Mar 22, 2026

What if the number on your syringe does not actually tell you how much tirzepatide you are injecting? That is the reality for anyone drawing 100 units from a compounded vial. The answer to "how many mg is 100 units of tirzepatide" is not a single number. It depends entirely on one critical variable that too many people overlook: the concentration printed on your vial label.
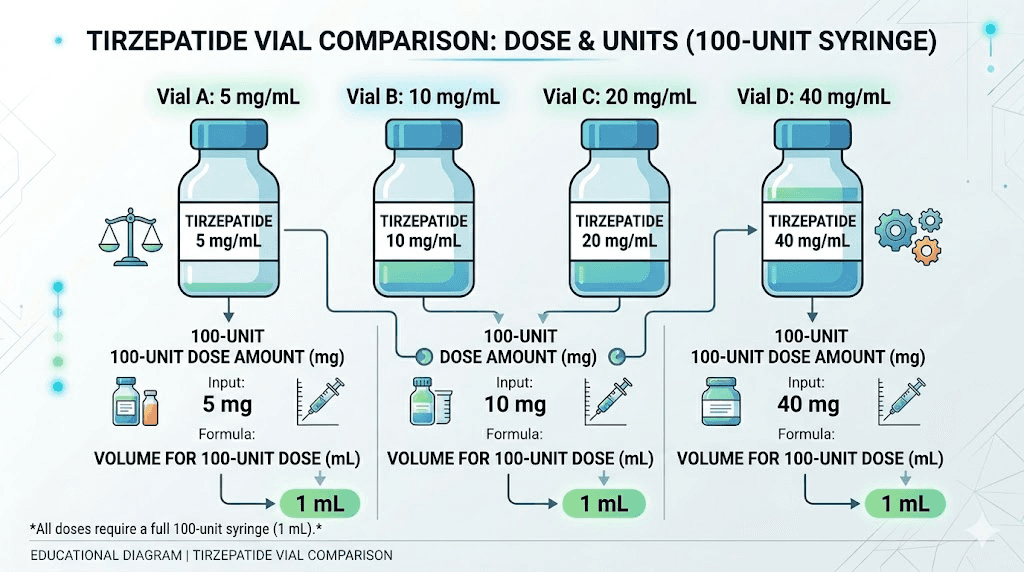
At a 5 mg/mL concentration, 100 units equals 5 mg. At 10 mg/mL, that same 100 units becomes 10 mg. Double the concentration. At 20 mg/mL, you are looking at 20 mg. And at 40 mg/mL, 100 units delivers a massive 40 mg, a dose far beyond what most protocols recommend. Same syringe reading. Wildly different doses. This distinction is not academic. It is the difference between a therapeutic dose and a dangerous one.
This guide breaks down every concentration you will encounter, walks through the math step by step, and shows you exactly how to verify your dose before every injection. Whether you are using a compounded tirzepatide dosage calculator or doing the conversion manually, understanding this relationship between units, milliliters, and milligrams will keep your dosing accurate and your protocols safe. SeekPeptides has helped thousands of researchers navigate exactly this kind of confusion, and the information ahead covers everything you need to know.
Why 100 units does not have a single mg answer
This is where most confusion starts. People search for a definitive number, expecting something clean like "100 units equals 10 mg." But that answer only works at one specific concentration. Change the concentration, and the entire calculation changes with it.
Units on an insulin syringe measure volume, not drug strength. One hundred units equals exactly 1 milliliter of liquid. Always. Regardless of what medication is inside that syringe. The syringe does not know or care whether it contains 5 mg of tirzepatide or 40 mg. It simply measures how much liquid you have drawn up.
The milligrams come from the concentration. A vial labeled 10 mg/mL contains 10 milligrams of tirzepatide dissolved in every milliliter of solution. Draw 1 mL (100 units), and you get 10 mg. Draw half a milliliter (50 units), and you get 5 mg. The math is straightforward once you understand the relationship. But missing this concept leads to dosing errors that can range from ineffective treatments to genuinely dangerous overdoses.
Compounding pharmacies produce tirzepatide at various concentrations. The four most common are 5 mg/mL, 10 mg/mL, 20 mg/mL, and 40 mg/mL. Each one changes what 100 units means in terms of actual medication delivered. If you have been following a tirzepatide dosing for weight loss in units guide without checking your vial concentration, you may have been taking the wrong dose all along.
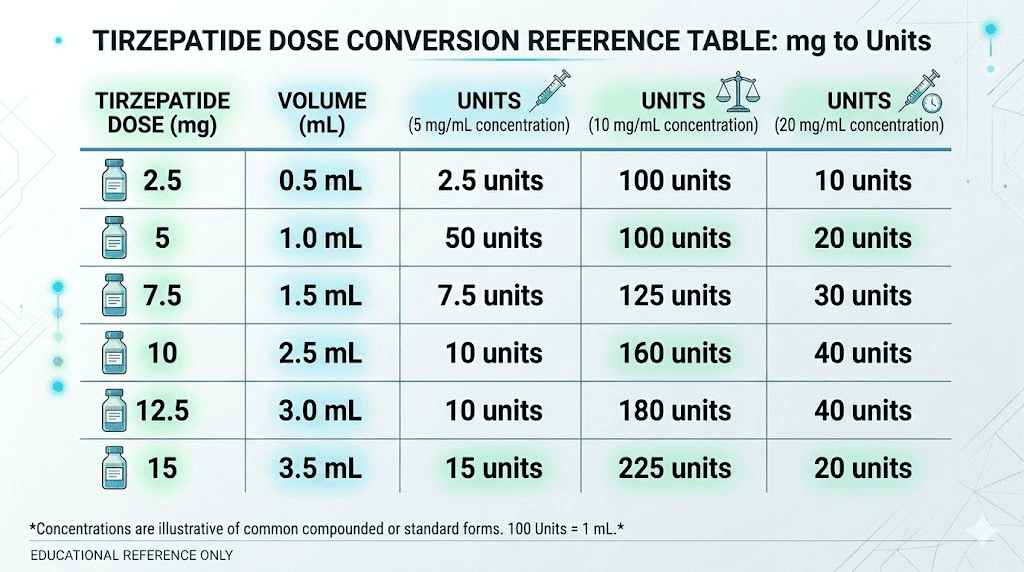
The complete conversion table: 100 units at every concentration
Here is the definitive answer. Find your vial concentration in the left column, and the right column tells you exactly how many milligrams 100 units delivers.
Vial concentration | 100 units equals | How it compares to standard doses |
|---|---|---|
5 mg/mL | 5 mg | Standard therapeutic dose (weeks 5-8 in FDA protocol) |
10 mg/mL | 10 mg | Higher therapeutic dose (weeks 9-12 in FDA protocol) |
20 mg/mL | 20 mg | Above maximum FDA-approved dose of 15 mg |
40 mg/mL | 40 mg | Far above any recommended protocol |
The pattern is simple. Whatever number appears before "mg/mL" on your vial label, that is how many milligrams you get when you draw 100 units. A 5 mg/mL vial gives 5 mg. A 20 mg/mL vial gives 20 mg. The concentration number and the milligram dose at 100 units are always identical, because 100 units equals exactly 1 mL.
This is critical for anyone transitioning between vials. If your pharmacy sends a 20 mg/mL vial to replace your usual 10 mg/mL vial, drawing your usual number of units will give you double the dose. People have ended up in emergency rooms because of exactly this mistake. Always check the label. Every single time you open a new vial. No exceptions.
For reference on how other unit amounts convert, see our guides on how many mg is 20 units of tirzepatide, how many mg is 30 units, how many mg is 40 units, and how many mg is 50 units of tirzepatide.
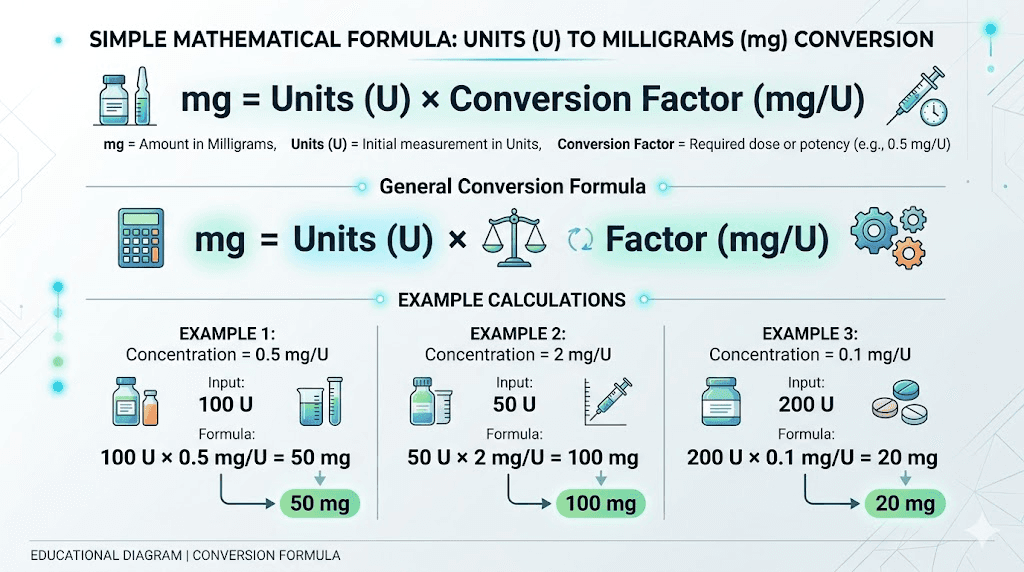
Understanding the formula behind the conversion
You do not need to be a mathematician. The formula is one line:
Milligrams = (Units / 100) x Concentration (mg/mL)
That is it. Divide your units by 100 to get milliliters. Multiply by the concentration to get milligrams. For 100 units, the math is even simpler because 100 divided by 100 is 1. So you are just multiplying 1 by whatever your concentration is.
Worked example at 5 mg/mL
Your vial reads 5 mg/mL. You draw 100 units on your insulin syringe. Plug those numbers into the formula: (100 / 100) x 5 = 1 x 5 = 5 mg. You are injecting 5 milligrams. This falls within the standard tirzepatide dose chart range for weeks 5 through 8 of a typical protocol.
Worked example at 10 mg/mL
Same syringe, same 100 units. Different vial: 10 mg/mL. The math: (100 / 100) x 10 = 1 x 10 = 10 mg. That is double the previous example. Ten milligrams is a significant dose, typically reserved for patients who have already titrated through lower amounts. If you are on a compounded tirzepatide starting dose, this would be far too much for a first injection.
Worked example at 20 mg/mL
Now things get serious. A 20 mg/mL vial at 100 units: (100 / 100) x 20 = 20 mg. Twenty milligrams exceeds the maximum FDA-approved dose of 15 mg for tirzepatide (Zepbound/Mounjaro). While some compounded protocols push beyond this, drawing a full 100 units from a 20 mg/mL vial without medical supervision is not recommended. Understanding the tirzepatide dosage in units at this concentration is essential for anyone using higher-concentration vials.
Worked example at 40 mg/mL
This concentration exists primarily for patients on high maintenance doses who want smaller injection volumes. At 100 units: (100 / 100) x 40 = 40 mg. This is not a typical dose for anyone. If you find yourself drawing 100 units from a 40 mg/mL vial, something has almost certainly gone wrong in your dosing calculations. Stop and recalculate before injecting.
How to identify your vial concentration
The concentration is printed directly on the vial label. Look for a number followed by "mg/mL" or "mg per mL." This is the single most important piece of information on that label for dosing purposes.
Some labels make it easy. They print the concentration in large, bold text. Others bury it among lot numbers, expiration dates, and pharmacy information. Regardless of label design, find this number before you draw your first dose from any new vial.
Here is what to look for on compounded tirzepatide labels:
Concentration statement: "Tirzepatide 10 mg/mL" or similar
Total content: Some labels show "50 mg/5 mL" which means 10 mg per mL
NDC or compound ID: This does not tell you the concentration but identifies the specific preparation
If the label shows total content like "100 mg/5 mL" instead of a per-milliliter concentration, divide the total milligrams by the total volume. In this case, 100 mg divided by 5 mL equals 20 mg/mL. That is your concentration. Use that number in your calculations.
When you receive a new vial, compare the concentration to your previous one. If it differs, you must recalculate your units. Do not assume every vial from the same pharmacy will have the same concentration. Pharmacies sometimes change formulations, switch suppliers, or send different concentrations based on availability. Your tirzepatide syringe dosage must match the specific vial in your hand, not a number you memorized from last month.
Common compounded tirzepatide concentrations explained
Not all concentrations serve the same purpose. Each one exists for a reason, and understanding why helps you work with your provider to choose the right option.
5 mg/mL: the starter concentration
This is the most forgiving concentration for new users. At 5 mg/mL, small changes in units translate to small changes in milligrams. Drawing 10 extra units by mistake only adds 0.5 mg to your dose. For someone following a microdosing tirzepatide chart, this concentration offers the finest control over small doses.
The trade-off is volume. Higher doses require larger injection volumes. A 15 mg dose at 5 mg/mL requires 3 mL of liquid, which means three separate 100-unit injections or switching to a larger syringe. Most people find this impractical beyond the 10 mg dose range.
At this concentration, 100 units gives you 5 mg. That is the standard dose for weeks 5 through 8 of the FDA titration schedule. A reasonable, moderate amount for someone who has already spent four weeks at 2.5 mg.
10 mg/mL: the most common concentration
This is the workhorse. Ten mg/mL strikes the ideal balance between precision and convenience. Every standard dose from 2.5 mg through 10 mg fits within a single 1 mL (100-unit) syringe. The unit readings come out to clean, round numbers that are easy to identify on the syringe barrel.
Here is what the common doses look like at 10 mg/mL:
Target dose | Units to draw |
|---|---|
2.5 mg | 25 units |
5 mg | 50 units |
7.5 mg | 75 units |
10 mg | 100 units |
Clean numbers. Easy to read. Hard to mess up. That is why most compounding pharmacies default to this concentration. If you are exploring how many units is 2.5 mg of tirzepatide, the answer at 10 mg/mL is a straightforward 25 units. For 5 mg in units, that is 50. Simple.
At 100 units from this concentration, you are getting 10 mg. This is a therapeutic dose in the higher range, appropriate for people who have been titrating for at least 8 weeks and tolerate the medication well.
20 mg/mL: the high-concentration option
Twenty mg/mL concentrations exist for patients on higher doses who want smaller injection volumes. Instead of injecting 1.5 mL for a 15 mg dose (which would be 150 units at 10 mg/mL and require overfilling a standard syringe), a 20 mg/mL vial lets you draw just 75 units for the same 15 mg.
The downside is reduced margin for error. Each unit now carries twice as much medication compared to 10 mg/mL. Drawing 5 extra units adds a full milligram to your dose instead of half a milligram. Precision matters more at this concentration.
At 100 units from a 20 mg/mL vial, you would be injecting 20 mg. That exceeds the maximum approved dose. If you are drawing 100 units from this concentration, double check with your prescriber. Most protocols cap tirzepatide at 15 mg weekly, though some researchers explore higher amounts under careful supervision. Review the complete tirzepatide dosing guide for standard protocols.
40 mg/mL: the specialty concentration
This concentration is less common and typically reserved for patients on maintenance doses who want minimal injection volume. A 15 mg dose requires only 37.5 units. Even a 10 mg dose is just 25 units, a tiny volume that some patients prefer.
But the risk profile is significantly higher. A 10-unit error at 40 mg/mL means a 4 mg dosing mistake. That is the difference between a 10 mg dose and a 14 mg dose with one small slip of the thumb on the syringe plunger. For this reason, 40 mg/mL is not recommended for anyone new to self-injection or anyone without experience reading insulin syringes accurately.
One hundred units at 40 mg/mL would deliver 40 mg of tirzepatide. This is far beyond any standard protocol and would almost certainly cause severe gastrointestinal side effects including constipation, diarrhea, intense nausea, and potentially dangerous complications. There is no legitimate protocol that calls for 40 mg in a single injection.
The reverse calculation: how many units for your prescribed dose
Most people actually need to work the formula backwards. Your provider prescribes a dose in milligrams, and you need to figure out how many units to draw. The reverse formula is just as simple:
Units = (Dose in mg / Concentration in mg/mL) x 100
Let us walk through the most commonly prescribed doses at each concentration.
2.5 mg (the starting dose)
Concentration | Units to draw for 2.5 mg |
|---|---|
5 mg/mL | 50 units |
10 mg/mL | 25 units |
20 mg/mL | 12.5 units |
40 mg/mL | 6.25 units |
Notice how the higher concentrations produce awkward fractional units. Drawing exactly 6.25 units on an insulin syringe is nearly impossible. This is one reason why 5 mg/mL and 10 mg/mL concentrations are preferred for lower starting doses. If your compounded tirzepatide starting dose is 2.5 mg, a 10 mg/mL vial gives you the cleanest measurement at 25 units.
5 mg (standard escalation dose)
Concentration | Units to draw for 5 mg |
|---|---|
5 mg/mL | 100 units (full syringe) |
10 mg/mL | 50 units |
20 mg/mL | 25 units |
40 mg/mL | 12.5 units |
At 5 mg/mL, a 5 mg dose requires the full 100 units (1 mL). This is important because you cannot go higher than 5 mg with this concentration without using more than one syringe or switching to a larger syringe type. For 5 mg tirzepatide in units at 10 mg/mL, you need exactly 50 units, right at the halfway mark of your syringe.
7.5 mg (intermediate dose)
Concentration | Units to draw for 7.5 mg |
|---|---|
5 mg/mL | 150 units (exceeds standard syringe) |
10 mg/mL | 75 units |
20 mg/mL | 37.5 units |
40 mg/mL | 18.75 units |
Here you can see why 5 mg/mL becomes impractical at higher doses. A 150-unit draw does not fit in a standard 100-unit insulin syringe. You would need a 1 mL TB syringe or two separate injections. The 10 mg/mL concentration handles this dose well at 75 units. Check our guide on how many units is 7.5 mg of tirzepatide for more detail on this specific conversion.
10 mg (higher therapeutic dose)
Concentration | Units to draw for 10 mg |
|---|---|
10 mg/mL | 100 units (full syringe) |
20 mg/mL | 50 units |
40 mg/mL | 25 units |
At 10 mg/mL, a 10 mg dose uses the entire syringe. This is one of the most common scenarios where people draw exactly 100 units. If you are reading this guide because you were told to draw 100 units from a 10 mg/mL vial, your dose is 10 mg. Confirmed. For context on this dose level, see our complete 10 mg tirzepatide unit conversion guide.
15 mg (maximum FDA-approved dose)
Concentration | Units to draw for 15 mg |
|---|---|
10 mg/mL | 150 units (exceeds standard syringe) |
20 mg/mL | 75 units |
40 mg/mL | 37.5 units |
Fifteen milligrams is the maximum dose approved by the FDA for tirzepatide. At 10 mg/mL, this dose exceeds a standard insulin syringe capacity. This is the primary reason pharmacies offer 20 mg/mL and 40 mg/mL concentrations, to keep the 15 mg dose within a single syringe. Our 15 mg conversion guide covers this in detail.
Insulin syringes vs TB syringes: a critical safety distinction
This is where dosing errors become dangerous. Insulin syringes and TB (tuberculin) syringes look almost identical. Both are small. Both have thin needles. Both measure small volumes. But they use different scales, and confusing the two can lead to massive overdoses.
An insulin syringe measures in units. One hundred units equals 1 mL. The markings on the barrel count up in units: 10, 20, 30, all the way to 100.
A TB syringe measures in milliliters. It typically marks in tenths of a milliliter: 0.1, 0.2, 0.3, up to 1.0 mL. Some TB syringes also show hundredths (0.01 mL increments).
Here is where the danger lies. If someone reads a TB syringe the same way they would read an insulin syringe, interpreting the "25" mark as 25 units, they could actually be drawing 0.25 mL on one scale or 2.5 mL on another depending on the syringe markings. With a 10 mg/mL concentration, 2.5 mL would deliver 25 mg of tirzepatide. That is roughly double the maximum recommended dose from a single injection.
Always use the syringe type your provider specifies. If they prescribed in units, use an insulin syringe. If they prescribed in milliliters, use a TB syringe. Never mix the two without recalculating. When learning to inject tirzepatide properly, the syringe type is one of the first things to verify.
How to verify your syringe type
Check the packaging. Insulin syringes will say "insulin syringe" or show a "U-100" designation. TB syringes will say "tuberculin" or simply show mL markings.
Look at the barrel markings. If the largest number on the barrel is 100 and the label mentions "units," it is an insulin syringe. If the largest number is 1.0 and the label mentions "mL," it is a TB syringe.
When in doubt, ask your pharmacist. This five-second conversation could prevent a serious dosing error. The difference between getting your tirzepatide syringe dosage right and getting it dangerously wrong often comes down to which syringe is in your hand.
Reading your insulin syringe correctly
Even with the right syringe, reading errors happen. Here are the most common mistakes and how to avoid them.
Parallax error
Looking at the syringe from above instead of straight on causes a consistent misread. The plunger appears to be at a different position depending on your viewing angle. Always hold the syringe at eye level with the barrel horizontal. Read the marking where the top of the plunger rubber meets the barrel wall. Not the bottom of the rubber. Not the top of the syringe. The point where rubber meets glass (or plastic), read straight on.
Air bubble displacement
A 5-unit air bubble trapped below the plunger means you are only injecting 95 units of actual medication, not 100. That is a 5% dose reduction. Over time, these small reductions add up. Before every injection, tap the syringe gently to move air bubbles to the needle end, then push the plunger slightly to expel the air. Recheck your unit reading after removing the bubbles.
Marking increments
Standard 100-unit insulin syringes have major markings every 10 units and minor markings every 2 units. That means each small line represents 2 units, not 1. If you are trying to draw an odd number of units (say 25), you need to position the plunger between the 24 and 26 marks. This is harder than it sounds, which is why the 10 mg/mL concentration with its clean multiples of 25 units is so popular.
Some 100-unit syringes have markings every 1 unit (100 individual lines). These are easier to read for precise doses. If your prescribed dose does not fall on an even number, ask your pharmacy for 1-unit increment syringes. Accurate measurement matters whether you are following a standard protocol or a microdose tirzepatide schedule.
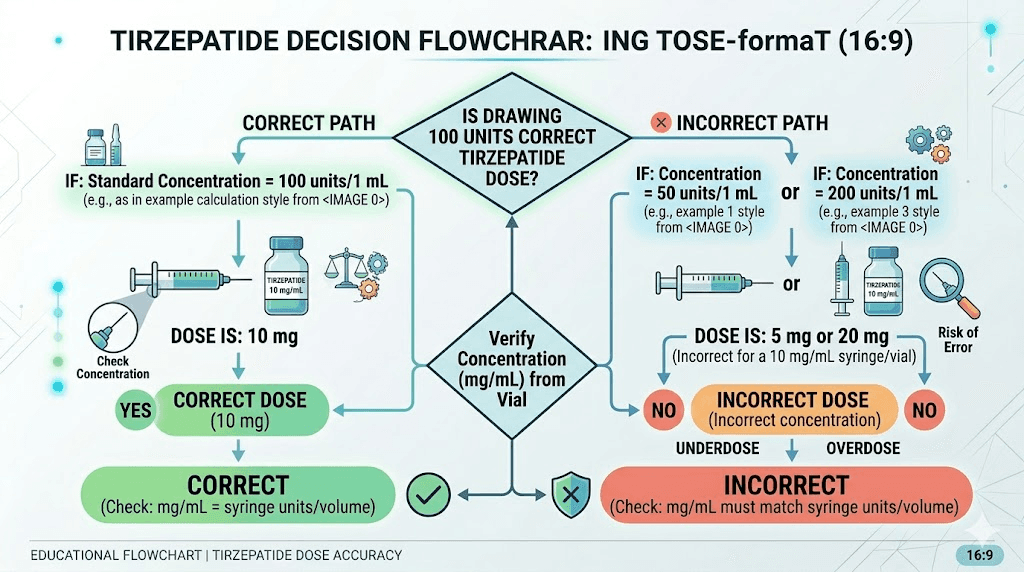
When would someone actually draw 100 units of tirzepatide?
Drawing a full 100 units (1 mL) is common in several scenarios. Understanding whether your situation is one of them helps confirm your dose is correct.
Scenario 1: 5 mg dose from a 5 mg/mL vial
You are on 5 mg weekly. Your vial is 5 mg/mL. Drawing 100 units gives you exactly 5 mg. This is a standard, appropriate dose for someone in weeks 5 through 8 of a tirzepatide protocol. Perfectly normal. No cause for concern.
Scenario 2: 10 mg dose from a 10 mg/mL vial
This is probably the most common reason someone draws 100 units. Ten milligrams from a 10 mg/mL vial equals a full syringe. This dose is appropriate for someone who has been titrating for at least 8 weeks and tolerates the medication well. If you are seeing tirzepatide before and after results at lower doses, your provider may increase you to this level for continued progress.
Scenario 3: 20 mg dose from a 20 mg/mL vial
This exceeds the maximum FDA-approved dose. While some compounded protocols use 20 mg, this should only happen under direct medical supervision. If your provider specifically prescribed 20 mg and your vial is 20 mg/mL, then 100 units is technically correct. But confirm with your provider before proceeding.
Scenario 4: a dosing error
If your prescribed dose is 2.5 mg and your vial is 10 mg/mL, your correct draw is 25 units, not 100. Drawing 100 units would give you 10 mg, four times your prescribed dose. This kind of error happens more often than anyone wants to admit, especially when people change vials or pharmacies. If your syringe is at 100 units and that number does not match your prescribed dose and concentration, stop. Recalculate. Review the compounded tirzepatide dosage calculator to verify.
How tirzepatide dosing compares to semaglutide at 100 units
Many people switch between tirzepatide and semaglutide, or compare the two before starting treatment. The unit-to-mg conversion works identically for both medications, because units always measure volume, not drug potency. But the concentrations and typical doses differ significantly.
Semaglutide is commonly compounded at concentrations like 2.5 mg/mL and 5 mg/mL. At 5 mg/mL, 100 units of semaglutide gives you 5 mg, the same math as tirzepatide. Our guide on 100 units of semaglutide is how many mg covers this conversion in detail.
The key difference is that semaglutide maximum dose (2.4 mg for weight management) is much lower than tirzepatide maximum dose (15 mg). So while 100 units of semaglutide at 5 mg/mL delivers more than double the maximum recommended dose, 100 units of tirzepatide at 10 mg/mL delivers a dose within the approved range. Same units, same syringe, very different clinical implications.
For a detailed comparison of dosing between these two GLP-1 medications, see our tirzepatide vs semaglutide dosage chart and the semaglutide to tirzepatide conversion chart. If you are considering switching between them, our guide on switching from tirzepatide to semaglutide covers what to expect.
Understanding how semaglutide dosing works in units can provide helpful context. Guides on semaglutide dosage in units, semaglutide units to mg conversion, and specific conversions like how many mg is 40 units of semaglutide or 20 units of semaglutide in mg all use the same fundamental formula.
Reconstitution and how it affects concentration
If you are working with lyophilized (freeze-dried) tirzepatide powder rather than a pre-mixed liquid, the concentration depends entirely on how much bacteriostatic water you add. This is where many dosing errors originate.
The formula for determining concentration after reconstitution:
Concentration (mg/mL) = Total mg in vial / Volume of water added (mL)
For a 10 mg vial:
Water added | Resulting concentration | 100 units equals |
|---|---|---|
1 mL | 10 mg/mL | 10 mg |
2 mL | 5 mg/mL | 5 mg |
0.5 mL | 20 mg/mL | 20 mg |
The same 10 mg vial produces completely different concentrations depending on how much water you add. Add 1 mL and 100 units gives you 10 mg. Add 2 mL and 100 units gives you only 5 mg. Add just 0.5 mL and 100 units gives you the full 20 mg.
This is why proper tirzepatide reconstitution is critical. The amount of bacteriostatic water you use determines your concentration, which determines how many milligrams each unit on your syringe represents. Our guide on how much bacteriostatic water to mix with 10 mg tirzepatide walks through this process step by step.
For reference, the same principle applies to other peptides. If you also use semaglutide, see how to reconstitute semaglutide and how much bacteriostatic water to mix with 10 mg semaglutide. The math is the same. The peptide reconstitution calculator on SeekPeptides handles all of this automatically if you prefer not to do the math manually.
Safety considerations for high-unit draws
Drawing 100 units means you are using the full capacity of a standard insulin syringe. This comes with specific safety considerations that smaller draws do not have.
No room for error in the upward direction
With a 50-unit draw, if you accidentally pull past your target, you have room to push back. With a 100-unit draw, there is no room above 100. Overfilling a syringe can cause the plunger to pop out, wasting medication and creating a mess. It can also mean you injected slightly more than 100 units before noticing the overfill.
Injection volume discomfort
One milliliter is a relatively large subcutaneous injection. Some people experience more discomfort, redness, or swelling at the injection site with larger volumes. If you are noticing injection site reactions from tirzepatide, the volume itself could be contributing.
Splitting the dose into two smaller injections at different sites can reduce discomfort. Instead of one 100-unit injection, try two 50-unit injections in different locations. The total dose remains the same, but each individual injection is smaller and generally better tolerated. This approach works well for anyone learning how to inject tirzepatide in the stomach or other sites.
Side effect intensity at higher doses
If 100 units represents a higher dose than you have taken before (for example, moving from 50 units to 100 units at the same concentration), expect potentially stronger side effects. Common effects that intensify with dose increases include nausea, constipation, headaches, body aches, and fatigue.
Managing these side effects is essential for staying on protocol. Dietary adjustments help significantly. Our guides on foods to avoid on tirzepatide and what to eat on tirzepatide cover nutrition strategies that reduce gastrointestinal discomfort. Supplements to take with tirzepatide can also make a significant difference in tolerability.
Overdose recognition
If you accidentally injected 100 units when you should have drawn less, knowing the signs of an overdose matters. Severe nausea, vomiting, abdominal pain, and dizziness are the most common symptoms. Because tirzepatide has a long half-life of approximately 5 days, symptoms from an overdose can persist for several days.
Do not induce vomiting or take additional medications without medical guidance. Contact your healthcare provider or Poison Control (1-800-222-1222) immediately. There is no specific antidote for tirzepatide overdose, but supportive care is generally effective when administered promptly.
Storing your tirzepatide vial for accurate dosing over time
Storage affects concentration stability. A degraded vial may not deliver the expected milligrams per unit, even if your math is perfect.
Compounded tirzepatide should be refrigerated at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). Temperature excursions, leaving the vial out on the counter, traveling without a cold pack, or storing it in a warm bathroom, can degrade the peptide and reduce its potency.
How long does it last? Our guide on how long tirzepatide lasts in the fridge covers shelf life in detail. If your vial has been left out of the fridge for extended periods, the concentration may have dropped, meaning 100 units delivers less than the labeled amount. Check tirzepatide expiration guidelines to know when to discard a vial.
Proper storage ensures that when you draw 100 units from a 10 mg/mL vial, you are actually getting close to 10 mg of active medication. Degraded peptides still look the same in the vial. You cannot see potency loss. Trust the storage requirements, not the appearance.
Compounded vs brand-name tirzepatide: does the conversion change?
The math does not change. Units always equal volume, and concentration always determines milligrams. But there are practical differences worth noting.
Brand-name tirzepatide (Mounjaro, Zepbound) comes in pre-filled pens with fixed doses. You do not measure units. The pen delivers a set amount (2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, or 15 mg) with each click. No syringe reading required.
Compounded tirzepatide comes in multi-dose vials requiring you to draw the correct amount with an insulin syringe. This is where concentration knowledge matters. The flexibility of compounded tirzepatide, including the ability to microdose or use non-standard doses, comes with the responsibility of accurate measurement.
Some people switch from brand-name pens to compounded vials for cost savings. If this describes you, the affordable tirzepatide guide and cheap compounded tirzepatide overview can help you navigate options. Just remember that moving from a pen (where the dose is automatic) to a vial (where you measure manually) introduces the possibility of dosing errors. The 100-unit question becomes very relevant at that point.
Compounded tirzepatide may also include additional ingredients. Formulations with vitamin B12, glycine, or niacinamide are increasingly common. These additives do not change the tirzepatide concentration or the units-to-mg conversion. The concentration listed on the label refers specifically to the tirzepatide content.
Common mistakes people make with 100-unit draws
Awareness is the best prevention. Here are the mistakes that send people to forums asking what went wrong.
Mistake 1: assuming all vials are the same concentration
Your first vial was 10 mg/mL. You drew 50 units for your 5 mg dose. Then your pharmacy sent a 20 mg/mL vial. You drew 50 units out of habit. You just injected 10 mg instead of 5 mg. Double your intended dose.
Prevention: check the label on every new vial before your first draw. Write your calculated units on a sticky note and attach it to the vial.
Mistake 2: confusing the syringe type
Grabbing a TB syringe instead of an insulin syringe and interpreting the markings as units. This can result in drawing volumes that are 10 times what you intended, depending on the syringe scale.
Prevention: keep insulin syringes and TB syringes in separate locations. Verify the syringe type before drawing. Look for "units" on the insulin syringe packaging.
Mistake 3: not accounting for air bubbles
Your syringe shows 100 units, but 8 of those units are air, not medication. You are only injecting 92 units of liquid, which at 10 mg/mL means 9.2 mg instead of 10 mg. An 8% dose reduction.
Prevention: after drawing to 100 units, tap the syringe, expel air bubbles, then top off back to 100 units with actual liquid.
Mistake 4: using dosing information from the wrong source
Someone on a forum says "I draw 100 units weekly." You copy their protocol. But their vial is 5 mg/mL and yours is 20 mg/mL. They are taking 5 mg. You just took 20 mg. Four times their dose from the same number of units.
Prevention: never copy unit amounts from others without confirming matching concentrations. Always convert to milligrams first, then calculate your own units based on your specific vial concentration.
Mistake 5: not recalculating after reconstitution changes
You added 1 mL of bacteriostatic water to your first 10 mg vial (creating 10 mg/mL). Your next vial is 20 mg. You add 1 mL again, creating 20 mg/mL instead of 10 mg/mL. Drawing the same units now gives double the dose.
Prevention: calculate your target concentration before reconstitution. If you want consistent 10 mg/mL concentration, add 2 mL of water to a 20 mg vial, not 1 mL. The reconstitution calculator can verify your math.
Titration schedules and how 100 units fits into your protocol
Tirzepatide dosing follows a gradual escalation schedule. Nobody should start at 100 units from a 10 mg/mL vial (10 mg) on day one. The standard titration looks like this:
Weeks | Dose | Units at 10 mg/mL |
|---|---|---|
1-4 | 2.5 mg | 25 units |
5-8 | 5 mg | 50 units |
9-12 | 7.5 mg | 75 units |
13-16 | 10 mg | 100 units |
17-20 | 12.5 mg | 125 units (need higher concentration) |
21+ | 15 mg | 150 units (need higher concentration) |
At a 10 mg/mL concentration, 100 units (10 mg) typically enters the protocol around weeks 13 through 16. That is three months into treatment. Reaching this dose means you have successfully tolerated three dose increases and your body has adapted to the medication.
If you are still in the early weeks and wondering about the tirzepatide weight loss timeline, know that results often appear well before reaching the 100-unit mark. Many people see significant progress at 5 mg (50 units at 10 mg/mL) or 7.5 mg (75 units). Not everyone needs to escalate to 10 mg or beyond. Your timeline for tirzepatide to work depends on many factors including diet, activity level, and individual metabolism.
For those already at higher doses who feel the medication is losing effectiveness, our guide on tirzepatide not working anymore offers strategies before simply increasing to the next dose level. Similarly, if you are not losing weight on tirzepatide, the issue may not be dosage at all but rather dietary or lifestyle factors that need addressing.
Using a dosage calculator to verify your conversion
Manual math works, but human error is real. Especially at 6 AM before your morning coffee. A dosage calculator removes the risk of arithmetic mistakes.
The compounded tirzepatide dosage calculator takes your vial concentration and prescribed dose as inputs, then outputs the exact number of units to draw. No mental math. No formula to remember. Just enter your numbers and get your answer.
For broader peptide calculations, SeekPeptides offers a general peptide calculator that handles tirzepatide along with other peptides. The semaglutide dosage calculator is available for those also using or comparing semaglutide protocols.
Even if you prefer doing the math yourself, running your calculation through a calculator as a double-check takes seconds and could catch an error before it becomes a problem. Think of it as a safety net, not a replacement for understanding the formula.
What to do if you drew the wrong amount
Mistakes happen. Here is what to do depending on the situation.
You drew too much but have not injected yet
Simply push the plunger to expel the excess back into the vial, adjusting to your correct unit amount. No harm done. The medication returns to the vial.
You already injected too much
Do not panic, but do take it seriously. Calculate how much you actually injected using the formula. If you took double your prescribed dose or more, contact your healthcare provider. Symptoms to watch for include severe nausea, vomiting, dizziness, and abdominal pain. These typically peak 24 to 48 hours after injection and can persist for several days due to tirzepatide long half-life.
Stay hydrated. Eat small, bland meals. Monitor blood sugar if you have diabetes or are taking concurrent diabetes medications. Most overdose situations resolve with supportive care, but medical guidance is important for determining whether you should skip your next scheduled dose to compensate.
You injected too little
A sub-therapeutic dose is generally not dangerous. You may simply experience reduced appetite suppression that week. Do not take a supplementary injection to "make up" the difference. Wait until your next scheduled injection day and draw the correct amount. Taking extra injections outside your weekly schedule can increase side effects without improving outcomes. If this is a recurring concern, review whether taking tirzepatide a day early is appropriate for your situation.
Tirzepatide dosing and lifestyle factors
Getting the units-to-mg conversion right is only part of the equation. What you do around your injection affects how well the medication works and how you feel.
Diet matters enormously. Following a tirzepatide diet plan optimized for GLP-1 receptor agonists can reduce side effects and improve weight loss outcomes. A structured tirzepatide meal plan takes the guesswork out of nutrition while on the medication.
Alcohol interacts with tirzepatide by intensifying nausea and slowing gastric emptying further. If you are wondering whether you can drink on tirzepatide, the short answer is that moderation is key and some people find they need to significantly reduce or eliminate alcohol consumption while on the medication.
Sleep disruption is another consideration. Some users report insomnia on tirzepatide, particularly during dose escalation phases. If moving to 100 units represents a dose increase for you, monitor your sleep quality for the first few weeks.
For women, tirzepatide can affect menstrual cycles. Our guide on tirzepatide and periods covers what to expect. This is especially relevant for anyone concerned about fertility, as the guide on pregnancy on tirzepatide addresses an increasingly common scenario. Anyone breastfeeding while considering tirzepatide should consult their healthcare provider before starting.
Comparing your options: tirzepatide vs other GLP-1 medications
If you are evaluating tirzepatide against other options, understanding dosing differences matters for making an informed choice.
Tirzepatide is a dual GIP/GLP-1 receptor agonist, which distinguishes it from pure GLP-1 agonists like semaglutide. Clinical trials show tirzepatide produces greater average weight loss, but it also tends to cause more gastrointestinal side effects at equivalent dose escalation speeds. Our semaglutide vs tirzepatide side effects comparison breaks this down in detail.
Newer GLP-1 options are also emerging. Survodutide, mazdutide, and CagriSema represent the next wave of weight loss peptides, each with unique mechanisms. Retatrutide, a triple agonist, is generating significant research interest. The retatrutide dosage chart follows similar unit-to-mg conversion principles.
For the comparison between brand-name and generic options, see our semaglutide vs tirzepatide comparison page. The oral vs injection tirzepatide comparison is also relevant for anyone exploring oral tirzepatide, tirzepatide drops, tirzepatide tablets, or the newer orally disintegrating tablet (ODT) formulation.
Where to source quality compounded tirzepatide
The quality of your compounded tirzepatide directly affects whether the labeled concentration is accurate. A poorly compounded vial labeled "10 mg/mL" might actually contain 8 mg/mL or 12 mg/mL, making all your careful calculations meaningless.
Work with reputable compounding pharmacies that provide certificates of analysis and follow current good manufacturing practices. Several pharmacies have established track records in the compounded GLP-1 space, including Empower Pharmacy and others reviewed on our site.
For those exploring different sources, our guides on grey market tirzepatide, tirzepatide in Mexico, and various vendor reviews like Peptide Sciences, Lavender Sky, and ProRx provide detailed comparisons. The bottom line is that reliable sourcing ensures the concentration on the label matches what is actually in the vial, which is the foundation of every conversion calculation in this guide.
Advanced dosing considerations
Combination protocols
Some researchers combine tirzepatide with other compounds. Formulations containing tirzepatide, glycine, and B12 are increasingly common. Others pair it with methylcobalamin for potential neuroprotective benefits. In these combination vials, the tirzepatide concentration is still listed separately on the label. The additional ingredients do not change the units-to-mg math for tirzepatide itself.
Some people also explore combining tirzepatide with other medications like phentermine for enhanced appetite suppression. Always consult with a healthcare provider before combining medications, as interactions can affect both efficacy and safety.
Microdosing protocols
The opposite end of the spectrum from drawing 100 units. Microdosing involves using very small amounts, sometimes 5 to 10 units at low concentrations, to achieve subtle metabolic effects with minimal side effects. A microdosing tirzepatide chart and a microdose schedule can guide this approach. The units-to-mg conversion is the same, just with smaller numbers.
Dose timing
Tirzepatide is administered once weekly. The best time to take your GLP-1 shot depends on your schedule and when you can best manage potential side effects. Some people prefer evening injections so that peak nausea occurs during sleep. Others prefer morning injections. Consistency matters more than timing.
The GLP-1 class of medications all share similar dosing principles. Understanding how long GLP-1 medications take to start working, where to inject, and how to inject properly applies across the class. Other side effects like GLP-1 fatigue, hair loss, and headaches are also common across GLP-1 receptor agonists, not unique to tirzepatide.
Quick reference: the numbers you actually need
After all the detail above, here is the simplified version for daily use. Print this or save it to your phone.
If your vial says 5 mg/mL:
2.5 mg = 50 units
5 mg = 100 units
If your vial says 10 mg/mL:
2.5 mg = 25 units
5 mg = 50 units
7.5 mg = 75 units
10 mg = 100 units
If your vial says 20 mg/mL:
2.5 mg = 12.5 units
5 mg = 25 units
7.5 mg = 37.5 units
10 mg = 50 units
12.5 mg = 62.5 units
15 mg = 75 units
If your vial says 40 mg/mL:
5 mg = 12.5 units
10 mg = 25 units
15 mg = 37.5 units
The formula: Units = (mg dose / concentration) x 100
The reverse: mg = (units / 100) x concentration
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, dosing calculators, and a community of thousands who have navigated these exact questions. SeekPeptides members access detailed protocol builders, weight-based calculators, and expert-reviewed dosing guides that account for individual factors most resources ignore.
Frequently asked questions
How many mg is 100 units of tirzepatide at 10 mg/mL?
At 10 mg/mL, 100 units equals exactly 10 mg of tirzepatide. This is because 100 units on an insulin syringe equals 1 mL, and at 10 mg/mL concentration, 1 mL contains 10 mg. See our tirzepatide dosage in units guide for complete conversion tables at every concentration.
Is 100 units of tirzepatide a high dose?
It depends entirely on your vial concentration. At 5 mg/mL, 100 units is a moderate 5 mg dose. At 10 mg/mL, it is 10 mg, which is a higher therapeutic dose. At 20 mg/mL, it would be 20 mg, which exceeds the maximum FDA-approved dose. Always check your concentration before drawing. The tirzepatide dose chart shows where each amount falls in the standard protocol.
Can I draw 100 units from any tirzepatide vial?
Physically, yes, as long as the vial contains at least 1 mL of liquid. But whether you should depends on your prescribed dose and vial concentration. Drawing 100 units from a 20 mg/mL or 40 mg/mL vial delivers a very high dose that most people should not be taking. Use the dosage calculator to confirm the right amount for your situation.
What is the difference between units and mg in tirzepatide?
Units measure volume (how much liquid you draw into the syringe). Milligrams measure drug amount (how much medication is dissolved in that liquid). The concentration (mg/mL) on your vial label is the bridge between the two. One hundred units always equals 1 mL of liquid, but the milligrams in that 1 mL depend on how concentrated the solution is.
What if my pharmacy changed my tirzepatide concentration?
Recalculate your units immediately. If you were drawing 50 units from a 10 mg/mL vial (5 mg) and your new vial is 20 mg/mL, drawing 50 units would give you 10 mg, double your intended dose. Use the formula: Units = (dose in mg / new concentration) x 100. For detailed guidance on switching, see the compound dosage chart.
How do I know if I am using an insulin syringe or a TB syringe?
Check the packaging and barrel markings. Insulin syringes display "units" and typically max out at 100 (for 1 mL syringes). TB syringes display "mL" markings. Using the wrong syringe type without adjusting your measurement can cause significant dosing errors. Our syringe dosage guide covers this distinction in detail.
Should I switch to a higher concentration vial when my dose increases?
Generally, yes. When your dose exceeds 10 mg, a 10 mg/mL vial requires more than 100 units (1 mL), which does not fit in a standard insulin syringe. Switching to 20 mg/mL lets you draw 15 mg as 75 units. Discuss concentration options with your prescriber when your dose escalates beyond what your current vial comfortably accommodates.
Is 100 units of tirzepatide the same as 100 units of semaglutide?
In terms of volume, yes, both are 1 mL. In terms of milligrams, it depends on each vial concentration. At matching concentrations (say both at 10 mg/mL), 100 units of either would deliver 10 mg. But since semaglutide and tirzepatide have different dosing ranges and potencies, 10 mg of semaglutide is not clinically equivalent to 10 mg of tirzepatide. See our conversion chart for clinical equivalency guidance.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your concentrations stay verified, your calculations stay accurate, and your protocols stay safe.