Mar 18, 2026

You have a vial of semaglutide in your refrigerator. You have a box of insulin syringes on the counter. And you have a thought that seems perfectly reasonable: why not draw up several doses at once and store them for later?
It would save time. It would reduce the number of times you puncture the vial septum. It would make your weekly injection routine faster, cleaner, and more convenient, especially if you travel or have a busy schedule that makes careful dose preparation difficult on injection day.
The short answer is yes, you can prefill semaglutide syringes. But whether you should depends on several factors that most guides completely ignore. Stability, sterility, dose accuracy, storage requirements, and the type of semaglutide you are using all play critical roles in determining whether prefilling is safe and effective for your specific situation. Understanding the fundamentals of compounded semaglutide is the first step toward making an informed decision about your preparation method.
This guide covers everything you need to know about prefilling semaglutide syringes, from the science behind peptide stability in polypropylene barrels to step-by-step preparation techniques, proper storage protocols, and the specific situations where prefilling makes sense versus when it introduces unnecessary risk. Whether you are using a 5mg vial or a 10mg vial, the principles remain the same, but the details matter more than you think. SeekPeptides members have access to detailed preparation protocols that account for these variables, and this guide distills the essential knowledge every researcher should have.
Why people want to prefill semaglutide syringes
The appeal is obvious. Drawing up a single dose from a reconstituted semaglutide vial requires careful measurement, steady hands, and a clean workspace. Multiply that process by four or five weekly doses, and the convenience argument practically makes itself.
But convenience is only part of the story.
Travel and portability
Carrying a full vial of reconstituted semaglutide while traveling with semaglutide introduces risks that prefilled syringes can eliminate. Vials can break. They require more careful temperature management during transport. And drawing up doses in hotel rooms or airport bathrooms is far from ideal. A sealed, prefilled syringe in a protective case simplifies the entire process. Many researchers who travel frequently find that prefilling a week or two of doses before departure reduces both stress and the chance of dosing errors on the road.
Dose accuracy and consistency
Here is something most people do not consider. When you draw from a vial repeatedly, the concentration can shift slightly if bacteriostatic water evaporates through the septum over time. Tiny amounts, yes, but they accumulate. Prefilling all doses at once, shortly after reconstitution, means every syringe contains the same concentration. Your semaglutide dosage calculator numbers stay accurate across every single dose.
This matters most at lower doses. If you are on a 0.25mg starting dose, even minor concentration changes represent a larger percentage of your total dose compared to someone on 2.4mg.
Reduced vial punctures
Every time a needle punctures a vial septum, it creates a microscopic pathway for contamination. One puncture is negligible risk. Ten punctures over several weeks? The risk climbs. Prefilling all doses in a single session means fewer septum punctures, less contamination opportunity, and better preservation of the sterile environment inside the vial. Understanding how long a semaglutide vial stays good in the fridge helps frame why minimizing punctures matters.
Physical limitations
Some researchers deal with arthritis, tremors, or visual impairment that makes precise dose measurement challenging. Having a caregiver or partner prefill syringes during a single careful session eliminates the need to perform fine motor tasks every injection day. This is not a minor consideration. Dose accuracy depends on steady hands and clear vision, and not everyone has both available at 7am on a Tuesday.
The science of semaglutide stability in prefilled syringes
Before you start drawing up a month of doses, you need to understand what happens to semaglutide when it sits in a plastic syringe barrel instead of a glass vial.
Peptide adsorption to syringe surfaces
Semaglutide is a modified GLP-1 receptor agonist with a fatty acid side chain that makes it somewhat lipophilic. This means it has an affinity for certain surfaces, including polypropylene, the plastic used in most insulin syringes. When semaglutide solution contacts the interior of a syringe barrel, some peptide molecules can adsorb onto the surface.
How much adsorption occurs depends on several factors. Concentration matters. Higher concentrations experience proportionally less surface loss because the bulk solution overwhelms the available binding sites. Temperature matters. Warmer temperatures increase molecular movement and adsorption rates. Time matters most of all. The longer semaglutide sits in a syringe, the more peptide can migrate to the barrel walls.
For practical purposes, studies on similar peptides in insulin syringes show that losses remain below 5% over 28 days when stored under refrigeration. At room temperature, losses can climb to 8-12% in the same timeframe. This is why refrigeration is not optional for prefilled syringes, and it is also why proper semaglutide refrigeration matters even more for prefilled preparations than for vials.
Bacteriostatic water and the preservative factor
If your semaglutide was reconstituted with bacteriostatic water containing 0.9% benzyl alcohol, you have a significant advantage for prefilling. The benzyl alcohol acts as a preservative that inhibits bacterial growth, giving you a wider safety window. This is the standard for multi-dose vials and the reason proper reconstitution with bacteriostatic water is emphasized so heavily in preparation guides.
Without bacteriostatic water, meaning if your vial was reconstituted with sterile water for injection, the math changes dramatically. Sterile water has no preservative. Any bacteria introduced during the prefilling process can multiply freely. In this scenario, prefilled syringes should be used within 24-48 hours at most, and honestly, the risk-benefit calculation tilts firmly against prefilling altogether.
Know what was used to reconstitute your vial. This single detail determines whether prefilling is reasonable or reckless.
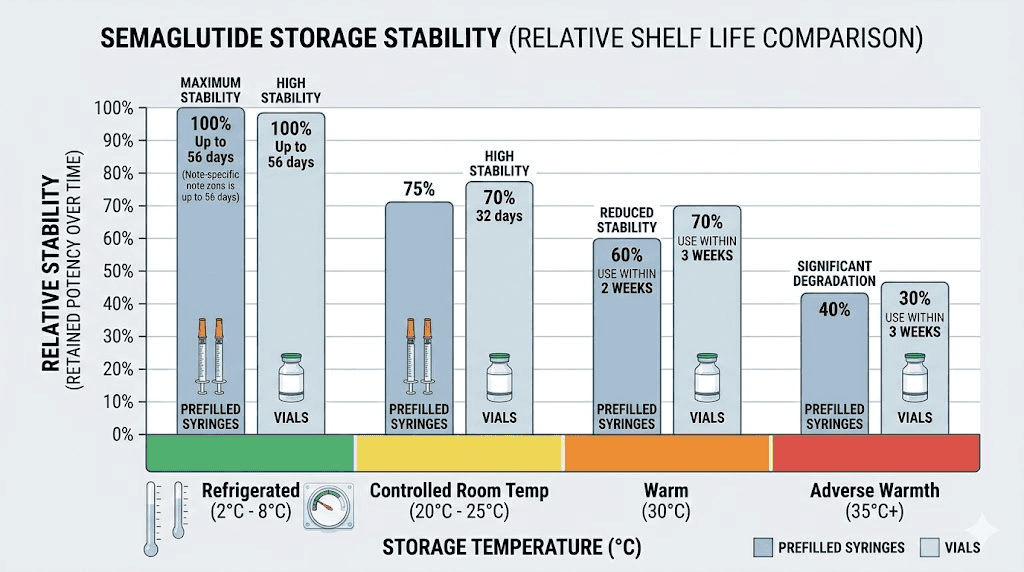
Temperature stability data
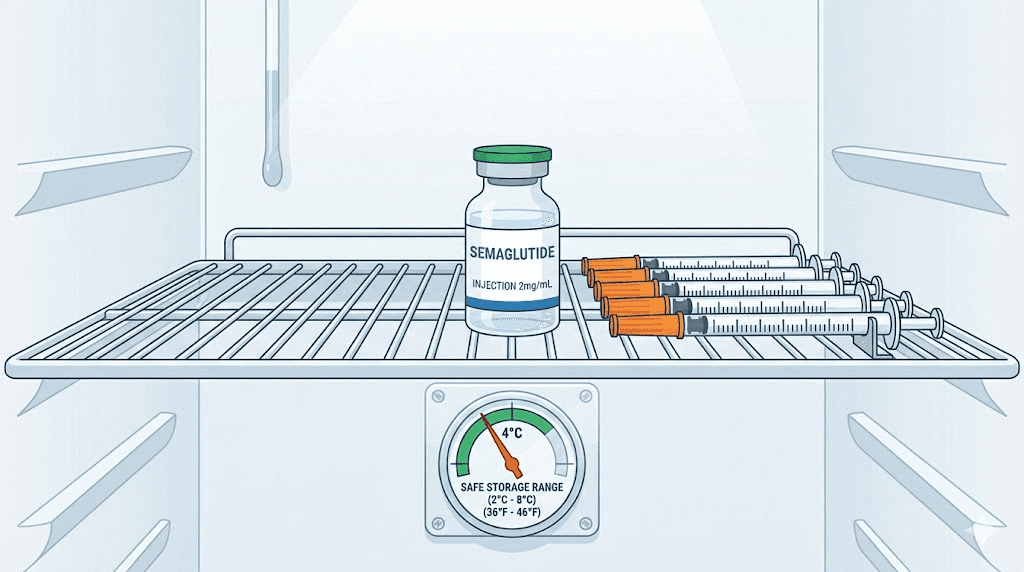
Semaglutide maintains its structural integrity within a specific temperature range. The manufacturer data for brand-name formulations indicates stability for up to 56 days at 36-46 degrees Fahrenheit (2-8 degrees Celsius). At room temperature, below 86 degrees Fahrenheit (30 degrees Celsius), stability holds for approximately 28 days.
For compounded semaglutide in prefilled syringes, the beyond-use date is typically more conservative. Most compounding pharmacies assign a 28-day expiration for refrigerated preparations and recommend against room temperature storage altogether. If your semaglutide gets warm or you accidentally leave it out overnight, the stability timeline compresses regardless of whether the peptide is in a vial or syringe.
The key numbers to remember for prefilled semaglutide syringes:
Refrigerated (2-8 degrees Celsius): stable for up to 28 days
Room temperature (below 30 degrees Celsius): use within 7 days maximum
Above 30 degrees Celsius: discard immediately
Frozen: do not freeze prefilled syringes, as ice crystals can denature the peptide and damage the syringe barrel
Step-by-step guide to prefilling semaglutide syringes safely
If you have decided that prefilling makes sense for your situation, the process itself requires careful attention to sterile technique. Rushing this step defeats the entire purpose. Take your time. Get it right once, and you have a week or more of perfectly measured, ready-to-use doses.
What you need before starting
Gather everything first. Do not start the process and then go hunting for supplies midway through.
Reconstituted semaglutide vial stored in the refrigerator (check your semaglutide shelf life to ensure it is still within the beyond-use date)
Insulin syringes (one per dose you plan to prefill, see our GLP-1 syringe guide for sizing recommendations)
Alcohol swabs (isopropyl alcohol, 70%)
A clean, flat workspace wiped down with isopropyl alcohol
Syringe caps or needle covers (these come with most insulin syringes)
A labeled container for storing the prefilled syringes in the refrigerator
A permanent marker for labeling syringes with dose and date
Your dosage chart so you know exactly how many units to draw (reference your semaglutide dosage chart in units or semaglutide syringe dosage chart)
Preparation: setting up your workspace
Wash your hands thoroughly with soap and water for at least 20 seconds. Dry them with a clean paper towel, not a cloth towel that may harbor bacteria. Wipe down your workspace with an alcohol pad or spray. Let it air dry completely. Place all supplies on the clean surface.
Remove the semaglutide vial from the refrigerator. Let it sit at room temperature for 5-10 minutes. Cold solution is slightly more viscous, which makes drawing accurate doses more difficult. Do not warm it artificially with hot water or body heat, as rapid temperature changes can affect peptide structure. Just let it come to a mild temperature naturally.
Drawing up the doses
This is where precision matters. Follow these steps for each syringe:
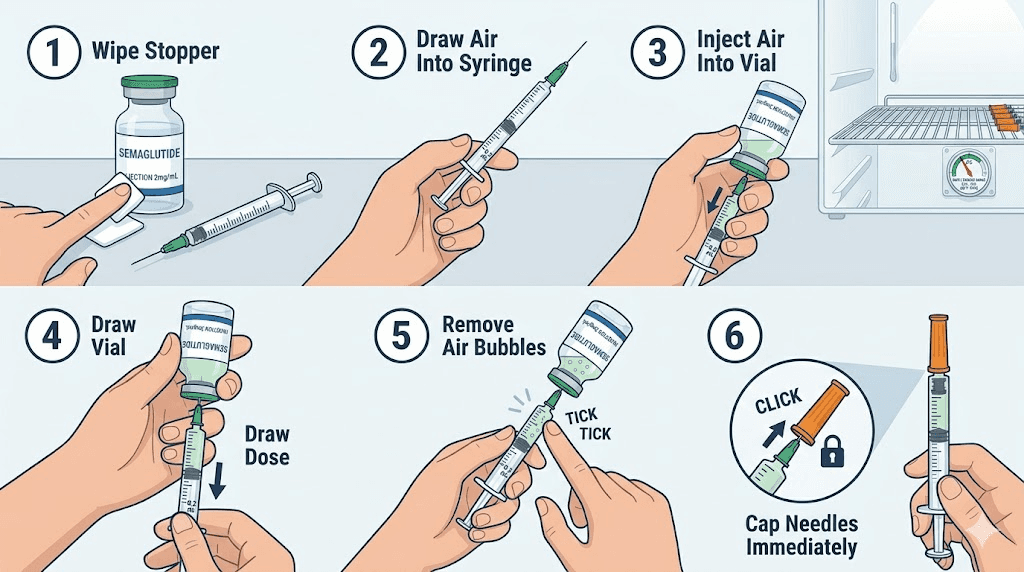
Step 1: Swab the vial septum with an alcohol pad. Let it air dry for 10 seconds. Do not blow on it.
Step 2: Remove the cap from a fresh insulin syringe. Pull the plunger back to the number of units you need, drawing air into the barrel.
Step 3: Insert the needle through the center of the vial septum at a slight angle. Push the air into the vial. This equalizes pressure and makes drawing easier. A trick that experienced researchers use: push the needle through slowly and steadily rather than jabbing quickly, which prevents bent needles and coring of the rubber septum.
Step 4: Invert the vial so the needle tip is submerged in the solution. Slowly pull the plunger back past your target dose by about 5 units.
Step 5: Check for air bubbles. If present, tap the syringe barrel firmly with your fingernail to move bubbles toward the needle. Push the plunger forward to expel air and excess solution back into the vial, stopping precisely at your target dose.
Step 6: Remove the needle from the vial. Immediately replace the needle cap using the one-handed scoop technique, never use two hands as it increases the risk of needlestick injury.
Step 7: Label the syringe. Write the dose in units and the date on the barrel with a permanent marker. If you are preparing multiple dose levels for a titration schedule, color-coding with different marker colors prevents dangerous mix-ups.
Repeat for each syringe. Use the same needle entry point on the vial septum each time to minimize additional puncture sites.
Proper storage after prefilling
Place all prefilled syringes in a clean, sealed container. A small plastic food storage container works perfectly. Store them in the refrigerator with the needle pointing up. This is critical, and here is why: if the needle points down, the solution pools around the needle hub where the plastic meets the metal, and this junction is the most vulnerable point for both leakage and contamination. Needle-up storage also prevents air bubbles from migrating to the needle end, which would affect your first few units of injection.
Position the container in the main body of the refrigerator, not in the door (temperature fluctuates too much) and not near the back wall (risk of accidental freezing). The middle shelf, toward the front, provides the most consistent temperature. This same principle applies to vial storage in the fridge.
How many syringes should you prefill at once?
More is not always better.
The temptation is to prefill an entire vial worth of doses in one session. And for some researchers, that makes perfect sense. But several factors should influence how many you prepare at once.
The 28-day rule
Never prefill more doses than you can use within 28 days. This is the conservative stability window for semaglutide in insulin syringes under refrigeration. Even if your reconstituted vial has a longer beyond-use date, the syringe environment is less protective than a sealed glass vial. The 28-day expiration guideline applies specifically here.
For weekly dosing, that means a maximum of 4 syringes per batch. For researchers who split their semaglutide dose twice a week, you could prepare up to 8 syringes, but this stretches the timeline and increases the risk of using a dose that has been sitting for nearly a month.
The practical sweet spot
Most experienced researchers find that prefilling 2-3 weeks of doses strikes the right balance between convenience and safety. This means:
Weekly dosing: 2-3 prefilled syringes per batch
Twice-weekly dosing: 4-6 prefilled syringes per batch
Preparing a smaller batch every 2-3 weeks also gives you regular opportunities to inspect your solution for changes. If the color of your semaglutide shifts, if cloudiness appears, or if you notice particles, catching these signs early prevents you from injecting compromised material. Knowing why semaglutide might turn red or other unexpected colors is part of responsible self-monitoring.
Dose titration considerations
If you are in the middle of a dose titration, the number of syringes you should prefill changes. During the first week on semaglutide or any dose increase, you might not know how you will respond. Prefilling four weeks of a dose you may need to adjust wastes both time and medication.
During titration phases, limit prefilling to 1-2 doses at most. Wait until you are on a stable maintenance dose before preparing larger batches. This approach also aligns with how semaglutide results develop week by week, since your body needs time to adjust at each dose level before committing to a longer supply.
Risks and safety concerns with prefilled semaglutide syringes
Prefilling semaglutide syringes is not without risk. Understanding these risks does not mean avoiding the practice altogether. It means mitigating them through proper technique and awareness.
Contamination risk
This is the biggest concern. Every time you handle a needle, open a package, or draw from a vial, you introduce potential contamination vectors. In a clinical pharmacy, this process happens under a laminar flow hood with HEPA-filtered air. At home, your kitchen counter is not that.
The contamination risk is manageable if you follow strict aseptic technique. But it is real. A study on insulin prefilled at home found that syringes remained sterile for up to 30 days when prepared with good technique and stored under refrigeration. The key phrase is "good technique." Cutting corners, touching needle tips, or working in a dusty or dirty environment dramatically increases the risk of introducing bacteria that bacteriostatic water alone cannot fully suppress.
If at any point during preparation you touch the needle tip, drop a syringe, or suspect contamination, discard that syringe and start fresh. The cost of one wasted syringe is nothing compared to the cost of an injection site infection or abscess.
Dose accuracy degradation
Insulin syringes are designed for single use. The graduation markings are accurate when the syringe is new, but the rubber plunger can compress slightly over time when held under spring tension, which happens when you draw a dose and cap the syringe. This compression can shift the apparent volume by 1-2 units over several weeks.
For researchers on higher doses, 1-2 units is negligible. If you are using a 5mg/mL concentration and drawing 50 units, a 2-unit variation represents about 4%. Manageable.
For those on very low doses, like the unit count for 1mg of semaglutide or especially 0.5mg, the same 2-unit variation could represent 10-15% of the dose. That is significant enough to affect both efficacy and side effect profiles. Researchers at lower doses should either avoid prefilling or use syringes within 7 days of preparation to minimize plunger compression effects.
The FDA position on prefilling
The FDA has issued guidance discouraging healthcare facilities from prefilling syringes outside of pharmacy-controlled environments. Their 2015 alert specifically addressed the risks of medication errors, contamination, and stability concerns when syringes are prepared ahead of time.
This guidance was directed at clinical settings where nurses were prefilling syringes for multiple patients. The individual researcher preparing their own doses is a different scenario, but the underlying risks the FDA identified remain relevant. Dosing errors, sterility concerns, and stability questions do not disappear because you are preparing your own medication rather than someone else preparing it for you.
Compounding pharmacies that distribute semaglutide in prefilled syringes must operate as 503B outsourcing facilities to do so legally and safely. These facilities use sterile compounding rooms, perform potency testing, and assign validated beyond-use dates. Your kitchen cannot replicate these conditions, which is why conservative practices are essential when prefilling at home.
Needle gauge and dead space considerations
Standard insulin syringes have a small amount of "dead space" in the needle hub, the area where the needle connects to the syringe barrel. This dead space holds a tiny amount of solution (approximately 0.01-0.05mL depending on the needle) that does not get injected. When you prefill a syringe, this dead space is filled with your semaglutide solution. Over time, evaporation through the needle tip can concentrate this small pocket, potentially causing a slight burning sensation during the initial portion of injection.
Low dead space syringes minimize this issue and are preferred for peptide preparation. If you are using standard insulin syringes, the dead space effect is minimal for single use but compounds across multiple days of storage. This is another reason to use prefilled syringes within 1-2 weeks rather than pushing the full 28-day window.
Prefilled syringes from compounding pharmacies versus doing it yourself
Not all prefilled syringes are created equal. There is a massive difference between syringes prefilled by a regulated compounding pharmacy and those you prepare at home.
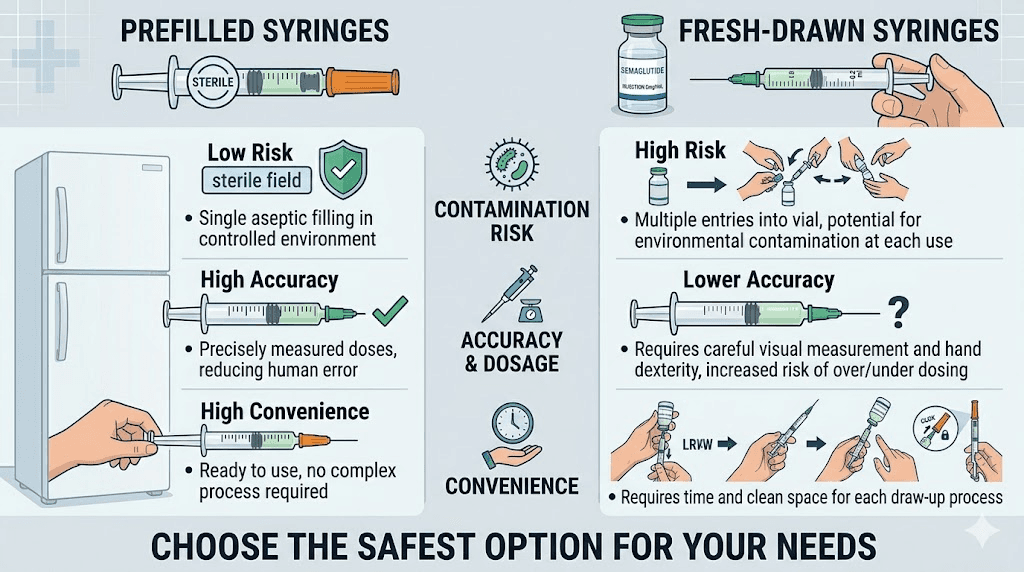
Pharmacy-prefilled syringes
Compounding pharmacies that provide semaglutide in prefilled syringes operate under strict regulatory oversight. The preparation happens in ISO Class 5 cleanrooms. Potency testing confirms dose accuracy. Sterility testing confirms the absence of microbial contamination. Beyond-use dates are based on validated stability studies, not estimates.
If your provider offers semaglutide in prefilled syringes from a 503B facility, this is generally the safest option. The convenience factor is identical to home prefilling, but the safety profile is substantially better. Pharmacies like Empower Pharmacy and Olympia Pharmacy have established reputations in the compounded semaglutide space, and understanding the landscape of compounded semaglutide options helps you make informed choices.
Home-prefilled syringes
When you prefill at home, you are acting as your own compounder. You control the sterility. You control the accuracy. You control the storage. And you bear the consequences if something goes wrong.
This is not meant to scare you away from the practice. Many researchers successfully prefill at home with no issues. But it requires treating the process with the same seriousness a pharmacist would. Casual preparation in between cooking dinner is not acceptable. Dedicated time, clean space, full attention.
When to choose each option
Factor | Pharmacy prefilled | Home prefilled |
|---|---|---|
Sterility assurance | High (tested) | Moderate (technique dependent) |
Dose accuracy | High (potency tested) | Good (depends on skill) |
Convenience | Excellent | Excellent |
Cost | Higher | Lower |
Flexibility | Limited to pharmacy doses | Any dose you need |
Beyond-use dating | Validated | Conservative estimate |
Best for | Standard dose schedules | Custom doses, titration, research |
Researchers who follow non-standard protocols, those doing customized semaglutide regimens or working with unusual concentrations, often find that home prefilling is the only practical option since pharmacies prepare fixed-dose syringes.
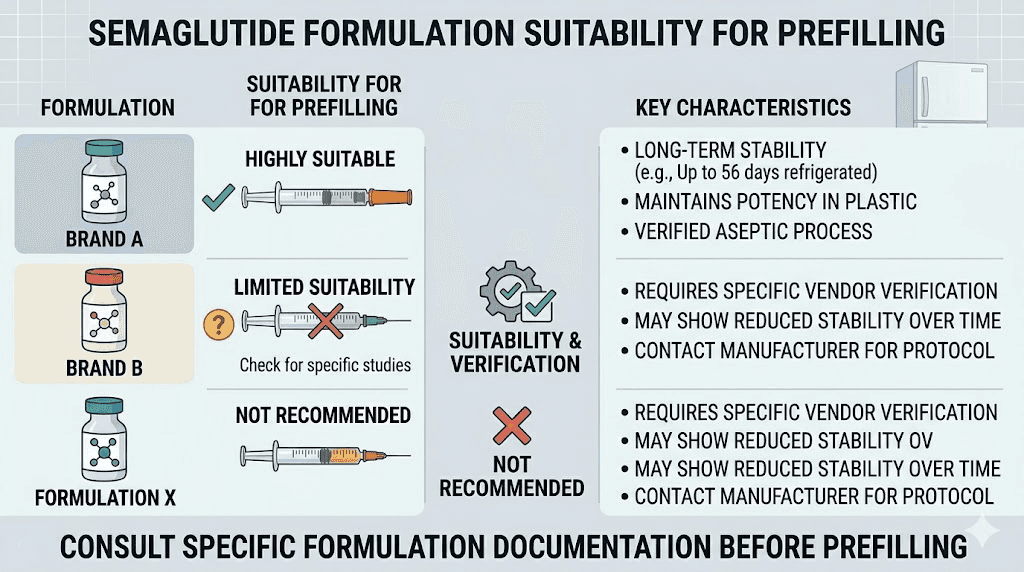
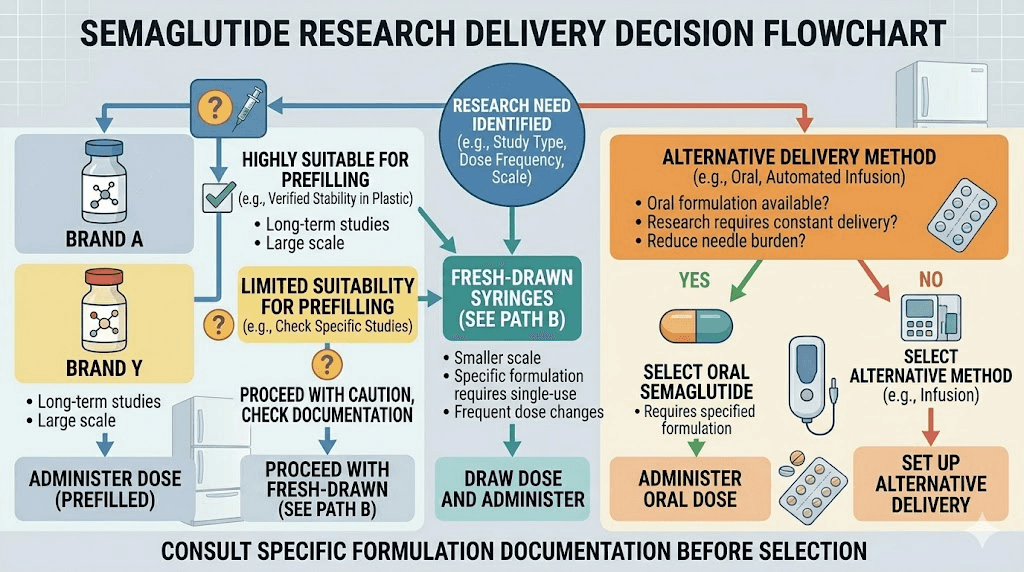
Semaglutide formulation types and prefilling compatibility
Not every form of semaglutide is equally suited for prefilling. The formulation you use determines whether prefilling is straightforward, possible with modifications, or simply not recommended.
Compounded lyophilized (powder) semaglutide
This is the most common scenario for researchers who prefill. You receive a vial of freeze-dried semaglutide powder, reconstitute it with bacteriostatic water, and draw your doses. The reconstituted solution is well-suited for prefilling because you control the concentration, you know exactly when reconstitution occurred, and bacteriostatic water provides preservative protection.
Use our peptide reconstitution calculator to determine exactly how much bacteriostatic water to add for your desired concentration. Getting the right amount of bacteriostatic water for 10mg or 5mg vials directly affects your dose accuracy in prefilled syringes.
Compounded liquid semaglutide (pre-mixed vials)
Some compounding pharmacies ship semaglutide already reconstituted in liquid form. These vials are also suitable for prefilling, but pay attention to two things. First, check whether the solution contains bacteriostatic water or a different diluent. Second, note the beyond-use date the pharmacy assigned. Your prefilled syringes cannot extend beyond this date, and ideally should be used well before it.
Compounded liquid vials from reputable sources like those reviewed in our Direct Meds guide or Belmar Pharmacy review typically use bacteriostatic water and provide clear expiration guidance.
Semaglutide with B12 or other additives
Many compounded semaglutide formulations now include vitamin B12 (cyanocobalamin), methylcobalamin, glycine, niacinamide, or L-carnitine. These blends, like the popular semaglutide glycine B12 blend, have additional stability considerations.
B12 is light-sensitive. Prefilled syringes containing B12 must be stored in an opaque container or wrapped in aluminum foil to prevent light degradation. Glycine acts as a stabilizer and may actually improve semaglutide stability in prefilled syringes. Niacinamide and L-carnitine add complexity but generally do not reduce the viability of prefilling.
The bottom line: compound blends can be prefilled, but store them carefully and lean toward shorter storage times (14-21 days rather than the full 28).
Brand-name semaglutide pens (Ozempic, Wegovy)
These are not candidates for prefilling. Brand-name semaglutide comes in manufacturer-sealed pens with built-in dose selection mechanisms. You cannot (and should not) extract solution from these pens to fill syringes. The pen is the delivery system, and it maintains its own sterile environment.
If you are on brand-name pens and want the convenience of prefilled doses, ask your provider about switching to compounded vials. Understanding the difference between peptide semaglutide and brand-name formulations helps clarify your options.
Oral and sublingual semaglutide
Obviously, oral semaglutide drops, sublingual formulations, and troches are not relevant to syringe prefilling. These alternative delivery methods have their own preparation and storage requirements.
Troubleshooting common prefilling problems
Even with careful preparation, you may encounter issues. Here is how to handle the most common ones.
Air bubbles in prefilled syringes
Small air bubbles are normal and not dangerous for subcutaneous injection. They will not cause an air embolism at the volumes involved in insulin syringes. However, they do affect dose accuracy because air displaces solution.
If you notice air bubbles developing in a prefilled syringe that was bubble-free when prepared, the most likely causes are temperature fluctuation (dissolved gases come out of solution as temperature changes) or a slight leak at the needle hub. For temperature-related bubbles, gently tap the syringe barrel to move the bubble toward the needle end, then push the plunger forward just enough to expel the air. Accept that you will lose a fraction of a unit, which is preferable to injecting with air in the barrel.
For persistent bubble formation, check that your refrigerator temperature is stable. Fluctuating between 33 and 45 degrees Fahrenheit causes exactly this kind of gas expansion and contraction.
Plunger becoming stiff or sticky
After several days in storage, you might find that the syringe plunger resists smooth movement. This happens because the silicone lubricant on the plunger can redistribute, especially in horizontal storage. It can also indicate that the solution has dried slightly around the plunger seal.
Do not force a stiff plunger. Gently roll the syringe between your palms to warm it slightly and redistribute the lubricant. If the plunger still resists, the syringe may be compromised. Discard it and use a fresh one from your batch.
Crystallization or precipitation
If you see crystals, cloudiness, or particles in a prefilled syringe, do not use it. Period. This indicates that the semaglutide has come out of solution, which can happen from temperature extremes, contamination, or simply exceeding the stability window. The same inspection criteria apply here as with semaglutide expiration assessment.
Discard any affected syringes. If multiple syringes from the same batch show precipitation, the entire batch is suspect, likely due to a storage issue affecting all of them.
Color changes
Semaglutide solution should be clear and colorless. Any yellowing, browning, or other color change in a prefilled syringe indicates degradation. Some semaglutide blends with B12 will have a pink or reddish tint that is normal, but this color should remain consistent. If a semaglutide B12 blend darkens significantly in a syringe compared to when you first drew it, that syringe should be discarded.
Leaking around the needle cap
A small amount of moisture around the needle cap is not unusual, especially if the syringe was stored cap-down (which you should not do). But visible fluid leakage means the seal is compromised. The dose inside may be inaccurate, and sterility cannot be guaranteed. Discard and replace.
Prefilling syringes for travel with semaglutide
Travel is one of the top reasons researchers prefill syringes. And it makes the most sense here. Transporting a glass vial with a separate bag of syringes, alcohol swabs, and reconstitution supplies is cumbersome and fragile. A few prefilled syringes in a small insulated case? Simple.
Air travel considerations
Prefilled syringes are permitted through TSA security. Medication that is medically necessary, including injectable medications with syringes, is allowed in carry-on luggage and does not need to fit in the quart-sized liquids bag. However, declaring your medication at the security checkpoint speeds up the process. Our full guide on traveling with semaglutide covers everything from airport protocols to international travel regulations.
For international flights, carry a letter from your prescriber or a copy of your prescription. Some countries are stricter about injectable medications crossing borders. Having documentation prevents delays and confiscation.
Keeping prefilled syringes cold during travel
Semaglutide needs refrigeration for optimal stability, but it tolerates room temperature for up to 28 days. For most trips, this means you do not need an active cooling system.
However, if you are traveling to a hot climate, temperatures above 86 degrees Fahrenheit (30 degrees Celsius) can degrade semaglutide faster. In these cases, use a small insulated travel case with a cooling element. Medical-grade travel coolers designed for insulin work perfectly for semaglutide syringes as well. Do not pack them in checked luggage where cargo hold temperatures are unpredictable. Always carry your syringes in your personal bag.
How many doses to prepare for travel
Calculate the number of injection days during your trip, then add one extra dose as a backup. If you are gone for two weeks with weekly dosing, prepare three syringes: two for your scheduled doses plus one in case of a dropped or contaminated syringe. The goal is to never be in a position where a mishap leaves you without medication.
If your trip extends beyond 28 days, you cannot prefill enough syringes to cover the entire duration safely. In this case, bring a vial and reconstitution supplies for the second half of the trip, and prefill only the first 2-3 weeks worth of doses.
Comparing prefilling with other convenience approaches
Prefilling syringes is not the only way to make semaglutide injection more convenient. Understanding the alternatives helps you choose the best approach for your specific needs.
Prefilled pens from compounding pharmacies
Some compounding pharmacies now offer semaglutide in pen-style devices similar to brand-name products. These provide pre-measured doses without the need for manual drawing. The trade-off is cost (significantly higher than vials) and dosing flexibility (pens offer fixed dose increments). For researchers on specific doses like 1.7mg, pen increments may not match exactly.
Drawing fresh doses each time
The traditional approach. Draw, inject, return the vial to the fridge. Maximum simplicity, maximum freshness, but maximum weekly effort. This remains the recommended approach for researchers who are new to semaglutide, still titrating, or uncomfortable with sterile technique. When you are just starting during your first week on semaglutide, sticking with fresh preparation each time makes the most sense until you are confident in your handling skills.
Having a partner or caregiver prepare doses
If sterile technique is a concern, having a healthcare-trained partner prepare prefilled syringes for you combines convenience with better aseptic practice. Nurses, pharmacists, or medically trained family members can prepare a batch using techniques they have practiced professionally. This is particularly valuable for researchers managing semaglutide fatigue or other side effects that make injection day preparation difficult.
Switching to alternative delivery methods
For researchers who find the entire syringe process burdensome, alternative delivery methods eliminate the question entirely. Oral semaglutide drops require no syringes at all. Sublingual formulations offer another needle-free option. And emerging technologies like GLP-1 patches may eventually make this entire discussion obsolete.
That said, injectable semaglutide remains the gold standard for bioavailability and predictable absorption. The convenience of prefilling helps maintain this advantage while reducing the practical burden. Comparing injectable versus oral peptides shows clear absorption differences that many researchers are not willing to sacrifice for convenience alone.
Dosage calculations for prefilled semaglutide syringes
Getting the math right before you start drawing is critical. Once solution is in a syringe, you cannot add more or remove some without compromising sterility.
Common concentrations and unit conversions
The number of units you draw depends entirely on your reconstitution concentration. Use the semaglutide dosage calculator for exact numbers, but here are common reference points:
5mg vial reconstituted with 2mL bacteriostatic water = 2.5mg/mL:
0.25mg = 10 units (referencing our 5mg/2mL dosage chart)
0.5mg = 20 units
1.0mg = 40 units (see how many mg is 40 units)
1.7mg = 68 units
2.4mg = 96 units
10mg vial reconstituted with 2mL bacteriostatic water = 5mg/mL:
0.25mg = 5 units
0.5mg = 10 units (compare with 10 units at different concentrations)
1.0mg = 20 units (see our 20 units conversion guide)
2.0mg = 40 units
2.4mg = 48 units
Use the semaglutide units to mg conversion guide if you need to work backward from your prescribed unit count to verify the milligram dose. The semaglutide reconstitution chart and mixing chart provide additional reference tables for different reconstitution volumes.
Choosing the right syringe size
Insulin syringes come in three common sizes: 0.3mL (30 units), 0.5mL (50 units), and 1.0mL (100 units). Match your syringe to your dose:
30-unit syringe: Best for doses below 25 units. The smaller barrel and finer graduation marks allow more precise measurement. Ideal for low-dose researchers on 0.25mg or those doing quarter-milligram doses.
50-unit syringe: Good for mid-range doses (20-45 units). Balances precision with capacity.
100-unit syringe: Necessary for larger doses or lower concentrations that require higher volumes. Less precise at low volumes but essential if your dose exceeds 50 units.
When prefilling, always use the smallest syringe that comfortably accommodates your dose. A 50-unit dose in a 100-unit syringe is harder to read precisely than the same dose in a 50-unit syringe. The markings are simply larger and easier to verify.
Calculating how many doses a vial provides
Before prefilling, calculate the total number of doses your vial contains. This prevents the frustrating situation of preparing your fourth syringe only to find the vial is empty halfway through.
The formula is straightforward. Total volume in the vial divided by volume per dose equals number of doses. For a 5mg vial reconstituted with 2mL of bacteriostatic water, at a dose of 0.5mg (20 units or 0.2mL), you get 10 doses. That is 10 weeks of supply from a single vial if dosing weekly.
In practice, you will get slightly fewer doses than the math suggests. Dead space in needles, solution clinging to vial walls, and the impossibility of extracting every last drop all reduce usable volume by approximately 5-10%. Plan for this. If the math says 10 doses, prepare for 9 reliable ones. Reference the 5mg vial dosage chart or 10mg dosage chart for pre-calculated numbers at common dose levels.
Syringe labeling and tracking systems
Labeling sounds like a minor detail. It is not. When you have four identical-looking syringes in a container in the refrigerator, mixing up doses is remarkably easy.
What to include on each label
Every prefilled syringe should be marked with:
Medication name: "Semaglutide" (or abbreviation like "SEM")
Dose: Both units and milligrams (e.g., "20u / 0.5mg")
Date prepared: The date you drew the syringe
Use by date: 28 days from preparation date
Sequence number: "1 of 4" or similar, so you use them in order
The FIFO principle
First In, First Out. Always use the oldest prefilled syringe first. This seems obvious, but when syringes look identical and you are groggy at 7am, reaching for whichever syringe is most accessible becomes default behavior. Numbering your syringes and storing them in order ensures you always use the oldest one first.
Tracking sheets for researchers managing multiple peptides
If you are researching semaglutide alongside other compounds, keeping track becomes even more critical. Some researchers use semaglutide alongside phentermine, or combine their GLP-1 protocol with other peptides. In these situations, a simple tracking sheet that logs each injection, the syringe used, the time, and any notes helps prevent dosing errors and provides useful data for optimizing your protocol.
SeekPeptides members get access to protocol tracking tools and dosing logs that simplify this process, especially for researchers running complex multi-compound protocols.
Special considerations for different dosing schedules
Standard semaglutide dosing is once weekly. But not every researcher follows the standard.
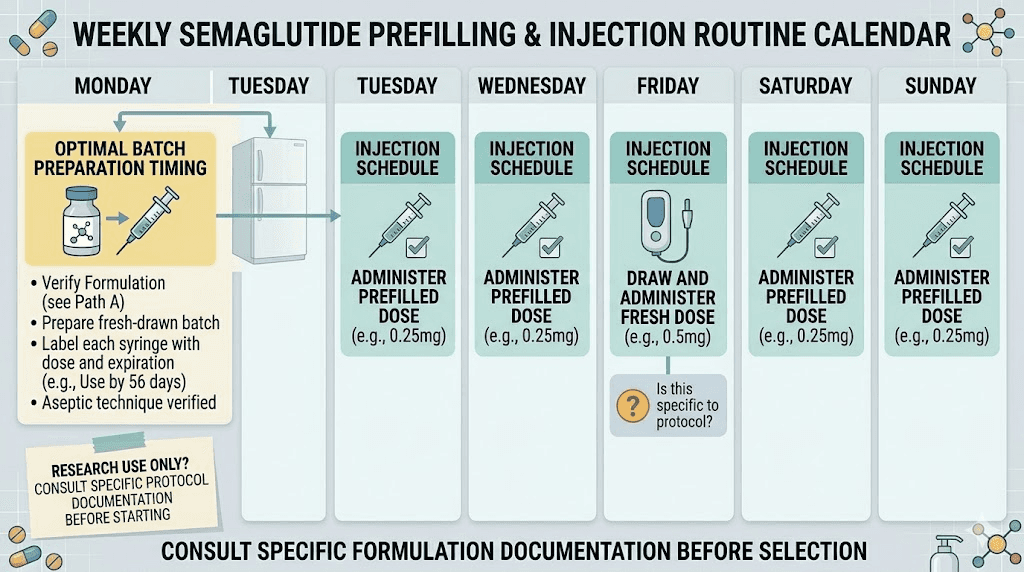
Weekly dosing (standard)
For once-weekly injectors, prefilling is most straightforward. Prepare 3-4 syringes at a time. Use one per week. The oldest syringe in your batch will be at most 21-28 days old when used, well within the stability window. Understanding the best time of day to take your semaglutide shot helps you plan when to pull a prefilled syringe from the fridge.
Split dosing (twice weekly)
Researchers who split their semaglutide dose twice weekly use syringes faster, which actually works in favor of prefilling. You go through the batch in half the time, meaning each syringe spends less time in storage. Prefilling 4-6 syringes provides 2-3 weeks of doses with the oldest syringe never exceeding 14-21 days.
Microdosing protocols
Microdosing semaglutide involves very small doses, sometimes daily. The tiny volumes involved (often under 5 units) make accurate measurement in stored syringes more challenging due to the plunger compression issue mentioned earlier. For microdosing protocols, fresh preparation is generally preferred over prefilling. The time savings from prefilling are minimal when the process of drawing up 3-5 units takes under a minute.
Dose titration periods
During titration, when you are gradually increasing your dose to manage side effects and find the optimal level, avoid prefilling large batches. You might need to adjust your dose based on how your body responds, and a batch of prefilled syringes at the wrong dose is wasted medication. Seeing how fast semaglutide works and monitoring your week-by-week results should guide dose decisions before committing to a prefilled batch.
Injection technique with prefilled semaglutide syringes
Using a prefilled syringe is slightly different from injecting a freshly drawn dose. Here is what you need to know.
Pre-injection preparation
Remove the prefilled syringe from the refrigerator 10-15 minutes before injection. Cold solution can cause more injection site discomfort and slower absorption. Let it reach a mild temperature naturally. Do not microwave, run under hot water, or place near a heater. Some researchers who experience GLP-1 injection site reactions find that warming the solution to room temperature beforehand reduces irritation significantly.
While the syringe warms, inspect it carefully. Hold it up to a light source. Check for particles, cloudiness, color changes, or air bubbles that were not present when you prepared it. If everything looks clear, proceed.
Choosing your injection site
The best injection site for semaglutide remains the same whether you are using a prefilled or freshly drawn syringe. The abdomen (at least 2 inches from the navel), the front of the thigh, and the back of the upper arm are all appropriate sites. Rotate between sites to prevent lipodystrophy, a condition where subcutaneous fat hardens from repeated injections in the same spot. Our semaglutide injection guide covers complete technique details.
The injection itself
Clean the injection site with an alcohol swab. Let it dry completely, as injecting through wet alcohol stings. Remove the needle cap from your prefilled syringe. Pinch a fold of skin at the injection site. Insert the needle at a 45-90 degree angle (90 degrees for most people with adequate subcutaneous fat, 45 degrees for thinner individuals). Push the plunger slowly and steadily. Hold for 5-10 seconds after the plunger is fully depressed to allow the solution to disperse. Withdraw the needle. Do not rub the site.
One thing to watch for with prefilled syringes: if the plunger feels slightly sticky from storage, do not force it quickly. A sudden forceful push can cause a jet of solution that stings and may not distribute properly under the skin. Steady pressure is the goal.
After injection
Dispose of the used syringe in a sharps container immediately. Note the injection date, site, and any reactions in your tracking log. Monitor the injection site for unusual redness, swelling, or pain that might indicate contamination. While some mild post-injection side effects are normal, signs of infection (increasing warmth, spreading redness, pus, or fever) require medical attention.
When you should NOT prefill semaglutide syringes
Prefilling is not appropriate in every situation. Knowing when to avoid it is as important as knowing how to do it.
When using sterile water instead of bacteriostatic water
If your semaglutide was reconstituted with plain sterile water (no preservative), do not prefill. Without benzyl alcohol to inhibit bacterial growth, any contamination introduced during drawing can multiply rapidly. Use sterile water reconstituted semaglutide within 24 hours, drawing each dose fresh.
When your technique is questionable
Be honest with yourself. If you have not practiced sterile technique, if your workspace is not clean, or if you are not confident in your ability to handle needles without contaminating them, prefilling introduces more risk than it eliminates. Get comfortable with drawing and injecting individual doses before attempting batch preparation.
When you are on unstable dosing
If your dose is being adjusted regularly, whether during initial titration or because you are experiencing issues like a semaglutide plateau or not losing weight on semaglutide, hold off on prefilling until your dose stabilizes.
When your semaglutide is near expiration
If your reconstituted vial is already 3-4 weeks old, prefilling additional syringes means those syringes will be used at 5-8 weeks post-reconstitution, potentially beyond the stability window. Only prefill from a relatively fresh vial. Check the overall shelf life of your semaglutide before preparing a batch.
When you lack proper storage
If your refrigerator temperature is unreliable, if you do not have a clean container for storage, or if other household members might tamper with medical supplies, the controlled environment necessary for safe prefilling does not exist. Fix the storage situation first.
Sterile technique deep dive for home prefilling
Sterile technique is not a single action. It is a system of habits that work together to prevent contamination. Miss one step and the entire system fails. Understanding this is what separates researchers who prefill safely from those who end up with infected injection sites or degraded peptides.
The three zones of contamination risk
Think of your workspace in three concentric zones. The inner zone is the critical area: needle tips, vial septum surfaces, and the interior of syringe barrels. These must remain sterile at all times. Nothing touches them except alcohol-swabbed surfaces and sterile solution.
The middle zone is the handling area: syringe barrels, vial bodies, and your gloved or freshly washed hands. These should be clean but do not need to be sterile. A stray fingerprint on the syringe barrel is not a problem. A fingerprint on the needle tip is.
The outer zone is everything else: your countertop, the air, nearby objects. Minimizing contamination from this zone means working in a clean space, avoiding unnecessary movement that stirs up dust, and keeping pets and other people away from your workspace during preparation. The same careful approach applies when you are learning how to give a semaglutide injection with a syringe for the first time.
Hand hygiene beyond basic washing
Washing hands with soap and water for 20 seconds is the minimum. For prefilling sessions where you will be handling multiple syringes over 10-15 minutes, consider these additional measures. Dry your hands with paper towels, not cloth. Apply hand sanitizer (60%+ alcohol) after drying. Avoid touching your face, hair, or phone during the entire process. If you need to answer the phone or scratch an itch, wash and sanitize again before returning to syringe preparation.
Some researchers wear nitrile gloves. Gloves are not strictly necessary if your hands are clean and you follow proper technique, but they add a barrier and serve as a reminder to maintain awareness of what you touch. If you wear gloves, change them if they become contaminated.
Alcohol swab technique that actually works
The way you use alcohol swabs matters more than most people realize. Swab the vial septum in a single direction, not back and forth. Back-and-forth motion drags contaminants back across the surface you just cleaned. One firm swipe from one side to the other. Let the alcohol dry completely for 10 seconds before puncturing. Wet alcohol on a needle does not sterilize it. Instead, it carries liquid contaminants through the septum into the vial.
Use a fresh swab for each vial puncture session. A single swab is adequate for cleaning the septum once, but if you need to reclean after an interruption, use a new one.
Managing the workspace during a prefilling session
A typical prefilling session for 4 syringes takes 15-20 minutes. During this time, your workspace needs to remain clean. Lay out a fresh paper towel as your working surface. Place the vial in the center. Arrange syringes on one side (unprepared) and the other side (prepared). This creates a clear left-to-right workflow that prevents accidentally reusing or skipping a syringe.
If the session is interrupted, cap the vial with an alcohol-swabbed surface before stepping away. When you return, re-swab and allow to dry before resuming. Treat every return to the workspace as a fresh start for contamination prevention.
Common mistakes researchers make when prefilling
After reviewing hundreds of community discussions and protocol reports, certain mistakes appear repeatedly. Avoiding these saves both medication and frustration.
Mistake 1: drawing doses from a near-empty vial
When a vial gets low, the remaining solution pools at the bottom and meniscus effects make accurate measurement nearly impossible. Air gets drawn into the syringe more easily. The temptation to tip and angle the vial to extract every last drop introduces a host of accuracy issues.
Stop drawing from a vial when the remaining volume drops below two full doses. The last bit of solution also tends to have higher concentration due to water evaporation through the septum over weeks of use, which means those final draws may contain more peptide per unit than expected. This is another reason why following a proper dosage chart and calculating total vial yields matters.
Mistake 2: not accounting for needle dead space
Researchers who forget about dead space consistently run short on their last syringe. Each standard insulin needle holds roughly 0.01-0.05mL in the hub that does not get injected and is also lost during the draw process. Over 8-10 draws from a vial, this dead space loss adds up to the equivalent of a full dose or more.
The fix is simple. When calculating your total doses per vial, subtract 10% from the theoretical yield. If math says 10 doses, plan for 9. This buffer accounts for dead space, wall adhesion, and the unusable residual at the bottom of the vial.
Mistake 3: storing syringes needle-down
This seems trivial. It is not. Needle-down storage means the solution sits against the needle hub seal, the weakest point of the syringe. It accelerates any potential leaking, concentrates solution around the metal-plastic junction where contamination risk is highest, and causes air bubbles to form at the plunger end where they are harder to remove before injection. Always store prefilled syringes needle-up.
Mistake 4: prefilling too many syringes at once
The enthusiasm of batch preparation can override good judgment. A researcher with a 10mg vial at 5mg/mL concentration on a 0.25mg weekly dose could theoretically prepare 40 syringes. That is 40 weeks of supply. And it would be a terrible idea.
Even under perfect refrigeration with bacteriostatic water, semaglutide stability in insulin syringes beyond 28 days is uncertain. Plunger compression accumulates. Adsorption to syringe walls continues. And the risk of one contaminated syringe among 40 means potentially discarding dozens of good doses after a single bad one. Keep batches small. 2-4 weeks maximum.
Mistake 5: reusing needles to reduce waste
Some researchers try to use the same needle to draw multiple doses before capping and storing, thinking this reduces vial septum punctures. The problem is that a needle that has been pushed through a rubber septum is no longer sharp. The tip deforms slightly, creating barbs that tear rather than pierce on subsequent use. This coring effect can push rubber particles into the vial, contaminating the remaining solution. One needle per syringe, every time.
Building a prefilling routine that works long-term
One-off prefilling is easy. Maintaining the habit consistently over months requires a system.
Weekly batch prep schedule
Choose a consistent day and time for your prefilling session. Many researchers align it with their injection day. For example, if you inject on Sunday mornings, your prefilling session happens Sunday after injection, when you have the vial out and your supplies ready. This way, you prepare next week and possibly the following week of doses while everything is accessible.
This approach also naturally reminds you to inspect your vial, check remaining volume, and assess whether you need to reconstitute a new vial soon. Staying ahead of your supply prevents the panicked last-minute preparation that leads to sloppy technique.
Inventory management
Keep a running inventory of your supplies. Track how many unreconstituted vials you have on hand, how many reconstituted vials are in the fridge, how many prefilled syringes are ready, and when the next batch needs to be prepared. A simple spreadsheet or notebook entry works. The key is preventing the situation where you need to inject but have no prepared dose, no clean syringes, or a vial that expired three days ago.
For researchers managing costs, understanding the peptide cost calculator numbers helps plan purchasing around your prefilling schedule. Buying in bulk reduces per-dose cost, but only if you can use everything before expiration.
Quality checks between batches
Before preparing a new batch, inspect any remaining syringes from the previous batch. Are they clear? Is the plunger still mobile? Any signs of leaking or discoloration? This 30-second inspection catches problems before they reach the injection stage.
Also check your vial. Is the reconstituted semaglutide still within its beyond-use date? Has the color remained consistent? Is the solution still crystal clear? Any deviation should trigger a new reconstitution rather than drawing from a potentially compromised vial. The standards for assessing whether expired semaglutide is still usable apply equally to vials and prefilled syringes.
Adapting your routine during life changes
Travel, illness, schedule changes, and dose adjustments all affect your prefilling routine. Build flexibility into your system. If you normally prefill 3 weeks of doses but have a trip coming up in 10 days, adjust that batch to 10 days worth instead. If you are restarting semaglutide after a break, you will likely be back at a lower dose, so previous batch sizes may not apply.
The researchers who maintain the most consistent protocols are those who treat their prefilling routine as a non-negotiable part of their week, like meal prep or medication management, rather than something they do when they feel like it.
Prefilling semaglutide versus tirzepatide: key differences
Many researchers use both semaglutide and tirzepatide, or are considering switching between them. If you have mastered prefilling semaglutide syringes, you might assume the same approach works for tirzepatide. It does, mostly, but several important differences deserve attention.
Stability profiles differ
Tirzepatide has a slightly different molecular structure as a dual GIP/GLP-1 receptor agonist, and its stability profile in insulin syringes has not been studied as extensively as semaglutide. The conservative approach is to use prefilled tirzepatide syringes within 21 days rather than the full 28-day window. Understanding how long tirzepatide lasts and its expiration timeline helps set appropriate prefilling windows.
The reconstitution process for tirzepatide follows similar principles. Our guide on how to reconstitute tirzepatide and the bacteriostatic water amounts for 10mg tirzepatide provides the foundation for accurate prefilling.
Concentration and dosing differences
Tirzepatide dosing schedules differ from semaglutide, and the unit counts per milligram depend on your reconstitution volume. The tirzepatide dosage in units guide and dosage chart in units help ensure your prefilled syringes contain the right amount. Common reference doses include 2.5mg in units, 5mg in units, and 10mg in units.
If you are managing both compounds simultaneously, which some researchers explore when combining semaglutide and tirzepatide or switching between them, rigorous labeling becomes critical. Use different colored markers for each compound. Store them in separate containers. Never rely on memory to distinguish identical-looking syringes containing different medications.
Compound blends add complexity
Tirzepatide compounds often include additives like B12, glycine, methylcobalamin, or levocarnitine. The same light sensitivity and storage concerns mentioned for semaglutide blends apply here. The tirzepatide glycine B12 compound is one of the more common formulations, and knowing what color tirzepatide with B12 should be helps you spot degradation in prefilled syringes.
The broader question of comparing these two peptides is covered in our comprehensive semaglutide versus tirzepatide comparison and side effect comparison.
Managing side effects during prefilled syringe use
Side effects from semaglutide are not influenced by whether you use a prefilled or freshly drawn syringe. The peptide is identical. But the convenience of prefilling can change how you manage certain side effects in practical terms.
Gastrointestinal side effects and dose flexibility
The most common semaglutide side effects are gastrointestinal: nausea, constipation, bloating, burping, and dizziness. When these hit hard, your prescriber might recommend reducing your dose temporarily. If you have a batch of prefilled syringes at your current dose, you cannot easily reduce them without wasting medication.
The workaround is straightforward. Simply inject fewer units from the prefilled syringe. If your syringe contains 40 units but you need to drop to 30, inject to the 30-unit mark. You will waste the remaining 10 units in that syringe, but the alternative, continuing at a dose causing significant side effects, is worse. Learning to manage how semaglutide makes you feel during the adjustment period involves this kind of flexibility.
Injection site reactions
Some researchers experience injection site reactions that are more pronounced with prefilled syringes than with freshly drawn doses. This is usually attributable to the solution temperature. A freshly drawn dose from a room-temperature vial is warmer than a prefilled syringe pulled directly from the fridge. Cold solution causes more vasoconstriction, slower absorption, and more local irritation.
The fix is patience. Let the prefilled syringe sit at room temperature for 15 minutes before injecting. That small window brings the solution close to body temperature and dramatically reduces injection site discomfort. Choosing the optimal injection site and rotating locations also minimizes reactions over time.
Tracking side effects across your prefilled batch
Here is an underappreciated advantage of prefilling. When all syringes in a batch come from the same draw session, using the same vial at the same concentration, any variation in side effects between doses is almost certainly attributable to other factors like diet, hydration, sleep, or stress. This eliminates the variable of "was this dose slightly different?" and gives you cleaner data for understanding what truly affects your response.
Pairing your prefilling routine with a consistent semaglutide diet plan and paying attention to foods that support your protocol while avoiding foods that worsen side effects creates a comprehensive system where prefilling is just one element of a well-managed semaglutide routine. Resources like our supplement guide for GLP-1 users and probiotic recommendations round out the support structure.