Mar 1, 2026

You are wasting up to half of every dose. That is the reality for most people taking GLP-1 drops without proper technique. The liquid sits under the tongue for thirty seconds, gets swallowed too early, and the digestive system destroys what should have been absorbed through the sublingual membrane. Expensive medication, poor results, mounting frustration.
The fix is not a higher dose. It is not switching products. It is technique.
Taking GLP-1 oral drops correctly requires understanding a few critical steps that most providers never explain in enough detail. Where you place the liquid matters. How long you hold it matters. What you eat beforehand, what you drink afterward, even your body position during administration, all of these factors determine whether 10% or 40% of the active compound actually reaches your bloodstream. That gap between 10% and 40% is the difference between seeing meaningful results and wondering why the drops are not working. This guide covers every detail of proper sublingual peptide administration, from preparation through absorption, with troubleshooting for the problems most people encounter along the way. Whether you are using semaglutide, tirzepatide drops, or a multi-compound GLP-1 oral liquid, the technique principles remain the same.
Why proper technique determines whether GLP-1 drops work
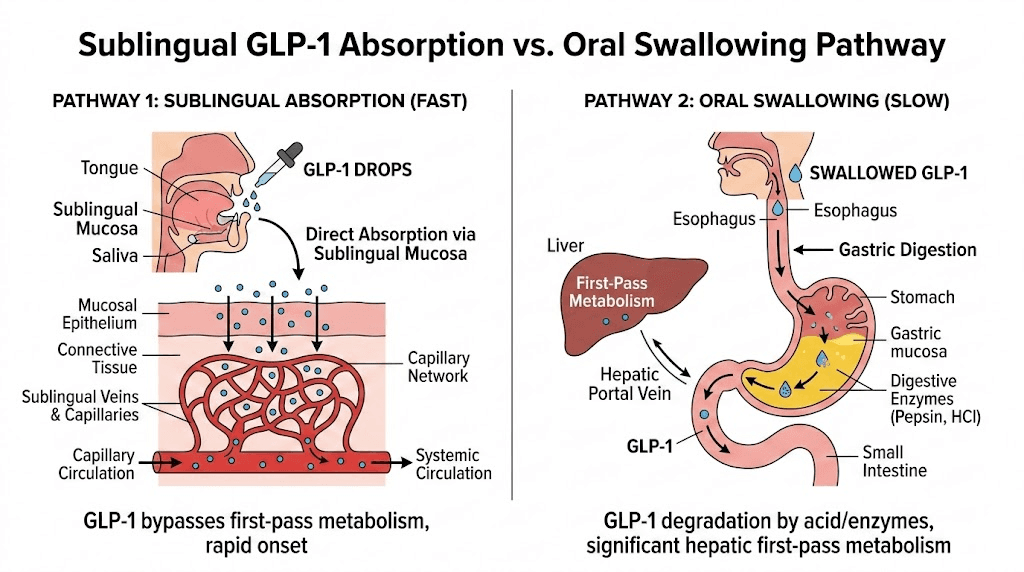
Here is what most people do not understand about sublingual medication. The tissue under your tongue contains a dense network of capillaries sitting just beneath a thin layer of mucosa. When a compound contacts this tissue and stays there long enough, it passes directly into the bloodstream without going through the stomach or liver first. This is called first-pass bypass, and it is the entire reason sublingual semaglutide and sublingual tirzepatide exist as alternatives to injections.
But here is the problem. Absorption only works when conditions are right.
Swallow too soon, and the peptide enters your digestive system where stomach acid breaks down roughly 98-99% of the active compound. The bioavailability of orally swallowed GLP-1 peptides sits between 0.4% and 1% without special absorption enhancers. Compare that to sublingual delivery, which research suggests can achieve bioavailability potentially reaching 40% under optimal conditions. That is a forty-fold difference based purely on technique.
Think about what that means in practical terms. Two people taking the exact same compounded semaglutide drops. Same concentration. Same dose volume. One person holds the liquid properly for several minutes on an empty stomach. The other rushes through administration, swallows after sixty seconds, and eats breakfast ten minutes later. Person one absorbs enough active compound to suppress appetite, reduce food noise, and drive meaningful weight loss results. Person two wonders why the medication does not seem to do anything.
The injectable forms of GLP-1 medications deliver nearly 100% of the active compound directly into subcutaneous tissue. No technique required beyond basic injection site selection. Drops demand more from you. They require understanding and consistency. But when done correctly, sublingual administration offers a needle-free alternative that many people prefer, and the results can be genuinely comparable when absorption is optimized.
Understanding how sublingual absorption actually works
Before diving into the step-by-step process, understanding the mechanism helps you appreciate why each instruction matters. Skip this section if you just want the protocol. But knowing the science makes the technique intuitive rather than memorized.
The sublingual membrane is different from the rest of your mouth
The floor of the mouth, directly under the tongue, has unique properties compared to other oral tissues. The mucosa here is thinner. The blood supply is more abundant. The permeability to water-soluble compounds is higher than anywhere else in the oral cavity. These three factors combine to create the most efficient absorption surface available outside of injection.
Two major blood vessels run directly beneath this tissue, the sublingual vein and the sublingual artery. Compounds that cross the mucosal barrier enter these vessels and travel through the systemic circulation without first passing through the gastrointestinal tract or liver. This direct entry means the compound avoids enzymatic degradation in the gut and first-pass metabolism in the liver, both of which destroy the vast majority of peptide-based medications when swallowed.
Why peptides are particularly challenging for sublingual delivery
Peptides like semaglutide and tirzepatide are large molecules compared to many sublingual drugs. Nitroglycerin tablets dissolve under the tongue in seconds because the molecules are tiny. GLP-1 receptor agonists are complex peptide chains with much higher molecular weights, which means they cross the sublingual membrane more slowly and less completely.
This is why hold time matters so much. A nitroglycerin tablet might absorb in 60 seconds. GLP-1 drops need several minutes of continuous contact with the sublingual tissue to achieve meaningful absorption. Every additional minute the liquid stays in contact with that membrane increases the percentage of active compound entering your bloodstream.
Saliva production is the enemy here. Your mouth naturally produces saliva in response to anything placed under the tongue. This saliva dilutes the medication, reduces the concentration gradient driving absorption, and triggers the swallowing reflex. Managing saliva is one of the most important and least discussed aspects of proper sublingual peptide technique.
Factors that increase absorption
Research on sublingual drug delivery identifies several factors that improve how much medication crosses the mucosal barrier. An empty stomach reduces competing absorption processes and keeps blood flow focused on the oral tissues. Higher concentration solutions provide a stronger diffusion gradient. Longer hold times allow more compound to cross. Proper placement directly over the richest capillary beds maximizes contact with blood vessels. And pH of the solution affects molecular charge, which influences how easily the compound passes through cell membranes.
Compounding pharmacies formulate compounded GLP-1 drops with these factors in mind. Many add permeation enhancers, adjust pH levels, and use specific concentrations designed to optimize sublingual absorption. Your job is to handle the factors within your control, which are placement, timing, hold duration, and pre and post-dose conditions.
Step by step guide to taking GLP-1 drops correctly
Follow these instructions precisely. Each step exists for a specific reason related to absorption science. Skipping or rushing any step reduces how much medication your body actually uses.
Step 1: Prepare your mouth
Start with a clean mouth. Brush your teeth at least 30 minutes before taking drops, not immediately before. Fresh brushing can create micro-abrasions in the oral tissue that alter absorption patterns, and toothpaste residue interferes with the medication formulation. If you need to brush closer to dosing time, rinse thoroughly with plain water afterward and wait at least 10 minutes.
Your mouth should be free of food, gum, candy, and anything flavored. Even a recent cup of coffee or tea changes the pH environment under your tongue. Plain water is fine up to a few minutes before dosing, but do not have a mouthful of water when you administer the drops.
Step 2: Prepare the medication
Remove the GLP-1 drops from the refrigerator. Most compounded GLP-1 medications require refrigeration and should be stored between 36-46 degrees Fahrenheit (2-8 degrees Celsius). Cold medication can feel uncomfortable under the tongue and may trigger an immediate swallowing response in some people. Holding the bottle in your hand for 1-2 minutes before dosing takes the edge off the cold without compromising stability.
Gently roll the bottle between your palms 5-10 times. Do not shake vigorously. Rolling ensures even distribution of the active compound throughout the solution without creating bubbles that affect dose accuracy. Some formulations settle slightly between doses, so this step ensures consistency.
Draw the prescribed amount into the oral syringe provided by your pharmacy. Check the measurement carefully. GLP-1 dosing with compounded formulations uses volume measurements (milliliters) rather than the milligram-based dosing you might see for FDA-approved formulations like Ozempic. The concentration varies between pharmacies, so the same milligram dose might require very different volumes depending on your specific product.
Step 3: Position your body
Sit upright. Do not recline. Do not lie down.
An upright position keeps the liquid pooled under your tongue rather than running toward your throat. People who take drops while lying in bed or reclining on a couch almost always swallow the medication prematurely because gravity pulls the liquid backward. Sit in a chair with your head level or slightly tilted forward.
Step 4: Administer the drops
Lift your tongue toward the roof of your mouth. Place the tip of the oral syringe under the tongue, slightly off-center. Slowly dispense the liquid into the sublingual space. The goal is to deposit the medication in the depression directly under the tongue where the tissue is thinnest and the blood supply is richest.
Do not squirt the liquid forcefully. A gentle, steady push on the syringe plunger creates a controlled deposit. Forceful squirting sprays the liquid across the floor of the mouth, reducing the concentrated contact needed for optimal absorption.
Lower your tongue back down gently over the liquid. Do not press hard. The tongue should rest naturally, keeping the liquid trapped in the sublingual space without squeezing it out to the sides or back of the mouth.
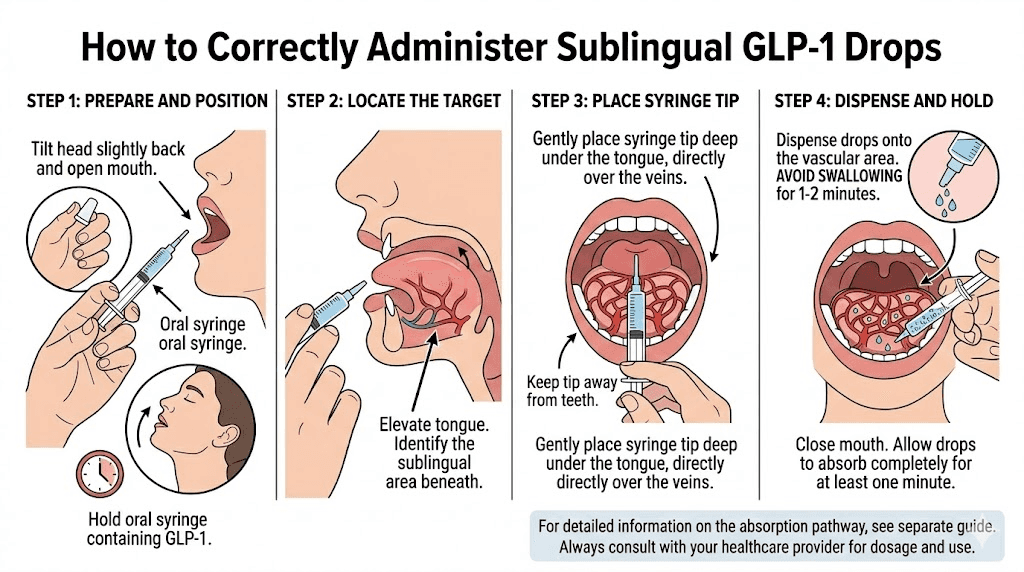
Step 5: Hold for the full duration
This is the most critical step. And it is where most people fail.
Hold the liquid under your tongue for a minimum of 2 minutes. Three to five minutes is better. Some pharmacies and providers recommend holding for up to 10 minutes for maximum absorption. The longer the medication stays in contact with the sublingual membrane, the more compound crosses into your bloodstream.
During the hold period, keep your mouth closed. Do not talk. Do not chew. Do not move your tongue around. Any movement shifts the liquid away from the optimal absorption zone and mixes it with saliva, diluting the concentration. Sit still, breathe through your nose, and let the medication do its work.
Saliva will accumulate. This is normal and unavoidable. Resist the urge to swallow for as long as possible. When you absolutely must swallow, do so gently and try to keep the area directly under the tongue undisturbed. Some people find it helpful to set a timer on their phone before starting so they do not have to guess when enough time has passed.
Step 6: Swish and swallow
After holding for the full duration, gently swish the remaining liquid around your mouth for about 15-30 seconds. This allows any medication still in your oral cavity to make contact with the buccal membranes along your cheeks and gums, which also have some absorptive capacity. Then swallow normally.
The swish step recovers some of the compound that mixed with saliva during the hold period. While buccal absorption is less efficient than sublingual, it is still better than sending the compound straight to the stomach. Every bit of additional absorption improves the effective dose you receive.
Step 7: Wait before eating or drinking
Do not eat, drink, brush your teeth, or use mouthwash for at least 30 minutes after dosing. This waiting period allows the medication that has been absorbed into the mucosal tissue to fully enter the bloodstream. Eating or drinking too soon can wash away compound that was in the process of absorbing, and food in the stomach redirects blood flow away from the oral tissues toward the digestive system.
Water is acceptable after the 30-minute mark. Food should wait even longer if possible, with many providers recommending a 45-60 minute fasting window after dosing for optimal results.
Best time of day to take GLP-1 drops
Timing affects both absorption and how well the medication manages appetite throughout the day. The research and clinical experience point toward morning dosing for most people, but the reasoning involves more than habit.
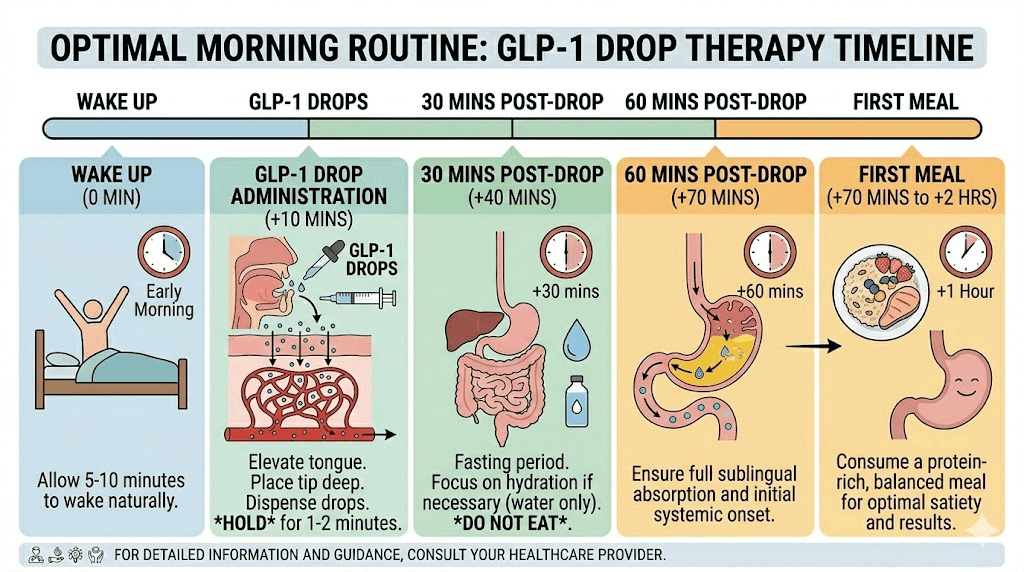
Why morning dosing works best
After sleeping all night, your stomach is naturally empty. This is the longest fasting period most people experience daily, and it creates ideal conditions for sublingual absorption. No food competing for blood flow. No digestive processes pulling resources away from the oral mucosa. No stomach contents that might cause nausea when combined with a GLP-1 agonist.
Morning administration also aligns the appetite suppression effects with the times when most people struggle most with food cravings. The compound reaches peak blood levels within 1-3 hours of sublingual administration, which means the strongest appetite control kicks in right around lunchtime, precisely when food decisions tend to get difficult for most people managing their diet on GLP-1 medications.
Taking drops first thing after waking creates a consistent routine. Consistency matters enormously with GLP-1 therapy because steady blood levels produce better results than erratic dosing. Missing doses or varying the time by several hours each day creates peaks and valleys in blood concentration that reduce overall effectiveness and can worsen side effects like nausea.
Alternative timing for people who cannot dose in the morning
If morning dosing is not possible, the next best option is taking drops at least 2 hours after your last meal, ideally in the evening before bed. The stomach needs to be reasonably empty. A light snack 2 hours prior is acceptable. A heavy dinner 90 minutes prior is not.
Some people split into twice-daily dosing under provider guidance, taking half the dose in the morning and half in the evening. This maintains more stable blood levels throughout the 24-hour period and may reduce GI side effects compared to a single larger dose. However, twice-daily dosing doubles the number of times you need to perform the complete sublingual technique, which some people find inconvenient.
Whatever time you choose, the critical requirement is an empty stomach. The best time to take your dose is always the time that allows for the longest pre-dose fast and the longest post-dose fast you can consistently maintain.
Common mistakes that reduce GLP-1 drop effectiveness
After working through forums, provider feedback, and pharmacy guidance, these are the mistakes that come up again and again. Fix any of these and you will likely notice a difference in how well the drops work.
Mistake 1: Not holding long enough
The single most common error. Sixty seconds feels like an eternity when you have liquid under your tongue, saliva building up, and a busy morning ahead. But sixty seconds is not enough. Research on sublingual drug absorption shows that peak absorption rates occur between minutes 2 and 5. Cutting the hold time short means cutting the absorbed dose short.
The fix is simple. Set a timer. Put your phone in front of you with a countdown running. Three minutes minimum. Five minutes if you can manage it. After a few days, the routine becomes automatic and the hold period feels less awkward.
Mistake 2: Taking drops with food in the stomach
Eating within 30 minutes before taking drops compromises absorption in two ways. First, digestion redirects blood flow from the oral mucosa to the GI tract, reducing the efficiency of sublingual uptake. Second, any food particles remaining in the mouth create a physical barrier between the medication and the mucosal surface.
The foods to avoid are everything, at least for the 30-minute window before dosing. Even coffee counts. Even a glass of juice. True fasting means nothing but plain water, and ideally nothing at all for the last 10 minutes before administration.
Mistake 3: Talking during the hold period
Talking moves the tongue. Moving the tongue shifts the liquid away from the sublingual absorption zone and accelerates mixing with saliva. One brief response to a question can redistribute the entire dose to areas of the mouth with much lower absorptive capacity.
Inform household members about your dosing routine. If you take drops in the morning, let family know you will be unavailable for conversation for a few minutes. This sounds excessive, but the impact on absorption is real. Even mouthing words shifts the tongue enough to matter.
Mistake 4: Lying down while taking drops
Gravity is not your friend when lying flat. The liquid pools toward the back of the throat instead of staying concentrated under the tongue. The swallowing reflex triggers earlier. And the overall contact time with the sublingual membrane decreases significantly.
Always sit upright. If you prefer to take drops in bed, sit up fully first, prop yourself with pillows if needed, and maintain the upright position for the entire hold period.
Mistake 5: Brushing teeth immediately before or after
Toothpaste contains surfactants, flavoring agents, and abrasives that alter the oral environment in ways that interfere with absorption. The menthol and sodium lauryl sulfate in most toothpastes can affect mucosal permeability. The abrasive action creates micro-inflammation that changes how the tissue handles absorption.
Brush at least 30 minutes before dosing. After dosing, wait 30 minutes before brushing. Morning routine adjustment: brush teeth, get ready, then take drops right before leaving for work or starting your day.
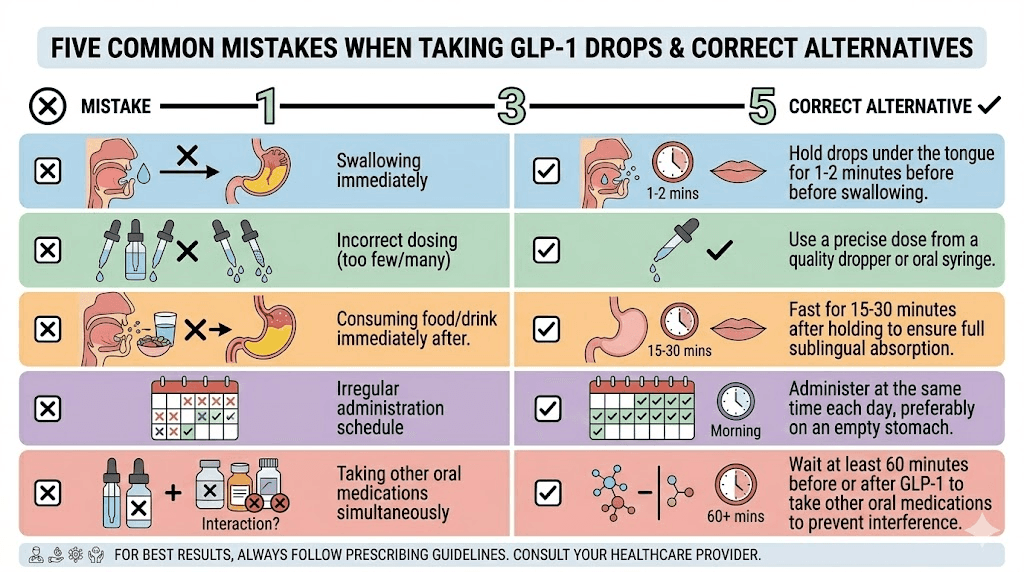
Mistake 6: Inconsistent daily timing
Taking drops at 7 AM one day, noon the next, and 9 PM the day after creates wildly inconsistent blood levels. GLP-1 oral liquid dosing frequency works best when the timing is consistent to within about an hour each day. This consistency allows your body to establish a predictable rhythm of peak and trough levels that produces more stable appetite suppression and fewer side effects like fatigue.
Mistake 7: Storing drops improperly
Compounded GLP-1 drops are sensitive to temperature. Leaving the bottle on the bathroom counter, in a warm car, or near a window can degrade the active compound well before the expiration date. Proper storage in the refrigerator at 36-46 degrees Fahrenheit maintains potency throughout the labeled shelf life, which is typically 30-90 days depending on the compounding pharmacy.
If your drops have been left out at room temperature, the compound may have lost potency. Some degradation occurs gradually, while exposure to heat above 77 degrees Fahrenheit can cause rapid breakdown. When in doubt about temperature exposure, contact your pharmacy about whether the medication is still viable. Using degraded drops means you are taking a lower effective dose than intended, which explains sudden loss of appetite control or weight loss plateaus.
Maximizing absorption from every dose
Beyond avoiding mistakes, several evidence-based strategies can improve how much active compound reaches your bloodstream from each dose. These are the techniques that separate adequate results from optimal results.
The dry mouth technique
Before administering drops, try to reduce the amount of saliva in your mouth. Swallow any existing saliva. Some people find it helpful to gently blot under the tongue with a clean tissue before placing the medication. A drier sublingual environment means the medication stays concentrated rather than immediately diluting with saliva.
Do not use mouth-drying agents like alcohol-based mouthwash. These damage the mucosal tissue and reduce absorption. The goal is a naturally dry mouth, not a chemically altered one.
Placement precision matters
Not all areas under the tongue are equal. The most efficient absorption zone is the central depression on the floor of the mouth, directly under the tip to mid-body of the tongue. Placing drops too far forward, near the front teeth, puts them in contact with less vascular tissue. Placing drops too far back triggers the swallowing reflex and sends the liquid toward the throat.
Aim for the sweet spot. About one inch behind the front teeth, centered between the left and right sides of the sublingual space. With practice, you will be able to position the syringe tip precisely without needing a mirror.
Concentration and formulation considerations
Higher concentration solutions generally absorb better because they maintain a stronger concentration gradient across the mucosal membrane. If your pharmacy offers the same dose in a smaller volume at higher concentration, the smaller volume option typically provides better absorption because the medication is less diluted by saliva.
Ask your compounding pharmacy about the formulation specifics. Some pharmacies add permeation enhancers that improve absorption. Others adjust the pH of the solution to optimize the balance between compound stability and mucosal permeability. Understanding what is in your specific formulation helps you work with it rather than against it. Use the semaglutide dosage calculator or general peptide calculator to verify your dose is within the expected range for your body weight and goals.
The extended hold strategy
If standard hold times of 2-3 minutes produce mediocre results, gradually extend to 5 minutes, then 7, then 10. The absorption curve does not plateau instantly after 2 minutes. It continues, albeit at a declining rate, for much longer. People who hold for 5-10 minutes consistently report better results than those who rush through a 90-second hold.
Make the hold time productive. Use it for morning meditation, reading on your phone (without talking), or simply sitting quietly. Reframe the hold period from an inconvenience to a deliberate pause in your morning routine. Those few minutes of stillness might be the calmest part of your day.
GLP-1 drops vs injections: what to expect from each delivery method
Understanding the differences between injectable and oral peptide delivery helps set realistic expectations and makes it easier to evaluate whether drops are working at the level they should.
Bioavailability comparison
The numbers tell the story clearly.
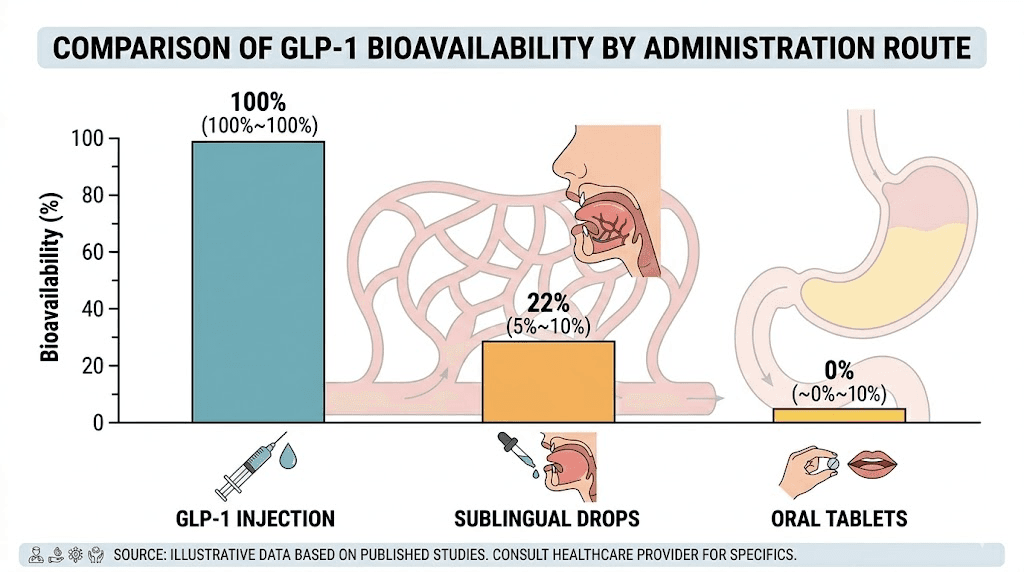
Subcutaneous injection delivers approximately 100% of the administered dose into systemic circulation. When you inject 0.5 mg of semaglutide, roughly 0.5 mg reaches your bloodstream. The math is straightforward, and the results are predictable.
Sublingual drops deliver an estimated 5-40% of the administered dose, depending on technique, formulation, and individual physiology. The wide range reflects how much technique matters. Optimal technique with a well-formulated product might achieve 30-40%. Poor technique might deliver as little as 5-10%, which is barely more effective than swallowing the medication outright.
Oral tablets like Rybelsus (the FDA-approved oral semaglutide) use a special compound called SNAC to protect against stomach acid, yet still achieve only 0.4-1% bioavailability. This is why Rybelsus requires a 14 mg tablet to deliver the equivalent of a 0.5 mg injection. Sublingual drops sidestep this problem by avoiding the stomach entirely, at least when taken correctly.
Onset and duration differences
Injectable semaglutide reaches peak levels within 1-3 days of injection and maintains therapeutic levels for roughly 7 days, which is why it is dosed weekly. Sublingual drops reach peak levels within 1-3 hours of administration but clear the system faster, which is why they are typically dosed daily.
The daily dosing of drops means more consistent blood levels throughout the week compared to the peak-and-trough pattern of weekly injections. Some people actually prefer this steadier exposure because it produces more consistent appetite suppression without the "wearing off" feeling that some experience toward the end of their injection week.
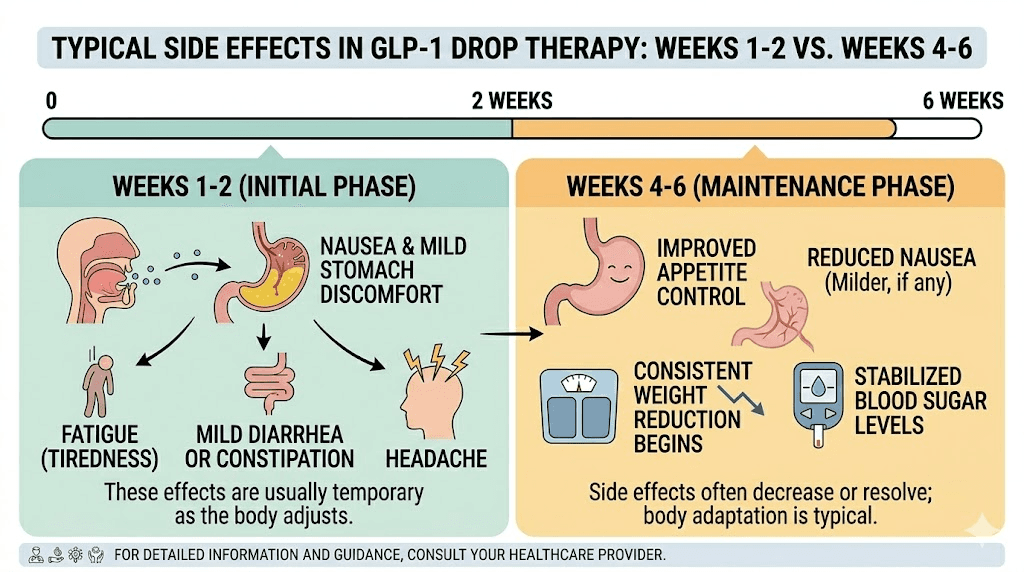
Side effect profile differences
Sublingual drops tend to produce milder GI side effects compared to injections, particularly during the dose escalation phase. The lower bioavailability actually works in favor here, as the body receives the active compound more gradually throughout the day rather than in a single bolus that can overwhelm GLP-1 receptors in the gut.
Common side effects from drops include mild constipation, occasional bloating, and reduced appetite that some people experience as more gradual than with injections. Severe nausea, vomiting, and dizziness are less commonly reported with sublingual formulations, though they can still occur, especially at higher doses or when escalating too quickly.
If you have been on injectable tirzepatide or semaglutide and are switching to drops, expect a transition period while your body adjusts to the different absorption pattern and potentially different effective dose. The dose conversion between formulations is not straightforward because bioavailability differs between delivery methods.
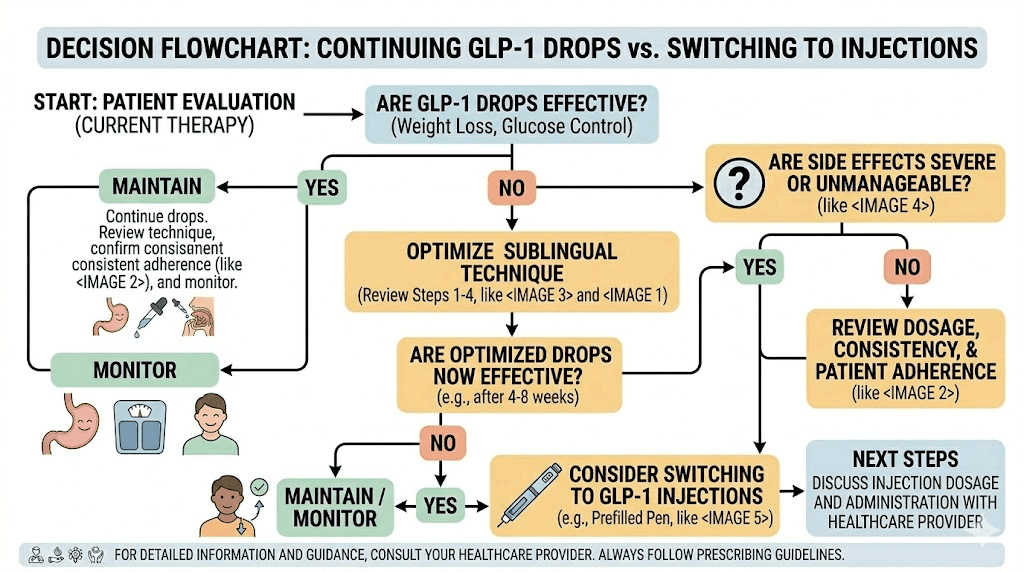
When to consider switching delivery methods
Drops work well for people who are needle-averse, travel frequently, or prefer the convenience of oral administration. But drops are not the right choice for everyone. If you have been using drops with perfect technique for 6-8 weeks and results are significantly below expectations, the bioavailability limitations of sublingual delivery may be the bottleneck.
Conversely, if you are on injections but struggling with side effects, switching to drops might provide adequate results with better tolerability. The drops versus injection decision involves weighing convenience, cost, needle tolerance, and the willingness to maintain meticulous sublingual technique every single day.
Different types of GLP-1 drops and how each one works
Not all GLP-1 drops are identical. Different active compounds and combination products require slightly different approaches and have different characteristics you should understand.
Semaglutide sublingual drops
Semaglutide drops are the most widely available compounded sublingual GLP-1 formulation. Semaglutide is a GLP-1 receptor agonist that mimics the natural incretin hormone to reduce appetite, slow gastric emptying, and improve blood sugar regulation. The sublingual version typically comes in concentrations ranging from 1 mg/mL to 5 mg/mL, with daily doses usually starting at 0.5-1 mg and escalating over several weeks.
The complete semaglutide sublingual guide covers dosing schedules in detail, but the administration technique remains exactly what is described in this article. Semaglutide has a relatively long half-life even in sublingual form, which provides some forgiveness for timing inconsistencies, though optimal results still come from consistent daily dosing.
Many compounded semaglutide drops include additional compounds like vitamin B12, glycine, or L-carnitine to support energy levels and metabolism during weight loss. These additions do not change the sublingual administration technique but may slightly alter the taste of the drops.
Tirzepatide sublingual drops
Tirzepatide drops represent the dual-agonist approach, targeting both GLP-1 and GIP receptors simultaneously. This dual action often produces more pronounced appetite suppression and potentially greater weight loss results compared to GLP-1-only medications. The tirzepatide sublingual dosage chart shows typical escalation patterns for the compounded sublingual form.
Administration technique for tirzepatide drops is identical to semaglutide drops. The same principles of placement, hold time, empty stomach, and post-dose fasting apply equally. Some users report that tirzepatide drops have a slightly different taste profile, but this varies between pharmacies and does not affect how you take them.
Tirzepatide formulations often include glycine and B12 or niacinamide as supporting compounds. The starting dose for compounded tirzepatide sublingual drops is typically lower than the injection equivalent, with gradual escalation based on tolerance and response.
Multi-compound GLP-1 oral liquids
Products like 6-in-1 GLP-1 oral liquids combine multiple active compounds in a single sublingual formulation. These may include a GLP-1 agonist plus supporting ingredients like amino acids, B vitamins, and metabolic cofactors designed to work synergistically.
Multi-compound formulations sometimes have higher total volume per dose because they contain more ingredients. Larger volumes can be slightly more challenging for sublingual administration because there is more liquid to hold in a relatively small space. If your dose volume exceeds 1 mL, consider splitting the dose into two sequential administrations, holding the first portion for 2-3 minutes before adding the second. This keeps the concentration higher for each portion rather than diluting a larger volume with saliva all at once.
ODT versus liquid drops
Some compounding pharmacies offer GLP-1 in orally dissolving tablet (ODT) form rather than liquid drops. Tirzepatide ODT and similar products dissolve under the tongue rather than being administered as liquid. The technique principles remain similar, with placement under the tongue and extended hold time, but the experience feels different because you are waiting for a tablet to dissolve rather than holding a liquid.
ODTs may be easier for some people because there is no syringe measurement involved and the tablet stays in position more naturally. However, the dissolution time adds to the overall absorption period. Wait until the tablet has fully dissolved, then continue holding for an additional 1-2 minutes before swishing and swallowing.
Managing side effects from GLP-1 oral liquid
Side effects from sublingual GLP-1 drops tend to be milder than injection versions, but they still occur. Understanding what to expect and how to manage each symptom makes the experience significantly more manageable.
Nausea
The most commonly reported side effect across all GLP-1 medications, including drops. Sublingual nausea tends to be milder than injection-related nausea because the medication absorbs more gradually. If nausea occurs, it typically appears within the first 1-2 hours after dosing and resolves within a few hours.
Management strategies include starting at the lowest prescribed dose and escalating slowly, taking drops in the morning when the stomach is empty (counterintuitively, an empty stomach often produces less nausea than taking drops after eating), and keeping bland foods available for your first meal after the fasting window. Ginger tea, peppermint, and small sips of water can help manage mild nausea. If nausea is severe or persistent, contact your provider about adjusting the dose or escalation schedule.
Taste and oral discomfort
Some GLP-1 drops have a distinctive taste that ranges from mildly unpleasant to tolerable depending on the formulation. Many pharmacies add peppermint flavoring to improve the experience. If the taste is problematic, do not try to mask it with food or drink before the 30-minute post-dose fasting window. Instead, ask your pharmacy if alternative flavoring options are available.
Mild burning or tingling under the tongue is normal and indicates the medication is in contact with the mucosal tissue. This sensation typically fades within a few minutes and does not indicate a problem. If you experience significant pain, swelling, or persistent irritation, discontinue use and contact your provider.
Reduced appetite and eating too little
Appetite suppression is the intended effect, but some people suppress their appetite so effectively that they struggle to eat enough to meet basic nutritional needs. This is particularly concerning during the first few weeks on a new dose when the effect can be surprisingly strong.
Plan your meals in advance. Even if you are not hungry, aim for adequate protein intake (at least 0.6-0.8 grams per pound of body weight) to prevent muscle loss and hair thinning that can accompany rapid weight loss. The tirzepatide diet plan and semaglutide diet plan resources provide meal frameworks designed for people managing reduced appetite on GLP-1 therapy.
Fatigue and energy changes
Some people experience fatigue on GLP-1 medications, especially during the first few weeks. This often relates to reduced caloric intake rather than a direct drug effect. If your appetite drops dramatically and you cut calories too aggressively, fatigue is the natural result. Taking supplements like B vitamins, magnesium, and iron alongside adequate nutrition helps maintain energy levels.
Interestingly, many people report improved energy after the initial adjustment period. Once the body adapts to the medication and you establish a consistent eating pattern with adequate nutrition, the energy improvements from reduced inflammation and better blood sugar regulation often outweigh any initial fatigue.
Storing GLP-1 drops properly to maintain potency
Poor storage destroys medication potency before you ever take a dose. All the perfect technique in the world means nothing if the active compound has degraded.
Temperature requirements
Most compounded GLP-1 drops require refrigeration at 36-46 degrees Fahrenheit (2-8 degrees Celsius). This is standard refrigerator temperature. Store the bottle on a shelf inside the refrigerator, not in the door where temperature fluctuates with opening and closing. Definitely not in the freezer. Freezing can damage the formulation irreversibly.
Temperature excursions above 77 degrees Fahrenheit cause accelerated degradation of the peptide. If your drops arrive warm from shipping, contact the pharmacy. If you accidentally leave them out on the counter overnight in a cool room (below 77F), they are probably fine. If they sat in a hot car for several hours, they may not be.
Shelf life and expiration
Compounded GLP-1 drops typically have a beyond-use date of 30-90 days from the date of compounding, depending on the pharmacy and formulation. This is shorter than FDA-approved products because compounded formulations undergo less stability testing. The date printed on your bottle is the date you should stop using that bottle, regardless of how much liquid remains.
Expired semaglutide does not become dangerous, but it loses potency over time. Using expired drops means taking an unknown, lower effective dose. If you notice that drops that previously worked well seem to be losing effectiveness toward the end of the bottle, degradation may be the cause.
Travel considerations
Traveling with GLP-1 drops requires maintaining the cold chain. Use an insulated bag with ice packs for trips longer than a few hours. For air travel, drops in their original pharmacy bottle are generally permitted in carry-on luggage. TSA allows liquid medications in quantities exceeding the 3.4-ounce limit when declared at the security checkpoint.
Hotel room refrigerators work adequately for short trips. For longer travel, consider requesting a pharmacy supply to be shipped to your destination rather than transporting medication in variable temperature conditions.
Dose escalation and what to expect at each level
GLP-1 therapy always begins with a lower dose and escalates over weeks to months. This applies equally to drops and injections. Understanding the escalation process prevents two common mistakes: escalating too quickly and not escalating when you should.
Typical escalation for semaglutide drops
Most providers start semaglutide sublingual drops at 0.5-1 mg daily. After 2-4 weeks of good tolerance, the dose increases to 1-1.5 mg daily. Further escalation to 2-2.4 mg daily follows after another 2-4 weeks if needed. The specific schedule varies by provider and pharmacy, and the compounded semaglutide dose chart provides typical progression patterns.
Do not increase your dose faster than your provider recommends. Each escalation allows your GLP-1 receptors to adapt to increased stimulation. Jumping to a high dose without the adaptation period dramatically increases the risk of severe nausea, vomiting, and diarrhea.
Typical escalation for tirzepatide drops
Tirzepatide escalation follows a similar pattern but with different milligram targets. The tirzepatide dosing guide and compound tirzepatide dosage chart outline the standard progression from starting dose through maintenance dose. Because tirzepatide acts on both GLP-1 and GIP receptors, many people find they need a lower maximum dose compared to semaglutide-only formulations to achieve similar results.
Signs you need a dose adjustment
Several indicators suggest the current dose needs to change. Persistent hunger throughout the day, no change in food noise or cravings, and no weight loss after 4 or more weeks on a stable dose all suggest the dose is too low or absorption is insufficient. On the other hand, inability to eat even small meals, severe nausea lasting more than a few days after dose escalation, and significant dizziness or lightheadedness suggest the dose is too high.
Before adjusting the dose upward, first optimize your technique using everything in this guide. Many people who think they need a higher dose actually need better absorption from the dose they are already taking. Perfect technique at a moderate dose often outperforms sloppy technique at a higher dose.
Tracking your progress with GLP-1 drops
Measuring results helps determine whether your technique and dosing are optimized, or whether adjustments are needed.
What to track
Weight alone is an incomplete measure. Track body weight, yes, but also track waist circumference, how your clothes fit, energy levels, appetite intensity on a 1-10 scale, food noise (the constant mental chatter about food), and any side effects. These secondary markers often change before the scale moves, providing early confirmation that the drops are working.
A simple weekly log works. Same time, same conditions, same scale. Weigh yourself in the morning after using the bathroom, before eating or drinking. Weekly measurements smooth out the daily fluctuations that make daily weigh-ins frustrating and misleading. GLP-1 progress trackers and weight loss calculators can help visualize your trajectory over time.
Realistic timelines for results
Do not expect injectable-level speed from sublingual drops. The lower bioavailability means the effective dose reaching your system is lower than the equivalent injection dose. Meaningful appetite suppression typically appears within the first 1-2 weeks. Measurable weight loss usually becomes apparent by weeks 3-4. Significant results accumulate over months, not days.
The appetite suppression timeline differs between individuals based on genetics, metabolic rate, and yes, sublingual technique quality. Some people feel the effects within the first dose. Others need several days of consistent dosing before noticing changes. Both responses are normal.
If you reach 6-8 weeks on an adequate dose with proper technique and see minimal results, the conversation with your provider should include discussing whether sublingual delivery is providing sufficient bioavailability for your needs, or whether transitioning to injectable administration might be more effective.
Special considerations for specific populations
Not everyone approaches GLP-1 drops from the same starting point. These situations require additional attention to technique and expectations.
Switching from injections to drops
The most common reason for switching is needle fatigue or preference for oral administration. When making this transition, understand that you may need a higher milligram dose of the sublingual formulation to achieve the same blood levels you had on injections. Your provider should help calculate an appropriate starting sublingual dose based on your previous injection dose, accounting for the bioavailability difference.
There is usually a transition period of 1-2 weeks where appetite control may feel weaker than what you experienced on injections. This does not necessarily mean the drops are not working. It often means your body is adjusting to the different pharmacokinetic profile of daily sublingual versus weekly injection dosing. Give it time before concluding the drops are insufficient.
Switching between GLP-1 compounds
Switching from tirzepatide to semaglutide or vice versa while also changing from injection to drops introduces two variables at once. When possible, change one variable at a time. Switch the delivery method first, stabilize, then consider switching the compound. Or switch the compound first via injection, stabilize, then transition to drops.
Combining drops with other medications
Some people take GLP-1 drops alongside other medications that also benefit from empty stomach administration. Thyroid medications, for example, are commonly taken first thing in the morning on an empty stomach. If you take both, consult with your provider about timing. One approach is to take the thyroid medication first, wait 30-60 minutes, then take GLP-1 drops, then wait another 30 minutes before eating.
Interactions between oral medications and sublingual compounds are generally minimal because they use different absorption pathways. However, anything that alters saliva production, oral pH, or blood flow to the oral mucosa could theoretically affect GLP-1 drop absorption. Report all medications to your provider so they can advise on timing and potential interactions.
SeekPeptides provides comprehensive guides on combining GLP-1 therapy with supporting compounds like glycine and B12 blends, berberine, and metformin to help members navigate complex protocols safely.
Alcohol, caffeine, and GLP-1 drops: what you need to know
Two of the most common questions about sublingual GLP-1 therapy involve alcohol and caffeine. Both substances interact with the medication in ways worth understanding.
Alcohol and GLP-1 drops
Drinking alcohol while on semaglutide or tirzepatide is a topic that generates significant debate. The direct interaction between alcohol and sublingual GLP-1 drops is minimal from an absorption standpoint, provided you are not drinking during the pre-dose fasting window or the post-dose absorption period. Alcohol consumed the evening before a morning dose does not meaningfully affect the next morning absorption.
However, alcohol complicates GLP-1 therapy in other ways. It adds empty calories that work against weight loss goals. It can worsen GI side effects, particularly nausea and bloating. And alcohol impairs judgment around food choices, which undermines the appetite management benefits the medication provides. Many people on GLP-1 therapy find their alcohol tolerance decreases significantly, making previously normal amounts of alcohol feel much stronger. If you choose to drink, the best alcohol choices on tirzepatide tend to be lower-calorie options consumed in moderation, well separated from dosing times.
Caffeine and morning dosing logistics
The morning coffee problem is real. You wake up. You need to take drops on an empty stomach. You need to hold them for 3-5 minutes. Then you need to wait 30 minutes before eating or drinking. That means no coffee for potentially 35-40 minutes after waking.
For dedicated coffee drinkers, this is the hardest part of the entire GLP-1 drop routine. Some workarounds exist. Drinking coffee first, then waiting at least 30 minutes before taking drops, is acceptable as long as the coffee is black (no sugar, no cream) and you wait long enough for the oral environment to return to baseline. The downside is extending the total morning routine significantly.
The alternative many people prefer is taking drops immediately upon waking, doing their morning routine during the hold and fasting period, then enjoying coffee after the 30-minute window. This turns the fasting period into productive time rather than idle waiting. By the time you have showered, dressed, and prepared for the day, the 30 minutes have passed and coffee is ready.
Caffeine itself does not interfere with GLP-1 mechanism of action. The concern is purely about the timing relative to sublingual absorption. Once the absorption window has closed, caffeine consumption is fine and may even complement the medication by providing an additional mild appetite suppressant effect.
GLP-1 drops for beginners: your first two weeks
Starting GLP-1 drops can feel overwhelming. Here is what to realistically expect during the first fourteen days, along with specific guidance for each phase.
Days 1-3: learning the technique
The first few doses are about establishing the physical routine. You will fumble with the syringe. The liquid will feel strange under your tongue. You will probably swallow too soon at least once. All of this is normal.
Focus on getting the basics right. Correct placement under the tongue. Timer set for the hold duration. Mouth closed. Tongue still. Do not worry about perfecting every detail immediately. Aim for a 2-minute hold minimum and build from there.
Side effects during days 1-3 are typically minimal. The first week on semaglutide often produces subtle effects, primarily mild appetite reduction and perhaps slight nausea that comes and goes. Some people feel nothing at all during the first few days, which does not mean the medication is not working. Therapeutic blood levels need time to build with daily dosing.
Days 4-7: establishing the routine
By the end of the first week, the physical mechanics should feel more natural. You know where to place the syringe. You know how the liquid feels. You have a spot where you sit during the hold period. The routine is becoming a habit rather than a conscious effort.
Appetite changes typically begin emerging around days 4-7. You might notice that your usual portion size feels like too much food. Food noise, the constant mental chatter about what to eat next, may start to quiet down. These are early signs that the medication is reaching therapeutic levels through consistent sublingual absorption.
If you experience nausea during this period, it is usually mild and manageable. Small, frequent meals of bland, protein-rich foods help. Avoid greasy, heavy, or highly processed meals that can exacerbate GI discomfort. The GLP-1 breakfast ideas guide provides meal suggestions specifically designed for the adjustment period.
Days 8-14: optimizing and adjusting
The second week is when technique optimization matters most. You have the basics down. Now focus on extending hold time toward 3-5 minutes, perfecting the pre-dose fasting routine, and paying attention to how different timing strategies affect your results throughout the day.
By day 14, you should have enough data to evaluate whether the starting dose is appropriate. Are you experiencing appetite suppression? Any side effects? How is your energy? This information helps your provider decide whether to maintain the current dose or begin dose escalation at the next scheduled adjustment.
Keep a brief daily log during these first two weeks. Note the time you took your dose, how long you held it, any side effects, appetite level on a 1-10 scale, and what you ate. This data is invaluable for troubleshooting and for conversations with your provider about dose adjustments. SeekPeptides members access progress tracking tools designed specifically for monitoring peptide-based weight loss protocols.
Advanced techniques for experienced users
Once you have been taking GLP-1 drops for several weeks and have the fundamental technique mastered, these advanced strategies can further optimize absorption and results.
Pre-hydration protocol
Drinking 8-16 ounces of water 15-20 minutes before taking drops, then stopping all fluids 5 minutes before administration, creates an interesting dynamic. The pre-hydration improves blood flow to the oral tissues (good for absorption) while the 5-minute dry period reduces initial saliva dilution. This is a small optimization, but experienced users report noticeably better absorption compared to either dehydrated or immediately-post-drinking administration.
Tongue positioning refinement
Beyond basic placement, the angle and pressure of the tongue over the medication pool affects absorption. The ideal position is a relaxed tongue resting lightly over the liquid, creating a sealed pocket without compression. Too much pressure pushes the liquid laterally into less absorptive tissue. Too little pressure allows the liquid to shift with any head movement. Finding the sweet spot takes practice but becomes automatic within a few weeks.
Combining drops with microdosing protocols
Some providers prescribe microdosing approaches where smaller doses are taken more frequently throughout the day. This strategy aims to maintain more consistent blood levels and reduce peak-related side effects. If your provider recommends microdosing, each individual administration still requires proper sublingual technique. Taking two half-doses with perfect technique is better than one full dose with rushed technique.
Building a sustainable daily routine around GLP-1 drops
Long-term success with sublingual GLP-1 therapy depends on making the administration routine feel effortless rather than burdensome. People who quit drops most often cite the daily routine as the primary frustration, not the side effects or results.
The morning protocol
Wake up. Use the bathroom. Sit in your designated dosing spot. Remove drops from fridge. Roll bottle. Draw dose. Administer. Start timer. Breathe through your nose for 3-5 minutes while the liquid absorbs. Swish. Swallow. Replace bottle in fridge. Continue morning routine.
Total time: 5-7 minutes including preparation and hold time. This is less time than most people spend scrolling their phone before getting out of bed. When framed as a small daily investment in health rather than a medical obligation, the routine becomes easier to maintain.
Creating environmental triggers
Leave the oral syringe on the bathroom counter as a visual reminder. Set a daily alarm on your phone. Attach the dosing routine to an existing habit like feeding the dog or starting the coffee maker. Habit stacking, linking the new behavior to an established one, dramatically increases consistency.
What to do when you miss a dose
Missing a single dose of daily sublingual GLP-1 is not a crisis. Do not double up the next day. Simply resume your normal dose at the usual time. If you miss two or more consecutive days, you may notice a temporary return of appetite and food noise. This resolves quickly once consistent dosing resumes.
If you frequently miss doses, reassess your routine. Is the timing unrealistic? Is the hold period too difficult to fit into your morning? Adjusting when and how you take the drops is better than skipping them regularly. A dose taken with imperfect timing is always better than a dose not taken at all.
When GLP-1 drops are not enough
Sublingual drops work well for many people, but they are not the optimal delivery method for everyone. Recognizing when drops are falling short prevents months of frustrating underperformance.
Absorption limitations
Some people have anatomical or physiological factors that limit sublingual absorption. Thick mucosal tissue, reduced blood flow to the sublingual area (common in smokers), chronic dry mouth from medications, and mouth breathing during sleep that carries over to the dosing period can all reduce how effectively drops work.
If you have optimized every aspect of technique, escalated to the highest recommended sublingual dose, and still see inadequate results after 8-12 weeks, the delivery method may be the limiting factor. This is not a failure. It is a sign that your body processes sublingual medication differently, and injectable delivery might serve you better.
When to talk to your provider
Contact your provider if you experience no appetite suppression after 4 weeks of consistent use, if side effects worsen rather than improve over time, if you develop mouth sores or persistent oral irritation, or if your results plateau significantly after previously good progress. These situations require professional evaluation to determine whether technique adjustment, dose modification, or a delivery method change is appropriate.
Alternative delivery methods to consider
If sublingual drops are not providing adequate results, several alternative delivery methods exist within the GLP-1 category. Weekly subcutaneous injections remain the gold standard for bioavailability and are the most extensively studied delivery method. GLP-1 patches represent a newer option that provides transdermal delivery, though evidence for their effectiveness compared to injections is still limited. Tablet formulations use absorption enhancers to survive the digestive tract, with FDA-approved oral semaglutide (Rybelsus) available for daily tablet dosing.
Each delivery method involves trade-offs between convenience, bioavailability, cost, and personal preference. The semaglutide versus tirzepatide comparison page outlines the differences between the two main GLP-1 compounds, while the decision between drops and injections comes down to individual physiology and lifestyle preferences. Some people cycle between delivery methods, using drops during periods when needle fatigue sets in and returning to injections when they want maximum effectiveness for specific goals.
Stacking GLP-1 drops with supporting compounds
Beyond the GLP-1 medication itself, many people use supporting compounds to enhance their results. Peptide stacks for weight loss sometimes include compounds like AOD-9604 for fat metabolism support, BPC-157 for gut health optimization, and various peptide combinations tailored to specific goals. The peptide stack calculator helps determine compatible combinations and timing.
Supporting compounds are separate from GLP-1 drops and typically administered via injection at a different time of day. They do not replace proper GLP-1 technique but can address secondary concerns like gut health, hair preservation, and energy levels that sometimes become issues during aggressive weight loss protocols.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. SeekPeptides members access detailed protocol builders, weight-based calculators, and expert-reviewed dosing guides that account for individual factors most resources ignore.
Frequently asked questions
How long should I hold GLP-1 drops under my tongue?
Hold for a minimum of 2 minutes, though 3-5 minutes produces significantly better absorption. Some providers recommend up to 10 minutes for maximum results. The longer you hold, the more active compound crosses the sublingual membrane into your bloodstream. Set a timer to avoid guessing, and keep your mouth closed and tongue still during the entire hold period.
Can I eat or drink right after taking GLP-1 drops?
No. Wait at least 30 minutes after administration before eating, drinking, or brushing your teeth. This fasting window allows the medication absorbed into the mucosal tissue to fully enter the bloodstream. Eating or drinking too soon washes away compound still in the process of absorbing and redirects blood flow from the oral tissues to the digestive system. Many providers recommend waiting 45-60 minutes for optimal results.
Do GLP-1 drops work as well as injections?
Drops have lower bioavailability than injections, typically 5-40% versus nearly 100% for subcutaneous injection. However, with proper technique and appropriate dosing, many people achieve meaningful results from sublingual drops. The daily dosing pattern of drops can produce more consistent blood levels than weekly injections, which some people prefer. Results vary significantly based on individual absorption and technique quality.
What should I do if my GLP-1 drops taste bad?
Many compounded formulations include peppermint or other flavoring to improve the taste. If the taste is difficult to tolerate, ask your compounding pharmacy about alternative flavoring options. Do not try to mask the taste with food, drink, or mouthwash before the 30-minute post-dose fasting window. The taste becomes less noticeable over time as you adjust to the routine.
Can I take GLP-1 drops if I have dry mouth?
Chronic dry mouth can actually improve sublingual absorption in some cases because the medication is not immediately diluted by excess saliva. However, if dry mouth is caused by medications that also reduce blood flow to the oral tissues, absorption may be impaired. Discuss your dry mouth condition with your provider so they can assess whether sublingual delivery is appropriate for your situation.
How do I know if my GLP-1 drops are still effective?
Check the beyond-use date on the bottle, typically 30-90 days from compounding. If the drops have been stored properly in the refrigerator, they should maintain potency until this date. Signs of degradation include changes in color, cloudiness, unusual smell, or a noticeable decrease in effectiveness despite consistent technique. If you suspect degradation, particularly after a temperature excursion, contact your pharmacy.
Is it safe to take GLP-1 drops while breastfeeding?
This is a question strictly for your healthcare provider. The safety of GLP-1 medications during breastfeeding has not been established with sufficient clinical data. The complete guide on GLP-1 and breastfeeding reviews the available evidence, but the decision to use any GLP-1 medication while nursing should involve a thorough risk-benefit discussion with your doctor.
Can I split my daily dose into two administrations?
Some providers prescribe twice-daily dosing, taking half the daily dose in the morning and half in the evening. This approach maintains more stable blood levels and may reduce side effects. However, it doubles the number of sublingual administrations, each requiring proper technique. Only split doses under provider guidance, and ensure each administration follows the complete technique outlined in this guide.
External resources
FDA: Concerns with unapproved GLP-1 drugs used for weight loss
Mayo Clinic: Semaglutide oral route description
In case I do not see you, good afternoon, good evening, and good night. May your drops stay potent, your technique stay precise, and your results stay consistent.