Apr 2, 2026

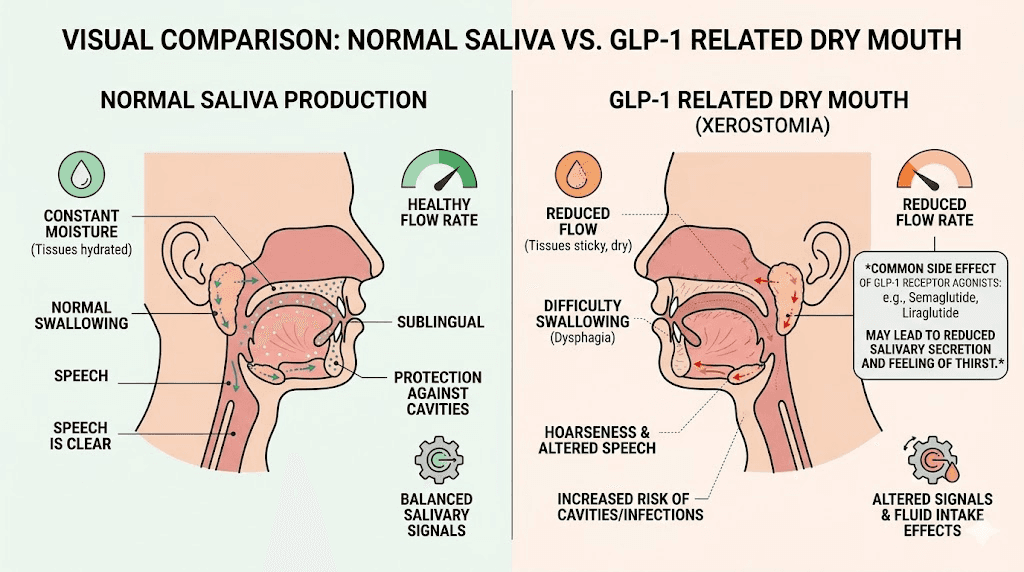
Your mouth feels like sandpaper. You wake up at 3 AM with your tongue stuck to the roof of your mouth, reaching for water that barely helps. The dryness lingers all day, making it hard to swallow food, talk comfortably, or even taste your meals properly. And nobody warned you this would happen when you started your GLP-1 medication.
You are not imagining it. Dry mouth is one of the most common yet least discussed side effects of semaglutide, tirzepatide, and other GLP-1 receptor agonists. Pharmacovigilance data show elevated reporting-odds ratios for dry mouth across the entire medication class, with semaglutide at 1.34 and tirzepatide at 1.35. Those numbers might seem small. They are not. They represent thousands of people dealing with a problem that goes far beyond simple discomfort.
Untreated dry mouth does not just feel unpleasant. It creates a cascade of oral health problems, from accelerated tooth decay to gum disease, that can become serious if ignored. The term "Ozempic teeth" has entered the cultural conversation for a reason. Reduced saliva means reduced protection for your teeth, your gums, and the entire oral ecosystem that depends on adequate moisture to function properly. Understanding why GLP-1 medications cause dry mouth, how long it typically lasts, and what you can do about it makes the difference between a manageable side effect and a genuine health concern. SeekPeptides has compiled everything researchers and users need to know about this underreported problem, from the molecular mechanisms behind it to the daily strategies that actually work.
What GLP-1 dry mouth actually feels like
Dry mouth from GLP-1 medications is not the same as being thirsty after a workout. It is a persistent, clinical dryness that affects multiple aspects of daily life. Understanding the symptoms helps you identify the problem early, before it leads to more serious complications.
The medical term is xerostomia. It describes a subjective sensation of oral dryness that may or may not correspond to measurably reduced saliva flow. Some people on compounded semaglutide or tirzepatide experience the sensation of dryness without significant changes in actual saliva production. Others develop genuine hyposalivation, where saliva output drops below 0.1 mL per minute at rest.
The difference matters clinically. But for you, the person living with it, the experience is miserable either way.
Common symptoms to watch for
The most obvious symptom is the feeling that your mouth simply does not have enough moisture. Your tongue feels thick and sticky. Swallowing becomes difficult, especially with dry foods like bread, crackers, or rice. Many people on their first weeks of semaglutide notice their lips cracking more frequently and their throat feeling scratchy even when they are not sick.
But dry mouth shows up in subtler ways too. Your sense of taste changes. Foods you used to enjoy taste bland or metallic. Speaking for extended periods becomes uncomfortable, and you find yourself clearing your throat constantly. Some users report waking up multiple times at night because the dryness becomes unbearable during sleep, when saliva production naturally decreases.
A thick, frothy saliva is another telltale sign. Instead of the thin, clear saliva that normally coats your mouth, you notice a white, stringy substance that does not provide the same protective coating. Published case reports describe three patients on semaglutide presenting with "minimal frothy saliva" and significant oral discomfort, confirming this is a recognized clinical finding rather than an isolated complaint.
How it differs from normal thirst
Many GLP-1 users initially mistake dry mouth for simple dehydration. They drink more water. The dryness persists. They drink even more. Still dry. This is the key distinction. Normal thirst resolves when you drink fluids. GLP-1 related dry mouth often persists regardless of fluid intake because the underlying cause involves changes in saliva production or composition, not just total body hydration.
That said, dehydration absolutely contributes to the problem and makes it worse. Many users experience reduced appetite and food intake on GLP-1 medications, which means they are also consuming less water from food sources. The result is a compounding effect where genuine dehydration layers on top of medication-induced changes in salivary function.
Why GLP-1 medications cause dry mouth
The mechanism behind GLP-1 related dry mouth is more complex than most people realize. It is not a single cause but rather a convergence of several biological pathways that all reduce the moisture in your mouth. Researchers are still untangling the exact contributions of each mechanism, but the current evidence points to three major factors working together.
The dehydration pathway
The most straightforward explanation starts with what GLP-1 medications do to your eating and drinking habits. Semaglutide suppresses appetite significantly, and this suppression can begin within days of the first dose. When you eat less, you drink less. When you drink less, your body has less fluid available for all its functions, including saliva production.
GLP-1 receptor agonists also slow gastric emptying. This means food and liquid sit in your stomach longer, which can cause bloating and reduce the desire to consume more fluids. The nausea that many users experience during the early weeks further suppresses fluid intake. Some users also experience vomiting or diarrhea, both of which accelerate fluid loss.
The math is simple. Less fluid in means less fluid available for saliva. Your body prioritizes vital organ function over salivary gland output. And your mouth pays the price.
Direct effects on salivary glands
Here is where the science gets interesting. GLP-1 receptors are not just found in the pancreas and gut. They are expressed in salivary gland tissue. This means GLP-1 medications can directly influence how your salivary glands function, independent of hydration status.
A comprehensive narrative review published in Biology synthesized 78 studies across five mechanistic domains and identified a compelling pathway. Normal salivary secretion depends on a carefully orchestrated interplay between calcium signaling and cyclic AMP (cAMP) within gland cells. These two signaling systems create a rhythmic pattern that drives healthy saliva production. When a GLP-1 receptor agonist binds to receptors on salivary gland tissue, it disrupts this rhythmic cross-talk.
Semaglutide presents a particularly interesting case. Its strong albumin binding gives it an exceptionally long half-life, which is why you only inject it once per week. But this same property means the drug maintains persistent stimulation of GLP-1 receptors, including those in salivary glands. Persistent stimulation leads to receptor desensitization. The receptors essentially become fatigued, triggering a process called beta-arrestin mediated internalization where the receptors are pulled from the cell surface and recycled internally.
The result is reduced gland responsiveness. Your salivary glands receive less effective signaling to produce saliva, even though the medication is actively stimulating them. It is a paradox of overstimulation leading to underperformance.
The biased agonism factor
Different GLP-1 medications interact with their target receptors in subtly different ways. This concept, called biased agonism, helps explain why some users experience more severe dry mouth with one medication versus another.
Semaglutide and native GLP-1 promote what researchers call conventional recycling and internalization of the GLP-1 receptor. The receptor gets stimulated, pulled inside the cell, and then recycled back to the surface. Tirzepatide, on the other hand, favors sustained receptor retention at the plasma membrane with reduced cytosolic trafficking. In simpler terms, tirzepatide keeps the receptor at the cell surface longer but may affect its internal signaling differently.
These molecular differences could explain the slightly different dry mouth profiles between medications. They also suggest that switching medications might help if dry mouth is severe, though the evidence for this approach is still emerging. Understanding the side effect differences between semaglutide and tirzepatide can help guide these decisions.
Which GLP-1 medications cause dry mouth most
Not all GLP-1 medications create the same degree of dry mouth. The pharmacovigilance data reveal meaningful differences that can inform your approach to managing this side effect or potentially avoiding the worst of it.
Semaglutide dry mouth profile
Semaglutide, marketed as Ozempic and Wegovy, carries a reporting-odds ratio of 1.34 for dry mouth in adverse event databases. The combination of its strong albumin binding and long half-life creates conditions for sustained receptor stimulation in salivary glands. Users taking higher doses tend to report more pronounced dryness, particularly during the dose escalation phase.
Dry mouth with semaglutide often appears alongside other oral symptoms. Users report taste changes, sulfur burps, and acid reflux, all of which can compound the discomfort. The compounded formulations that include B12 or glycine do not appear to significantly change the dry mouth profile, though some users anecdotally report that glycine-B12 blends produce slightly fewer side effects overall.
Tirzepatide dry mouth profile
Tirzepatide, marketed as Mounjaro and Zepbound, shows a reporting-odds ratio of 1.35 for dry mouth, marginally higher than semaglutide. As a dual GIP/GLP-1 receptor agonist, tirzepatide works through additional pathways compared to pure GLP-1 agonists. Whether GIP receptor activation in salivary gland tissue contributes to dry mouth remains an open research question. Users taking various tirzepatide doses report different severity levels, with higher doses producing more pronounced symptoms in most cases.
Users who have tried both medications report mixed experiences. Some find switching between medications changes their dry mouth severity, while others notice no difference. The dosage conversion charts between these medications can help guide transitions. The individual variation suggests that personal genetics, hydration habits, and baseline salivary function play significant roles beyond the medication itself. Those experiencing other tirzepatide body aches or muscle pain alongside dry mouth may benefit from a comprehensive side effect management approach rather than addressing each symptom in isolation.
Retatrutide and newer agents
Retatrutide, a triple agonist targeting GLP-1, GIP, and glucagon receptors, is still in clinical development but early data suggest similar gastrointestinal side effect profiles. Users exploring retatrutide protocols should anticipate dry mouth as a potential side effect and plan accordingly. The retatrutide dosage chart typically starts low and escalates gradually, and dry mouth may worsen at each step. The addition of glucagon receptor activation introduces another variable that could theoretically affect fluid balance and salivary function, though specific data on retatrutide versus tirzepatide for dry mouth are not yet available. Users interested in how long retatrutide takes to work should factor in a similar adjustment period for side effects including dry mouth.
Survodutide and mazdutide represent other emerging options in this space. The three-way comparison between semaglutide, tirzepatide, and retatrutide continues to evolve as more clinical data becomes available. As the pipeline of GLP-1 based medications expands, monitoring for dry mouth will likely become a standard part of side effect management across the entire class.
How long does GLP-1 dry mouth last
This is the question everyone asks. The honest answer is that it varies enormously from person to person. But the data we do have provide some useful guideposts for setting expectations.
The typical timeline
For most users, dry mouth is worst during the first few weeks of treatment and during dose escalation periods. Your body is adjusting to a new medication that fundamentally changes how your digestive system operates. The first week on semaglutide often brings the most dramatic side effects, including dry mouth, as the medication reaches therapeutic levels.
Many users report significant improvement by weeks four through six. The body adapts. Salivary glands adjust to the new signaling environment. Hydration habits improve as nausea subsides and eating patterns stabilize. Published case reports document one patient whose symptoms improved within four weeks, while another required 16 weeks for salivary flow to normalize.
However, some users experience persistent dry mouth throughout their entire course of treatment. This tends to correlate with higher doses and longer treatment durations. If you are on a maintenance dose and still experiencing dry mouth after several months, the strategies in the remedies section become essential rather than optional.
What happens when you stop
The good news is that dry mouth typically resolves after discontinuing GLP-1 medications. Case report data show salivary flow returning to normal within four weeks of stopping semaglutide. This aligns with the medication pharmacology, as semaglutide has a half-life of approximately one week, meaning it takes roughly five weeks for the drug to be essentially cleared from your system.
Users weaning off tirzepatide or managing semaglutide withdrawal should expect dry mouth to gradually improve as tissue levels decrease. The key word is gradually. Do not expect overnight resolution.
Dose escalation and dry mouth flares
Each time you increase your dose, dry mouth may temporarily worsen. This is a predictable pattern that catches many users off guard. You might have adapted to your starting dose and feel fine, only to have dry mouth return when you move to the next tier.
Plan for this. Intensify your hydration and oral care strategies around dose increases. Having electrolyte solutions and xylitol products ready before a scheduled increase prevents the worst of the flare from catching you unprepared.
The hidden danger: dry mouth and oral health
Here is where this side effect becomes genuinely concerning. Dry mouth is not just uncomfortable. It is a direct threat to your teeth, gums, and overall oral health. Saliva does far more than keep your mouth wet. It is an active defense system, and when it fails, problems escalate quickly.
Why saliva matters more than you think
Saliva contains antibacterial enzymes that suppress harmful bacteria. It provides a mineral-rich coating that repairs early enamel damage through a process called remineralization. It buffers acids from food and drink, maintaining a pH that protects tooth enamel. It washes away food particles that would otherwise feed cavity-causing bacteria. And it contains immunoglobulins that support gum tissue health.
Remove saliva from this equation and every one of these protective functions collapses.
The result is what dental professionals now call "Ozempic teeth," a pattern of accelerated decay, increased sensitivity, and gum disease appearing in patients on GLP-1 medications. Reports include rapid tooth decay, enamel erosion, increased sensitivity, bad breath, and in severe cases, tooth fractures or loss. These outcomes are not caused by the medication directly attacking teeth. They are caused by the loss of saliva protection that the medication indirectly creates.
The bacterial shift
When saliva flow decreases, the bacterial environment in your mouth changes dramatically. Beneficial bacteria that thrive in well-hydrated, neutral-pH conditions decline. Opportunistic bacteria, particularly Streptococcus mutans, the primary driver of tooth decay, proliferate. This bacterial shift can happen within weeks of sustained dry mouth and can persist even after saliva flow normalizes, because the new bacterial colonies have established themselves.
This is why addressing dry mouth early matters so much. Every week of unmanaged dryness gives harmful bacteria more opportunity to colonize and damage your teeth. Users focused on managing other GLP-1 side effects like constipation or fatigue sometimes overlook dry mouth as a minor inconvenience. It is anything but minor.
The acid reflux connection
GLP-1 medications commonly cause acid reflux and gastroesophageal symptoms. When stomach acid reaches the mouth, it erodes enamel directly. Normally, saliva buffers this acid quickly, limiting exposure time. But with reduced saliva, acid contact with tooth enamel lasts longer and causes more damage.
The combination of dry mouth plus acid reflux is particularly destructive. Users experiencing both should consider this a dental emergency in slow motion and act accordingly. Rinsing with water or a sodium bicarbonate solution after any reflux episode helps neutralize acid when saliva cannot do the job effectively.
Scheduling dental care on GLP-1 medications
If you are taking any GLP-1 medication, inform your dentist. Standard recommendations suggest dental cleanings every six months, but patients on GLP-1 medications experiencing dry mouth should consider cleanings every three to four months. More frequent professional monitoring catches early decay and gum inflammation before they become serious problems.
Your dentist may also recommend prescription-strength fluoride treatments, custom fluoride trays for home use, or specific remineralizing products that help compensate for the protective role that saliva normally plays.
12 proven remedies for GLP-1 dry mouth
Managing dry mouth on GLP-1 medications is not about finding one magic solution. It is about layering multiple strategies that address different aspects of the problem. Some target hydration. Others stimulate saliva production. Others protect your teeth from the damage that dry mouth enables. Used together, they can make this side effect far more manageable.
1. Strategic hydration (not just drinking more water)
Everyone says "drink more water." That advice is incomplete. The goal is not just volume but timing and composition.
Sip water continuously throughout the day rather than drinking large amounts at once. Large gulps pass through quickly without sustained benefit to your oral tissues. Small, frequent sips maintain consistent moisture. Keep water within arm reach at all times, including on your nightstand, at your desk, and in your car.
Add electrolytes to at least some of your daily water intake. Electrolytes improve water retention at the cellular level, meaning your body holds onto more of what you drink rather than simply excreting it. This is especially important for users experiencing dizziness or lightheadedness, which often indicate dehydration compounding dry mouth.
2. Xylitol products
Xylitol is a sugar alcohol that does double duty for dry mouth. It stimulates saliva production by activating sweetness receptors on the tongue, and it actively inhibits Streptococcus mutans, the bacteria primarily responsible for tooth decay. Research shows that using xylitol-containing gum or lozenges four to five times daily after meals significantly reduces cavity-producing bacteria.
Look for xylitol gum, mints, or lozenges specifically. Products like Spry, XyliMelts, and Ice Chips are widely available. XyliMelts are particularly useful at night because they adhere to your gum tissue and slowly release xylitol while you sleep, when dry mouth tends to be worst.
3. Saliva substitutes and oral sprays
When your glands are not producing enough saliva, artificial saliva products fill the gap. Biotene makes a range of products including oral rinse, spray, and gel specifically formulated for dry mouth. Aquoral is a prescription spray that creates a protective lipid barrier on oral tissues.
These products do not fix the underlying cause. They manage the symptom. But they manage it effectively, providing immediate relief and protecting tissues that would otherwise be exposed. The gel formulations work well at bedtime, providing longer-lasting moisture than sprays.
4. Humidifier use at night
Nighttime is when dry mouth hits hardest. Saliva production naturally drops during sleep, and mouth breathing, which many people do without realizing it, accelerates moisture loss. Running a humidifier in your bedroom adds moisture to the air you breathe, reducing evaporative loss from oral tissues.
Target 40-50% humidity in your sleeping environment. A cool-mist humidifier works well and avoids the burn risk of warm-mist models. This simple intervention provides passive moisture support all night without requiring you to wake up and drink water.
5. Dietary adjustments for oral moisture
What you eat affects how dry your mouth feels. Emphasize moist, soft foods, especially during the early weeks of GLP-1 treatment when dry mouth and appetite changes are most intense. Soups, stews, smoothies, and yogurt all provide both nutrition and moisture.
Avoid foods that make dryness worse. Salty snacks pull moisture from oral tissues. Dry, crumbly foods like crackers and bread become difficult to swallow and can irritate already-dry mucous membranes. Spicy foods may increase discomfort. Users following a semaglutide diet plan or tirzepatide meal plan should incorporate moisture-rich foods as a deliberate priority, not an afterthought.
6. Eliminate drying agents
Several common substances actively worsen dry mouth. Caffeine is a mild diuretic that increases fluid loss. Alcohol, both in drinks and in many commercial mouthwashes, dries oral tissues directly. Tobacco products of all types reduce saliva production and damage salivary gland tissue.
Switch to alcohol-free mouthwash immediately. This is non-negotiable if you are experiencing dry mouth. Standard mouthwashes containing alcohol provide a temporary clean feeling but leave your mouth drier than before. Products like Biotene mouthwash, CloSYS, or any formulation labeled "alcohol-free" are appropriate substitutes.
Reducing caffeine does not mean eliminating it entirely. But be aware that every cup of coffee or caffeinated tea slightly increases your net fluid loss. Compensate with additional water or switch some caffeinated beverages to herbal tea. Users wondering whether alcohol is safe on semaglutide or tirzepatide should factor dry mouth into their decision, as alcohol compounds the problem significantly.
7. Citric acid stimulation (with caution)
Sour flavors are among the most powerful natural stimulants for saliva production. Citric acid and malic acid activate taste receptors that trigger a reflexive increase in salivary output. Sugar-free lemon drops, sour candies, and adding lemon or lime to water can all provide temporary relief.
The caution is important. Citric acid is also acidic enough to erode tooth enamel, particularly when saliva is not present in sufficient quantities to buffer it. Use citric acid stimulation strategically, not constantly. And always rinse with plain water afterward to dilute any residual acid on tooth surfaces.
8. Proper oral hygiene protocol
Standard oral hygiene is not enough when you have dry mouth. You need an enhanced protocol that compensates for lost salivary protection.
Brush twice daily with fluoride toothpaste. Consider a prescription-strength fluoride toothpaste (1.1% sodium fluoride) if your dentist recommends it. Floss daily. Use an alcohol-free fluoride rinse before bed. Some dentists recommend a remineralizing toothpaste or gel containing hydroxyapatite, which directly repairs enamel without relying on saliva to deliver minerals.
After meals, rinse your mouth with plain water if brushing is not immediately possible. This simple step removes food debris that bacteria would otherwise feast on, a job that saliva normally handles automatically.
9. Nasal breathing practice
Mouth breathing accelerates moisture loss from oral tissues. Many people, particularly during sleep, breathe through their mouths without awareness. Taping your mouth lightly during sleep, a practice that has gained popularity in recent years, encourages nasal breathing and dramatically reduces overnight dry mouth.
During the day, simply being conscious of breathing through your nose makes a noticeable difference. If nasal congestion makes nose breathing difficult, address that issue with saline sprays or decongestants, because solving nasal obstruction can indirectly improve dry mouth.
10. Timing your medication strategically
Some users find that timing their semaglutide injection or tirzepatide dose to coincide with a specific day of the week helps them manage side effects better. Injecting on a day when you can prioritize hydration and rest, rather than a busy workday, gives your body more support during the peak side-effect window.
The best time to take your GLP-1 shot varies by individual, but consistency matters. Taking it at the same time and on the same day each week helps your body establish predictable patterns that make side effect management easier.
11. Sugar-free gum throughout the day
Chewing stimulates saliva production mechanically, independent of any ingredient effect. The physical act of chewing activates the parotid glands and triggers increased salivary output. Sugar-free gum with xylitol combines this mechanical stimulation with the antimicrobial benefits of xylitol, making it one of the most effective and accessible dry mouth interventions available.
Aim for 5-10 minutes of chewing after each meal and whenever dryness becomes particularly bothersome. Keep gum accessible in multiple locations so it is always within reach when symptoms flare.
12. Prescription options for severe cases
When over-the-counter approaches are not sufficient, prescription medications can stimulate saliva production at a pharmacological level. Pilocarpine (Salagen) and cevimeline (Evoxac) are cholinergic agonists that directly stimulate salivary gland secretion. These medications have their own side effect profiles and are not appropriate for everyone, but they represent a genuine option for severe dry mouth that does not respond to conservative measures.
Discuss these options with your healthcare provider if your dry mouth is significantly affecting quality of life or if you are developing dental complications despite implementing the strategies above. Users who are also dealing with anxiety from tirzepatide or insomnia from semaglutide should discuss all symptoms together, as a comprehensive approach to side effect management is more effective than treating each in isolation.
When to talk to your doctor about GLP-1 dry mouth
Mild dry mouth that responds to hydration and over-the-counter products is manageable on your own. But certain situations warrant professional attention sooner rather than later.
Red flags that require medical evaluation
See your healthcare provider if dry mouth is severe enough to interfere with eating, speaking, or sleeping despite implementing management strategies. If you notice rapid changes in your teeth, including new sensitivity, visible white spots (early decay), or dark spots, see a dentist immediately. Persistent bad breath despite good oral hygiene suggests bacterial overgrowth that needs professional assessment.
Difficulty swallowing, called dysphagia, is a more serious symptom that goes beyond simple dryness. If you cannot swallow food or pills without significant effort, your provider needs to evaluate whether dose adjustment or medication change is appropriate. Users experiencing multiple side effects simultaneously, such as dry mouth combined with severe constipation, fatigue, and headaches, should discuss overall tolerability with their prescriber.
Dose adjustment considerations
If dry mouth is severe and persistent, your provider may consider slowing dose escalation, reducing the current dose, or switching to a different GLP-1 medication. Some users find that a microdosing approach produces fewer side effects while still providing meaningful therapeutic benefit. The conversion between semaglutide and tirzepatide is another option, as individual responses to each medication vary significantly.
Never adjust your dose without consulting your prescriber. But know that dose modification is a legitimate tool for managing side effects, and a good provider will work with you to find the balance between therapeutic benefit and tolerability. If you are considering stopping treatment entirely, understanding the semaglutide withdrawal process or how to wean off tirzepatide safely is essential for avoiding rebound effects.
Preventing dry mouth before it starts
The best approach to GLP-1 dry mouth is proactive, not reactive. If you know you are starting a GLP-1 medication, implementing preventive strategies before your first dose significantly reduces the severity of dry mouth when it appears.
Pre-treatment preparation
Schedule a dental cleaning and exam before starting your GLP-1 medication. Identify and treat any existing dental issues, because dry mouth will accelerate their progression. Ask your dentist about fluoride varnish application as a protective measure.
Stock your home with dry mouth management products. Have xylitol gum, Biotene products, electrolyte packets, and a bedside water bottle ready before your first injection. This is the same preparation mindset that helps with managing other early side effects like constipation or bloating.
Establish a hydration baseline. Track your daily fluid intake for a week before starting treatment. Most people underestimate how much they drink. Knowing your baseline helps you ensure you maintain or increase intake once appetite suppression kicks in and the natural urge to drink decreases.
First week strategies
The first week on semaglutide or the initial tirzepatide dose is when side effects are most likely to appear. Prioritize fluid intake even if you do not feel thirsty. Set phone reminders to drink water every 30-60 minutes. Use an app or marked water bottle to track intake, aiming for at least 64 ounces daily, more if you are active or in a warm climate.
Start using xylitol products immediately, before dry mouth appears. Prevention is significantly more effective than treatment for maintaining oral bacterial balance. Once harmful bacteria establish colonies, reversing that shift takes much longer than preventing it in the first place. Users can calculate their specific dosing needs using the semaglutide dosage calculator or the peptide calculator to ensure they are starting at the appropriate level for their body weight.
Diet and nutrition adjustments for GLP-1 dry mouth
Your diet plays a dual role in managing dry mouth. The right foods provide moisture directly and support the body systems that produce saliva. The wrong foods exacerbate dryness and create additional oral health risks. Users already working on their food choices while on semaglutide or tirzepatide should integrate these dry mouth considerations into their meal planning.
Foods that help
Water-rich fruits and vegetables provide hydration plus nutrients that support oral tissue health. Cucumbers, watermelon, celery, oranges, strawberries, and lettuce all contain 90% or more water by weight. Incorporating these into meals and snacks adds meaningful hydration beyond what you drink.
Soups and broths deliver both fluid and electrolytes. Bone broth in particular provides collagen precursors that support mucosal tissue integrity. Smoothies made with yogurt, fruit, and ice offer a nutrient-dense meal option that also bathes oral tissues in moisture. Many of the GLP-1 friendly recipes naturally incorporate moisture-rich ingredients, and dinner ideas for GLP-1 users often feature soups and braised dishes that provide fluid alongside nutrition. Breakfast options like overnight oats with yogurt and fruit deliver early-morning moisture when dry mouth is often worst.
Yogurt and fermented foods introduce beneficial bacteria that can help maintain a healthy oral microbiome even when saliva is reduced. The probiotics beneficial for GLP-1 users often support oral health as a secondary benefit, because the oral and gut microbiomes are interconnected.
Foods that hurt
Sugar is the primary enemy when saliva is low. Without adequate saliva to neutralize acid and wash away sugar, every sugary food or drink becomes a more potent threat to your teeth. Minimize candy, soda, juice, and sweetened coffee drinks. If you consume sugar, rinse your mouth with water immediately afterward.
Very salty foods draw moisture from oral tissues through osmosis, worsening the sensation of dryness. Dry, hard, or crunchy foods are more difficult to chew and swallow when your mouth is dry, and they can scratch irritated mucous membranes. Acidic foods like tomatoes, citrus, and vinegar-based dressings can cause discomfort on dry, sensitive oral tissues.
The foods to avoid on semaglutide and the foods to avoid on tirzepatide overlap significantly with foods that worsen dry mouth. Following these dietary guidelines addresses multiple side effects simultaneously.
Protein and nutrient considerations
Getting adequate protein on semaglutide is important for multiple reasons, including maintaining salivary gland function. The salivary glands are metabolically active tissues that require adequate nutrition to function optimally. Severe caloric restriction, which can happen when appetite suppression is intense, may impair gland function beyond what the medication itself causes. Protein shakes designed for GLP-1 users can help maintain adequate intake even when solid food feels unappealing.
Calcium and vitamin D support the remineralization process that protects teeth from decay. When saliva-mediated remineralization is reduced, ensuring adequate dietary intake of these minerals becomes even more critical. Consider a GLP-1 supplement regimen that includes these nutrients if your diet does not provide sufficient amounts. Users on tirzepatide can explore tirzepatide-specific supplement recommendations for a more tailored approach.
Supplements that support saliva production
While no supplement directly replaces saliva, several nutrients support the biological processes that keep salivary glands functioning and oral tissues healthy. These work best as part of a comprehensive approach rather than standalone solutions.
Omega-3 fatty acids
Research on Sjogren syndrome, an autoimmune condition that attacks salivary glands, shows that omega-3 supplementation can improve dry mouth symptoms and support gland function. While GLP-1 dry mouth has a different mechanism, the anti-inflammatory properties of omega-3 fatty acids may help maintain gland health under pharmacological stress. Fish oil supplements providing 1,000-2,000 mg of combined EPA and DHA daily are a reasonable addition.
B vitamins
B vitamin deficiency can independently cause oral symptoms including dry mouth, glossitis (tongue inflammation), and angular cheilitis (cracked corners of the mouth). Many semaglutide formulations now include B12, and tirzepatide with B12 is similarly available. The semaglutide methylcobalamin compounds and tirzepatide methylcobalamin formulations use the more bioavailable form of B12. If your formulation does not include it, supplementing B12 and a B-complex ensures this potential contributor to dry mouth is addressed.
Zinc
Zinc plays a role in taste perception and salivary gland function. Some research suggests that zinc supplementation can improve taste disturbances associated with dry mouth. A modest daily supplement of 15-30 mg of zinc may help, particularly if taste changes accompany your dry mouth symptoms.
Probiotics
Oral probiotics, particularly strains of Lactobacillus reuteri, can help maintain a healthy oral microbiome when saliva is reduced. These products are designed to colonize the mouth and compete with harmful bacteria. The Pendulum GLP-1 Probiotic Pro includes strains that support both gut and oral health, making it a dual-purpose option for GLP-1 users dealing with dry mouth alongside other gastrointestinal side effects.
GLP-1 dry mouth at night: special considerations
Nighttime presents unique challenges for managing dry mouth. Saliva production naturally decreases by up to 50% during sleep, and many people unconsciously breathe through their mouths while sleeping. For GLP-1 users who already have reduced salivary function, nights can become genuinely miserable.
Building a nighttime dry mouth protocol
Start with your sleeping environment. Run a humidifier set to 40-50% humidity. Position it near your bed for maximum benefit. Keep a water bottle on your nightstand, not across the room where reaching for it fully wakes you up.
Apply a Biotene gel or similar dry mouth gel to your oral tissues before bed. These products create a protective layer that maintains moisture for several hours. XyliMelts adhering tablets are another option, they stick to your gum tissue and slowly dissolve through the night, providing continuous xylitol release and moisture.
Consider mouth taping if you are a mouth breather. This sounds extreme but has become a mainstream sleep hygiene practice. Small, specially designed mouth tape strips gently hold the lips together, encouraging nasal breathing. Better nasal breathing means less evaporative moisture loss from oral tissues throughout the night.
If you take your GLP-1 injection on a specific day, expect nights to be worse in the 48-72 hours following injection when drug levels are peaking. Plan accordingly with extra hydration and additional dry mouth products during this window.
The connection between GLP-1 dry mouth and other side effects
Dry mouth rarely exists in isolation. It typically appears alongside other GLP-1 side effects, and understanding these connections helps you manage everything more effectively.
Dry mouth and nausea
Nausea reduces the desire to eat and drink, worsening dehydration and dry mouth. Dry mouth can worsen the sensation of nausea because a dry, uncoated mouth is more sensitive to gagging and taste disturbances. Breaking this cycle requires addressing both symptoms simultaneously rather than treating them separately.
Small sips of ginger tea provide both hydration and anti-nausea benefit. Sucking on sugar-free hard candy stimulates saliva while settling the stomach. Users dealing with persistent nausea should explore the strategies in our semaglutide tips guide alongside dry mouth management.
Dry mouth and constipation
GLP-1 constipation and dry mouth share a common underlying factor: insufficient fluid intake. When your body is dehydrated enough to reduce saliva production, it is also diverting water away from the colon, hardening stool. Addressing hydration aggressively helps both problems. The fiber supplements recommended for GLP-1 users require adequate water intake to work properly, creating another reason to prioritize fluids.
Dry mouth and fatigue
Dehydration causes fatigue. Semaglutide-related fatigue and GLP-1 tiredness may partially result from the same fluid deficits that cause dry mouth. Improving hydration often provides noticeable improvement in both symptoms. Users who feel persistently tired on their medication should evaluate their fluid intake before attributing fatigue solely to the drug itself.
Dry mouth and taste changes
Saliva is essential for taste perception. It dissolves food molecules and carries them to taste receptors on the tongue. When saliva is insufficient, food tastes bland, metallic, or simply wrong. This taste distortion can further reduce the desire to eat, creating a downward spiral of reduced intake, worse dehydration, and worse dry mouth.
Moistening food with sauces, gravies, or broth helps compensate for reduced saliva in carrying flavor molecules to taste receptors. Some users find that slightly stronger seasonings (not spicy, just more flavorful) help overcome the dulled taste perception that dry mouth creates.
Oral care products specifically for GLP-1 dry mouth
The market for dry mouth products has expanded significantly as GLP-1 medications have become more popular. Here is what works, based on clinical evidence and user experience.
Toothpaste
Switch to a toothpaste formulated for dry mouth. Biotene Gentle Mint toothpaste is designed for this purpose and does not contain sodium lauryl sulfate, a foaming agent in standard toothpastes that can irritate dry oral tissues. Alternatively, a hydroxyapatite toothpaste like Boka or RiseWell provides remineralization support without requiring fluoride, though fluoride remains the most evidence-backed option for cavity prevention.
Mouthwash
Absolutely avoid any mouthwash containing alcohol. Standard Listerine and similar products will make dry mouth dramatically worse. Use Biotene Dry Mouth Oral Rinse, CloSYS Ultra Sensitive, or ACT Dry Mouth Rinse instead. These products provide antimicrobial benefit without the drying effect of alcohol.
Moisturizing gels and sprays
Biotene Moisturizing Gel provides long-lasting relief and works well applied before bed. Aquoral spray, available by prescription, creates a lipid-based barrier that locks in moisture more effectively than water-based products. Oasis Moisturizing Mouth Spray is an over-the-counter option for daytime use.
Lozenges and tablets
XyliMelts are adhering tablets that stick to your gum or cheek and slowly release xylitol over several hours. They are specifically designed for dry mouth and can be used during sleep. Salese lozenges provide longer-lasting moisture than standard hard candy. ACT Dry Mouth lozenges combine xylitol with soothing agents for immediate relief.
Long-term management strategies for chronic GLP-1 dry mouth
Some users experience dry mouth for the entire duration of their GLP-1 treatment. When dry mouth persists for months rather than weeks, the management approach needs to shift from acute symptom relief to sustainable long-term habits that protect oral health over extended periods.
Building sustainable hydration habits
Short-term hydration pushes work for a few weeks. Long-term success requires systems. Set recurring reminders on your phone every hour to drink water. Use a marked water bottle that shows intake goals by time of day. Many GLP-1 users find that linking hydration to other habits works better than willpower alone. Every time you check your phone, take a sip. Every time you stand up, drink water. Every time you use the bathroom, refill your bottle.
Track your daily intake. The goal for most adults on GLP-1 medications is at least 80-100 ounces of fluid daily, more in hot weather or if you exercise. Users managing their calorie intake on semaglutide should remember that reduced food consumption also means reduced water from food sources, requiring deliberate compensation through additional fluid intake.
Quarterly dental monitoring protocol
Standard twice-yearly dental visits are not sufficient for long-term GLP-1 users with persistent dry mouth. Shift to a quarterly schedule that includes professional cleaning, caries risk assessment, and salivary flow evaluation. Ask your dentist to document baseline salivary flow at your first visit after starting medication, which provides a reference point for tracking changes over time.
Between dental visits, perform a monthly self-check. Run your tongue along all tooth surfaces and note any new rough spots, sensitivity, or changes in texture. Check your gums for redness, swelling, or bleeding. Look for white patches on your tongue or cheeks, which can indicate fungal overgrowth that thrives in dry conditions. Early detection of any changes allows early intervention, which is always less invasive and less expensive than treating advanced problems.
Adapting your approach over time
What works at month one may not work at month six. Your body changes. Doses change. Seasons change. Reassess your dry mouth management strategy every few months. If xylitol gum was sufficient initially but dryness is worsening at higher doses, layer in a Biotene gel at night. If nighttime dryness improves but daytime symptoms persist, add more frequent sipping intervals or a daytime oral spray.
Users who have been on semaglutide long-term or those considering maintaining results after tirzepatide should view dry mouth management as an evolving practice rather than a one-time fix.
Exercise, physical activity, and GLP-1 dry mouth
Physical activity creates additional challenges for GLP-1 users dealing with dry mouth. Exercise increases respiratory rate, which accelerates evaporative moisture loss from oral tissues. It increases metabolic water demand. And it diverts blood flow away from salivary glands toward working muscles, temporarily reducing saliva production even in people with normal salivary function.
Hydration strategies for active GLP-1 users
Pre-hydrate before exercise. Drink 16-20 ounces of fluid in the hour before your workout. During exercise, sip every 10-15 minutes rather than waiting until you feel thirsty. Thirst is a lagging indicator of dehydration, and on GLP-1 medications, your thirst signals may be further blunted by the appetite-suppressing effects of the drug.
Electrolyte drinks become more important during exercise because you lose sodium, potassium, and other minerals through sweat. These minerals support fluid retention and cellular hydration. Plain water alone may not be sufficient for workouts lasting longer than 30 minutes. The best electrolytes for GLP-1 users replace what exercise depletes without adding excessive sugar that feeds oral bacteria.
Post-exercise rehydration is equally important. Continue drinking for at least an hour after your workout finishes. Your body continues to lose fluid through cooling mechanisms even after exercise stops. Users wondering whether they can lose weight on semaglutide without exercise might consider that moderate activity, when properly hydrated, actually supports better overall side effect management including dry mouth.
For those building muscle while on GLP-1 medications, the increased protein demands create another reason to prioritize hydration. Protein metabolism requires water, and higher protein diets can contribute to dehydration if fluid intake does not keep pace.
Breathing technique during exercise
Nasal breathing during moderate-intensity exercise reduces oral moisture loss compared to mouth breathing. This is not always possible during high-intensity work, but during warm-ups, cooldowns, walking, and moderate-effort activities, consciously breathing through your nose preserves oral moisture. Train yourself to default to nasal breathing whenever exercise intensity allows it.
GLP-1 dry mouth in specific populations
Dry mouth severity and management needs vary across different populations. Factors like age, hormonal status, existing medical conditions, and concurrent medications all influence both the likelihood and severity of GLP-1 related dry mouth.
Women and hormonal considerations
Hormonal fluctuations independently affect salivary function. Estrogen and progesterone influence salivary gland activity, which is why some women notice dry mouth during menstrual cycle phases, pregnancy, or menopause even without medication. Adding a GLP-1 agonist to this baseline can amplify dry mouth symptoms significantly during certain hormonal windows.
Women tracking whether semaglutide affects their period or tirzepatide changes their cycle should also note whether dry mouth worsens during specific phases. This information helps providers make better-informed decisions about dose timing and management strategies. Women who are breastfeeding while considering GLP-1 medications face additional fluid demands that compound the dry mouth risk.
Older adults
Salivary gland function naturally declines with age. Older adults starting GLP-1 medications already have reduced baseline saliva production, meaning the additional reduction from the medication creates a more severe deficit. Many older adults also take other medications, including blood pressure medications, antidepressants, antihistamines, and diuretics, that independently cause dry mouth. The combination can be particularly challenging.
Older adults should be especially aggressive about dental monitoring and preventive oral care when starting any GLP-1 medication. The cumulative effect of age-related decline plus multiple drying medications plus GLP-1 effects can accelerate dental deterioration rapidly if unmanaged.
Users with existing oral health conditions
If you already have gum disease, active cavities, or other oral health conditions before starting a GLP-1 medication, address these issues first. Dry mouth will accelerate the progression of any existing problem. Starting GLP-1 treatment with a clean bill of dental health gives you the best foundation for managing the oral side effects that may follow.
Users with a history of frequent cavities are at particularly high risk. Their oral bacterial ecology already favors cavity-producing organisms, and reduced saliva removes one of the few remaining protective barriers. These individuals should consider prescription fluoride products from the start rather than waiting to see if problems develop.
Managing dry mouth with different GLP-1 administration routes
The way you take your GLP-1 medication can influence your dry mouth experience. Injectable, oral, and sublingual formulations each have distinct considerations worth understanding.
Injectable GLP-1 medications
Standard injectable GLP-1 medications deliver the drug systemically, meaning it affects salivary glands through bloodstream distribution rather than direct oral contact. The injection site does not significantly influence dry mouth severity, whether you inject in the stomach, thigh, or arm. The systemic effects on salivary function remain the same regardless of where the needle goes.
Users who experience injection site reactions sometimes wonder if the local inflammation contributes to dry mouth. It does not. Injection site reactions are local immune responses that do not affect salivary gland function. These are separate issues requiring separate management strategies.
Oral and sublingual formulations
The growing availability of oral semaglutide drops, tirzepatide drops, and sublingual semaglutide introduces a unique consideration. These formulations contact oral tissues directly during administration, which can temporarily worsen the sensation of dry mouth immediately after dosing. Some users report a lingering dryness or altered taste that persists for hours after taking oral GLP-1 liquids.
However, the long-term systemic effects on salivary glands are likely similar regardless of administration route. The medication still circulates through the bloodstream and interacts with GLP-1 receptors on salivary tissue. The route simply adds a short-term local component on top of the same systemic effects. SeekPeptides members frequently discuss the differences between oral versus injectable tirzepatide and which route produces more tolerable side effects for their individual situation.
Tracking and measuring your dry mouth
You cannot manage what you do not measure. Tracking dry mouth severity over time helps you identify patterns, evaluate which interventions are working, and provide useful information to your healthcare providers.
The xerostomia inventory
Researchers use a standardized tool called the Xerostomia Inventory to quantify dry mouth severity. While you do not need the full clinical version, adapting its approach is useful. Rate the following on a scale of 1-5 each week:
How dry does your mouth feel overall?
How difficult is swallowing dry foods?
How often do you wake at night due to dry mouth?
How much does dry mouth affect your ability to speak?
How concerned are you about your oral health?
Total scores range from 5 to 25. Track this weekly and note it alongside your dose, any dose changes, and any new management strategies you implemented. Patterns become visible within a few weeks. You might discover that dry mouth correlates with specific days post-injection, with certain foods, or with hydration lapses.
Correlating with other side effects
Track dry mouth alongside other side effects to identify common patterns. If dry mouth worsens on the same days as fatigue or dizziness, dehydration is likely the primary driver and aggressive hydration is your highest-priority intervention. If dry mouth persists even when you are well-hydrated and other side effects have resolved, the salivary gland mechanism is more likely the cause, and saliva substitutes and stimulating products become the priority.
This distinction matters because the two causes respond to different interventions. Treating a hydration problem with saliva substitutes provides only partial relief. Treating a glandular problem with water alone provides even less. The right diagnosis guides the right treatment. SeekPeptides provides comprehensive side effect tracking guidance and protocols that help members identify these patterns faster and respond more effectively.
How GLP-1 dry mouth compares to other medication-induced dry mouth
GLP-1 medications are far from the only drugs that cause dry mouth. Comparing the GLP-1 experience with other well-studied medication classes provides useful context and additional management insights.
Antidepressants and anticholinergics
Anticholinergic medications, including many antidepressants, antihistamines, and bladder medications, cause dry mouth by directly blocking the nerve signals that stimulate saliva production. This mechanism is well understood and produces consistent, often severe dry mouth. GLP-1 dry mouth, by contrast, appears to involve a more complex and variable mechanism that differs between individuals.
The practical implication is that users taking both an anticholinergic medication and a GLP-1 agonist face compounded dry mouth risk. If you take any medication from the anticholinergic class, discuss this combination with your provider. They may be able to switch the anticholinergic to an alternative with less drying effect, reducing the total dry mouth burden.
Blood pressure medications
Diuretics, commonly prescribed for hypertension, reduce total body fluid volume. Combined with GLP-1 medications that reduce fluid intake through appetite suppression, the result can be significant dehydration that manifests as severe dry mouth, lightheadedness, and leg cramps. If you take a diuretic alongside a GLP-1 medication, monitoring your fluid balance becomes doubly important.
ACE inhibitors, another common blood pressure medication class, can cause a persistent dry cough that worsens the subjective sensation of oral dryness. Understanding which of your medications contributes to which symptoms helps you and your provider make targeted adjustments.
What GLP-1 dry mouth research tells us about the future
The growing recognition of GLP-1 related oral side effects is driving new research into targeted solutions. Investigations into biased agonism, where medications are designed to selectively activate beneficial GLP-1 receptor pathways while minimizing those that cause side effects, could eventually produce GLP-1 medications with significantly reduced dry mouth profiles.
In the nearer term, companies are developing oral care products specifically for the GLP-1 medication population. These products aim to provide more effective saliva replacement, longer-lasting oral moisture, and enhanced antimicrobial protection tailored to the specific bacterial shifts that occur during GLP-1 treatment. As the population of long-term GLP-1 users grows into the tens of millions, the market for these solutions will expand accordingly.
For now, the strategies outlined in this guide represent the best available evidence-based approaches. SeekPeptides continues to monitor emerging research and will update recommendations as new evidence becomes available.
Frequently asked questions
Does dry mouth from GLP-1 medications go away on its own?
Many users experience improvement after the first four to six weeks as the body adapts to the medication. However, some experience persistent dry mouth throughout treatment, especially at higher doses. Active management strategies significantly improve outcomes regardless of whether the symptom fully resolves on its own. If dry mouth persists beyond two months, discuss options with your healthcare provider.
Can switching from semaglutide to tirzepatide help with dry mouth?
The reporting-odds ratios for dry mouth are very similar between the two medications (1.34 for semaglutide versus 1.35 for tirzepatide), so switching may not provide significant relief. However, individual responses vary considerably. Some users report different side effect profiles when switching between these medications. Consult your prescriber before making any changes.
Will lowering my GLP-1 dose reduce dry mouth?
In many cases, yes. Dry mouth tends to be dose-dependent, meaning higher doses produce more pronounced symptoms. A microdosing approach may maintain therapeutic benefit while reducing side effect severity. Work with your healthcare provider to find the optimal dose that balances efficacy with tolerability.
Is GLP-1 dry mouth dangerous?
Dry mouth itself is not dangerous, but the downstream effects on oral health can be serious if unmanaged. Reduced saliva increases the risk of tooth decay, gum disease, oral infections, and difficulty swallowing. The damage accumulates over time, so early intervention is important. Maintaining regular dental visits every three to four months while on GLP-1 medications helps catch problems before they become severe.
Can I use regular mouthwash for GLP-1 dry mouth?
Avoid mouthwash containing alcohol, which includes most standard commercial mouthwashes. Alcohol-based mouthwash dries oral tissues further and worsens the problem. Use alcohol-free alternatives like Biotene Dry Mouth Oral Rinse, CloSYS, or ACT Dry Mouth Rinse instead. These products provide antimicrobial protection without contributing to dryness.
Does drinking more water fix GLP-1 dry mouth?
Hydration helps but does not fully resolve dry mouth in most cases. GLP-1 dry mouth involves changes in salivary gland function beyond simple dehydration. Drinking more water addresses the dehydration component but does not reverse receptor desensitization in salivary glands. A combination of hydration, saliva-stimulating products, and protective oral care products provides the most complete relief.
Should I tell my dentist I am taking a GLP-1 medication?
Absolutely. Your dentist needs to know because it changes their approach to your care. They may recommend more frequent cleanings, prescription fluoride treatments, and closer monitoring for early signs of decay. Many dental professionals are now specifically screening for dry mouth and related complications in patients on GLP-1 medications like Ozempic and Mounjaro.
Are oral or sublingual GLP-1 formulations better for dry mouth?
Oral semaglutide drops and sublingual formulations may actually worsen the local sensation of dry mouth because the medication contacts oral tissues directly. However, the systemic effects on salivary glands are likely similar regardless of administration route. Injectable formulations avoid direct oral tissue contact but produce the same downstream effects on saliva production through systemic GLP-1 receptor activation.
External resources
GLP-1 Receptor Signaling and Oral Dysfunction: A Narrative Review (PMC)
Semaglutide-associated hyposalivation: A report of case series (PMC)
For researchers serious about optimizing their peptide protocols and managing side effects effectively, SeekPeptides provides the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. SeekPeptides members access detailed side effect management strategies, expert-reviewed protocols, and personalized support that goes far beyond what any single article can provide.
In case I do not see you, good afternoon, good evening, and good night. May your saliva flow stay strong, your oral health stay protected, and your GLP-1 journey stay comfortable.