Mar 31, 2026

Before you fill that next syringe with a pink-tinted solution from your compounding pharmacy, stop. Read this first. The landscape around compounded tirzepatide with B12 has shifted dramatically, and what you do not know could genuinely put your health at risk. Cyanocobalamin tirzepatide, the combination of the dual GIP/GLP-1 receptor agonist tirzepatide with vitamin B12 in its cyanocobalamin form, has become one of the most commonly dispensed compounded weight loss formulations in the country. Millions of people inject it weekly. Many of them have never questioned what is actually inside the vial, how the two compounds interact at the molecular level, or whether the combination is even stable. That is a problem. Eli Lilly, the manufacturer of branded tirzepatide, has now released testing data showing significant impurities in compounded tirzepatide-B12 products, and the findings raise questions that every single person using these formulations needs to understand.
This guide covers everything. The science behind cyanocobalamin in the compound, the specific safety concerns that have emerged, how this formulation compares to methylcobalamin-based tirzepatide alternatives, what the dosing looks like in practice, and what your options are if you decide the risk profile no longer fits your comfort level. Whether you are currently using this compound, considering it, or simply trying to make sense of the headlines, this is the resource you need.
What cyanocobalamin tirzepatide actually is
Cyanocobalamin tirzepatide is a compounded injectable formulation that combines two distinct compounds into a single vial. The first is tirzepatide, a synthetic peptide that activates both the GIP and GLP-1 receptors in the body. The second is cyanocobalamin, the synthetic form of vitamin B12 that gives the solution its distinctive pink to light red color.
This is not a branded pharmaceutical product.
No FDA-approved medication contains both tirzepatide and cyanocobalamin together. Instead, this combination exists exclusively through compounding pharmacies that prepare custom formulations by mixing the two ingredients. The typical formulation you will encounter is tirzepatide/cyanocobalamin at a concentration of 2.5mg/1mg per 0.5mL, though concentrations vary widely between pharmacies and prescriptions.
To understand why this combination exists, you need to understand what each component does on its own. Tirzepatide works by mimicking two natural hormones in the body, glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1). These hormones regulate blood sugar, slow gastric emptying, reduce appetite, and influence how the body stores and burns fat. The dual-receptor mechanism is what separates tirzepatide from semaglutide and other single-receptor GLP-1 agonists, and clinical data from the SURMOUNT-1 trial demonstrated that patients on the highest tirzepatide dose of 15mg lost an average of 52 pounds, representing a 22.5% reduction in body weight over 72 weeks. The placebo group lost just 5.3 pounds.
Those numbers changed everything about weight management.
Cyanocobalamin, the other half of this compound, is vitamin B12 in one of its most common supplemental forms. The body needs B12 for DNA synthesis, red blood cell formation, neurological function, and energy metabolism. The cyano prefix refers to the cyanide group attached to the cobalt center of the molecule, which sounds alarming but is present in such trace amounts that it poses no toxicity concern when used at standard supplemental doses. The body cleaves off the cyanide group during metabolism and converts cyanocobalamin into its active coenzyme forms, methylcobalamin and adenosylcobalamin, which then participate in critical biochemical reactions throughout the body.
Why pharmacies combine them
The rationale is straightforward. People on tirzepatide eat significantly less food. Caloric restriction reduces nutrient intake across the board, and B12 is one of the nutrients most likely to become deficient during aggressive weight loss. Research has shown that individuals with obesity already carry a higher baseline risk of B12 deficiency, and layering a GLP-1 medication that causes fatigue on top of that creates a perfect storm for energy depletion.
Compounding pharmacies saw an opportunity. By adding cyanocobalamin directly to the tirzepatide injection, patients receive their B12 supplementation automatically with each weekly dose. No extra pills. No separate injections. One shot handles both the weight loss peptide and the nutritional support.
The convenience factor drove massive adoption. But convenience and safety are not the same thing, and that distinction has become critically important.
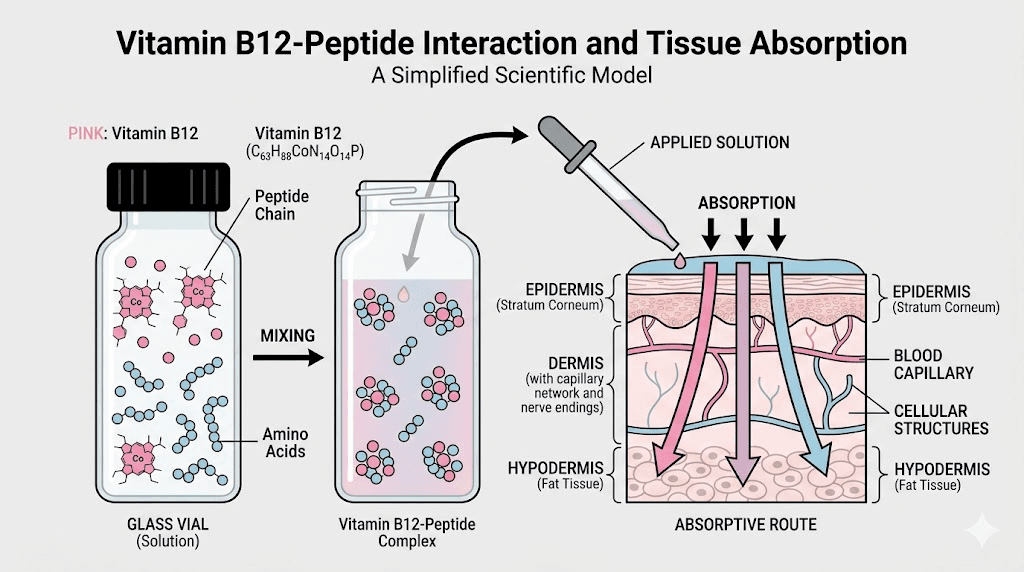
How cyanocobalamin works inside the formulation
When cyanocobalamin is added to a tirzepatide solution, it dissolves readily and produces the characteristic pink to light red color that many users recognize. That color comes from the cobalt-corrin ring structure of the B12 molecule, which absorbs light in specific wavelengths and reflects back in the red-pink spectrum. If your compounded tirzepatide is pink, it contains some form of B12. If it is clear, it does not.
The color of your tirzepatide tells you something important about what is in the vial.
Once injected subcutaneously, the two compounds theoretically operate independently. Tirzepatide begins its journey to GIP and GLP-1 receptors throughout the body, while cyanocobalamin enters the bloodstream and is transported to cells that need it for metabolic processes. The B12 binds to transcobalamin proteins in the blood, which carry it to tissues where it is converted into its active forms and put to work in methylation reactions, mitochondrial energy production, and red blood cell synthesis.
The problem is what happens before injection. Inside the vial. Over time.
Tirzepatide is a complex 39-amino-acid peptide with a C20 fatty diacid chain that facilitates its extended half-life. Cyanocobalamin is a large organometallic compound with a reactive cobalt center. When these two molecules sit together in solution, they can interact chemically in ways that neither the pharmacy nor the patient can see, smell, or detect without sophisticated analytical equipment. And that is exactly what Eli Lilly found when they tested these products, but more on that in the safety section below.
The pharmacokinetics of combined delivery
When you inject tirzepatide with a syringe into subcutaneous tissue, the compound forms a depot at the injection site. Tirzepatide releases slowly from this depot over the course of a week, which is what allows for once-weekly dosing. Its half-life is approximately five days, meaning it takes about five days for half the dose to be eliminated from the body.
Cyanocobalamin behaves differently. It is water-soluble and absorbs relatively quickly from the injection site. There is no slow-release mechanism for B12 in this formulation. The body takes what it needs, stores some in the liver (which can hold several years worth of B12 reserves), and excretes the rest through urine. This is why people sometimes notice bright yellow or pink-tinged urine after their injection. That is excess B12 being eliminated.
The mismatch in absorption kinetics matters. You are getting a week-long sustained release of tirzepatide but a rapid bolus of cyanocobalamin. Whether this delivery pattern is optimal for B12 supplementation compared to daily oral supplementation or periodic standalone B12 injections is an open question. Some clinicians argue that the weekly B12 bolus from the compound is perfectly adequate. Others suggest that daily oral B12 supplementation provides more consistent levels and avoids the risks of combining it with the peptide altogether.
Cyanocobalamin versus methylcobalamin in tirzepatide compounds
This is one of the most common questions people ask about their compounded tirzepatide, and the answer is more nuanced than most sources let on.
Cyanocobalamin and methylcobalamin are both forms of vitamin B12. They share the same corrin ring structure with a central cobalt atom. The difference lies in what is attached to that cobalt. In cyanocobalamin, it is a cyanide group. In methylcobalamin, it is a methyl group.
Methylcobalamin is bioactive. The body can use it directly in methylation reactions without any conversion. Cyanocobalamin is not bioactive. It must first be converted by the body, a process that involves removing the cyanide group and replacing it with either a methyl group (creating methylcobalamin) or an adenosyl group (creating adenosylcobalamin). This conversion happens primarily in the liver and requires adequate levels of glutathione and other cofactors.
So methylcobalamin is better, right? Not necessarily. And definitely not in this context.
Here is the reality. Cyanocobalamin is significantly more stable in solution than methylcobalamin. It resists degradation from light, heat, and time far better than its methylated counterpart. In a compounded formulation that might sit in your refrigerator for weeks, stability of the ingredients matters enormously. Methylcobalamin is notoriously light-sensitive and can degrade rapidly when exposed to ambient conditions, potentially reducing the effective B12 dose you receive with each injection.
But here is the critical update that changes this entire conversation. Eli Lilly testing found impurities in compounded tirzepatide products containing B12, and this finding applies to ALL forms of B12. Cyanocobalamin. Methylcobalamin. Hydroxocobalamin. Every single one. The chemical interaction between tirzepatide and B12 is not limited to one form. The cobalt center that is common to all B12 variants appears to be involved in the reaction that produces these impurities.
That means the cyanocobalamin versus methylcobalamin debate, while academically interesting, may be beside the point entirely if combining any form of B12 with tirzepatide in the same vial creates degradation products of unknown safety.
Quick comparison of B12 forms used in tirzepatide compounds
Cyanocobalamin - Most stable in solution, requires body conversion, contains trace cyanide group, produces pink color, lowest cost for pharmacies
Methylcobalamin - Bioactive form, light-sensitive and less stable, no conversion needed, produces pink color, slightly higher cost
Hydroxocobalamin - Precursor form, moderate stability, used less commonly in compounds, produces pink/red color, intermediate cost
All three forms produce the same characteristic pink color in the tirzepatide solution. And according to the available testing data, all three forms may participate in the same problematic chemical reactions with the peptide.
If your primary concern is getting adequate B12 supplementation without the risks of combining it with tirzepatide, the simplest approach is to take B12 separately. Oral cyanocobalamin supplements are inexpensive, widely available, and effective for most people. Standalone B12 injections are another option. Either approach eliminates the interaction risk entirely while still providing the nutritional support your body needs during tirzepatide-driven weight loss.
Benefits of adding B12 to tirzepatide
Despite the safety concerns, it is important to understand why B12 was added to these formulations in the first place. The rationale was not arbitrary. There are genuine physiological reasons to ensure adequate B12 status during GLP-1 receptor agonist therapy, even if the delivery method of combining them in one vial is now being questioned.
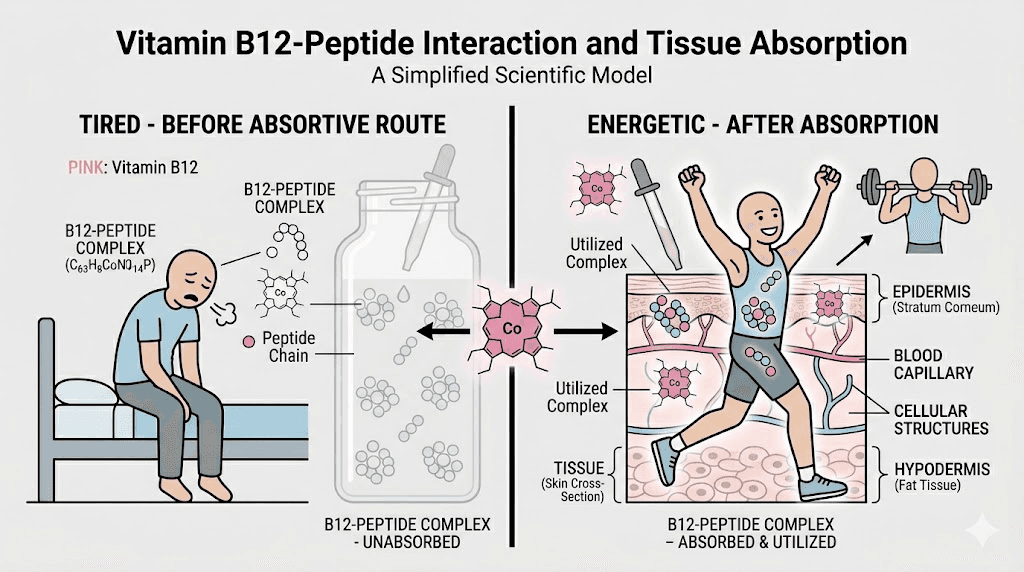
Energy support during caloric restriction
Fatigue is one of the most commonly reported side effects of tirzepatide therapy. Does tirzepatide make you tired? Absolutely. And for many users, the fatigue is significant enough to affect daily functioning, work performance, and exercise capacity. B12 plays a central role in cellular energy production through its involvement in the citric acid cycle and mitochondrial function. When B12 levels are adequate, cells can efficiently convert nutrients into ATP, the molecular currency of energy. When B12 is deficient, energy production suffers, and fatigue worsens.
The logic of adding B12 to tirzepatide was simple. If the medication causes fatigue and the resulting caloric restriction depletes B12, then providing supplemental B12 directly in the injection could mitigate both problems simultaneously.
Metabolic support for fat and carbohydrate metabolism
B12 is a cofactor for two critical enzymes in human metabolism. The first is methionine synthase, which is involved in methylation reactions and the recycling of homocysteine back into methionine. The second is methylmalonyl-CoA mutase, which plays a direct role in the metabolism of certain fatty acids and amino acids. Without adequate B12, these pathways slow down, and metabolic intermediates accumulate.
During active weight loss, your body is breaking down stored fat at an accelerated rate. That fat breakdown generates large quantities of metabolic intermediates that need to be processed through pathways that depend on B12. Supporting these pathways with supplemental B12 made theoretical sense as a way to optimize fat metabolism during tirzepatide therapy.
Red blood cell production
B12 deficiency causes a specific type of anemia called megaloblastic anemia, where the body produces abnormally large, dysfunctional red blood cells. These oversized cells cannot carry oxygen efficiently, leading to fatigue, weakness, shortness of breath, and poor exercise tolerance. For someone on tirzepatide who is already dealing with body aches, reduced caloric intake, and potential muscle loss, adding anemia to the mix would be counterproductive.
Maintaining adequate B12 status ensures normal red blood cell production and oxygen-carrying capacity.
Higher baseline deficiency risk in the target population
Research has consistently shown that individuals with obesity have higher rates of B12 deficiency compared to the general population. The reasons are multifactorial. Certain obesity-related conditions affect B12 absorption. Medications commonly prescribed alongside weight loss drugs, particularly metformin and proton pump inhibitors, deplete B12 levels. Dietary patterns associated with obesity often include lower intake of B12-rich foods like organ meats, shellfish, and fortified cereals.
When you start tirzepatide on top of an already marginal B12 status, the dramatic reduction in food intake can push levels from borderline into genuinely deficient territory relatively quickly. Supplementation alongside tirzepatide is not just nice to have. For many patients, it is medically necessary.
Neurological protection
B12 is essential for the maintenance of the myelin sheath, the protective coating around nerve fibers that ensures rapid signal transmission. Prolonged B12 deficiency can cause irreversible neurological damage, including peripheral neuropathy, cognitive decline, balance problems, and mood disturbances. These are not minor issues. They are serious clinical consequences that develop insidiously and may not be reversible once established.
For patients on long-term tirzepatide therapy with consistently reduced food intake, monitoring and maintaining B12 levels is a legitimate medical priority. The question is not whether B12 supplementation is important. It is. The question is whether combining it directly with tirzepatide in the same vial is the safest way to deliver it.
The Eli Lilly impurity warning: what you need to know
This is the section that matters most. Read it carefully.
Eli Lilly, the company that manufactures branded tirzepatide under the name Mounjaro (for diabetes) and Zepbound (for weight loss), conducted testing on compounded tirzepatide products containing B12. What they found was alarming. Their analytical testing detected significant levels of an unknown impurity that appears to result from a chemical reaction between tirzepatide and B12 molecules within the compounded solution.
This impurity had not been previously identified or characterized. Its toxicological profile is completely unknown. Nobody knows what it does in the human body because nobody knew it existed until Lilly looked for it. The short-term effects are unknown. The long-term effects are unknown. Whether it accumulates in tissues is unknown. Whether it triggers immune reactions is unknown.
That level of uncertainty should concern anyone injecting these products.
Lilly also reported finding bacterial contamination and elevated endotoxin levels in some of the compounded tirzepatide-B12 products they tested. Endotoxins are components of bacterial cell walls that trigger inflammatory responses in the body. Even in sterile products where bacteria have been killed, residual endotoxins can cause fever, inflammation, and in severe cases, septic shock. The presence of elevated endotoxins suggests inadequate quality control in the manufacturing process at certain compounding facilities.
The scope of the warning
Critically, Lilly stated that this warning applies to ALL forms of B12 combined with tirzepatide. Not just cyanocobalamin. Not just methylcobalamin. All of them. The chemical reaction generating the impurity appears to involve the cobalt-corrin core structure that is common to every form of vitamin B12. Switching from cyanocobalamin to methylcobalamin or hydroxocobalamin does not eliminate the problem.
Lilly urged the FDA to recall all compounded tirzepatide products containing B12 additives. Whether the FDA will take that step remains to be seen, but the request itself is significant. Pharmaceutical companies do not make public recall requests lightly. The data Lilly presented was apparently compelling enough to warrant that level of response.
What this means for current users
If you are currently using a cyanocobalamin tirzepatide compound, you do not need to panic. But you do need to have a conversation with your prescribing provider. The impurity finding does not mean that everyone who has used these products has been harmed. It means that a potential risk has been identified that was not previously known, and the magnitude of that risk has not yet been determined.
Some users will choose to continue their current compound until their supply runs out and then switch to a B12-free formulation. Others will want to switch immediately. Still others may decide that the potential benefits of the combined formulation outweigh the currently undefined risks. All of these are reasonable positions, but they should be made with full awareness of the available information, not in ignorance of it.
SeekPeptides provides members with regularly updated safety information on compounded peptide formulations, including detailed breakdowns of emerging research findings like this one. When the landscape shifts, having access to current, unbiased information is not a luxury. It is a necessity.
Putting the warning in context
It is worth noting that Eli Lilly has a financial interest in reducing the use of compounded tirzepatide. Compounding pharmacies represent significant competition for their branded products, and Lilly has pursued multiple legal and regulatory strategies to limit compounded alternatives. This does not mean their testing data is wrong. The impurity findings are either real or they are not, and independent verification will eventually confirm or refute them. But it does mean that the source of the warning has a commercial interest in the outcome.
The responsible approach is to take the data seriously while recognizing the source. If the impurities are confirmed by independent laboratories, the case for separating B12 from tirzepatide becomes overwhelming. If the findings cannot be replicated, the picture changes. Until then, the precautionary principle suggests that tirzepatide formulations without B12 are the lower-risk option for people who want to continue compounded therapy.
Dosing and concentration details
Understanding the dosing of cyanocobalamin tirzepatide requires understanding both components separately and how they are combined in practice.
Tirzepatide dosing protocol
The standard tirzepatide dosing protocol follows a gradual titration schedule. You start low and increase over time to allow the body to adjust and minimize gastrointestinal side effects.
Weeks 1 through 4: 2.5mg once weekly (the starting dose)
Weeks 5 through 8: 5mg once weekly
Weeks 9 through 12: 7.5mg once weekly
Weeks 13 through 16: 10mg once weekly
Weeks 17 through 20: 12.5mg once weekly
Week 21 and beyond: 15mg once weekly (maximum dose)
Not everyone needs to reach 15mg. Some people achieve their weight loss goals at lower doses. The right dose is the one that produces meaningful results with manageable side effects. If you are losing weight steadily at 7.5mg with minimal bloating and nausea, there may be no reason to increase further.
Compounded formulations typically come in multi-dose vials with varying concentrations. A dosage calculator is essential for determining the correct injection volume based on your specific vial concentration and prescribed dose. Getting this wrong can mean under-dosing (wasting money and getting suboptimal results) or over-dosing (increasing side effects unnecessarily).
Cyanocobalamin dosing in the compound
The cyanocobalamin component is typically dosed at 1mg per injection in most compounded formulations. This is a standard therapeutic B12 dose, comparable to what you would receive in a standalone B12 injection at a clinic. For reference, the daily recommended intake of B12 for adults is just 2.4 micrograms, so 1mg (1,000 micrograms) is roughly 400 times the daily requirement delivered in a single weekly dose.
This is not unusual for B12 supplementation. Because B12 is water-soluble and excess is excreted through urine, mega-dosing B12 is generally considered safe. The body absorbs what it can use, stores some in the liver, and eliminates the rest. There is no established upper toxicity limit for B12 from supplemental sources.
Common formulation concentrations
Compounding pharmacies prepare cyanocobalamin tirzepatide in various concentrations. Here are the most common you will encounter.
A typical starting-dose vial might contain tirzepatide at 5mg/mL with cyanocobalamin at 2mg/mL. To get your 2.5mg starting dose of tirzepatide, you would draw 0.5mL, which would also deliver 1mg of cyanocobalamin. As you titrate up through higher tirzepatide doses, you may need vials with higher tirzepatide concentrations to keep the injection volume manageable.
At higher doses like 10mg or 15mg of tirzepatide, pharmacies often use more concentrated formulations such as 20mg/mL or 30mg/mL tirzepatide. The cyanocobalamin concentration is adjusted proportionally, though some pharmacies keep the B12 dose constant regardless of the tirzepatide strength. This means your B12 intake per injection may vary depending on your specific pharmacy and formulation.
Always check with your pharmacy about the exact concentrations in your vial. Do not assume. Use the peptide calculator tools available through SeekPeptides to verify your injection volumes and ensure you are drawing the correct dose of both components.
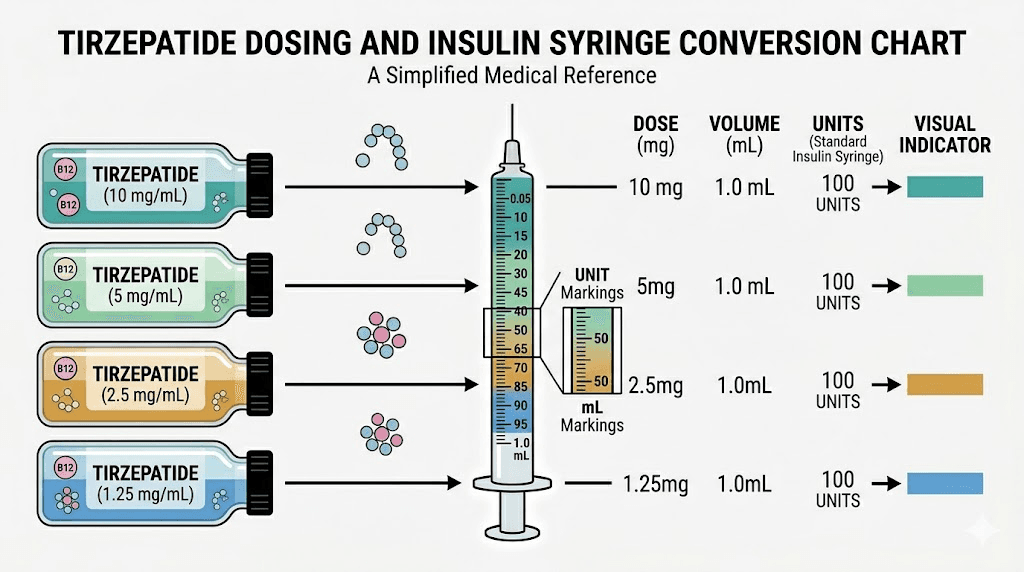
Converting between units and milligrams
One of the most confusing aspects of compounded tirzepatide dosing is the relationship between units on your syringe and milligrams of active ingredient. The conversion depends entirely on the concentration of your specific vial.
For a 5mg/mL formulation in a standard insulin syringe:
20 units equals 0.2mL, which delivers 1mg of tirzepatide
50 units equals 0.5mL, which delivers 2.5mg of tirzepatide
100 units equals 1.0mL, which delivers 5mg of tirzepatide
For a 10mg/mL formulation:
The numbers change again for 20mg/mL and 30mg/mL concentrations. A dosage chart specific to your vial concentration is the safest reference tool. Never guess. Never estimate. The difference between 30 units and 40 units might not seem like much on the syringe, but it could represent a significant dose difference depending on your concentration.
The pink color explained
The color of tirzepatide with B12 is one of the most immediately noticeable characteristics of these compounded formulations, and it serves as a useful visual indicator of what is in your vial.
Pure tirzepatide in solution is clear and colorless. The moment cyanocobalamin is added, the solution turns pink. The intensity of the color depends on the concentration of B12. Low concentrations produce a faint, almost translucent pink. Higher concentrations produce a deeper, more saturated rose or light red color.
This color comes from the molecular structure of cyanocobalamin itself. The corrin ring system surrounding the central cobalt atom absorbs light in the green-yellow portion of the visible spectrum and reflects back red-pink wavelengths. This is an inherent property of the molecule that cannot be avoided. If your B12-containing tirzepatide is not pink, something is wrong. Either the B12 has degraded, the concentration is negligibly low, or the product does not actually contain B12 despite the label.
The color should be consistent throughout the solution. Swirl the vial gently before drawing your dose. If you see particles, cloudiness, color separation, or a dramatically different shade from your previous vial, do not use the product. Contact your pharmacy.
For comparison, tirzepatide with glycine and B12 will also be pink due to the B12 component, while tirzepatide with glycine alone (no B12) will be clear. Tirzepatide with niacinamide is clear as well, since niacinamide (vitamin B3) does not produce visible color at typical formulation concentrations.
Storage and handling for cyanocobalamin tirzepatide
Proper storage of compounded cyanocobalamin tirzepatide is critical for maintaining both the potency of the tirzepatide and the stability of the cyanocobalamin. Get this wrong, and you risk injecting degraded product that may be less effective or potentially contain higher levels of the decomposition products that Lilly identified in their testing.
Refrigeration requirements
Tirzepatide must be refrigerated. Store your compound between 36 and 46 degrees Fahrenheit (2 to 8 degrees Celsius). This is the standard temperature range inside a properly functioning household refrigerator. Do not store it in the door where temperature fluctuations are greatest. Place it in the main compartment, ideally in the back where the temperature is most stable.
Cyanocobalamin is one of the more heat-stable B12 forms, but it is light-sensitive. Most compounding pharmacies dispense the product in amber or opaque vials to protect against light degradation. If your vial is clear glass, store it in its original box or wrap it in foil to minimize light exposure.
How long does tirzepatide last in the fridge? Compounded products typically carry a beyond-use date (BUD) assigned by the pharmacy, usually 30 to 90 days depending on the formulation and the pharmacy facility type. A 503B outsourcing facility may assign longer dating based on stability testing, while a traditional 503A pharmacy typically assigns shorter dating based on default USP guidelines.
What happens when the temperature changes
What happens if tirzepatide gets warm? Brief excursions to room temperature, such as removing the vial to draw your dose and returning it to the fridge within 30 minutes, are generally fine. Extended exposure to room temperature accelerates degradation of the peptide and may accelerate the chemical interaction between tirzepatide and cyanocobalamin.
How long can compounded tirzepatide be out of the fridge? Most pharmacies recommend no more than a few hours at room temperature. If you are traveling with tirzepatide, use an insulated bag with ice packs to maintain cold chain. Never leave it in a hot car, near a window, or in direct sunlight.
Can you freeze tirzepatide? Generally no. Freezing and thawing can cause the peptide to aggregate and denature, reducing potency. Some lyophilized (freeze-dried) tirzepatide products are designed for cold storage before reconstitution, but once reconstituted and mixed with cyanocobalamin, freezing is not recommended.
Checking expiration and potency
Always check the expiration date on your vial before each injection. Does tirzepatide expire? Yes. All compounded products have a finite shelf life, and using product past its beyond-use date means you may be injecting a less potent, more degraded formulation. With the added concern about B12-tirzepatide interactions producing impurities over time, using fresh product within its dating window becomes even more important.
Side effects and what to watch for
The side effect profile of cyanocobalamin tirzepatide is primarily driven by the tirzepatide component. Cyanocobalamin at standard supplemental doses causes very few side effects on its own. The tirzepatide, however, comes with a well-documented list of potential adverse effects that anyone using this compound should understand.
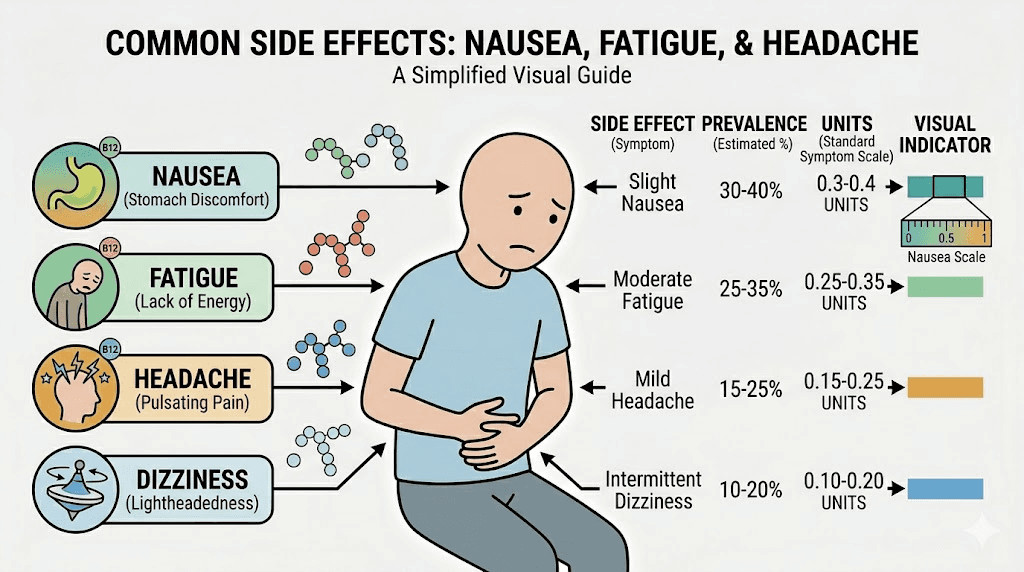
Common gastrointestinal side effects
Nausea is the most frequently reported side effect, particularly during dose titration. It tends to be worst in the first few days after increasing to a new dose and often improves over subsequent weeks as the body adapts. Eating smaller, more frequent meals, avoiding fatty or greasy foods, and taking your injection at the best time for your schedule can help manage nausea.
Constipation affects a significant percentage of users. The slowed gastric motility that reduces appetite also slows transit through the entire digestive tract. Adequate hydration, fiber supplementation, and stool softeners are common management strategies. If constipation becomes severe or is accompanied by abdominal pain, contact your provider.
Diarrhea can also occur, sometimes alternating with constipation. This typically resolves within the first few weeks on a new dose. If it persists, it may indicate that your dose is too high or that your body needs more time to adjust.
Bloating and dry mouth round out the most common GI complaints. Both are manageable with dietary modifications and adequate fluid intake.
Energy and neurological effects
Fatigue is extremely common, especially during the first weeks of treatment and after dose increases. This is where the cyanocobalamin component was intended to help. Whether the B12 actually mitigates the fatigue in practice is debated. Some users report noticeably more energy with the B12 compound compared to tirzepatide alone. Others notice no difference.
Headaches occur in a meaningful percentage of users. They may be related to the metabolic shifts caused by the medication, dehydration from reduced fluid intake, or blood sugar fluctuations. Staying hydrated and eating regularly, even if portions are small, helps prevent them.
Insomnia and anxiety have been reported by some users. The relationship between GLP-1 receptor agonists and neurological effects is an active area of research. GLP-1 receptors exist in the brain, and activating them can influence mood, sleep, and cognitive function in ways that are not yet fully understood.
Injection site reactions
Injection site reactions including redness, swelling, itching, and pain are common with all subcutaneous injections. Red and itchy injection sites are particularly common with compounded formulations, and some users have speculated that the B12 component, with its distinctive color, may contribute to local irritation. Whether this is true or simply a perception bias is unclear.
Rotating injection sites between the abdomen, thigh, and upper arm can help minimize site reactions. Multiple injection sites are available, and using a consistent rotation pattern gives each area time to recover between injections.
Muscle and joint effects
Muscle pain and body aches affect some users, particularly during rapid weight loss. This may be related to electrolyte imbalances, reduced protein intake, or the metabolic stress of significant caloric restriction. Ensuring adequate protein and supplement intake is essential during tirzepatide therapy.
Hair loss is another side effect that concerns many users. This is typically telogen effluvium, a temporary shedding condition triggered by the physiological stress of rapid weight loss rather than a direct drug effect. It usually resolves on its own once weight stabilizes, but it can be distressing while it occurs.
Side effects specific to the cyanocobalamin component
At the doses used in these compounds, cyanocobalamin-specific side effects are rare. However, some potential considerations include mild injection site pain (B12 injections can sting slightly, though this is masked by the tirzepatide in the compound), rare allergic reactions in individuals with cobalt sensitivity, and the theoretical concern about cyanide accumulation in people with severe kidney disease who cannot efficiently excrete the trace cyanide released during cyanocobalamin metabolism.
For the vast majority of users, the cyanocobalamin component adds negligible side effect risk beyond what tirzepatide alone produces. The primary concern with the combination is not the direct side effects of either component but rather the unknown impurities created by their interaction in the vial.
Who this compound is designed for
Cyanocobalamin tirzepatide was designed for a specific patient population, and understanding whether you fit that profile helps you evaluate whether this particular formulation makes sense for your situation.
The ideal candidate
The original target was someone who meets the clinical criteria for tirzepatide therapy (BMI of 30 or greater, or BMI of 27 or greater with at least one weight-related comorbidity) and who also has documented or suspected B12 deficiency. This might include people with a history of low B12 levels on blood work, those taking metformin or proton pump inhibitors that deplete B12, vegetarians or vegans with limited dietary B12 intake, individuals with absorption issues from gastric conditions, or anyone experiencing the pronounced fatigue that often accompanies early tirzepatide therapy.
For these people, the combined formulation offered genuine convenience. One injection, two treatments.
Who should consider alternatives
Given the emerging safety data, several groups should particularly consider switching to a B12-free tirzepatide formulation with separate B12 supplementation.
People with compromised kidney function should be cautious. Cyanocobalamin produces trace amounts of free cyanide during metabolism, and while this is clinically insignificant in people with normal kidney function, impaired renal clearance could theoretically allow accumulation. Additionally, the unknown impurities from the tirzepatide-B12 interaction may be renally cleared, and impaired kidney function could affect their elimination.
Pregnant or breastfeeding women should avoid compounded formulations in general, and the unknown impurity profile of B12-containing tirzepatide compounds adds another reason for caution. People with a history of allergic reactions to B12 injections or cobalt sensitivity should also avoid the combined product.
Anyone who is particularly risk-averse or who wants to minimize unknowns should strongly consider separating their B12 supplementation from their tirzepatide injection. The convenience of the combined formulation simply may not justify the uncertainty that now surrounds it.
Alternatives to B12-containing tirzepatide compounds
If the safety concerns around B12-tirzepatide combinations have you reconsidering your current formulation, several alternatives exist that provide weight loss support without the B12 interaction risk.
Tirzepatide with niacinamide
Tirzepatide with niacinamide (vitamin B3) has emerged as one of the most popular alternatives to B12-containing compounds. Niacinamide serves as a stabilizer for the tirzepatide peptide in solution and provides its own metabolic benefits, including support for NAD+ production and cellular energy metabolism. Critically, niacinamide does not share the cobalt-corrin structure that appears to be involved in the problematic interaction between B12 and tirzepatide.
The solution is clear, not pink. It does not carry the same impurity concerns identified in Lilly testing. And it has a long track record of safe use as a pharmaceutical excipient.
Tirzepatide with glycine
Tirzepatide with glycine is another B12-free option. Glycine is the simplest amino acid and serves as a stabilizer in the formulation while also providing its own benefits, including support for collagen synthesis, sleep quality, and digestive health. The glycine formulation is clear and colorless.
Tirzepatide with levocarnitine
Tirzepatide with levocarnitine combines the peptide with L-carnitine, an amino acid derivative that plays a central role in fatty acid transport into mitochondria for energy production. This blend was designed specifically to support fat metabolism during weight loss, and the clear formulation avoids the B12 interaction concern.
Tirzepatide with pyridoxine (B6)
Tirzepatide with vitamin B6 offers another nutrient-enhanced option. Pyridoxine supports protein metabolism, neurotransmitter synthesis, and immune function. It does not contain cobalt or share the structural features of B12 that appear to drive the impurity formation.
Plain tirzepatide with separate B12
The simplest approach is to use tirzepatide without any additives and take B12 separately. Oral cyanocobalamin or methylcobalamin supplements are available over the counter for a few dollars per month. Sublingual tablets dissolve under the tongue for better absorption. If you prefer injections, standalone B12 shots can be administered separately on a different day or at a different injection site. This approach gives you complete control over both components without any interaction risk.
You can also explore NAD+ alongside tirzepatide for additional energy support, or consider probiotics for digestive health during GLP-1 therapy.
How to evaluate compounding pharmacy quality
If you choose to continue using compounded cyanocobalamin tirzepatide, or if you switch to any other compounded tirzepatide formulation, the quality of your compounding pharmacy matters enormously. The Lilly testing that found impurities and bacterial contamination in some products underscores this point. Not all compounding pharmacies are equal, and the difference between a well-run facility and a substandard one could be the difference between a safe product and a dangerous one.
503A versus 503B facilities
503B outsourcing facilities operate under stricter regulatory oversight than traditional 503A pharmacies. They must register with the FDA, follow current good manufacturing practices (cGMP), and submit to regular inspections. Their products must undergo testing for potency, sterility, and endotoxin levels before release. They can prepare larger batches and do not require individual patient prescriptions for each unit produced.
Traditional 503A pharmacies operate under state pharmacy board oversight, which varies significantly by state. They compound on a per-prescription basis, and testing requirements are generally less rigorous. Some excellent 503A pharmacies voluntarily test every batch, while others perform minimal quality assurance.
For injectable products that go directly into your body, 503B facilities offer a higher baseline quality assurance standard. This does not guarantee perfection, but it does mean the product has passed quantitative testing before reaching you.
Questions to ask your pharmacy
Before using any compounded tirzepatide product, ask these questions.
Do you test every batch for potency? A pharmacy that tests ensures that the labeled dose actually matches what is in the vial. Without potency testing, you are relying on the compounding process being perfect every time, which is unrealistic.
Do you test for sterility and endotoxins? This is non-negotiable for injectable products. Sterility testing confirms the absence of viable microorganisms. Endotoxin testing (LAL testing) confirms the absence of bacterial cell wall fragments that can cause inflammatory reactions even in sterile products.
What is your facility classification? Understanding whether you are dealing with a 503A or 503B operation sets your expectations for the level of regulatory oversight and quality control.
What is the beyond-use date for this formulation? Shorter dating may indicate more conservative, safety-conscious policies. Extremely long dating on compounded injectables should raise questions about what testing supports that dating.
Where do you source your tirzepatide API? The raw peptide quality matters. Reputable pharmacies source from registered, inspected API manufacturers. Bulk tirzepatide powder from unknown sources carries obvious risks. Understanding the supply chain behind your medication is part of being an informed consumer.
Do you have certificates of analysis available? A COA documents the testing results for each batch of raw material and finished product. Pharmacies willing to provide COAs on request demonstrate transparency and accountability.
Avoiding grey market tirzepatide is essential. Products sourced outside legitimate pharmaceutical supply chains may contain incorrect doses, contaminants, or entirely different compounds than what the label claims. The savings are not worth the risk.
Red flags to watch for
Be wary of pharmacies that cannot or will not answer the questions above. Be suspicious of prices dramatically lower than other pharmacies, which may indicate corners being cut in testing or sourcing. Watch for products with unusually long beyond-use dates, unclear labeling, or shipping without cold chain packaging. And be skeptical of any pharmacy that claims its products are equivalent to branded Mounjaro or Zepbound. They are not. Compounded tirzepatide is a different product made by a different process with different quality control standards.
Empower Pharmacy is one of the larger 503B facilities that has produced tirzepatide compounds, and finding affordable tirzepatide from a reputable source requires balancing cost considerations against quality standards. The cheapest option is rarely the best option when you are injecting something into your body.
Reconstitution and injection technique
Some cyanocobalamin tirzepatide products come as ready-to-inject solutions, while others, particularly those based on lyophilized tirzepatide, require reconstitution before use. Understanding the proper technique for both scenarios ensures you get an accurate dose of both the tirzepatide and the cyanocobalamin.
For pre-mixed liquid formulations
Most compounded cyanocobalamin tirzepatide ships as a ready-to-use liquid in a multi-dose vial. Before drawing your dose, remove the vial from the refrigerator and allow it to warm to room temperature for 15 to 20 minutes. Cold injections are more uncomfortable and may affect absorption slightly.
Inspect the solution visually. It should be pink (from the B12) and clear. No particles. No cloudiness. No unusual color changes from previous inspections. If anything looks off, do not use it.
Clean the vial stopper with an alcohol swab. Draw the correct volume into your syringe based on your prescribed dose and the vial concentration. Refer to a dosing chart or calculator if you are unsure of the volume. Remove air bubbles by tapping the syringe and pushing the plunger slightly until a small drop appears at the needle tip.
For lyophilized formulations requiring reconstitution
Reconstituting tirzepatide requires mixing the freeze-dried powder with a sterile diluent, typically bacteriostatic water. The amount of water you add determines the final concentration, which determines how much you draw for each dose.
For a 10mg vial of tirzepatide, adding the correct amount of bacteriostatic water is critical. Too much water and the solution will be too dilute, requiring larger injection volumes. Too little and it will be too concentrated, making accurate dosing difficult with standard syringes.
The general process for mixing peptides with bacteriostatic water is straightforward but must be done carefully. Inject the water slowly down the side of the vial, not directly onto the powder. Swirl gently. Never shake. Shaking can denature the peptide, reducing its potency. Allow the powder to dissolve completely before drawing your dose.
If your cyanocobalamin tirzepatide product comes in lyophilized form, the cyanocobalamin may be included in the powder or provided separately. Follow your pharmacy specific instructions for reconstitution.
Injection technique
Injecting tirzepatide is a subcutaneous injection, meaning the needle goes into the fatty tissue just beneath the skin. You do not need to reach muscle. The recommended injection sites include the abdomen (at least two inches from the navel), the front of the thigh, and the back of the upper arm.
Pinch a fold of skin at the injection site. Insert the needle at a 45 to 90 degree angle (90 degrees if you have adequate subcutaneous fat at the site). Inject slowly and steadily. Hold the needle in place for 5 to 10 seconds after the plunger is fully depressed to ensure complete delivery and minimize leakage. Withdraw the needle and apply gentle pressure with a cotton ball or gauze if needed.
Rotate injection sites with each dose. The best injection site for weight loss is less about location and more about consistency. Pick a rotation pattern and stick with it. Many users find the abdomen most comfortable and accessible.
The best time of day to inject depends on your personal schedule and when side effects are most manageable. Some users prefer morning injections to ride out any nausea during the day. Others prefer evening injections so they can sleep through the peak side effect window. Experiment to find what works best for your body and routine.
Diet and lifestyle considerations during treatment
Cyanocobalamin tirzepatide changes your relationship with food. Dramatically. Understanding how to eat and live while on this compound is just as important as getting the dosing right.
What to eat on tirzepatide
What to eat on tirzepatide is a question that every user asks eventually. When your appetite is suppressed and meals feel like a chore, making every bite count becomes essential. Prioritize protein. Adequate protein intake is critical for preserving lean muscle mass during rapid weight loss. Aim for at least 0.7 to 1 gram of protein per pound of ideal body weight daily.
A structured tirzepatide diet plan helps ensure you hit your nutritional targets even when you do not feel hungry. Focus on nutrient-dense foods. Lean proteins, colorful vegetables, healthy fats, and complex carbohydrates. Avoid empty calories. When you are eating 800 to 1,200 calories per day because of appetite suppression, there is no room for nutritionally void foods.
Foods to avoid on tirzepatide include greasy, fried, and high-fat foods that can worsen nausea. Carbonated beverages can increase bloating. Very spicy foods may exacerbate GI symptoms. And large meals overwhelm the slowed digestive system, so eating smaller, more frequent meals is almost always better tolerated.
Alcohol on tirzepatide deserves specific mention. Many users find their alcohol tolerance dramatically reduced. Blood sugar fluctuations can be amplified. Dehydration risk increases. And the calories from alcohol are particularly wasteful when your total caloric intake is already limited. Most clinicians recommend significantly reducing or eliminating alcohol during active tirzepatide therapy.
For meal inspiration, GLP-1 breakfast ideas, dinner ideas, and recipes for weight loss can help you build a sustainable eating pattern that supports your weight loss while maintaining nutrition.
How tirzepatide compares to other weight loss peptides
Understanding where cyanocobalamin tirzepatide sits in the broader landscape of weight loss peptides helps you evaluate whether it is the right choice for your goals.
Tirzepatide versus semaglutide
The most common comparison. Semaglutide activates only the GLP-1 receptor. Tirzepatide activates both GLP-1 and GIP receptors. Clinical trial data consistently shows tirzepatide producing greater average weight loss than semaglutide, though individual results vary widely. The side effect profiles are similar between the two, with GI symptoms being the most common for both.
Semaglutide also has B12-containing compound versions. Semaglutide with B12 carries similar concerns about potential interactions, though the Lilly testing focused specifically on tirzepatide. Semaglutide methylcobalamin formulations, semaglutide glycine B12 blends, and semaglutide B12 dosage charts are all available through compounding pharmacies.
For people considering switching from tirzepatide to semaglutide or vice versa, the decision should be based on efficacy, tolerability, cost, and availability rather than on the B12 additive, since both compounds have B12-containing versions with the same potential concerns.
Can you take semaglutide and tirzepatide together? This is not standard practice and is generally not recommended, as both drugs work on the GLP-1 receptor and combining them would likely amplify side effects without proportional additional benefit.
Emerging alternatives
Retatrutide is a triple receptor agonist (GIP, GLP-1, and glucagon) currently in clinical trials that has shown even greater weight loss than tirzepatide in early data. Mazdutide is another dual-agonist in development. Both represent the next generation of incretin-based weight loss medications.
Traditional weight loss medications like phentermine work through completely different mechanisms (central nervous system stimulation rather than incretin mimicry) and offer a different risk-benefit profile.
For a broader view of peptide-based approaches to weight management, the best peptides for weight loss guide covers the full spectrum of options.
Results and what to expect
Setting realistic expectations about what cyanocobalamin tirzepatide can and cannot do for your body is essential for maintaining motivation and making informed decisions about continuing treatment.
Weight loss timeline
The tirzepatide weight loss timeline varies between individuals, but general patterns emerge from clinical trial data and real-world experience. Most people notice appetite suppression within the first week of their initial 2.5mg dose. Meaningful weight loss, usually at least 5 pounds, typically appears within the first four weeks.
How long does it take for tirzepatide to work? The pharmacological effects begin immediately, but visible results take time. The first month is often about adjustment, not dramatic transformation. Real momentum builds during months two through six as doses titrate up and cumulative fat loss becomes visible.
Before and after results from real users show tremendous variability. Some people lose 15% of their body weight. Others lose 25% or more. Genetics, starting weight, adherence to dietary recommendations, physical activity, sleep quality, stress management, and a dozen other factors influence individual outcomes.
Documented weight loss results from the SURMOUNT-1 trial showed average losses of 34.4 pounds at the 5mg dose, 49 pounds at the 10mg dose, and 52 pounds at the 15mg dose over 72 weeks. Men and women tend to show similar percentage-based weight loss, though men often lose more absolute weight due to higher starting weights.
Does tirzepatide actually burn fat?
Does tirzepatide burn fat or just suppress appetite? Both. The appetite suppression is the most obvious mechanism, reducing caloric intake by 20 to 40% in most users. But tirzepatide also appears to influence metabolism directly. Research suggests it increases metabolic rate to some degree, though the exact magnitude is debated. The GIP receptor activation may specifically influence how the body handles fat storage and mobilization, providing a metabolic advantage beyond simple caloric restriction.
Maintaining results long-term
Maintaining weight loss after tirzepatide is one of the biggest challenges. Studies show that patients who stop tirzepatide tend to regain a significant portion of their lost weight within a year. This has led to the understanding that obesity is a chronic condition requiring ongoing management, similar to hypertension or diabetes.
Some patients transition to maintenance doses rather than stopping entirely. Others develop the dietary and exercise habits during treatment that allow them to maintain results independently. Weaning off tirzepatide gradually rather than stopping abruptly may help with the transition, and approaches like microdosing tirzepatide have gained interest as a potential maintenance strategy.
Frequently asked questions
What makes cyanocobalamin tirzepatide pink?
The pink to light red color comes from the cyanocobalamin (vitamin B12) in the formulation. The cobalt-corrin ring structure of B12 absorbs certain wavelengths of light and reflects back in the pink-red spectrum. The intensity of the color corresponds to the B12 concentration. Higher concentrations produce deeper pink. Lower concentrations produce a lighter, more translucent pink. Pure tirzepatide without B12 is clear and colorless.
Is cyanocobalamin the same as methylcobalamin in tirzepatide compounds?
No. Both are forms of vitamin B12, but they differ structurally. Cyanocobalamin has a cyanide group attached to its cobalt center and must be converted by the body into active forms before it can be used. Methylcobalamin already carries a methyl group and is bioactive without conversion. In the context of tirzepatide compounds, cyanocobalamin is more stable in solution, but both forms have been implicated in the impurity concerns raised by Eli Lilly testing. The choice between them may matter less than whether any form of B12 should be combined with tirzepatide at all.
Should I switch away from cyanocobalamin tirzepatide after the Lilly warning?
That is a decision to make with your prescribing provider based on your individual risk tolerance and health status. The Lilly testing found impurities from a chemical reaction between tirzepatide and B12 with unknown safety profiles. Some providers are recommending a switch to B12-free formulations like tirzepatide with niacinamide or tirzepatide with glycine. Others are maintaining current prescriptions while awaiting independent verification. Discuss your specific situation with your provider.
Can I take B12 separately instead of in the compound?
Yes, and many clinicians now recommend this approach. Oral cyanocobalamin or methylcobalamin supplements taken daily, sublingual B12 tablets, or standalone B12 injections on a different day from your tirzepatide all provide adequate B12 supplementation without the interaction risk. This is the simplest way to get the benefits of both compounds without combining them in the same vial.
How do I know if my compounding pharmacy is reputable?
Look for 503B outsourcing facility registration with the FDA, willingness to provide certificates of analysis for each batch, potency and sterility testing on every lot, transparent sourcing of raw materials, appropriate cold chain shipping, and realistic beyond-use dating supported by stability data. Avoid pharmacies that cannot answer basic questions about their quality control processes or that offer prices dramatically below market rates.
What is the correct storage temperature for cyanocobalamin tirzepatide?
Store between 36 and 46 degrees Fahrenheit (2 to 8 degrees Celsius) in your refrigerator. Keep it away from light, in the original packaging or wrapped in foil if the vial is clear glass. Do not freeze. Allow the vial to reach room temperature for 15 to 20 minutes before injecting for comfort, but return it to the refrigerator promptly after drawing your dose. Follow the peptide storage guide principles and the specific dating on your vial.
Does the cyanocobalamin in the compound really help with energy?
For people with genuine B12 deficiency or suboptimal levels, supplemental B12 can meaningfully improve energy levels, mental clarity, and exercise tolerance. For people with already adequate B12 levels, additional B12 supplementation provides minimal benefit since the body simply excretes what it does not need. Blood testing can determine your baseline B12 status and help predict whether the supplementation component is likely to benefit you personally.
Is the trace cyanide in cyanocobalamin dangerous?
At supplemental doses, no. The amount of free cyanide released during cyanocobalamin metabolism is far below any toxicologically significant level. The body detoxifies these trace amounts through the rhodanese enzyme pathway, converting cyanide to thiocyanate which is excreted in urine. The only population that might warrant extra caution is people with severe kidney disease who have impaired excretion capacity. For everyone else, the cyanide component of cyanocobalamin is clinically irrelevant at standard B12 supplementation doses.
External resources
FDA compounding questions and answers - Official FDA guidance on compounded medications and regulatory framework
SURMOUNT-1 trial results (NEJM) - Pivotal clinical trial data on tirzepatide for weight management
NIH vitamin B12 fact sheet - Comprehensive reference on B12 forms, requirements, and deficiency
National Association of Boards of Pharmacy - Verify pharmacy licensing and accreditation status
USP compounding standards - Quality standards for compounded preparations including beyond-use dating
SeekPeptides members get access to regularly updated safety alerts, detailed compound comparisons, dosing protocol guides, and the tools needed to navigate the compounded peptide landscape with confidence. When formulations evolve and safety data changes, having a trusted resource that keeps pace matters. The reconstitution calculator, peptide calculator, and dosage calculator are available free of charge, and membership unlocks the full library of protocols, safety guides, and compound analyses that turn confusion into clarity.
In case I do not see you, good afternoon, good evening, and good night.