Mar 24, 2026

You take your levothyroxine every morning. Same dose. Same time. Same routine for months or years. Then you start tirzepatide, and suddenly your thyroid labs look different. Your TSH drops. Maybe you feel jittery. Your doctor wants to adjust your dose. And nobody warned you this would happen.
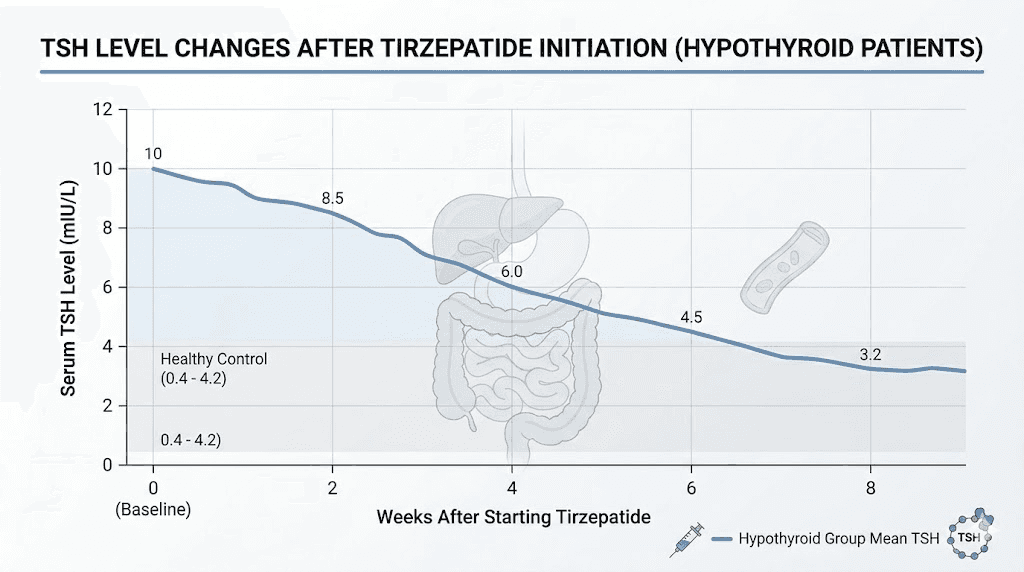
This is not a rare occurrence. A retrospective study found that 65% of hypothyroid patients on stable levothyroxine doses experienced TSH decreases within just 4 to 8 weeks of starting tirzepatide. Even more concerning, 29% of those patients had their TSH suppressed below the normal range, putting them at risk for iatrogenic hyperthyroidism. The interaction between these two medications is more nuanced than most prescribers realize, and if you are managing both thyroid health and weight loss, understanding exactly how these drugs influence each other could be the difference between optimized results and months of unnecessary side effects.
This guide covers everything researchers and patients need to know about combining tirzepatide with levothyroxine. The mechanism behind their interaction. The clinical data showing real TSH changes. Practical timing protocols that minimize absorption issues. When to test your thyroid levels after starting a GLP-1 agonist. And the warning signs that your levothyroxine dose needs adjusting. SeekPeptides has compiled the most current research on this interaction so you can navigate it with confidence rather than confusion.
How tirzepatide affects levothyroxine absorption
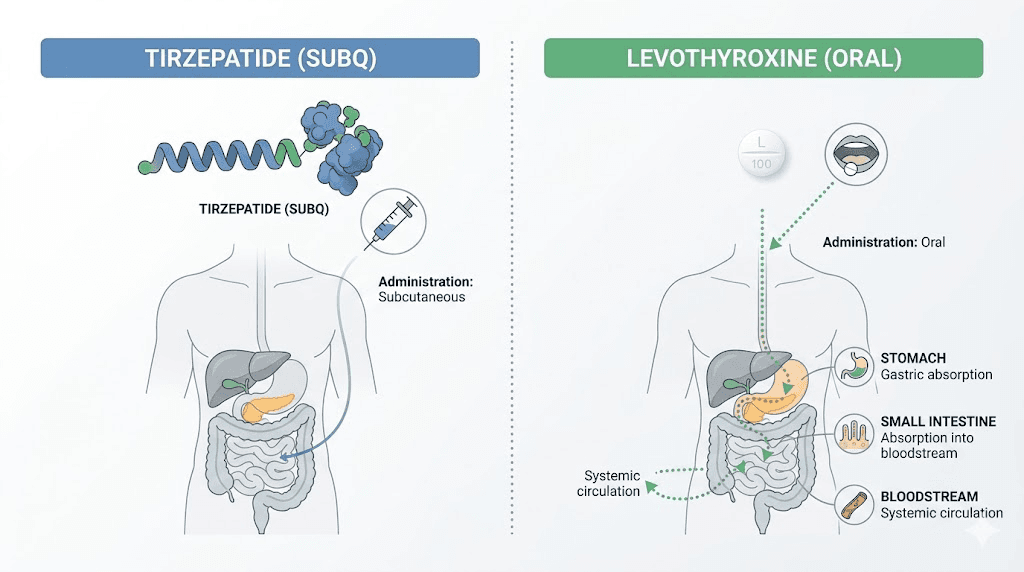
The core issue is gastric emptying. Tirzepatide, like all GLP-1 receptor agonists, slows the rate at which your stomach empties its contents into the small intestine. This is actually one of the primary mechanisms through which it reduces appetite and promotes weight loss. Food stays in your stomach longer, you feel full longer, and you eat less.
But levothyroxine absorption depends heavily on gastric conditions.
Levothyroxine is best absorbed in an acidic stomach environment, ideally on an empty stomach with nothing else competing for absorption. When tirzepatide delays gastric emptying, it creates a longer transit time for levothyroxine in the gastrointestinal tract. This extended window can actually increase how much levothyroxine your body absorbs. A pharmacokinetic study examining oral semaglutide, a related GLP-1 medication, found that levothyroxine exposure increased by approximately 33% when the two drugs were taken together.
That 33% increase matters. A lot.
If you have been stable on 100mcg of levothyroxine for years, and your body suddenly absorbs it as though you are taking 133mcg, your thyroid hormone levels shift. Your TSH drops because your pituitary gland detects excess thyroid hormone and reduces its signaling. You might start experiencing symptoms of overmedication without ever changing your actual dose.
The dual mechanism problem
There are actually two separate mechanisms at play when you combine tirzepatide with levothyroxine, and both push in the same direction. The first is the absorption change from delayed gastric emptying. The second is weight loss itself.
Levothyroxine dosing is partially based on body weight. The standard replacement dose is roughly 1.6mcg per kilogram of body weight. When tirzepatide produces significant weight loss, often 15 to 20% of body weight over 72 weeks, your levothyroxine requirement naturally decreases. A person weighing 100kg on 150mcg of levothyroxine who loses 20kg may now only need 120mcg.
Researchers who studied this interaction noted something important. TSH changes appeared early, within 4 to 8 weeks, before significant weight loss had occurred. This suggests the gastric emptying mechanism drives the initial changes, while weight loss compounds the effect over the following months. Both mechanisms reduce the amount of levothyroxine you need, and both happen simultaneously when you are on tirzepatide. Without monitoring, you could end up significantly overmedicated without realizing it.
How tirzepatide compares to other GLP-1 medications
Tirzepatide is a dual GIP and GLP-1 receptor agonist, which distinguishes it from pure GLP-1 drugs like semaglutide. Both classes slow gastric emptying, but tirzepatide has shown particularly potent effects on gastric motility, especially after the initial 5mg dose. Research indicates the impact on gastric emptying was greatest after a single dose of 5mg and diminished somewhat after subsequent doses as the body adapted.
This means the first few weeks of tirzepatide treatment may produce the most dramatic effects on levothyroxine absorption. Your body adjusts to some degree over time, but the effect does not disappear entirely. The gastrointestinal effects of tirzepatide persist throughout treatment, though they typically become less intense after the initial titration period.
For people considering semaglutide versus tirzepatide, the levothyroxine interaction concern applies to both medications. The formal pharmacokinetic data showing a 33% increase in levothyroxine exposure was studied with oral semaglutide specifically, but injectable formulations of both drugs also slow gastric emptying enough to affect thyroid medication absorption.
Clinical evidence for thyroid function changes on tirzepatide
The strongest direct evidence comes from a retrospective study presented at the Endocrine Society meeting in 2023. Researchers screened 70 hypothyroid patients on tirzepatide, ultimately analyzing 17 who met strict criteria, including stable levothyroxine doses before starting tirzepatide and adequate follow-up data.
The results were striking.
Mean TSH dropped from 2.288 at baseline to 1.569 within a median of 47 days. That is a 31% reduction in TSH in under two months. Eleven of 17 patients, a full 65%, showed TSH decreases from their baseline values. Five patients, representing 29%, had their TSH suppressed below the normal reference range entirely.
These numbers deserve attention because suppressed TSH means excess thyroid hormone circulation. For patients with Hashimoto thyroiditis or post-thyroidectomy hypothyroidism who rely on precise levothyroxine dosing, an unexpected shift of this magnitude can produce real symptoms and real risks. Excess thyroid hormone over extended periods increases the risk of atrial fibrillation, bone density loss, and cardiovascular complications.
Case reports supporting the data
Beyond the retrospective study, multiple case reports have documented TSH suppression after starting GLP-1 agonists in patients on levothyroxine. One particularly instructive case involved a post-thyroidectomy patient who had been stable on levothyroxine replacement for years. After starting subcutaneous semaglutide, the patient required a 25% reduction in levothyroxine dose to bring TSH back into the normal range.
Another case report documented iatrogenic thyrotoxicosis, meaning clinically significant hyperthyroidism caused by medication interaction, in a patient who started semaglutide therapy while on levothyroxine. The patient developed classic hyperthyroid symptoms including palpitations, tremor, and anxiety before labs confirmed the TSH suppression.
These cases illustrate that the interaction is not merely a laboratory curiosity. It produces real clinical consequences that require proactive management. Whether you are on compounded tirzepatide or brand-name formulations, the mechanism and risk remain the same.
What the research says about mechanism timing
One of the most important findings from the retrospective study was that TSH changes occurred early, before patients had achieved significant weight loss. The median follow-up was only 47 days, too short for most patients to lose enough weight to meaningfully alter their levothyroxine requirements through the weight-based mechanism alone.
This early timing points strongly toward the gastric emptying mechanism as the primary driver of initial thyroid function changes. The enhanced absorption of levothyroxine due to delayed gastric emptying begins with the first dose of tirzepatide. Over subsequent months, the weight loss mechanism compounds this effect, potentially requiring further dose adjustments as body weight decreases.
Understanding this two-phase timeline helps explain why some patients experience symptoms very quickly after starting tirzepatide, while others notice gradual changes over several months as their weight drops. Both phases require monitoring and potentially different dose adjustments.
Symptoms of levothyroxine overmedication to watch for
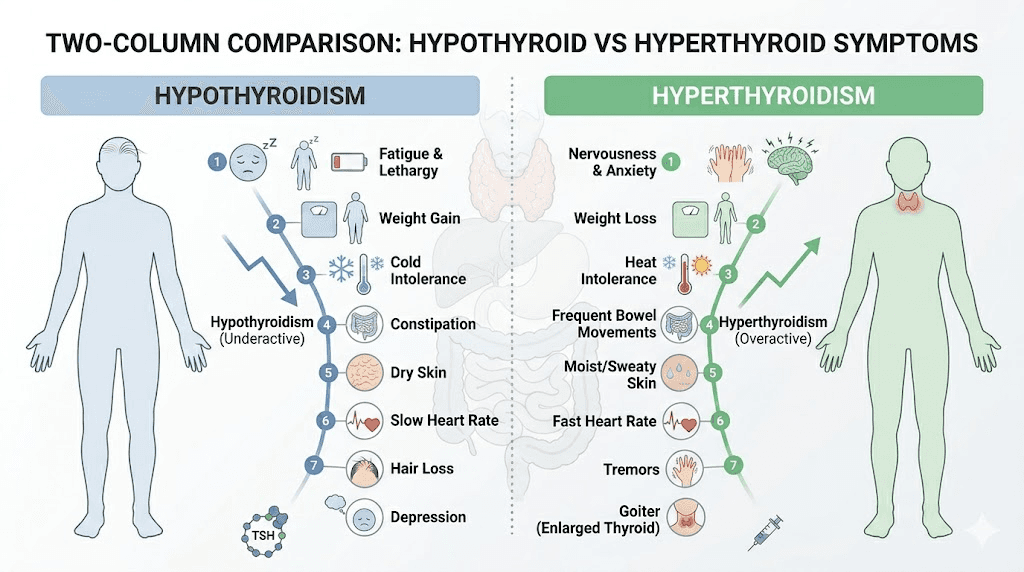
When tirzepatide increases your effective levothyroxine dose, the symptoms mirror those of hyperthyroidism. Some of these overlap with common tirzepatide side effects, which can make them easy to dismiss or misattribute.
Watch for these specific signs.
Cardiovascular symptoms are often the earliest and most concerning indicators. Heart palpitations, a racing pulse at rest, or a feeling that your heart is pounding are classic signs of excess thyroid hormone. If you notice your resting heart rate climbing above its usual range after starting tirzepatide, this could indicate levothyroxine overmedication rather than a direct tirzepatide effect. Sustained excess thyroid hormone significantly raises the risk of cardiovascular complications.
Neurological and mood changes include anxiety, irritability, nervousness, tremor in the hands, and difficulty concentrating. These can be subtle at first. A general feeling of being "wired" or unable to relax, difficulty falling asleep despite feeling tired, or a noticeable increase in anxiety levels all warrant thyroid lab testing. Insomnia from tirzepatide should always prompt consideration of whether thyroid hormone levels have shifted.
Metabolic symptoms include unexplained heat intolerance, excessive sweating, or feeling warm when others are comfortable. Unintended weight loss beyond what you would expect from tirzepatide alone can occur. While tirzepatide does increase metabolism through its own mechanisms, dramatic or unexpected weight loss should prompt a thyroid function check.
Digestive symptoms present a particular diagnostic challenge. Both tirzepatide and excess thyroid hormone can cause diarrhea, sulfur burps, nausea, and changes in bowel habits. Persistent acid reflux that worsens rather than improves as your body adjusts to tirzepatide could indicate thyroid overmedication rather than a direct GLP-1 effect. If these symptoms persist or intensify rather than improving over the first few weeks, consider whether thyroid overmedication might be contributing.
Symptoms of undermedication
Less commonly, some patients may experience worsened hypothyroid symptoms if tirzepatide causes enough gastrointestinal disruption, through severe nausea or vomiting, to reduce their levothyroxine absorption on certain days. Watch for increasing fatigue, cold intolerance, constipation beyond what tirzepatide typically causes, dry skin, hair thinning, depression, or unexplained weight gain despite following your diet protocol.
The bottom line: any significant change in how you feel after starting tirzepatide, whether matching hyper or hypothyroid patterns, should trigger a thyroid function test. Do not assume every symptom is from the tirzepatide itself.
Timing protocols for taking tirzepatide and levothyroxine
The good news is that you can safely take both medications. The key is strategic timing to minimize absorption interference and consistent monitoring to catch any changes early.
The morning levothyroxine protocol
Most people take levothyroxine first thing in the morning on an empty stomach, waiting 30 to 60 minutes before eating. This remains the gold standard approach. When adding tirzepatide to this routine, separation is your best tool.
Take your levothyroxine immediately upon waking with a small amount of water, no more than 4 ounces. Wait at least 30 to 60 minutes before eating anything. Since tirzepatide is a once-weekly injection, administer it at a completely different time of day, ideally in the evening. This creates maximum separation between the two medications and reduces the chance that tirzepatide delayed gastric emptying from the previous day interferes with your morning levothyroxine absorption.
Choose a consistent day each week for your tirzepatide injection. Many patients find that injecting on a day when they can manage potential GI side effects most comfortably works best, often a Friday evening so any initial nausea occurs over the weekend. Proper injection technique also matters for consistent absorption, so review the best injection sites for tirzepatide and thigh injection guidance to ensure you are rotating sites appropriately.
The bedtime levothyroxine alternative
Some endocrinologists recommend switching levothyroxine to bedtime dosing for patients on GLP-1 medications. Research supports that bedtime dosing of levothyroxine can be equally effective as morning dosing, provided you take it at least 3 to 4 hours after your last meal.
This approach offers several advantages when combined with tirzepatide. Evening levothyroxine dosing completely eliminates any morning timing conflicts. It removes the "wait 30 to 60 minutes before eating" restriction that some patients find inconvenient. And if you administer your weekly tirzepatide injection in the morning, the maximum separation between the two medications occurs naturally.
If you are considering switching from morning to bedtime levothyroxine, discuss it with your prescriber first. The transition may temporarily affect your TSH levels, so you will want baseline labs and a follow-up test 6 to 8 weeks after making the switch.
Injection timing for tirzepatide
Tirzepatide is administered once weekly at the same time each week. The best time to take your tirzepatide shot when also managing thyroid medication is whichever time creates the most separation from your levothyroxine dose. If you take levothyroxine at 6am, inject tirzepatide in the evening. If you take levothyroxine at bedtime, inject tirzepatide in the morning.
Some patients worry about whether the day they choose for their tirzepatide injection matters in relation to their daily levothyroxine. Since tirzepatide has a half-life of approximately 5 days and its effects on gastric emptying persist throughout the dosing interval, the specific day matters less than maintaining consistent timing and monitoring your labs regularly. The gastric emptying effect is present every day of the week, not just on injection day.
Thyroid monitoring schedule when starting tirzepatide
Standard thyroid monitoring for patients on stable levothyroxine doses typically involves annual TSH testing. When you add tirzepatide, this schedule needs to become significantly more frequent, at least temporarily.
Recommended monitoring timeline
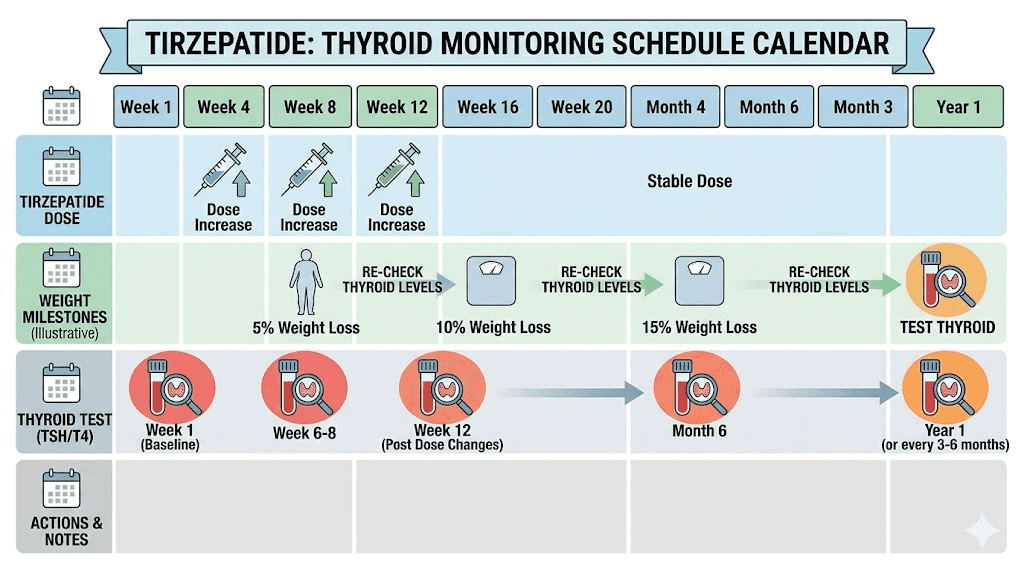
Before starting tirzepatide: Get a comprehensive thyroid panel including TSH, free T4, and free T3. This establishes your true baseline on your current levothyroxine dose. If you have not had labs in more than 3 months, get fresh ones before your first tirzepatide injection. This baseline is critical because without it, you have no reference point for detecting changes.
6 to 8 weeks after starting tirzepatide: Repeat TSH and free T4. This is the most important test in the entire monitoring protocol. The retrospective study data shows that clinically significant TSH changes occur within this window. Do not skip or delay this test. If your TSH has dropped below your usual range or below the normal reference range entirely, your prescriber may need to reduce your levothyroxine dose.
After each tirzepatide dose escalation: Consider repeat testing 6 to 8 weeks after each increase in tirzepatide dose. Higher tirzepatide doses may further affect gastric emptying, though the effect tends to plateau somewhat after initial adaptation. Standard tirzepatide dose escalation involves increases every 4 weeks, so coordinating thyroid labs with your dose increases creates an efficient monitoring system.
After significant weight loss milestones: Once you have lost 10% or more of your starting body weight, recheck thyroid labs regardless of your last test date. Each subsequent 10% weight loss milestone warrants another check. Weight loss directly reduces levothyroxine requirements, and this effect stacks on top of the absorption changes.
Every 6 to 12 months once stable: After your thyroid levels have stabilized and any levothyroxine dose adjustments have been made, you can return to testing every 6 to 12 months. However, any future changes to your tirzepatide dose, either increases or decreases, should trigger another monitoring cycle.
What your labs should look like
Most endocrinologists target a TSH between 0.5 and 2.5 for patients on levothyroxine replacement, though your individual target may differ. Free T4 should remain within the normal reference range. If your TSH drops below 0.3 or your free T4 rises above normal, your levothyroxine dose likely needs reduction.
Some practitioners also monitor free T3 levels, particularly if you experience symptoms despite normal TSH and free T4 values. The interaction between tirzepatide and blood work is an important consideration for anyone managing multiple medications simultaneously.
Levothyroxine dose adjustments on tirzepatide
Adjusting your levothyroxine dose while on tirzepatide is not a one-time event. It is an ongoing process that may require multiple adjustments over the first year of treatment.
When to reduce your levothyroxine dose
A dose reduction is warranted when your TSH consistently falls below your target range. The key word is consistently. A single slightly low TSH reading might reflect normal variation, a timing issue with your blood draw, or a temporary fluctuation. But if two consecutive tests show TSH below your target, or if a single test shows significant suppression below 0.3 combined with symptoms of overmedication, your prescriber should reduce the dose.
Typical reductions are in increments of 12.5 to 25mcg. Most endocrinologists prefer gradual adjustments rather than large changes to avoid swinging from overmedicated to undermedicated. After any adjustment, recheck TSH and free T4 in 6 to 8 weeks to confirm the new dose is appropriate.
The case reports suggest that reductions of 15 to 25% from the original levothyroxine dose are common in patients experiencing significant weight loss on GLP-1 agonists. One documented case required a 25% dose reduction after starting semaglutide. Your individual adjustment will depend on how much weight you lose, how your body responds to the absorption changes, and your personal thyroid function baseline.
Why you should not adjust your own dose
It can be tempting to preemptively reduce your levothyroxine when starting tirzepatide, especially after reading about the interaction. Do not do this. Preemptive dose changes without lab confirmation can push you into hypothyroidism, causing fatigue, weight gain that undermines your tirzepatide results, depression, and other symptoms that make the weight loss journey significantly harder.
Always make levothyroxine changes based on lab results and under medical supervision. The interaction does not affect every patient equally. Some people will need significant dose reductions. Others will need minimal adjustments. Your individual response depends on factors including your specific thyroid condition, your tirzepatide dose, the magnitude of your weight loss, and individual variation in drug absorption and metabolism.
What happens if you stop tirzepatide
If you discontinue tirzepatide for any reason, your levothyroxine requirements may shift back toward your original dose. Gastric emptying returns to normal relatively quickly after stopping GLP-1 medications. However, if you have lost significant weight while on tirzepatide, your body composition has changed permanently, at least until weight regain occurs, and your levothyroxine dose should reflect your current weight rather than your pre-treatment weight.
When stopping tirzepatide, schedule thyroid labs 6 to 8 weeks after discontinuation to reassess your levothyroxine needs. This is especially important if your dose was reduced during tirzepatide treatment, as you may need to increase it back partially or fully.
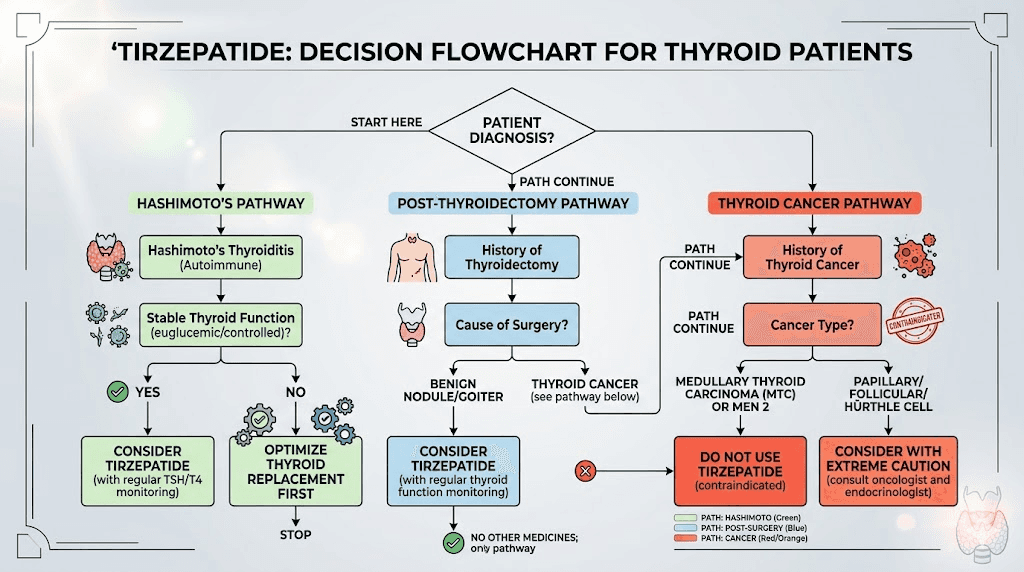
Special considerations for different thyroid conditions
Hashimoto thyroiditis
Patients with Hashimoto disease represent the largest group of people on levothyroxine who might consider tirzepatide. Hashimoto is an autoimmune condition that gradually destroys thyroid tissue, and most patients eventually require full thyroid hormone replacement.
The interaction concerns apply fully to Hashimoto patients. However, there is an additional consideration. Some research suggests that GLP-1 agonists may have anti-inflammatory effects that could theoretically influence the autoimmune process itself, though this remains speculative and has not been demonstrated in clinical trials specifically for thyroid autoimmunity.
For Hashimoto patients, weight management is often particularly challenging because hypothyroidism slows metabolism and promotes fluid retention. Tirzepatide can be an effective tool for breaking through weight loss plateaus that thyroid medication alone does not resolve. The metabolic effects of tirzepatide complement thyroid hormone replacement rather than conflicting with it, provided the interaction is properly managed through monitoring and dose adjustment.
Post-thyroidectomy patients
People who have had their thyroid gland removed, whether for cancer, Graves disease, or large goiter, depend entirely on exogenous levothyroxine. They have zero endogenous thyroid hormone production. This makes precise dosing even more critical because their bodies cannot compensate for dose changes the way a partially functioning thyroid might.
Post-thyroidectomy patients on tirzepatide need the most vigilant monitoring. The case report of a post-thyroidectomy patient requiring a 25% levothyroxine dose reduction on semaglutide illustrates how significant the interaction can be in this population. Any change in absorption directly translates to a change in circulating thyroid hormone because there is no residual thyroid tissue to buffer the effect.
If you are post-thyroidectomy and considering tirzepatide, ensure your endocrinologist is aware and has planned a monitoring schedule before you start treatment. Review the first dose expectations carefully and be prepared for potentially more dramatic effects than patients with partial thyroid function experience. The combination is safe with proper oversight but requires more attention than in patients with residual thyroid tissue.
Thyroid cancer survivors on TSH suppression therapy
Some thyroid cancer survivors are maintained on intentionally suppressive levothyroxine doses, keeping their TSH below the normal range to reduce cancer recurrence risk. For these patients, the tirzepatide interaction is particularly complex because their target TSH is already below normal, and further suppression could increase cardiovascular risk without providing additional cancer protection.
Thyroid cancer survivors should discuss the interaction with both their oncologist and endocrinologist before starting tirzepatide. The monitoring protocol remains the same, but the interpretation of results and dose adjustment decisions require specialized expertise. The relationship between tirzepatide and thyroid nodules is another consideration for patients with thyroid cancer history.
Practical tips for managing both medications
Supplements and nutrient considerations
Several nutrients become particularly important when managing both thyroid health and GLP-1 treatment. Supplements for tirzepatide users should be considered alongside thyroid-specific nutritional needs.
Selenium supports thyroid function and may reduce thyroid antibody levels in Hashimoto patients. Vitamin D deficiency is common in both hypothyroid and overweight populations, and adequate vitamin D supports thyroid function. Iron and calcium supplements must be separated from levothyroxine by at least 4 hours because they directly interfere with absorption, and this timing becomes even more important when gastric motility is already altered by tirzepatide.
Protein intake deserves special attention. Adequate protein, roughly 1.2 to 1.6 grams per kilogram of body weight daily, helps preserve muscle mass during tirzepatide-induced weight loss. Muscle loss can affect metabolic rate, which in turn influences thyroid hormone requirements. Following a structured tirzepatide diet plan that prioritizes protein can help maintain metabolic health while losing weight.
Exercise and thyroid function
Regular exercise, particularly resistance training, supports both weight management goals and thyroid health. Exercise improves insulin sensitivity, which tirzepatide also targets, and helps maintain the metabolically active lean mass that influences thyroid hormone requirements.
The combination of tirzepatide, levothyroxine, and consistent exercise creates a synergistic effect for weight loss that exceeds what any single intervention achieves alone. However, exercise tolerance can be affected by both thyroid hormone levels and tirzepatide side effects. If you notice a significant decrease in exercise capacity, especially combined with a rapid heart rate, consider whether thyroid overmedication might be contributing.
Tracking your progress
Keep a simple log tracking several key metrics. Record your weight weekly. Note any symptoms that could indicate thyroid changes, particularly energy levels, heart rate, heat or cold tolerance, and mood. Track your tirzepatide injection dates and any dose changes. Record your levothyroxine dose and any adjustments. And document all thyroid lab results with dates.
This log becomes invaluable when discussing your care with your prescriber. Patterns emerge that might not be obvious from lab values alone. For example, symptoms that consistently appear 2 to 3 days after your tirzepatide injection might indicate that peak gastric emptying effects are coinciding with a particularly sensitive absorption window for your levothyroxine.
Using GLP-1 injection tracking tools can simplify this process considerably. SeekPeptides members access comprehensive tracking templates and monitoring resources designed specifically for managing multiple medications alongside peptide protocols.
Drug interactions beyond levothyroxine
If you are on levothyroxine, there is a reasonable chance you are also taking other medications that tirzepatide might interact with. Understanding the broader interaction profile helps you manage your entire medication regimen more effectively.
Oral contraceptives
Tirzepatide can reduce the absorption of oral contraceptive pills through the same gastric emptying mechanism that affects levothyroxine. If you are on both levothyroxine and oral contraceptives, the timing considerations multiply. Some prescribers recommend switching to non-oral contraceptive methods, such as patches, rings, or IUDs, while on tirzepatide to eliminate this variable entirely.
Metformin
Many hypothyroid patients also have insulin resistance or type 2 diabetes and take metformin alongside tirzepatide. Metformin absorption can also be affected by delayed gastric emptying, though the clinical significance appears to be less dramatic than with levothyroxine. If you are on all three medications, spacing them throughout the day becomes even more important.
Calcium and iron supplements
Both calcium and iron directly interfere with levothyroxine absorption even without tirzepatide in the picture. When you add delayed gastric emptying to the mix, the potential for absorption interference increases. Separate calcium and iron supplements from levothyroxine by at least 4 hours, and ideally take them at the opposite end of the day from your thyroid medication.
Blood thinners
Some patients on levothyroxine are also on warfarin or other blood thinners. Changes in thyroid function can affect warfarin metabolism, meaning that thyroid level shifts caused by the tirzepatide-levothyroxine interaction could secondarily affect your anticoagulation. If you are on all three medications, monitoring INR more frequently when starting tirzepatide is prudent.
The tirzepatide dose escalation and thyroid impact
Understanding how the standard tirzepatide dosing schedule interacts with thyroid function helps you anticipate when changes are most likely to occur.
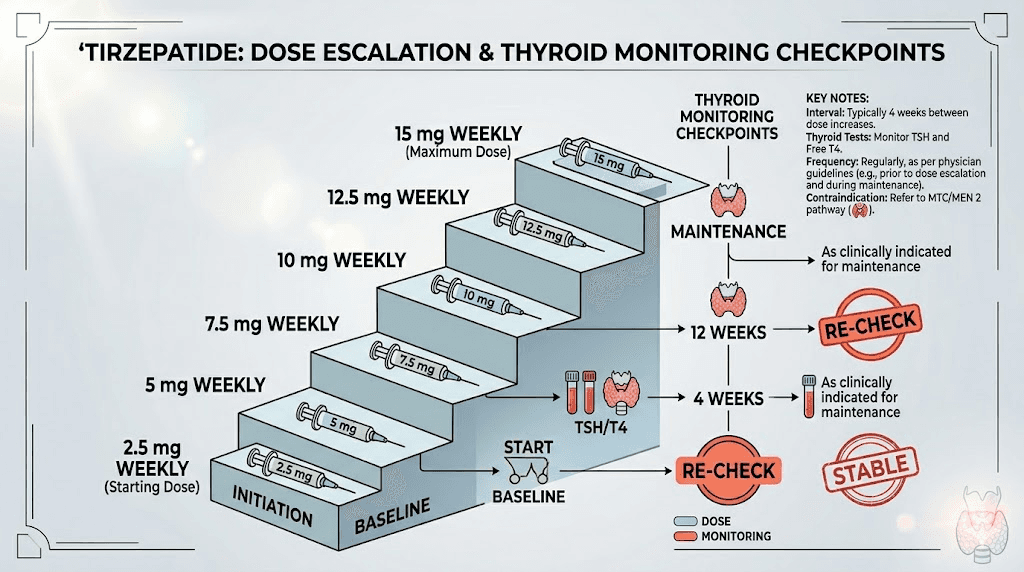
Starting dose phase (2.5mg)
The initial 2.5mg dose produces the least gastric emptying delay but is often when you first notice GI side effects. Levothyroxine absorption changes may begin at this dose but are typically modest. This is your adjustment period for both medications, and getting baseline thyroid labs before this phase is essential.
Early escalation phase (5mg to 7.5mg)
Research suggests the gastric emptying impact is strongest around the 5mg dose. This is when levothyroxine absorption changes are likely to be most pronounced. Plan your 6 to 8 week thyroid check to fall during or shortly after this phase. Many of the side effects during escalation resolve as your body adapts.
Mid escalation phase (10mg)
By this point, your body has partially adapted to the gastric emptying effects, but weight loss is typically accelerating. The weight-based mechanism starts contributing more significantly to thyroid function changes. If your TSH was normal at your initial check, recheck it around this dose level.
Maintenance dose phase (10mg to 15mg)
At maintenance doses, gastric emptying effects have largely plateaued. However, weight loss may continue for months, meaning ongoing thyroid monitoring remains important. Many patients achieve their maximum weight loss between months 6 and 12 of treatment, and levothyroxine adjustments may be needed even after thyroid labs initially normalized at lower doses.
Understanding your injection in units
If you are using compounded tirzepatide, understanding your dose in units is important for tracking. Check resources like our tirzepatide dosage chart in units to ensure accurate dosing. Consistent, accurate dosing helps stabilize the gastric emptying effects and makes thyroid monitoring more reliable because you are comparing equivalent doses at each lab check.
Weight loss expectations with hypothyroidism on tirzepatide
One of the most common concerns for hypothyroid patients considering tirzepatide is whether their thyroid condition will limit their weight loss results. The short answer is no, not significantly, provided thyroid levels are well-managed. But the relationship between thyroid function and weight loss on tirzepatide is more nuanced than that simple answer suggests.
How hypothyroidism affects weight loss mechanics
Untreated or undertreated hypothyroidism reduces basal metabolic rate by 15 to 40%, depending on severity. This means your body burns fewer calories at rest. It also promotes fluid retention, increases cholesterol levels, and can reduce motivation for physical activity through fatigue and depression. All of these factors work against weight loss.
When thyroid hormone replacement is optimized, meaning your TSH is within target range and you feel well, your metabolic rate returns to approximately normal. At this point, tirzepatide should produce weight loss comparable to what it achieves in people without thyroid disease. The key insight is that thyroid optimization must come first or alongside tirzepatide initiation, not after.
If you are starting tirzepatide and suspect your GLP-1 related fatigue is excessive, consider whether suboptimal thyroid levels might be compounding the effect. Fatigue is common in both undertreated hypothyroidism and early tirzepatide use, and the combination can feel overwhelming if both are contributing.
Expected weight loss timeline with thyroid management
Most hypothyroid patients on properly dosed levothyroxine can expect weight loss patterns similar to the general tirzepatide population, though with some important caveats. The first month on tirzepatide typically produces 3 to 5 pounds of weight loss, much of which is water weight and reduced food volume from appetite suppression.
By months 2 through 4, as the dose escalates, weight loss typically accelerates to 4 to 8 pounds per month. This is when thyroid monitoring becomes critical because the enhanced levothyroxine absorption from delayed gastric emptying may push you into slight overmedication. Mild thyroid overmedication can actually accelerate weight loss, which sounds beneficial but carries cardiovascular risks that outweigh any weight loss advantage.
Months 4 through 12 represent the sustained weight loss phase where most people achieve their maximum results. The average monthly weight loss on GLP-1 medications settles into a predictable pattern during this phase. For hypothyroid patients, this is also when weight-based levothyroxine adjustments become most important because cumulative weight loss changes your medication requirements.
Plateau management for thyroid patients
Weight loss plateaus on tirzepatide can have thyroid-related causes that non-thyroid patients do not experience. If your levothyroxine dose becomes too low relative to your current weight and metabolism, you may develop subclinical hypothyroidism, which slows weight loss without producing obvious symptoms.
Conversely, if your levothyroxine dose has not been reduced despite significant weight loss, you might be slightly overmedicated. While this does not typically cause weight plateaus, the associated symptoms like anxiety, insomnia, and digestive changes can interfere with your meal planning and dietary compliance.
When hitting a plateau, the first step for thyroid patients should always be checking labs. A weight loss plateau that does not respond to standard interventions like dietary adjustment or increased exercise may have a thyroid component that only lab work can identify.
Comparison with other GLP-1 medications and thyroid interactions
Tirzepatide is not the only GLP-1 medication that interacts with levothyroxine. Understanding how different options compare helps you make informed decisions about your treatment plan.
Semaglutide and levothyroxine
Semaglutide was actually the subject of the formal pharmacokinetic study that quantified the 33% increase in levothyroxine exposure. This study specifically examined oral semaglutide, which has additional absorption concerns because it is taken by mouth daily rather than injected weekly. Injectable semaglutide formulations also delay gastric emptying but have not been studied as formally for levothyroxine interaction.
The key difference between semaglutide and tirzepatide regarding thyroid interaction is potency. Tirzepatide produces more weight loss than semaglutide, averaging 20 to 24% body weight reduction compared to semaglutide at approximately 15%. More weight loss means larger levothyroxine dose adjustments may be needed over time. Both medications require the same monitoring protocol, but tirzepatide patients may need more aggressive levothyroxine reductions as treatment progresses.
For patients considering whether to start with semaglutide or tirzepatide, the thyroid interaction should not be the deciding factor. Both produce comparable effects on levothyroxine absorption. The choice should be based on weight loss goals, side effect tolerance, availability, and cost.
Retatrutide and thyroid considerations
Retatrutide, the triple agonist targeting GLP-1, GIP, and glucagon receptors, represents the next generation of weight loss peptides. It produces even more weight loss than tirzepatide, with Phase 3 trials showing up to 28.7% body weight reduction. For hypothyroid patients, this means potentially even larger levothyroxine dose adjustments would be needed.
The glucagon receptor agonism in retatrutide adds a unique dimension. Glucagon has direct effects on hepatic metabolism that could theoretically influence thyroid hormone metabolism and clearance. While no specific studies have examined the retatrutide-levothyroxine interaction, the same monitoring principles apply, likely with even more vigilant oversight given the greater weight loss potential.
Comparison table for thyroid patients
Medication | Mechanism | Average weight loss | Gastric emptying effect | Thyroid monitoring needs |
|---|---|---|---|---|
Semaglutide | GLP-1 agonist | 15-16% | Moderate | Standard protocol |
Tirzepatide | GIP + GLP-1 agonist | 20-24% | Significant | Enhanced protocol |
Retatrutide | GIP + GLP-1 + glucagon agonist | 24-29% | Significant | Most vigilant protocol |
Regardless of which medication you choose, the fundamental approach remains the same. Establish baseline thyroid labs, monitor at 6 to 8 weeks, recheck after dose changes and weight milestones, and adjust levothyroxine as needed based on lab results and symptoms.
Navigating the healthcare system for optimal care
Managing the tirzepatide-levothyroxine interaction often involves coordinating between multiple healthcare providers. Your endocrinologist manages thyroid levels. Your weight loss prescriber manages tirzepatide. Your primary care physician may be involved in either or both. Without clear communication between these providers, important dose adjustments can be missed.
Questions to ask your prescriber before starting
Before your first tirzepatide injection, ensure your prescriber is aware you take levothyroxine and has a monitoring plan. Specific questions to ask include the following.
What is my current TSH, and is it within my personal target range? When will you recheck my thyroid levels after I start tirzepatide? At what TSH level would you adjust my levothyroxine dose? Should I change when I take my levothyroxine? Do you want me to track specific symptoms? Who should I contact if I experience symptoms between appointments, your office or my endocrinologist?
Having these conversations upfront prevents the common scenario where a patient starts tirzepatide, experiences symptoms of thyroid overmedication, and does not get labs drawn for months because nobody specified when to test. Proactive care always produces better outcomes than reactive care.
Insurance and cost considerations
Managing two medications with frequent lab monitoring can create cost concerns. Thyroid function tests, specifically TSH and free T4, are relatively inexpensive and widely covered by insurance. Most insurance plans cover these tests every 6 to 8 weeks when medically justified, and starting a new medication that interacts with levothyroxine qualifies as medical justification.
If you are using affordable compounded tirzepatide, your overall medication costs may already be lower than brand-name alternatives. Factor in the cost of additional thyroid monitoring, typically 50 to 100 dollars per lab draw without insurance, when budgeting for your treatment plan. The monitoring cost is small compared to the cost of managing complications from undetected thyroid overmedication.
Some patients explore whether insurance covers GLP-1 medications for weight loss. If your hypothyroidism contributes to weight management difficulty, documenting this in your medical records can strengthen insurance authorization requests. The coverage landscape for GLP-1 medications is evolving rapidly, and thyroid-related weight management may be a covered indication depending on your plan.
Long-term management strategies
Building a sustainable monitoring routine
The intensive monitoring required in the first year of combining tirzepatide with levothyroxine eventually settles into a manageable routine. Most patients find their thyroid levels stabilize after 6 to 12 months, once weight loss has plateaued and levothyroxine dose adjustments have been completed.
At that point, standard monitoring of every 6 to 12 months is typically sufficient, provided your tirzepatide dose remains stable and your weight is not changing significantly. Set calendar reminders for lab appointments so they do not get forgotten during periods when you feel well. Feeling good does not guarantee your levels are optimal, and subtle shifts can develop without obvious symptoms.
Using home monitoring tools can supplement your formal lab schedule. While home TSH tests are not precise enough to replace laboratory testing, they can provide early warning if something has shifted between your scheduled appointments.
Preparing for dose changes in either medication
Any time either medication changes, reset your monitoring cycle. Increasing your tirzepatide dose may further alter levothyroxine absorption. Changing your levothyroxine dose alters the baseline against which you measure tirzepatide effects. Even switching levothyroxine brands can affect absorption because different manufacturers use different fillers and binding agents.
If you are switching from tirzepatide to semaglutide or vice versa, treat it as a new medication start from a thyroid monitoring perspective. Different GLP-1 medications produce different degrees of gastric emptying delay, and your levothyroxine absorption may change with the switch.
Pregnancy planning considerations
For women of reproductive age managing both hypothyroidism and weight with tirzepatide, pregnancy planning adds another layer of complexity. Tirzepatide should be discontinued at least 2 months before planned conception due to its long half-life. When you stop tirzepatide, your levothyroxine absorption returns to its pre-treatment baseline, potentially requiring a dose increase.
Pregnancy itself increases levothyroxine requirements by 30 to 50% in most women, so the combination of stopping tirzepatide and becoming pregnant creates a double adjustment. Work closely with your endocrinologist to establish a monitoring plan that covers the transition from tirzepatide treatment through conception and pregnancy. Women who have been on GLP-1 medications should ensure adequate thyroid monitoring during this transition period.
Real-world protocol for combining tirzepatide and levothyroxine
Based on the clinical evidence and practical experience, here is a comprehensive protocol for safely managing both medications simultaneously.
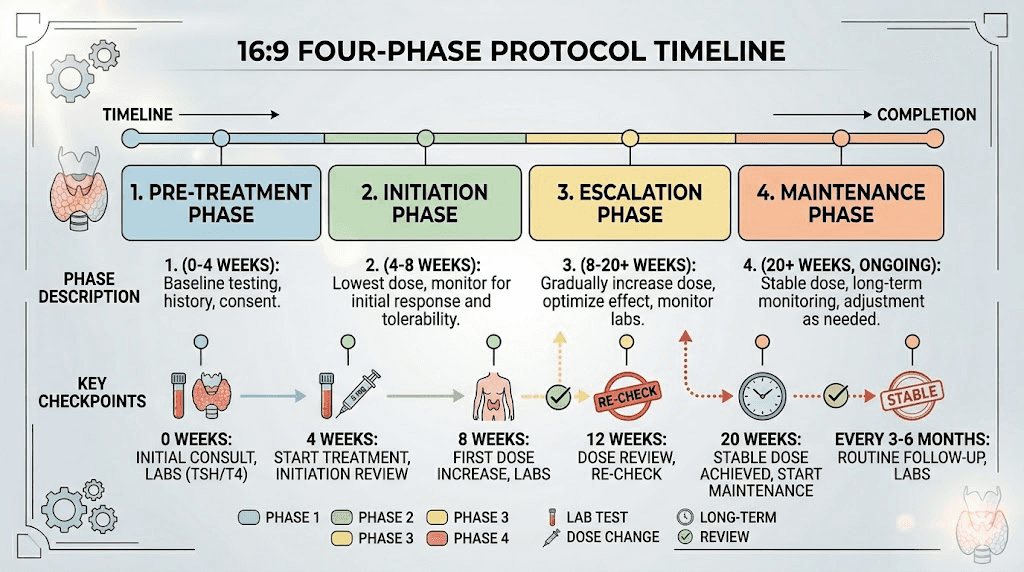
Protocol phase 1: pre-treatment (2 weeks before starting tirzepatide)
Labs: Get TSH, free T4, and free T3 drawn. Record results as your baseline. If your TSH is outside your personal target range, optimize your levothyroxine dose before starting tirzepatide. Adding a new variable when your thyroid is already unstable makes management significantly harder.
Timing decision: Decide whether to keep morning levothyroxine dosing or switch to bedtime. If switching to bedtime, make the change now and plan to recheck thyroid labs in 6 weeks to establish a new baseline before starting tirzepatide. This ensures you have a stable reference point.
Documentation: Start your medication log. Record your current levothyroxine dose, your TSH target, your tirzepatide start date, and your planned monitoring schedule. Having everything documented prevents confusion later. Use your injection tracking system from day one.
Protocol phase 2: initiation (weeks 1 through 8)
Week 1: Begin tirzepatide at 2.5mg. Take levothyroxine at your established time, separated from tirzepatide by maximum hours. Note any new symptoms daily for the first 2 weeks, paying particular attention to heart rate, energy levels, and mood changes.
Week 4: Escalate tirzepatide to 5mg per standard dosing protocol. This is when gastric emptying effects may be most pronounced. Increased GI symptoms are normal during dose escalation but should be monitored alongside thyroid symptoms.
Weeks 6 to 8: Get thyroid labs drawn. This is the most critical test in the entire protocol. If TSH has dropped below target or below normal range, discuss levothyroxine dose reduction with your prescriber. Typical reduction is 12.5 to 25mcg.
Protocol phase 3: escalation and optimization (months 3 through 6)
Continue tirzepatide dose escalation according to your prescribed schedule. Recheck thyroid labs 6 to 8 weeks after each tirzepatide dose increase, or after any levothyroxine adjustment. Track weight loss and note each time you reach a 10% weight loss milestone from baseline, as each milestone should trigger additional thyroid monitoring.
During this phase, most patients who need levothyroxine adjustments will have their first or second dose reduction. The goal is to keep TSH within your personal target range while maximizing the weight loss benefits of tirzepatide.
Protocol phase 4: maintenance (months 6 through 12 and beyond)
Once your tirzepatide dose is stable at maintenance level and your weight loss has begun to plateau, thyroid monitoring can decrease to every 3 to 6 months for the remainder of the first year, then annually if levels remain stable. Continue taking levothyroxine at your adjusted dose with consistent timing.
Ongoing weight management with GLP-1 maintenance dosing supports long-term metabolic health. Your levothyroxine dose during this phase should reflect your current body weight and composition, not your pre-treatment weight.
Protocol summary table
Phase | Timeline | Key actions | Thyroid labs |
|---|---|---|---|
Pre-treatment | 2 weeks before | Baseline labs, timing decision, documentation | TSH, fT4, fT3 |
Initiation | Weeks 1-8 | Start tirzepatide, escalate to 5mg, symptom tracking | Recheck at week 6-8 |
Escalation | Months 3-6 | Continue dose escalation, weight monitoring | Every 6-8 weeks after dose changes |
Maintenance | Month 6+ | Stable dosing, lifestyle optimization | Every 3-6 months, then annually |
Diet and lifestyle optimization for thyroid patients on tirzepatide
Managing the dual demands of thyroid health and GLP-1 treatment requires thoughtful attention to nutrition, hydration, and daily habits. The standard dietary recommendations for tirzepatide need slight modification when thyroid health is part of the equation.
Nutrition priorities for thyroid and weight loss
Protein becomes your most critical macronutrient when combining these medications. Both tirzepatide-induced weight loss and hypothyroidism can contribute to muscle loss if protein intake is inadequate. Target 1.2 to 1.6 grams of protein per kilogram of body weight daily, spread across multiple meals. The protein guidelines for GLP-1 users apply equally to tirzepatide, but thyroid patients should be especially vigilant because muscle mass directly influences metabolic rate and thyroid hormone requirements.
Iodine intake matters for thyroid function but rarely needs supplementation if you eat a varied diet including seafood, dairy, and iodized salt. Over-supplementing iodine can actually worsen autoimmune thyroid conditions like Hashimoto disease. Selenium, found in Brazil nuts, fish, and eggs, supports thyroid enzyme function and may reduce thyroid antibody levels. Two to three Brazil nuts daily provides approximately 200mcg of selenium, which is within the recommended range.
Fiber intake requires careful management. Both tirzepatide and hypothyroidism can cause constipation, so adequate fiber, 25 to 30 grams daily, is important. However, high-fiber meals can reduce levothyroxine absorption, so separate your highest-fiber meals from your levothyroxine dose by at least 2 to 4 hours. The best fiber supplements for GLP-1 users should be taken at a time that does not interfere with thyroid medication absorption.
Hydration is particularly important because both tirzepatide and thyroid hormone metabolism depend on adequate fluid intake. Aim for at least 64 to 80 ounces of water daily. Dehydration can concentrate thyroid hormone in the blood, artificially altering lab values, and can worsen the thirst that tirzepatide sometimes causes.
Foods that interfere with levothyroxine
Beyond the tirzepatide interaction, certain foods and supplements directly interfere with levothyroxine absorption. These become even more important to manage when gastric emptying is already altered.
Soy products can reduce levothyroxine absorption and should be consumed at least 4 hours away from your thyroid medication. Coffee, even black coffee, reduces absorption and should be consumed at least 30 minutes after taking levothyroxine. Calcium-fortified foods and beverages, including fortified orange juice and plant milks, should be separated by 4 hours. Grapefruit can alter thyroid hormone metabolism in some individuals.
When following a structured diet plan on tirzepatide, build your meal timing around your levothyroxine schedule rather than the other way around. The thyroid medication timing is more rigid and has more food interactions than tirzepatide, which can be injected at any time regardless of meals.
Exercise considerations for thyroid patients on GLP-1 medications
Resistance training is not optional when combining tirzepatide with levothyroxine. Both weight loss and hypothyroidism predispose to muscle loss, and losing muscle mass reduces metabolic rate, which can paradoxically increase your levothyroxine needs while simultaneously making weight loss harder. Two to three strength training sessions per week targeting all major muscle groups provides the minimum effective dose for muscle preservation.
Cardiovascular exercise supports both weight loss and thyroid health. The combination of creatine and tirzepatide may support exercise performance and muscle maintenance during weight loss. Start with 20 to 30 minutes of moderate-intensity cardio most days and increase gradually as your fitness improves and side effects stabilize.
Monitor your exercise tolerance carefully. If your levothyroxine dose is too high, you may notice an abnormally elevated heart rate during exercise, exercise intolerance, or excessive fatigue after workouts. These signs should prompt a thyroid function check. Conversely, if your dose is too low, you may feel sluggish during workouts with poor recovery, which also warrants lab testing.
Understanding thyroid blood tests and what they mean
To manage the tirzepatide-levothyroxine interaction effectively, you need a basic understanding of what your thyroid tests actually measure and what changes indicate.
TSH (thyroid-stimulating hormone)
TSH is produced by your pituitary gland. When your body has enough thyroid hormone, TSH drops. When thyroid hormone is insufficient, TSH rises. This inverse relationship is why a low TSH on tirzepatide can indicate levothyroxine overmedication, your body is absorbing more thyroid hormone than intended, so the pituitary reduces TSH production.
Normal TSH range is typically 0.4 to 4.0, though most endocrinologists prefer TSH between 0.5 and 2.5 for patients on replacement therapy. Your personal target may differ based on your specific condition, age, and symptoms. Below 0.3 generally indicates overmedication. Below 0.1 indicates significant suppression that requires prompt dose reduction.
Free T4 (free thyroxine)
Free T4 is the unbound, active form of the thyroid hormone T4 in your blood. It provides a direct measurement of thyroid hormone availability. While TSH tells you what your pituitary thinks about your thyroid status, free T4 tells you how much thyroid hormone is actually circulating. If TSH is low and free T4 is elevated, you are definitively overmedicated. If TSH is low but free T4 is normal, the situation is less clear and may warrant monitoring rather than immediate dose change.
Free T3 (free triiodothyronine)
T3 is the more biologically active thyroid hormone. Most T3 is converted from T4 in peripheral tissues. Some practitioners monitor free T3, particularly in patients who report symptoms despite normal TSH and free T4 values. Changes in body composition from tirzepatide weight loss can theoretically affect T4-to-T3 conversion, though this effect has not been well-studied in the context of GLP-1 treatment.
Thyroid antibodies
For Hashimoto patients, thyroid peroxidase (TPO) and thyroglobulin (TG) antibodies indicate the degree of autoimmune activity against your thyroid. While tirzepatide does not directly affect these antibodies, some research suggests that significant weight loss can reduce systemic inflammation, which may secondarily reduce antibody levels in some patients. However, this is not a reliable or expected outcome and should not influence your decision to start tirzepatide.
Common mistakes to avoid
After reviewing the clinical data and common patient experiences, several recurring mistakes emerge that can be easily prevented with awareness.
Mistake 1: not telling your prescriber about levothyroxine
This seems obvious, but many patients start tirzepatide through telehealth platforms or compounding pharmacy services without providing a complete medication history. Every prescriber involved in your care needs to know about both medications. If you are obtaining tirzepatide through one provider and levothyroxine through another, both need to be informed about the other medication.
Mistake 2: skipping the 6 to 8 week thyroid check
The single most impactful monitoring test is the 6 to 8 week post-initiation thyroid panel. Skipping it means flying blind during the period of greatest risk for absorption-driven thyroid changes. Even if you feel perfectly fine, get the labs drawn. TSH changes can precede symptoms by weeks.
Mistake 3: adjusting levothyroxine without lab confirmation
Neither preemptive dose reductions before starting tirzepatide nor reactive dose changes based on symptoms alone are appropriate. Always confirm with lab work before changing your levothyroxine dose. The interaction affects patients differently, and assumptions about how it will affect you specifically are unreliable.
Mistake 4: attributing all symptoms to tirzepatide
When you start a new medication, every new symptom gets attributed to it. But palpitations, anxiety, insomnia, tremor, and excessive sweating on tirzepatide might actually be thyroid overmedication masquerading as tirzepatide side effects. A simple blood test distinguishes between the two, and the treatment for each is completely different.
Mistake 5: ignoring the storage and preparation basics
Proper tirzepatide storage matters for consistent medication potency. If your tirzepatide degrades from improper storage, its effects on gastric emptying become unpredictable, which makes your levothyroxine absorption equally unpredictable. Follow shelf life guidelines carefully and verify that temperature excursions have not compromised your medication before injecting. Inconsistent tirzepatide potency creates an extra variable that makes thyroid management unnecessarily complicated.
Mistake 6: forgetting about the interaction when stopping tirzepatide
If you discontinue tirzepatide, your levothyroxine requirements change again. Gastric emptying normalizes, absorption decreases to its original level, and if you regain weight, your dose may need to increase. Post-discontinuation thyroid monitoring at 6 to 8 weeks is just as important as the initial monitoring.
Frequently asked questions
Can I take tirzepatide and levothyroxine at the same time?
You should not take them at the same time. Separate the two medications by as many hours as possible. Take levothyroxine in the morning on an empty stomach and administer your weekly tirzepatide injection in the evening, or vice versa. The delayed gastric emptying caused by tirzepatide can increase GLP-1 effects on levothyroxine absorption if they are taken in close proximity.
How soon after starting tirzepatide should I check my thyroid levels?
Get a baseline thyroid panel before starting tirzepatide, then recheck TSH and free T4 at 6 to 8 weeks. Research shows that 65% of hypothyroid patients on stable levothyroxine experienced TSH changes within this timeframe. Earlier testing at 4 weeks may be warranted if you experience symptoms of thyroid overmedication such as palpitations, anxiety, or tremor.
Will tirzepatide make my hypothyroidism worse?
Tirzepatide does not worsen hypothyroidism itself. The concern is that it alters how your body absorbs levothyroxine, potentially increasing absorption and causing overmedication. With proper monitoring and dose adjustments, most hypothyroid patients tolerate tirzepatide well. The benefits of tirzepatide for weight management can actually improve overall metabolic health in hypothyroid patients.
Does tirzepatide affect thyroid function in people without thyroid disease?
For people with normally functioning thyroids who do not take levothyroxine, tirzepatide is unlikely to cause clinically significant thyroid problems. The interaction concern is specific to people taking exogenous thyroid hormone, where absorption changes translate directly to dose changes. All GLP-1 agonists carry a precautionary label about thyroid C-cell tumors based on rodent studies, though this has not been confirmed in humans.
Should I take my levothyroxine before or after my tirzepatide injection day?
Since tirzepatide effects persist throughout the dosing interval due to its approximately 5-day half-life, the specific day matters less than consistent daily timing for your levothyroxine. Take your levothyroxine at the same time every day, maintain separation from your tirzepatide injection, and focus on regular monitoring rather than trying to time around injection days.
Can I still lose weight on tirzepatide if I have hypothyroidism?
Yes. Clinical evidence supports that tirzepatide produces significant weight loss in hypothyroid patients, provided their thyroid hormone levels are well-managed. Properly treated hypothyroidism should not significantly limit tirzepatide effectiveness. If you are not losing weight on tirzepatide, ensure your thyroid levels are optimized as a first step, because untreated or undertreated hypothyroidism can blunt the metabolic effects of any weight loss intervention.
Do I need to see an endocrinologist, or can my primary care doctor manage this?
Most primary care physicians can manage straightforward cases, meaning Hashimoto patients on stable levothyroxine doses adding tirzepatide for weight loss. However, referral to an endocrinologist is advisable for post-thyroidectomy patients, thyroid cancer survivors on suppression therapy, patients with difficulty achieving stable thyroid levels, or anyone experiencing persistent symptoms despite lab adjustments.
Is the interaction worse with compounded tirzepatide versus brand-name Mounjaro?
The mechanism of interaction is identical regardless of the tirzepatide formulation. Both compounded and brand-name tirzepatide act on the same GIP and GLP-1 receptors and produce the same gastric emptying effects. The important variable is your tirzepatide dose, not the source. Use the same monitoring protocol whether you are on compounded tirzepatide or pharmaceutical formulations. The difference between brand names does not affect the thyroid interaction.
Can I take berberine or metformin alongside both medications?
Both berberine and metformin are commonly used alongside tirzepatide for blood sugar management. Neither directly interacts with levothyroxine, but adding more oral medications to the mix increases the importance of strategic timing. Space berberine or metformin at least 2 hours from levothyroxine, and maintain the same separation from tirzepatide injection timing. If you are managing three or more daily medications alongside weekly tirzepatide, create a written schedule to ensure consistent spacing.
External resources
Levothyroxine and tirzepatide drug interaction checker (Drugs.com)
Hypothyroidism overview and treatment guidelines (Mayo Clinic)
Understanding thyroid function tests (American Thyroid Association)
Managing thyroid health alongside weight loss medication is a balancing act, but it does not have to be a guessing game. The interaction between tirzepatide and levothyroxine is well-documented, predictable, and manageable with the right monitoring protocol. Whether you are using a tirzepatide dosage calculator to dial in your dose or reviewing your reconstitution charts, adding thyroid monitoring to your routine is straightforward once you understand the protocol.
The most successful patients are those who approach both medications with equal attention and respect. Your thyroid health is the foundation upon which tirzepatide results are built. When that foundation is solid, through proper monitoring, timely dose adjustments, and consistent medication timing, the combination of these two medications can produce transformative results for both weight management and metabolic health.
For researchers and patients navigating these medications together, SeekPeptides offers comprehensive protocol guides, dosing calculators, and a community of people who have successfully managed this exact combination. Members access detailed interaction databases, personalized protocol guidance, and direct support from experienced researchers who understand the nuances of combining GLP-1 therapy with thyroid management.
In case I do not see you, good afternoon, good evening, and good night. May your thyroid levels stay balanced, your weight loss stay consistent, and your monitoring stay on schedule.