Mar 25, 2026

What if the real problem with your semaglutide protocol is not the dose itself, but how often you inject it? Thousands of people ask this question every month. They have reached their goal weight. They feel good. The side effects have calmed down. And now they wonder whether they really need to keep jabbing themselves every seven days for the rest of their lives.
It is a fair question. Semaglutide costs real money. The injections, even when routine, still require planning around travel, storage, and schedules. And for people who have already lost the weight, the idea of stretching doses to every other week sounds like a reasonable compromise between staying on the medication and stopping entirely.
But reasonable and safe are not the same thing. The pharmacology of semaglutide was designed around a very specific dosing interval.
Changing that interval changes the drug levels in your blood, the appetite suppression you feel, and the metabolic effects that keep the weight off. Some of those changes matter more than others. And a modeling study published in early 2025 suggests the picture is more nuanced than most people realize.
This guide breaks down everything you need to know about semaglutide every other week dosing. The pharmacokinetics behind it. What the research actually shows about weight loss retention. Who might benefit, who should avoid it, and how to make the transition safely if your provider approves it. No guesswork. No oversimplifications. Just the data and what it means for your protocol.
The short answer
Yes, some people do take semaglutide every other week. No, it is not FDA-approved at that frequency. The standard approved schedule for both Ozempic and Wegovy is once weekly, and every clinical trial that established the safety and efficacy of semaglutide used weekly dosing exclusively.
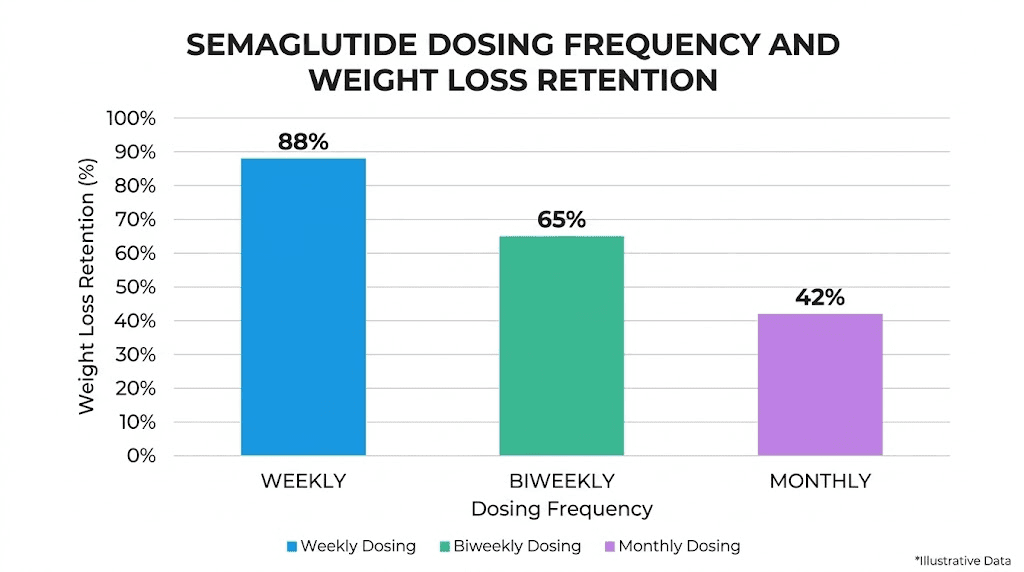
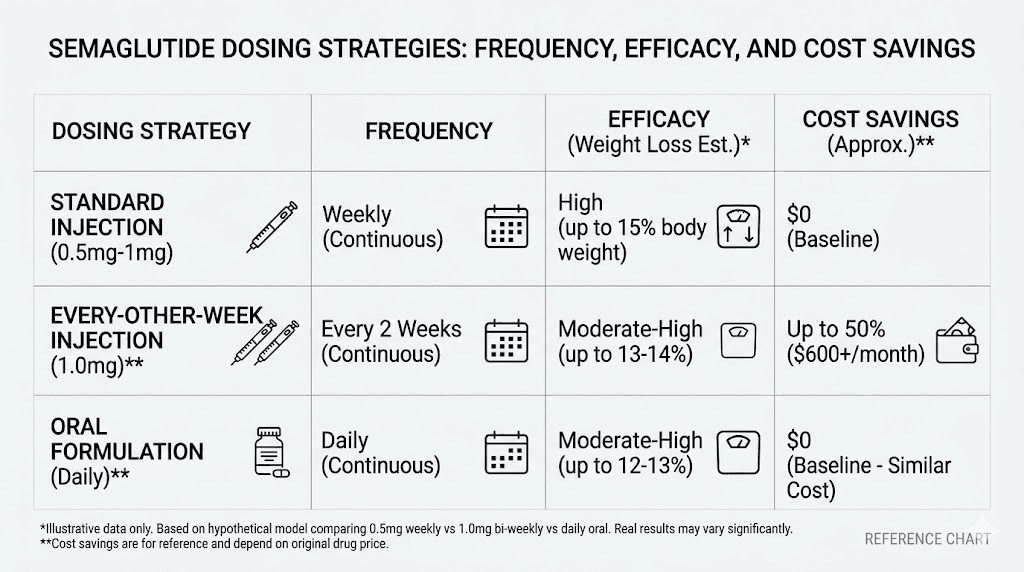
That said, every other week dosing has emerged as an off-label maintenance strategy. Some clinicians prescribe it for patients who have already reached their weight loss goals and want to reduce cost, injection frequency, or side effect burden. A 2025 pharmacokinetic modeling study found that switching from weekly to every-two-weeks dosing at the same dose retains approximately 72 to 75 percent of the weight loss effect. Not zero. Not full. Somewhere in between.
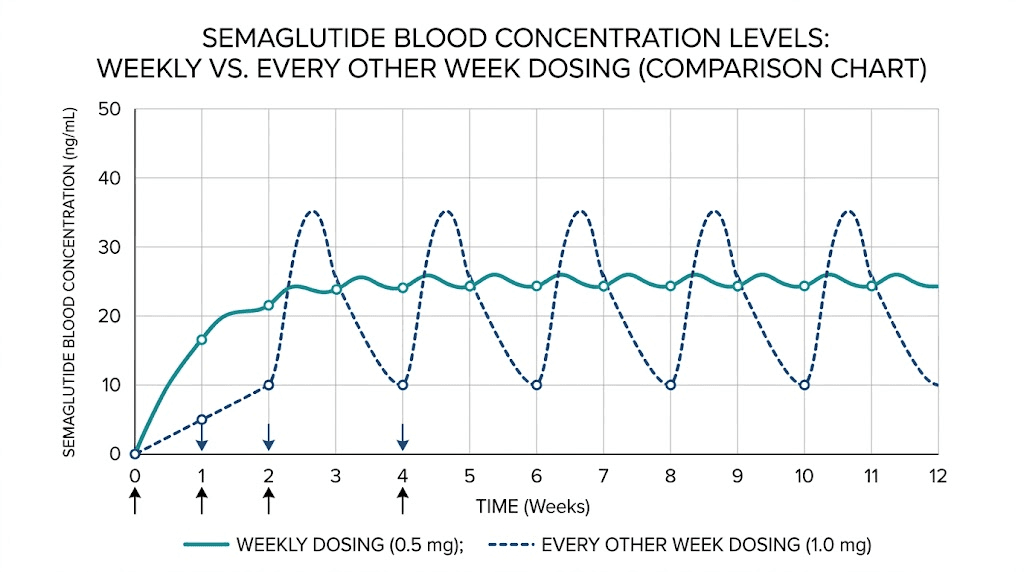
The catch? Your blood levels of semaglutide will fluctuate significantly more. Peak-to-trough variability increases by about 34 percent compared to weekly dosing, and peak concentrations drop by roughly 38 percent. That means the appetite suppression you rely on will wax and wane in ways it does not with weekly injections.
For someone actively losing weight, this matters a lot. For someone maintaining a stable weight with established habits, it might matter less.
Why semaglutide is designed for weekly dosing
Understanding why every other week dosing is even a conversation requires understanding what makes semaglutide different from older GLP-1 medications. The answer comes down to one number. 168 hours. That is the approximate half-life of semaglutide, which translates to roughly seven days.
Half-life means the time it takes for your body to eliminate half the drug from your bloodstream. With a seven-day half-life, semaglutide was engineered specifically for once-weekly administration. The structural modifications that make this possible, primarily albumin binding and resistance to DPP-4 enzymatic breakdown, keep the molecule circulating far longer than natural GLP-1, which lasts only minutes.
How steady state works
When you inject semaglutide weekly, each dose builds on the previous one. The drug accumulates gradually over the first four to five weeks until it reaches what pharmacologists call steady state. At that point, the amount entering your system each week roughly equals the amount being eliminated. Your blood levels stabilize into a predictable pattern with relatively small peaks and troughs.
This is important. The appetite suppression you feel, the metabolic improvements, the glucose control, all of these depend on maintaining drug levels within a therapeutic window. Weekly dosing keeps those levels remarkably consistent once steady state is achieved.
Switch to every other week, and the math changes. Drug levels peak after injection, then decline much further before the next dose arrives. Instead of a gentle wave pattern, you get deeper valleys. During those valleys, the therapeutic effects diminish.
The accumulation factor
Here is another detail most guides skip. Because semaglutide has such a long half-life, it does not disappear between doses even with biweekly spacing. After your injection, levels peak around 24 to 72 hours, then slowly decline. By day 14, you still have meaningful drug in your system. Just less of it.
How much less? The modeling data suggests peak concentrations drop by approximately 38 percent compared to weekly dosing. That is significant but not catastrophic. You are not starting from zero every two weeks. You are starting from a lower baseline and riding a bigger wave up and down.
This pharmacokinetic reality is why every other week dosing retains some efficacy rather than cutting it in half. The drug simply does not leave your body fast enough for a 14-day gap to wipe out all therapeutic effects. It takes roughly five weeks after your final dose for semaglutide to be essentially cleared from your system.
What the research actually shows
The most important piece of evidence on this topic comes from a pharmacokinetic and pharmacodynamic modeling study published in 2025 in the medical literature. This was not a traditional clinical trial with patients receiving every other week doses. It was a mathematical modeling analysis using established pharmacological data to predict what would happen with alternative dosing regimens.
The distinction matters. We are talking about predictions based on solid pharmacological models, not observed outcomes from a randomized controlled trial. That said, the findings are compelling and internally consistent.
Key findings for semaglutide
At the standard 2.4 mg weekly dose used for weight management, semaglutide produces approximately 17 percent steady-state body weight reduction. Switching to the same 2.4 mg dose every two weeks reduces that to approximately 12 percent, retaining about 72 percent of the weight loss effect.
The numbers get more interesting when you adjust the dose.
At 1.7 mg weekly, switching to 1.7 mg every two weeks retains 69 percent of weight loss while cutting costs by 50 percent. But if you increase to 2.4 mg every two weeks, which means injecting a higher single dose less frequently, you retain approximately 82 percent of the weight loss at half the cost. That is a meaningful difference.
The study also modeled even less frequent dosing. Monthly semaglutide at the same dose retained about 50 percent of the weekly weight loss effect. Less impressive, but still not nothing for someone primarily focused on maintenance rather than active loss.
The cost-efficacy tradeoff
This is where the modeling gets genuinely useful. The researchers framed their findings around a critical public health question. If the drug supply is limited, which it often is, does it make more sense to give full weekly doses to fewer people or biweekly doses to more people?
Their analysis suggested that at a fixed national supply of 3.3 billion mg annually, weekly dosing at 2.4 mg could reach about 25 percent of obese adults and save approximately 70,000 lives. Biweekly dosing at the same dose could reach 50 percent of obese adults and save approximately 100,000 lives. More people receiving less frequent treatment produced a bigger population-level benefit than fewer people receiving the standard protocol.
For individuals rather than populations, the calculation is different. You are not optimizing for national health outcomes. You are optimizing for your own results. And those results depend heavily on where you are in your weight loss journey.
Who might benefit from every other week dosing
Not everyone should even consider this. But for the right candidates, biweekly dosing can be a legitimate maintenance strategy. The key word is maintenance. This is not an approach for the active weight loss phase.
People who have reached their goal weight
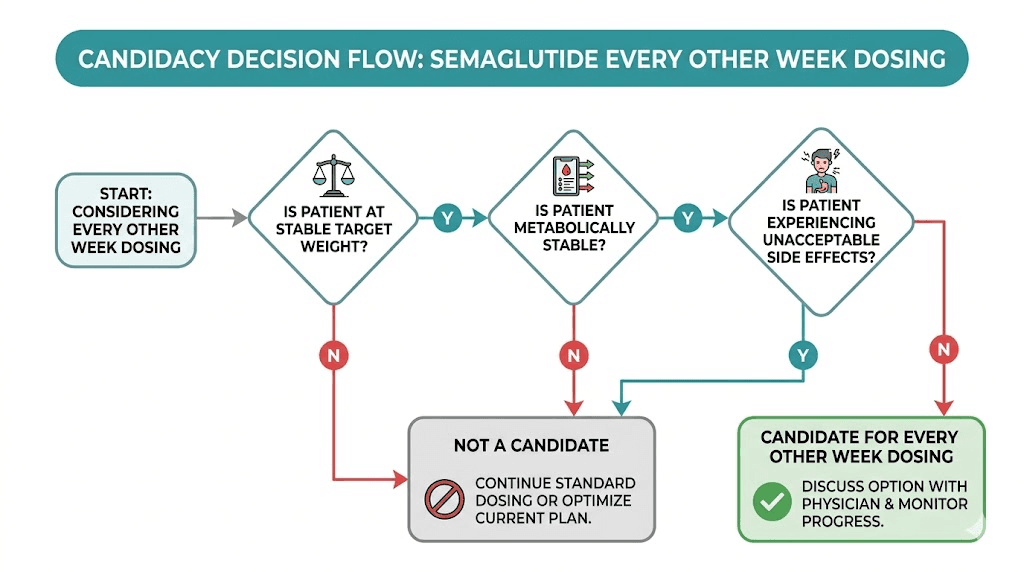
If you have already achieved your target weight and maintained it on standard weekly dosing for several months, you are in the strongest position to consider this change. Your body has adapted. Your eating habits have shifted. The medication is doing maintenance work rather than heavy lifting.
The difference is substantial. During active weight loss, you need consistent appetite suppression and metabolic support to push through plateaus and override your body natural tendency to resist further loss. During maintenance, you primarily need enough medication to prevent the gradual return of old eating patterns and food noise.
People with stable metabolic markers
If you are using semaglutide for type 2 diabetes management, this gets more complicated. Blood sugar control depends on consistent GLP-1 receptor activation, and the fluctuations from biweekly dosing could lead to periods of suboptimal glycemic control. Your A1c, fasting glucose, and postprandial numbers all need to be stable and within target range before any frequency reduction is safe to discuss.
For weight management patients without diabetes, the metabolic considerations are simpler but still matter. Your blood work should show stable liver enzymes, kidney function, and inflammatory markers.
People with cost as a primary barrier
Let us be honest about this. Semaglutide is expensive. Even with insurance, copays can be significant. Without insurance, the cost is prohibitive for many people. If the choice is between every other week dosing and stopping entirely, biweekly injections at 72 to 82 percent efficacy dramatically outperform zero percent efficacy from discontinuation.
Research consistently shows that people who stop semaglutide entirely can regain up to two-thirds of their lost weight. That makes even a reduced-frequency protocol vastly superior to stopping. Compounded semaglutide options may also help with cost, but availability varies and the regulatory landscape changes frequently.
People with lifestyle or travel constraints
Weekly injections require consistent access to refrigeration, injection supplies, and a private space. For people who travel frequently or have demanding schedules, reducing injection frequency by half removes a real practical burden. A travel case for GLP-1 medications helps, but fewer injections means fewer logistics to manage.
Who should NOT switch to every other week
Some people should stay on weekly dosing. Period.
People actively losing weight
If you have not yet reached your goal weight, reducing frequency will almost certainly slow your progress. The 25 to 28 percent reduction in efficacy from biweekly dosing means less appetite suppression during the phase when you need it most. Your caloric deficit becomes harder to maintain. Cravings return partially. And the metabolic advantages that help push through plateaus diminish.
If you are currently in the early weeks of treatment, switching to biweekly dosing would prevent you from ever reaching steady state at therapeutic levels. The escalation protocol exists for a reason. Follow it.
People with uncontrolled diabetes
If your A1c is not at target, if your fasting glucose fluctuates significantly, or if your provider has recently adjusted your diabetes medications, biweekly semaglutide creates unacceptable gaps in glycemic control. The deeper troughs in drug levels mean periods where your GLP-1 receptor activation drops well below the therapeutic threshold for blood sugar management.
People with a history of rapid weight regain
Some people are metabolically predisposed to rapid rebound. If you have a history of losing weight and gaining it back quickly when you reduce or stop interventions, the valleys in drug levels during biweekly dosing could trigger exactly the kind of appetite surge and metabolic shift that leads to regain. For this group, the risks of reduced efficacy outweigh the convenience benefits.
People who experience strong hunger signals between doses
Even on weekly dosing, some people notice a return of food noise and increased appetite in the day or two before their next injection. If you already feel the medication wearing off by day six or seven, doubling that gap to 14 days will create an extended period of reduced appetite control. That is a recipe for overeating, guilt, and frustration.
How to transition safely
If you and your provider decide that every other week dosing is worth trying, the transition should be methodical. Rushing this creates unnecessary risk.
Step 1: Establish a stable baseline
Before changing anything, you need at least three months of stable weight on your current weekly dose. Not actively losing. Not fluctuating. Stable. This proves that your current habits, combined with the medication, are enough to maintain your results. It also means you have been at steady state long enough for your body to establish a reliable equilibrium.
Document your weight, key measurements, and how you feel. Note your hunger patterns, energy levels, and any side effects on weekly dosing. This becomes your comparison point.
Step 2: Have a detailed conversation with your provider
This is not a DIY decision. Your provider needs to evaluate your metabolic markers, weight stability, medication interactions, and overall health status before approving a frequency change. They may want to check your blood work as a baseline before the switch.
Be direct about your reasons. Cost, convenience, side effect management, or simply wanting fewer injections are all valid motivations. Your provider can help determine if the tradeoff makes sense for your specific situation.
Step 3: Consider a dose adjustment
The modeling research shows that simply extending the interval at the same dose retains about 72 percent of efficacy. But increasing the dose while extending the interval can recover much of that lost ground. Moving from 1.7 mg weekly to 2.4 mg every two weeks, for example, retains approximately 82 percent of weight loss.
Your provider may suggest maintaining or even slightly increasing your per-injection dose to compensate for the longer interval. Use the semaglutide dosage calculator to understand how different doses translate in terms of units and concentrations, especially if you use compounded semaglutide.
Step 4: Run a trial period of 4 to 8 weeks
Switch to biweekly dosing and monitor closely. Weigh yourself at the same time, same conditions, at least twice per week. Track your hunger levels daily, noting specifically how you feel during days 10 through 14, the period when drug levels will be at their lowest.
Use a GLP-1 injection tracker to maintain consistency. The two-week interval is longer and easier to lose track of than a weekly habit.
Step 5: Apply the three-pound rule
This is a practical threshold many clinicians use. If your weight increases by more than three pounds above your stable maintenance weight during the trial period, the biweekly protocol is not providing enough coverage. At that point, you either return to weekly dosing or discuss increasing the biweekly dose with your provider.
Three pounds matters because it sits above normal daily fluctuations from water, food, and hormonal cycles, but catches meaningful regain before it snowballs. Do not wait for five or ten pounds of regain before acting. Early intervention preserves results.
Step 6: Reassess at 8 weeks
After two months on biweekly dosing, evaluate comprehensively. Has your weight been stable? Have your metabolic markers remained in range? Are you managing hunger adequately? Has your relationship with food shifted in ways that concern you?
If everything looks good, continue with regular monitoring. If there are warning signs, return to weekly dosing before the situation worsens.
What to monitor during every other week dosing
Switching to biweekly dosing means accepting greater variability in how the medication works throughout the two-week cycle. Monitoring becomes more important, not less.
Weight trends
Do not obsess over daily fluctuations. Look at weekly averages plotted over time. A stable trendline means the protocol is working. An upward drift, even a gradual one, means it is not. The monitoring tools available for home use can help you track trends objectively rather than reacting to individual weigh-ins.
Hunger patterns through the cycle
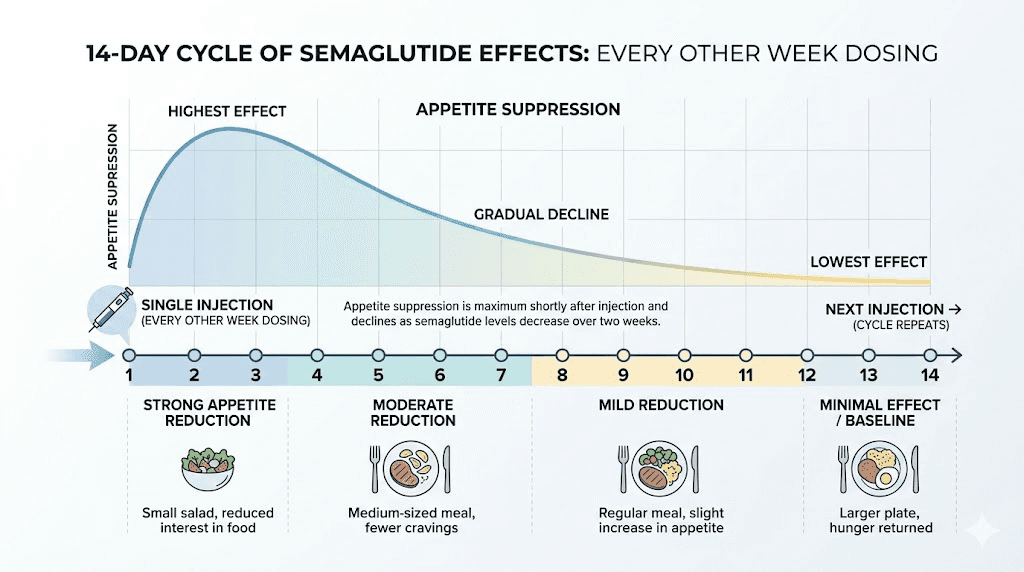
Pay close attention to how your appetite changes across the 14-day interval. Most people on biweekly dosing report a pattern that looks something like this.
Days 1 through 3 after injection: strong appetite suppression, minimal food noise, easy to maintain healthy portions. Similar to what you experience on standard weekly dosing.
Days 4 through 7: moderate appetite suppression, still manageable, slightly more awareness of food.
Days 8 through 10: appetite suppression noticeably weaker, food noise begins returning, portion control requires more conscious effort.
Days 11 through 14: the trough period. Drug levels are at their lowest. Appetite may approach pre-medication levels. This is the danger zone for overeating.
If you can navigate days 11 through 14 with the habits you have built, biweekly dosing can work. If those days consistently lead to binge eating or loss of control, the protocol needs adjustment.
Blood glucose (if applicable)
For anyone using semaglutide for diabetes or prediabetes, blood glucose monitoring during biweekly dosing is essential. Check fasting glucose and postprandial readings more frequently during the first few cycles to identify any concerning patterns during the trough period.
Gastrointestinal symptoms
This is counterintuitive, but some people experience more GI side effects with biweekly dosing, not fewer. The larger peak-to-trough swings mean your gut goes through repeated cycles of higher drug exposure followed by withdrawal. Constipation, bloating, and acid reflux may worsen in the first few days after each injection, then improve during the trough. If GI symptoms were your reason for switching to biweekly dosing, monitor whether the pattern actually improves.
Alternative strategies to reduce dosing burden
Every other week dosing is not the only option for people who want less frequent injections or lower costs. Several alternatives exist, each with different tradeoff profiles.
Dose reduction on a weekly schedule
Instead of extending the interval, you can reduce the dose while maintaining weekly timing. Dropping from 2.4 mg to 1.7 mg or even 1.0 mg weekly maintains the consistent drug levels that prevent appetite rebound while reducing the total amount of medication used. For many people in maintenance, a lower weekly dose provides enough appetite suppression without the peaks and troughs of biweekly dosing.
This approach has a pharmacokinetic advantage. Your blood levels stay smooth and predictable. The therapeutic effects remain consistent rather than cycling between strong and weak. The downside is that it does not reduce injection frequency, which matters for people whose primary motivation is fewer needles.
Extended interval compromise: 10 days
Some providers suggest a middle-ground approach. Instead of jumping from 7 days to 14, try 10-day intervals. This keeps drug levels closer to the weekly pattern while still reducing annual injections from 52 to about 36. It is a compromise that works well for people who tolerate a slight reduction in consistency but find 14 days too long.
The challenge is scheduling. A 10-day cycle does not align neatly with weeks, so your injection day constantly shifts. Using a tracking system becomes essential.
Splitting doses
An entirely different approach involves splitting your weekly dose into two smaller injections. Instead of one 2.4 mg injection weekly, you take two 1.2 mg injections. This actually smooths out blood levels even more than standard weekly dosing, potentially reducing side effects like dizziness and lightheadedness that come from high peak concentrations.
Splitting does not save money or reduce injection frequency. It is primarily a strategy for managing side effects rather than convenience. But it is worth knowing about if your reason for considering biweekly dosing is side effect management.
Oral semaglutide
The sublingual and oral semaglutide options eliminate the injection entirely while maintaining daily or weekly dosing. Rybelsus, the FDA-approved oral form, is taken daily. Compounded sublingual versions vary. The bioavailability is lower with oral administration, so doses are adjusted accordingly.
For people whose primary objection is needles rather than cost, oral options may solve the problem more directly than biweekly injectable dosing.
Switching to a longer-acting GLP-1
Other GLP-1 receptor agonists have different pharmacokinetic profiles. Tirzepatide, for example, has a half-life of about 5 days, and some people find its effects last well into the second week. The modeling study that examined semaglutide also found that tirzepatide every two weeks retains about 75 percent of weight loss, with less peak-to-trough variability than semaglutide at the same reduced frequency. Switching from semaglutide to tirzepatide could be a path worth discussing with your provider if less frequent dosing is a priority.
Every other week vs other frequency adjustments
How does biweekly dosing compare to other modifications? Here is a side-by-side look.
Strategy | Injection frequency | Estimated efficacy retained | Cost savings | Blood level stability | Best for |
|---|---|---|---|---|---|
Standard weekly 2.4 mg | Every 7 days | 100% | None | High | Active weight loss |
Reduced weekly 1.7 mg | Every 7 days | ~85% | ~30% | High | Maintenance, side effect management |
Every 10 days 2.4 mg | Every 10 days | ~85-90% | ~30% | Moderate | Moderate cost savings |
Every 2 weeks 2.4 mg | Every 14 days | ~72% | ~50% | Lower | Maintenance with cost priority |
Every 2 weeks higher dose | Every 14 days | ~82% | ~50% | Lower | Maintenance with optimized dose |
Monthly 2.4 mg | Every 30 days | ~50% | ~75% | Low | Minimal maintenance only |
Split dose twice weekly | Every 3-4 days | 100% | None | Very high | Side effect reduction |
The data tells a clear story. For people prioritizing cost savings, biweekly dosing at an adjusted dose offers the best balance between savings and retained efficacy. For people prioritizing consistent appetite suppression, reduced weekly dosing or split dosing maintains smoother drug levels. There is no single best answer. Only the best answer for your specific priorities.
Managing side effects during the transition
The shift from weekly to biweekly dosing changes your side effect profile. Some effects improve. Others may temporarily worsen.
Gastrointestinal effects
On weekly dosing, your gut adapts to a consistent level of GLP-1 receptor activation. The constipation, nausea, and delayed gastric emptying stabilize into a predictable pattern. Switch to biweekly, and you introduce larger swings. The days immediately after injection may bring stronger nausea as your body reacts to a relative surge after the trough period. Then symptoms ease as levels decline.
Managing this requires being strategic about food choices around injection day. Lighter meals, more fiber, adequate hydration, and electrolytes all help smooth the transition. The recommended foods for semaglutide users become even more important when your drug levels cycle more dramatically.
Energy and fatigue
Fatigue on semaglutide is common, and the pattern may shift with biweekly dosing. Some people report feeling more tired in the first two to three days after injection, when levels are highest, followed by improved energy during the trough period. Others find the opposite: fatigue worsens during the trough as the body adjusts to declining medication levels.
Track your energy patterns carefully through at least two full cycles. If fatigue worsens significantly, it may indicate that biweekly dosing is creating too much physiological stress from the repeated cycling.
Headaches and dizziness
The headaches and dizziness that some people experience on semaglutide may fluctuate more with biweekly dosing. These symptoms often correlate with blood sugar changes, and the wider drug level swings can mean wider glucose swings, particularly in the trough period when GLP-1 receptor activation is at its lowest.
Staying well-hydrated, maintaining consistent meal timing, and ensuring adequate protein intake all help stabilize blood sugar independent of medication levels. These habits become your safety net during the trough days.
The food noise cycle
This is perhaps the most noticeable change. On weekly dosing, food noise, that persistent background chatter about what to eat, when to eat, and how much to eat, stays relatively quiet. On biweekly dosing, expect it to return partially during days 10 through 14.
The key is recognizing this as a pharmacological phenomenon, not a personal failure. The medication is wearing off. Your brain reward circuits are getting louder. Having a structured meal plan and knowing which foods to avoid during this vulnerable window helps you ride it out without derailing your progress.
The role of lifestyle habits in making biweekly dosing work
Here is the truth that most dosing guides do not tell you. Every other week dosing works best for people who have already built strong habits that function independently of the medication. The drug provides a foundation, but during the trough period, your habits carry the weight.
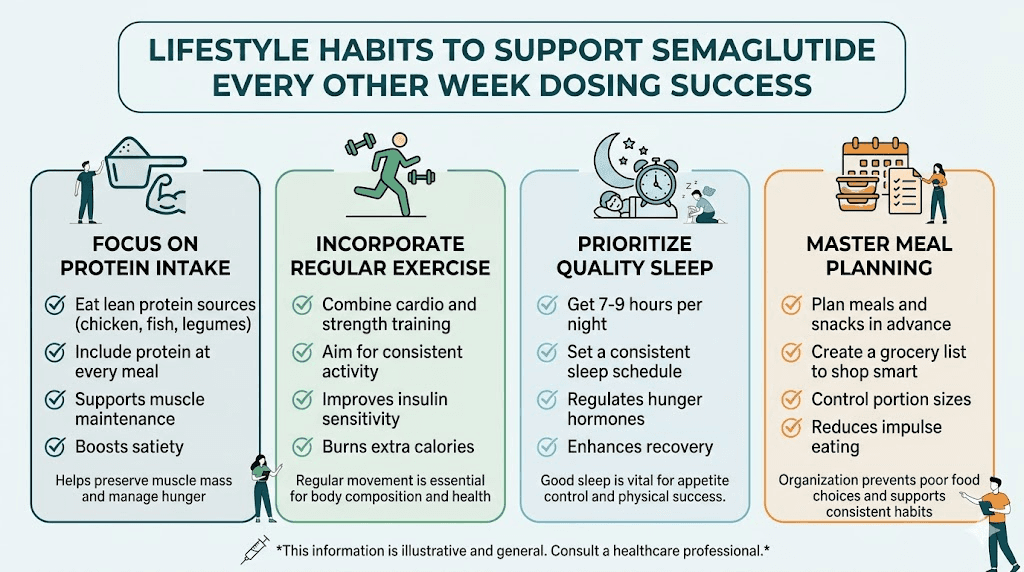
Protein is non-negotiable
Aim for 1.2 to 1.5 grams of protein per kilogram of body weight daily. Protein provides satiety that partially compensates for reduced medication-driven appetite suppression during the trough. It also protects muscle mass, which becomes more important with any reduction in GLP-1 therapy intensity. Creatine supplementation can further support muscle preservation.
Exercise as appetite regulation
Regular resistance training and moderate cardio both help regulate appetite through pathways independent of GLP-1. The appetite-suppressing effects of exercise are modest but real, and they stack with whatever medication-driven suppression remains during the trough. People who rely solely on medication without exercise have a harder time maintaining results at any dosing frequency.
Sleep and stress management
Poor sleep and chronic stress both increase appetite through cortisol and ghrelin pathways. If semaglutide already affects your sleep, switching to biweekly dosing may improve insomnia symptoms during the trough but worsen them around injection day. Managing stress through consistent routines, movement, and adequate rest creates a buffer that helps compensate for reduced pharmacological support.
Meal structure and timing
Having a consistent meal structure matters more on biweekly dosing than weekly. When drug levels are high, you naturally eat less and make better choices without much effort. When levels drop, structure prevents drift. Planning meals ahead of time, keeping GLP-1 friendly recipes in rotation, and having high-protein breakfasts ready to go all reduce the decision fatigue that leads to poor choices during the trough.
Supplements that support the transition
Several supplements commonly taken with GLP-1 medications become more valuable during biweekly dosing. B12 supplementation addresses potential absorption issues. Probiotics support gut function through the GI cycling. Glycine may support metabolic function. And electrolyte supplementation prevents the dehydration-related symptoms that fluctuating drug levels can exacerbate.
What happens if you need to go back to weekly
Good news. Returning to weekly dosing after a period of biweekly injections is straightforward. You do not need to re-titrate from the lowest dose like you did when first starting. Your body has already adapted to semaglutide, and resuming weekly timing simply restores the higher, more consistent drug levels you had before.
Some people experience a temporary increase in GI side effects when returning to weekly dosing, similar to what happens after restarting semaglutide after a break. This typically resolves within one to two weeks as your gut readjusts to the more frequent drug exposure.
The important thing is not to view a return to weekly dosing as failure. Think of it as information. You tested biweekly dosing, collected data on how your body responded, and made an informed decision to return to the protocol that works better for you. That is how responsible medication management works.
Compounded semaglutide and biweekly dosing
The every other week conversation becomes especially relevant for people using compounded semaglutide. Compounded versions often come in multi-dose vials at various concentrations, and the flexibility to adjust both dose size and frequency is built into the format.
If you are using compounded semaglutide, work with your provider to calculate the correct dose for biweekly administration. The math matters. You need to understand how units convert to milligrams and how your specific vial concentration affects the volume per injection. Using the semaglutide dosage calculator helps prevent dosing errors that become more consequential when you are injecting less frequently.
Storage considerations also change slightly. With weekly dosing, a vial of compounded semaglutide gets used relatively quickly. With biweekly dosing, the same vial lasts longer, which means proper refrigeration and shelf life management becomes more important. Make sure your vial will not expire before you finish it at the slower usage rate.
Some people on compounded semaglutide also use formulations that include additional ingredients like B12, glycine, or niacinamide. When switching to biweekly dosing, remember that you are also halving your intake of these additional compounds. Discuss with your provider whether supplementation is needed to compensate.
The missed dose question
Understanding the missed dose protocols for brand-name semaglutide provides useful context for the every other week discussion.
For Ozempic, if you miss a dose and fewer than five days have passed, take it as soon as you remember. If more than five days have passed, skip it and take your next scheduled dose.
For Wegovy, the guidance is slightly different. If your next dose is more than 48 hours away, take the missed dose. If it is within 48 hours, skip and wait for the next scheduled injection.
These protocols essentially tell you something important. The manufacturers acknowledge that occasional gaps of up to about 12 days (a missed weekly dose where you wait for the next one) are manageable. That is not the same as recommending biweekly dosing. But it does suggest that the drug remains active and useful even with irregular spacing.
If you are on biweekly dosing and miss your injection day, try to take it within two to three days. If you miss more than that, take it as soon as you remember and reset your two-week count from that point. Do not double up to compensate for the missed dose. Consistency in timing matters more than making up for gaps.
What about diabetes management specifically?
This deserves its own section because the stakes are higher. For people using semaglutide (specifically Ozempic) for type 2 diabetes, reducing dosing frequency directly impacts blood sugar control in ways that carry real health consequences.
The GLP-1 receptor activation that semaglutide provides serves multiple functions in diabetes. It stimulates insulin secretion in response to meals, suppresses glucagon release, slows gastric emptying, and reduces hepatic glucose output. All of these effects depend on adequate drug levels.
During the trough period of biweekly dosing, each of these effects weakens. The result can be higher fasting glucose readings, larger postprandial spikes, and a gradual drift upward in A1c over time. For someone whose diabetes is well-controlled on weekly semaglutide, even a modest deterioration in glycemic control carries cardiovascular implications.
If you have diabetes and want to reduce injection frequency, discuss alternatives with your endocrinologist rather than self-adjusting. They may suggest combining a lower dose of semaglutide with metformin or other oral diabetes medications to maintain glycemic control during the periods of lower GLP-1 activity.
Real-world experiences
Online communities are full of anecdotal reports from people who have tried biweekly semaglutide dosing. While anecdotal evidence has limitations, patterns emerge that align with the pharmacological predictions.
Many users report that biweekly dosing works well for maintenance but poorly for active weight loss. The most common complaint is the return of food noise and appetite in the second week. Some describe it as feeling like they are constantly fighting cravings for several days before each injection, while feeling great in the first week after.
Others report that biweekly dosing actually improved their quality of life. Fewer injections, fewer GI side effects overall, and a sense of normalcy that weekly dosing did not provide. These tend to be people who had already reached their goals and established strong healthy habits.
A common theme is the importance of not going it alone. People who worked with their providers to make the switch report better outcomes than those who simply started skipping doses without medical guidance. The difference often comes down to dose optimization, monitoring protocols, and having a clear plan for what to do if the approach is not working.
The insurance and cost reality
One practical consideration that drives many people to explore biweekly dosing is cost. Brand-name semaglutide, whether Ozempic or Wegovy, carries significant monthly costs that may or may not be covered by insurance.
Important note. Insurance companies that do cover semaglutide typically base coverage on the FDA-approved weekly dosing schedule. If your provider writes a prescription for biweekly dosing, it may not be covered, or the quantity limits on your prescription may not align with the biweekly schedule. Some people work around this by filling a standard weekly prescription and simply using it less frequently, effectively making their supply last twice as long.
For people using compounded semaglutide, the cost calculation is simpler. You buy the medication directly, and using it less frequently directly reduces your monthly spend. Compounded semaglutide from reputable providers already costs substantially less than brand-name versions, so biweekly dosing on top of compounded pricing can make the medication genuinely affordable for people on tight budgets.
Some people use flexible spending accounts or payment plans to manage costs. If cost is your primary motivator for biweekly dosing, explore all the financial options before making a pharmacological compromise.
Long-term outlook
The question of how long you can stay on biweekly semaglutide dosing does not have a definitive answer. No long-term studies have followed patients on this schedule for years. The modeling data suggests it is pharmacologically coherent. The clinical experience of providers who prescribe it suggests it works for maintenance. But we lack the 5-year and 10-year data that weekly dosing has from the STEP and SUSTAIN trials.
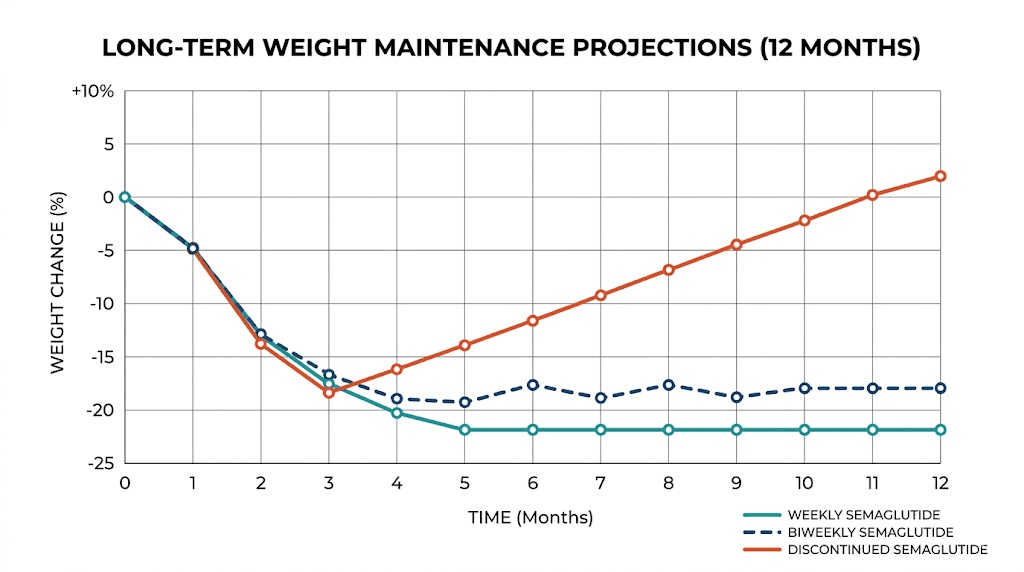
What we do know is that stopping semaglutide entirely leads to substantial weight regain in most people, with studies showing up to two-thirds of lost weight returning over time. We also know from the STEP 4 trial that continued weekly dosing maintains weight loss effectively. Biweekly dosing sits somewhere between these extremes, both pharmacologically and in terms of outcomes.
The GLP-1 maintenance dose strategy you choose should be one you can sustain long-term. If weekly dosing is too expensive or burdensome to maintain for years, a biweekly protocol that you actually stick with may produce better lifetime outcomes than a weekly protocol you eventually abandon due to cost or fatigue.
For researchers serious about optimizing their protocols, SeekPeptides offers comprehensive guides, dosing calculators, and evidence-based resources that help you make informed decisions about medication management. The platform provides access to detailed dosing charts, expected outcome data, and practical tools for tracking your results over time.
Frequently asked questions
Will I gain weight if I switch to semaglutide every other week?
Not necessarily. Research modeling suggests you retain approximately 72 to 82 percent of your weight loss effect depending on the dose used. However, you may experience a slight upward drift in weight if your habits do not compensate for the reduced medication coverage during the trough period. Monitor your weight closely during the first 4 to 8 weeks and use the three-pound rule as your guardrail.
Is every other week dosing FDA-approved?
No. The FDA has approved semaglutide for once-weekly use only, both for diabetes (Ozempic) and weight management (Wegovy). Every other week dosing is an off-label use that should only be pursued under medical supervision.
Can I just skip a dose one week and take it the next?
Occasional missed doses happen and are addressed in the prescribing information. But deliberately skipping every other dose as a consistent pattern is different from an occasional miss. If you want biweekly dosing, discuss it with your provider as a planned protocol change rather than simply skipping doses.
What dose should I take every other week?
The optimal biweekly dose depends on your current weekly dose and individual response. Maintaining or slightly increasing the per-injection dose can offset some of the efficacy loss. For example, switching from 1.7 mg weekly to 2.4 mg biweekly retains more efficacy than simply taking 1.7 mg biweekly. Use the semaglutide dosage calculator to work through the math with your provider.
Will my side effects improve on biweekly dosing?
Possibly. Overall drug exposure decreases, which may reduce chronic side effects like fatigue and constipation. However, the larger peak-to-trough swings may create a pattern of stronger acute effects after each injection followed by improvement during the trough. Net effect varies by individual.
Can I switch to biweekly during the dose escalation phase?
No. The initial dose escalation is specifically designed to build tolerance to semaglutide and reach therapeutic levels gradually. Switching to biweekly before completing escalation and reaching stable maintenance would prevent you from achieving steady state and could result in inadequate therapeutic coverage.
How long does it take to adjust to biweekly dosing?
Most people need two to four full biweekly cycles (4 to 8 weeks) to establish a new steady state and understand how the pattern affects them. The first cycle is often the most noticeable as your body adapts to the lower trough levels. By the third or fourth cycle, the pattern typically stabilizes.
Is biweekly dosing better than stopping entirely?
Yes, significantly. Research shows that stopping semaglutide completely leads to regain of up to two-thirds of lost weight. Biweekly dosing retains 72 to 82 percent of the weight loss effect, making it vastly superior to discontinuation for anyone who wants to maintain their results.
External resources
Once-Weekly Semaglutide in Adults with Overweight or Obesity, New England Journal of Medicine
STEP 4 Trial: Effect of Continued Weekly Subcutaneous Semaglutide on Weight Loss Maintenance, JAMA
In case I do not see you, good afternoon, good evening, and good night. May your drug levels stay stable, your appetite stay manageable, and your results stay lasting.