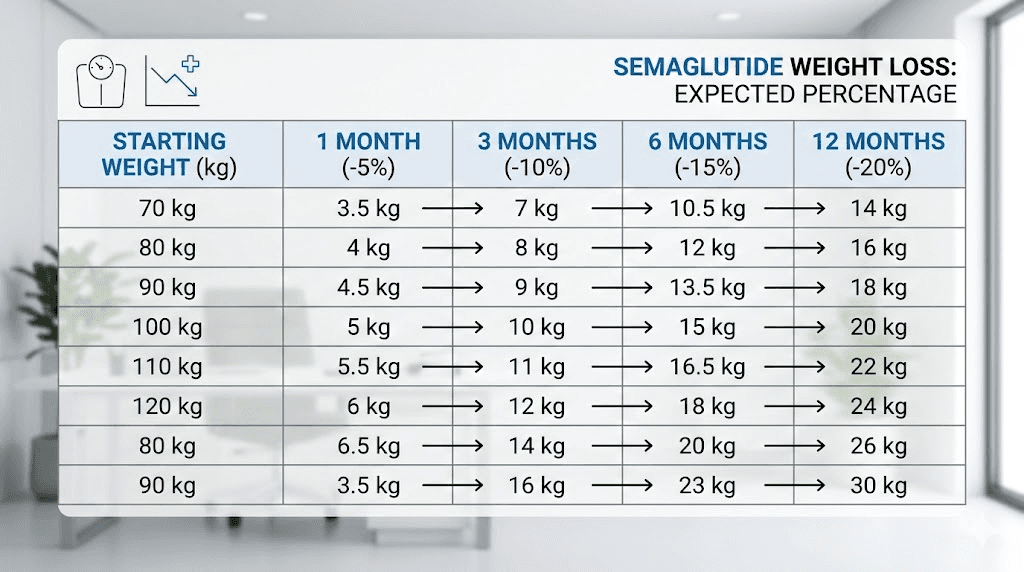
Since semaglutide weight loss is reported as a percentage of starting body weight, heavier individuals tend to lose more total pounds even though the percentage may be similar. Use our semaglutide dosage calculator for personalized estimates.
Starting weight | 3 months (10%) | 6 months (14%) | 12 months (17%) |
|---|---|---|---|
170 lbs | 17 lbs (153 lbs) | 24 lbs (146 lbs) | 29 lbs (141 lbs) |
200 lbs | 20 lbs (180 lbs) | 28 lbs (172 lbs) | 34 lbs (166 lbs) |
230 lbs | 23 lbs (207 lbs) | 32 lbs (198 lbs) | 39 lbs (191 lbs) |
260 lbs | 26 lbs (234 lbs) | 36 lbs (224 lbs) | 44 lbs (216 lbs) |
300 lbs | 30 lbs (270 lbs) | 42 lbs (258 lbs) | 51 lbs (249 lbs) |
These projections use the average percentages from STEP 1 and STEP 5 trials. Individual results vary substantially. Some people will exceed these numbers. Others will fall short. The percentage-based approach is more accurate than a fixed pounds-per-week target because it accounts for the relationship between body size and energy expenditure.
What average actually means
When a clinical trial reports 14.9% average weight loss, it does not mean everyone lost 14.9%. The distribution looks more like a bell curve, skewed toward higher losses. Some participants lost 25% or more. Others lost 5% or less. The average captures the middle of this spread.
Roughly 86% of participants lost at least 5%. Approximately 70% lost at least 10%. About 50 to 64% lost at least 15%. And roughly 30 to 35% lost 20% or more. Where you fall depends on factors that are partly within your control and partly determined by biology.
The before and after results you see online tend to showcase the best outcomes. Remember that selection bias drives what gets shared. The person who lost 60 pounds posts about it. The person who lost 15 pounds usually does not. Both results are real. Both are valid. Do not measure your progress against curated success stories.
Rate of loss by phase
Understanding the different phases helps prevent discouragement during normal slowdowns.
Month 1 (dose escalation): 0.5 to 2 lbs per week, highly variable
Month 2 to 4 (acceleration): 1.5 to 3 lbs per week, most rapid sustained loss
Month 5 to 8 (steady state): 1 to 2 lbs per week, consistent but decelerating
Month 9 to 12 (deceleration): 0.5 to 1 lb per week, gradual slowing
Month 12+ (maintenance): minimal further loss, weight stabilization
These ranges assume consistent medication use, appropriate dosing, and reasonable dietary habits. Significant deviations in any of these areas will shift the timeline.
The semaglutide dosage escalation and why it matters for speed
One of the most misunderstood aspects of semaglutide weight loss speed is the role of dosage escalation. You do not start at the full therapeutic dose. Instead, the dose increases gradually over 16 to 20 weeks, which directly affects how quickly results appear.
The standard escalation schedule
The FDA-approved escalation protocol for weight loss (Wegovy) follows this timeline, and most compounding pharmacies follow a similar pattern for compounded semaglutide.
Weeks 1 to 4: 0.25 mg once weekly
Weeks 5 to 8: 0.5 mg once weekly
Weeks 9 to 12: 1.0 mg once weekly
Weeks 13 to 16: 1.7 mg once weekly
Week 17 and onward: 2.4 mg once weekly (maintenance dose)
This means you do not reach the full weight loss dose until roughly month four. Everything before that is building up. The 0.25 mg starting dose produces minimal weight loss on its own. The 0.5 mg dose starts to show more consistent effects. And the 1.0 mg dose is where many people experience the dramatic appetite suppression that drives significant caloric reduction.
By the time you reach 1.7 mg and then 2.4 mg, the appetite suppression is typically profound. Many users report forgetting to eat, feeling full after a few bites, and losing interest in foods they previously craved. This is the dose range where the STEP trial results were achieved.
How each dose level affects weight loss rate
Understanding the dose-response relationship helps explain why early results sometimes disappoint. At 0.25 mg, the GLP-1 receptor activation is modest. Appetite suppression is subtle. Gastric emptying slows slightly. But the metabolic impact is limited.
At 0.5 mg, the effects become more noticeable. Most people report reduced hunger and earlier satiety. Weight loss accelerates modestly compared to the initial dose.
At 1.0 mg, a significant step change occurs. This is where many users describe the medication as truly transformative. Food noise, that constant background hum of thinking about eating, goes quiet. Portions shrink naturally. Cravings diminish substantially.
The jump from 1.0 mg to 1.7 mg and then to 2.4 mg provides incremental improvements. Not everyone needs the full 2.4 mg dose to achieve meaningful results. Some people respond well at 1.0 mg or 1.7 mg. Your provider may adjust the dosage schedule based on your response and tolerance.
Why you should not skip the escalation
It is tempting to jump to a higher dose faster, especially when you see others posting dramatic results while you are still on 0.25 mg. Do not do this.
The escalation exists because GLP-1 receptor agonists cause significant gastrointestinal side effects when introduced too quickly. Nausea, vomiting, severe constipation, and abdominal pain can be debilitating at higher doses without proper titration. These side effects, not the medication itself, are the primary reason people discontinue treatment.
Slow and steady wins this particular race.
The four-week intervals at each dose allow your GLP-1 receptors to adapt, your gut microbiome to adjust, and your digestive system to accommodate the slower gastric emptying. Skipping this process virtually guarantees a miserable experience that could put you off the medication entirely. Follow the proper dosing protocol and let the timeline work as designed.
Factors that speed up or slow down your results
The clinical trials provide averages. But you are not an average. Dozens of individual factors influence how fast semaglutide works for you. Some of these factors are within your control. Others are not. Understanding the difference helps you focus energy where it matters while accepting what you cannot change.
Starting BMI and body composition
People with higher starting BMI tend to lose more total weight but may lose a similar or slightly lower percentage compared to those with moderate obesity. This makes sense from a metabolic standpoint. A larger body burns more calories at rest, creating a larger deficit when appetite decreases.
Body composition also matters. People with more lean muscle mass tend to have higher metabolic rates, which can support faster fat loss. Those with a higher proportion of visceral fat (the deep abdominal fat around organs) often see faster initial results because visceral fat is more metabolically active and responds more readily to caloric restriction.
If you are concerned about body composition changes, explore peptides that support both weight loss and muscle preservation as complementary options.
Diet quality and caloric intake
Semaglutide reduces appetite. It does not make food choices for you. The quality of what you eat during treatment has an enormous impact on both the speed and sustainability of weight loss.
High-protein diets consistently produce better outcomes with GLP-1 medications. Protein preserves muscle mass during weight loss, maintains metabolic rate, enhances satiety beyond what semaglutide alone provides, and supports body composition improvements. The recommended intake is 0.7 to 1.0 grams of protein per pound of ideal body weight, spread across meals.
The best foods to eat on semaglutide prioritize protein, vegetables, healthy fats, and complex carbohydrates while minimizing highly processed foods, added sugars, and refined grains. A structured semaglutide diet plan can make the difference between average and exceptional results.
Conversely, the foods to avoid on semaglutide are essentially the same foods that undermine any weight loss effort. High-sugar beverages, deep-fried foods, excessive alcohol, and ultra-processed snacks all slow progress. Alcohol deserves special mention. Besides adding empty calories, it impairs judgment around food choices and can worsen gastrointestinal side effects. Review the guidelines for drinking on semaglutide before making decisions about alcohol intake.
Exercise type and frequency
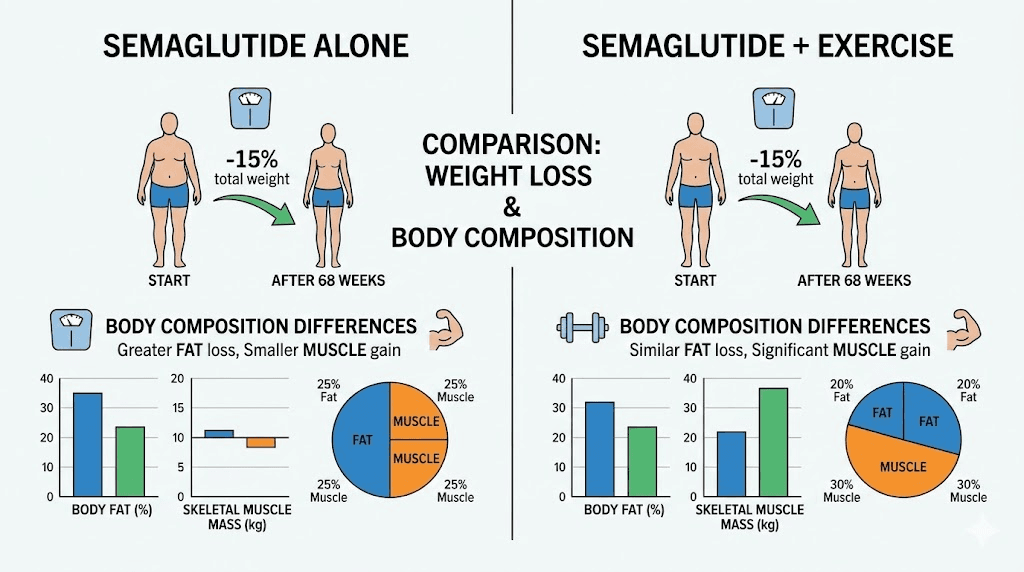
Exercise is not required for semaglutide to work. You can lose weight on semaglutide without exercise. The medication handles the caloric deficit through appetite suppression. But exercise accelerates results and, more importantly, dramatically improves the quality of weight lost.
Without exercise, roughly 25 to 40% of weight lost on semaglutide comes from lean mass (muscle). That is a problem. Muscle loss reduces metabolic rate, impairs physical function, and creates the dreaded "skinny fat" appearance where you weigh less but still look soft. Resistance training reduces muscle loss to 10 to 15% of total weight lost, preserving the metabolic engine that keeps weight off long-term.
The best exercise approach combines three elements. Resistance training 2 to 3 times per week preserves and builds muscle. Moderate cardio (walking, cycling, swimming) 3 to 5 times per week burns additional calories and improves cardiovascular health. And daily movement, walking 7,000 to 10,000 steps, maintains overall activity levels that support sustained weight loss.
For those interested in peptides that support exercise performance during weight loss, energy-boosting peptides and compounds that support fat loss specifically may complement a semaglutide protocol.
Age and metabolic rate
Age affects semaglutide results through several mechanisms. Metabolic rate declines with age, roughly 1 to 2% per decade after age 30. Hormonal changes, particularly declining testosterone in men and estrogen in women, alter fat distribution and muscle preservation. And the accumulated metabolic damage from years of yo-yo dieting can impair the body response to weight loss interventions.
That said, semaglutide works across all adult age groups studied. The STEP trials included participants up to age 75 and showed meaningful weight loss in all age brackets. Older adults may lose weight slightly more slowly and should pay extra attention to protein intake and resistance training to preserve muscle mass and bone density.
Women approaching or in menopause face additional challenges. Hormonal shifts promote visceral fat accumulation and can make weight loss more resistant. Explore peptides for menopause-related weight concerns for additional strategies. SeekPeptides provides in-depth guides on navigating these hormonal challenges while optimizing peptide protocols.
Sleep quality and stress
Two factors that do not appear on any dosing chart but profoundly affect weight loss speed are sleep and stress.
Poor sleep (less than 7 hours or fragmented sleep) increases hunger hormones, decreases satiety signals, impairs insulin sensitivity, and promotes fat storage over fat burning. One study found that sleep-restricted individuals lost 55% less fat and 60% more lean mass compared to well-rested individuals on the same caloric deficit. Semaglutide can suppress appetite even during sleep deprivation, but the metabolic penalties of poor sleep still slow overall results.
Chronic stress elevates cortisol, which promotes visceral fat accumulation, increases cravings for high-calorie foods, and directly inhibits fat mobilization. Addressing sleep quality and stress management is not optional for people serious about maximizing their semaglutide results. It is foundational. If semaglutide is causing insomnia or contributing to fatigue, these issues need to be addressed to avoid undermining the weight loss process.
Other medications and medical conditions
Certain medications can either accelerate or slow semaglutide results. Metformin, for example, may provide a modest additional benefit when combined with semaglutide. Phentermine combined with semaglutide is another combination that some providers prescribe, though the evidence for this specific combination is still emerging.
Thyroid disorders, insulin resistance, polycystic ovary syndrome (PCOS), and other metabolic conditions can slow weight loss. These conditions do not make semaglutide ineffective, but they may reduce the speed of results and require additional management strategies. Regular blood work helps monitor these factors during treatment.
Genetic factors and individual response
Here is the uncomfortable truth. Some people simply respond better to semaglutide than others, and genetics plays a meaningful role in this variation.
Research has identified several genetic variants that influence GLP-1 receptor sensitivity, hunger hormone regulation, and metabolic rate. These variants can make one person a rapid responder who drops weight effortlessly and another a slow responder who struggles for every pound.
You cannot control your genetics. What you can control is everything else on this list. Optimize the modifiable factors, diet, exercise, sleep, stress, medication adherence, and you give yourself the best possible outcome regardless of your genetic baseline.
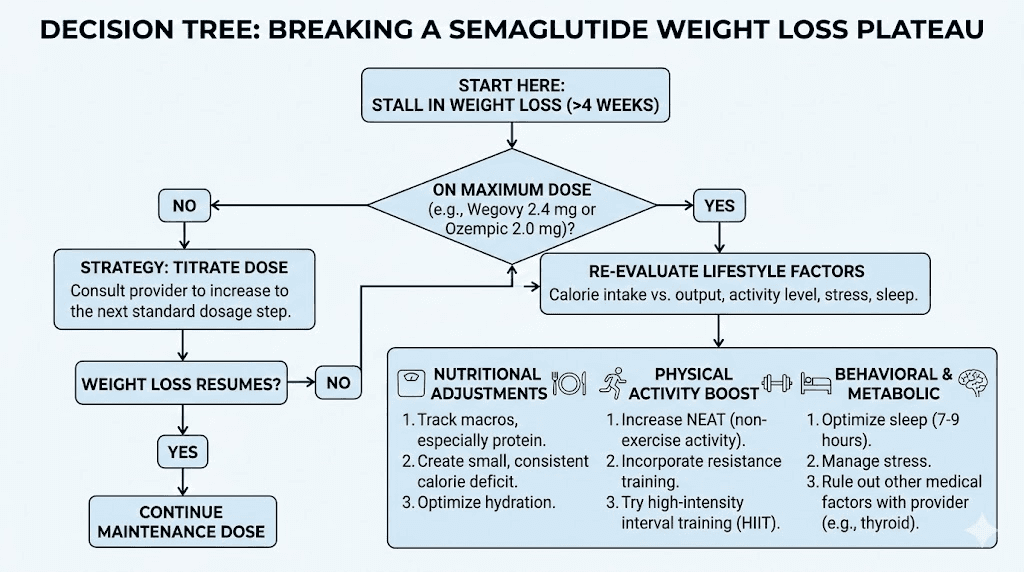
The semaglutide weight loss plateau explained
Every person on semaglutide will eventually hit a plateau. It is not a question of if but when. Understanding why plateaus happen and what to do about them is critical for maintaining motivation and continuing progress.
When the plateau typically happens
Based on clinical trial data, the major plateau occurs around week 60, roughly 14 months into treatment. Weight loss at this point has essentially reached its maximum, and the body stabilizes at a new, lower weight.
However, many people experience mini-plateaus earlier. These can last anywhere from two to six weeks and typically occur during dose escalation transitions, after periods of rapid loss, or during hormonal fluctuations. These are not true plateaus. They are temporary stalls that resolve on their own or with minor adjustments.
A true plateau is defined as no measurable weight change for 8 or more weeks despite consistent medication use and adherence to dietary guidelines. Anything shorter is likely a normal fluctuation, not a plateau.
Why plateaus happen
The primary mechanism is metabolic adaptation. As you lose weight, three things change simultaneously.
First, your resting metabolic rate drops. A smaller body burns fewer calories at rest. Someone who weighed 250 pounds and now weighs 210 pounds burns roughly 200 to 300 fewer calories per day at rest. That deficit adds up.
Second, your non-exercise activity thermogenesis (NEAT), the calories burned through fidgeting, walking, postural adjustments, decreases. Your body unconsciously conserves energy when it senses sustained weight loss.
Third, the thermic effect of food decreases because you are eating less. Digestion burns calories, and less food means less thermic expenditure.
These three factors combined can reduce your daily caloric expenditure by 400 to 600 calories compared to what it was at your starting weight. Since semaglutide reduces appetite by a relatively fixed amount, the caloric deficit shrinks as your body adapts, until eventually expenditure matches intake. That is your plateau.
How to break through a plateau
Not every plateau needs to be broken. If you have reached a healthy weight and your metabolic markers are good, the plateau may simply be your body at its optimal set point on this medication. But if you believe further weight loss is both desirable and achievable, several evidence-based strategies can help.
Reassess caloric intake. As your weight dropped, so did your caloric needs. The portion sizes that created a deficit at 250 pounds might be maintenance-level at 210 pounds. A modest reduction of 100 to 200 calories, primarily from carbohydrates or added fats, can restart the deficit.
Increase protein intake. Protein has the highest thermic effect of any macronutrient, meaning your body burns more calories digesting it. Increasing protein to 30 to 35% of total calories can boost metabolic rate slightly while preserving muscle mass. Explore protein shakes designed for GLP-1 users as a convenient option.
Add or intensify resistance training. Muscle is metabolically active tissue. Adding muscle increases your resting metabolic rate, directly countering the metabolic adaptation that caused the plateau. Even modest gains in lean mass, 2 to 3 pounds, can increase daily expenditure by 30 to 50 calories.
Discuss dose adjustment with your provider. If you are not yet at the maximum 2.4 mg dose, increasing may reignite appetite suppression and restart weight loss. Check your dosage conversion chart to understand how unit measurements translate to milligrams.
Consider complementary approaches. Some providers add B12 supplementation or compounds like L-carnitine with semaglutide to support energy metabolism during plateaus. The evidence for these combinations is limited but the safety profile is generally favorable.
What happens when you stop semaglutide
This is the section nobody wants to read. But understanding it is essential for making informed decisions about treatment.
The weight regain data
The STEP 1 extension study tracked participants for one year after they stopped semaglutide at week 68. The findings were sobering. On average, participants regained two-thirds of the weight they had lost within 12 months of discontinuation. The appetite suppression vanished. The hunger came back. The metabolic advantages reversed.
This does not mean semaglutide failed. It means obesity is a chronic condition that requires ongoing management, similar to hypertension or type 2 diabetes. When you stop the medication that was managing the condition, the condition returns. This is biology, not willpower failure.
The weight regain was not instantaneous. It happened gradually over months, with the fastest regain occurring in the first three to six months after stopping. By month 12, approximately 66% of the lost weight had returned. For someone who had lost 30 pounds, that means regaining roughly 20 pounds within a year of stopping. If you are considering stopping semaglutide, understanding these dynamics is critical for planning your transition.
Minimizing regain if you stop
While complete prevention of regain after stopping semaglutide appears unlikely based on current evidence, several strategies can slow the process.
Establishing strong exercise habits before discontinuation is the single most protective factor. People who maintained consistent resistance training and cardiovascular exercise regained less weight than sedentary individuals. The muscle mass preserved through exercise maintains a higher metabolic rate, partially offsetting the return of appetite.
Behavioral habits matter too. The appetite suppression from semaglutide creates a window for establishing new eating patterns, portion control reflexes, and food preparation routines. If you used that window to build genuine habits rather than simply eating less because you felt less hungry, those habits provide some protection against regain.
Gradual tapering rather than abrupt cessation may help. Although not extensively studied, some providers recommend a slow dose reduction over several weeks to months rather than sudden discontinuation. This allows the body to adjust more gradually to the return of normal appetite signaling. Review the process for restarting semaglutide after a break if you need to resume treatment.
Semaglutide versus tirzepatide: which works faster for weight loss
One of the most common questions from people considering semaglutide is whether tirzepatide might work faster. The data suggests it does, though the comparison requires context.
Head-to-head data
The SURMOUNT-1 trial studied tirzepatide at doses of 5 mg, 10 mg, and 15 mg for weight loss. At the highest dose (15 mg), participants lost an average of 22.5% of their body weight over 72 weeks, compared to semaglutide average of 14.9% over 68 weeks in STEP 1. The SURPASS-2 trial directly compared tirzepatide to semaglutide 1 mg (not the 2.4 mg weight loss dose) and found tirzepatide produced greater weight loss at all dose levels.
Metric | Semaglutide 2.4 mg | Tirzepatide 15 mg |
|---|---|---|
Average weight loss | 14.9% | 22.5% |
Achieved 5% loss | 86% | 96% |
Achieved 10% loss | 70% | 89% |
Achieved 20% loss | 32% | 63% |
Trial duration | 68 weeks | 72 weeks |
The difference is substantial. Tirzepatide, which activates both GLP-1 and GIP receptors (dual agonism), appears to produce faster and greater weight loss than semaglutide, which activates only GLP-1 receptors. For a detailed breakdown of how these medications compare in terms of side effects and dosing protocols, check the dedicated comparison guides.
Why semaglutide might still be the right choice
Despite the head-to-head numbers favoring tirzepatide, semaglutide remains the right choice for many people. It has a longer track record. More real-world safety data exists. It is more widely available and often more affordable, especially in compounded form. And 14.9% average weight loss is still a profound, life-changing result for most people.
The decision between semaglutide and tirzepatide should involve your healthcare provider and consider factors like cost, availability, medical history, and personal response. Some people who do not respond well to semaglutide find success with tirzepatide, and vice versa. The conversion chart can help if you are considering a switch.
For those curious about the next generation of weight loss peptides, retatrutide is showing even more dramatic results in early trials, with triple receptor agonism targeting GLP-1, GIP, and glucagon receptors simultaneously.
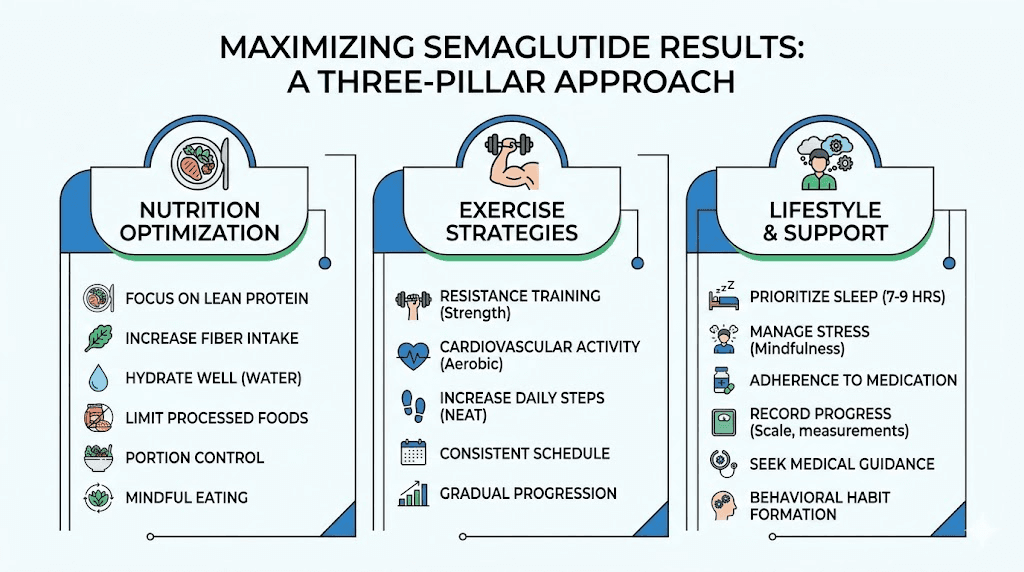
Maximizing your semaglutide weight loss speed
You have the timeline. You understand the factors. Now here is how to stack the deck in your favor and achieve the fastest possible results within a safe and sustainable framework.
Nutrition strategies for faster results
The appetite suppression from semaglutide makes it easier to eat less. But eating less of the wrong things still produces suboptimal results. Here is a framework built on the evidence.
Protein first, always. Aim for 0.8 to 1.0 grams per pound of ideal body weight. This means 130 to 160 grams of protein daily for most people. Spread it across three to four meals. Each meal should contain 30 to 40 grams of protein from sources like lean meat, fish, eggs, Greek yogurt, or plant-based alternatives. Check the complete food list for semaglutide users for specific recommendations.
Fill half your plate with vegetables. Non-starchy vegetables provide volume and nutrients with minimal calories. They also provide fiber, which supports digestive health during semaglutide treatment. This is especially important given the constipation that many users experience.
Manage carbohydrates without eliminating them. Extreme low-carb diets are unnecessary on semaglutide and can worsen fatigue and exercise performance. Instead, focus carbohydrate intake around workouts and choose complex sources like sweet potatoes, brown rice, oats, and legumes.
Do not fear healthy fats. Avocado, olive oil, nuts, and fatty fish provide essential nutrients and help maintain hormonal health during rapid weight loss. But fats are calorically dense (9 calories per gram versus 4 for protein and carbohydrates), so moderate portions matter.
Hydrate aggressively. Aim for half your body weight in ounces of water daily (a 200-pound person should target 100 ounces). Dehydration mimics hunger, impairs metabolic function, and worsens constipation. Many people on semaglutide naturally drink less because they are eating less. Conscious hydration effort is essential.
For a complete, structured approach to eating on semaglutide, the GLP-1 breakfast ideas guide provides specific meal frameworks that align with these principles.
Exercise protocols that accelerate results
The optimal exercise program on semaglutide looks different from a standard weight loss exercise program. Because the medication handles the caloric deficit, exercise serves three primary purposes: preserving muscle, boosting metabolic rate, and improving body composition.
Resistance training (3 times per week): Full-body workouts focusing on compound movements. Squats, deadlifts, presses, rows, and lunges. Progressive overload, meaning gradually increasing weight or repetitions over time. This is non-negotiable for anyone who wants to look good after significant weight loss, not just weigh less.
Zone 2 cardio (3 to 5 times per week): Low-to-moderate intensity cardio where you can hold a conversation. Walking, cycling, swimming, or elliptical training for 30 to 60 minutes. This burns fat directly, improves cardiovascular health, and does not interfere with muscle recovery. Find the best injection site that does not interfere with your exercise routine.
Daily steps (7,000 to 10,000): Outside of formal exercise, staying active throughout the day contributes significantly to total caloric expenditure. A desk worker who hits 3,000 steps naturally needs to consciously add walking to reach the target.
Lifestyle optimization
Sleep 7 to 9 hours per night. Non-negotiable. The weight loss penalty for chronic sleep deprivation is severe.
Manage stress actively. Meditation, therapy, nature exposure, social connection, whatever works for you. Cortisol is a weight loss antagonist.
Limit alcohol to rare occasions. It adds empty calories, impairs judgment, disrupts sleep, and worsens GI side effects.
Take the medication at the optimal time of day and use proper injection technique at the best injection site for consistent absorption.
SeekPeptides members access comprehensive protocol guides, weight-based dosing calculators, and structured programs designed to maximize results from GLP-1 medications. The platform provides personalized approaches that account for the individual factors discussed throughout this guide.
Common mistakes that slow semaglutide weight loss
Understanding what slows results is just as valuable as knowing what speeds them up. These are the most common mistakes that prevent people from achieving their full weight loss potential on semaglutide.
Not eating enough protein
This is the number one mistake. Semaglutide suppresses appetite broadly, affecting all food categories equally. Without conscious effort to prioritize protein, most people default to eating whatever is convenient and palatable in small quantities, which usually means carbohydrate-heavy, protein-light meals.
The consequences compound over time. Muscle loss accelerates. Metabolic rate drops faster than necessary. Body composition suffers. Hair thinning occurs (protein deficiency is a major contributor to GLP-1 related hair loss). And the eventual plateau arrives sooner because less muscle means fewer calories burned at rest.
Track protein intake for at least the first few months. Most people are shocked at how little they actually consume when they start measuring.
Skipping meals entirely
Semaglutide can suppress appetite to the point where eating feels like a chore. Some users skip meals, eat only once a day, or go entire days with minimal intake. This feels productive in the short term but causes long-term damage.
Extreme caloric restriction triggers adaptive thermogenesis, a metabolic slowdown that persists even after normal eating resumes. It also depletes glycogen stores, leading to the flat, drained feeling that makes exercise impossible. And it sends stress signals that elevate cortisol, further promoting fat storage.
Even if you are not hungry, aim for three structured meals containing protein, vegetables, and moderate portions of complex carbohydrates. Think of eating as fueling your body, not satisfying hunger. The medication removed the hunger signal. The nutrition need remains.
Inconsistent medication adherence
Missing doses or taking them at irregular intervals undermines the steady-state drug levels that produce consistent appetite suppression. Semaglutide has a half-life of approximately one week, meaning a missed dose causes a noticeable dip in appetite control.
Set a consistent weekly schedule. Same day, same time. Use phone reminders. Keep your medication stored properly, check semaglutide storage guidelines, to ensure potency. If you travel frequently, review the travel guide for semaglutide to maintain consistency on the road.
Ignoring gastrointestinal side effects
Nausea, constipation, and bloating are not just uncomfortable. They can actively slow weight loss by reducing physical activity, disrupting sleep, and creating aversions to nutritious foods. People who tolerate side effects silently instead of addressing them often eat worse (choosing bland, simple carbohydrates that do not trigger nausea) and move less.
Proactive side effect management matters. Address bloating with probiotics and fiber. Manage constipation with magnesium, hydration, and fiber intake. Combat headaches with adequate hydration and electrolytes. If side effects are severe, discuss dose adjustments with your provider rather than pushing through or abandoning treatment.
Comparing yourself to others
The most psychologically damaging mistake. Social media is filled with dramatic transformation stories: "I lost 40 pounds in three months on semaglutide." These outlier results create unrealistic expectations and make normal, healthy progress feel like failure.
Your results are your results. They are determined by your unique combination of genetics, starting weight, diet, exercise, sleep, stress, hormonal status, and medication response. Comparing your week 6 to someone else week 12 across entirely different circumstances tells you nothing useful. Track your own trend over time. That is the only comparison that matters.
Compounded semaglutide versus brand-name: does it affect speed
With the growth of compounding pharmacies offering semaglutide, many people wonder whether the source affects how quickly they lose weight. The answer requires nuance.
Brand-name semaglutide (Wegovy for weight loss, Ozempic for diabetes) contains the exact FDA-approved formulation. Compounded semaglutide is produced by compounding pharmacies, often at lower cost, using the same active ingredient but in different formulations.
The active molecule is identical in both cases. Semaglutide is semaglutide. However, differences in formulation, concentration accuracy, and quality control can theoretically affect absorption and consistency. Reputable compounding pharmacies like Empower Pharmacy and Olympia Pharmacy maintain strict quality standards that produce results comparable to brand-name products.
Some compounded versions include additional ingredients like vitamin B12, glycine, or niacinamide. These additions may provide ancillary benefits but have not been shown to significantly affect the speed of weight loss from the semaglutide itself.
The key factor is not brand versus compounded. It is consistent dosing, proper storage (check storage duration guidelines), and correct reconstitution if using lyophilized powder. Use a reconstitution calculator to ensure accurate mixing.
Special populations: how speed varies by group
Women versus men
Men typically lose weight faster than women on semaglutide, particularly in the early months. This mirrors the general pattern seen with any weight loss intervention and is driven primarily by differences in lean mass, metabolic rate, and hormonal profiles. Men carry more muscle on average, which means a higher baseline metabolic rate and a larger caloric deficit when appetite decreases.
Women, particularly those dealing with menstrual cycle fluctuations, perimenopause, or menopause, may see more variable week-to-week progress. Scale weight can fluctuate 3 to 5 pounds across a menstrual cycle from water retention alone, masking fat loss progress. The best approach for women is to compare weight at the same point in each cycle rather than tracking weekly changes. Semaglutide can affect menstrual cycles, which may add further variability.
Despite faster initial loss in men, the long-term percentage lost tends to converge between genders by month 12. Women should not be discouraged by slower early progress.
People with type 2 diabetes
Semaglutide was originally developed as a diabetes medication (Ozempic). People with type 2 diabetes tend to lose slightly less weight than those without diabetes, roughly 10 to 12% versus 14 to 15% in clinical trials. This is partly because insulin resistance impairs fat mobilization and partly because the lower doses used for diabetes management (up to 2.0 mg for Ozempic versus 2.4 mg for Wegovy) produce less appetite suppression.
That said, 10% weight loss in a person with type 2 diabetes produces dramatic health benefits: improved blood sugar control, reduced medication needs, lower cardiovascular risk, and in some cases, partial or complete diabetes remission. The speed of weight loss matters less than the metabolic improvements that accompany it.
People with higher BMI
Counterintuitively, people with very high BMI (40 or above) sometimes lose weight more slowly as a percentage of body weight but faster in absolute pounds. A person starting at 350 pounds might lose 30 pounds in three months, a tremendous result, but that represents only 8.6% of starting weight, below the clinical trial average.
For individuals with very high starting weights, the total weight loss journey is longer. The same medication that brings someone from 200 pounds to 170 pounds over 12 months might bring someone from 350 pounds to 290 pounds in the same period. Both results represent successful treatment. The percentage-based targets from clinical trials are less useful at extreme weights, where absolute weight loss and improvement in health markers are more meaningful benchmarks. The BMI requirements for GLP-1 medications guide helps determine eligibility and set appropriate goals.
How semaglutide compares to other weight loss approaches in speed
Context helps. How does semaglutide weight loss speed stack up against other options?
Diet alone (caloric restriction): typical loss of 5 to 10% body weight over 6 months, with high regain rates. Semaglutide roughly doubles this outcome.
Diet plus exercise: typical loss of 7 to 12% over 6 months. Semaglutide with diet and exercise produces results in the 15 to 20% range.
Phentermine: typical loss of 5 to 7% over 3 months (short-term use only). Semaglutide produces greater and more sustained results.
Bariatric surgery (gastric bypass): typical loss of 25 to 35% over 12 to 18 months. Surgery still produces greater average weight loss than semaglutide alone, though the gap is narrowing with newer medications like tirzepatide and retatrutide.
Other weight loss peptides like AOD-9604, MOTS-c, and fat-burning peptide stacks produce modest results compared to GLP-1 receptor agonists. They may serve as complementary tools but do not approach semaglutide efficacy as standalone weight loss agents.
Semaglutide occupies a unique position: more effective than any non-surgical intervention, less invasive and risky than surgery, and sustainable with continued use. For most people, it represents the best balance of efficacy, safety, and convenience available. SeekPeptides offers comprehensive comparison tools and protocol databases that help members evaluate these options based on their individual situations and goals.
Tracking your progress the right way
How you measure progress significantly affects your perception of how fast semaglutide is working. The scale is useful but limited. A comprehensive tracking approach prevents false discouragement and reveals progress that the scale misses.
Scale weight: necessary but not sufficient
Weigh yourself daily at the same time (morning, after using the bathroom, before eating or drinking). Record every number. Then look at the weekly average, not individual days.
Daily weight fluctuates 2 to 5 pounds based on water retention, food volume in the digestive tract, hormonal shifts, and sodium intake. A single day reading tells you almost nothing. The seven-day rolling average tells you everything. If that average is trending downward over weeks, the medication is working regardless of what any single morning weigh-in shows.
Body measurements: the hidden progress tracker
Waist circumference, hip circumference, chest, arms, and thighs tell a story the scale cannot. It is entirely possible to lose inches without losing pounds, especially if you are exercising. The body is simultaneously losing fat and gaining or preserving muscle, which weighs more per unit volume than fat.
Measure the same spots every two weeks using a flexible tape measure. Consistency of measurement location matters more than the exact numbers. Look for trends across multiple sites.
Photos: the most honest metric
Take full-body photos in the same clothing, same lighting, same angle, every two weeks. Your brain adapts to your appearance in the mirror, making gradual changes invisible. Side-by-side photos from week 1 and week 8 reveal changes that you literally cannot see in real time.
Health markers: the most important metric
Blood pressure, fasting glucose, HbA1c, lipid panel, inflammatory markers. These numbers improve with weight loss on semaglutide, often dramatically and sometimes before significant scale changes appear. A person whose blood pressure dropped from 145/92 to 125/80 has achieved a profound health improvement even if the scale only shows 8 pounds lost. Regular blood work monitoring reveals these changes and provides motivation when the scale does not cooperate.
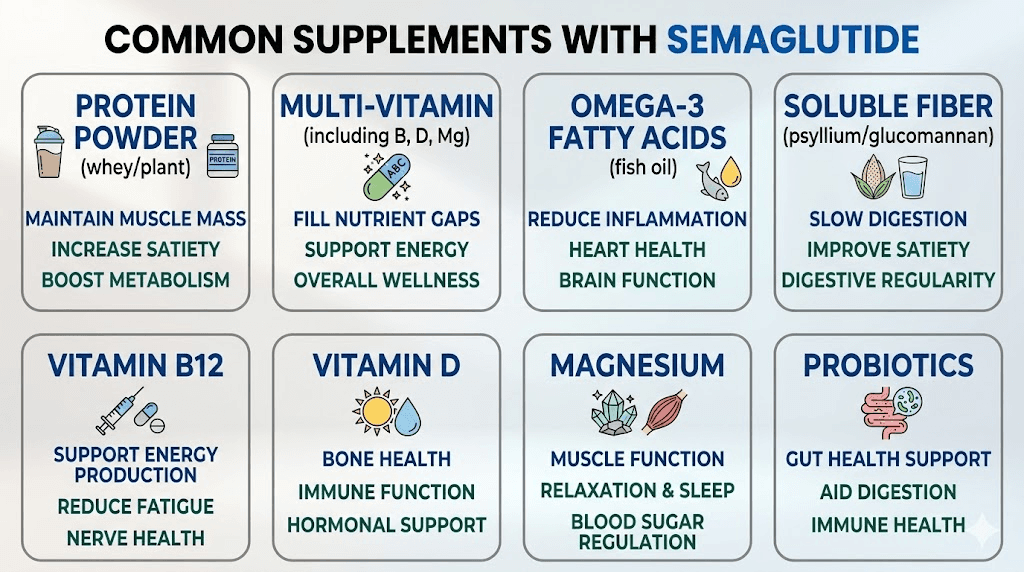
The role of supplements and adjunct therapies
Several supplements are commonly recommended alongside semaglutide to support weight loss speed and overall health during treatment.
Vitamin B12: Semaglutide with B12 is one of the most popular compounded combinations. B12 supports energy metabolism and can help counteract fatigue during caloric restriction. While it does not directly accelerate weight loss, maintaining energy levels supports physical activity, which does.
Protein supplements: Protein shakes designed for GLP-1 users provide a concentrated protein source that is easier to consume when appetite is suppressed. Whey protein, casein, or plant-based protein powders can bridge the gap between actual and target protein intake.
Electrolytes: Reduced food intake often means reduced electrolyte intake. Sodium, potassium, and magnesium supplementation can prevent the weakness, cramping, and dizziness that sometimes accompany semaglutide use.
Fiber: Supplemental fiber (psyllium husk, glucomannan) supports digestive regularity and can help manage the constipation that affects many semaglutide users.
Berberine: Some users combine berberine with semaglutide for additional blood sugar management. The evidence for additive weight loss effects is limited, but the combination appears safe for most people.
L-carnitine: L-carnitine supplementation supports fatty acid transport into mitochondria for energy production. Some evidence suggests it may modestly enhance fat oxidation during caloric restriction, though the effect is small.
For researchers interested in comprehensive peptide protocols that complement GLP-1 medications, SeekPeptides provides evidence-based stacking guides, interaction databases, and dosing protocols. Members access detailed information on combining healing peptides with GLP-1 medications and optimizing overall peptide use alongside weight management.
Your personal semaglutide timeline: putting it all together
Every individual timeline is unique. But here is a realistic framework based on the clinical data and the modifiable factors discussed throughout this guide.
Best-case scenario (optimal diet, exercise, sleep, and medication adherence):
Month 1: 4 to 6% body weight lost
Month 3: 12 to 15% body weight lost
Month 6: 18 to 22% body weight lost
Month 12: 22 to 28% body weight lost
Average scenario (reasonable diet, some exercise, good adherence):
Month 1: 3 to 4% body weight lost
Month 3: 8 to 10% body weight lost
Month 6: 13 to 15% body weight lost
Month 12: 15 to 18% body weight lost
Below-average scenario (no dietary changes, no exercise, inconsistent adherence):
Month 1: 1 to 2% body weight lost
Month 3: 4 to 6% body weight lost
Month 6: 7 to 10% body weight lost
Month 12: 8 to 12% body weight lost
Even the below-average scenario represents clinically meaningful weight loss. But the gap between below-average and optimal is enormous, potentially double the total weight lost. The medication provides the floor. Your choices determine how far above that floor you rise.
Use the peptide calculator to estimate your specific targets based on starting weight and goals. The cost calculator can help estimate the financial commitment for your projected treatment duration.
Frequently asked questions
How much weight can I lose in the first month on semaglutide?
Clinical trial data shows an average of 3.8% body weight lost in the first four weeks. For a 200-pound person, that is roughly 7 to 8 pounds. Results vary widely based on starting weight, diet, activity level, and individual response to the medication. Review the complete first month results breakdown for detailed benchmarks.
Why am I not losing weight on semaglutide after two weeks?
Two weeks is too early to evaluate semaglutide effectiveness. The starting dose of 0.25 mg is sub-therapeutic for weight loss and exists only to allow your body to adjust. Meaningful weight loss typically begins after dose escalation to 0.5 mg or higher. If you are still not seeing results after 8 to 12 weeks at therapeutic doses, check our guide on why semaglutide might not be working.
Does semaglutide work faster with exercise?
Yes. Exercise does not dramatically increase the total pounds lost but significantly improves the quality of weight loss by preserving muscle mass, maintaining metabolic rate, and improving body composition. People who exercise while taking semaglutide tend to reach their goal weight faster and look better at that weight than those who rely on medication alone. You can lose weight without exercise, but results are better with it.
Can I speed up semaglutide weight loss by increasing the dose faster?
Skipping dose escalation steps is not recommended and can backfire. Rapid dose increases cause severe gastrointestinal side effects (nausea, vomiting, diarrhea) that often lead to medication discontinuation. The slow escalation ensures tolerability and sustained use, which produces better long-term results than a fast start followed by quitting due to side effects.
Is semaglutide or tirzepatide faster for weight loss?
Tirzepatide produces faster and greater weight loss on average (22.5% versus 14.9% in clinical trials). However, both medications are effective, and individual response varies. Some people respond better to semaglutide than tirzepatide. Review the complete semaglutide versus tirzepatide comparison for detailed analysis.
How long should I stay on semaglutide for weight loss?
Current evidence supports continued use for weight maintenance. Discontinuation leads to significant weight regain in most cases. Most healthcare providers consider semaglutide a long-term or potentially lifelong medication for weight management, similar to medications for hypertension or diabetes. Read our detailed guide on semaglutide treatment duration for the full picture.
What happens during a semaglutide weight loss plateau?
Weight loss plateaus are normal and expected, typically occurring around month 12 to 15. They happen because your body metabolic needs decrease as you lose weight, eventually matching your reduced caloric intake. Strategies to address plateaus include increasing protein intake, adding resistance training, adjusting caloric intake, and discussing dose changes with your provider. Our semaglutide plateau guide provides a complete troubleshooting framework.
Does the source of semaglutide (compounded vs brand-name) affect weight loss speed?
The active molecule is identical. Reputable compounding pharmacies produce semaglutide that delivers comparable results to brand-name products. The key factors are consistent dosing, proper storage, and accurate reconstitution. Quality varies between pharmacies, so choose established providers like Empower or Olympia with verified testing protocols.
External resources
STEP 5 Trial: Two-Year Effects of Semaglutide in Adults with Overweight or Obesity (Nature Medicine)
Weight Loss Outcomes Associated With Semaglutide Treatment (JAMA Network Open)
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, personalized dosing calculators, and a community of thousands who have navigated these exact questions about semaglutide timing, dosing, and results optimization.
In case I do not see you, good afternoon, good evening, and good night. May your doses stay consistent, your progress stay steady, and your patience stay strong.