Mar 31, 2026

Semaglutide and liraglutide look identical on paper. Both are GLP-1 receptor agonists. Both come from the same pharmaceutical company. Both reduce blood sugar, curb appetite, and help people lose weight. In practice? Completely different outcomes. One requires a daily injection. The other, a single weekly shot. One produces roughly 6% body weight loss in clinical trials. The other nearly triples that number. And the molecular modifications that separate them, tiny changes at the amino acid level, create a gap in potency, convenience, and clinical results that surprises even seasoned researchers.
The confusion between these two peptides runs deep. Physicians switch patients from one to the other without fully explaining why. Online forums mix up brand names, dosing schedules, and side effect profiles. People starting their GLP-1 fat loss treatment journey often assume the two are interchangeable. They are not.
Understanding the real difference between semaglutide and liraglutide requires going beyond surface-level comparisons. It means examining pharmacokinetics, receptor binding affinity, clinical trial data, titration protocols, and real-world tolerability. This guide covers all of it, with the specific numbers, study references, and practical details that actually help you make an informed decision. Whether you are exploring how fast semaglutide works or wondering if liraglutide might be a better fit for your situation, the answer lies in the details that most comparison articles skip entirely.
What GLP-1 receptor agonists actually do
Before comparing these two peptides head to head, it helps to understand what they share. Both semaglutide and liraglutide belong to the class of GLP-1 receptor agonists. They mimic a natural hormone called glucagon-like peptide-1, which the gut produces after eating. This hormone does several things simultaneously. It signals the pancreas to release insulin. It tells the liver to stop producing excess glucose. It slows the rate at which food leaves the stomach. And it communicates with the brain to reduce hunger.
The natural GLP-1 hormone has a problem. It breaks down within minutes. The enzyme DPP-4 degrades it almost immediately after release, giving it a half-life of roughly two minutes. That is far too short for therapeutic use.
Both semaglutide and liraglutide solve this degradation problem, but they solve it differently. And those different solutions create the cascading differences in dosing, efficacy, and side effects that matter to anyone choosing between them. Understanding whether GLP-1 is the same as Ozempic starts with grasping this fundamental mechanism. The natural hormone, the synthetic analogs, and the brand-name products each represent a different layer of the same biological system.
The shared mechanism of action
When you inject either semaglutide or liraglutide, the peptide circulates through the bloodstream and binds to GLP-1 receptors throughout the body. These receptors sit on pancreatic beta cells, in the hypothalamus, along the vagus nerve, and in the gastrointestinal tract. The binding triggers a cascade of effects that researchers studying how long GLP-1 takes to start working have documented extensively.
Insulin secretion increases, but only when blood sugar is elevated. This glucose-dependent mechanism is what makes GLP-1 agonists safer than older diabetes drugs that could cause dangerous hypoglycemia. Glucagon, the hormone that raises blood sugar, gets suppressed. Gastric emptying slows down, meaning food stays in the stomach longer, creating prolonged feelings of fullness. And appetite centers in the brain receive signals that reduce hunger and food cravings.
Both peptides do all of this.
The difference lies in how well they do it, how long they do it, and what side effects accompany the process. Those differences trace back to molecular structure, which determines everything downstream.
Molecular structure: where the real differences begin
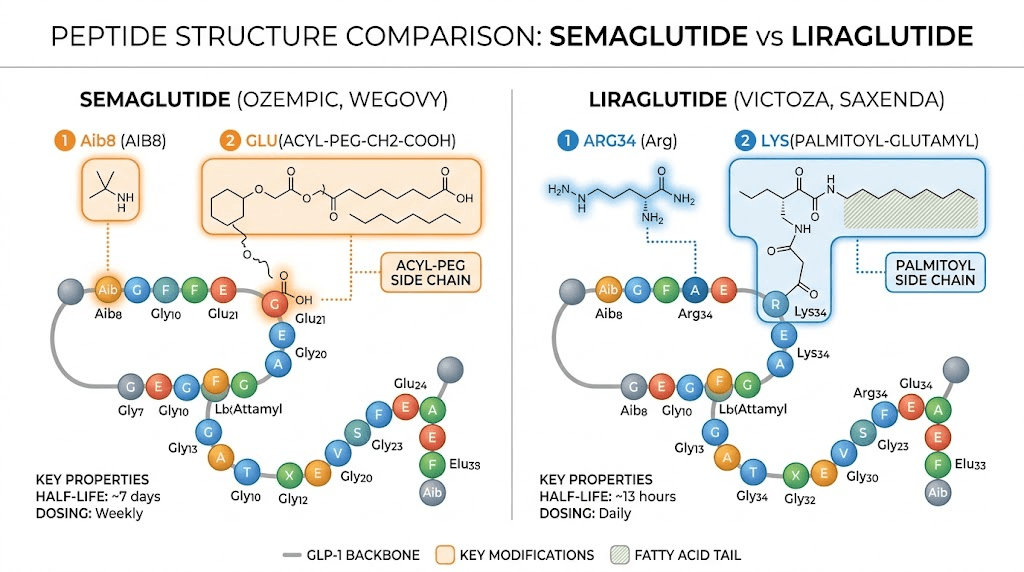
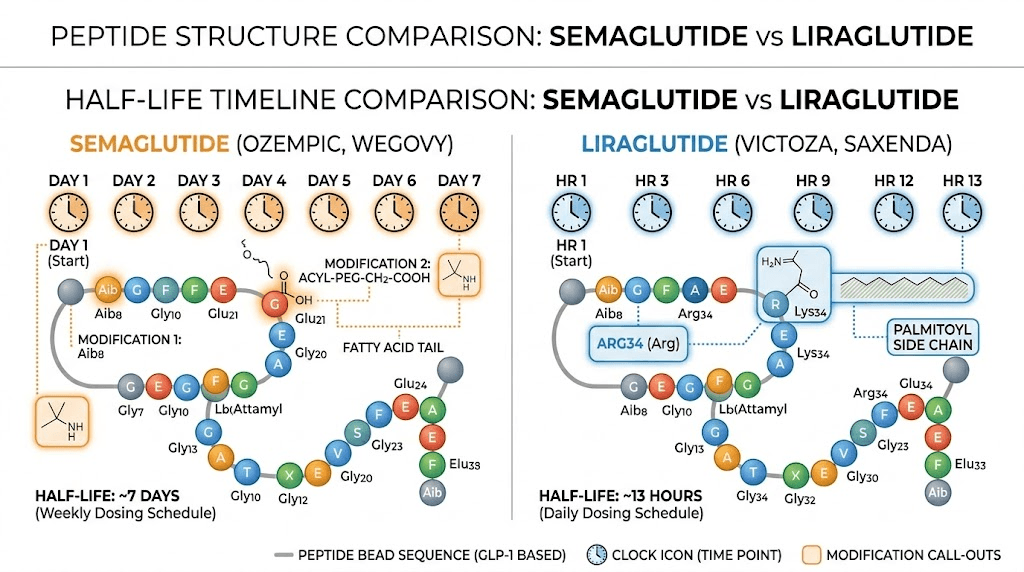
Liraglutide was the first modification. Scientists took the natural GLP-1 molecule and made a single key change: they attached a C16 fatty acid chain (palmitic acid) at position 26. This fatty acid allows the molecule to bind to albumin, a protein in the blood. Albumin acts like a protective shield, slowing degradation and extending the half-life from two minutes to 13 to 15 hours. A massive improvement.
But 13 hours is still short enough to require daily dosing.
Semaglutide came later, building on everything researchers learned from liraglutide. The modifications were more extensive and more strategic. First, a longer C18 fatty diacid chain replaced the C16 fatty acid, creating stronger albumin binding. Second, and this is the critical change, an alpha-aminoisobutyric acid (Aib) substitution was placed at position 2 of the peptide chain. This single amino acid swap makes semaglutide nearly resistant to DPP-4 degradation, the enzyme that destroys natural GLP-1 within minutes.
The result? A half-life of approximately 165 hours. That is seven full days. One injection per week maintains therapeutic blood levels continuously, compared to liraglutide requiring a needle every single day. For anyone interested in the practical details of administering these peptides, understanding the best injection site for semaglutide and proper injection technique with a syringe becomes important.
Why molecular modifications matter more than you think
The Aib substitution at position 2 does not just extend the half-life. It fundamentally changes how the molecule interacts with GLP-1 receptors. Semaglutide demonstrates approximately three times greater potency at GLP-1 receptors compared to liraglutide. Three times. That means each molecule of semaglutide activates the receptor more effectively, producing stronger downstream effects on insulin release, appetite suppression, and gastric emptying.
This enhanced potency explains why semaglutide produces greater weight loss at lower relative doses. It explains why the appetite suppression from semaglutide tends to be more pronounced. And it explains why some patients who respond poorly to liraglutide see better results when switching to semaglutide, despite both drugs targeting the exact same receptor.
Think of it this way. Liraglutide knocks on the door of the GLP-1 receptor. Semaglutide kicks it open.
Dosing schedules and titration protocols
The dosing differences between semaglutide and liraglutide reflect their pharmacokinetic profiles. Because liraglutide has a 13 to 15 hour half-life, it must be injected daily to maintain effective blood levels. Semaglutide, with its 165-hour half-life, requires only a weekly injection. This single distinction shapes the entire treatment experience.
Liraglutide dosing protocol
Liraglutide for weight management (marketed as Saxenda) follows a five-week titration schedule. Patients start at 0.6 mg daily during week one. The dose increases to 1.2 mg in week two, then 1.8 mg in week three, 2.4 mg in week four, and finally reaches the maintenance dose of 3.0 mg daily from week five onward. Each step allows the gastrointestinal system to adapt gradually.
For diabetes management (marketed as Victoza), the maximum dose is lower at 1.8 mg daily. The titration is simpler: start at 0.6 mg daily for one week, then increase to 1.2 mg, with an optional increase to 1.8 mg if additional glycemic control is needed.
The daily injection requirement means 365 injections per year. For someone using liraglutide long-term, that adds up. Each injection needs proper timing, proper technique, and consistent compliance. Missing doses creates gaps in coverage that affect both blood sugar control and appetite suppression.
Semaglutide dosing protocol
Semaglutide for weight management (marketed as Wegovy) uses a 16-week titration. The starting dose is 0.25 mg weekly for four weeks. It increases to 0.5 mg for the next four weeks, then 1.0 mg for four weeks, followed by 1.7 mg for four weeks, before reaching the full maintenance dose of 2.4 mg weekly. This slower escalation helps minimize gastrointestinal side effects, though the bloating that some users experience can still occur during titration.
For diabetes (Ozempic), the dosing starts at 0.25 mg weekly for four weeks, increases to 0.5 mg, and can go up to 1.0 mg or 2.0 mg depending on glycemic needs. The semaglutide dosage calculator on SeekPeptides can help you understand the precise unit measurements for different concentrations.
Weekly dosing means 52 injections per year instead of 365. That is an 86% reduction in injection frequency, which dramatically improves adherence. Studies consistently show that patients comply better with weekly injections than daily ones. Fewer injections mean fewer opportunities to miss a dose, forget, or simply get tired of the routine. For a detailed breakdown of how units translate to milligrams, the semaglutide dosage in units guide provides the specific conversions.
Comparing the titration experience
Liraglutide reaches its full dose in five weeks. Semaglutide takes sixteen. That longer titration is intentional. Because semaglutide is more potent and stays in the system for a full week, rushing to the maintenance dose would overwhelm the gastrointestinal system. The gradual increase gives the body time to adapt to the stronger receptor activation.
For people who are impatient to see results, the first week on semaglutide can feel underwhelming. The 0.25 mg starting dose is primarily about tolerability, not therapeutic effect. Real appetite suppression and weight loss typically begin after moving to higher doses. Understanding when you start losing weight on semaglutide requires patience and realistic expectations about the titration timeline.
Weight loss results: the clinical evidence
This is where the data gets compelling. Head-to-head clinical trials have directly compared semaglutide and liraglutide for weight loss, and the results are not close.
The STEP 8 trial: direct comparison
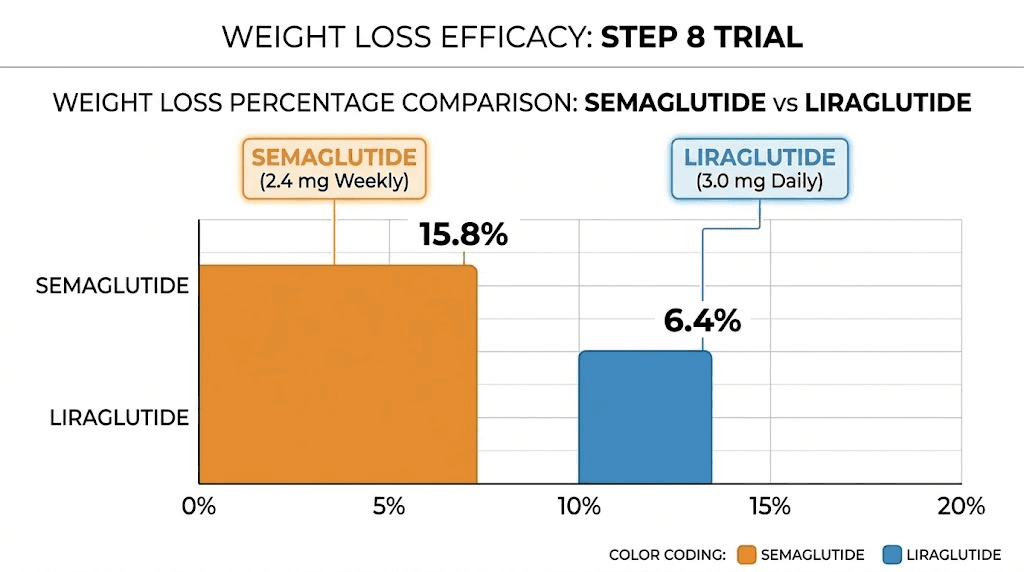
The STEP 8 trial is the most important study for this comparison because it pitted semaglutide 2.4 mg weekly directly against liraglutide 3.0 mg daily in adults with overweight or obesity but without diabetes. The trial ran for 68 weeks with 338 participants.
The results were decisive. Semaglutide produced a mean body weight reduction of 15.8%. Liraglutide produced 6.4%. Semaglutide nearly tripled the weight loss. In absolute terms, semaglutide users lost an average of 15.3 kg compared to 6.0 kg with liraglutide. The proportion of participants achieving at least 10% weight loss was 70.9% with semaglutide versus 25.6% with liraglutide. For 20% or greater weight loss, it was 38.5% versus 6.0%.
Those are not marginal differences. They represent fundamentally different levels of efficacy.
Individual trial results
Looking at each drug independently reinforces the pattern. The STEP 1 trial studied semaglutide 2.4 mg weekly in adults without diabetes and found 14.9% mean body weight loss versus 2.4% with placebo at 68 weeks. Nearly a 15% reduction in body weight from a single weekly injection combined with lifestyle modifications. The week-by-week semaglutide results show that weight loss accelerates after the first few months as patients reach higher doses.
The SCALE trial for liraglutide showed approximately 8% body weight loss versus about 2.6% with placebo at 56 weeks. Solid results by historical standards, but clearly outpaced by semaglutide. Understanding how fast you can lose weight on semaglutide requires looking at these trial timelines carefully, because the weight loss curve is not linear.
For people tracking their own progress, semaglutide one-month results and before-and-after comparisons provide useful benchmarks, though individual results vary significantly based on diet, exercise, starting weight, and adherence.
Why does semaglutide produce more weight loss?
Three factors explain the gap.
First, greater receptor potency. Semaglutide activates GLP-1 receptors approximately three times more effectively than liraglutide. This translates to stronger appetite suppression, more pronounced satiety signals, and greater reduction in food intake. People on semaglutide consistently report feeling less hungry, less preoccupied with food, and more satisfied with smaller portions. The way semaglutide makes you feel differs from liraglutide in both intensity and duration of appetite control.
Second, sustained exposure. With a weekly injection, semaglutide maintains steady blood levels around the clock. There are no daily peaks and troughs like with liraglutide. This continuous receptor stimulation provides uninterrupted appetite control, whereas liraglutide levels dip between doses, potentially allowing brief windows of increased hunger.
Third, central nervous system effects. Research suggests semaglutide may have enhanced ability to cross the blood-brain barrier compared to liraglutide, leading to stronger effects on the hypothalamic appetite centers.
This could explain why semaglutide users report more profound changes in food preferences, reduced cravings, and less emotional eating.