Mar 24, 2026

Experienced researchers have figured something out about tirzepatide that most people miss entirely. The weight comes off. Quickly, sometimes dramatically. But something else comes off too. Muscle. Bone density. The metabolic machinery that keeps weight off long term. And that is the dirty secret of GLP-1 weight loss, the part nobody wants to talk about when celebrating those before and after photos.
Up to 40% of the weight lost on GLP-1 medications can be lean tissue. Not fat. Muscle. The very tissue that drives metabolism, supports joints, and determines whether lost weight stays lost or comes roaring back.
This is where sermorelin enters the conversation.
Sermorelin is a growth hormone releasing hormone analog, a 29-amino-acid peptide that tells your pituitary gland to produce and release growth hormone naturally. When paired with tirzepatide, it creates something neither compound achieves alone: aggressive fat loss with meaningful muscle preservation. Two different systems working through two completely different pathways, targeting the same goal from opposite directions. SeekPeptides has tracked growing interest in this combination as researchers look beyond single-compound approaches to body composition optimization. This guide covers everything about combining these two peptides, from mechanisms and protocols to timing, side effects, monitoring, and realistic expectations for results.
What sermorelin is and how it works
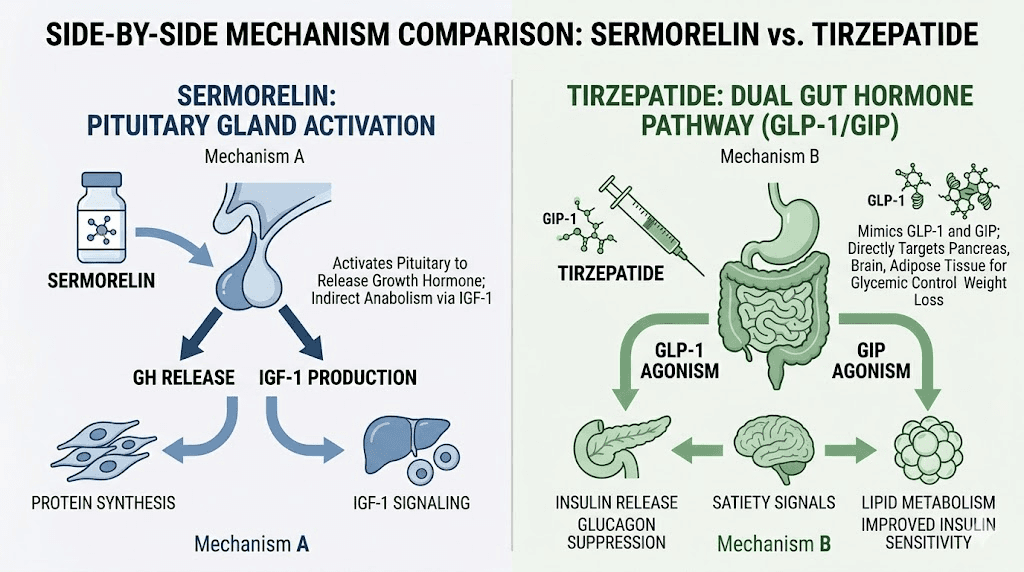
Sermorelin is not growth hormone. This distinction matters more than most people realize. Rather than flooding the body with exogenous hormone, sermorelin works upstream. It is a synthetic version of growth hormone releasing hormone, specifically the first 29 amino acids of the 44-amino-acid GHRH molecule. Those 29 amino acids represent the shortest fully functional fragment that can still activate the GHRH receptor on the pituitary gland.
Here is the key difference. When you inject synthetic HGH directly, you bypass every natural feedback mechanism. The pituitary gets no say. The hypothalamus gets no say. You simply dump a bolus of growth hormone into circulation and hope for the best. Sermorelin asks the pituitary to do its job. The gland responds by releasing growth hormone in natural pulses, maintaining the feedback loops that prevent overproduction.
Think of it this way. Direct HGH is like pouring water directly into a glass. Sermorelin is like turning on the faucet and letting the glass fill naturally, with the overflow drain still working.
The practical implications are significant. Because sermorelin preserves physiological pulsatility, the risk of supraphysiological growth hormone levels stays low. Side effects associated with HGH excess, things like insulin resistance, joint pain, carpal tunnel syndrome, and abnormal tissue growth, are far less likely with sermorelin than with direct growth hormone injection.
What sermorelin does in the body
When sermorelin binds to GHRH receptors on the anterior pituitary, it triggers a cascade that results in growth hormone release. That growth hormone then stimulates the liver to produce IGF-1 (insulin-like growth factor 1), which mediates many of the downstream effects people associate with growth hormone therapy.
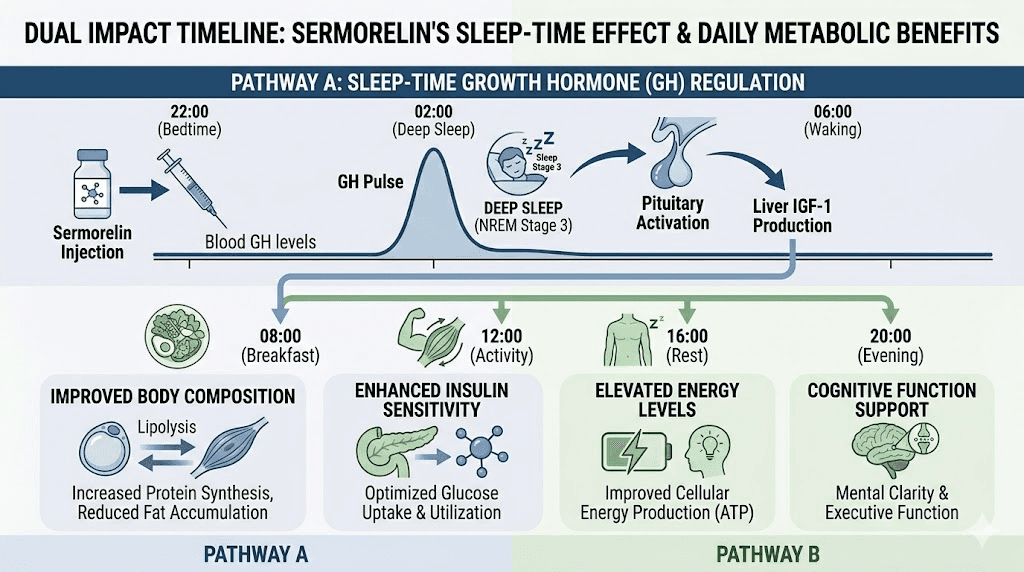
Those effects include increased lipolysis, the breakdown of stored fat for energy. They include enhanced protein synthesis, which supports muscle preservation and growth. Improved sleep quality, since growth hormone release naturally peaks during deep sleep phases. Better recovery from exercise and physical stress. Enhanced collagen synthesis for skin, connective tissue, and joint health. And improved bone mineral density over time.
One study found a 1.26 kg increase in lean mass after 16 weeks of sermorelin treatment in older adults. Not massive. But in the context of someone simultaneously losing fat on a GLP-1 medication, even maintaining lean mass, let alone gaining it, represents a significant advantage.
Sermorelin dosage basics
Standard sermorelin protocols use 200 to 300 mcg administered subcutaneously once daily. The injection goes under the skin, typically in the abdominal area, and is administered 30 to 60 minutes before bedtime on an empty stomach. The timing matters because it aligns with the natural nocturnal growth hormone surge that occurs during deep sleep.
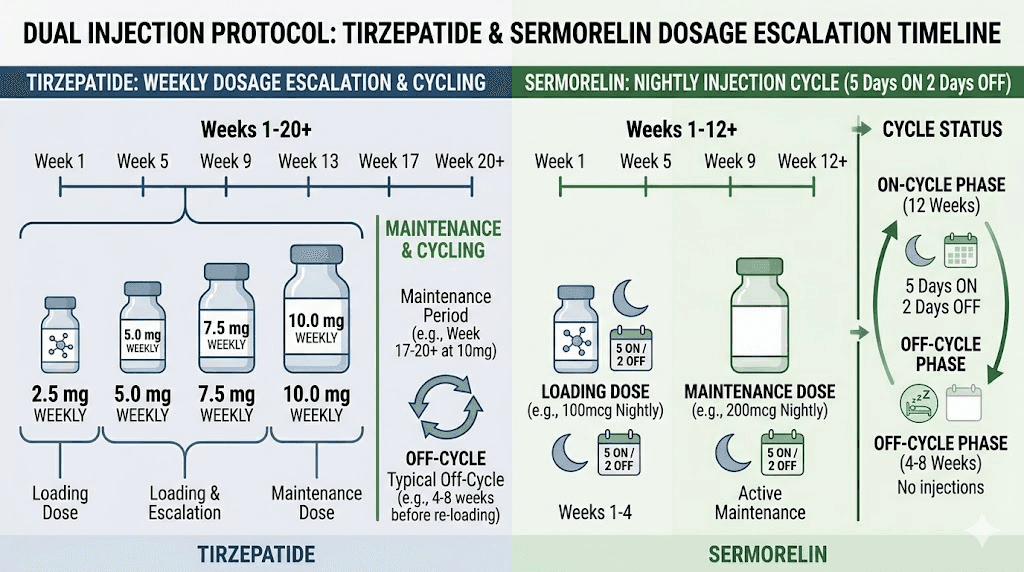
Most protocols run in cycles. Eight to twelve weeks of daily use followed by four weeks off. This cycling approach prevents receptor desensitization and maintains long-term pituitary responsiveness. Some researchers use a 5-days-on, 2-days-off pattern within each active cycle for similar reasons.
Women generally require lower doses than men, typically starting at 100 to 200 mcg daily. Age also factors in. Adults over 50 may benefit from starting at the lower end and adjusting based on blood work results, particularly IGF-1 levels.
What tirzepatide is and how it works
Tirzepatide is a dual GIP/GLP-1 receptor agonist. That dual action is what separates it from semaglutide and other pure GLP-1 medications. By activating both the glucose-dependent insulinotropic polypeptide receptor and the glucagon-like peptide-1 receptor, tirzepatide triggers overlapping but distinct metabolic pathways that produce more pronounced effects on weight loss, glucose control, and appetite suppression than either pathway alone.
The numbers tell the story. In clinical trials, tirzepatide produced average weight loss of 15 to 22.5% of body weight at the highest doses. That translates to 30, 40, even 50 or more pounds for many people. These results exceeded anything achieved by pure GLP-1 agonists in head-to-head comparisons. The before and after results speak volumes.
But raw weight loss tells only part of the story.
How tirzepatide produces weight loss
Tirzepatide works through several mechanisms simultaneously. First, it slows gastric emptying. Food stays in the stomach longer, which creates a sustained feeling of fullness after smaller meals. People on tirzepatide often report that their relationship with food changes fundamentally, that the constant background noise of hunger simply quiets down.
Second, it acts on appetite centers in the brain. The GLP-1 receptor activation in the hypothalamus reduces food-seeking behavior, decreases cravings, and changes food preferences. Many users report losing interest in high-calorie, highly processed foods without consciously trying. If you want to understand whether tirzepatide burns fat or just suppresses appetite, the answer is both, through different mechanisms.
Third, tirzepatide improves insulin sensitivity and glucose metabolism. The GIP component enhances the insulin response to meals while also promoting fat oxidation, particularly in adipose tissue. This creates metabolic conditions favorable to fat loss rather than muscle catabolism. Understanding the metabolic effects of tirzepatide helps explain why it works so effectively.
Fourth, participants on tirzepatide naturally reduce caloric intake by 30 to 40% without consciously trying. This spontaneous caloric deficit drives the majority of the weight loss. The problem is that caloric deficits do not discriminate between fat and muscle. The body breaks down both for energy, especially when protein intake is insufficient.
Tirzepatide dosage protocol
Tirzepatide follows a standardized escalation protocol designed to minimize gastrointestinal side effects. The starting dose is 2.5 mg once weekly for four weeks. Then 5 mg weekly for four weeks. Then gradual escalation in 2.5 mg increments every four weeks up to a maximum of 15 mg weekly, depending on tolerance and response.
The tirzepatide dose chart provides detailed breakdowns for each escalation phase. For those using compounded versions, the compounded tirzepatide starting dose guide covers the specifics of unit-based dosing from vials. Injection technique matters too, and our guide on how to inject tirzepatide in the stomach walks through proper subcutaneous administration.
The muscle preservation problem with GLP-1 medications
This is the elephant in the room. And it is a big one.
The SEMALEAN study, published in Diabetes, Obesity and Metabolism in 2026, tracked 106 patients with obesity taking semaglutide 2.4 mg for 12 months. Weight loss was significant, averaging 10% at 7 months and 13% at 12 months. Total fat mass decreased by 14% at 7 months and 18% at 12 months. But lean mass also declined, dropping by approximately 3 kg at 7 months before stabilizing.
Three kilograms of lean mass. That is roughly 6.6 pounds of muscle, connective tissue, and other metabolically active tissue gone. Not from a starvation diet. Not from months of neglect. From a medication designed to help people get healthier. The irony is hard to ignore.
And the SEMALEAN study used semaglutide, not tirzepatide. Tirzepatide produces even greater weight loss, averaging 15 to 22.5% of body weight at higher doses compared to semaglutide averages of 10 to 15%. More weight loss means more total lean mass at risk, making the muscle preservation question even more urgent for tirzepatide users tracking their weight loss timeline.
A study presented at ENDO 2025 by the Endocrine Society found that women and older adults on semaglutide face even higher risk of muscle loss. Being older, being female, or eating less protein all correlated with greater lean mass decline. Those consuming less than 1.0 grams of protein per kilogram of body weight daily lost an average of 39% lean mass relative to total weight loss. Those consuming 1.6 grams per kilogram or higher lost only 22% lean mass.
Even 22% is substantial. If someone loses 50 pounds total, 22% lean mass loss means 11 pounds of muscle gone alongside 39 pounds of fat. That muscle loss slows metabolism, weakens the body, reduces functional capacity, and makes weight regain more likely once the medication stops.
This is exactly why the combination with sermorelin has gained traction. Researchers are looking for ways to keep the fat loss while protecting the muscle. Adequate protein intake helps. Resistance training helps. But growth hormone support through sermorelin adds another layer of protection that diet and exercise alone may not provide, particularly for older adults or those with limited exercise capacity.
Why protein and exercise are not always enough
The standard advice for GLP-1 users goes like this: eat more protein, lift weights, problem solved. And for many people, that advice works reasonably well. A 2024 study published in The Lancet found that participants on semaglutide who combined adequate protein intake at 1.6 grams per kilogram with twice-weekly strength training preserved 95% of their lean mass during a 6-month weight loss period.
But consider the real world. Many people on tirzepatide struggle to eat enough food, period. Appetite suppression is the whole point of the medication, and that suppression makes hitting protein targets genuinely difficult. Nausea, which affects a significant percentage of tirzepatide users especially during dose escalation, makes protein-rich foods particularly unappealing. Meat, eggs, dairy, the foods highest in protein, are often the first things people cannot stomach.
Then there is exercise. Older adults with joint issues, mobility limitations, or simply decades of sedentary living cannot always perform the kind of progressive resistance training needed to preserve muscle. People recovering from injuries, dealing with chronic fatigue from the medication itself, or managing other health conditions face real barriers to consistent strength training. Our guide on GLP-1 fatigue explores why energy levels drop for many users, making exercise even harder.
Sermorelin does not replace protein intake or exercise. Nothing does. But it provides growth hormone support that helps the body prioritize muscle retention even when nutrition and training are not perfect.
How sermorelin and tirzepatide work together
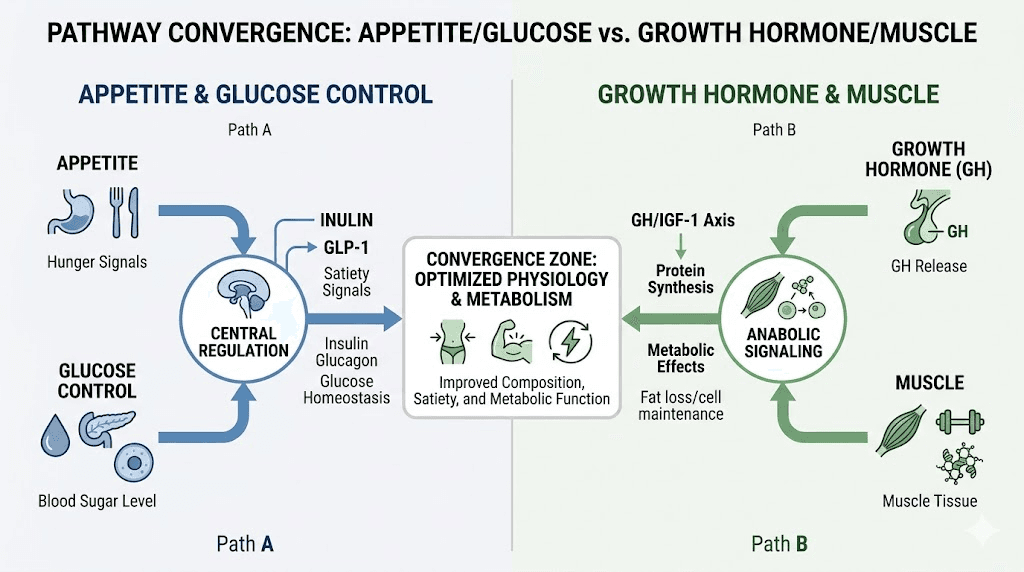
The synergy between these two compounds comes from their completely different mechanisms of action. They do not compete. They do not interfere. They complement each other by addressing body composition from opposite angles.
Tirzepatide creates the caloric deficit. It suppresses appetite, improves insulin sensitivity, enhances glucose metabolism, and drives fat loss through reduced food intake and improved metabolic efficiency. It is the engine of weight loss in this combination.
Sermorelin protects the muscle. By stimulating natural growth hormone production, it enhances protein synthesis, promotes lipolysis over proteolysis, improves recovery capacity, and supports the anabolic processes that keep lean tissue intact during periods of caloric restriction.
Together, they create conditions for what body composition researchers call preferential fat loss, where a higher percentage of weight lost comes from fat rather than lean tissue.
The metabolic advantage
Growth hormone and GLP-1 activation interact in interesting ways metabolically. Growth hormone is inherently lipolytic, meaning it promotes the breakdown of stored fat for energy. When combined with the caloric deficit created by tirzepatide, this lipolytic effect means the body has greater access to fat stores as fuel, potentially reducing the need to break down muscle for energy.
Growth hormone also increases basal metabolic rate. This partially offsets the metabolic adaptation, the slowdown in metabolism, that naturally occurs during weight loss. When you lose weight, your body becomes more efficient and burns fewer calories at rest. This adaptation is one of the primary drivers of weight regain. By supporting metabolic rate through growth hormone stimulation, sermorelin may help maintain a higher calorie burn throughout the weight loss process.
The average weight loss per month on GLP-1 medications varies significantly between individuals, but the quality of that weight loss, the ratio of fat to muscle, may matter more than the speed.
Recovery and sleep benefits
There is another angle that gets less attention. Sermorelin improves sleep quality, and sleep quality directly impacts muscle preservation, metabolic health, and weight loss outcomes.
Growth hormone release naturally peaks during deep sleep. Sermorelin amplifies this peak when administered before bedtime. Better growth hormone pulsatility during sleep means better recovery, better protein synthesis, better tissue repair. For someone on tirzepatide who is training with resistance exercise to preserve muscle, improved recovery between sessions allows for more productive training and better adaptation.
Tirzepatide insomnia is a real issue for some users. Ironically, adding sermorelin to the protocol may help address this side effect while simultaneously supporting muscle preservation. Better sleep, better recovery, better body composition outcomes. The benefits compound.
Sermorelin and tirzepatide dosage protocol
Establishing the right protocol for combining these compounds requires understanding each one individually before layering them together. Neither medication should be started at the same time. Staggering the introduction allows you to identify how your body responds to each compound independently and makes it easier to troubleshoot if side effects emerge.
Phase 1: establish tirzepatide (weeks 1 through 8)
Most protocols begin with tirzepatide alone. Start at 2.5 mg weekly as recommended by the standard tirzepatide compound dosage chart. Spend four weeks at this starting dose to assess tolerance. Common initial side effects include nausea, decreased appetite, occasional constipation, and bloating.
At week 5, escalate to 5 mg weekly if the 2.5 mg dose was well tolerated. Continue at 5 mg for another four weeks. By week 8, you should have a clear understanding of how tirzepatide affects your appetite, energy, digestion, and overall wellbeing.
During this phase, focus on establishing nutritional habits that support the combination protocol. Aim for adequate protein intake of at least 1.2 grams per kilogram of body weight daily. This can be challenging with reduced appetite, so high-protein breakfast strategies and GLP-1 friendly recipes become essential tools.
Phase 2: introduce sermorelin (weeks 9 through 12)
Once tirzepatide is established and well tolerated, introduce sermorelin at a conservative starting dose. Begin with 100 to 200 mcg subcutaneously once daily, administered 30 to 60 minutes before bedtime. The injection should be given on an empty stomach, meaning no food for at least 2 hours prior.
Why bedtime? Growth hormone release naturally peaks during the first few hours of deep sleep. Sermorelin administered before bed amplifies this natural pulse rather than creating an artificial one. Eating before the injection blunts the growth hormone response because elevated blood sugar and insulin suppress GH release. Fasting for 2 or more hours before the injection optimizes the response.
At this dose, side effects are typically minimal. Mild facial flushing lasting a few minutes after injection is the most common. Some people report brief headaches or slight dizziness. Injection site reactions, including redness or mild soreness, occur in roughly 1 in 6 users but are generally transient.
Phase 3: optimize (weeks 13 and beyond)
Once both compounds are established, optimization begins. Tirzepatide dosage continues to escalate per standard protocol, moving from 5 mg to 7.5 mg, then potentially to 10 mg or higher based on weight loss progress and tolerance. The tirzepatide dosing guide in units provides detailed conversion charts for those using compounded vials.
Sermorelin dosage can increase to the standard 200 to 300 mcg daily range once the lower dose is well tolerated. Some protocols push to 400 to 500 mcg for men, though this should be guided by IGF-1 blood work rather than arbitrary escalation.
The cycling protocol for sermorelin remains important even when combined with tirzepatide. Run sermorelin for 8 to 12 weeks, then take 4 weeks off. During the off period, continue tirzepatide as normal. The sermorelin break prevents receptor downregulation and maintains pituitary responsiveness for subsequent cycles.
Complete dosing summary table
Phase | Weeks | Tirzepatide | Sermorelin | Notes |
|---|---|---|---|---|
Phase 1 | 1-4 | 2.5 mg weekly | None | Establish GLP-1 tolerance |
Phase 1 | 5-8 | 5 mg weekly | None | First dose escalation |
Phase 2 | 9-12 | 5-7.5 mg weekly | 100-200 mcg nightly | Introduce sermorelin |
Phase 3 | 13-20 | 7.5-10 mg weekly | 200-300 mcg nightly | Full optimization |
Sermorelin break | 21-24 | 10-15 mg weekly | Off cycle | 4-week sermorelin break |
Phase 3 restart | 25+ | Maintenance dose | 200-300 mcg nightly | Resume sermorelin cycle |
Timing and injection schedule
Getting the timing right with two injectable compounds requires planning. But it is simpler than it sounds once you understand the logic behind each injection window.
Tirzepatide timing
Tirzepatide is a once-weekly injection. Pick any day of the week that works for your schedule and stick with it. Many users prefer the same day each week for consistency. The best time to take your tirzepatide shot depends on personal preference and side effect patterns. Some users inject in the morning, others at night. If nausea is an issue, evening injection allows you to sleep through the worst of it.
The injection site should rotate between the abdomen, thigh, and upper arm. Never inject in the same exact spot twice in a row. Our tirzepatide injection guide covers proper technique in detail.
Sermorelin timing
Sermorelin is a daily injection, administered every night before bed. The ideal window is 30 to 60 minutes before you plan to fall asleep, on an empty stomach. No food for at least 2 hours prior. No carbohydrates or sugary drinks within that window. Even a small snack can blunt the growth hormone response by elevating insulin.
The stomach is the most common injection site for sermorelin. Pinch a fold of skin, insert the needle at a 45-degree angle, inject slowly, and release. Rotate sites within the abdominal area to prevent tissue irritation.
Can you inject both on the same day?
Yes. On the day you take your weekly tirzepatide injection, you still take your nightly sermorelin injection as usual. They work through completely different receptor systems and do not interact pharmacologically at the injection level. Simply use different injection sites, for example, tirzepatide in the thigh in the morning and sermorelin in the abdomen at bedtime.
There is no need to separate the injections by a specific number of hours unless your healthcare provider instructs otherwise. The only timing constraint is sermorelin before bed on an empty stomach. Tirzepatide can be injected at any time of day.
What about injection days off?
If you follow the 5-days-on, 2-days-off cycling approach for sermorelin, choose your two off days strategically. Some researchers prefer weekends off for simplicity. Others prefer spacing the off days throughout the week, for example, Wednesday and Sunday. The key is consistency. Pick a pattern and maintain it.
Tirzepatide does not cycle. It is taken every week without breaks unless you are discontinuing treatment or weaning off under medical guidance.
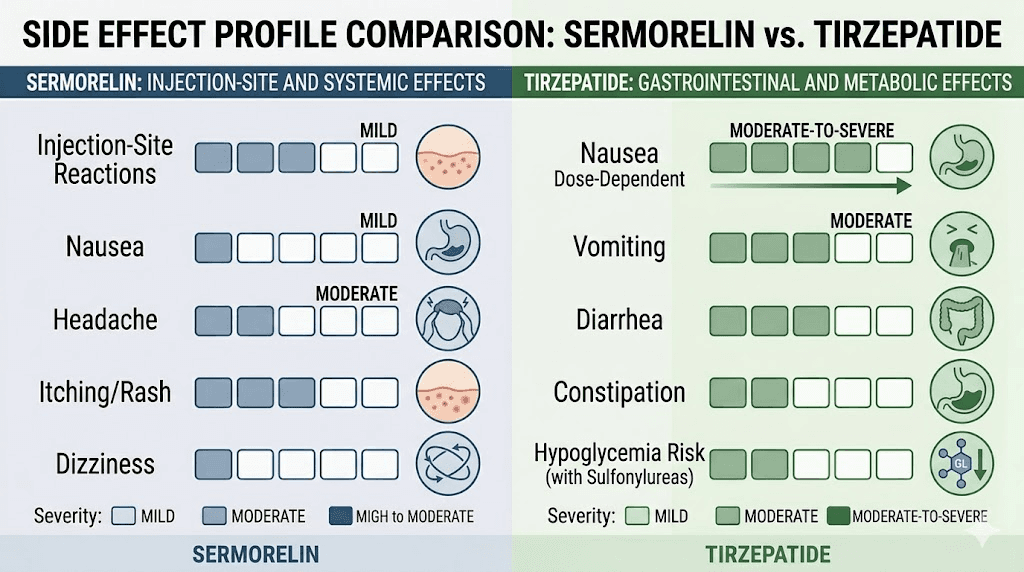
Side effects of combining sermorelin and tirzepatide
Understanding the side effect profile of each compound individually helps distinguish what might be causing any given symptom when running both together. This matters for troubleshooting.
Side effects from tirzepatide
The most common tirzepatide side effects are gastrointestinal. Nausea tops the list, affecting 20 to 30% of users, especially during the first few weeks and after each dose escalation. Diarrhea, constipation, and bloating are also common. These typically improve as the body adjusts over 2 to 4 weeks at each dose level.
Other tirzepatide side effects include fatigue, headaches, dry mouth, feeling cold, injection site reactions, and changes in bowel habits. Less commonly, some users report anxiety, body aches, muscle pain, and joint pain.
Side effects from sermorelin
Sermorelin is generally well tolerated with a milder side effect profile than tirzepatide. The most common reaction is transient facial flushing, a brief warmth and redness in the face that occurs within minutes of injection and resolves within 10 to 15 minutes. This affects roughly 1 in 6 users and is harmless.
Injection site reactions, including mild pain, redness, and swelling at the injection spot, are the second most common issue. These are typically transient and improve with proper injection technique and site rotation.
Less common side effects include headaches, dizziness, nausea, and restlessness. Serious adverse reactions are rare but can include allergic reactions or significant swelling. If difficulty breathing or swallowing occurs after injection, seek immediate medical attention.
Potential interaction concerns
While no formal drug-drug interactions have been identified between sermorelin and tirzepatide, there is one important consideration. Growth hormone has anti-insulin effects. It can increase blood glucose levels and reduce insulin sensitivity. Tirzepatide works in part by improving insulin sensitivity and glucose control.
This creates a theoretical tension. Sermorelin, by stimulating growth hormone release, could partially counteract the glucose-lowering effects of tirzepatide. In practice, the doses of sermorelin used clinically produce modest growth hormone increases that are unlikely to significantly oppose tirzepatide. But for people with diabetes or prediabetes, blood glucose monitoring becomes especially important when combining these compounds.
Regular blood work, including fasting glucose, HbA1c, and insulin levels, helps ensure the combination is producing the intended metabolic effects without unintended glucose dysregulation. The importance of monitoring metabolic markers cannot be overstated when running combination protocols.
Who should consider this combination
Not everyone on tirzepatide needs sermorelin. But certain populations stand to benefit more than others from the combined approach.
Adults over 40 losing significant weight
Natural growth hormone production declines with age. By 40, most adults produce significantly less growth hormone than they did in their twenties. By 60, levels may be a fraction of youthful output. This age-related decline in growth hormone makes older adults more vulnerable to muscle loss during weight loss, which is exactly what the ENDO 2025 research confirmed.
For adults over 40 on tirzepatide who are losing 20 or more pounds, sermorelin provides growth hormone support that their bodies can no longer produce at youthful levels. This population represents the clearest case for the combination.
People struggling with protein intake
If tirzepatide side effects are making it difficult to eat enough protein, sermorelin provides a backup layer of muscle protection. It does not replace the need for protein, but it supports protein synthesis efficiency, meaning the protein you do manage to consume gets used more effectively for muscle preservation.
Strategies for increasing protein intake on GLP-1 medications include protein shakes, which are often better tolerated than solid protein foods when nausea is present. Supplements that pair well with tirzepatide can also help fill nutritional gaps.
People with limited exercise capacity
Resistance training is the gold standard for muscle preservation during weight loss. But not everyone can do it. Joint pain, mobility issues, chronic conditions, post-surgical restrictions, and simple time constraints all create real barriers. For people who cannot perform adequate resistance training, sermorelin provides an alternative pathway to support muscle retention.
This does not mean you should skip exercise if you can do it. The combination of tirzepatide plus sermorelin plus resistance training plus adequate protein produces the best possible body composition outcomes. But for those who can only manage two or three of those four elements, sermorelin helps compensate for the missing piece.
People prioritizing body composition over scale weight
Some people do not just want to lose weight. They want to lose fat specifically, while maintaining or even improving muscle mass, strength, and physical function. These are different goals that require different strategies.
If you care about how you look and function after weight loss, not just what the scale says, the sermorelin and tirzepatide combination deserves consideration. The tirzepatide results are impressive on the scale, but the mirror and the gym tell a more nuanced story when lean mass preservation is part of the equation.
Who should avoid this combination
Certain conditions and situations make this combination inappropriate. Understanding contraindications protects against unnecessary risk.
Active cancer or history of certain cancers
Growth hormone promotes cell growth and proliferation. This is a double-edged sword. While it supports muscle, bone, and tissue health in healthy individuals, it can theoretically promote the growth of existing tumors. Anyone with active cancer, a recent history of cancer (particularly hormone-sensitive cancers), or a strong family history of growth hormone-dependent malignancies should avoid sermorelin.
Tirzepatide carries its own precaution regarding thyroid C-cell tumors based on animal studies. The combination amplifies the theoretical concern, and anyone with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 should avoid both compounds.
Uncontrolled diabetes
The opposing effects on glucose metabolism, tirzepatide lowering blood sugar and sermorelin potentially raising it through growth hormone, make this combination tricky for people with poorly controlled diabetes. Blood glucose swings become harder to predict and manage. Only individuals with well-controlled glucose levels under close medical supervision should consider the combination.
Pregnant or breastfeeding women
Neither sermorelin nor tirzepatide has established safety data in pregnancy. Tirzepatide and breastfeeding is a topic that warrants caution, and adding sermorelin to the picture introduces additional unknowns. Women who are pregnant, planning to become pregnant, or breastfeeding should avoid this combination entirely.
People under 25
Growth plates may not be fully closed in individuals under 25. Stimulating growth hormone production in this population could have unintended effects on bone growth. Additionally, natural growth hormone levels are typically adequate in younger adults, making sermorelin unnecessary for most people in this age group.
Monitoring and blood work
Running two compounds simultaneously demands more rigorous monitoring than either one alone. Blood work is not optional with this combination. It is essential for safety and optimization.
Baseline blood work (before starting)
Before beginning either compound, establish baseline values for the following markers. Complete metabolic panel including fasting glucose, HbA1c, liver enzymes, and kidney function. Lipid panel. IGF-1 levels, which serve as the primary indicator of growth hormone status. Thyroid function, including TSH, free T3, and free T4. Complete blood count. Fasting insulin levels.
These baselines allow you to track changes over time and identify any concerning trends early. The role of blood work in peptide protocols is critical and should not be skipped.
Follow-up blood work schedule
Recheck key markers at specific intervals throughout the protocol.
At 4 weeks after starting tirzepatide: fasting glucose, metabolic panel. This confirms the GLP-1 is producing expected metabolic improvements without unexpected liver or kidney stress.
At 4 weeks after introducing sermorelin: IGF-1 levels, fasting glucose, fasting insulin. The IGF-1 check confirms that sermorelin is effectively stimulating growth hormone production. Values should increase from baseline but remain within the upper normal range. Fasting glucose ensures the growth hormone effect is not significantly opposing tirzepatide.
Every 8 to 12 weeks thereafter: full panel including IGF-1, metabolic markers, lipids, and thyroid function. This ongoing monitoring catches trends before they become problems.
What the numbers should look like
Marker | Target range | Red flag |
|---|---|---|
IGF-1 | Upper third of age-adjusted normal range | Above normal range consistently |
Fasting glucose | 70-100 mg/dL | Rising trend above 110 mg/dL |
HbA1c | Below 5.7% | Rising despite tirzepatide |
Fasting insulin | Below 10 uIU/mL | Rising trend above 15 uIU/mL |
Liver enzymes (ALT/AST) | Within normal limits | More than 2x upper limit |
If IGF-1 levels climb above the normal range, reduce sermorelin dosage or extend the off-cycle period. If fasting glucose or HbA1c trends upward despite tirzepatide, the growth hormone effect may be counterproductive, and sermorelin dosage reduction or discontinuation should be considered.
Comparing sermorelin plus tirzepatide to alternatives
Sermorelin is not the only peptide people consider combining with GLP-1 medications. Understanding how this stack compares to alternatives helps inform the decision.
Sermorelin plus tirzepatide versus tirzepatide alone
Tirzepatide alone produces excellent weight loss, averaging 15 to 22.5% of body weight in clinical trials. The tirzepatide weight loss timeline shows steady progress over months. The trade-off is lean mass loss, which ranges from 20 to 40% of total weight lost depending on protein intake and exercise habits.
Adding sermorelin aims to shift that ratio, preserving more lean mass while maintaining or even enhancing fat loss. The trade-offs are additional cost, a second daily injection, the need for cycling, and the requirement for more frequent blood work.
For someone who hits their protein targets consistently and strength trains regularly, the marginal benefit of adding sermorelin may be small. For someone who cannot do those things effectively, the benefit is likely more substantial.
Sermorelin plus tirzepatide versus ipamorelin plus tirzepatide
Ipamorelin is a growth hormone secretagogue rather than a GHRH analog. It stimulates growth hormone release through a different receptor, the ghrelin receptor, and produces a slightly different growth hormone release pattern. Some researchers prefer ipamorelin because it is more selective for growth hormone release and has less impact on cortisol and prolactin compared to other secretagogues.
In practice, sermorelin and ipamorelin produce similar growth hormone increases and similar body composition benefits when combined with tirzepatide. The choice often comes down to availability, cost, and individual response. Some protocols stack both sermorelin and ipamorelin together for a synergistic growth hormone response, though this adds complexity and cost.
Sermorelin plus tirzepatide versus semaglutide plus sermorelin
The sermorelin versus semaglutide comparison addresses a common question, but the real question for many is whether to pair sermorelin with tirzepatide or semaglutide.
Tirzepatide generally produces greater weight loss than semaglutide due to its dual GIP/GLP-1 mechanism. The side effect profiles differ between the two GLP-1 medications. Semaglutide tends to cause more nausea while tirzepatide produces slightly more gastrointestinal side effects overall but often less severe nausea.
For pure weight loss, tirzepatide plus sermorelin likely produces better results than semaglutide plus sermorelin due to tirzepatide producing greater fat loss. But individual response varies enormously. Some people respond better to semaglutide. Others respond better to tirzepatide. The conversion chart between the two helps when switching between them.
Sermorelin plus tirzepatide versus creatine plus tirzepatide
Creatine and tirzepatide is a simpler, less expensive combination that also supports lean mass. Creatine is the most well-studied supplement for muscle performance and retention. It is cheap, safe, orally administered, and has decades of research behind it.
The mechanisms are different from sermorelin. Creatine enhances ATP regeneration in muscle cells, improving strength performance and supporting muscle volume through intracellular water retention. It does not directly stimulate growth hormone. But for people who exercise regularly, creatine plus tirzepatide may provide meaningful muscle preservation at a fraction of the cost of adding sermorelin.
The strongest approach would combine all three: tirzepatide for fat loss, sermorelin for growth hormone support, and creatine for direct muscle performance enhancement. But cost and complexity increase with each addition.
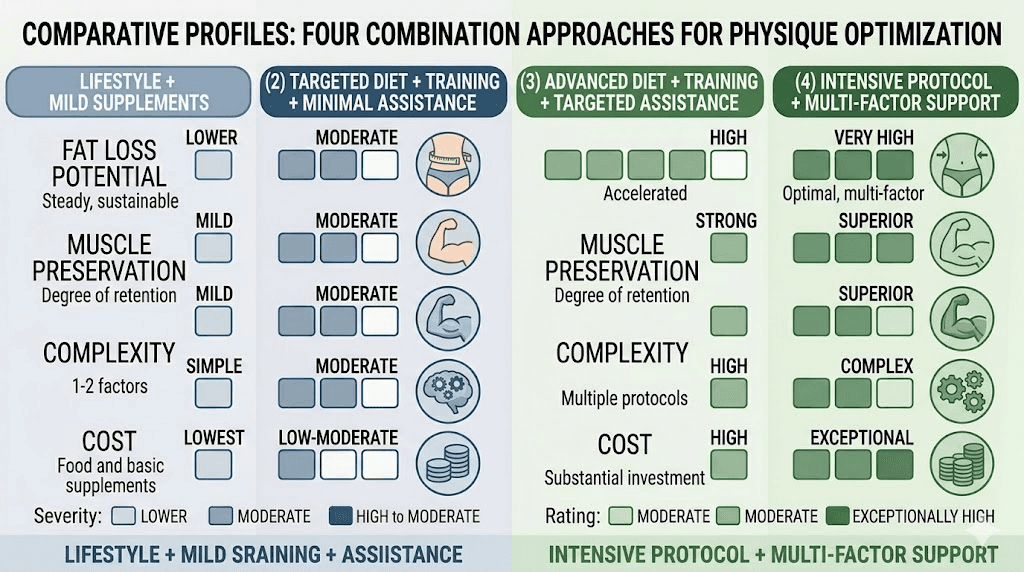
Combination | Fat loss | Muscle preservation | Complexity | Cost |
|---|---|---|---|---|
Tirzepatide alone | Excellent | Moderate (with protein/exercise) | Low | $ |
Tirzepatide + creatine | Excellent | Good | Low | $ |
Tirzepatide + sermorelin | Excellent | Very good | Moderate | $$ |
Tirzepatide + sermorelin + creatine | Excellent | Best | Moderate | $$ |
Expected results and timeline
Setting realistic expectations prevents frustration and supports adherence to the protocol. Here is what the research and clinical experience suggest for the combination approach.
Weeks 1 through 4 (tirzepatide only)
Weight loss typically begins within the first 1 to 2 weeks of tirzepatide, primarily from reduced caloric intake and fluid shifts. Expect 2 to 5 pounds during this initial phase at the 2.5 mg starting dose. The first month on tirzepatide sets the foundation. Appetite suppression becomes noticeable within days for most people.
No sermorelin effects during this phase since it has not been introduced yet.
Weeks 5 through 8 (tirzepatide dose escalation)
At 5 mg, weight loss accelerates. The speed of tirzepatide results varies, but most people see 1 to 3 pounds per week at this dose. Appetite suppression deepens. Gastrointestinal side effects may temporarily increase with the dose bump.
Still no sermorelin effects. But this is when you should optimize protein intake and establish an exercise routine if possible, as preparation for the combined phase.
Weeks 9 through 16 (combination phase)
When sermorelin is introduced, the effects are not immediately dramatic. Growth hormone levels increase gradually over 2 to 4 weeks. Sleep quality often improves within the first 1 to 2 weeks. Energy and recovery may improve around weeks 3 to 4 of sermorelin use.
The real benefit of sermorelin shows up in body composition data over months, not weeks. Weight loss continues from tirzepatide, but the ratio of fat to muscle in that weight loss starts to shift. The scale may not show a dramatic difference because you are losing less muscle while losing more fat, and fat is less dense than muscle. But body measurements, how clothes fit, strength in the gym, and body composition scans (DEXA) will tell the real story.
Months 3 through 6
This is where the combination shines. Cumulative weight loss on tirzepatide at optimized doses often reaches 10 to 15% of starting body weight by month 6. With sermorelin supporting muscle retention, a higher percentage of that loss should be fat tissue.
Users of the combination often report looking "more toned" or "more muscular" at the same weight compared to people who lost weight on tirzepatide alone. This is the body composition advantage in action: less muscle loss means a leaner, more defined appearance even at a higher scale weight.
If you want to track progress effectively, do not rely solely on the scale. Use waist circumference, progress photos, strength benchmarks, and ideally DEXA scans every 3 to 6 months for accurate body composition tracking. The monitoring tools for home use can help between professional assessments.
Beyond 6 months
Long-term results depend on adherence to the complete protocol: tirzepatide at appropriate doses, sermorelin cycling, adequate protein, regular exercise, and consistent monitoring. The maintenance strategy after tirzepatide becomes important as you approach goal weight.
Some people transition from active weight loss doses to GLP-1 maintenance doses while continuing sermorelin cycles for ongoing body composition support. Others eventually discontinue both compounds and rely on the habits and muscle mass they have built to maintain results.
Common mistakes with the sermorelin and tirzepatide combination
Knowing what not to do is just as important as knowing the protocol. These are the errors that derail results most often.
Starting both compounds simultaneously
This is the most common mistake, and it creates immediate problems. When side effects appear, and they will, you have no way of knowing which compound is causing them. Nausea could be from tirzepatide or from sermorelin. Headaches could be either. Injection site reactions could be either. Without knowing the source, you cannot adjust the right variable.
Always stagger by at least 4 to 8 weeks. Establish tirzepatide first. Let side effects stabilize. Then introduce sermorelin. This sequential approach gives you clear cause-and-effect information for troubleshooting.
Eating before sermorelin injection
Sermorelin must be taken on an empty stomach. Food, particularly carbohydrates, elevates blood sugar and insulin. Elevated insulin suppresses growth hormone release. If you eat a meal 30 minutes before your sermorelin injection, you are essentially wasting the dose. The growth hormone response will be blunted significantly, sometimes by 50% or more.
The two-hour fasting window before injection is not a suggestion. It is a requirement for the compound to work as intended. Some researchers extend this to three hours for optimal results. If you find yourself hungry close to bedtime, eat your last meal earlier in the evening to ensure the fasting window is met.
Skipping the sermorelin off cycle
Continuous sermorelin use without cycling leads to receptor desensitization. The pituitary GHRH receptors become less responsive over time, requiring higher doses to achieve the same growth hormone release. Eventually, the response diminishes regardless of dose.
The 4-week off period every 8 to 12 weeks allows receptors to resensitize. When you restart, the pituitary responds robustly again. Skipping cycles might seem like you are getting more benefit by not taking breaks, but the opposite is true. Cycling maintains long-term effectiveness.
Neglecting protein intake because sermorelin is handling it
Sermorelin supports muscle preservation. It does not create muscle from nothing. Growth hormone enhances protein synthesis, but protein synthesis requires amino acids from dietary protein. Without adequate protein intake, sermorelin has nothing to work with. You cannot out-supplement a poor diet, even with growth hormone support.
Think of it this way. Sermorelin is the construction crew. Protein is the building material. You need both. Hiring more workers when there are no materials on site does not build anything. The high-protein food lists for GLP-1 users and foods to avoid on GLP-1 medications help structure a nutrition plan that supports the combination protocol.
Ignoring blood work
Running two compounds without monitoring is like driving without a dashboard. You might be fine. You might not. Blood work reveals whether sermorelin is effectively stimulating growth hormone production (via IGF-1 levels), whether the growth hormone effect is disrupting glucose control, and whether liver and kidney function remain normal under the combined metabolic load.
The minimum monitoring schedule is baseline blood work before starting, repeat at 4 weeks after each compound introduction, and then every 8 to 12 weeks during ongoing use. This is not optional. It is the difference between informed protocol management and blind experimentation.
Expecting immediate body composition changes
Growth hormone works slowly. Unlike tirzepatide, which produces noticeable appetite changes within days and measurable weight loss within weeks, the body composition benefits of sermorelin accumulate over months. People who add sermorelin expecting to see dramatic muscle gains in 2 weeks will be disappointed and may abandon the protocol prematurely.
The timeline is realistic. Sleep improvements in weeks 1 to 2. Energy and recovery improvements in weeks 3 to 4. Measurable body composition differences over 2 to 3 months. Significant cumulative benefits over 4 to 6 months. Patience is required.
Practical tips for the sermorelin and tirzepatide combination
Beyond the protocol itself, practical logistics make a real difference in adherence and results.
Storage matters
Both compounds require refrigeration after reconstitution. Sermorelin should be stored at 2 to 8 degrees Celsius and used within 28 days of reconstitution. Tirzepatide follows similar storage requirements, which our guide on tirzepatide refrigeration covers in detail. The shelf life of reconstituted tirzepatide provides specific timelines.
Keep a dedicated section of your refrigerator for peptide storage. Away from the freezer section, which can accidentally freeze and damage the compounds. Away from the door, where temperature fluctuates most with opening and closing. The back of a shelf in the main compartment is ideal.
For travel, a GLP-1 travel case with cold packs keeps both compounds at proper temperature during transit.
Injection supplies
Running two injectables means going through more supplies. Insulin syringes with 29 or 31 gauge needles work for both compounds. The GLP-1 syringe guide covers needle selection and proper use. Stock enough alcohol swabs, syringes, and needles for your full protocol cycle to avoid running out.
Consider tracking your injections with an app or simple log sheet. With two compounds on different schedules, one weekly and one daily, tracking prevents missed doses and helps identify patterns in side effects relative to injection timing.
Nutrition strategy
Protein is the single most important nutritional factor for this combination. Aim for at least 1.2 grams per kilogram of body weight daily, with 1.6 grams per kilogram being the gold standard for muscle preservation during weight loss.
Practical protein strategies for tirzepatide users include starting every meal with protein before anything else. Using protein shakes when solid food is not appealing. Choosing easily digestible protein sources like Greek yogurt, eggs, fish, and cottage cheese. Spreading protein across 3 to 4 meals with 25 to 40 grams per meal rather than trying to get it all in one sitting.
The tirzepatide diet plan and what to eat on tirzepatide guides provide comprehensive meal planning strategies. For specific recipes designed around GLP-1 users, the GLP-1 dinner ideas and breakfast ideas offer practical inspiration.
Fiber supplementation supports digestive health, which often gets disrupted on GLP-1 medications. Other supplements worth considering include a quality multivitamin, magnesium, and omega-3 fatty acids.
Exercise recommendations
The ideal exercise protocol alongside sermorelin and tirzepatide prioritizes resistance training. Three to four sessions per week targeting all major muscle groups provides the stimulus needed to signal the body that muscle should be preserved. You do not need to train like a bodybuilder. Basic compound movements, squats, deadlifts, rows, presses, and pulls, performed with moderate weights and progressive overload, are sufficient.
Cardiovascular exercise complements resistance training but should not replace it. Walking 20 to 30 minutes daily is an excellent starting point. More intense cardio can be added as fitness improves, but never at the expense of resistance training frequency.
Creatine supplementation alongside GLP-1 medications further supports exercise performance and muscle retention. Five grams daily of creatine monohydrate is the standard, well-researched dose.
Reconstitution
If using lyophilized sermorelin or compounded tirzepatide from vials, proper reconstitution is essential. The tirzepatide reconstitution guide and peptide reconstitution calculator ensure accurate mixing. The peptide dosage calculator helps convert between milligrams and units for syringe measurement.
General reconstitution principles apply to both. Use bacteriostatic water. Direct the water stream along the vial wall, not directly onto the powder. Swirl gently, never shake. Label every vial with the reconstitution date and concentration. Discard after 28 days.
Sermorelin and tirzepatide for specific populations
Different groups may approach this combination differently based on their specific needs and circumstances.
Women on the combination
Women face unique considerations with this stack. The ENDO 2025 research showed women are at higher risk for muscle loss on GLP-1 medications than men, making the case for sermorelin stronger. However, women also tend to be more sensitive to growth hormone stimulation, which is why starting doses for sermorelin are typically lower, 100 to 200 mcg versus 200 to 300 mcg for men.
Tirzepatide and menstrual changes are a documented phenomenon, with some women reporting irregular periods during significant weight loss. Sermorelin does not directly affect menstrual cycles, but the overall hormonal changes from rapid body composition shifts can compound existing disruptions. The relationship between GLP-1 medications and estrogen is an evolving area of research.
Women considering or taking HRT alongside GLP-1 medications should discuss the addition of sermorelin with their prescribing physician, as the hormonal picture becomes more complex with multiple compounds.
Men on the combination
Men generally tolerate higher sermorelin doses and may see more pronounced muscle preservation effects, partly because men typically have more muscle mass to preserve and higher baseline growth hormone responsiveness. The interaction between growth hormone stimulation and tirzepatide effects on testosterone is worth monitoring, as testosterone levels can fluctuate during significant weight loss.
Men on TRT (testosterone replacement therapy) who add tirzepatide and sermorelin are running a triple-hormone protocol that requires careful monitoring. The anabolic support from testosterone plus growth hormone stimulation from sermorelin creates a strongly anabolic environment even during the catabolic state of caloric restriction from tirzepatide.
People with autoimmune conditions
GLP-1 medications show emerging evidence for anti-inflammatory effects, and some researchers are exploring microdosing GLP-1 for autoimmune conditions. Growth hormone also has immunomodulatory properties. The combination of sermorelin and tirzepatide in people with autoimmune conditions is largely uncharted territory.
For those with Hashimoto thyroiditis, lipedema, or endometriosis, the theoretical benefits of reduced inflammation from tirzepatide combined with tissue repair support from sermorelin are appealing but unproven. Proceed with caution and close medical supervision.
What the research actually says (and does not say)
Transparency matters. And the transparency here is straightforward: there are no published clinical trials specifically studying the combination of sermorelin and tirzepatide.
The evidence supporting this combination is theoretical and extrapolated from separate bodies of research. We know sermorelin stimulates growth hormone release. We know growth hormone supports muscle preservation. We know tirzepatide causes weight loss that includes lean mass loss. The logical conclusion is that combining them should reduce lean mass loss during tirzepatide-driven weight loss.
That logic is sound. But it has not been validated by a controlled, randomized trial. The claims made by wellness clinics offering this combination often exceed what the evidence supports.
What we do have is individual-level clinical experience from prescribers who have used the combination in their patients. Many report positive results: better body composition outcomes, improved energy and recovery, less muscle loss on DEXA scans compared to patients on tirzepatide alone. But clinical observations without controlled comparisons carry inherent bias. Patients who can afford and choose to add sermorelin are typically more health-conscious overall, making it difficult to separate the effect of sermorelin from the effect of greater health awareness.
The SeekPeptides position on this is clear: the combination has a strong theoretical basis, appears to be safe when properly monitored, and has growing clinical support, but it remains an off-label, unvalidated protocol until properly studied. Anyone considering it should understand this limitation and make an informed decision.
Alternatives to sermorelin for muscle preservation on tirzepatide
If sermorelin is not accessible, affordable, or appropriate for your situation, several other strategies can support muscle preservation during GLP-1 mediated weight loss.
Protein optimization
The simplest and most evidence-based approach. Target 1.6 grams of protein per kilogram of body weight daily. Distribute across 3 to 4 meals. Start each meal with protein. Use shakes and supplements to fill gaps. Our protein guide for GLP-1 users provides specific strategies and food lists.
Resistance training
Three to four sessions weekly with progressive overload. Focus on compound movements. Even low-intensity resistance training preserves more muscle than no training. The Lancet study showed that 1.6 g/kg protein plus twice-weekly strength training preserved 95% of lean mass during semaglutide weight loss.
Creatine
Five grams daily. Cheap, safe, well-researched. Creatine and tirzepatide is a practical, accessible combination. No injections required. No cycling needed. No blood work specifically for creatine monitoring.
Other peptide combinations
Some researchers explore combining tirzepatide with other compounds for body composition optimization. AOD-9604, a fragment of human growth hormone, has been studied for fat loss properties. Tesofensine works through different neurotransmitter pathways. And other tirzepatide alternatives may produce similar weight loss with potentially different effects on body composition.
For researchers ready to commit to the most comprehensive approach, SeekPeptides provides detailed protocol builders, dosing calculators, and evidence-based guides that account for individual factors most resources ignore. SeekPeptides members access comprehensive stacking calculators, safety databases, and a community of experienced researchers who have navigated these exact protocol decisions.
How to tell if the combination is working
One of the trickiest aspects of the sermorelin and tirzepatide combination is measuring success. The scale alone is misleading. Someone losing fat while preserving muscle might weigh more than someone losing both fat and muscle at the same rate, yet have far better health outcomes and aesthetics.
Body composition metrics that matter
DEXA scans are the gold standard for tracking fat mass, lean mass, and bone density separately. If you can access a DEXA scan every 3 months, the data will clearly show whether sermorelin is preserving lean tissue. Look for the lean mass to total mass ratio to stay stable or improve over time, even as total weight decreases.
Waist circumference is a cheap, practical alternative. Losing inches from the waist while maintaining or gaining inches on the arms and legs suggests preferential fat loss with muscle preservation. Measure weekly, same time of day, same spot on the body.
Strength benchmarks provide functional evidence. If you can maintain or increase the weight you lift in the gym while losing body weight, your muscle is being preserved. This is one of the most encouraging signs that the combination is working. Track 3 to 5 key lifts and test them every 4 weeks.
Progress photos taken monthly under consistent lighting and angles show visual changes that numbers miss. The "look" of someone who preserved muscle while losing fat is distinctly different from someone who lost both. More definition. Better proportions. Less of the "deflated" appearance that sometimes accompanies rapid weight loss.
Blood markers that confirm growth hormone response
IGF-1 is the primary blood marker confirming sermorelin is working. Levels should increase from baseline within 4 to 6 weeks of starting sermorelin. The target is the upper third of the age-adjusted normal range. If IGF-1 has not increased meaningfully after 6 weeks of consistent use with proper timing (bedtime, empty stomach), the dose may need adjustment, or adherence to the fasting window may need improvement.
Body fat percentage, when measured consistently with the same method (DEXA, bioimpedance, or calipers), provides the clearest single number for combination protocol success. The goal is for body fat percentage to decrease faster than it would on tirzepatide alone, indicating that a greater share of weight loss is coming from fat tissue rather than lean tissue.
Subjective indicators
Beyond the numbers, several subjective experiences suggest the combination is producing beneficial effects. Improved sleep quality, particularly deeper sleep with fewer nighttime awakenings, often appears within the first two weeks of sermorelin. Faster recovery from workouts, measured by less soreness and better performance in subsequent sessions, typically emerges by week 3 to 4. Higher baseline energy throughout the day, better skin quality, and improved mood are commonly reported by weeks 4 to 8.
If you are experiencing significant energy changes on tirzepatide, the sleep and recovery improvements from sermorelin often help counterbalance the fatigue that some GLP-1 users experience, particularly during dose escalation phases. This alone makes the combination worthwhile for many users, independent of the body composition benefits.
Frequently asked questions
Can you take sermorelin and tirzepatide at the same time?
Yes. There are no known drug-drug interactions between sermorelin and tirzepatide because they work through completely different receptor systems. They can be taken on the same day, though they should be injected at different sites. Tirzepatide is given once weekly at any time of day, while sermorelin is given nightly before bed on an empty stomach.
How long does it take to see results from adding sermorelin to tirzepatide?
Sleep quality often improves within 1 to 2 weeks of starting sermorelin. Energy and recovery improvements typically appear around weeks 3 to 4. Body composition benefits, specifically better fat-to-muscle ratios in weight loss, become measurable over 2 to 3 months. Track progress with body measurements, strength benchmarks, and before and after documentation rather than relying solely on scale weight.
Does sermorelin make tirzepatide work better for weight loss?
Not directly. Sermorelin does not increase the rate of fat loss from tirzepatide. What it does is change the quality of the weight loss. By supporting muscle preservation through growth hormone stimulation, sermorelin ensures that a higher percentage of the weight you lose is fat rather than lean tissue. The scale might show similar numbers, but the body composition underneath is different.
Do I still need to exercise if I take both sermorelin and tirzepatide?
Yes. Neither compound replaces the need for physical activity, particularly resistance training. Exercise provides the stimulus that tells your body muscle tissue is being used and should be preserved. Sermorelin provides growth hormone support that enhances this process. The combination of exercise, proper nutrition, and peptide support produces the best outcomes.
Is the sermorelin and tirzepatide combination FDA approved?
No. Tirzepatide is FDA approved for type 2 diabetes (as Mounjaro) and weight management (as Zepbound). Sermorelin was previously FDA approved for diagnosis and treatment of growth hormone deficiency but is now primarily used off-label. The combination of these two compounds has not been studied in clinical trials and is not FDA approved as a combination therapy. Medical supervision is essential.
How much does the sermorelin and tirzepatide combination cost?
Costs vary widely depending on source, location, and whether brand-name or compounded versions are used. The peptide cost calculator can help estimate expenses based on dosage and frequency. Tirzepatide typically represents the larger expense. Sermorelin adds a moderate additional cost. Budget for regular blood work as well, which is essential for safe monitoring of the combination.
Can I take sermorelin with semaglutide instead of tirzepatide?
Yes. The sermorelin and semaglutide combination follows similar principles. The choice between semaglutide and tirzepatide depends on individual response, availability, and prescriber recommendation. Tirzepatide generally produces greater weight loss, but semaglutide is effective for many people and may be preferred for various reasons.
What happens if I stop sermorelin but continue tirzepatide?
Growth hormone levels return to baseline within days to weeks of stopping sermorelin. Any muscle preservation benefits diminish as growth hormone support ends. Continuing tirzepatide without sermorelin means lean mass loss risk returns to baseline levels for GLP-1 therapy. The off-cycle periods built into sermorelin protocols help your body maintain pituitary responsiveness for when you resume.
External resources
Endocrine Society - Protein and Muscle Loss on Semaglutide (ENDO 2025)
SEMALEAN Study - Impact of Semaglutide on Fat Mass and Lean Mass (PMC)
In case I do not see you, good afternoon, good evening, and good night. May your growth hormone stay pulsatile, your lean mass stay preserved, and your body composition stay optimized.