Feb 1, 2026

Your training is dialed in. Your diet looks solid on paper. You are in a caloric deficit, lifting heavy, sleeping enough. And yet that stubborn layer of fat across your midsection will not budge. It sits there, quietly mocking every ab exercise and every cardio session you throw at it. Sound familiar?
Here is the uncomfortable truth most fitness content will not tell you. For men, especially those over 30, fat loss becomes a hormonal puzzle more than a caloric math problem. Declining growth hormone levels, shifting testosterone ratios, increasing cortisol from stress and poor sleep, all of these conspire to make your body hold onto fat in the exact places you want to lose it most. The belly. The love handles. The chest.
This is where fat burning peptides enter the conversation. Not as magic bullets. Not as replacements for the work. But as targeted tools that address the specific hormonal and metabolic roadblocks that keep men stuck at frustrating body fat percentages despite doing everything else right.
What follows is a comprehensive breakdown of every fat burning peptide relevant to men. We will cover the mechanisms, the protocols, the stacking strategies, and the honest truth about what works and what does not. Whether you are dealing with visceral belly fat, looking to preserve muscle during a cut, or trying to push past a plateau that has lasted months, this guide covers every angle. SeekPeptides has assembled this information from published research, documented protocols, and community feedback to give you the most complete resource available on the subject.
Why men store fat differently and why it matters for peptide selection
Before choosing a peptide, you need to understand what you are actually fighting. Male fat storage follows specific hormonal patterns that differ significantly from female patterns, and this distinction changes everything about which peptides will work best for you.
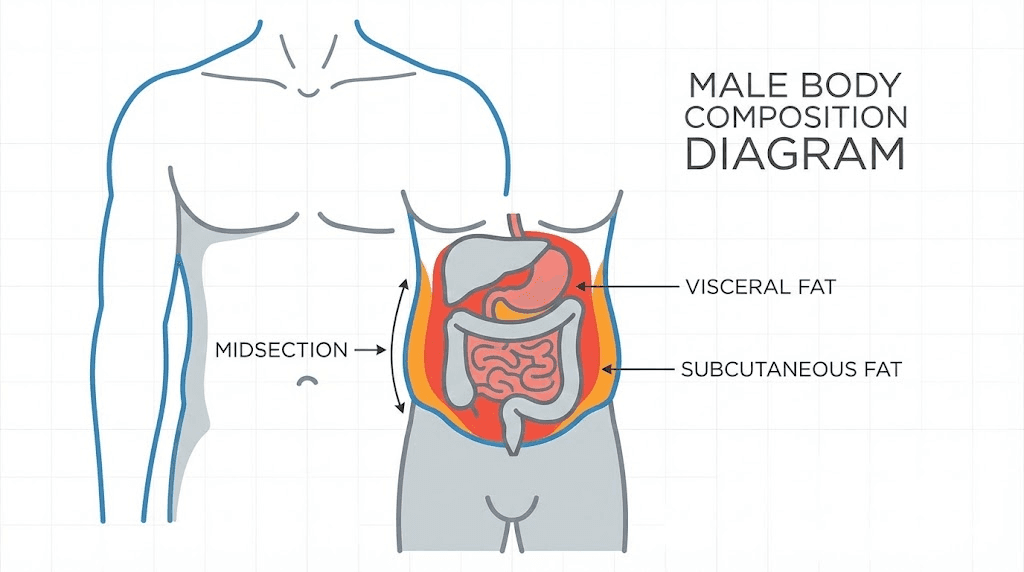
Men predominantly store fat viscerally. This means the fat accumulates around and between your internal organs, deep in the abdominal cavity. It is not the fat you can pinch. It is the fat that pushes your belly outward and creates that hard, distended look. Visceral fat is metabolically active, meaning it releases inflammatory cytokines, disrupts testosterone production, and increases insulin resistance. This creates a vicious cycle. More visceral fat leads to lower testosterone, which leads to more fat storage, which leads to even lower testosterone.
Subcutaneous fat, the kind you can pinch on your love handles and lower back, follows different rules. This fat responds more directly to caloric deficits and exercise. Visceral fat, however, responds more to hormonal optimization. This is a critical distinction.
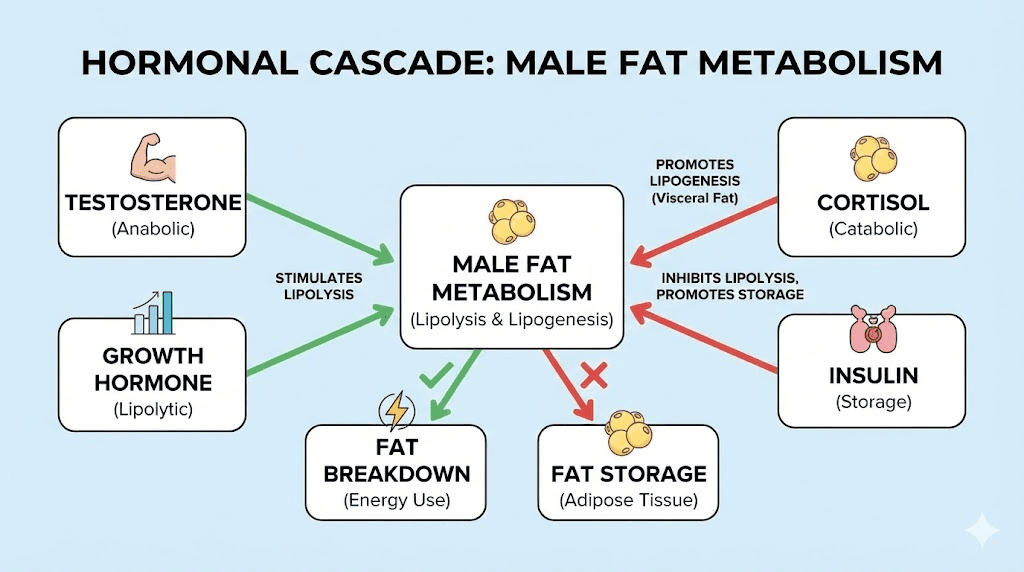
Growth hormone plays a central role in male fat metabolism. GH directly stimulates lipolysis, the process of breaking stored fat into free fatty acids that can be burned for energy. In men, GH levels peak in the late teens and early twenties, then decline roughly 14% per decade. By age 40, most men are producing less than half the growth hormone they did at 20. By 60, some men produce barely measurable amounts.
This is why muscle building gets harder with age. And why fat loss becomes exponentially more difficult despite maintaining the same diet and exercise habits that kept you lean in your twenties. The hormonal environment has fundamentally changed.
Insulin sensitivity also plays a massive role. Men with higher visceral fat develop progressive insulin resistance, meaning their cells stop responding efficiently to insulin signals. The body compensates by producing more insulin, and elevated insulin is one of the most potent signals for fat storage. It literally locks fat inside your cells and prevents its release. No amount of cardio will override this biochemical lock if insulin remains chronically elevated.
Understanding these mechanisms is not academic. It directly informs which fat burning peptides will actually move the needle for you. A peptide that boosts growth hormone will address the lipolysis problem. A GLP-1 agonist will address the insulin and appetite problem. A mitochondrial peptide will address the cellular energy problem. The right choice depends on where your specific bottleneck lies.
The complete ranking of fat burning peptides for men
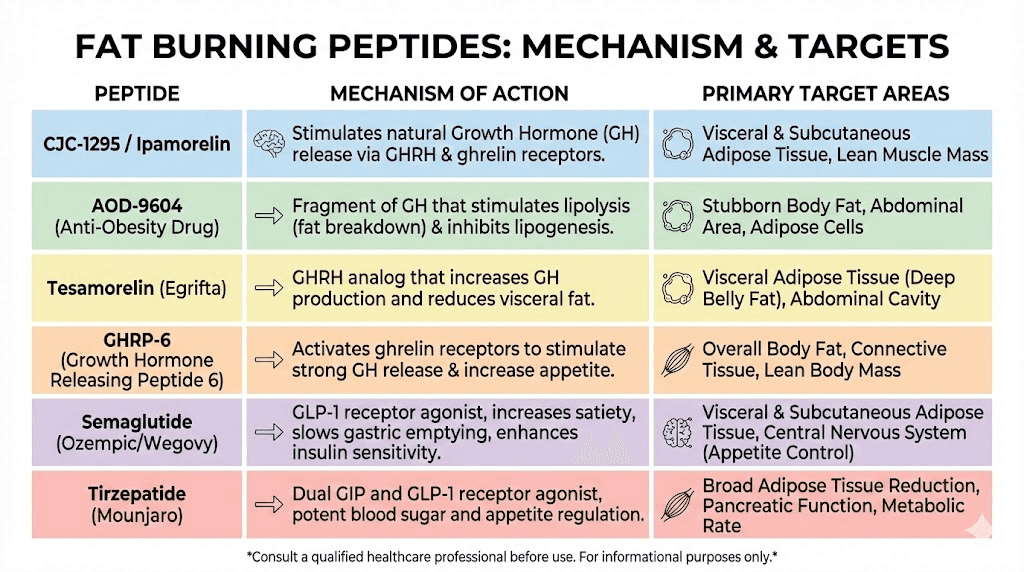
Not all fat burning peptides work the same way. Some target growth hormone pathways. Others address appetite and insulin. A few work at the mitochondrial level to change how your cells process energy. Here is every peptide worth considering, ranked by the strength of evidence and real-world results for male fat loss.
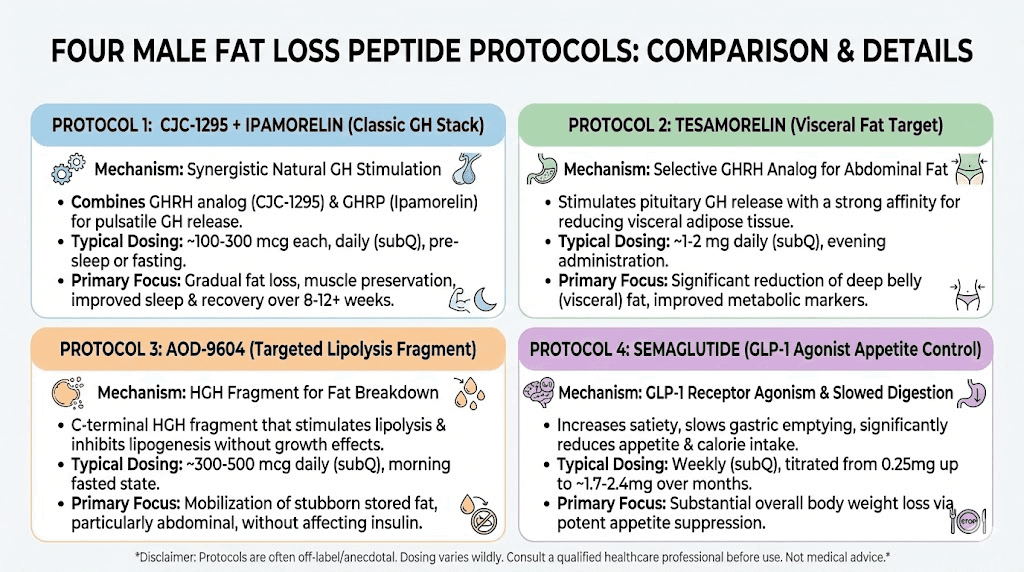
Tesamorelin: the visceral fat specialist
If there is one peptide specifically designed for male belly fat, tesamorelin is it. This growth hormone releasing hormone analog has the strongest clinical evidence of any peptide for visceral fat reduction, with actual FDA approval for reducing excess abdominal fat in HIV patients with lipodystrophy.
The mechanism is straightforward. Tesamorelin stimulates the pituitary gland to release growth hormone in a physiologically natural pattern. This elevated GH then triggers increased production of IGF-1, which directly promotes lipolysis in visceral fat tissue. Clinical studies show an average 18% reduction in visceral fat without significant changes to subcutaneous fat, making it uniquely targeted.
For men, tesamorelin offers several specific advantages. It does not suppress your natural GH production the way exogenous growth hormone does. It works with your body, amplifying existing signals rather than replacing them. Research subjects also showed improvements in body composition including increased lean mass alongside the fat reduction.
Side effects tend to be mild. Some men report flu-like symptoms early in the protocol, particularly fatigue and mild nausea. Joint stiffness is possible due to increased GH activity, and injection site reactions are common but manageable. These effects typically resolve within the first two weeks.
Tesamorelin is especially effective for men over 40 dealing with that stubborn visceral fat accumulation that seems resistant to diet and exercise. If your waist circumference keeps increasing despite consistent training, this is often the first peptide worth investigating. The peptide calculator can help determine appropriate dosing based on your individual parameters.
CJC-1295 and ipamorelin: the gold standard stack
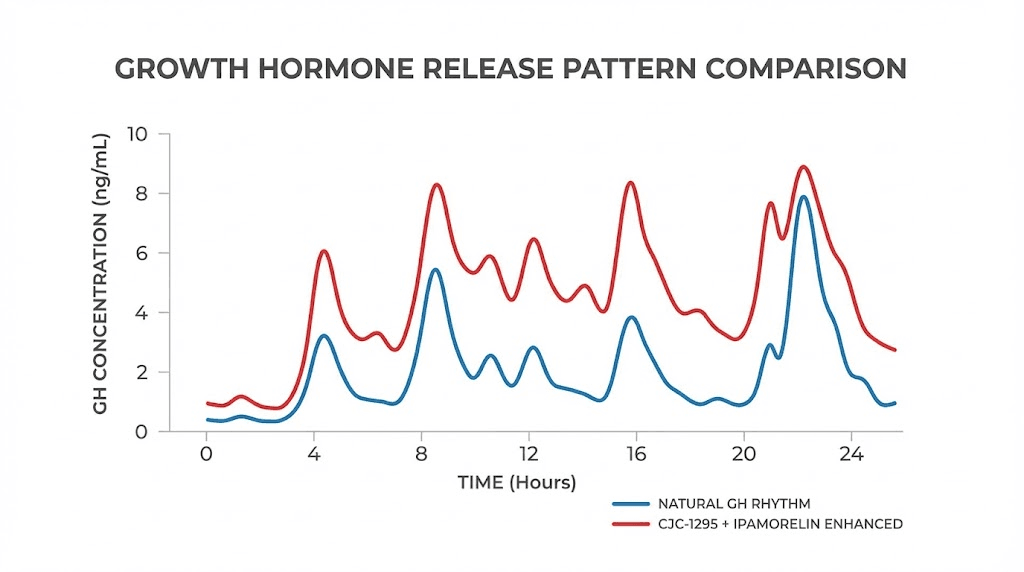
This combination has earned its reputation as the most popular fat loss peptide stack for men, and for good reason. CJC-1295 provides sustained growth hormone elevation while ipamorelin delivers precise, pulsatile releases that closely mimic your body natural GH patterns.
CJC-1295 is a growth hormone releasing hormone analog with a half-life of approximately 6 to 8 days when combined with DAC (Drug Affinity Complex). This extended half-life means sustained elevation of GH levels rather than the sharp spike-and-crash pattern seen with direct GH administration. The result is more consistent fat oxidation throughout the day and night.
Ipamorelin is a selective growth hormone secretagogue that stimulates GH release without significantly affecting cortisol or prolactin levels. This selectivity is important for men because elevated cortisol directly promotes visceral fat storage, and elevated prolactin can suppress testosterone. Other GH releasing peptides like GHRP-6 and GHRP-2 stimulate hunger and affect cortisol, making them less ideal for pure fat loss goals.
Together, CJC-1295 and ipamorelin create a synergistic effect. CJC-1295 amplifies the amplitude of each GH pulse while ipamorelin controls the timing and frequency. The combination typically elevates GH levels 2 to 10 times above baseline, depending on dosing.
Common protocols involve subcutaneous injection at 100mcg of each peptide, administered before bed on an empty stomach. The CJC-1295 dosage calculator provides precise measurements. Many men follow a 5 days on, 2 days off weekly schedule to prevent receptor desensitization, with cycle planning typically running 8 to 12 weeks followed by a 4 to 6 week break.
Results typically appear as improved sleep quality within the first week, increased energy and recovery by week two, and visible body composition changes starting around week 6. The fat loss effect is gradual but cumulative, with most men reporting the most dramatic changes between weeks 8 and 16 of consistent use.
For detailed information on ipamorelin specifically, the ipamorelin benefits guide covers the full spectrum of effects beyond fat loss, including improved sleep, recovery, and skin quality. Understanding the ipamorelin side effects profile is also essential before starting any protocol.
AOD-9604: the targeted fat fragment
AOD-9604 takes a different approach. Rather than stimulating growth hormone release, this peptide is actually a modified fragment of the growth hormone molecule itself, specifically amino acids 177 through 191 of the human GH sequence.
What makes AOD-9604 unique is what it does not do. It stimulates fat breakdown without affecting blood sugar levels, muscle mass, or insulin sensitivity. This is significant for men who may have prediabetic tendencies or insulin resistance, as many GH-based therapies can temporarily worsen glucose control. AOD-9604 skips that problem entirely.
An Australian clinical study involving 300 obese subjects found that the group receiving 1mg daily lost an average of 2.8 kilograms over 12 weeks, more than three times the weight lost by placebo. The study also showed modest improvements in cholesterol levels. The complete AOD-9604 guide breaks down these findings in detail.
AOD-9604 specifically targets areas heavy with unwanted fat, particularly the abdominal region and thighs. The mechanism involves stimulating lipolysis while simultaneously inhibiting lipogenesis, the formation of new fat. This dual action makes it particularly effective for men who are in a caloric deficit but still struggling with stubborn fat deposits.
Side effects are minimal. The most common complaint is injection site irritation. Because AOD-9604 does not affect the growth hormone axis as a whole, it avoids the joint pain, water retention, and insulin effects associated with full GH elevation. The AOD-9604 side effects profile remains one of the cleanest among all fat loss peptides.
The AOD-9604 dosage guide recommends morning administration on an empty stomach for optimal absorption and fat mobilization throughout the day.
Semaglutide: the appetite and insulin game-changer
Semaglutide deserves its own section because its mechanism of action is fundamentally different from every other peptide on this list. While the GH-based peptides work on the fat burning side of the equation, semaglutide works on the energy intake side by mimicking GLP-1, a hormone that controls appetite, insulin secretion, and gastric emptying.
Clinical trials show average weight loss of 14.9% of body weight over 68 weeks. For a 200-pound man, that translates to roughly 30 pounds. The semaglutide dosage calculator helps determine appropriate starting doses and titration schedules.
How does it work? Semaglutide activates GLP-1 receptors in the brain that regulate hunger signals. Users consistently report a dramatic reduction in food noise, that constant background chatter about what to eat next. Meals become smaller because satiety arrives faster. Cravings, particularly for high-calorie processed foods, diminish substantially.
For men specifically, semaglutide addresses a common fat loss obstacle: portion control. Many men who train hard also eat hard. The appetite reduction from semaglutide creates a natural caloric deficit without the mental warfare of constant restriction. The comprehensive weight loss peptide guide compares semaglutide against every other option in detail.
The semaglutide versus tirzepatide comparison is worth reviewing because tirzepatide, a dual GLP-1/GIP agonist, shows even greater weight loss results at 20.2% average body weight reduction. Tirzepatide activates two metabolic pathways simultaneously, making it potentially more effective but also newer with less long-term safety data.
Side effects include nausea, particularly during dose escalation, constipation, and potential muscle loss if protein intake is not maintained. For men combining semaglutide with resistance training, the research published in our peptides to combine with Ozempic article provides strategies to preserve lean mass during GLP-1 treatment.
MOTS-c: the mitochondrial metabolic enhancer
MOTS-c represents a newer class of peptide that works at the cellular energy level rather than through hormonal pathways. Encoded by mitochondrial DNA, this 16-amino acid peptide activates AMPK, the master switch of cellular energy metabolism.
Think of AMPK as your cells internal fuel gauge. When AMPK is activated, cells shift from storing energy to burning it. Specifically, MOTS-c drives fatty acid oxidation, meaning your cells preferentially burn fat for fuel rather than storing it. This effect is particularly pronounced in visceral fat tissue, liver cells, and skeletal muscle.
For men, MOTS-c offers something unique. It does not suppress appetite. It does not cause nausea. It does not affect growth hormone or testosterone. Instead, it changes the fundamental way your cells process energy at the mitochondrial level. The MOTS-c benefits guide covers the full range of metabolic effects.
Common protocols run 5 to 15mg per week, split across 2 to 3 administrations. Many researchers stack MOTS-c with GH secretagogues for a multi-pathway approach to fat loss. Because MOTS-c works through an entirely different mechanism than CJC-1295/ipamorelin or tesamorelin, the effects stack additively without competing for the same receptors.
The MOTS-c dosage chart provides weight-based calculations for precise administration. Side effects are generally mild and rare, as MOTS-c is naturally produced by your own mitochondria. The MOTS-c side effects profile confirms its favorable safety record in early human and animal studies.
5-amino-1MQ: the oral fat loss option
Most fat burning peptides require subcutaneous injection. 5-amino-1MQ stands out as an oral option, which makes it appealing to men who prefer to avoid needles entirely.
This small molecule works by inhibiting NNMT, an enzyme called nicotinamide N-methyltransferase. NNMT is overactive in individuals with excess abdominal fat and metabolic dysfunction. By blocking NNMT, 5-amino-1MQ boosts intracellular NAD+, a coenzyme essential for energy production, DNA repair, and mitochondrial function. Higher NAD+ levels promote fat oxidation and improve metabolic efficiency.
Anecdotal reports are promising. One documented case involved a 38-year-old male on TRT and MK-677 who added 10mg daily of injectable 5-amino-1MQ. After four weeks with no changes to macros or training, bioimpedance scanning showed 6.3 pounds of fat loss and 1.1 pounds of lean mass gain simultaneously. The complete 5-amino-1MQ guide examines all available evidence.
Typical oral dosing ranges from 50mg one to three times daily, taken with meals. Unlike continuous-use peptides, 5-amino-1MQ works best when cycled. Effects tend to diminish after 4 to 6 weeks of daily use, so strategic breaks are recommended to reset the body responsiveness.
The appeal for men is obvious. No injections. Oral administration. Minimal side effects. Visible results within 10 to 14 days for many users. The trade-off is that human clinical data remains limited, and the peptide safety considerations apply especially to newer compounds like this one.
Sermorelin: the natural GH restorer
Sermorelin is one of the oldest and most studied growth hormone releasing peptides. It mimics GHRH (growth hormone releasing hormone) to stimulate your pituitary gland to produce and release more natural GH. The key word is natural. Unlike exogenous growth hormone, sermorelin preserves the pulsatile pattern of GH release that your body relies on for optimal fat metabolism.
For men experiencing age-related GH decline, sermorelin essentially turns back the clock on growth hormone production. Studies show that men treated with sermorelin experience reduced waist circumference, improved strength, and elevated quality of life metrics. The sermorelin benefits guide provides a detailed analysis of all documented effects.
Sermorelin is particularly well-suited for men who want a conservative, well-studied approach to GH optimization. It has decades of clinical use behind it, a well-understood side effect profile, and reliable results. The sermorelin before and after results show typical timelines and outcomes.
The downside compared to newer peptides like CJC-1295/ipamorelin is that sermorelin has a very short half-life, approximately 10 to 20 minutes. This means the GH elevation is more brief and requires more frequent dosing. Many protocols call for nightly injections before bed to align with the natural GH release during deep sleep.
For men considering the cost of various approaches, the sermorelin cost guide breaks down pricing across different sources and formats. The sermorelin and ipamorelin blend guide explores how combining sermorelin with ipamorelin can provide both the sustained and pulsatile GH patterns simultaneously.
Retatrutide: the triple agonist with unprecedented results
Retatrutide is the newest entry in the fat loss peptide landscape, and the clinical trial results are staggering. As a triple agonist targeting GLP-1, GIP, and glucagon receptors simultaneously, retatrutide produced average weight loss of 24% of body weight in trials, with the highest dose (12mg weekly) showing 28.7% average reduction over 68 weeks.
To put that in perspective, a 220-pound man could potentially lose 63 pounds. And 23.7% of subjects in the trial achieved weight loss exceeding 35% of body weight, the highest numbers ever recorded in any obesity trial.
The triple mechanism works through complementary pathways. GLP-1 reduces appetite and slows gastric emptying. GIP enhances insulin sensitivity and fat metabolism. Glucagon receptor activation directly promotes hepatic fat oxidation and energy expenditure. Together, these three pathways create a more comprehensive metabolic shift than any single or dual agonist can achieve.
Retatrutide is not yet FDA approved, with approval expected no earlier than mid-2026. The retatrutide dosage chart provides the protocol information from clinical trials. The retatrutide 20mg dosing guide covers the higher dose protocols that showed maximum efficacy. The ZLZ peptide retatrutide overview explains its relationship to the broader class of incretin therapies.
For men who have tried GLP-1 monotherapy (semaglutide) without adequate results, retatrutide represents the next evolution. The additional glucagon receptor activation is particularly relevant for men because glucagon directly promotes visceral fat breakdown, addressing the specific type of fat that plagues male physiology.
MK-677 (ibutamoren): the oral growth hormone secretagogue
MK-677 is technically not a peptide but a growth hormone secretagogue that mimics ghrelin signaling to stimulate GH and IGF-1 release. It is included here because it is frequently discussed alongside fat burning peptides and offers an oral alternative to injectable GH secretagogues.
The appeal is simple. Oral administration, significant GH elevation (comparable to injectable options), and documented effects on body composition. Studies in healthy older men showed meaningful improvements in lean mass and strength over six months of use.
The catch. MK-677 stimulates appetite significantly due to its ghrelin-mimetic properties. This can directly undermine fat loss goals if caloric intake is not carefully controlled. For men using MK-677 specifically for fat loss, strict dietary discipline becomes even more important.
MK-677 also increases water retention, which can mask fat loss on the scale. Many men see the number go up initially and assume the peptide is not working, when in reality they are losing fat while gaining water weight. Body measurements and visual progress tracking become essential.
The combination of appetite stimulation and water retention makes MK-677 better suited for body recomposition (gaining muscle while slowly losing fat) rather than aggressive cutting phases. For men in a significant caloric deficit, the injectable options like CJC-1295/ipamorelin provide similar GH benefits without the appetite increase.
Cagrilintide: the emerging amylin analog
Cagrilintide mimics amylin, a hormone co-released with insulin from pancreatic beta cells. Amylin slows gastric emptying, reduces glucagon secretion, and promotes satiety through direct CNS signaling. For men dealing with both excess fat and blood sugar control issues, cagrilintide addresses both simultaneously.
The cagrilintide weight loss profile shows meaningful fat reduction when used alone, but the real power emerges in combination with semaglutide. The cagrilintide and semaglutide combination, marketed as CagriSema, targets three distinct satiety pathways simultaneously and has shown weight loss results approaching retatrutide levels.
For men, cagrilintide is particularly interesting because amylin signaling appears to preferentially reduce visceral fat. The cagrilintide for men guide examines the male-specific data in detail, while the cagrilintide dosing protocols provide the clinical framework.
How male hormones affect peptide effectiveness
Peptides do not work in a vacuum. Their effectiveness depends heavily on your existing hormonal environment, and for men, three hormones dictate how well any fat burning peptide will perform.
Testosterone: the foundation
Low testosterone creates a metabolic environment that actively resists fat loss. Testosterone promotes protein synthesis, maintains lean mass, and directly influences fat distribution patterns. Men with clinically low testosterone (below 300 ng/dL) will get reduced results from any fat burning peptide because the hormonal foundation is compromised.
This does not mean you need TRT before starting peptides. But it means awareness of your testosterone levels can explain why results vary between individuals. The peptides versus TRT comparison breaks down when each approach makes more sense. The testosterone-focused peptide guide covers specific options for men looking to address both T levels and fat loss simultaneously.
Some peptides indirectly support testosterone. Elevated GH from CJC-1295/ipamorelin or tesamorelin can improve testicular function. Reduced visceral fat from any effective protocol removes an aromatase-rich tissue (visceral fat converts testosterone to estrogen), naturally allowing testosterone levels to recover. The enclomiphene guide covers a more direct approach to testosterone support.
Cortisol: the fat storage signal
Chronically elevated cortisol tells your body to store fat viscerally. Period. Men under high stress, poor sleep, or excessive training volume often have cortisol levels that actively counteract their fat burning efforts. This is why some men train harder, eat less, and actually get fatter. The cortisol is winning.
Peptide selection matters here. Ipamorelin is preferred over GHRP-6 or GHRP-2 specifically because it does not elevate cortisol. Anxiety-reducing peptides like selank and semax can indirectly support fat loss by lowering cortisol. The DSIP peptide, which promotes deep sleep, addresses another major cortisol driver, since poor sleep is one of the most potent cortisol elevators.
Insulin: the gatekeeper
Elevated fasting insulin keeps fat locked in storage. No peptide will override this signal completely. GLP-1 agonists like semaglutide directly improve insulin sensitivity and reduce fasting insulin levels. GH-based peptides can temporarily worsen insulin sensitivity, which is why fasting protocols around injection timing matter. AOD-9604 sidesteps the insulin question entirely by not affecting glucose metabolism.
Men with elevated C-peptide levels (a marker of insulin production) may benefit more from GLP-1 based approaches than GH based approaches. Understanding your metabolic profile helps determine which peptide pathway will produce the best results for your specific situation.
Fat burning peptide stacks for men: protocols by goal
Single peptides produce results. Stacking multiple peptides that work through different pathways produces significantly better results. Here are the most effective stacking protocols organized by specific male fat loss goals.
Protocol 1: aggressive visceral fat reduction
Goal: Maximum visceral belly fat reduction in 12 weeks
Stack:
Tesamorelin: 2mg subcutaneous injection nightly before bed
AOD-9604: 300mcg subcutaneous injection each morning on empty stomach
MOTS-c: 10mg split into 2 weekly administrations (Monday and Thursday)
Why this works: Tesamorelin drives GH-mediated visceral fat lipolysis overnight. AOD-9604 targets fat breakdown during daytime fasting windows without affecting insulin. MOTS-c enhances cellular fat oxidation at the mitochondrial level. Three different mechanisms, three different pathways, no receptor competition.
Schedule: 5 days on, 2 days off for tesamorelin and AOD-9604. MOTS-c administered on consistent days regardless. The peptide cycling guide explains how to coordinate multiple compounds.
Expected timeline:
Week 1 to 2: Improved sleep quality, increased morning energy
Week 3 to 4: Noticeable reduction in abdominal bloating
Week 6 to 8: Measurable reduction in waist circumference (typically 1 to 3 inches)
Week 10 to 12: Significant visible changes in abdominal composition
Important: This protocol assumes concurrent caloric deficit of 300 to 500 calories, resistance training 3 to 5 times weekly, and 7 to 8 hours of quality sleep. Peptides amplify the work. They do not replace it.
Protocol 2: body recomposition (lose fat, gain muscle)
Goal: Simultaneous fat loss and muscle gain over 16 weeks
Stack:
CJC-1295 (no DAC): 100mcg before bed nightly
Ipamorelin: 100mcg before bed nightly (combined with CJC-1295)
5-amino-1MQ: 50mg oral twice daily with meals (weeks 1 through 6, then 2 weeks off, repeat)
Why this works: CJC-1295/ipamorelin elevates GH and IGF-1, promoting both lipolysis and protein synthesis simultaneously. The increased GH supports muscle recovery and growth while mobilizing fat stores. 5-amino-1MQ adds mitochondrial support through NAD+ elevation, enhancing the body ability to partition nutrients toward muscle and away from fat storage.
Nutrition: Maintenance calories or slight deficit (100 to 200 calories below maintenance). High protein intake at 1g per pound of bodyweight minimum. The caloric deficit should come from carbohydrate reduction, not protein. The peptide stacking guide provides additional combination strategies.
Expected timeline:
Week 1 to 3: Better sleep, faster recovery between training sessions
Week 4 to 6: Strength increases despite caloric restriction
Week 8 to 12: Visible muscle definition improvement with simultaneous fat loss
Week 12 to 16: Noticeable body composition transformation
For men interested in maximizing the muscle growth benefits alongside fat loss, the strength protocol guide provides complementary training recommendations.
Protocol 3: maximum weight loss with appetite control
Goal: Significant total weight loss (20+ pounds) over 6 months
Stack:
Semaglutide: Weekly subcutaneous injection, titrated from 0.25mg to 2.4mg over 16 weeks
CJC-1295/ipamorelin: 100mcg/100mcg nightly before bed (to preserve muscle during caloric deficit)
Why this works: Semaglutide creates the caloric deficit through appetite reduction and improved insulin sensitivity. CJC-1295/ipamorelin preserves lean mass that would otherwise be lost during significant weight reduction. This combination addresses the biggest complaint about GLP-1 monotherapy, which is muscle loss alongside fat loss.
The best peptide stack for weight loss article compares this protocol against alternatives. For men considering the alternatives to Ozempic, peptide combinations can sometimes provide comparable results with different side effect profiles.
Expected timeline:
Month 1: 4 to 8 pounds lost, primarily appetite-driven deficit
Month 2 to 3: 2 to 4 pounds per week sustained loss
Month 4 to 6: Continued loss with improved body composition from muscle preservation
Protocol 4: the over-40 male optimization stack
Goal: Address age-related metabolic slowdown and body composition changes
Stack:
Tesamorelin: 2mg nightly before bed
CJC-1295/ipamorelin: 100mcg/100mcg nightly (can be combined in same injection as tesamorelin)
MOTS-c: 10mg weekly
Why this works: After 40, GH decline accelerates and mitochondrial function degrades. This triple approach restores GH signaling through two pathways (tesamorelin for sustained release, ipamorelin for pulsatile release) while MOTS-c addresses the mitochondrial energy production deficit that contributes to the sluggish metabolism many men experience in their forties and beyond.
The longevity peptides guide covers the broader anti-aging benefits of this stack beyond fat loss. Many men using this combination report improvements in sleep, mood, cognitive function, and recovery that go well beyond body composition changes.
Use the peptide stack calculator to determine precise amounts for multi-peptide protocols and the reconstitution calculator to prepare each vial correctly.
Injection protocols and practical considerations for men
Knowing which peptides to use means nothing if the execution is wrong. Improper reconstitution, bad timing, incorrect storage, all of these can render expensive peptides useless. Here are the practical details that separate successful protocols from wasted money.
Reconstitution basics
Most fat burning peptides come as lyophilized (freeze-dried) powder in sealed vials. Before use, they must be reconstituted with bacteriostatic water. The process is straightforward but requires attention to detail.
The complete reconstitution guide walks through every step. The bacteriostatic water guide explains why this specific water type is necessary (the benzyl alcohol preservative prevents bacterial growth in the vial). The mixing guide covers common mistakes to avoid.
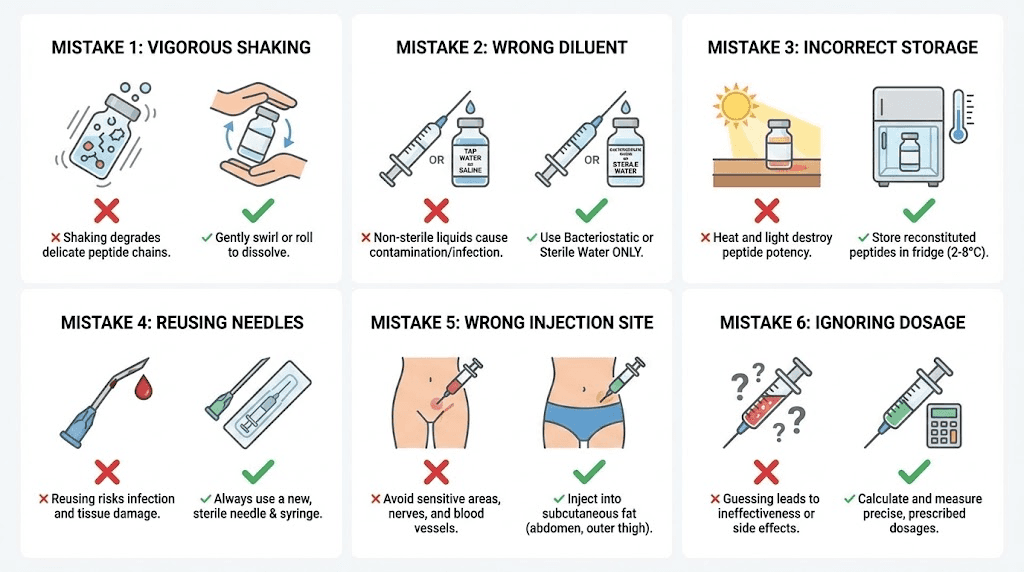
Critical rules: Never shake the vial. Let the water run down the side of the glass and allow the powder to dissolve naturally. Direct streams of water onto lyophilized powder can denature the peptide. Store reconstituted peptides in the refrigerator and use within 4 to 6 weeks. The reconstituted peptide shelf life guide provides storage timelines for each specific peptide.
For dosing calculations, the dosage calculation guide explains the math behind converting milligrams to micrograms and determining how many units to draw in an insulin syringe based on the reconstitution ratio. The peptide dosage calculator does the math automatically.
Timing and fasting
GH-based peptides (CJC-1295, ipamorelin, tesamorelin, sermorelin) should be administered on an empty stomach. Food, particularly carbohydrates and fats, blunts growth hormone release significantly. The optimal approach is injection at least 2 hours after your last meal, with most men choosing bedtime administration.
Why bedtime? Your body naturally produces the largest GH pulse during deep sleep, approximately 30 to 60 minutes after falling asleep. Injecting GH secretagogues just before bed amplifies this natural pulse rather than fighting against it. The synchronized approach produces better results than random timing throughout the day.
AOD-9604 follows different rules. Morning administration on an empty stomach is preferred because AOD-9604 promotes fat mobilization, and morning dosing allows fat to be utilized as fuel during daytime activity. Some men inject immediately upon waking, then wait 30 to 45 minutes before eating breakfast.
GLP-1 agonists like semaglutide are dosed weekly and are not timing-sensitive relative to meals. Pick a consistent day and time, and stick with it. The peptide dosing guide covers timing for every major peptide.
Injection sites and rotation
Subcutaneous injections go into the fatty layer just beneath the skin. For men, the most common sites are the lower abdomen (at least 2 inches from the navel), the front of the thigh, and the back of the upper arm. Rotate injection sites to prevent tissue irritation and ensure consistent absorption.
The peptide injection fundamentals guide covers proper technique. The detailed injection guide includes site rotation maps and troubleshooting for common issues like bruising, lumps, and redness.
For men who want to avoid injections entirely, options exist. 5-amino-1MQ is oral. Nasal spray peptides offer another non-injection route for certain compounds. Peptide capsules are available for some formulations, though bioavailability is generally lower than injectable forms.
Storage and stability
Unreconstituted lyophilized peptides should be stored in the freezer for long-term storage or the refrigerator for short-term storage. The peptide storage guide provides temperature ranges and shelf life expectations for each compound.
Once reconstituted, all peptides must be refrigerated at 36 to 46 degrees Fahrenheit. Never freeze reconstituted peptides, as ice crystal formation destroys the molecular structure. The fridge storage timeline guide and powder form shelf life guide provide specific durations for each peptide. The room temperature stability guide covers what happens if your peptides accidentally spend time outside the refrigerator.
Cycling and long-term protocol management
Continuous peptide use without breaks leads to receptor desensitization. Your body adapts. The receptors that respond to peptide signaling downregulate, meaning the same dose produces progressively weaker effects. Smart cycling prevents this problem entirely.
Weekly cycling: 5 on, 2 off
The most common approach for GH secretagogues. Inject Monday through Friday, rest Saturday and Sunday. This gives receptors enough recovery time to maintain sensitivity while providing consistent stimulation during the work week. Most men find this schedule easy to maintain because it aligns with their weekly routine.
Block cycling: 8 to 12 weeks on, 4 to 6 weeks off
For longer-term protocols, block cycling provides a more complete receptor reset. Run your stack for 8 to 12 weeks at full dose, then discontinue all peptides for 4 to 6 weeks. During the off period, your receptors fully resensitize, and the next cycle produces results comparable to the first.
The peptide cycle planning guide provides detailed frameworks for both approaches. The cycling different peptides guide explains how to rotate between different compounds across cycles for continued progress.
Monitoring during cycles
Smart protocols include blood work. At minimum, check the following before starting and at the midpoint of each cycle:
IGF-1 levels: Confirms GH secretagogues are working. Target range is 200 to 300 ng/mL for most men
Fasting glucose and insulin: GH elevation can temporarily increase blood sugar. Monitor to ensure you stay in healthy ranges
Testosterone (total and free): Ensure fat loss is improving, not worsening, your T levels
Thyroid panel: GH can affect thyroid conversion. Monitor T3 and T4
Cortisol: Elevated cortisol will counteract fat burning effects
The peptide research guide covers the clinical markers most relevant to fat loss protocols.
Nutrition and training to maximize peptide fat loss
Peptides are tools. Powerful tools. But they work with your lifestyle, not instead of it. Men who combine the right peptides with optimized nutrition and training see dramatically better results than those who use peptides alone.
Nutrition principles for men on fat burning peptides
Protein first. Aim for 1 to 1.2 grams per pound of bodyweight. This is non-negotiable when using GH secretagogues because elevated GH increases protein synthesis capacity. If you do not provide enough protein, the anabolic signal goes to waste. For men on GLP-1 agonists, high protein intake is even more critical because reduced appetite makes it easy to under-eat protein.
Caloric deficit should be moderate. 300 to 500 calories below maintenance is sufficient when peptides are doing their job. Aggressive deficits (1000+ calories) trigger cortisol elevation and metabolic adaptation that can counteract peptide benefits. The peptides create the metabolic conditions for fat loss. A moderate deficit provides the trigger.
Carbohydrate timing matters. Keep the 2 to 3 hours before GH secretagogue injections low-carb or carb-free. Elevated blood sugar and insulin blunt GH release. Many men on evening injection protocols simply cut carbs after dinner, injecting 2 to 3 hours later before bed. This naturally creates a low-insulin window for maximum GH release.
Fats should come from quality sources. Omega-3 fatty acids, found in fish oil and fatty fish, directly support anti-inflammatory pathways that synergize with peptide mechanisms. Avoid trans fats and excessive omega-6 consumption, both of which promote the inflammatory environment that visceral fat creates.
Training principles for men on fat burning peptides
Resistance training is mandatory. Not optional. Not secondary. Mandatory. Elevated GH and IGF-1 from peptides create an enhanced anabolic environment. Weight training provides the stimulus that directs these hormones toward muscle preservation and growth rather than other tissues.
Compound movements deliver the most synergy with peptide protocols. Squats, deadlifts, bench press, rows, overhead press. These movements create the largest acute hormonal response and recruit the most muscle tissue. The combination of training-induced GH release plus peptide-induced GH release creates a multiplicative effect on both fat loss and muscle preservation.
Cardio should be strategic, not excessive. Low-intensity steady-state cardio (walking, cycling at conversational pace) promotes fat oxidation without significantly elevating cortisol. High-intensity interval training (HIIT) creates acute GH spikes but can elevate cortisol if overdone. Two to three HIIT sessions per week is the upper limit for most men on peptide protocols. More than that risks cortisol-driven fat storage that counteracts the peptides.
The performance peptide guide covers specific compounds that enhance training output alongside fat burning peptides. For men interested in the joint support benefits that can keep training consistent, peptides like BPC-157 and TB-500 play a complementary role.
Common mistakes men make with fat burning peptides
After reviewing thousands of community reports and protocol logs, certain patterns emerge. These are the most common reasons men fail to get results from fat burning peptides, along with how to fix each one.
Mistake 1: expecting peptides to override a bad diet
No peptide will produce visible fat loss if you are eating 500 calories above maintenance. Even semaglutide, the strongest appetite suppressant available, can be overridden by conscious overeating. Peptides optimize the process. They do not replace the caloric deficit.
Mistake 2: wrong timing around meals
Injecting CJC-1295/ipamorelin 30 minutes after eating a carb-heavy meal is one of the most common protocol errors. The insulin spike from the meal directly suppresses GH release. You get maybe 20% of the GH response you would have gotten on an empty stomach. Two to three hours fasted before injection is the minimum.
Mistake 3: inconsistent dosing
Peptides work through accumulated signaling over time. Missing two or three injections per week dramatically reduces their effectiveness. This is especially true for GH secretagogues, where consistent nightly dosing builds a sustained elevation in IGF-1. Sporadic use never allows IGF-1 levels to reach the threshold needed for meaningful fat mobilization.
Mistake 4: never cycling off
Men who run peptides continuously for 6 or more months without a break almost universally report diminishing returns. Receptor desensitization is real. The 4 to 6 week break every 8 to 12 weeks is not optional. It is what keeps the peptides working long-term. The guide to combining multiple peptides addresses cycling schedules for complex stacks.
Mistake 5: poor peptide quality
The peptide market has quality issues. Underdosed vials, contaminated product, and outright fakes exist. Men who buy the cheapest option available often get exactly what they pay for. Nothing. The peptide testing labs guide explains how to verify purity through third-party testing. The peptide vial research guide covers what to look for when evaluating sources.
Choosing reliable sources is critical. The vendor evaluation guide provides frameworks for assessing quality, transparency, and reliability before purchasing. The grey market peptides guide explains the regulatory landscape and how to navigate it safely.
Mistake 6: ignoring sleep
Sleep is not a nice-to-have when using GH secretagogues. It is the primary environment in which these peptides work. 70 to 80% of daily GH secretion occurs during deep sleep. Men who sleep 5 to 6 hours are literally cutting the window in which their peptides produce results. Seven to eight hours minimum, with consistent sleep and wake times, is foundational to protocol success.
Peptides that directly support sleep quality, like DSIP and pinealon, can complement fat burning protocols by ensuring the sleep environment optimizes GH release.
Peptide fat loss compared to other approaches for men
Men considering fat burning peptides are usually comparing them against other tools they have heard about. Here is how peptides stack up against the most common alternatives.
Peptides versus steroids for fat loss
Anabolic steroids can produce dramatic body composition changes, but the mechanisms and risks are fundamentally different. Steroids directly replace or supplement testosterone and other androgens, causing both muscle growth and indirect fat loss through increased metabolic rate and nutrient partitioning.
Peptides, by contrast, work through signaling. They tell your body to produce more of its own hormones rather than replacing them externally. This means less shutdown of natural hormone production and fewer long-term endocrine disruptions. The peptides versus steroids comparison provides a thorough analysis of both approaches.
Peptides versus SARMs for fat loss
SARMs (Selective Androgen Receptor Modulators) target muscle and bone tissue with less impact on prostate and other androgen-sensitive organs compared to traditional steroids. For fat loss specifically, SARMs provide minimal direct benefit. Their primary mechanism is muscle preservation and growth, which indirectly supports metabolic rate.
Peptides offer more direct fat loss mechanisms through GH elevation, appetite control, and metabolic enhancement. The peptides versus SARMs comparison and the detailed comparison page cover both the efficacy and safety differences.
Peptides versus natural supplements
Fat burner supplements (caffeine, green tea extract, L-carnitine, yohimbine) work through much milder mechanisms than peptides. They provide modest thermogenic or lipolytic effects, typically in the range of 50 to 100 extra calories burned per day. Peptides operate at the hormonal level, producing changes that natural supplements simply cannot achieve.
That said, certain supplements complement peptide protocols effectively. L-carnitine helps transport the fatty acids mobilized by peptide-driven lipolysis into mitochondria for burning. Caffeine enhances AMPK activation alongside MOTS-c. The bioactive peptides for weight loss guide covers compounds that bridge the gap between supplements and injectable peptides.
Peptides versus exogenous HGH
Direct growth hormone injections bypass the pituitary entirely, providing supraphysiological GH levels. The fat loss effects are pronounced but come with significant concerns: potential insulin resistance, joint pain, carpal tunnel symptoms, and organ growth with prolonged use.
GH secretagogues like CJC-1295/ipamorelin achieve 2 to 10x GH elevation while preserving natural pulsatile patterns and feedback mechanisms. The results are more moderate but more sustainable, with significantly lower risk profiles. The HGH alternatives guide compares peptide-based approaches against direct GH replacement.
Legal status and sourcing considerations
The legal landscape for peptides is complex and varies by jurisdiction. Understanding what is and is not legal matters for making informed decisions.
GLP-1 agonists (semaglutide, tirzepatide, liraglutide) are FDA-approved prescription medications for weight management. Obtaining them requires a prescription from a licensed medical provider. The peptide legality guide covers the current regulatory framework in detail.
Tesamorelin is FDA-approved specifically for HIV-associated lipodystrophy. Its use for general fat loss is considered off-label.
Other peptides, including CJC-1295, ipamorelin, AOD-9604, MOTS-c, and 5-amino-1MQ, are classified as research chemicals in most jurisdictions. They are legal to purchase for research purposes but not approved for human use by the FDA. This is an important distinction. The research-grade prescribing guide explains the relationship between compounding pharmacies, research chemicals, and clinical use.
For men seeking medically supervised peptide therapy, the online peptide therapy guide covers telehealth options. Various peptide therapy clinics across the country offer supervised protocols for fat loss.
Quality sourcing is critical regardless of pathway. Third-party testing with certificates of analysis (COA) verifying purity above 98% should be the minimum standard. The testing labs guide provides a framework for evaluating product quality.
Safety, side effects, and contraindications specific to men
Every effective compound has potential downsides. Here are the side effects and risks most relevant to men using fat burning peptides.
Growth hormone secretagogue side effects
Water retention: Mild to moderate, especially in the first 2 to 4 weeks. More pronounced with MK-677 than with CJC-1295/ipamorelin. Usually self-limiting
Joint stiffness: Related to increased GH activity and water retention in joint spaces. Typically mild and resolves with continued use
Carpal tunnel symptoms: Tingling or numbness in hands, particularly at night. Indicates GH levels may be too high. Reduce dose if persistent
Elevated blood glucose: GH antagonizes insulin signaling. Monitor fasting glucose, especially if prediabetic. The safety and risks guide covers glucose management strategies
Increased appetite: Specifically with MK-677 and GHRP-6. Ipamorelin avoids this side effect, making it preferred for fat loss
GLP-1 agonist side effects
Nausea: The most common side effect, particularly during dose escalation. Slow titration reduces severity. Usually resolves within 4 to 6 weeks
Constipation: Related to slowed gastric emptying. Increased fiber and water intake helps. Magnesium supplementation can also address this
Muscle loss: A legitimate concern with significant weight loss from GLP-1 therapy alone. Resistance training and high protein intake are essential countermeasures
Fatigue: Some men report reduced energy during the first month, likely related to caloric reduction. Usually resolves as the body adapts
Who should not use fat burning peptides
Men with active cancer or a history of cancer should avoid GH-elevating peptides, as GH and IGF-1 can potentially promote tumor growth. Men with uncontrolled diabetes should approach GH secretagogues carefully due to glucose effects. Those with severe kidney or liver disease may process peptides differently and require medical supervision.
The beginner mistakes guide covers safety fundamentals for anyone new to peptide protocols. The getting started guide provides a structured introduction for men entering the peptide space for the first time.
Real-world results: what men actually report
Clinical trials provide data. Community experience provides context. Here is what men consistently report across different fat burning peptide protocols.
CJC-1295/ipamorelin users
Most men report 8 to 15 pounds of fat loss over a 12-week cycle when combined with proper diet and training. Sleep quality improvement is nearly universal, with many men describing the best sleep of their lives. Skin quality improvements are frequently mentioned but rarely expected. Muscle fullness and pumps during training increase noticeably by week 3 to 4.
The complaint? Results are gradual. Men expecting dramatic changes in the first two weeks are often disappointed. The real transformation becomes apparent around the 8-week mark when cumulative GH elevation has built sufficient IGF-1 levels to produce visible changes. Patience is required.
Semaglutide users
Weight loss is the most consistent and dramatic outcome. Men report 15 to 30 pounds lost over 3 to 6 months, with some losing significantly more. The appetite reduction is described as transformative by men who previously struggled with portion control and cravings.
The concern most men raise is muscle loss. Without resistance training and adequate protein, semaglutide-driven weight loss includes a significant lean mass component. Men who prioritize strength training during GLP-1 therapy consistently report better body composition outcomes than those who rely on the appetite suppression alone.
Tesamorelin users
Waist circumference reduction is the most commonly reported metric. Men typically see 1 to 3 inches lost from the waist over 8 to 12 weeks, with the changes concentrated in the visceral fat compartment. The scale may not move dramatically because visceral fat is dense but occupies less volume than subcutaneous fat.
Men over 40 report the most satisfaction with tesamorelin because it addresses the specific type of fat accumulation (visceral, hormonal) that characterizes middle-aged male physiology. Younger men with primarily subcutaneous fat may see less dramatic results.
The peptides before and after results page compiles documented transformation data across multiple peptide protocols. For a broader perspective on what peptides can achieve for male health, the complete peptides for men guide covers applications beyond fat loss.
Cost analysis and value comparison
Fat burning peptides represent a financial investment, and understanding the cost-to-benefit ratio helps men make informed decisions about which approaches fit their budget.
GH secretagogues (CJC-1295/ipamorelin, sermorelin) typically cost $100 to $300 per month depending on source and quality. Tesamorelin runs higher, typically $200 to $400 per month. AOD-9604 is moderately priced at $80 to $200 per month. GLP-1 agonists like semaglutide range from $200 to $1300+ per month depending on whether obtained through insurance, telehealth, or compounding pharmacies.
The peptide cost breakdown provides detailed pricing across every major peptide. The therapy cost guide includes insurance coverage information where applicable. The peptide cost calculator can estimate monthly expenses based on your specific protocol.
For men evaluating whether the investment is worthwhile, consider this. A single month of peptide therapy costs less than many monthly gym memberships combined with supplement stacks that produce minimal results. The hormonal optimization that peptides provide addresses root causes that no amount of supplements, diet adjustments, or training modifications can match on their own.
Age-specific considerations for male fat loss with peptides
A 25-year-old man and a 55-year-old man face fundamentally different fat loss challenges, even when body composition looks similar from the outside. Peptide selection should reflect these differences.
Men in their 20s and 30s
Younger men typically still have adequate baseline GH production. For this group, GH secretagogues provide a boost rather than a rescue. The primary value lies in accelerating fat loss during cutting phases and improving recovery between training sessions. CJC-1295/ipamorelin is usually sufficient without the need for tesamorelin, as the pituitary still responds robustly to stimulation.
Men in this age range often benefit more from GLP-1 based approaches if their primary challenge is overeating. Semaglutide can be particularly effective for younger men whose fat gain stems from lifestyle factors (dining out, alcohol, irregular eating patterns) rather than hormonal decline. The appetite regulation creates immediate behavioral change that compounds over months.
Stacking is generally less necessary for younger men. A single compound approach, whether GH secretagogues or GLP-1 therapy, often delivers meaningful results when combined with consistent training and nutrition. Save the complex stacks for when single-compound protocols plateau.
Men in their 40s
This is the decade where fat loss peptides show the most dramatic relative improvement. GH levels have dropped meaningfully. Testosterone often begins declining. Visceral fat starts accumulating even in men who maintained lean physiques throughout their thirties. The metabolic shift is real and frustrating.
GH secretagogue stacks (tesamorelin plus ipamorelin, or CJC-1295/ipamorelin) become more valuable because they are restoring function that has measurably declined. Many men in their forties report that peptides allow them to achieve body composition results they had given up on, believing their metabolism had simply slowed permanently.
MOTS-c becomes relevant in this age group because mitochondrial function declines with age. Adding mitochondrial support to a GH-based protocol addresses both the hormonal and cellular energy components of age-related metabolic slowdown. The energy optimization guide covers the fatigue and metabolism connection in detail.
Men in their 50s and beyond
For men over 50, peptide therapy becomes less about optimization and more about restoration. GH production may be at 20 to 30% of peak levels. Insulin sensitivity has often deteriorated. Muscle mass loss (sarcopenia) accelerates, directly reducing metabolic rate and making fat gain easier with each passing year.
Medical supervision becomes more important in this age group. The risk of complicating conditions (cardiovascular disease, diabetes, cancer) increases, and these conditions can affect both peptide safety and effectiveness. Blood work monitoring before and during any protocol is not optional for men over 50.
The combination of tesamorelin, low-dose CJC-1295/ipamorelin, and MOTS-c represents the most comprehensive approach for this age group. Each compound addresses a different aspect of age-related metabolic decline. For men also on TRT, the synergy between testosterone replacement and GH-based peptides can produce body composition improvements that rival what was possible in their thirties. The complete guide to peptides for men covers age-specific protocols in detail.
The role of body fat percentage in peptide selection
Starting body fat percentage influences which peptides will work best and how quickly you will see results. Here is a practical framework.
Above 30% body fat
Men with significant excess fat benefit most from appetite-driven approaches. Semaglutide or tirzepatide provides the caloric deficit needed for meaningful weight loss, while CJC-1295/ipamorelin preserves muscle mass during the deficit. At this level, the sheer volume of fat to lose means that hormonal optimization through GH secretagogues alone will not produce fast enough visible results to maintain motivation. Appetite control is the primary lever.
20 to 30% body fat
This is the sweet spot for GH-based peptide protocols. There is enough fat to produce visible changes but not so much that hormonal optimization alone is insufficient. CJC-1295/ipamorelin or tesamorelin combined with a moderate caloric deficit and consistent training produces reliable, visible results within 8 to 12 weeks. AOD-9604 can accelerate progress when targeted at specific stubborn areas.
15 to 20% body fat
Getting from this range into lean territory (12 to 15%) is where peptides truly shine. This is the range where hormonal factors matter most. Stubborn fat deposits that resist diet and cardio are often visceral or hormonally driven, making them ideal targets for tesamorelin and GH secretagogues. MOTS-c adds meaningful benefit at this level because cellular energy efficiency becomes a limiting factor when dietary deficit is already dialed in.
Below 15% body fat
Achieving single-digit body fat or extremely lean physiques is a different game. The closer you get to essential body fat levels, the more your body resists further loss through increased hunger, reduced energy expenditure, and hormonal adaptations. At this level, stacking multiple compounds, precise nutrition timing, and careful cycling become essential. GLP-1 agonists help manage the extreme hunger that accompanies very low body fat. GH secretagogues prevent muscle loss during aggressive dieting. The weight loss peptide guide covers protocols for each body fat range.
Frequently asked questions
What is the single best fat burning peptide for men?
There is no single best option because it depends on your specific situation. For visceral belly fat, tesamorelin has the strongest evidence. For overall weight loss with appetite control, semaglutide produces the most dramatic results. For body recomposition (losing fat while maintaining muscle), the CJC-1295/ipamorelin stack is the most popular choice. For men who want an oral, non-injectable option, 5-amino-1MQ is worth investigating.
How quickly do fat burning peptides work for men?
GH secretagogues typically show initial effects (better sleep, increased energy) within 1 to 2 weeks, with visible fat loss starting around weeks 6 to 8. GLP-1 agonists like semaglutide produce noticeable appetite reduction within days and measurable weight loss within the first month. The peptide timeline guide provides compound-specific expectations.
Can you use fat burning peptides with testosterone therapy?
Yes. Peptide therapy and TRT are commonly used together. Testosterone supports muscle preservation and metabolic rate while peptides address fat burning through complementary pathways. The TRT and peptide guide covers combination strategies. The testosterone boosters versus peptides comparison helps determine which approach to prioritize.
Are fat burning peptides safe for men over 50?
GH secretagogues can be particularly beneficial for men over 50 because GH decline is most severe in this age group. However, monitoring is more important because older men are more likely to have insulin sensitivity issues, cardiovascular concerns, or cancer risk factors. Blood work before, during, and after cycles is essential. The safety guide covers age-specific considerations.
Do fat burning peptides show up on drug tests?
GH secretagogues and many research peptides are not included in standard employment drug panels. However, they may be detectable on specialized anti-doping tests used in professional and amateur athletics. GLP-1 agonists are prescription medications and are not flagged on drug tests. The drug testing guide provides comprehensive information on detection windows and test types.
Can fat burning peptides cause hair loss in men?
GH-based peptides do not cause hair loss and may actually support hair health through improved growth factor signaling. GLP-1 agonists have been associated with temporary hair thinning in some users, likely related to the rapid weight loss rather than the peptide itself. The peptides for hair loss guide covers both prevention and treatment options.
What happens when you stop taking fat burning peptides?
With GH secretagogues, your GH levels return to baseline over 2 to 4 weeks after discontinuation. Fat loss gains are maintained if diet and training remain consistent. With GLP-1 agonists, appetite typically returns to pre-treatment levels, and weight regain is common without lifestyle changes. The key is using the peptide period to establish sustainable habits that maintain results independently.
Can you stack semaglutide with GH peptides?
Yes, and this combination is increasingly popular among men seeking maximum fat loss with muscle preservation. Semaglutide handles the caloric deficit through appetite reduction while CJC-1295/ipamorelin preserves lean mass through GH elevation. The weight loss stack guide covers this combination in detail.
External resources
Research and prospect of peptides for use in obesity treatment (PMC Review)
NIDDK: Prescription Medications to Treat Overweight and Obesity
For men serious about optimizing their fat loss protocols, SeekPeptides provides the most comprehensive resource available. Members access evidence-based protocol guides, dosing calculators, community feedback from thousands of experienced researchers, and expert-reviewed stacking strategies tailored to male-specific goals.
In case I do not see you, good afternoon, good evening, and good night. May your body fat stay low, your growth hormone stay elevated, and your protocols stay dialed in. Join SeekPeptides.