Dec 29, 2025

Cagrilintide dosing isn't straightforward. Unlike daily medications where you take the same dose every day, this powerful amylin analog requires careful weekly titration over 12-16 weeks, precise reconstitution calculations if using research peptides, and strategic dose adjustments based on tolerance and results.
Get the dosing wrong and you'll either suffer intolerable nausea or miss out on the 10-25% body weight loss this peptide can deliver.
The challenge?
Most available information comes from clinical trial protocols that don't translate easily to real-world use. Trial participants had medical supervision, standardized doses, and specific titration schedules.
Meanwhile, individual users need practical guidance on starting doses, when to increase, how to manage breakthrough nausea, whether to reduce or push through side effects, and optimal maintenance dosing after achieving weight loss goals.
Standard cagrilintide dosing follows a 12-week titration from 0.6mg to 2.4mg weekly (0.6mg weeks 1-4, 1.2mg weeks 5-8, 1.8mg weeks 9-12, 2.4mg week 13+). Conservative approaches extend this to 16-20 weeks for better GI tolerance. When combined with semaglutide, both peptides titrate simultaneously but on different schedules. Maintenance dosing after weight loss may reduce to 1.8-2.0mg weekly to sustain results while minimizing cost and side effects.
This guide provides exact cagrilintide dosing protocols for every situation - standard titration, conservative approaches for GI-sensitive individuals, aggressive protocols for maximum weight loss, combination dosing with semaglutide or tirzepatide, maintenance strategies after goal weight, dose adjustments for side effects, and reconstitution calculations for research peptides.
We'll cover the clinical trial dosing that produced 10-12% weight loss, then break down practical protocols you can actually implement.
Clinical trial dosing: what the research shows
Understanding proven protocols provides the foundation.
OASIS trials: establishing effective doses
Phase 2 OASIS 1 findings:
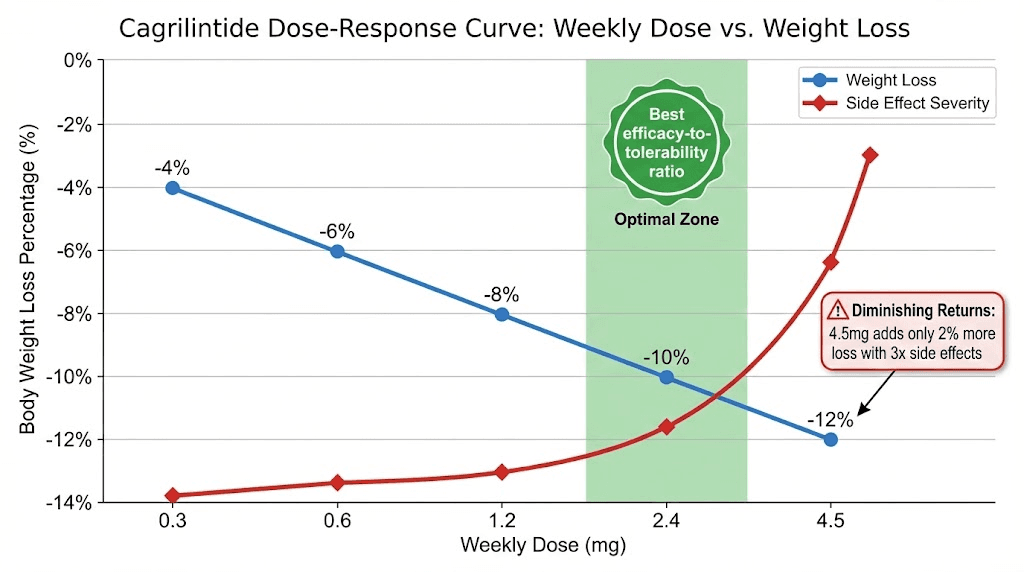
Tested multiple dose levels: 0.3mg, 0.6mg, 1.2mg, 2.4mg, 4.5mg weekly
Duration: 26 weeks
Primary endpoint: Weight loss at each dose
Dose-response results:
0.3mg weekly: ~4% body weight loss
0.6mg weekly: ~6% body weight loss
1.2mg weekly: ~8% body weight loss
2.4mg weekly: ~10% body weight loss
4.5mg weekly: ~12% body weight loss
Key insight: Clear dose-response relationship. Higher doses = more weight loss, but also more side effects.
Optimal balance: 2.4mg weekly emerged as best efficacy-to-tolerability ratio. This became the standard dose.
Learn the fundamentals at SeekPeptides - explore what are peptides, how peptides work, and what are peptides used for.
Standard titration schedule from trials
12-week escalation protocol:
Weeks 1-4: 0.6mg weekly
Initiation dose
Body adapts to amylin effects
Minimal side effects at this level
Weight loss begins (modest)
Weeks 5-8: 1.2mg weekly
First dose increase (doubling)
Gastric slowing becomes more noticeable
Appetite suppression strengthens
Accelerated weight loss
Weeks 9-12: 1.8mg weekly
Second increase
Strong satiety effects
More pronounced GI effects possible
Approaching maximum efficacy
Week 13+: 2.4mg weekly (maintenance)
Target therapeutic dose
Maximum weight loss velocity
Maintained indefinitely
Nausea typically resolved by this point (adapted)
Why this schedule works:
Gradual exposure reduces side effects
4-week intervals allow full adaptation
Doubling steps (0.6→1.2→2.4) are tolerable
Proven in hundreds of patients
Balances speed with tolerability
Use our peptide calculator and peptide dosing guide at SeekPeptides for precise calculations.
Higher dose exploration (4.5mg trials)
Rationale for testing 4.5mg:
Investigate maximum tolerable dose
Determine if higher = better weight loss
Establish safety ceiling
Results at 4.5mg weekly:
Weight loss: ~12% (vs 10% at 2.4mg)
Incremental benefit: Only 2% additional loss
Side effects: Significantly worse nausea/vomiting
Dropout rate: Higher than 2.4mg
Clinical verdict:
4.5mg not recommended for routine use
Risk-benefit ratio unfavorable
2.4mg remains optimal
Some individuals may tolerate 3.0mg as compromise
CagriSema combination dosing trials
REDEFINE-1 protocol:
Semaglutide: 2.4mg weekly (standard titration over 16 weeks)
Cagrilintide: 2.4mg weekly (12-week titration)
Both given as separate injections
Started simultaneously from week 1
Semaglutide escalation (standard):
Weeks 1-4: 0.25mg
Weeks 5-8: 0.5mg
Weeks 9-12: 1.0mg
Weeks 13-16: 1.7mg
Week 17+: 2.4mg
Cagrilintide escalation (when combined):
Weeks 1-4: 0.6mg
Weeks 5-8: 1.2mg
Weeks 9-12: 1.8mg
Week 13+: 2.4mg
Results:
15.6% average weight loss (68 weeks)
Superior to either alone
Side effects manageable with slow titration
Combination well-tolerated
See our cagrilintide and semaglutide combination guide and semaglutide dosage calculator.
Standard cagrilintide dosing protocol (monotherapy)
This is the proven approach for most of our users.
Week-by-week titration guide
Complete 13-week escalation:
Week | Dose | What to Expect | Side Effects | Weight Loss | Tips |
|---|---|---|---|---|---|
1-4 | 0.6mg | Mild appetite reduction, slightly fuller after meals | Minimal (10-20% experience mild nausea) | 1-3 lbs | Take with food, ginger for nausea, stay hydrated |
5-8 | 1.2mg | Stronger satiety, noticeable gastric slowing, eating less | Moderate (30-40% mild-moderate nausea) | 4-8 lbs total | Smaller meals, avoid fatty foods, expect fullness |
9-12 | 1.8mg | Very full after eating, smaller portions needed | Higher (40-50% nausea, usually temporary) | 10-15 lbs total | Protein priority, slow eating, don't overfill stomach |
13+ | 2.4mg | Maximum appetite suppression, adapted to effects | Moderate (30-40% as body adapts) | 1-2 lbs/week steady | Maintain small frequent meals, protein focus |
Titration comparison by approach:
Protocol Type | Time to 2.4mg | Total Titration Weeks | Nausea Severity | Weight Loss at 6 Months | Best For |
|---|---|---|---|---|---|
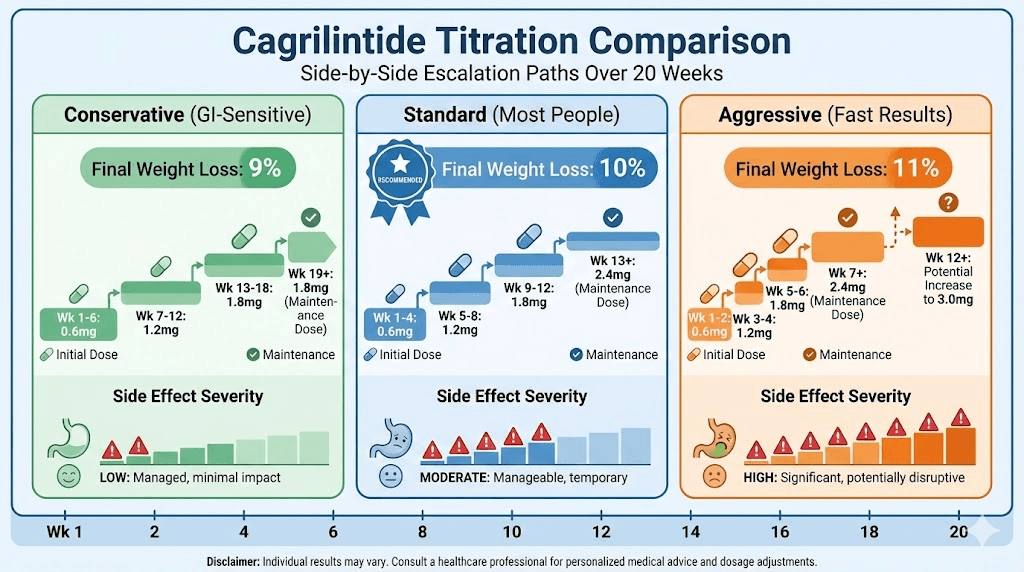
Conservative | 19-20 weeks | 20 weeks | Low (20-30%) | 18-22 lbs | GI-sensitive, first-time peptide users, prefer comfort |
Standard (Recommended) | 13 weeks | 13 weeks | Moderate (40-50%) | 20-26 lbs | Most people, balanced approach, proven protocol |
Aggressive | 7 weeks | 8 weeks | High (60-70%) | 22-28 lbs | Excellent GI tolerance, want fast results, experienced users |
Maximum (4.5mg) | 16+ weeks | 18 weeks | Very High (70-80%) | 24-30 lbs | Exceptional tolerators only, research setting |
Injection logistics:
Route: Subcutaneous (under skin)
Sites: Abdomen, thighs, upper arms
Frequency: Once weekly, same day
Timing: Any time of day (many prefer evening)
Rotate sites to prevent irritation
Critical success factors:
Never skip doses (breaks adaptation)
Don't rush titration (invites severe nausea)
Stay on each dose full 4 weeks minimum
Track weight and side effects weekly
Adequate protein every day (60-80g minimum)
When to increase vs hold current dose
Increase dose on schedule if:
Minimal or no nausea at current dose
Tolerating current dose well for 3+ weeks
Weight loss continuing (any amount)
Following standard protocol
No concerning side effects
Stay at current dose longer if:
Moderate nausea still present
Had vomiting episode(s)
Not eating adequate protein due to appetite suppression
Rapid weight loss (>3 lbs/week consistently)
General feeling unwell
Need more adaptation time
Add 1-2 extra weeks at dose level, then reassess
Reduce dose if:
Severe persistent nausea despite management
Multiple vomiting episodes
Unable to maintain nutrition
Dehydration occurring
Intolerable side effects
Drop back to previous dose, stabilize 2-4 weeks, then retry increase
Planning your titration schedule? SeekPeptides provides personalized dosing calendars based on your GI tolerance and weight loss goals. Our peptide cycle planning guide helps map your complete protocol.
Reconstitution math for research peptides
Common vial sizes and mixing:
Vial Size | Water to Add | Final Concentration | Dose Calculations | Lasts (at 2.4mg) |
|---|---|---|---|---|
2.4mg | 1ml | 2.4mg/ml | 0.6mg = 0.25ml, 1.2mg = 0.5ml, 1.8mg = 0.75ml, 2.4mg = 1.0ml | 1 week |
5mg | 2ml | 2.5mg/ml | 0.6mg = 0.24ml, 1.2mg = 0.48ml, 1.8mg = 0.72ml, 2.4mg = 0.96ml | 2 weeks |
10mg | 4ml | 2.5mg/ml | 0.6mg = 0.24ml, 1.2mg = 0.48ml, 1.8mg = 0.72ml, 2.4mg = 0.96ml | 4+ weeks |
10mg (concentrated) | 2ml | 5mg/ml | 0.6mg = 0.12ml, 1.2mg = 0.24ml, 1.8mg = 0.36ml, 2.4mg = 0.48ml | 4+ weeks |
2.4mg vial (1-week supply at maintenance):
Add 1ml bacteriostatic water → 2.4mg/ml concentration
Each 1ml = one full 2.4mg dose
Simple 1:1 ratio
5mg vial:
Add 2ml bacteriostatic water → 2.5mg/ml
0.6mg dose = 0.24ml
1.2mg dose = 0.48ml
2.4mg dose = 0.96ml (~1ml)
10mg vial (bulk):
Add 4ml bacteriostatic water → 2.5mg/ml
Same dosing as 5mg vial
More economical if available
Lasts 4+ weeks at maintenance
Calculation formula: Total mg ÷ ml water = concentration (mg/ml) Desired dose ÷ concentration = ml to inject
Example: 10mg vial + 4ml water = 2.5mg/ml Want 2.4mg dose → 2.4 ÷ 2.5 = 0.96ml to inject
Use our peptide reconstitution calculator or free peptide reconstitution calculator for instant calculations. See our how to reconstitute peptides guide for step-by-step instructions.
Storage and stability
Before reconstitution:
Freezer (-20°C): 12-24+ months
Refrigerator (2-8°C): 6-12 months
Room temperature: Not recommended (days only)
After reconstitution:
Refrigerator (2-8°C): 28-30 days maximum
Never freeze liquid peptide
Protect from light (amber vial or box)
Maintain sterile technique always
Visual quality check:
Should be clear, slightly blue-tinted
No particles or cloudiness
If contaminated (cloudy, particles) → discard
See our peptide storage guide, how long reconstituted peptides last in fridge, bacteriostatic water for peptides, water to mix with peptides, and lyophilized vs liquid peptides.
Conservative dosing approach (GI-sensitive individuals)
For those who need gentler escalation.
Extended 20-week titration
Slower, more gradual protocol:
Weeks 1-6: 0.6mg weekly (extended from 4 weeks)
Weeks 7-12: 1.2mg weekly (6 weeks at this dose)
Weeks 13-18: 1.8mg weekly (6 weeks)
Week 19+: 2.4mg weekly OR stay at 1.8-2.0mg
Advantages:
Significantly reduced nausea
Better long-term adherence
More comfortable adaptation
Lower dropout risk
Trade-offs:
Slower initial weight loss
Takes longer to reach maximum efficacy
More weeks of injections to get to target
Similar total weight loss (just slower progression)
Lower maintenance doses
Alternative endpoint options:
1.8mg weekly maintenance:
~9% average weight loss (vs 10% at 2.4mg)
Notably better tolerated
Fewer ongoing side effects
25% cost savings
Many find this sufficient
2.0mg weekly maintenance:
~9.5% average weight loss
Middle ground approach
Good efficacy, good tolerance
Slight cost savings
Recommended trial first
When to choose lower maintenance:
Achieved satisfactory weight loss before reaching 2.4mg
Significant nausea at 2.4mg
Budget constraints (research peptides expensive)
Prefer comfort over maximum results
Already combining with semaglutide (lower cagrilintide dose acceptable)
Managing breakthrough nausea during titration
First-line interventions:
Pause escalation (stay at current dose 1-2 extra weeks)
Ginger supplementation (500-1,000mg before meals)
Smaller, more frequent meals (5-6 per day)
Avoid trigger foods (fatty, spicy, fried)
Stay upright 2 hours after eating
Second-line strategies:
Vitamin B6 (25-50mg daily)
Sea-Bands acupressure wristbands
Cold foods vs hot (better tolerated)
Liquid nutrition if solids difficult (protein shakes)
Medication options:
Zofran/ondansetron (most effective, prescription)
Promethazine (prescription)
Meclizine/Dramamine (OTC, less effective)
When to reduce dose:
Nausea interfering with daily life
Unable to eat adequate protein
Vomiting more than occasionally
Preference for slower approach
SeekPeptides helps you optimize your titration based on real-time side effects. Track symptoms and get AI-powered recommendations for dose adjustments.
Aggressive dosing protocols (maximum weight loss)
For excellent tolerators seeking fastest results.
Faster escalation (8-week to 2.4mg)
Accelerated titration:
Weeks 1-2: 0.6mg weekly
Weeks 3-4: 1.2mg weekly
Weeks 5-6: 1.8mg weekly
Week 7+: 2.4mg weekly
Who can attempt:
No significant nausea on GLP-1s previously
Generally strong GI tolerance
Motivated for rapid weight loss
Willing to accept higher side effect risk
Can reduce dose if needed
Expected experience:
More pronounced nausea (weeks 3-5 especially)
Faster adaptation curve
Quicker weight loss onset
Reaches maximum efficacy 4+ weeks sooner
Success factors:
Aggressive nausea management from start
Ginger, B6, anti-nausea meds ready
Small meal prep planned
Ready to slow down if needed
Higher maintenance doses (3.0-4.5mg)
Rationale:
Trials showed 3.0mg and 4.5mg produce slightly more weight loss
Some individuals tolerate well
Investigational approach
3.0mg weekly:
~11% average weight loss
Moderate increase in side effects
Reasonable middle ground
Some find optimal here
4.5mg weekly:
~12% average weight loss (maximum)
Significantly worse nausea/vomiting
High dropout rate
Not recommended routinely
Only for exceptional tolerators
Titration to higher doses:
Reach 2.4mg first (standard titration)
Stable at 2.4mg for 4-8 weeks
Increase to 3.0mg if tolerating perfectly
Consider 4.5mg only if 3.0mg easy
Risk-benefit analysis:
3.0mg: May be worth it for some (1% extra loss)
4.5mg: Usually not worth it (2% extra loss, major side effects)
Cost increases proportionally
Individual decision
Combination with other peptides for synergy
Cagrilintide + Semaglutide (CagriSema):
Most studied, proven synergy
Both at 2.4mg weekly
15-25% total weight loss
See detailed combination protocols below
Cagrilintide + CJC-1295/Ipamorelin:
Cagrilintide: 2.4mg weekly (fat loss)
CJC-1295: 200-300mcg 5x weekly (muscle preservation)
Ipamorelin: 200-300mcg 5x weekly (body composition)
Preserves muscle during aggressive weight loss
Better body composition outcomes
Cagrilintide + BPC-157:
Cagrilintide: 2.4mg weekly (weight loss)
BPC-157: 250-500mcg twice daily (gut health)
BPC-157 may help with GI side effects
Supports gut during weight loss
Complementary mechanisms
See our peptide stacks guide, peptide stack calculator, CJC-1295 dosage calculator, Ipamorelin benefits, BPC-157 guide, and BPC-157 dosage calculator.
Combination dosing protocols
Strategies when using multiple peptides together.
CagriSema: Cagrilintide + Semaglutide dosing
Simultaneous start (from day 1):
Week | Semaglutide Dose | Cagrilintide Dose | Combined Weekly Cost (Research) | Cumulative Weight Loss |
|---|---|---|---|---|
1-4 | 0.25mg | 0.6mg | $50-80 | 2-4 lbs |
5-8 | 0.5mg | 1.2mg | $80-120 | 6-10 lbs |
9-12 | 1.0mg | 1.8mg | $150-250 | 12-18 lbs |
13-16 | 1.7mg | 2.4mg | $250-350 | 18-28 lbs |
17+ | 2.4mg | 2.4mg | $350-500 | 30-50+ lbs (by week 68) |
Semaglutide titration:
Weeks 1-4: 0.25mg weekly
Weeks 5-8: 0.5mg weekly
Weeks 9-12: 1.0mg weekly
Weeks 13-16: 1.7mg weekly
Week 17+: 2.4mg weekly
Cagrilintide titration (running parallel):
Weeks 1-4: 0.6mg weekly
Weeks 5-8: 1.2mg weekly
Weeks 9-12: 1.8mg weekly
Week 13+: 2.4mg weekly
CagriSema vs monotherapy comparison:
Approach | Average Weight Loss | Timeline to Max Dose | Side Effect Severity | Monthly Cost (Research) | Best For |
|---|---|---|---|---|---|
Semaglutide alone | 10-15% | 17 weeks | Moderate | $150-300 | Proven GLP-1 therapy, FDA approved |
Cagrilintide alone | 10-12% | 13 weeks | Moderate-High | $800-1,600 | Amylin pathway, investigational |
CagriSema combo | 15-25% | 17 weeks | High | $950-1,900 | Maximum medical weight loss |
Tirzepatide alone | 15-22% | 20 weeks | Moderate | $300-500 | Dual GIP/GLP-1, FDA approved |
Key points:
Both injected same day (different sites) OR different days
Cagrilintide reaches target faster (13 weeks vs 17 weeks)
Side effects additive but manageable
Maximum synergy
Sequential start (adding cagrilintide later):
Already on semaglutide 2.4mg:
Stable on semaglutide for 4+ weeks
Continue semaglutide 2.4mg weekly
Add cagrilintide starting 0.6mg weekly
Titrate cagrilintide: 0.6mg (weeks 1-4) → 1.2mg (weeks 5-8) → 1.8mg (weeks 9-12) → 2.4mg (week 13+)
Maintain both at 2.4mg
Advantages of sequential:
Semaglutide establishes baseline weight loss first
Easier to attribute new side effects (know it's cagrilintide)
Less overwhelming than both at once
Can see incremental benefit of adding cagrilintide
Expected combination results:
15-20% average weight loss (most users)
20-25% weight loss (excellent responders)
Superior to either alone consistently
Optimize your CagriSema protocol at SeekPeptides - we help you coordinate both titration schedules and manage combined side effects. See our cagrilintide and semaglutide guide and semaglutide vs tirzepatide comparison.
Adding cagrilintide to tirzepatide
Theoretical protocol (not clinically studied):
If on tirzepatide 10-15mg:
Stable on tirzepatide for 4+ weeks
Continue tirzepatide at current dose
Add cagrilintide 0.6mg weekly
Standard cagrilintide titration to 2.4mg
Rationale:
Tirzepatide is dual GIP/GLP-1 (very powerful alone)
Adding amylin pathway could theoretically enhance
No clinical data on this combination
Uncertain if additional benefit over tirzepatide alone
Concerns:
GI side effects may be severe (both slow gastric emptying)
Tirzepatide already produces 15-22% weight loss alone
Unclear if cagrilintide adds meaningful benefit
Expensive combination
Verdict: Wait for clinical data. Tirzepatide + semaglutide or CagriSema better established.
See our tirzepatide dosing guide.
Lower cagrilintide doses in combinations
When combining, can reduce cagrilintide:
1.8mg cagrilintide + 2.4mg semaglutide:
Still very effective (14-18% weight loss estimated)
Better tolerated than both at 2.4mg
Cost savings on cagrilintide
Consider if GI-sensitive
1.2mg cagrilintide + 2.4mg semaglutide:
Modest benefit from cagrilintide addition
Minimal GI side effects from cagrilintide
Semaglutide does heavy lifting
May still achieve 12-15% total weight loss
Testing approach:
Start with standard doses (both 2.4mg)
If intolerable, reduce cagrilintide first
Maintain semaglutide at 2.4mg (well-tolerated, established)
Find optimal cagrilintide dose for your tolerance
Maintenance dosing after weight loss
Strategies to sustain results long-term.
Transitioning from weight loss to maintenance
Determining goal weight achievement:
Lost 10-12% body weight (cagrilintide alone)
Lost 15-25% body weight (CagriSema)
Weight stable for 4-8 weeks
Satisfied with current weight
Ready to focus on maintenance
Maintenance dose options comparison:
Maintenance Strategy | Dose | Expected Weight Stability | Side Effects | Monthly Cost Savings vs 2.4mg | Success Rate | Notes |
|---|---|---|---|---|---|---|
Continue same dose | 2.4mg weekly | Excellent (95%+ maintain) | Moderate ongoing | $0 (baseline) | Highest | Most conservative, ensures no regain |
Reduce to 2.0mg | 2.0mg weekly | Very good (85-90% maintain) | Mild-moderate | $150-300/month | High | Recommended first attempt |
Reduce to 1.8mg | 1.8mg weekly | Good (75-85% maintain) | Mild | $200-400/month | Moderate-high | Monitor closely for regain |
Every 10 days | 2.4mg every 10 days | Variable (60-75% maintain) | Mild | $350-500/month | Moderate | Requires close monitoring |
Discontinue | None | Poor (20-30% maintain) | None | $800-1,600/month | Very low | Weight regain typical |
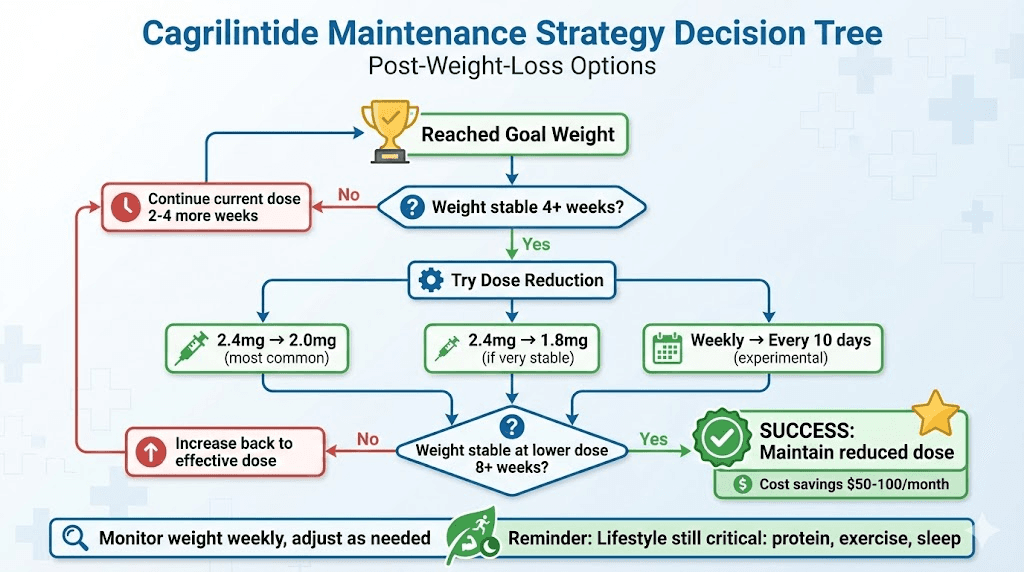
Option 1: Continue same dose
Keep cagrilintide at 2.4mg weekly
Ensures no regain
Most conservative approach
Highest cost
Option 2: Reduce dose slightly
Decrease to 1.8-2.0mg weekly
Monitor weight for 4 weeks
If stable, maintain
If gaining, increase back
20-25% cost savings
Option 3: Try every 10 days
Instead of weekly, inject every 10 days
Effectively 30% dose reduction
Some maintain weight this way
Requires close monitoring
Recommendation: Try Option 2 first (reduce to 1.8-2.0mg). Most people maintain weight loss at slightly lower dose.
Preventing weight regain
Critical factors beyond peptides:
Protein intake (1g per lb current weight minimum)
Resistance training (3-4x weekly to maintain muscle)
Daily movement (8,000-10,000 steps)
Sleep (7-9 hours)
Stress management
Regular weight monitoring (weekly)
Early intervention if regaining:
Gain 3-5 lbs: Tighten diet, increase movement
Gain 5-10 lbs: Increase cagrilintide dose back to 2.4mg
Gain >10 lbs: Consider adding semaglutide or revisiting full protocol
Realistic expectations:
Some fluctuation normal (2-5 lbs)
Lifelong management required
Peptides not cure, management tools
May need indefinite use at maintenance dose
Long-term safety of continuous use
Current evidence:
Cagrilintide trials up to 68 weeks (safe)
Pramlintide (similar) used for years in diabetes (safe)
No tolerance development observed
Continued efficacy long-term
Theoretical concerns:
Very long-term (5-10+ years) unknown
Amylin physiology alterations
Potential adaptation
Monitoring recommendations:
Annual comprehensive metabolic panel
Gallbladder ultrasound if symptoms
A1c if diabetic
Lipid panel
Monitor for side effects
Cost consideration:
Maintenance indefinite = ongoing expense
Budget $200-400/month (1.8-2.4mg weekly)
Or $800-1,600/month if combination
Factor into decision to start
Track your maintenance phase with SeekPeptides - our platform helps you find the minimum effective dose to sustain weight loss while minimizing cost and side effects.
Troubleshooting dosing issues
Solutions for common problems.
Nausea won't resolve at current dose
If nausea persistent after 3+ weeks:
Extend time at dose - Stay another 2-4 weeks (total 6-8 weeks)
Reduce dose temporarily - Drop to previous level for 2 weeks, then retry
Split dose experiment - Some try 1.2mg every 3.5 days instead of 2.4mg weekly (not standard, experimental)
Add pharmaceutical anti-nausea - Zofran prescription can be game-changer
Reassess goal dose - Maybe 1.8mg is your maximum tolerable
When to accept lower target:
9% weight loss at 1.8mg still excellent
Better adherence matters more than extra 1%
Quality of life important
Plateaued weight loss mid-protocol
Weight loss stalled before reaching 2.4mg:
Likely causes:
Not at therapeutic dose yet (need to continue titrating)
Temporary plateau (common at weeks 8-12)
Inadequate protein intake
Not in calorie deficit despite appetite suppression
Solutions:
Continue titration on schedule (don't stop early)
Track calories temporarily (ensure deficit)
Increase protein to 1.2g per lb goal weight
Add resistance training if not already
Wait 4 more weeks before declaring true plateau
Plateaued at maintenance dose (2.4mg):
Normal after 12-16 weeks
Body adapting to new weight
Consider adding semaglutide for synergy
Or accept current weight loss (likely 10-12% achieved)
Extreme appetite suppression (underfeeding)
If barely able to eat:
Warning signs:
Eating <1,000 calories daily
Protein <50g daily
Excessive fatigue
Hair thinning
Muscle weakness
Interventions:
Reduce cagrilintide dose (may be too high for you)
Liquid nutrition (protein shakes easier)
Nutrient-dense small meals
Set eating schedule (force meals even if not hungry)
May need to discontinue temporarily
Minimum nutrition targets:
1,200-1,500 calories daily (women)
60-80g protein minimum
Multivitamin
Hydration 64+ oz
Don't sacrifice health for faster weight loss
Injection site reactions
If developing irritation, redness, lumps:
Prevention:
Rotate sites religiously (6-8 different spots)
Clean site with alcohol, let dry completely
Don't inject into same spot within 2 weeks
Use shorter needles (5mm vs 8mm)
Treatment:
Avoid affected area until healed
Ice after injection (5-10 minutes)
Topical hydrocortisone cream
Allow 3+ weeks between same site
Concerning reactions:
Severe pain, swelling, fever → see doctor
May indicate infection or allergy
Rare but requires evaluation
Get personalized troubleshooting at SeekPeptides - our AI advisor analyzes your specific dosing issues and suggests evidence-based solutions.
How you can use SeekPeptides for optimal cagrilintide dosing
SeekPeptides provides comprehensive dosing guidance for cagrilintide at every stage. Get personalized titration schedules based on your GI tolerance, weight loss goals, and whether you're using cagrilintide alone or in combination.
Our platform helps you determine when to increase doses, when to hold current dose, how to manage breakthrough nausea, optimal maintenance dosing after weight loss, and reconstitution calculations for research peptides.
Track your weekly doses, side effects, and weight to optimize your protocol in real-time.
Access our calculators - peptide calculator, peptide dosing guide, peptide dosage chart, how to calculate peptide dosages, peptide reconstitution calculator, free peptide reconstitution calculator, peptide cost calculator, peptide stack calculator - for precise cagrilintide protocols.
Learn proper administration through our guides - peptide injections guide, how to reconstitute peptides, peptide storage guide, bacteriostatic water for peptides, water to mix with peptides, getting started with peptides.
Access our best peptide vendors guide for quality sourcing and common peptide mistakes beginners make to avoid errors.
Final thoughts
Cagrilintide dosing success depends on following proven titration protocols rather than rushing to maximum doses. The standard 12-week escalation from 0.6mg to 2.4mg weekly balances efficacy with tolerability, producing 10-12% weight loss for most users. GI-sensitive individuals benefit from extended 16-20 week titrations and may find optimal results at maintenance doses of 1.8-2.0mg weekly rather than pushing to 2.4mg.
Combination protocols with semaglutide require coordinating two separate titration schedules, with cagrilintide reaching 2.4mg at 13 weeks and semaglutide at 17 weeks. This dual-peptide approach produces 15-25% weight loss - significantly superior to monotherapy - making the dosing complexity worthwhile for those seeking maximum results.
Maintenance dosing after achieving weight loss often allows reduction to 1.8-2.0mg weekly while sustaining results, providing cost savings and better tolerability for long-term use. However, lifestyle factors - protein intake, resistance training, sleep, stress management - remain critical for preventing regain regardless of dose.
Research peptide users must master reconstitution calculations, proper storage, and sterile technique alongside dosing protocols. Quality sourcing with third-party testing ensures you're actually getting pharmaceutical-grade cagrilintide at stated concentrations.
Your cagrilintide dosing journey requires patience during titration, willingness to adjust based on tolerance and results, commitment to minimum 12-16 weeks before assessing full efficacy, and understanding that optimal dosing varies individually - what works perfectly for one person may be intolerable or insufficient for another. Start with proven protocols, adjust systematically, and prioritize sustainable approaches over aggressive shortcuts.
Helpful resources for cagrilintide dosing
Peptide calculator - Calculate all doses
Peptide reconstitution calculator - Mix correctly
Free peptide reconstitution calculator - Alternative calculator
See you soon, join SeekPeptides