Apr 3, 2026

If someone told you sermorelin is a GLP-1 receptor agonist, they were wrong. Full stop. This confusion is everywhere right now, and it makes sense on the surface. Both are peptides. Both come in injectable form. Both show up on the menus of weight management clinics. Both require a prescription.
But the similarity ends there, completely, at the molecular level, at the mechanism of action, at the target receptor, and at the clinical outcome. Treating them as interchangeable is like confusing insulin with adrenaline because both involve your pancreas. Understanding what GLP-1 actually means is the first step toward clarity. The category overlap is superficial. The underlying biology is entirely different.
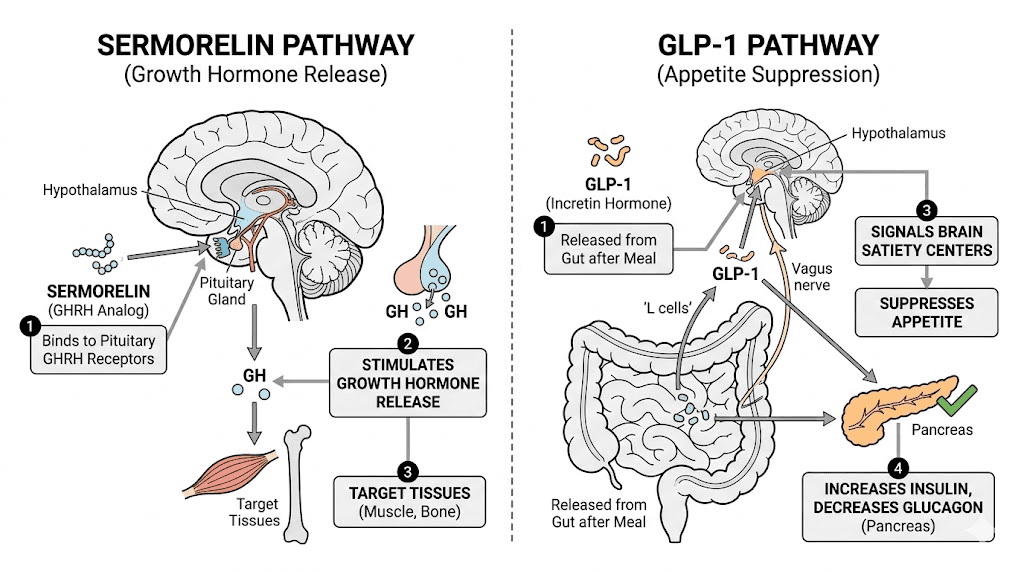
Sermorelin belongs to a class called growth hormone-releasing hormone analogs, or GHRH analogs. It works by talking to your pituitary gland, coaxing it to release more of your own growth hormone in a natural, pulsatile pattern. GLP-1 receptor agonists, on the other hand, talk to your gut, your pancreas, and your brain, suppressing appetite and slowing digestion to drive dramatic weight loss. These are two separate pharmacological universes.
The confusion matters because choosing the wrong peptide for your goals can mean months of disappointment. Someone looking for aggressive fat loss who starts sermorelin expecting Ozempic-like results will be underwhelmed. Someone who needs body recomposition and muscle preservation who starts semaglutide instead might lose significant lean mass alongside fat. Understanding what each peptide actually does, at the cellular level, changes the decision completely.
This guide covers everything. What sermorelin actually is. What GLP-1 receptor agonists actually are. How they work at the receptor level. How their weight loss outcomes differ. How their side effect profiles compare. Whether you can combine them. And which one genuinely fits your goals. If you have been getting conflicting information about these two peptide classes, this is where it ends.
What sermorelin actually is
Sermorelin is a synthetic analog of growth hormone-releasing hormone, commonly abbreviated as GHRH. It represents the first 29 amino acids of the naturally occurring 44-amino-acid GHRH molecule that your hypothalamus produces. That truncated structure is not an accident. Researchers discovered that the first 29 amino acids contain the biologically active portion of the full GHRH molecule, meaning sermorelin delivers the same signal to the pituitary with a shorter, more stable, and more cost-effective peptide chain.
To understand what sermorelin does, you need to understand the growth hormone axis. Your hypothalamus sits at the top. It produces GHRH, which travels to the anterior pituitary gland and binds to specific GHRH receptors on cells called somatotrophs. Those cells respond by synthesizing and releasing growth hormone into the bloodstream. Growth hormone then travels to the liver, where it stimulates production of insulin-like growth factor 1, or IGF-1. IGF-1 is the downstream mediator responsible for most of the anabolic, fat-mobilizing, and tissue-repair effects that people associate with growth hormone.
Sermorelin mimics GHRH. When you inject it, it binds to GHRH receptors on pituitary somatotrophs and triggers GH release in a pulse pattern that mirrors the body natural secretion rhythm. This is fundamentally different from injecting synthetic human growth hormone, which bypasses the hypothalamic-pituitary axis entirely and floods the body with exogenous GH at unnaturally high, non-pulsatile levels. For an overview of how lyophilized vs liquid peptides differ in how they are prepared and administered, that comparison is useful context for understanding the reconstitution process sermorelin requires. Sermorelin works with your biology. Direct HGH works around it.
The pituitary also has its own built-in brake system. Somatostatin, another hypothalamic hormone, counteracts GHRH and suppresses GH secretion. When sermorelin drives GH release, somatostatin rises as a counterbalance. This negative feedback loop means you physically cannot overdose your pituitary into releasing dangerous amounts of GH on sermorelin. The body self-regulates. This is one of the key safety advantages over exogenous HGH, which bypasses this regulatory mechanism entirely.
Sermorelin was FDA approved as a diagnostic tool for childhood growth hormone deficiency and later as a treatment for pediatric GH deficiency under the brand name Geref. Off-label adult use for anti-aging, body recomposition, and general wellness followed as the research base grew.
Today it is commonly prescribed through compounding pharmacies for adult patients who want to restore declining GH levels without the risks associated with direct HGH administration. The landscape of research vs pharmaceutical peptides is relevant context for understanding how sermorelin is accessed. For those researching peptides for anti-aging, sermorelin is frequently among the first discussed.
The typical sermorelin dosing protocol runs 200-500mcg per injection, administered subcutaneously once daily, ideally in the 30-60 minutes before bedtime. The bedtime timing aligns with the body natural GH surge that occurs during deep sleep, amplifying the pulse and maximizing nighttime tissue repair and recovery. Some protocols split the dose, injecting smaller amounts in the morning and evening, but most researchers find the single bedtime injection sufficient. You can explore dosing details and volume calculations with a peptide reconstitution calculator when preparing your vials.
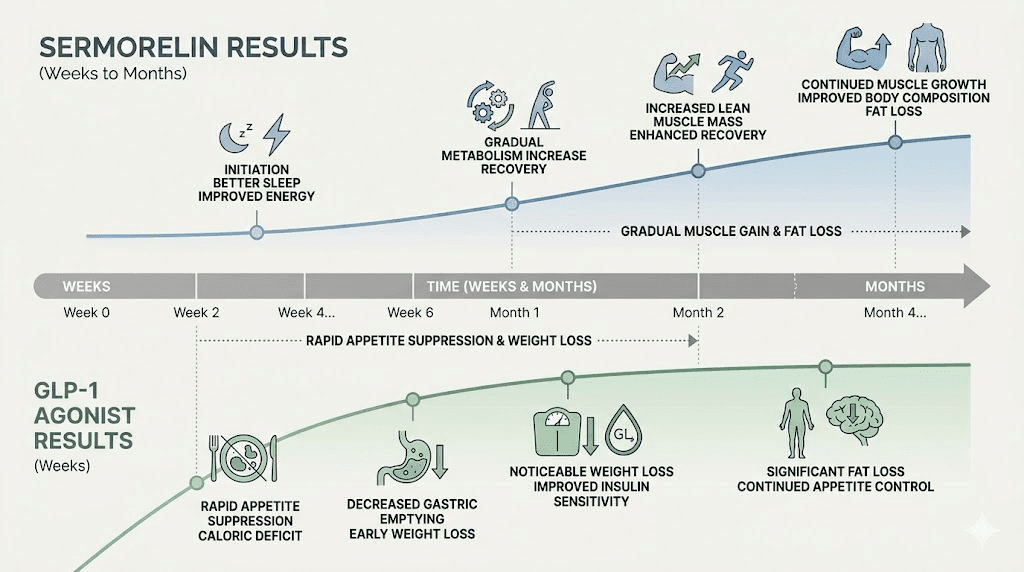
Results from sermorelin do not arrive overnight. The peptide restores a pattern of GH secretion rather than flooding the system with GH directly. Energy improvements and sleep quality changes often appear within the first few weeks. Meaningful body composition changes, including increased lean mass and decreased visceral fat, typically require three to six months of consistent use. This gradual, physiological timeline is very different from the rapid, dramatic weight loss associated with GLP-1 receptor agonists. For a visual sense of what sermorelin protocols produce over time, sermorelin before and after results from documented protocols are instructive.
What GLP-1 receptor agonists actually are
GLP-1 stands for glucagon-like peptide-1. It is a hormone produced naturally by L-cells in the small intestine in response to eating. Its primary roles are to stimulate insulin release from the pancreas, suppress glucagon secretion, slow gastric emptying, and signal satiety to the brain. In healthy individuals, GLP-1 is released after meals, helps manage blood glucose, and contributes to the feeling of fullness. The problem is that native GLP-1 has an extremely short half-life, measured in minutes, because an enzyme called DPP-4 rapidly degrades it.
GLP-1 receptor agonists are synthetic peptides engineered to mimic GLP-1 but resist DPP-4 degradation, giving them half-lives ranging from hours to days or even a week. The most widely known is semaglutide, sold as Ozempic for type 2 diabetes and Wegovy for obesity. Whether you encounter GLP-1 medications through oral tirzepatide formulations or traditional injections, the core mechanism is the same. Tirzepatide, sold as Mounjaro and Zepbound, adds GIP receptor agonism to GLP-1 agonism, making it a dual incretin agonist. The newest class includes retatrutide, a triple agonist that activates GLP-1, GIP, and glucagon receptors simultaneously. None of these have any relationship to the GHRH-pituitary-GH axis. They operate in an entirely different physiological system.
The weight loss produced by GLP-1 receptor agonists is genuinely dramatic by pharmaceutical standards. Semaglutide at the 2.4mg weekly dose produced an average 15-17% reduction in body weight over 68 weeks in the STEP trials. Tirzepatide, in the SURMOUNT trials, produced average weight loss of up to 22.5% over 72 weeks at the 15mg dose. Retatrutide, in phase 2 trials, produced approximately 24% weight loss over 48 weeks, though phase 3 data continues to accumulate. For those tracking retatrutide development, the retatrutide vs semaglutide comparison puts its efficacy in context against established agents. For context on how these numbers compare and what they mean practically, the semaglutide vs tirzepatide breakdown covers the clinical trial data in depth.
GLP-1 receptor agonists are not peptides in the casual sense that the word gets used in wellness circles. They are prescription medications with established clinical trials, FDA approval for specific indications, and meaningful side effect profiles. Semaglutide and tirzepatide are not obscure research chemicals. They are among the most prescribed and most studied weight loss medications in history. That clinical evidence base is both a major advantage and something that confuses the comparison with sermorelin, which has a much smaller clinical trial footprint. The landscape continues to evolve with new options like switching between GLP-1 agents becoming increasingly common as users and clinicians optimize protocols based on individual response.
The GLP-1 mechanism at the receptor level involves binding to GLP-1R, a G-protein coupled receptor expressed in the gut wall, the pancreatic beta cells, the brainstem, and critically, in the arcuate nucleus of the hypothalamus. That last location is where appetite suppression primarily occurs. Activation of hypothalamic GLP-1 receptors reduces food-seeking behavior, decreases meal size, and produces a sustained reduction in caloric intake that drives the dramatic weight loss numbers seen in clinical trials. For more on how the appetite suppression timeline works, how quickly semaglutide suppresses appetite explains the onset pattern in detail. The broader question of how long tirzepatide takes to suppress appetite follows a similar but distinct timeline.
Understanding this distinction is important when someone asks whether sermorelin is a GLP-1. It is not. Not even close. Sermorelin binds GHRH receptors in the pituitary. GLP-1 receptor agonists bind GLP-1R receptors in the gut and brain. The peptide bond classification they share is about as meaningful as saying a locksmith and a lockpick are the same thing because both involve locks. The superficial category is shared. The function is entirely different.
Why people confuse sermorelin with GLP-1
The confusion is understandable. Both peptides are injectable. Both require a prescription. Both appear on the formulary of weight management and anti-aging clinics. Both have entered mainstream wellness culture at roughly the same moment in history. New delivery formats like GLP-1 patches and oral semaglutide drops further blur the lines by expanding GLP-1 beyond traditional injections. When a clinic offers a "peptide weight loss program" and lists sermorelin alongside semaglutide, the natural assumption is that these work similarly. They do not, but the marketing context blurs the distinction.
The peptide category itself is part of the problem. The word "peptide" describes any short chain of amino acids, which covers an enormous and physiologically diverse range of compounds. BPC-157 is a peptide. So is insulin. So is oxytocin. So is semaglutide. So is sermorelin. Grouping them all under "peptides" is accurate but deeply misleading about how they work. People see "peptide weight loss" content, hear about both sermorelin and semaglutide, and assume they belong to the same therapeutic category. They do not. For a clearer taxonomy of peptide types and their differences, the injectable vs oral peptides guide helps orient the broader landscape.
Marketing language at clinics also contributes. When a medically supervised weight loss program describes sermorelin as part of a "metabolic optimization protocol" that also includes GLP-1 medications, patients understandably assume these are variations on the same theme. Some online forums and social media accounts treat them interchangeably, further entrenching the confusion. The people asking "is sermorelin a GLP-1" online are not confused because they failed to pay attention. They are confused because the information environment around peptides is genuinely messy. Similar classification questions arise constantly, such as whether toujeo is a GLP-1 or whether tresiba is a GLP-1, showing how widespread the confusion extends across multiple drug classes.
There is also the functional overlap at the weight management outcome level, at least in the broadest sense. Both sermorelin and GLP-1 medications can contribute to improved body composition. Sermorelin does so gradually, through GH-mediated metabolic improvements and lean mass preservation. GLP-1 medications do so rapidly and dramatically, through appetite suppression and caloric restriction. The endpoint of "losing fat" is shared. The mechanism, timeline, magnitude, and side effect profile are completely different. For people primarily focused on the output rather than the mechanism, the distinction can seem academic. But it is not. It determines which one actually fits your situation. The peptides for fat loss guide explains these distinctions clearly.
One more source of confusion: some clinics combine sermorelin with GLP-1 medications in a single protocol. When patients see both on the same treatment plan, they may assume they are in the same drug class. They are not. They are complementary compounds working through entirely different pathways, prescribed together precisely because they address different aspects of body composition. More on combination approaches later in this guide.
Social media compounds the confusion in specific ways worth naming. Influencer content about "peptide therapy for weight loss" often groups GH-releasing peptides and GLP-1 medications together because the creator uses both without clearly delineating the mechanisms. Someone watching a before-and-after video where the creator credits "peptides" for their dramatic weight loss may not realize the actual weight loss came from tirzepatide while the sermorelin or ipamorelin contributed to muscle preservation. The attribution is loose, the category is blurred, and the viewer comes away assuming all peptides in the protocol work the same way.
There is also genuine overlap in the clinical populations. People seeking peptide therapy for weight management often have overlapping concerns: fatigue, body composition issues, metabolic sluggishness, and aging-related changes in muscle and fat distribution. Both GH axis peptides like sermorelin and GLP-1 medications address aspects of these concerns, just through radically different mechanisms. The shared patient population does not mean shared mechanism. Understanding that distinction is what separates an informed decision from a marketing-driven one. SeekPeptides exists precisely to bridge that gap, providing the mechanism-level clarity that clinic marketing material often omits.
How sermorelin works at the cellular level
Walk through the pathway step by step. Sermorelin is injected subcutaneously, usually in the abdomen or thigh. It enters systemic circulation and crosses into the brain, where it binds to GHRH receptors located on somatotroph cells in the anterior pituitary gland. This binding event activates adenylyl cyclase through a Gs-protein coupled mechanism, increasing intracellular cyclic AMP. The rise in cAMP activates protein kinase A, which triggers both the synthesis of new growth hormone and the exocytosis of stored GH from secretory granules.
The released GH enters the bloodstream in a pulse. This pulsatile release pattern is critical and is one of the primary reasons sermorelin is considered safer and more physiological than direct HGH injection. The body responds to pulsatile GH by briefly upregulating receptors and then downregulating them between pulses. Continuous, non-pulsatile GH exposure, as seen with exogenous HGH injections, tends to cause receptor downregulation and resistance over time. Sermorelin preserves the natural pattern.
GH circulates and binds to GH receptors throughout the body. In the liver, this triggers significant IGF-1 production. IGF-1 is the primary mediator of GH anabolic effects. It promotes protein synthesis in muscle tissue, stimulates lipolysis in adipose tissue, supports bone density, and participates in cellular repair and regeneration. This is why the body composition effects of sermorelin, increased muscle mass and decreased body fat, typically require three to six months of consistent use. The process runs through multiple biochemical steps, each taking time to accumulate into visible changes. For those using sermorelin alongside other growth hormone-related peptides, the sermorelin ipamorelin blend for men protocol illustrates how stacking GHRH analogs with GH secretagogues can amplify the GH pulse.
Somatostatin, the inhibitory counterpart to GHRH, provides the safety valve. When sermorelin drives GH release, rising GH and IGF-1 levels signal the hypothalamus to release more somatostatin, which then suppresses further GH secretion until GH levels fall again. This is the negative feedback loop that prevents pathological GH excess. A person injecting 500mcg of sermorelin cannot force their pituitary to produce pathological amounts of GH because somatostatin will intervene. This is categorically different from injecting exogenous HGH, where there is no such regulatory brake.
The practical implications of this mechanism include a specific side effect profile. Because sermorelin acts through the body regulatory systems rather than bypassing them, the side effects are generally mild. Injection site reactions occur in roughly one in six users, including redness, swelling, or discomfort at the injection site. Some users report transient headache, flushing, or dizziness in the hours after injection, likely related to the GH pulse. These typically diminish as the body adjusts. There are no reports of the severe gastrointestinal side effects that characterize GLP-1 therapy, because sermorelin has no activity at GLP-1 receptors, GIP receptors, or any gut receptor pathway. For those also managing GLP-1 side effects, understanding GLP-1 fatigue and GLP-1 hair loss can be valuable for full protocol management.
Sermorelin also preserves the natural relationship between sleep and GH secretion. The largest GH pulse in healthy individuals occurs during slow-wave sleep, roughly 60-90 minutes after sleep onset. Injecting sermorelin 30-60 minutes before bed amplifies this natural pulse rather than creating an artificial one. Users frequently report improved sleep quality as an early benefit, before meaningful body composition changes appear, because the enhanced GH pulse during sleep promotes deeper sleep architecture. This sleep improvement is one of the consistent early indicators that sermorelin is working. You can track how protocols evolve over time using the peptide calculator to optimize dose timing and volume for your specific situation.
How GLP-1 receptor agonists work at the cellular level
Start with the gut. When you eat, L-cells in the small intestine and colon release native GLP-1 into the portal circulation. Natural GLP-1 has a plasma half-life of one to two minutes because DPP-4, a ubiquitous enzyme, cleaves it rapidly. GLP-1 receptor agonist drugs are engineered to resist this cleavage, extending their half-life to hours for short-acting agents like exenatide or to approximately one week for semaglutide.
Semaglutide binds GLP-1 receptors throughout multiple tissues simultaneously. In the pancreatic beta cells, GLP-1R activation stimulates glucose-dependent insulin secretion, meaning insulin release increases only when blood glucose is elevated. This glucose-dependent mechanism is why GLP-1 medications carry low hypoglycemia risk when used alone, unlike older diabetes medications that stimulate insulin release regardless of blood sugar. GLP-1R activation also suppresses glucagon secretion from pancreatic alpha cells, preventing the liver from dumping excess glucose between meals.
In the gastrointestinal tract, GLP-1R activation slows gastric emptying significantly. Food moves more slowly from the stomach into the small intestine. This produces prolonged satiety after meals because the mechanical stretch in the stomach persists longer. It also blunts post-meal glucose spikes by slowing carbohydrate absorption. For many users, this gastric slowing effect is the primary driver of early nausea during GLP-1 therapy, as the stomach adjusts to a different emptying rate. The semaglutide constipation treatment guide addresses one of the most common downstream GI effects.
The appetite suppression mechanism is where GLP-1 receptor agonists generate the most clinical interest. GLP-1 receptors in the hypothalamus, particularly in the arcuate nucleus and the ventromedial nucleus, mediate appetite and feeding behavior. When GLP-1R in these regions is activated, the brain reduces food-seeking behavior, decreases meal frequency and size, and shifts the reward response to food downward. Many users on semaglutide or tirzepatide report not just feeling less hungry but also losing interest in foods they previously craved. This "food noise" reduction is a central part of the therapeutic mechanism and is distinct from anything sermorelin does. Sermorelin has no activity in hypothalamic feeding centers through GLP-1 pathways. For how quickly this appetite suppression sets in on different agents, how fast semaglutide works and how fast tirzepatide works cover the respective timelines.
Tirzepatide adds GIP receptor agonism to this picture. GIP, or glucose-dependent insulinotropic polypeptide, also acts in the hypothalamus and adipose tissue. The dual GIP/GLP-1 agonism of tirzepatide appears to drive superior weight loss compared to GLP-1 agonism alone, which is why SURMOUNT trial results exceed STEP trial results. Retatrutide adds glucagon receptor agonism on top of both, increasing hepatic fat oxidation and energy expenditure through a third pathway. Each layer of receptor engagement adds incremental weight loss benefit. The retatrutide vs semaglutide comparison and the difference between tirzepatide and retatrutide explore these distinctions in depth.
GLP-1 medications are dosed on escalating schedules to allow GI tolerance to develop. Semaglutide starts at 0.25mg weekly for four weeks, advances to 0.5mg, and can increase up to 2.4mg weekly in 0.25-0.5mg increments every four weeks. Tirzepatide starts at 2.5mg weekly and escalates to a maximum of 15mg. Rushing dose escalation is the most common driver of severe nausea and vomiting. Proper reconstitution and injection technique matter too. For semaglutide preparation, how to reconstitute semaglutide and for tirzepatide, how to reconstitute tirzepatide walk through the process step by step. Injection site selection also matters; where to inject GLP-1 and how to inject GLP-1 cover the specifics.
Weight loss comparison
This is where the two peptide classes diverge most dramatically in clinical outcomes. GLP-1 receptor agonists produce weight loss that is frankly remarkable by the historical standards of pharmaceutical intervention. Sermorelin produces gradual body recomposition that is genuinely useful but operates on a different scale entirely.
Semaglutide at the 2.4mg dose in the STEP 1 trial produced an average weight loss of 14.9% of body weight over 68 weeks. STEP 2, conducted in people with type 2 diabetes, showed 9.6% average weight loss. STEP 4, which extended the protocol, showed continued weight loss in responders. Tirzepatide at the 15mg dose in SURMOUNT-1 produced an average weight loss of 22.5% over 72 weeks, with a significant proportion of participants losing 25% or more. These are not modest improvements. These are results that outperform bariatric surgery for some patients. The average GLP-1 weight loss per month breaks down how the weekly losses accumulate and what realistic monthly expectations look like.
Sermorelin does not produce weight loss in this magnitude or on this timeline. What it does is shift body composition over months by increasing GH and IGF-1, which promotes muscle protein synthesis and fat mobilization, particularly visceral fat. Studies on GHRH analogs consistently show improvements in lean mass and reductions in body fat percentage in GH-deficient adults, but these are body recomposition effects rather than dramatic scale weight loss. A person starting sermorelin at 200 pounds might see two to four pounds of fat loss over several months while simultaneously gaining muscle, resulting in a scale weight change that understates the metabolic improvement. For those whose primary concern is rapid, visible results, tirzepatide before and after results and men before and after tirzepatide show the dramatic body changes GLP-1 medications can produce, while sermorelin before and after documentation shows the more gradual, composition-focused improvements. This is a completely different clinical experience from semaglutide, where scale weight drops significantly and quickly.
Head-to-head clinical trials comparing sermorelin directly to GLP-1 medications do not exist in the published literature. The patient populations are different, the indications are different, and the study designs would be challenging to justify given the distinct mechanisms. What we have is parallel evidence, robust for GLP-1 from large phase 3 trials, and moderate for sermorelin from smaller studies and real-world protocols. Neither body of evidence tells us which is "better" in an absolute sense, because that framing misses the point. They address different problems.
Factor | Sermorelin | Semaglutide | Tirzepatide | Retatrutide |
|---|---|---|---|---|
Mechanism | GHRH analog, pituitary GH stimulation | GLP-1R agonist | GLP-1R + GIP agonist | GLP-1R + GIP + glucagon agonist |
Average weight loss | 2-5% (body recomposition) | 15-17% | 20-22.5% | ~24% (phase 2) |
Muscle preservation | Excellent (promotes lean mass) | Poor without resistance training | Moderate | Under study |
Dosing frequency | Daily | Weekly | Weekly | Weekly |
Results timeline | 3-6 months for body comp | 4-8 weeks for appetite change | 4-8 weeks for appetite change | 4-8 weeks for appetite change |
Primary side effects | Injection site, mild headache | Nausea, GI distress | Nausea, GI distress | Nausea, GI distress, potential muscle loss |
FDA status (adults) | Off-label | Approved (obesity, T2D) | Approved (obesity, T2D) | Phase 3 trials ongoing |
The table above makes clear that these are not competing products targeting the same indication. They are complementary tools addressing different aspects of metabolic health. For those trying to decide between semaglutide and tirzepatide specifically, the semaglutide vs tirzepatide side effects comparison covers the nuances, and the semaglutide dosage calculator helps with dose management once you are underway.
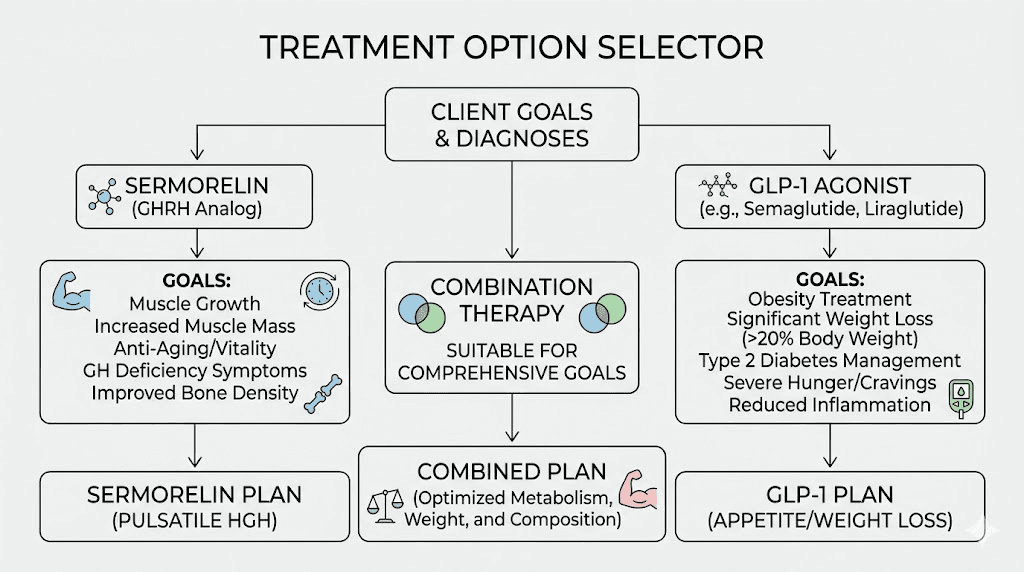
Who gets better results with which? If your goal is significant, scale-weight fat loss, particularly if you have 50 or more pounds to lose, GLP-1 medications produce results that sermorelin simply cannot match. If your goal is body recomposition, anti-aging, improved recovery, better sleep, and modest fat reduction without dramatic caloric restriction, sermorelin is more appropriate. If you are on GLP-1 medications and concerned about muscle loss alongside fat loss, that is where sermorelin can serve as a complement rather than a competitor.
Side effect comparison
The side effect profiles of sermorelin and GLP-1 receptor agonists are as different as their mechanisms.
Sermorelin side effects are generally mild and transient. Injection site reactions are the most common, reported in approximately one in six users, typically presenting as redness, mild swelling, or local irritation that resolves within hours. Headache occurs in some users, thought to be related to the GH pulse driving mild fluid shifts. Flushing and dizziness have been reported rarely, most commonly in the period immediately following injection. These side effects typically diminish after the first two to four weeks as the body adjusts to the new GH pulse pattern. Serious adverse events are rare, and the self-regulatory mechanism through somatostatin prevents the acromegaly risk associated with pharmacological HGH doses. Water retention and joint discomfort, common with exogenous HGH, are generally not significant issues at normal sermorelin doses. Some users do report leg cramps or lightheadedness on GLP-1 medications, but these are unique to that drug class and not seen with sermorelin.
GLP-1 receptor agonist side effects are more prominent, particularly early in therapy. Nausea is the most prevalent, affecting 40-50% of users in the early weeks of treatment. Vomiting occurs in 10-20% of users. Diarrhea and constipation both occur, and some users cycle between the two. These GI effects are directly related to slowed gastric emptying and the gut receptor activation that drives the mechanism. For most users, GI side effects diminish significantly after four to eight weeks as the body adjusts. For those who find constipation particularly problematic, GLP-1 constipation relief and tirzepatide constipation treatment offer practical strategies. Other GI-adjacent effects include heartburn on tirzepatide and GLP-1 dry mouth, both of which resolve as tolerance builds.
Other GLP-1 side effects worth knowing include fatigue, particularly in the early weeks. The semaglutide fatigue guide explains why this occurs and how to manage it. Hair loss has been reported by some GLP-1 users, likely related to the caloric deficit and nutritional stress of rapid weight loss rather than the medication directly. The GLP-1 hair loss guide covers this in detail. Headaches are reported by some users, particularly during dose escalation phases. Understanding tirzepatide headaches and when they indicate a problem versus a normal adjustment can prevent unnecessary protocol changes.
Side effect | Sermorelin | GLP-1 medications |
|---|---|---|
Injection site reactions | Common (1 in 6) | Mild, less frequent |
Nausea | Rare | Very common (40-50% early) |
Vomiting | Not reported | Common (10-20%) |
Diarrhea/Constipation | Not reported | Common |
Headache | Mild, occasional | Moderate, dose-related |
Fatigue | Not typical | Common early weeks |
Hair loss | Not reported | Possible with rapid weight loss |
Muscle loss | None (promotes lean mass) | Significant without resistance training |
Water retention | Mild possible | Not typical |
Overdose risk | Minimal (somatostatin brake) | Low (glucose-dependent mechanism) |
The side effect comparison underscores a core difference. Sermorelin asks relatively little of the body in terms of tolerance. GLP-1 medications ask significantly more, especially in the first eight weeks, but for most users the side effects are temporary and the weight loss benefits justify the adjustment period. The interaction with other medications also differs. For example, alcohol and semaglutide have specific considerations, and combining metformin with semaglutide requires awareness of GI overlap. The wellbutrin and tirzepatide interaction is another consideration GLP-1 users encounter that sermorelin users do not. The right choice depends on your tolerance threshold, your health status, and what your goals actually require.
Body composition differences
This is where the conversation gets clinically meaningful for anyone who cares about more than scale weight.
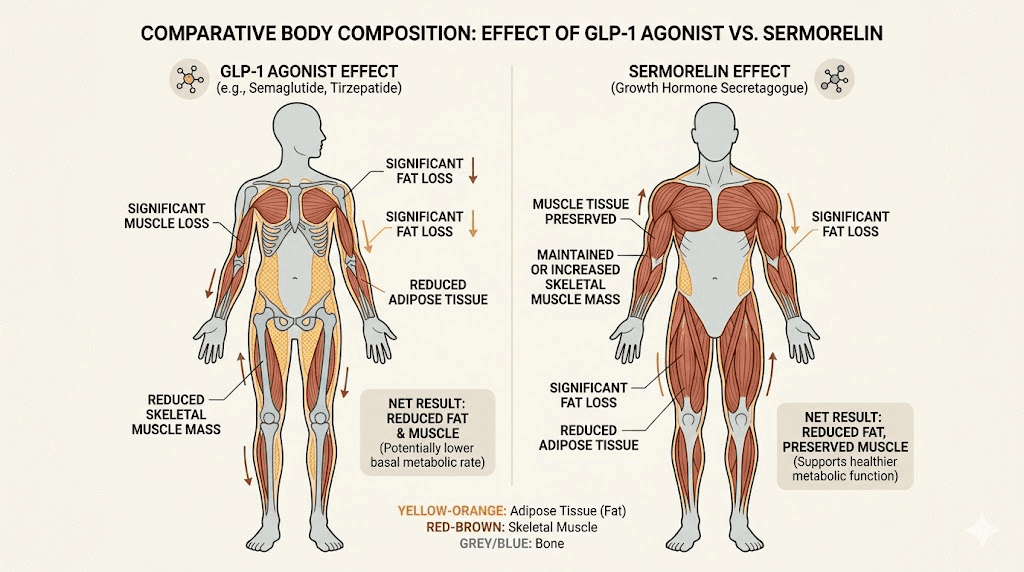
GLP-1 medications produce impressive fat loss. They also produce muscle loss, sometimes significant muscle loss, as a byproduct of the severe caloric deficit they create. In the STEP trials, approximately 39% of the weight lost by semaglutide users was lean mass, including muscle tissue and bone mineral content. In the SURMOUNT trials for tirzepatide, the proportion of lean mass loss was somewhat lower but still present. For someone who loses 30 pounds on semaglutide, roughly 11-12 of those pounds might come from muscle rather than fat. The question of whether tirzepatide burns fat or just suppresses appetite has important implications here, and the answer involves both. Some users also report muscle pain on tirzepatide, which may relate to the lean tissue loss process and further distinguishes the GLP-1 experience from the sermorelin experience.
Muscle loss matters beyond aesthetics. Muscle tissue is metabolically active, meaning it burns calories at rest. Losing muscle while losing fat means a lower basal metabolic rate, which increases the risk of weight regain when the medication is discontinued. It also means reduced functional strength, particularly concerning for older adults. The question of whether you can build muscle while on GLP-1 is not purely hypothetical. With adequate protein intake and resistance training, many users do preserve or even increase muscle mass during GLP-1 therapy, but it requires deliberate effort. The protein requirements on semaglutide guide explains why higher protein targets matter during GLP-1 therapy.
Sermorelin works in the opposite direction on muscle tissue. GH and IGF-1 promote muscle protein synthesis and nitrogen retention. Some GLP-1 users add B12 to semaglutide protocols or B12 to tirzepatide protocols for energy support, but these nutritional additions do not address the muscle loss issue the way sermorelin does. Users on sermorelin protocols frequently report preserved or improved muscle mass alongside gradual fat reduction, particularly visceral fat. For older adults with growth hormone deficiency, where muscle wasting and increased visceral adiposity are clinical features of the deficiency itself, sermorelin can produce genuine body recomposition improvements without the muscle loss risk. This makes sermorelin particularly relevant for those who cannot afford to lose lean mass, such as competitive athletes, older adults managing sarcopenia, or GLP-1 users concerned about muscle tissue loss. Whether retatrutide causes muscle loss is a related concern in the newer triple agonist space. For athletes specifically, peptides for muscle growth and peptides for athletic performance provide context for how GHRH analogs fit into performance-oriented protocols.
The body composition contrast is the most clinically important argument for considering sermorelin as a complement to GLP-1 therapy rather than an alternative. If you are on semaglutide or tirzepatide and losing fat rapidly, adding sermorelin to preserve lean mass addresses one of the primary long-term concerns with GLP-1 monotherapy.
Visceral fat versus subcutaneous fat
Not all fat is equivalent from a metabolic standpoint, and this distinction matters when comparing sermorelin and GLP-1 therapy. Visceral fat, the fat packed around internal organs deep in the abdomen, is far more metabolically damaging than subcutaneous fat, which sits just beneath the skin. Visceral fat secretes inflammatory cytokines, impairs insulin sensitivity, and contributes directly to cardiovascular disease risk. Reducing visceral fat is more clinically meaningful than reducing subcutaneous fat, even if the scale weight change looks similar.
Both GLP-1 medications and sermorelin reduce visceral fat, but through different mechanisms. GLP-1 medications reduce overall caloric intake, producing a generalized fat reduction that includes visceral deposits. The visceral fat loss on semaglutide and tirzepatide is often preferential in the early stages, partly because visceral fat is more metabolically accessible than deep subcutaneous stores. Sermorelin, through GH and IGF-1 elevation, specifically targets visceral adiposity. GH deficiency is characterized by pathologically elevated visceral fat accumulation, and GH restoration through GHRH analogs consistently reduces visceral fat in deficient patients, even without dramatic scale weight changes.
This is why body composition measurements, specifically DEXA scans or body fat percentage measurements, are more informative than scale weight for evaluating sermorelin protocols. A person on sermorelin who loses three pounds of visceral fat while gaining two pounds of muscle has genuinely improved their metabolic health, even though the scale shows only a one-pound difference. For those tracking changes across a GLP-1 protocol, understanding the distinction between fat types also helps interpret tirzepatide before and after results and tirzepatide weight loss results over time.
Bone density considerations
A less-discussed body composition concern with rapid weight loss on GLP-1 medications is bone mineral density. The STEP trials noted modest reductions in bone mineral density alongside the lean mass losses, particularly in postmenopausal women who are already at higher risk for osteoporosis. This is an emerging area of research rather than a settled concern, but it warrants attention for at-risk populations. GH and IGF-1, elevated by sermorelin, play important roles in bone metabolism. GH deficiency is associated with reduced bone mineral density, and GH restoration is used clinically to improve bone density in deficient patients. This suggests another potential complementary benefit of adding sermorelin to GLP-1 protocols, particularly in older populations. For those concerned about bone health in the context of peptide use, the peptides for osteoporosis resource covers the broader landscape of peptide approaches to bone preservation.
Can you combine sermorelin with GLP-1 medications
Yes. And there are good theoretical reasons to consider it.
The mechanisms are completely complementary. GLP-1 receptor agonists drive fat loss through appetite suppression and caloric restriction. Sermorelin drives GH elevation, which promotes muscle protein synthesis and fat mobilization through the IGF-1 pathway. Combining them addresses both sides of the body composition equation simultaneously. You get the powerful fat-loss effect of the GLP-1 medication while preserving, or even building, lean mass through the sermorelin-GH-IGF-1 axis.
There are no known pharmacokinetic interactions between sermorelin and GLP-1 medications. They act through entirely different receptors in different tissues. Sermorelin does not affect GLP-1 receptor activity, and GLP-1 medications do not affect GHRH receptor activity. There is no theoretical basis for a negative interaction. Clinics that specialize in metabolic optimization increasingly offer combination protocols for exactly this reason.
What we lack is large-scale randomized clinical trial data on the combination. The combination approach is used in practice and reported anecdotally with favorable outcomes, but robust clinical evidence specifically for combined sermorelin plus GLP-1 therapy has not been published in peer-reviewed literature as of this writing. That absence of evidence is not evidence of absence. It reflects the clinical reality that research on combination protocols lags significantly behind real-world adoption. For those interested in how sermorelin specifically pairs with tirzepatide, the sermorelin and tirzepatide combination protocol covers the practical considerations in detail. Some users also explore pairing GLP-1 medications with other compounds entirely, such as semaglutide with glycine or tirzepatide with glycine for additional metabolic support.
From a protocol standpoint, the combination involves taking sermorelin at its standard dosing schedule (200-500mcg subcutaneously before bed, daily) while maintaining the GLP-1 medication weekly injection schedule unchanged. There is no dose adjustment required for either compound when adding the other. Some users on combination protocols report that the energy and recovery benefits of sermorelin help offset the fatigue that sometimes accompanies early GLP-1 therapy. Others note that improved sleep quality from the sermorelin-mediated GH pulse supports the metabolic benefits of the GLP-1 medication. These are consistent anecdotal observations without randomized data behind them, but the physiological logic is sound. The peptide stack calculator can help with volume and timing planning when managing multiple compounds.
The main considerations for combining are practical rather than pharmacological: cost, injection frequency, and monitoring. Adding sermorelin to an existing GLP-1 protocol means daily injections alongside weekly GLP-1 injections, increasing the total injection burden. Cost increases, as both compounds require prescriptions and ongoing supply. Lab monitoring should include IGF-1 levels alongside standard GLP-1 monitoring panels to ensure GH is in the optimal range and not supraphysiological. These are manageable considerations for motivated patients with clear goals. The peptide cost calculator helps estimate monthly costs when planning multi-compound protocols.
Practical combination protocol framework
For those seriously considering a combination approach, here is what a structured sermorelin plus GLP-1 protocol typically looks like in real clinical practice.
Start with GLP-1 alone for the first four to eight weeks. Let the GI side effects settle and let dose escalation proceed without adding variables. Once you are stable on your GLP-1 dose and tolerating it well, introduce sermorelin. Beginning sermorelin at a lower dose of 200mcg nightly and holding it there for two to four weeks before increasing to 300-500mcg allows you to assess tolerance and initial response without confounding the picture with multiple changes simultaneously.
Lab work should ideally include a baseline IGF-1 before starting sermorelin and a follow-up IGF-1 at 8-12 weeks to confirm the peptide is producing the expected GH response. Target IGF-1 levels for optimal body composition effects in adults generally fall in the upper quartile of the age-appropriate reference range, not above it. Supraphysiological IGF-1 is not a goal and is associated with potential adverse effects including fluid retention and joint discomfort. If IGF-1 climbs above the upper limit of the reference range, the sermorelin dose should be reduced.
Nutrition strategy matters significantly in combination protocols. GLP-1 medications reduce caloric intake, which helps with fat loss but can make it challenging to consume adequate protein for muscle preservation. The sermorelin-GH-IGF-1 axis makes the body more efficient at using dietary protein for muscle protein synthesis, but there still needs to be adequate protein available. Targeting 1.6-2.0 grams of protein per kilogram of body weight daily is a reasonable approach during combination therapy. The semaglutide diet plan and tirzepatide diet plan resources cover the dietary strategy in the GLP-1 context, which applies equally when adding sermorelin. Specific food choices matter too; the list of foods to eat while on semaglutide and tirzepatide foods to avoid guides help optimize the nutritional side of the equation. For calorie target guidance specifically, calorie targets on semaglutide and calorie targets on tirzepatide provide structured frameworks, and the GLP-1 friendly meals resource translates those targets into practical meal ideas.
Resistance training is the third pillar of any combination protocol aimed at preserving lean mass. Neither sermorelin nor any GLP-1 medication replaces the anabolic stimulus of progressive resistance training. The combination of GLP-1-driven caloric deficit, sermorelin-driven IGF-1 elevation, and resistance training creates the optimal environment for fat loss with muscle preservation. Without the training stimulus, even elevated IGF-1 from sermorelin will not fully offset the muscle loss tendency of deep caloric restriction. For supplementation alongside GLP-1 therapy, the supplements to take with tirzepatide guide and the creatine resources, including creatine and semaglutide, creatine and tirzepatide, and creatine and GLP-1, address how to support muscle during aggressive fat loss phases.
Other peptides people confuse with GLP-1
Sermorelin is not the only peptide that gets incorrectly grouped with GLP-1 receptor agonists. The confusion extends across several other common peptides, and understanding where each one actually sits in the pharmacological taxonomy prevents misdirected expectations.
Ipamorelin
Ipamorelin is a growth hormone-releasing peptide, or GHRP. It does not work through GHRH receptors like sermorelin and does not work through GLP-1 receptors. Ipamorelin binds the ghrelin receptor, GHSR-1a, in the pituitary and other tissues. This receptor activation triggers GH secretion through a different molecular pathway than sermorelin, which is why combining ipamorelin with a GHRH analog like sermorelin produces synergistic GH release rather than redundant stimulation. The two signals work through different receptors and amplify each other. Neither has any GLP-1 receptor activity. The ipamorelin vs CJC-1295 comparison explains the differences between the main GH-releasing peptide options. For a broader view of how different peptide types compare outside of both the GLP-1 and GH axes, the peptides vs SARMs comparison helps distinguish peptide therapy from other performance-oriented compounds.
CJC-1295
CJC-1295 is a GHRH analog, like sermorelin, but with key structural modifications that dramatically extend its half-life. Native GHRH and sermorelin have half-lives measured in minutes. CJC-1295 DAC (with drug affinity complex) has a half-life of approximately one week because the DAC modification allows it to bind serum albumin and be released slowly. This extended half-life means CJC-1295 stimulates more continuous rather than pulsatile GH release, which has trade-offs. CJC-1295 is not a GLP-1 receptor agonist. It works through GHRH receptors, exactly like sermorelin, just for much longer. The CJC-1295 dosage calculator helps with volume calculations when using this longer-acting GHRH analog.
Tesamorelin
Tesamorelin is another GHRH analog. It represents the complete 44-amino-acid GHRH sequence with a modification that extends its half-life. It is FDA approved for reducing visceral adiposity in HIV-positive patients with lipodystrophy, making it the only GHRH analog with a specific approved adult indication beyond pediatric GH deficiency. Tesamorelin has been studied more extensively than sermorelin for fat reduction, with the phase 3 trials showing significant visceral fat reduction over 26 weeks. It is not a GLP-1 receptor agonist. Its mechanism is identical to sermorelin in principle, working through GHRH receptors on pituitary somatotrophs to drive GH release.
BPC-157 and TB-500
BPC-157 and TB-500 are healing and repair peptides. BPC-157, the 15-amino-acid fragment of body protection compound, promotes angiogenesis, modulates nitric oxide pathways, and accelerates tissue repair. TB-500, a fragment of thymosin beta-4, promotes actin polymerization and cell migration. Neither has GLP-1 receptor activity, GH-releasing activity, or any direct metabolic effect on weight or appetite. They appear in the weight management context only because they are sometimes combined with other protocols for systemic health support, not because they address weight or appetite through any mechanism resembling GLP-1. The peptides for gut health guide covers where BPC-157 genuinely fits in gut-related protocols.
AOD-9604
AOD-9604 is a fragment of the human growth hormone molecule, specifically amino acids 177-191, sometimes called the fat-burning fragment of HGH. It was developed specifically because this region of the HGH molecule appears to mediate the lipolytic effects without the anabolic or glucose-regulating effects of full HGH. AOD-9604 is not a GLP-1 receptor agonist and does not work through any incretin pathway. It also has no GHRH receptor activity. For broader context on peptides designed for fat loss, that guide maps where AOD-9604 fits. For those comparing it to GLP-1 medications directly, the AOD-9604 vs semaglutide comparison is the appropriate reference, not the present article.
Is phentermine a GLP-1?
Since this article targets the "is X a GLP-1" question format, it is worth briefly addressing phentermine in the same framing. Phentermine is not a GLP-1 receptor agonist. It is a sympathomimetic amine, structurally related to amphetamine, that suppresses appetite through central nervous system stimulation and catecholamine release. It has a completely different mechanism than both sermorelin and GLP-1 medications. The question comes up because phentermine also shows up on weight management clinic formularies alongside GLP-1 medications, sometimes in combination. The is phentermine a GLP-1 article answers that question directly, and phentermine vs semaglutide covers the comparison in detail. Some providers do combine them; see whether you can take phentermine and semaglutide together for the relevant considerations.
Liraglutide and other older GLP-1 medications
Liraglutide (Saxenda, Victoza) is an older GLP-1 receptor agonist with a shorter half-life than semaglutide, requiring daily rather than weekly injections. It is not sermorelin and does not work through the GH axis. It uses the same GLP-1R mechanism as semaglutide but with lower efficacy for weight loss, approximately 5-8% compared to semaglutide 15-17%. The difference between semaglutide and liraglutide explains why semaglutide has largely displaced liraglutide as the preferred GLP-1 agent in weight management. Neither liraglutide nor semaglutide shares any mechanism with sermorelin. For those considering GLP-1 medications from a financial coverage perspective or HSA eligibility for GLP-1 medications, the cost considerations differ significantly between prescription GLP-1 agents and compounded sermorelin.
Complete comparison: sermorelin vs GLP-1 medications
Factor | Sermorelin | Semaglutide | Tirzepatide | Retatrutide |
|---|---|---|---|---|
Peptide class | GHRH analog | GLP-1R agonist | GLP-1R / GIP dual agonist | GLP-1R / GIP / glucagon triple agonist |
Target receptor | GHRH-R on pituitary | GLP-1R in gut, brain, pancreas | GLP-1R + GIPR | GLP-1R + GIPR + glucagon-R |
Primary indication | GH deficiency (off-label adult) | Obesity, type 2 diabetes | Obesity, type 2 diabetes | Obesity (phase 3) |
Weight loss magnitude | 2-5% (recomposition) | 15-17% | 20-22.5% | ~24% |
Muscle impact | Positive (promotes lean mass) | Negative (39% of loss is lean) | Moderately negative | Under study (concern exists) |
Appetite suppression | None directly | Strong | Very strong | Very strong |
Dosing schedule | Daily subcutaneous injection | Weekly subcutaneous injection | Weekly subcutaneous injection | Weekly subcutaneous injection |
Dose range | 200-500mcg/day | 0.25mg to 2.4mg/week | 2.5mg to 15mg/week | 0.5mg to 12mg/week (protocol-dependent) |
Main side effects | Injection site reaction, headache | Nausea, vomiting, constipation | Nausea, vomiting, constipation | Nausea, GI distress |
GH axis impact | Raises GH and IGF-1 | None | None | None |
Blood glucose effect | Mild improvement via IGF-1 | Strong glycemic control | Strongest glycemic control | Strong glycemic control |
FDA approved for adults | No (compounding pharmacies) | Yes (Ozempic, Wegovy) | Yes (Mounjaro, Zepbound) | No (phase 3 trials) |
Combination potential | Combines well with GLP-1 | Can combine with sermorelin | Can combine with sermorelin | Combination data limited |
Best for | GH deficiency, aging, muscle, mild fat loss | Significant weight loss, T2D | Maximum weight loss, T2D | Maximum weight loss (experimental) |
This table represents the clearest single-view comparison available. Use it to orient the decision, not to make it. The right choice depends on factors beyond any table: your current health status, your lab values, your goals, your physician guidance, and your personal tolerance for different side effect profiles. SeekPeptides members access detailed protocol comparisons, evidence summaries, and member experiences that go beyond what any general guide can offer.
Who should choose sermorelin over GLP-1
Sermorelin is the better choice in specific clinical and personal situations.
Growth hormone deficiency is the most clear-cut indication. If lab work shows low IGF-1 and clinical symptoms of GH deficiency, including fatigue, poor sleep, decreased lean mass, increased visceral fat, reduced recovery, and cognitive fog, sermorelin addresses the root cause directly. GLP-1 medications do not treat GH deficiency. They might help the weight component, but they leave the underlying deficiency untreated. Starting with sermorelin (or a GHRH analog like tesamorelin or CJC-1295) makes more sense when the primary diagnosis is GH deficiency rather than obesity per se.
Anti-aging and longevity goals without significant obesity align better with sermorelin. Someone who is moderately overweight but primarily concerned about the effects of aging, declining recovery, muscle loss, cognitive changes, and sleep degradation will benefit more from sermorelin than from GLP-1 medications, which are primarily weight loss and diabetes drugs. The peptides for anti-aging resource covers the full landscape of compounds relevant to longevity goals.
Muscle preservation priority is a strong argument for sermorelin. Competitive athletes, bodybuilders, older adults managing sarcopenia, and anyone for whom maintaining or building lean mass is a primary goal should approach GLP-1 medications with caution as a standalone tool. Sermorelin actively promotes lean mass while facilitating gradual fat loss, making it appropriate for body recomposition goals where the scale number matters less than the ratio of muscle to fat. The peptides for muscle growth guide explains how GH-axis stimulation contributes to long-term muscle development.
Those who cannot tolerate GLP-1 side effects may find sermorelin more manageable. For individuals who experience severe nausea, persistent GI distress, or other significant side effects on GLP-1 medications even at low doses, sermorelin offers a gentler metabolic improvement pathway. The results are less dramatic and slower, but the tolerance is considerably better for most users. This is not a direct substitution, since the mechanisms differ, but for someone whose primary concern is general metabolic health and gradual fat reduction rather than rapid weight loss, sermorelin is a viable alternative.
Finally, someone already at a healthy weight who wants to optimize recovery, sleep, and body composition will find more utility in sermorelin than in GLP-1 medications, which are designed for overweight and obese populations and can cause excessive weight loss in already-lean individuals. GLP-1 medications suppress appetite regardless of whether the user needs to lose weight. Sermorelin improves GH axis function regardless of starting weight and is appropriate across a wider range of baseline weights. For those considering whether semaglutide gives energy, the answer is mixed, and many users find sermorelin delivers more consistent energy improvements through the GH pathway.
Hormonal health contexts also make sermorelin more relevant in some cases. For individuals on hormone replacement therapy, the interaction between HRT and GLP-1 medications is an emerging consideration. The HRT and GLP-1 together guide covers these interactions. Sermorelin, by restoring GH axis function, complements rather than interferes with sex hormone optimization. For individuals managing thyroid conditions, the tirzepatide and levothyroxine interaction and broader endocrine health contexts are worth understanding before combining any peptide protocols with thyroid medications. For those managing autoimmune conditions, tirzepatide and autoimmune disease is another consideration when choosing between peptide classes. Some autoimmune conditions, including Hashimoto thyroiditis, have specific GLP-1 considerations covered in the GLP-1 for Hashimoto disease guide.
Who should choose GLP-1 over sermorelin
GLP-1 receptor agonists are the stronger choice in other situations.
Significant weight loss needs, typically defined as 50 or more pounds to lose, or a BMI above 30, represent the clearest indication for GLP-1 medications. The clinical evidence for GLP-1-mediated weight loss is overwhelming, multi-center, multi-country, and published in the highest-impact journals. Sermorelin does not produce 15-22% body weight reduction. GLP-1 medications do, reliably and reproducibly, in clinical settings. If scale weight reduction is the primary clinical need, GLP-1 is the appropriate tool.
Type 2 diabetes management is an established indication where GLP-1 medications have proven, FDA-approved utility. Even the newer agents entering the space, like mazdutide and cagrilintide, build on this GLP-1 foundation rather than the GH axis. Semaglutide reduces HbA1c by 1.5-2 percentage points on average and reduces cardiovascular events in high-risk patients with type 2 diabetes. Sermorelin has no established utility for glycemic management in type 2 diabetes. This is not a close call. GLP-1 medications for T2D management represent one of the most significant pharmacological advances in endocrinology in decades. For women navigating hormonal complexity alongside weight management, specific GLP-1 considerations like semaglutide effects on periods, tirzepatide effects on periods, and tirzepatide sexual side effects are worth understanding before committing to a protocol. Sermorelin does not produce these reproductive or sexual side effects.
Strong appetite suppression needs, independent of the weight loss goal itself, favor GLP-1 medications. For individuals who struggle with food cravings, emotional eating, hyperphagia, or simply find that hunger overrides their best dietary intentions, the hypothalamic GLP-1R activation that drives "food noise" reduction is genuinely life-changing. Sermorelin does not suppress appetite through any mechanism. The appetite suppression timeline on semaglutide shows how quickly this effect arrives for most users.
Clinical evidence priority also favors GLP-1 medications for risk-averse patients or those with complex medical histories who need the security of large-scale safety data. The STEP trials, SURMOUNT trials, SELECT cardiovascular outcomes trial, and SUSTAIN series represent hundreds of thousands of patient-years of data across diverse populations. Sermorelin clinical evidence, while positive, operates at a much smaller scale. For a patient who needs to show robust evidence of safety and efficacy before committing to a protocol, GLP-1 medications have the more convincing data package.
Comparing specific GLP-1 medication options is also worth thinking through carefully. The decision between semaglutide and tirzepatide, for example, involves looking at the comparative side effect profiles and individual health goals. For those considering compounded versions, compounded semaglutide is a practical option worth understanding in full detail, including storage requirements, how long compounded semaglutide lasts in the fridge, and refrigeration requirements for compounded semaglutide.
For those who have hit a plateau on GLP-1 therapy, the reasons are worth understanding before switching peptide classes. The why you might not be losing weight on semaglutide and why you might not be losing weight on tirzepatide guides cover the most common protocol and dietary factors that limit results. Sometimes the answer is not switching to a different peptide class but optimizing the GLP-1 protocol you are already on. Questions like four weeks on semaglutide with no weight loss are common enough to warrant specific attention. For those whose GLP-1 journey is reaching its endpoint and thinking about the long-term, the how long to stay on semaglutide guide and the GLP-1 maintenance dose considerations are important planning tools. When transition off GLP-1 therapy becomes appropriate, sermorelin is worth serious consideration as a long-term metabolic maintenance tool, using the GH axis to sustain the metabolic improvements achieved through GLP-1-driven fat loss.
Dosing and administration comparison
Understanding how each compound is administered helps clarify what the practical experience of using them actually looks like day to day.
Sermorelin dosing protocol
Standard sermorelin dosing runs 200-500mcg per injection, administered subcutaneously once daily. The most common approach is a single bedtime injection to align with the natural sleep-associated GH pulse. Some protocols use 200mcg nightly for beginners and advance to 300-500mcg as tolerance is established and response is assessed. The peptide is supplied as a lyophilized powder that requires reconstitution with bacteriostatic water. For volume calculations when reconstituting sermorelin or similar peptides, the peptide reconstitution calculator takes the guesswork out of the math. Injection sites include the abdomen, thigh, or upper arm, rotating to avoid tissue fatigue. Storage after reconstitution requires refrigeration at 2-8 degrees Celsius, generally stable for 20-30 days depending on the formulation. Similar storage principles apply to GLP-1 medications. Understanding compounded semaglutide refrigeration and whether tirzepatide can go bad is important for anyone maintaining a multi-compound protocol.
Semaglutide dosing protocol
Semaglutide at the 2.4mg maintenance dose (Wegovy for obesity) follows a structured escalation. Week 1-4: 0.25mg weekly. Week 5-8: 0.5mg weekly. Week 9-12: 1.0mg weekly. Week 13-16: 1.7mg weekly. Week 17 and beyond: 2.4mg weekly. For some patients, the escalation is slowed if side effects are significant at any step. The semaglutide dosage in units guide translates these milligram doses to insulin syringe unit measurements for compounded preparations. The semaglutide dosage calculator simplifies the dose volume calculations.
Semaglutide for compounded preparations requires reconstitution and the same refrigeration as sermorelin. Understanding how to reconstitute 5mg semaglutide and how much bacteriostatic water to mix with 10mg semaglutide are fundamental for those using compounded supply. The best time of day to take semaglutide covers timing optimization to minimize side effects.
Tirzepatide dosing protocol
Tirzepatide escalates from 2.5mg weekly (first four weeks) to 5mg weekly, then 7.5mg, 10mg, 12.5mg, and 15mg, each dose level held for four weeks minimum before advancing. The tirzepatide dosing in units converts the milligram doses to unit measurements for compounded tirzepatide, and the microdosing tirzepatide chart covers alternative approaches for those who prefer slower escalation than the standard protocol. For the complete escalation reference, the tirzepatide compound dosage chart is the primary reference.
Retatrutide dosing protocol
Retatrutide is not yet FDA approved, so dosing comes from clinical trial protocols and emerging real-world compounded use. Phase 2 trial protocols used dose escalation from 0.5mg to 12mg over several months. For current reference on retatrutide dosing, retatrutide dosage chart and retatrutide dose complete guide cover what is known from trial data and emerging protocols. Storage guidelines for retatrutide follow similar principles to semaglutide and tirzepatide, covered in dedicated storage guides.
The practical difference in injection burden between sermorelin and GLP-1 medications is notable. Sermorelin requires daily injections, meaning 365 injections per year. GLP-1 medications require weekly injections, meaning 52 injections per year. For someone averse to frequent injections, the weekly GLP-1 schedule is considerably more convenient. Those combining both accept the daily sermorelin injection plus weekly GLP-1 injection as the price of addressing both sides of body composition simultaneously. Tracking injections across multiple compounds can be managed with the GLP-1 injection tracking guide for the GLP-1 component. For monitoring progress visually, the GLP-1 plotter and GLP-1 monitoring tools for home use can help assess whether your protocol is delivering the expected results. Understanding whether to take GLP-1 a day early or take semaglutide every other week during maintenance phases is also relevant for long-term protocol flexibility.
Frequently asked questions
Is sermorelin the same as semaglutide?
No. Sermorelin and semaglutide are completely different compounds with different mechanisms, different targets, and different clinical outcomes. Sermorelin is a GHRH analog that stimulates the pituitary to release growth hormone. Semaglutide is a GLP-1 receptor agonist that suppresses appetite and slows gastric emptying to produce weight loss. The only things they share are that both are peptides and both are injectable. For a direct comparison of the two agents as weight loss options, the AOD-9604 vs semaglutide comparison also helps illustrate how different peptide classes behave versus GLP-1 medications.
Does sermorelin suppress appetite like Ozempic?
No. Sermorelin does not suppress appetite through any direct mechanism. Some users report modestly reduced appetite as a secondary effect of improved GH levels and metabolic function, but this is not a primary effect and is not comparable to the dramatic "food noise" reduction produced by semaglutide through hypothalamic GLP-1R activation. If appetite suppression is your primary goal, semaglutide or tirzepatide are the appropriate tools. For the timeline of semaglutide appetite suppression, how long semaglutide takes to work covers what to expect week by week.
Can I take sermorelin and semaglutide at the same time?
Yes. There are no known pharmacological interactions between sermorelin and semaglutide or tirzepatide. They act through entirely different receptors in different tissues. Many clinics prescribe combination protocols specifically to leverage the fat-loss effect of GLP-1 medications alongside the muscle-preserving and GH-restorative effects of sermorelin. Cost and injection frequency increase with the combination. Lab monitoring should include IGF-1 levels to confirm sermorelin is producing the expected GH response. The sermorelin and tirzepatide combination guide covers the practical protocol in detail.
Which produces more weight loss, sermorelin or GLP-1?
GLP-1 receptor agonists produce dramatically more scale weight loss. Semaglutide produces 15-17% average body weight reduction. Tirzepatide produces up to 22.5%. Sermorelin produces gradual body recomposition with modest scale weight changes, typically 2-5% over months, with improvements in lean mass that the scale does not capture. If scale weight reduction is your primary metric, GLP-1 medications are substantially more effective. If body composition quality (muscle-to-fat ratio) is your primary metric, sermorelin or sermorelin combined with GLP-1 produces superior results. The average GLP-1 weight loss per month puts the numbers in practical context.
Is sermorelin safer than GLP-1 medications?
The side effect profiles are different rather than one being universally safer. Sermorelin has a milder side effect profile with primarily injection site reactions and occasional mild headache. GLP-1 medications carry more prominent GI side effects, particularly early in therapy. The somatostatin negative feedback mechanism gives sermorelin an inherent safety advantage against GH excess. GLP-1 medications have the advantage of extensive large-scale clinical trial safety data, including cardiovascular outcomes data. Neither is "safer" in absolute terms; the right choice depends on the individual health context and what risks are most relevant. For those considering stopping GLP-1 therapy and its effects, semaglutide withdrawal symptoms and getting off GLP-1 cover the cessation experience. Mental health side effects can also factor into the decision, with tirzepatide anxiety and tirzepatide brain fog reported by some users. Sermorelin does not produce these neurological side effects because it does not act on hypothalamic feeding circuits.
What is the difference between sermorelin and ipamorelin?
Both sermorelin and ipamorelin stimulate GH release but through different receptors. Sermorelin binds GHRH receptors (works like the hypothalamus natural signal). Ipamorelin binds ghrelin receptors (GHSR-1a), which is a separate GH-releasing pathway. They are complementary rather than redundant, which is why they are often combined in sermorelin ipamorelin blends. Neither is a GLP-1 receptor agonist. Both work entirely in the GH axis.
Do you need a prescription for sermorelin?
Yes. Sermorelin is a prescription peptide hormone in the United States. It is available through compounding pharmacies with a valid prescription from a licensed physician. The prescribing context is typically an anti-aging clinic, functional medicine practice, or endocrinology office that monitors labs including IGF-1 levels. GLP-1 medications (semaglutide, tirzepatide) also require prescriptions. Neither sermorelin nor GLP-1 medications are available legally without a prescription in the United States.
How long does it take sermorelin to work versus GLP-1?
GLP-1 medications produce appetite suppression within days to weeks of starting. Meaningful weight loss typically begins within the first four to eight weeks. Sermorelin produces early improvements in sleep and energy within two to four weeks. Meaningful body composition changes, including measurable lean mass increases and fat reduction, typically require three to six months of consistent use. The sermorelin before and after timeline documents what users typically report at each phase of a protocol.
External resources
New England Journal of Medicine: STEP 1 trial, once-weekly semaglutide in adults with obesity
New England Journal of Medicine: SURMOUNT-1 trial, tirzepatide for the treatment of obesity
Endocrine Society: growth hormone and IGF-1 patient education
StatPearls: GLP-1 receptor agonists, mechanism and clinical use
FDA drug information: Wegovy (semaglutide) approval and trial data
For researchers who want to go deeper on any of the protocols, comparisons, or decision frameworks covered in this guide, SeekPeptides offers comprehensive member resources, including detailed protocol libraries, evidence summaries, lab interpretation guides, and a community of experienced researchers who have navigated these exact questions. When you are choosing between peptide classes, making informed decisions rather than assumption-based ones, membership access to structured, evidence-grounded guidance is worth more than any single article, including this one.
In case I do not see you, good afternoon, good evening, and good night. May your peptide research stay evidence-based, your protocols stay well-informed, and your results stay aligned with your actual goals.