Mar 24, 2026

Before you write off that 3 a.m. calf cramp as a random annoyance, read this. Because if you are on semaglutide and your legs are seizing up in the middle of the night, there is a reason. And that reason probably has nothing to do with your mattress, your exercise routine, or bad luck.
Leg cramps are one of the most underreported side effects of semaglutide therapy. They do not appear in FDA prescribing information as a recognized adverse event. Clinical trials did not flag them at significantly higher rates than placebo. Yet thousands of people on GLP-1 receptor agonists report the same thing: painful, involuntary muscle contractions that wake them from sleep, strike during walks, or grip their calves without warning.
The disconnect between official labeling and lived experience exists because leg cramps are not a direct pharmacological effect. They are an indirect consequence of what semaglutide does to your gastrointestinal system, your kidney function, your electrolyte balance, and your body composition. Understanding that chain of events is the difference between suffering through cramps for months and preventing them entirely.
This guide covers every mechanism behind semaglutide leg cramps, the specific electrolyte depletions that trigger them, the supplement protocols that actually work, and the warning signs that mean your cramps are signaling something far more serious. Whether you are in your first week on semaglutide or months into treatment, this is the resource you will wish someone had given you on day one.
Why semaglutide causes leg cramps
Semaglutide does not directly cause muscle cramps. No receptor pathway links GLP-1 activation to involuntary muscle contraction. But semaglutide triggers a cascade of physiological changes that create the perfect conditions for cramping, and understanding each link in that chain matters if you want to break it.
Three primary mechanisms connect semaglutide to leg cramps. Each one is well-documented. Together, they explain why so many people experience this problem even though clinical trials did not catch it.
The gastrointestinal trigger pathway
This is where everything starts. Semaglutide slows gastric emptying, enhances intestinal motility, and triggers the nausea-vomiting-diarrhea triad that dominates early treatment. Pooled analysis of the STEP clinical trials revealed the scope of this problem: 43.9% of semaglutide users experienced nausea compared to 16.1% on placebo. Dizziness and diarrhea affected 29.7% versus 15.9%. Vomiting hit 24.5% versus 6.3%.
Those are not small numbers.
Every episode of vomiting strips your body of 20 to 80 milliequivalents of sodium and 10 to 30 milliequivalents of potassium. Every bout of diarrhea flushes 50 to 100 milliequivalents of sodium along with significant magnesium and potassium. And these episodes cluster during dose escalation, which means the electrolyte losses are heaviest exactly when your body is adjusting to the medication.
The GI side effects peak during the first weeks at each new dose and typically plateau after week 20 of treatment. Median nausea duration is about 8 days per escalation step. Median diarrhea duration runs about 3 days. Vomiting averages 2 days. But for some people, particularly those who escalate too quickly, these symptoms persist longer and drain more minerals than the body can replenish through diet alone. Constipation affected 24.2% of users as well, and while it does not cause direct electrolyte loss the way vomiting and diarrhea do, it contributes to the overall GI disruption that reduces nutrient absorption.
If you are dealing with bloating, burping, acid reflux, or sulfur burps alongside your leg cramps, those symptoms are all connected through this same GI disruption pathway.
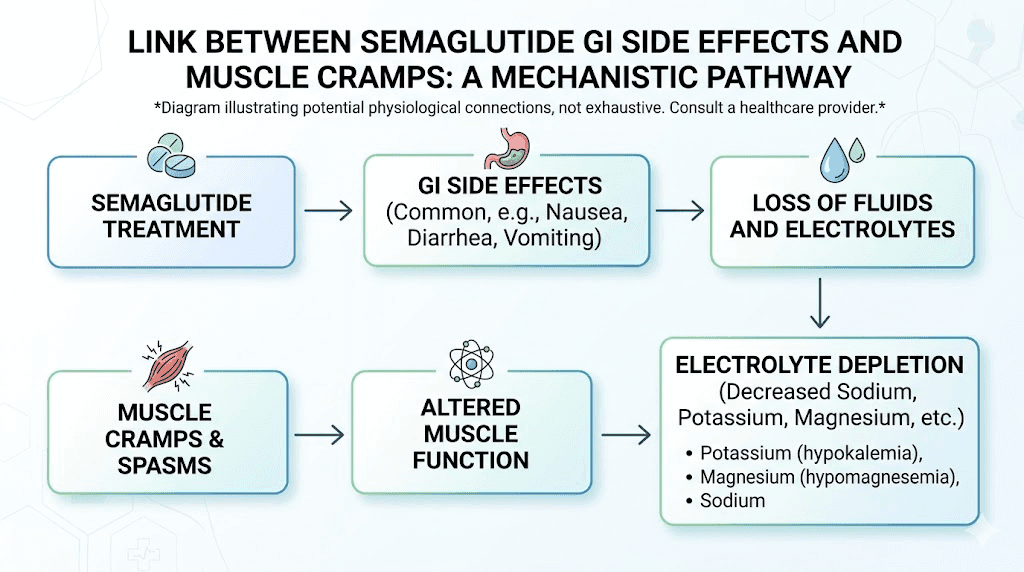
Electrolyte depletion mechanisms
Your muscles run on electricity. That is not a metaphor. Muscle contraction and relaxation depend on the precise balance of electrically charged minerals moving across cell membranes. Sodium initiates nerve signals. Potassium stabilizes muscle cell electrical activity. Magnesium enables muscle relaxation after contraction. Calcium triggers the contraction itself.
Disrupt any of these, and cramps follow.
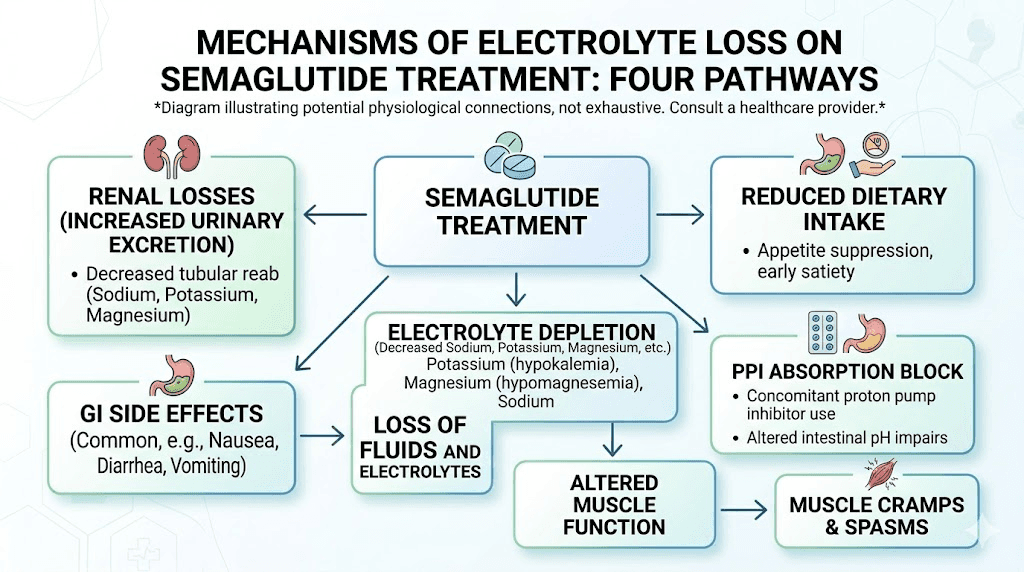
Semaglutide disrupts all of them simultaneously through multiple pathways. The GI losses described above are the most obvious route, but they are not the only one. Appetite suppression, which is the therapeutic effect people want, reduces total food intake. Less food means fewer dietary minerals. Someone eating 1,200 calories instead of 2,000 is getting roughly 40% fewer electrolytes from their diet, even if they are making excellent food choices.
This is why understanding how many calories to eat on semaglutide matters beyond just weight loss. Caloric restriction without mineral supplementation creates a deficit that the body cannot sustain without consequences. And those consequences often show up first as muscle cramps, particularly in the calves and feet where circulation is most distant from the heart.
Roughly 48% of Americans are already deficient in magnesium before starting any medication. Layer semaglutide-induced GI losses and reduced food intake on top of a pre-existing deficiency, and leg cramps become almost inevitable for a significant portion of users.
The renal sodium loss factor
Here is something most guides on this topic completely miss. Semaglutide does not just cause electrolyte loss through the gut. It actively increases sodium excretion through the kidneys.
GLP-1 receptor activation inhibits a protein called NHE3, the sodium-hydrogen exchanger 3, in the proximal tubule of the kidney. This means your kidneys start dumping more sodium into the urine than they normally would. The result is natriuresis, increased sodium excretion, which pulls water along with it and contributes to both dehydration and electrolyte imbalance from a completely different direction than the GI pathway.
GLP-1 also modulates the epithelial sodium channel in the distal nephron, adding another layer of renal sodium loss. This dual mechanism, gut losses plus kidney losses, explains why electrolyte depletion on semaglutide can be more severe than you might expect from GI symptoms alone.
For people also taking metformin alongside semaglutide, the renal effects can compound. Both medications affect kidney handling of minerals, and the combination deserves extra attention to hydration and electrolyte status.
The electrolyte crisis most guides ignore
Most articles about semaglutide leg cramps tell you to drink more water and eat a banana. That advice is not wrong. It is just woefully incomplete. The electrolyte dynamics at play during GLP-1 therapy are far more complex than simple dehydration, and understanding them can be the difference between managing cramps and eliminating them.
Magnesium, the muscle mineral
Magnesium is involved in over 300 enzymatic reactions in the human body. It is absolutely critical for muscle relaxation. When magnesium levels drop, muscles contract but struggle to fully relax. That incomplete relaxation is what you experience as a cramp.
The recommended daily intake of magnesium is 310 to 320 milligrams for women and 400 to 420 milligrams for men. Normal serum levels run between 1.7 and 2.2 milligrams per deciliter. But here is the problem with testing: only 1% of your total body magnesium circulates in the blood. You can have a normal serum magnesium level and still be profoundly deficient at the cellular level. Red blood cell magnesium testing is more accurate but rarely ordered.
A published case report demonstrates how extreme this can get. A 73-year-old woman on semaglutide 0.25 to 0.5 milligrams presented with serum magnesium that was literally undetectable, below 0.3 millimoles per liter against a normal range of 0.7 to 1.1. She had been experiencing longstanding muscle cramps for months before she suddenly collapsed while making tea, sustaining head injuries and burns. Her calcium was also critically low at 0.85 millimoles per liter ionized, well below the normal 1.15 to 1.30 range.
After intravenous electrolyte replacement, her levels normalized within 8 hours. And her chronic muscle cramps, the ones she had been ignoring, resolved completely.
That case is extreme. But it illustrates a critical point: chronic, low-grade magnesium depletion can simmer for months as nothing more than annoying leg cramps before it becomes a medical emergency.
The potassium-magnesium connection
This is the detail that changes everything about how you approach electrolyte supplementation.
Magnesium deficiency often causes potassium depletion. That is well established. But here is the critical part: you cannot correct potassium levels until magnesium is restored first. Supplementing potassium without addressing magnesium is like pouring water into a bucket with a hole in it. The potassium will not stay where it belongs because magnesium is required for the cellular pumps that keep potassium inside cells.
This means someone experiencing leg cramps who takes a potassium supplement but ignores magnesium will often see no improvement. The fix has to start with magnesium. Then potassium levels will correct, sometimes without any additional potassium supplementation at all.
Normal serum potassium runs between 3.5 and 5.0 milliequivalents per liter. Levels below 3.0 become critical and can cause cardiac arrhythmias. For GLP-1 users experiencing significant GI side effects, monitoring both magnesium and potassium through blood work is important, especially during dose escalation phases when fatigue and muscle symptoms are most common.
When PPIs compound the problem
Many semaglutide users take proton pump inhibitors to manage the acid reflux and nausea that accompany treatment. This creates a compounding problem that most people and many prescribers do not recognize.
PPIs decrease the activity of a protein called TRPM6 in the intestinal lining. TRPM6 is responsible for actively absorbing magnesium from food. When PPI use suppresses this channel, intestinal magnesium absorption drops significantly. The FDA issued a specific safety communication about the association between long-term PPI use and low magnesium levels.
So the picture looks like this: semaglutide causes GI losses of magnesium. It causes renal losses of sodium. Appetite suppression reduces dietary mineral intake. And the PPI prescribed to manage semaglutide side effects blocks one of the primary pathways for absorbing whatever magnesium does make it into the gut.
If you are on both semaglutide and a PPI and experiencing leg cramps, this combination is very likely your culprit. Talk to your provider about magnesium supplementation and potentially switching from a PPI to an H2 blocker, which does not carry the same magnesium absorption risk.
How much electrolyte loss actually happens
Vague warnings about dehydration do not help anyone. Specific numbers do. Here is what the research tells us about the actual mineral losses that occur during GLP-1 therapy.
What GI side effects cost your body
A single severe day of GI symptoms, six to eight vomiting episodes plus eight to twelve diarrhea episodes, can strip the body of 3 to 5 liters of fluid, 500 to 800 milliequivalents of sodium, and 200 to 400 milliequivalents of potassium. That is an extreme scenario, but even moderate GI symptoms create meaningful deficits over time.
Consider someone with mild nausea who skips breakfast and eats a reduced lunch and dinner. They might be getting 250 milligrams of magnesium from food instead of 350. Add two episodes of diarrhea per week, each flushing additional magnesium and potassium. Over four to six weeks of dose escalation, the cumulative deficit becomes substantial even without dramatic symptoms.
This slow drain is actually more dangerous than acute losses because it flies under the radar. A violent stomach bug sends people to the hospital for IV fluids. But gradual depletion from semaglutide GI effects just manifests as persistent fatigue, muscle cramps, poor sleep, and headaches that people chalk up to the medication itself rather than a fixable mineral deficiency.
Clinical trial numbers that matter
The STEP trials provide the most comprehensive data on semaglutide side effects. Here are the numbers relevant to understanding cramp risk:
Any adverse event occurred in 89.7% of semaglutide users versus 86.4% on placebo. GI disorders specifically affected 74.2% of semaglutide users versus 47.9% on placebo. That is a massive gap. Three out of four people on semaglutide experienced some form of GI disruption.
Severe GI events occurred in 4.1% of semaglutide users versus 0.9% on placebo. Treatment discontinuation due to GI events happened in 4.3% of participants. And the risk appears dose-dependent, with higher incidence at the 2.4 milligram dose used for weight management compared to the lower doses used for diabetes.
These numbers tell us that the vast majority of semaglutide users will experience some degree of GI disruption, and therefore some degree of electrolyte loss. The question is not whether it happens but how much it happens and whether you are replenishing what you lose. Proper dosing and a careful dose escalation schedule can minimize GI severity, but cannot eliminate it entirely.
Lean mass loss and muscle vulnerability
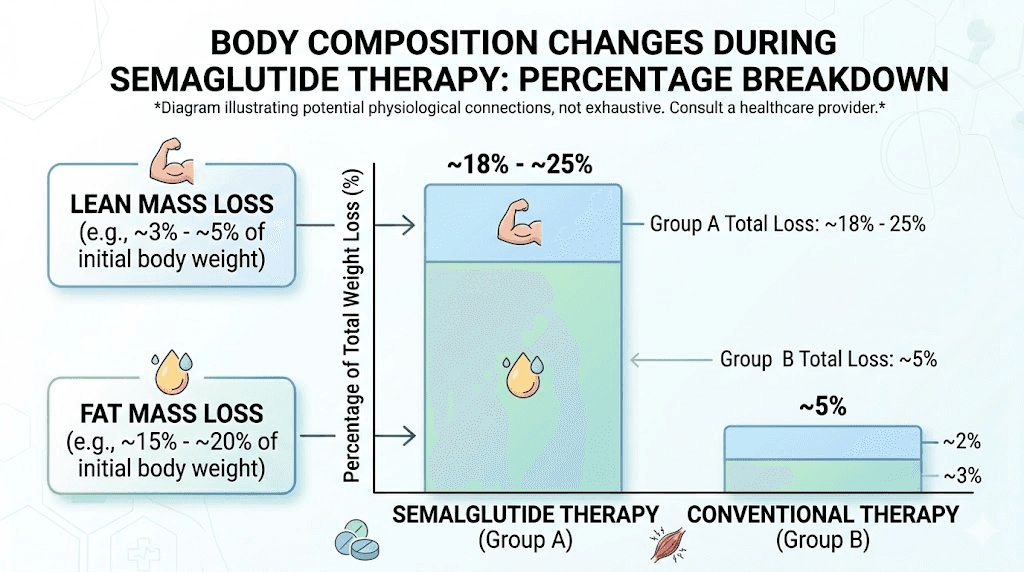
There is another factor that receives far too little attention in discussions about semaglutide and leg cramps. Weight loss on GLP-1 therapy does not come exclusively from fat.
STEP trial body composition data
The STEP 1 DEXA substudy measured exactly where the weight loss came from. Total weight loss averaged 15.0%. Fat mass decreased by 19.3%. Visceral fat dropped an impressive 27.4%. But lean body mass also decreased by 9.7%.
Across GLP-1 weight loss studies, lean mass accounts for approximately 25% to 40% of total weight lost. That means someone who loses 30 pounds might lose 7 to 12 pounds of muscle along with the fat. The proportion of lean mass to total body mass actually improved by about 3 percentage points, which is good news for body composition ratios. But the absolute loss of muscle tissue has consequences.
This matters for semaglutide results beyond just the number on the scale. Understanding body composition changes helps explain why adequate protein intake on semaglutide is critical for long-term outcomes.
Why weakened muscles cramp more
Muscles that have lost mass are more susceptible to cramping. They fatigue faster under the same workload. They generate more metabolic waste relative to their capacity. And they have fewer reserves of intracellular minerals to buffer against electrolyte fluctuations.
Additionally, many people who lose significant weight on semaglutide increase their physical activity. Someone who was sedentary at 250 pounds might start walking regularly at 220 pounds. That increased activity is excellent for health but places new demands on muscles that are simultaneously losing mass. The combination of reduced muscle tissue, increased activity, and electrolyte depletion creates a triple threat for cramping.
This is why protein supplementation and resistance training are not optional extras during GLP-1 therapy. They are protective measures against both muscle loss and the cramping that comes with it. Combining adequate protein with creatine supplementation may offer additional muscle-protective benefits, though you should discuss any supplement additions with your healthcare provider.
When leg cramps signal something serious
Most semaglutide-related leg cramps are uncomfortable but harmless. They respond to electrolyte supplementation, hydration, and time. But in rare cases, leg cramps can be the first warning sign of a dangerous condition that requires immediate medical attention.
Rhabdomyolysis case reports
Rhabdomyolysis is the breakdown of muscle tissue that releases a protein called myoglobin into the bloodstream. Myoglobin can damage the kidneys and, in severe cases, cause kidney failure. The condition carries a mortality rate of up to 8% and causes acute renal failure in 10% to 30% of cases.
Two published case reports document rhabdomyolysis associated with semaglutide therapy.
The first case involved a 47-year-old woman who had tolerated liraglutide (another GLP-1 agonist) for five months without issues. After switching to semaglutide at 1.7 milligrams weekly, she developed symptoms after just two doses. Her creatine kinase level, the primary marker of muscle breakdown, reached 2,619 units per liter. Normal range is 26 to 192. Her AST, a liver enzyme that also rises with muscle damage, hit 73 units per liter against a normal ceiling of 43.
She presented with burning skin, muscle pain in her right shoulder and flank, diffuse weakness so severe she had difficulty rising from bed, along with diarrhea, nausea, and chills. After discontinuation, her CK normalized to 354 within four days. When she was later rechallenged at lower doses, she tolerated 0.5 and 1.0 milligrams. But symptoms recurred at 1.7 milligrams, this time with myoglobin appearing in her urine.
The second case was more severe. A 36-year-old man had his dose rapidly escalated to 2.4 milligrams over approximately one month, far faster than the recommended four-week intervals between increases. Six days after reaching the highest dose, he developed bilateral lower extremity cramping rated 9 out of 10 in severity, with dark urine for 24 hours. His CK peaked at 25,000 units per liter. His blood pressure was elevated at 147/92 and heart rate was 111. Aggressive IV hydration resolved the crisis, and he later tolerated semaglutide at 0.25 milligrams without recurrence.
These cases are rare. But they carry an important lesson: dose matters, escalation speed matters, and severe muscle pain with dark urine is a medical emergency, not something to push through.
Warning signs that need immediate attention
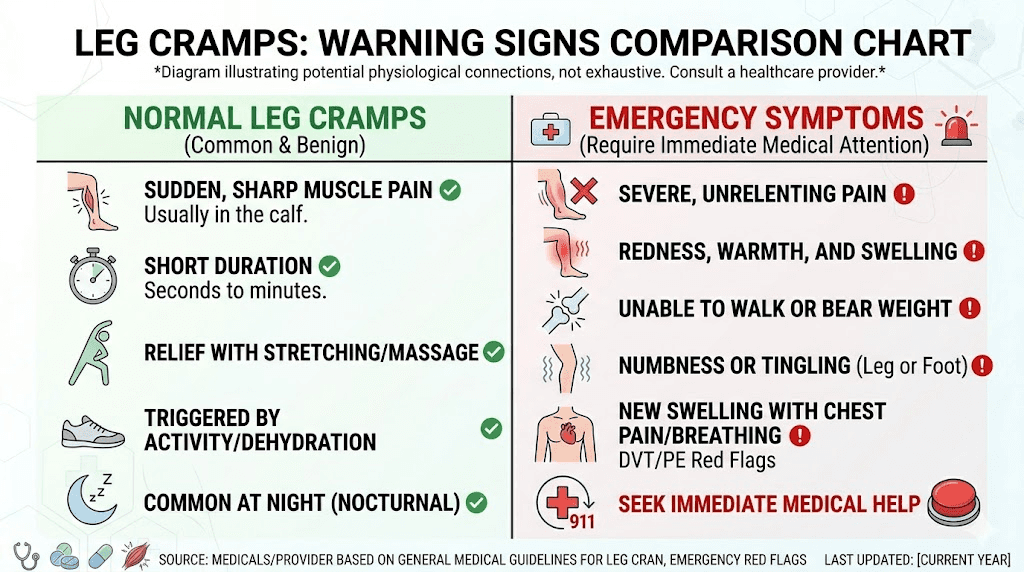
Normal semaglutide leg cramps are brief, lasting seconds to a few minutes. They affect one muscle group at a time, usually the calf. They resolve with stretching and do not leave lasting pain.
Seek same-day medical evaluation if you experience cramps lasting more than 10 minutes that do not respond to stretching, swelling or redness in the affected leg (which could indicate a blood clot), cramps in multiple muscle groups simultaneously, or cramps accompanied by significant weakness.
Seek emergency care if you notice dark brown or cola-colored urine after severe cramping, extreme bilateral leg pain rated 7 or higher out of 10, chest pain or difficulty breathing alongside leg symptoms, or inability to bear weight on the affected leg.
Understanding whether semaglutide causes blood clots is relevant here because deep vein thrombosis can mimic severe cramping, and the two conditions require very different responses. When in doubt, get evaluated.
How to prevent semaglutide leg cramps
Prevention is straightforward once you understand the mechanisms. You need to replace what semaglutide is taking away, protect the muscle you are building, and support the systems that keep minerals where they belong. Here is the complete protocol.
Electrolyte supplementation protocol
Start supplementation when you start semaglutide. Do not wait for cramps to appear. By the time cramping begins, you are already significantly depleted, and it takes days to weeks to restore normal levels through oral supplementation.
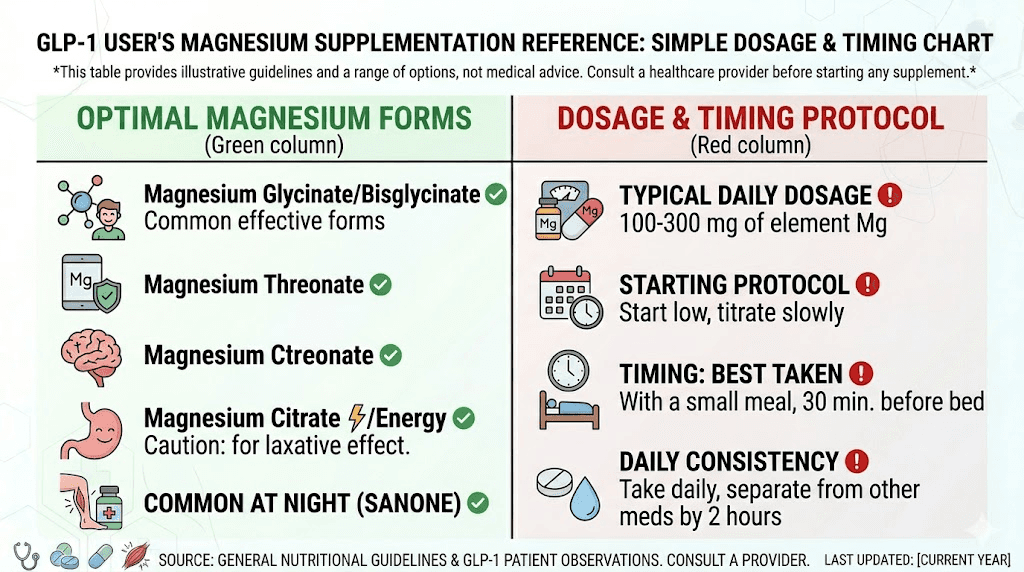
The foundation of your protocol should be magnesium. Begin with 100 to 200 milligrams of elemental magnesium daily for the first week, then increase to 300 to 450 milligrams daily. The National Academy of Medicine sets the supplemental upper limit at 350 milligrams per day, but this refers to supplemental magnesium specifically. Magnesium from food does not count toward this limit. Take it in the evening, as magnesium also supports sleep quality, which helps counter the insomnia some semaglutide users experience.
For potassium, over-the-counter supplements are limited to 99 milligrams per tablet for safety reasons. Higher doses require medical supervision. Rather than relying on supplements for potassium, focus on potassium-rich foods: avocados, sweet potatoes, spinach, white beans, and coconut water. If your magnesium levels are adequate, potassium retention improves naturally because of the magnesium-potassium interdependence described earlier.
Sodium replacement during acute GI episodes is also important. Electrolyte drinks or oral rehydration solutions are more effective than plain water during vomiting or diarrhea because they replace both fluid and minerals simultaneously. Choosing the right supplements for GLP-1 therapy makes a significant difference in how well your body handles the transition.
Magnesium form comparison
Not all magnesium supplements are created equal. The form you choose dramatically affects absorption, GI tolerance, and effectiveness for cramp prevention.
Magnesium glycinate offers the highest absorption with minimal GI side effects. This is the best choice for most semaglutide users because their stomachs are already under stress. Glycinate does not cause the loose stools that other forms can trigger, which matters when you are already dealing with GI disruption from GLP-1 therapy.
Magnesium citrate has superior bioavailability and a mild laxative effect. This can actually be beneficial for the 24.2% of semaglutide users who experience constipation rather than diarrhea. If constipation is your primary GI complaint, citrate kills two birds with one stone.
Magnesium oxide has the lowest absorption rate of common forms but is also the cheapest. It works primarily as a stool softener at higher doses. For cramp prevention, it is the least effective option per milligram taken.
Magnesium threonate has high absorption and crosses the blood-brain barrier, making it popular for cognitive benefits. It works for cramps but is significantly more expensive than glycinate for a similar muscle-relaxation effect.
For most semaglutide users, magnesium glycinate at 300 to 400 milligrams daily is the optimal choice. Maintain a 2 to 4 hour gap between magnesium and any antibiotics or bisphosphonates, as these medications can interfere with absorption.
An underreported option is taurine supplementation. A randomized clinical trial found that 1,000 milligrams twice daily (2 grams total) significantly reduced leg cramping in patients with liver disease, producing 7 fewer cramps per fortnight and 89 fewer minutes of total cramping. While the strongest evidence comes from liver disease populations, taurine plays a role in muscle cell membrane stabilization that is relevant to any cramp condition. No adverse effects were reported in trials.
Hydration strategy
Drink 2 to 3 liters of fluid daily while on semaglutide. That sounds simple. But semaglutide suppresses thirst along with appetite for many people, which means you cannot rely on thirst signals to keep you adequately hydrated.
Set specific hydration targets. Drink 500 milliliters upon waking. Drink 250 milliliters before each meal. Sip throughout the day. Monitor urine color, which should be pale yellow. Dark yellow or amber urine means you are already dehydrated.
During active GI symptoms, increase fluid intake beyond baseline. Replace each vomiting or diarrhea episode with an additional 250 to 500 milliliters of electrolyte-containing fluid, not plain water. Plain water dilutes whatever electrolytes you have left without replacing the ones you lost.
If you are using oral semaglutide drops or sublingual formulations, hydration is equally important because the GI side effect profile remains similar regardless of administration route.
Exercise and stretching
Gentle calf stretches before bed can reduce nocturnal cramp frequency. Hold each stretch for 30 seconds, repeating three times per leg. Wall stretches, step stretches, and towel stretches all target the gastrocnemius and soleus muscles where most leg cramps originate.
Resistance training during semaglutide therapy serves double duty. It preserves lean mass, which reduces cramp susceptibility, and it improves circulation in the legs, which helps deliver minerals to muscle tissue. Even two to three sessions per week of basic lower body exercises, squats, lunges, calf raises, can make a measurable difference.
Avoid starting intense exercise programs during dose escalation phases when GI symptoms peak. Ramp up activity gradually and ensure adequate nutrition on training days. Understanding caloric needs on semaglutide becomes especially important when you add exercise to the equation.
Complete electrolyte supplementation guide for GLP-1 users
Here are the specific daily targets and recommended forms for each electrolyte that matters during semaglutide therapy.
Magnesium: 300 to 450 milligrams daily as magnesium glycinate. Start at 100 to 200 milligrams and increase over one to two weeks. Take in the evening. This is the single most important supplement for cramp prevention.
Potassium: 2,600 milligrams daily for women, 3,400 milligrams for men. Prioritize food sources: one avocado provides about 700 milligrams, one cup of cooked spinach about 840 milligrams, one medium sweet potato about 540 milligrams. OTC supplements max at 99 milligrams per tablet, making food the more practical source. Your semaglutide diet plan should prioritize these potassium-rich foods.
Sodium: 1,500 milligrams ideal daily intake. During acute GI symptoms, temporarily increase through electrolyte drinks or broth. Do not chronically oversupplement sodium if you have hypertension.
Calcium: 1,000 to 1,200 milligrams daily for women, 1,000 milligrams for men. Food sources include dairy, fortified plant milks, sardines, and leafy greens. Supplement if dietary intake falls short, but separate calcium supplements from magnesium by at least 2 hours for optimal absorption of both.
Optional additions: Taurine at 1,000 milligrams twice daily for persistent cramps. B12 if on metformin concurrently, as metformin depletes B12 over time. A quality probiotic to support gut mineral absorption that GI disruption impairs.
The best foods to eat on semaglutide should deliver many of these minerals through diet. But when appetite is suppressed and portions are small, supplementation bridges the gap that food alone cannot cover. Checking the complete food list for semaglutide users can help you plan meals that maximize mineral intake within limited calories.
Practical management strategies that work
Beyond supplementation, several practical strategies can reduce cramp frequency and severity at different stages of treatment.
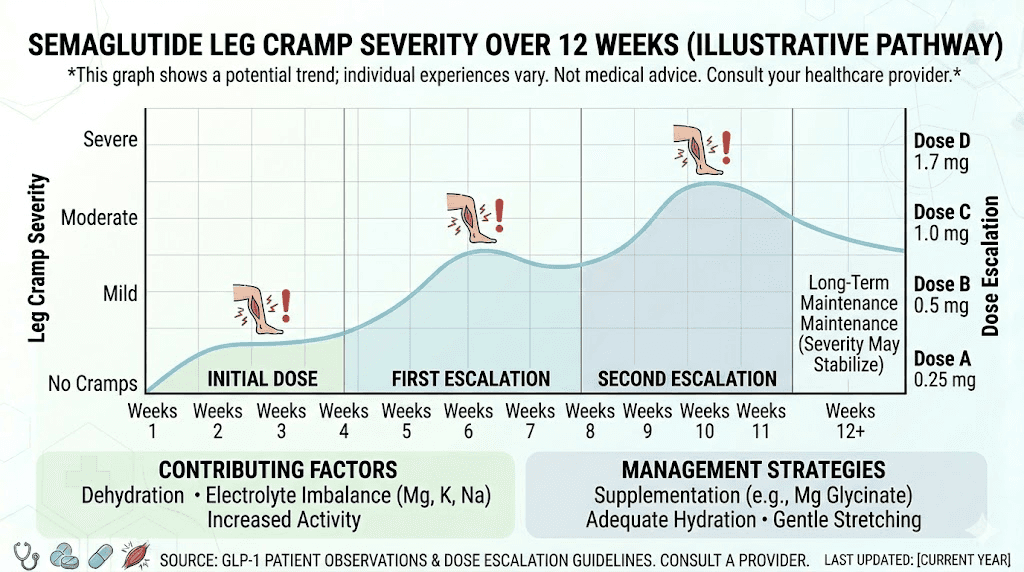
During dose escalation
The first four weeks at any new dose carry the highest cramp risk because GI side effects peak during this window. Plan for this proactively.
Increase magnesium intake by 100 milligrams above your baseline during escalation weeks. Front-load hydration in the morning before GI symptoms typically worsen. Keep electrolyte drinks readily available. Consider splitting your dose if your provider approves, as some people find that two smaller doses produce milder GI effects than one larger one.
Track your GI symptoms during escalation. If you are having more than two to three episodes of diarrhea or vomiting per day consistently, talk to your provider about slowing the escalation timeline. Rapid titration, as the rhabdomyolysis case demonstrated, carries real risks. Following the recommended dosing schedule with adequate time between increases protects you.
Your first week on semaglutide sets the tone. Starting electrolyte support from day one prevents the deficit from developing rather than trying to correct it after cramps have already started.
For nighttime cramps
Nocturnal leg cramps are the most common pattern semaglutide users report. Several targeted strategies help.
Take your magnesium supplement 30 to 60 minutes before bed. Magnesium glycinate in particular has a mild calming effect that supports sleep onset while providing muscle-relaxing benefits during the hours when cramps are most likely. This also helps with the fatigue that many users experience.
Perform calf stretches before getting into bed. A warm bath with Epsom salts (magnesium sulfate) before bed provides both topical magnesium absorption and muscle relaxation through heat. Keep a rolled towel next to your bed so you can immediately stretch by pulling your toes toward your shin if a cramp strikes. Dorsiflexion, pulling the toes up, is the fastest way to interrupt a calf cramp in progress.
Sleep with a light sheet rather than heavy blankets. Pressure from heavy bedding can push feet into a plantar-flexed position (toes pointing down), which shortens the calf muscles and makes them more vulnerable to spontaneous contraction.
If you are also dealing with insomnia on semaglutide, optimizing your injection timing may help reduce both sleep disruption and nighttime cramping.
Long-term prevention
After the initial adjustment period, most semaglutide users find that leg cramps decrease significantly. The body adapts to the medication, GI side effects diminish, and if supplementation is consistent, electrolyte levels stabilize.
Long-term prevention relies on three pillars. First, maintaining consistent magnesium supplementation for the duration of semaglutide therapy. Do not stop supplements just because cramps improve. The depletion mechanisms remain active as long as you are on the medication.
Second, prioritizing resistance training and adequate protein intake to preserve lean mass. The STEP 1 data showing 9.7% lean mass loss reinforces that muscle preservation requires active effort. Protein shakes designed for GLP-1 users can help hit daily protein targets when appetite makes large meals difficult.
Third, regular monitoring through blood work. Ask your provider to check magnesium (ideally RBC magnesium, not just serum), potassium, sodium, and calcium at baseline and every three to six months during treatment. Catching a developing deficiency through lab work is far better than discovering it through a severe cramp or worse.
If you experience a plateau in weight loss, do not compensate by further restricting calories. Aggressive caloric restriction while on semaglutide amplifies both muscle loss and electrolyte depletion, creating conditions where cramps and dizziness become nearly guaranteed.
Semaglutide leg cramps versus tirzepatide muscle pain
If you are considering switching between semaglutide and tirzepatide, understanding how muscle symptoms compare between the two can inform your decision.
Tirzepatide, as a dual GIP/GLP-1 agonist, carries a similar GI side effect profile and therefore a similar risk of electrolyte-mediated muscle cramps. Tirzepatide muscle pain and body aches are reported at comparable rates. The mechanisms are essentially identical: GI losses, renal effects, reduced intake, and lean mass changes all occur with both medications.
However, some users report that side effect profiles differ between the two in practice, even though clinical trial rates are similar. Individual response varies significantly, and someone who experiences severe cramps on semaglutide might tolerate tirzepatide better or vice versa. The first rhabdomyolysis case report is notable because the patient had tolerated liraglutide without any muscle issues, suggesting that response can be drug-specific rather than class-wide.
If you are considering a switch, review the semaglutide to tirzepatide conversion chart and the dosage comparison chart with your provider. Supplement recommendations for tirzepatide follow the same electrolyte support principles outlined in this guide.
The electrolyte supplementation protocol described above applies equally to both medications. If you are switching to manage side effects, continue your magnesium and electrolyte support through the transition.
What to eat to prevent cramps on semaglutide
Diet is your first line of defense against electrolyte depletion. When you are eating less due to appetite suppression, every bite needs to count. Prioritize foods that deliver the minerals your muscles need.
Magnesium-rich foods: Pumpkin seeds (156 milligrams per ounce), almonds (80 milligrams per ounce), spinach (157 milligrams per cooked cup), dark chocolate (65 milligrams per ounce), and black beans (120 milligrams per cooked cup). Even a small handful of pumpkin seeds as a snack delivers a meaningful dose.
Potassium-rich foods: Avocados (700 milligrams each), cooked spinach (840 milligrams per cup), sweet potatoes (540 milligrams each), bananas (420 milligrams each), and coconut water (600 milligrams per cup). Coconut water does double duty as a hydration source.
Calcium-rich foods: Yogurt (300 milligrams per cup), sardines with bones (325 milligrams per 3 ounces), fortified plant milks (300 milligrams per cup), and kale (180 milligrams per cooked cup).
Building meals around these foods while following a semaglutide-compatible diet provides a foundation of mineral support that supplements then build upon. Check our GLP-1 breakfast ideas and dinner ideas for meal inspiration that incorporates these mineral-rich foods. For complete meal frameworks, the GLP-1 recipe collection and semaglutide diet guide offer structured approaches to eating well on reduced appetite.
A quality fiber supplement can also support gut health and mineral absorption, but introduce fiber gradually to avoid worsening GI symptoms during the adjustment period.
Timing your injection to minimize side effects
Some semaglutide users find that injection timing affects the severity of GI side effects and, by extension, electrolyte-related cramps. While no definitive research identifies the optimal injection time, practical patterns emerge from user experience.
Taking your injection in the morning gives your body the full day to manage GI effects while you are awake and can stay hydrated. Evening injections mean GI symptoms may peak during sleep when you are not drinking fluids to compensate for losses.
The best time of day for semaglutide varies by individual, but consistency matters more than the specific hour. Pick a time that lets you manage any GI effects comfortably and stick with it.
Injection technique also matters. Proper injection site selection and rotation can minimize local reactions. If you are new to self-injection, review the complete guide on how to give semaglutide injections to ensure correct technique. Some users report that injection site reactions contribute to localized leg discomfort, particularly when injecting in the thigh. Rotating between abdomen and thigh injection sites can help determine whether injection placement is a factor in your leg symptoms.
Medications that can worsen semaglutide leg cramps
Several commonly used medications can compound electrolyte depletion when taken alongside semaglutide. Being aware of these interactions helps you and your provider anticipate and prevent cramps.
Proton pump inhibitors reduce magnesium absorption through TRPM6 suppression, as discussed above. If you need acid suppression, discuss H2 blockers as an alternative.
Diuretics increase renal excretion of multiple electrolytes. Thiazide diuretics specifically deplete potassium and magnesium. If you take a diuretic for blood pressure management alongside semaglutide, electrolyte monitoring becomes essential.
Metformin can affect kidney handling of minerals and depletes B12 over time. The combination of metformin and semaglutide is common for Type 2 diabetes management and generally safe, but warrants closer attention to mineral status.
If you are taking phentermine alongside semaglutide or exploring combinations like berberine and semaglutide, discuss the combined electrolyte impact with your provider. Each additional medication or supplement that affects the GI tract or kidneys adds another variable to the electrolyte equation.
How long do semaglutide leg cramps last
For most people, the worst of the cramping occurs during the first two to four weeks at each new dose level. As GI side effects subside and the body adapts, cramp frequency typically decreases. Many users report that cramps resolve substantially by weeks four to eight at a stable dose, particularly if they implement electrolyte supplementation early.
However, this timeline assumes you are actively addressing the mineral losses. Without supplementation, cramps can persist indefinitely because the mechanisms causing them, GI effects, renal changes, and reduced food intake, remain active throughout treatment. Someone who has been on semaglutide for six months without electrolyte support may actually have worse cramps than they did at the start because of cumulative depletion.
The semaglutide week-by-week timeline can help you understand what to expect at each stage. If cramps persist beyond eight weeks at a stable dose despite adequate supplementation and hydration, bring this up with your provider. Persistent cramping may indicate an underlying deficiency that needs blood work to identify, or it may suggest a need for dose adjustment.
If you are evaluating how long semaglutide takes to work, know that the side effect timeline and the therapeutic effect timeline are related but not identical. Appetite suppression often appears before weight loss, and GI symptoms often appear before appetite suppression fully kicks in. Planning your electrolyte strategy around this timeline positions you for a smoother experience.
For researchers exploring the long-term question of how long to stay on semaglutide, electrolyte support should continue for the entire duration of therapy. It is not a temporary measure.
What to do if cramps persist despite everything
You have optimized your magnesium. Your hydration is on point. Your potassium intake is solid. And your legs are still cramping. What next?
First, get comprehensive blood work. Request serum magnesium, RBC magnesium (more accurate), serum potassium, sodium, calcium, phosphorus, and a metabolic panel including kidney function. If your serum magnesium is below 1.8 milligrams per deciliter, you are likely significantly depleted at the cellular level and may benefit from a short course of higher-dose oral or even IV magnesium replacement.
Second, evaluate your full medication list with your provider. The combination of semaglutide with PPIs, diuretics, or other medications may create a depletion pattern that standard supplementation cannot fully overcome.
Third, consider whether your dose is too high. The rhabdomyolysis cases both involved higher doses (1.7 and 2.4 milligrams). Some people achieve excellent therapeutic results at lower doses with far fewer side effects. Finding your optimal maintenance dose may mean accepting slightly slower weight loss in exchange for dramatically better quality of life.
Fourth, if you have tried everything and are still struggling, discuss switching to a different GLP-1 agonist. The first rhabdomyolysis case report showed that the patient tolerated liraglutide perfectly but had severe muscle reactions to semaglutide specifically. Individual drug response within the GLP-1 class varies. If semaglutide is not working for you, switching agents is a legitimate option.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers comprehensive resources including detailed protocol guides, dosing calculators, and evidence-based approaches to managing exactly these kinds of challenges. SeekPeptides members access personalized support and a community of experienced researchers who have navigated these issues firsthand.
The role of compounded semaglutide in cramp management
Compounded semaglutide formulations sometimes include additional ingredients that can affect cramp risk. Semaglutide compounded with glycine may offer a slight advantage because glycine itself supports muscle function and may have a mild relaxing effect on muscle tissue.
Semaglutide with methylcobalamin (active B12) addresses B12 status, which is relevant for nerve function and can contribute to muscle cramping when deficient. B12-enhanced formulations may be particularly beneficial for people also taking metformin.
Regardless of which formulation you use, the electrolyte supplementation protocol remains the same. The compounded additions help but do not replace the need for magnesium, potassium, and proper hydration. Whether you use compounded semaglutide or brand-name versions, the muscle cramp mechanisms and solutions are fundamentally identical.
If your compounded semaglutide does not seem to be working or you are experiencing more side effects than expected, potency and storage may be factors. Ensure your medication is properly stored per the compounded semaglutide storage guidelines and has not expired.
Frequently asked questions
Are leg cramps a common side effect of semaglutide?
Leg cramps are not listed in official FDA prescribing information for semaglutide. However, they are frequently reported by users and occur as an indirect result of electrolyte depletion from GI side effects, reduced food intake, and increased renal sodium excretion. Clinical trial data suggests less than 5% of participants formally reported cramps, but real-world prevalence appears higher based on user reports. Understanding how semaglutide makes you feel overall helps contextualize this symptom.
What is the best supplement for semaglutide leg cramps?
Magnesium glycinate at 300 to 400 milligrams daily is the most effective single supplement for semaglutide-related leg cramps. It has high absorption, is gentle on an already-stressed GI system, and directly addresses the most common mineral deficiency behind muscle cramping. Add taurine at 2 grams daily if magnesium alone does not resolve the issue. See our full guide on supplements to take with GLP-1 medications for a complete protocol.
Do semaglutide leg cramps go away on their own?
Cramps often improve as the body adjusts to semaglutide, typically decreasing after four to eight weeks at a stable dose. However, without addressing the underlying electrolyte depletion through supplementation and dietary changes, cramps can persist or worsen over time due to cumulative mineral losses. Proactive supplementation resolves cramps faster than waiting.
Can semaglutide cause muscle damage?
In rare cases, semaglutide has been associated with rhabdomyolysis, a condition involving breakdown of muscle tissue. Two published case reports document this, one with CK levels of 2,619 and another peaking at 25,000 units per liter. Both cases involved higher doses and resolved with discontinuation and IV hydration. If you experience severe bilateral muscle pain with dark urine, seek emergency care immediately. For related concerns, see our guide on semaglutide and blood clots.
Should I stop semaglutide if I get leg cramps?
Mild to moderate leg cramps do not require stopping semaglutide. They typically respond well to magnesium supplementation, improved hydration, and dietary adjustments. Only consider discontinuation in consultation with your provider if cramps are severe (pain rated 7 or above out of 10), accompanied by dark urine, bilateral, or not responding to aggressive electrolyte replacement. Stopping semaglutide abruptly has its own set of considerations, so work with your provider on any dose changes.
Does alcohol make semaglutide leg cramps worse?
Yes. Alcohol is a diuretic that increases urinary losses of magnesium and other electrolytes. It also impairs intestinal absorption of minerals and can worsen GI symptoms. The severe hypomagnesemia case report involved a patient who consumed 10 to 20 units of alcohol weekly alongside semaglutide. If you are experiencing cramps, reducing or eliminating alcohol is one of the most impactful changes you can make. For more detail, see our guide on drinking on semaglutide.
Are leg cramps worse at higher semaglutide doses?
Yes. Higher doses produce more GI side effects, which cause greater electrolyte losses. The risk appears dose-dependent, with higher incidence at the 2.4 milligram dose used for weight management compared to lower doses. Both rhabdomyolysis cases involved patients at higher doses (1.7 and 2.4 milligrams). If cramps are severe, discuss a dose reduction with your provider rather than simply enduring them.
Can I take magnesium with semaglutide?
Yes. There are no known interactions between magnesium supplements and semaglutide. In fact, magnesium supplementation is strongly recommended for most semaglutide users given the electrolyte depletion mechanisms involved. Take magnesium at least 2 hours apart from any antibiotics, bisphosphonates, or thyroid medications that may be affected by mineral supplements. The semaglutide dosage calculator on SeekPeptides can help you dial in your overall protocol.
External resources
Rhabdomyolysis associated with semaglutide therapy: a case report (PubMed Central)
Gastrointestinal tolerability of semaglutide 2.4 mg: pooled analysis of STEP trials (PubMed Central)
STEP 1 trial: semaglutide 2.4 mg for weight management (New England Journal of Medicine)
FDA safety communication: low magnesium and proton pump inhibitors
Severe hypomagnesemia case report associated with semaglutide therapy (PubMed Central)
For researchers who want comprehensive, evidence-based guidance on every aspect of peptide protocols, SeekPeptides provides the most thorough resource available. Members access detailed protocol guides, dosing calculators, interaction databases, and a community of thousands who have navigated these exact challenges. From reconstitution guides to safety protocols, SeekPeptides is where serious researchers go for answers they can trust.
In case I do not see you, good afternoon, good evening, and good night. May your electrolytes stay balanced, your muscles stay relaxed, and your semaglutide journey stay on track.