Mar 10, 2026

Before you draw your next dose, read this carefully. A single mistake in converting milligrams to units can mean injecting five times the intended amount of semaglutide, or barely injecting anything at all. The FDA has received multiple reports of dosing errors with compounded semaglutide, and almost every case traces back to one root cause: confusion between milligrams and semaglutide units.
The answer to how many units is 0.5 mg of semaglutide depends entirely on the concentration of your specific vial. That is not a technicality. That is the single most important factor in getting this right. A 0.5 mg dose from a 5 mg/mL vial requires 10 units on an insulin syringe. The same 0.5 mg dose from a 2.5 mg/mL vial requires 20 units. Same medication, same dose in milligrams, completely different volume in the syringe. Get this wrong and the consequences range from a wasted injection to genuinely dangerous side effects.
This guide breaks down the exact conversion for every common concentration you might encounter. It covers the math, the practical syringe technique, the common mistakes, and everything you need to confidently measure a 0.5 mg dose of semaglutide from any vial sitting in your refrigerator. Whether you are using compounded semaglutide, a pre-filled pen, or a lyophilized vial you reconstituted yourself, the principles are the same. The math is the same. And getting it right matters more than most people realize.
The quick answer for every concentration
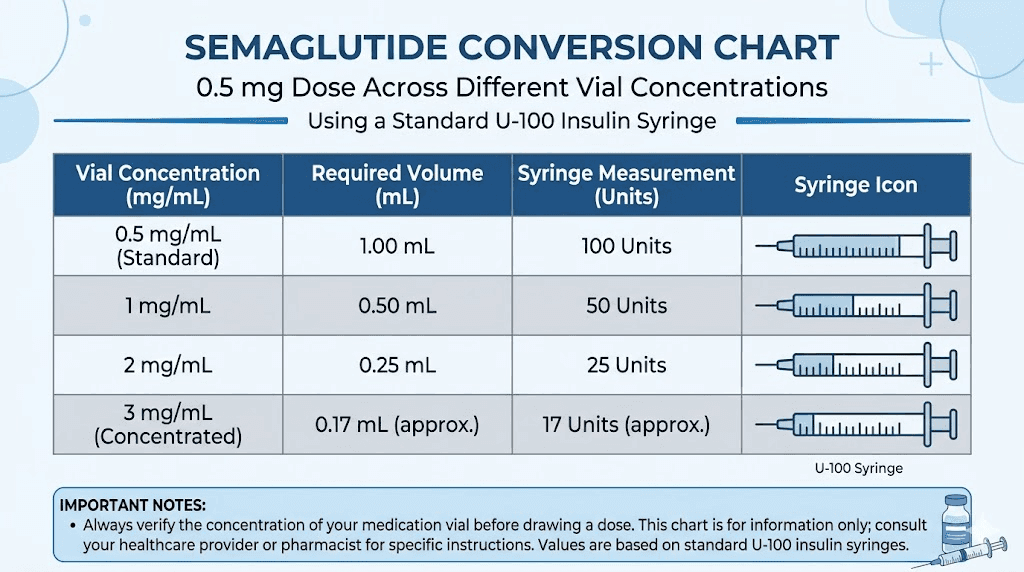
Here is the direct answer. For a 0.5 mg dose of semaglutide, the number of units you draw on a U-100 insulin syringe depends on the concentration printed on your vial label.
Vial concentration | Units to draw for 0.5 mg | Volume in mL |
|---|---|---|
1 mg/mL | 50 units | 0.50 mL |
2 mg/mL | 25 units | 0.25 mL |
2.5 mg/mL | 20 units | 0.20 mL |
3 mg/mL | 16.7 units | 0.167 mL |
3.33 mg/mL | 15 units | 0.15 mL |
5 mg/mL | 10 units | 0.10 mL |
6.67 mg/mL | 7.5 units | 0.075 mL |
10 mg/mL | 5 units | 0.05 mL |
Print this table. Photograph it. Keep it next to your vials. But before you draw anything, verify the concentration on YOUR specific vial. Not the concentration from a chart you found online. Not the concentration someone mentioned in a forum. The actual number printed on the label of the vial in your hand.
If you are working with a 5 mg vial that was reconstituted with a specific amount of bacteriostatic water, your concentration depends on exactly how much water you added. We will cover that calculation in detail below.
Why concentration changes everything about your dose
This is where most dosing errors begin. People search for a simple answer, find a number, and inject that number of units without checking their specific vial. That approach works exactly once, by accident, when the concentration happens to match.
Concentration tells you how many milligrams of semaglutide are dissolved in each milliliter of liquid. A vial labeled 5 mg/mL contains five milligrams of semaglutide in every milliliter. A vial labeled 2.5 mg/mL contains half that amount in the same volume. So if you need 0.5 mg from a 5 mg/mL vial, you draw a very small volume. If you need 0.5 mg from a 2.5 mg/mL vial, you draw twice as much liquid to get the same amount of medication.
Think of it like coffee. A double espresso and a large americano can contain the same amount of caffeine. One is concentrated into a tiny cup. The other is diluted across a large mug. The caffeine content is identical. The volume is completely different.
Semaglutide works the same way. Your dose in milligrams stays constant. The volume you inject changes based on how concentrated the solution is. And because insulin syringes measure volume in units (where 100 units equals 1 mL), the number of units changes with concentration too.
Common concentrations and where they come from
Different sources of semaglutide produce different concentrations. Understanding where your vial came from helps you know what concentration to expect, though you should always verify against the label.
Compounding pharmacies typically produce semaglutide in concentrations of 2.5 mg/mL, 5 mg/mL, or occasionally 1 mg/mL. Some pharmacies that add vitamin B12 or glycine may use slightly different concentrations depending on the total volume of the formulation. If your vial comes from an established compounding pharmacy, the concentration will be clearly printed on the label.
Lyophilized (freeze-dried) semaglutide vials come as a powder. You determine the concentration yourself when you add bacteriostatic water. A 5 mg vial reconstituted with 1 mL of water yields 5 mg/mL. The same vial reconstituted with 2 mL yields 2.5 mg/mL. This is precisely why reconstitution matters so much for accurate dosing.
Pre-filled Ozempic pens use a fixed concentration of 1.34 mg/mL across all pen strengths. But pen users do not need to calculate units manually because the pen dial handles the conversion. This article focuses primarily on vial-and-syringe dosing, which is where the calculation becomes critical.
The concentration problem with compounded formulations
Here is a scenario that causes real problems. A researcher uses a 5 mg/mL vial from one pharmacy and draws 10 units for a 0.5 mg dose. That is correct. They run out and order from a different pharmacy that ships a 2.5 mg/mL formulation. They draw 10 units out of habit. They just injected 0.25 mg instead of 0.5 mg, half their intended dose.
The reverse is worse. Switching from 2.5 mg/mL to 5 mg/mL while drawing the same 20 units means injecting 1.0 mg instead of 0.5 mg. Double the dose. That jump can trigger significant gastrointestinal side effects, dizziness, and potentially dangerous complications.
Always recalculate when you receive a new vial.
The formula that works for any concentration
One formula. Any concentration. Any dose. Learn this and you will never need to rely on someone else's chart again.
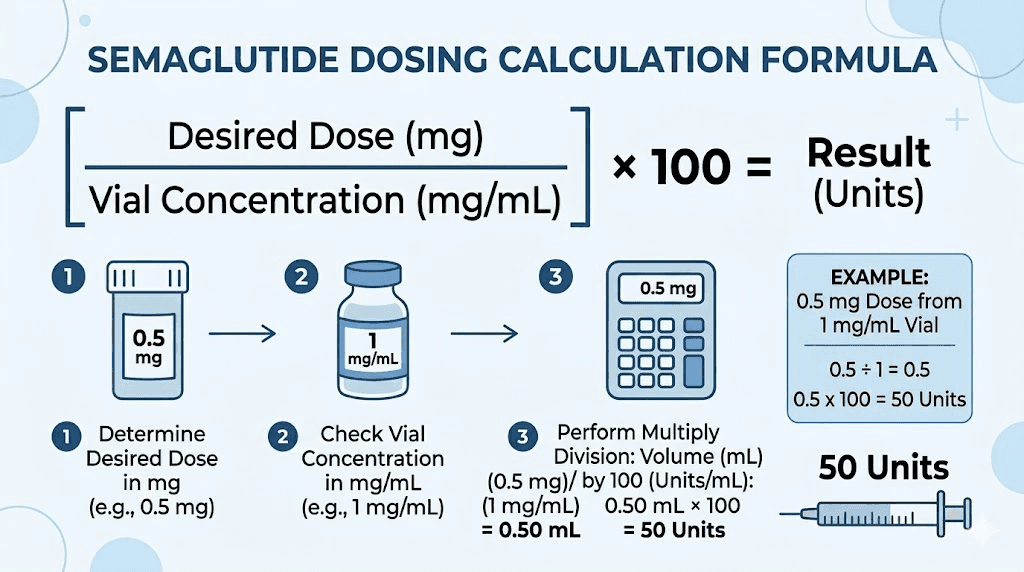
Units = (Desired dose in mg / Concentration in mg per mL) x 100
That is it. The entire conversion in one line. The number 100 comes from the fact that a standard U-100 insulin syringe contains 100 units per milliliter. So you calculate the volume in milliliters, then multiply by 100 to convert to syringe units.
For 0.5 mg from a 5 mg/mL vial:
(0.5 / 5) x 100 = 10 units
For 0.5 mg from a 2.5 mg/mL vial:
(0.5 / 2.5) x 100 = 20 units
For 0.5 mg from a 10 mg/mL vial:
(0.5 / 10) x 100 = 5 units
See how it works? The higher the concentration, the fewer units you draw. The lower the concentration, the more units you draw. The dose in milligrams stays exactly the same. You can also use the SeekPeptides semaglutide dosage calculator to run this calculation instantly for any concentration and any dose.
Breaking down the math step by step
Some people freeze when they see a formula. Fair enough. Let us walk through it with plain language.
Step one: look at your vial. Find the concentration. It will say something like "5 mg/mL" or "2.5 mg per mL" or possibly just list the total amount and volume (like "5 mg in 2 mL"). If it lists total amount and volume, divide the total milligrams by the total milliliters to get the concentration. A 5 mg vial in 2 mL equals 2.5 mg/mL.
Step two: divide your desired dose by that concentration. You want 0.5 mg. Your concentration is 5 mg/mL. Divide 0.5 by 5. You get 0.1. That number is your dose in milliliters.
Step three: multiply by 100 to convert milliliters to insulin syringe units. 0.1 times 100 equals 10. Draw 10 units.
Three steps. Check concentration. Divide dose by concentration. Multiply by 100. Done.
If math is not your strength, peptide calculators exist for exactly this reason. Input your vial size, your reconstitution volume, and your desired dose, and the calculator handles everything. SeekPeptides offers free dosage calculation tools that eliminate the guesswork entirely.
Every common vial size and the exact units for 0.5 mg
Let us get specific. These are the most common semaglutide vial configurations you will encounter, along with the exact units to draw for a 0.5 mg dose from each one.
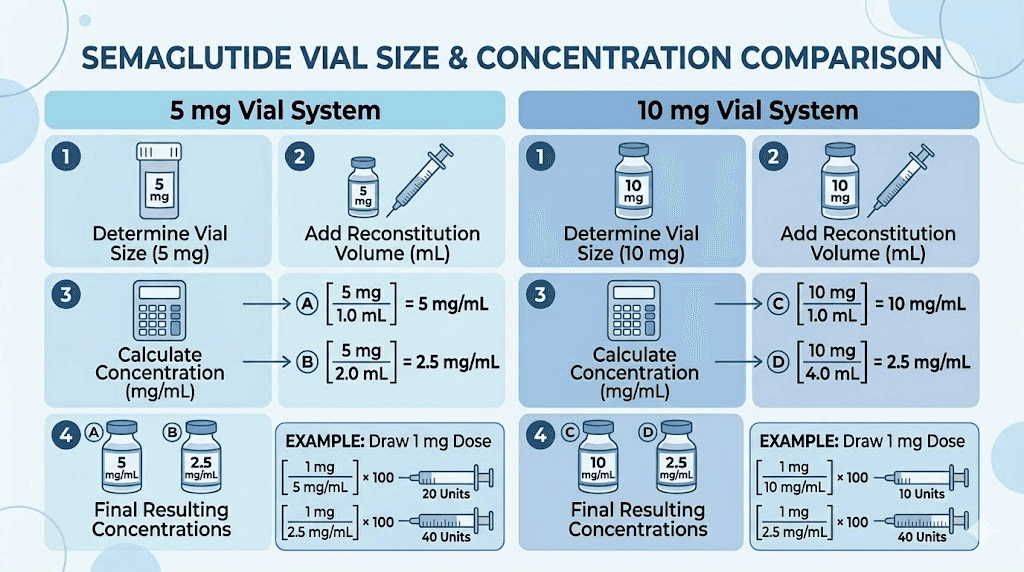
5 mg vials
The 5 mg vial is the most popular size for researchers using compounded semaglutide. The concentration depends entirely on how much bacteriostatic water was added during reconstitution, or the concentration set by the compounding pharmacy.
5 mg vial reconstituted with | Resulting concentration | Units for 0.5 mg |
|---|---|---|
0.5 mL BAC water | 10 mg/mL | 5 units |
1.0 mL BAC water | 5 mg/mL | 10 units |
1.5 mL BAC water | 3.33 mg/mL | 15 units |
2.0 mL BAC water | 2.5 mg/mL | 20 units |
2.5 mL BAC water | 2 mg/mL | 25 units |
Most guides recommend adding 2 mL of bacteriostatic water to a 5 mg vial, producing a 2.5 mg/mL concentration. At that concentration, 0.5 mg equals exactly 20 units. Clean. Easy to measure. No awkward fractions on the syringe. For detailed reconstitution instructions for this vial size, see our 5 mg semaglutide reconstitution guide.
Some researchers prefer adding just 1 mL to get a higher 5 mg/mL concentration. This means smaller injection volumes (10 units for 0.5 mg) but less room for measurement error. Each unit on the syringe represents more medication. For a complete chart of every dose at this concentration, check our 5 mg vial dosage chart.
If you are unsure how much bacteriostatic water to add to a 5 mg vial, 2 mL is the standard recommendation. It provides a manageable concentration that makes measuring most dose increments straightforward.
10 mg vials
The 10 mg vial offers more total medication per vial, which means more doses before you need a new vial. Here is how the concentration changes based on reconstitution volume.
10 mg vial reconstituted with | Resulting concentration | Units for 0.5 mg |
|---|---|---|
1.0 mL BAC water | 10 mg/mL | 5 units |
2.0 mL BAC water | 5 mg/mL | 10 units |
3.0 mL BAC water | 3.33 mg/mL | 15 units |
4.0 mL BAC water | 2.5 mg/mL | 20 units |
With a 10 mg vial, the most common recommendation is 2 mL of bacteriostatic water, yielding 5 mg/mL. At that concentration, 0.5 mg is a clean 10 units. Some clinics recommend 3 mL for a 3.33 mg/mL concentration, where 0.5 mg equals 15 units. Both work. The key is knowing which one applies to your specific vial.
For the full mixing and dosing breakdown, our 10 mg vial dosage chart covers every possible dose at every common concentration. And if you need help with the reconstitution process itself, the 10 mg reconstitution guide walks through each step.
Pre-mixed compounded vials
If your semaglutide arrives already mixed as a liquid (not a powder you reconstitute), the concentration is set by the pharmacy. Common pre-mixed concentrations include 2 mg/mL, 2.5 mg/mL, and 5 mg/mL. Some B12 combination formulations use concentrations like 2.5 mg/mL or 5 mg/mL depending on the pharmacy.
For pre-mixed vials, the math is straightforward. Check the label. Apply the formula. Draw your units. No reconstitution variables to worry about.
How reconstitution determines your conversion
If you are working with lyophilized (freeze-dried) semaglutide, the amount of bacteriostatic water you add during reconstitution directly determines your concentration, which directly determines how many units equal 0.5 mg.
This is not optional knowledge. This is the foundation of accurate dosing.
The reconstitution equation
Concentration = Total peptide in vial (mg) / Total water added (mL)
A 5 mg vial plus 2 mL of water equals 2.5 mg/mL. A 5 mg vial plus 1 mL of water equals 5 mg/mL. The peptide amount stays the same. The water volume changes the concentration. And the concentration changes your unit calculation.
Some researchers add less water to minimize injection volume. Some add more water to make precise measurements easier. Neither approach is wrong, as long as you calculate your units based on the actual concentration you created. Our semaglutide reconstitution chart shows the resulting concentration for every common water volume and vial size combination.
Recommended reconstitution for easy 0.5 mg dosing
If you want the simplest possible measurement for a 0.5 mg dose, here are the cleanest options.
5 mg vial + 1 mL BAC water = 5 mg/mL. Draw exactly 10 units. Clean number, easy to read on the syringe. The downside is that 5 mg/mL is a relatively high concentration, so each unit represents 0.05 mg. Small measurement errors have a bigger impact.
5 mg vial + 2 mL BAC water = 2.5 mg/mL. Draw exactly 20 units. Still a clean number. The slightly lower concentration means each unit represents 0.025 mg, so you have more room for minor measurement imprecision. This is the most commonly recommended reconstitution volume for 5 mg vials.
10 mg vial + 2 mL BAC water = 5 mg/mL. Same 10-unit draw for 0.5 mg, but your vial lasts twice as long since it contains double the medication.
For a complete walkthrough of the reconstitution process, including proper technique to preserve peptide integrity, our peptide reconstitution guide covers everything. You can also use the reconstitution calculator to determine exact concentrations before you even open the vial.
What if you do not know your concentration
This happens more often than it should. Someone reconstituted a vial weeks ago and cannot remember how much water they added. Or a vial arrived from a pharmacy without a clear concentration label.
If you genuinely cannot determine the concentration, do not guess. Do not estimate. Do not use a chart from a different vial. Contact the pharmacy that supplied the medication and ask. If you reconstituted it yourself and forgot the amount of water, it is safer to start with a fresh vial and document everything this time.
Guessing at concentration is how serious dosing errors happen. A 2x overdose of semaglutide can cause severe nausea and gastrointestinal distress lasting several days. A 5x overdose, which is entirely possible if you confuse a 1 mg/mL concentration with a 5 mg/mL one, could require medical attention.
Step-by-step guide to measuring 0.5 mg with an insulin syringe
Knowing the number is one thing. Actually drawing it accurately from the vial is another. Let us walk through the physical process of measuring a 0.5 mg dose using a U-100 insulin syringe.
Understanding your syringe
A standard U-100 insulin syringe holds 1 mL of liquid, divided into 100 units. Each small line on the syringe represents 1 unit (0.01 mL). Syringes come in different total capacities. A 0.3 mL syringe holds up to 30 units. A 0.5 mL syringe holds up to 50 units. A 1.0 mL syringe holds up to 100 units.
For a 0.5 mg dose, you will typically draw between 5 and 25 units depending on concentration. A 0.3 mL (30-unit) syringe works well for most scenarios and provides the most precise markings for small volumes. The finer gradations make it easier to hit your target exactly.
Drawing the dose
Wash your hands thoroughly. Clean the vial stopper with an alcohol swab and let it dry completely.
Pull back the syringe plunger to the unit marking that matches your calculated dose. If your concentration is 5 mg/mL, pull to 10 units. If your concentration is 2.5 mg/mL, pull to 20 units. This draws air into the syringe.
Insert the needle through the rubber stopper. Push the plunger to inject the air into the vial. This equalizes pressure and makes drawing the liquid easier.
Invert the vial so the stopper faces down and the needle tip is submerged in the liquid. Pull the plunger back slowly to your target unit marking. Check for air bubbles. If you see any, tap the syringe gently with your finger to move bubbles to the top, then push the plunger slightly to expel them. Draw back again to your target if needed.
Read the measurement at the top edge of the rubber plunger, not the bottom. This is where accuracy matters most. For detailed injection technique, our semaglutide injection guide covers proper form, angle, and site selection. And for optimal injection site placement, the abdomen is generally recommended, though the thigh and upper arm work well too.
Double-checking your measurement
Before injecting, confirm three things.
First, check the concentration on your vial label one more time. Match it to the unit count in your syringe. Second, look for air bubbles. Even a small bubble displaces medication and reduces your actual dose. Third, verify the plunger sits at the correct line. Off by one line on a 5 mg/mL vial means a 0.05 mg error. Off by one line on a 10 mg/mL vial means a 0.1 mg error. Precision matters, especially at higher concentrations.
Why 0.5 mg is a critical dose in the semaglutide protocol
The 0.5 mg dose is not arbitrary. It occupies a specific and important position in the standard semaglutide titration schedule, and understanding why helps you appreciate what this dose is doing in your body and what to expect.
Where 0.5 mg fits in the titration ladder
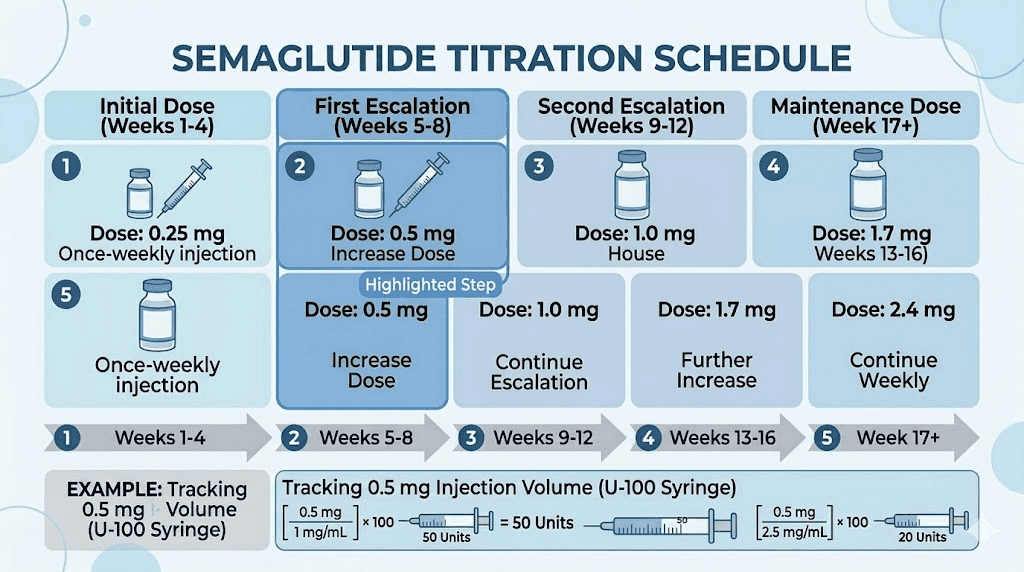
The standard semaglutide dosing protocol follows a gradual escalation designed to minimize side effects while allowing the body to adjust to the medication. The typical schedule looks like this.
Phase | Weekly dose | Duration | Purpose |
|---|---|---|---|
Initiation | 0.25 mg | 4 weeks | Introduction and tolerance assessment |
Step 2 | 0.5 mg | 4 weeks | First therapeutic dose |
Step 3 | 1.0 mg | 4 weeks | Standard therapeutic dose |
Step 4 | 1.7 mg | 4 weeks | Enhanced efficacy |
Maintenance | 2.4 mg | Ongoing | Maximum therapeutic dose |
At 0.5 mg, you have moved past the introductory phase. This is the first dose where many people begin noticing meaningful appetite suppression. The 0.25 mg starting dose exists primarily to let your digestive system adapt. The 0.5 mg dose is where the actual therapeutic work begins for many users.
Clinical trials showed that even the 0.5 mg dose produces measurable weight loss compared to placebo, approximately 5.7 pounds more than placebo over the study period. That said, most weight loss protocols aim for higher maintenance doses. The 0.5 mg phase is a stepping stone, not the destination for most people.
What to expect at the 0.5 mg dose
Everyone responds differently. But there are patterns worth knowing.
Appetite changes become more noticeable. Many people report feeling satisfied with smaller meals, reduced cravings for high-calorie foods, and less frequent hunger between meals. This is the GLP-1 receptor agonist mechanism doing what it was designed to do, slowing gastric emptying and signaling satiety to the brain. For a detailed breakdown of what semaglutide feels like at each dose, see our guide on how semaglutide makes you feel.
Side effects may appear or intensify compared to the 0.25 mg dose. The most common include mild nausea (especially in the first 24-48 hours after injection), reduced appetite (which is technically the desired effect), occasional constipation, and fatigue. Most of these diminish within the first week at each new dose level. If side effects are severe or persistent, that is information your healthcare provider needs. For a timeline on when side effects typically appear, check when you feel side effects after injection.
Some people feel great at 0.5 mg and stay there. Others need higher doses for meaningful results. There is no single right answer. The protocol is designed to be flexible.
How long to stay at 0.5 mg
The standard recommendation is at least 4 weeks before increasing to 1.0 mg. Some protocols extend this to 6-8 weeks if the person is responding well and tolerating the dose without issues. There is no rush to escalate. Moving up too quickly increases the risk of gastrointestinal side effects without necessarily improving outcomes.
If you are losing weight steadily at 0.5 mg and side effects are manageable, staying at this dose is perfectly reasonable. The goal is the lowest effective dose, not the highest tolerable one. For perspective on how long people typically stay on semaglutide, treatment duration varies widely based on individual goals and response.
Comparing 0.5 mg to other semaglutide doses in units
Seeing where 0.5 mg sits relative to other doses helps you understand the full dosing landscape. Here is a comprehensive comparison using the two most common concentrations.
At 5 mg/mL concentration
Dose | Units to draw | Volume (mL) |
|---|---|---|
0.25 mg | 5 units | 0.05 |
0.5 mg | 10 units | 0.10 |
1.0 mg | 20 units | 0.20 |
1.7 mg | 34 units | 0.34 |
2.4 mg | 48 units | 0.48 |
At 5 mg/mL, the jumps between doses are relatively small in terms of syringe volume. Going from 0.25 mg to 0.5 mg means drawing just 5 more units. Going from 0.5 mg to 1.0 mg means drawing an additional 10 units. These small increments are easy to measure accurately on a 0.3 mL or 0.5 mL syringe. For the complete chart at this concentration, see our 5 mg/mL dosage guide.
At 2.5 mg/mL concentration
Dose | Units to draw | Volume (mL) |
|---|---|---|
0.25 mg | 10 units | 0.10 |
0.5 mg | 20 units | 0.20 |
1.0 mg | 40 units | 0.40 |
1.7 mg | 68 units | 0.68 |
2.4 mg | 96 units | 0.96 |
At 2.5 mg/mL, the volumes are larger. A 0.5 mg dose requires 20 units. Higher doses like 1.7 mg and 2.4 mg start approaching the full capacity of a 1.0 mL syringe. This is one reason some researchers prefer higher concentrations for maintenance doses, the injection volume stays manageable.
Notice how the unit count exactly doubles when the concentration is halved. That mathematical relationship holds for any two concentrations. If you know the units for one concentration, you can calculate another by simple ratio. Our comprehensive conversion chart shows every dose at every common concentration in a single reference table.
If you are curious about higher doses like 1.7 mg in units or 2.4 mg in units, we have dedicated guides for each step of the titration ladder.
Microdosing and dose splitting at 0.5 mg
Some practitioners and researchers explore modified dosing strategies at the 0.5 mg level. Two approaches come up frequently.
Splitting the 0.5 mg dose
Instead of injecting 0.5 mg once per week, some people split the dose across two injections. This means injecting 0.25 mg twice per week, typically spaced 3-4 days apart. The total weekly dose remains 0.5 mg, but the medication is distributed more evenly.
Why would someone do this? The primary reason is managing side effects. Semaglutide levels peak roughly 1-3 days after injection and then gradually decline. Some people experience strong nausea or appetite suppression in the first 48 hours followed by a return of hunger by day 6 or 7. Splitting the dose creates more stable blood levels throughout the week.
If you are splitting at 5 mg/mL concentration, each injection would be 5 units (0.25 mg). At 2.5 mg/mL, each injection would be 10 units. Precise measurement becomes even more critical at these smaller volumes.
Transitioning from 0.25 mg to 0.5 mg
The jump from 0.25 mg to 0.5 mg represents a doubling of the dose. For most people this transition goes smoothly, especially after four weeks of adaptation at 0.25 mg. But if you experienced notable side effects at 0.25 mg, you might consider an intermediate step.
Some protocols suggest moving to 0.375 mg for two weeks before reaching 0.5 mg. At 5 mg/mL, that would be 7.5 units (splitting the difference between 5 and 10). At 2.5 mg/mL, that would be 15 units. This is not part of the standard FDA-approved titration but represents a practical approach some practitioners use for sensitive individuals.
Common mistakes when measuring 0.5 mg of semaglutide
These mistakes happen constantly. Some are harmless. Some are dangerous. All are preventable.
Mistake 1: using the wrong concentration for your calculation
This is the most dangerous mistake and the most common. Someone reads online that "0.5 mg equals 10 units" and draws 10 units from a 2.5 mg/mL vial. They just injected 0.25 mg instead of 0.5 mg. The reverse scenario, drawing 20 units from a 5 mg/mL vial thinking it is 2.5 mg/mL, delivers 1.0 mg instead of 0.5 mg.
The fix is simple. Always, every single time, check the concentration on your specific vial before drawing. Treat every new vial as if it might be different from the last one, because sometimes it is.
Mistake 2: confusing mg and units
Milligrams measure the amount of active medication. Units measure the volume of liquid in the syringe. They are not the same thing. They are not interchangeable. 0.5 mg does not mean 0.5 units. Drawing 0.5 units (if you could even measure that small) would be an absurdly tiny amount of medication from almost any concentration.
This confusion is responsible for the most severe dosing errors reported to the FDA. People draw 50 units thinking that matches 0.5 mg, when 50 units from a 5 mg/mL vial actually delivers 2.5 mg, five times the intended dose. For a deep dive on this conversion relationship, our units to mg guide explains exactly how these two measurements relate to each other.
Mistake 3: air bubbles in the syringe
Air bubbles take up space that should contain medication. A small air bubble in a 20-unit draw might reduce your actual dose by 5-10%. While a subcutaneous air bubble itself is not dangerous (the body absorbs small amounts of injected air safely), the underdosing can affect your results.
Tap the syringe with your fingernail to move bubbles to the top. Push the plunger gently to expel them. Then readjust to your target volume.
Mistake 4: reusing concentrations from a previous vial
You finished one vial from a pharmacy that supplied 5 mg/mL. You order from a new source. The new vial is 2.5 mg/mL. You draw 10 units out of habit. You just halved your dose without realizing it. Always recalculate when starting a new vial, even from the same pharmacy. Formulations can change.
Mistake 5: reading the syringe incorrectly
On a U-100 syringe, the numbered markings (10, 20, 30, etc.) correspond to units, not milligrams. The small lines between numbers each represent 1 unit on most syringes, though some 1.0 mL syringes have 2-unit increments. Know which syringe you are using. A 0.3 mL syringe typically has single-unit markings. A 1.0 mL syringe may have markings every 2 units.
If precision is critical (and it should be), use the smallest syringe that can hold your dose. For a 10-unit draw, a 0.3 mL syringe gives you the most accurate measurement. For a 20-unit draw, a 0.3 mL or 0.5 mL syringe works well.
What to do if you accidentally draw too much or too little
Mistakes happen. Here is how to handle them.
Drew too much
If you have not injected yet, simply push the plunger to expel the excess back into the vial. Readjust to the correct measurement. No medication is wasted because it goes right back where it came from.
If you already injected a higher dose than intended, do not panic. A single dose of 1.0 mg instead of 0.5 mg is within the normal therapeutic range and will not cause serious harm for most people. You may experience more pronounced side effects like nausea, reduced appetite, or bloating for a few days. Stay hydrated, eat small bland meals, and note the error so you can correct it next time.
If you accidentally injected significantly more than intended (3x or more your usual dose), contact your healthcare provider. While semaglutide has a wide safety margin, very large doses can cause severe nausea, vomiting, and other gastrointestinal complications that may need medical management.
Drew too little
If you realize before injecting, draw up additional medication to reach the correct volume. If you already injected a lower dose, you have two options. You can accept the lower dose for this week, it will not set you back significantly. Or you can draw and inject the difference if you catch the error immediately.
Do not try to "make up" a missed dose by doubling the next one. Semaglutide has a long half-life (approximately 7 days), so a slightly lower dose one week will not dramatically affect your overall trajectory. Our guide on what to expect your first week on semaglutide covers how the medication builds up in your system over time.
How 0.5 mg of semaglutide compares to tirzepatide doses
Many researchers compare semaglutide and tirzepatide when choosing a GLP-1 protocol. The dosing scales are different between these two peptides, and understanding the equivalency helps when considering a switch or comparing results.
Semaglutide at 0.5 mg roughly corresponds to tirzepatide at the 2.5 mg starting dose in terms of where each sits on its respective titration schedule. Both represent early therapeutic doses, past the initiation phase but below maximum efficacy. For a detailed breakdown of how doses map between these two medications, see our semaglutide vs tirzepatide dosage chart.
The unit conversion for tirzepatide follows the exact same formula as semaglutide, just with different concentrations. If you are curious about tirzepatide dosing in units, our tirzepatide units guide covers every concentration and dose level. And if you are thinking about switching from semaglutide to tirzepatide, the conversion chart helps you find the equivalent starting point.
Side effect profiles differ between the two as well. Our side effect comparison breaks down exactly what to expect from each medication and where the key differences lie.
Tracking your doses accurately
At 0.5 mg weekly, one vial should last a specific number of doses. Knowing how many doses your vial contains helps you plan refills, track usage, and spot any discrepancies that might indicate measurement errors.
How many 0.5 mg doses in each vial
Vial size | Number of 0.5 mg doses | Duration at weekly dosing |
|---|---|---|
3 mg | 6 doses | 6 weeks |
5 mg | 10 doses | 10 weeks |
10 mg | 20 doses | 20 weeks (about 5 months) |
20 mg | 40 doses | 40 weeks (about 10 months) |
These numbers assume perfect measurement with zero waste. In practice, you will lose small amounts to the needle dead space (the liquid that stays in the needle hub) and occasional measurement imprecision. Most people get 1-2 fewer doses than the theoretical maximum from each vial.
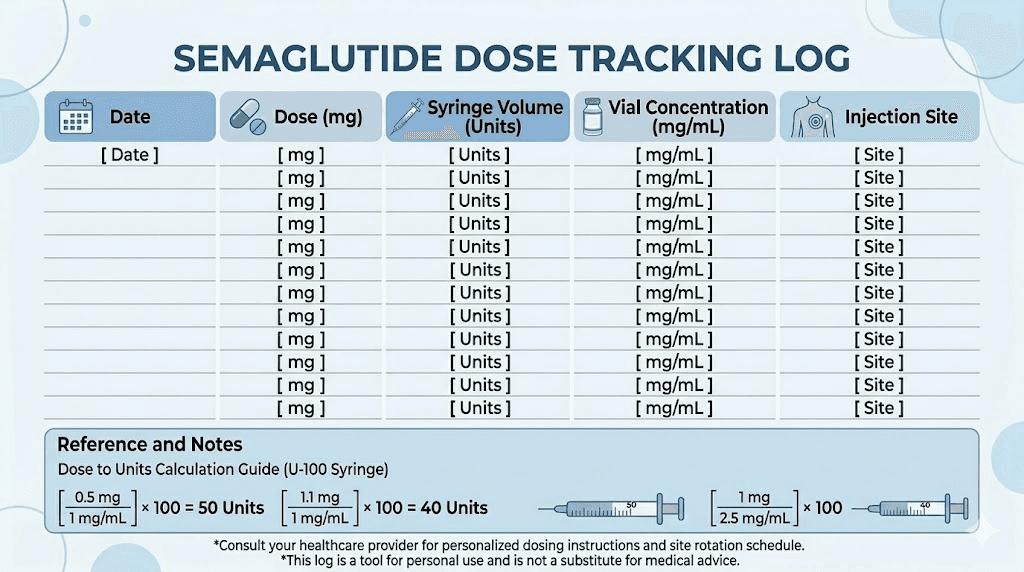
Track each injection in a log. Record the date, the dose in milligrams, the units drawn, and the concentration of the vial. This creates a reference you can look back on if anything seems off. It also helps your healthcare provider understand your dosing history if questions arise.
When planning your supply and budget, our peptide cost calculator can help estimate per-dose costs across different vial sizes and sources. And for a broader comparison of cost across different pharmacies and formulations, the affordable peptide guide covers pricing strategies.
Storage matters for dose accuracy
Semaglutide potency degrades if stored improperly. A vial that has lost potency means your 0.5 mg dose might deliver less active medication than expected, even if your measurement is perfect. Store reconstituted semaglutide in the refrigerator at 36-46 degrees Fahrenheit (2-8 degrees Celsius).
Reconstituted semaglutide is generally considered stable for approximately 28 days in the refrigerator. Some compounded formulations may last longer depending on preservatives and preparation methods. Check with your pharmacy for their specific stability data.
Never freeze reconstituted semaglutide. Avoid leaving it at room temperature for extended periods. If your vial was accidentally left out or arrived warm during shipping, assess the situation carefully. Brief temperature excursions (a few hours) are usually fine. Extended exposure to heat can reduce potency significantly.
Understanding different syringe types and sizes
Not all syringes are created equal, and the type you use affects how easily you can measure a 0.5 mg dose.
U-100 insulin syringes (standard)
These are the standard for peptide dosing. 100 units per mL. Available in 0.3 mL (30 units max), 0.5 mL (50 units max), and 1.0 mL (100 units max) sizes. For a 0.5 mg dose, the 0.3 mL or 0.5 mL sizes provide the best precision because their markings are spaced further apart relative to the volume you are measuring.
Tuberculin (TB) syringes
TB syringes measure in milliliters rather than units. They are marked in 0.01 mL increments up to 1.0 mL. Some people prefer these because the measurement is in mL directly, eliminating the units conversion step. For a 0.5 mg dose from a 5 mg/mL vial, you would draw to the 0.10 mL mark. From a 2.5 mg/mL vial, draw to the 0.20 mL mark.
The math is simpler with TB syringes: mL = mg / concentration. No need to multiply by 100. However, insulin syringes typically have finer needles (29-31 gauge) that cause less discomfort during injection. TB syringes often come with larger gauge needles that may require a separate needle for injection.
Needle gauge considerations
For subcutaneous injection of semaglutide, 29-31 gauge needles are standard. These are thin enough to minimize discomfort while still allowing the slightly viscous semaglutide solution to pass through easily. Our peptide injection guide covers needle selection, angle of insertion, and proper technique for comfortable injections.
Concentration-specific quick reference cards
Here are expanded reference tables for the three most commonly encountered concentrations. Keep the one that matches your vial.
Quick reference: 5 mg/mL concentration
Dose (mg) | Units | mL |
|---|---|---|
0.125 | 2.5 | 0.025 |
0.25 | 5 | 0.05 |
0.375 | 7.5 | 0.075 |
0.5 | 10 | 0.10 |
0.75 | 15 | 0.15 |
1.0 | 20 | 0.20 |
1.25 | 25 | 0.25 |
1.5 | 30 | 0.30 |
1.7 | 34 | 0.34 |
2.0 | 40 | 0.40 |
2.4 | 48 | 0.48 |
This concentration works beautifully for the entire titration range. Even the maximum 2.4 mg dose fits easily in a standard 0.5 mL syringe. Our semaglutide syringe dosage chart provides these tables in a printable format.
Quick reference: 2.5 mg/mL concentration
Dose (mg) | Units | mL |
|---|---|---|
0.125 | 5 | 0.05 |
0.25 | 10 | 0.10 |
0.375 | 15 | 0.15 |
0.5 | 20 | 0.20 |
0.75 | 30 | 0.30 |
1.0 | 40 | 0.40 |
1.25 | 50 | 0.50 |
1.5 | 60 | 0.60 |
1.7 | 68 | 0.68 |
2.0 | 80 | 0.80 |
2.4 | 96 | 0.96 |
At 2.5 mg/mL, all measurements land on clean numbers, making this concentration popular with compounding pharmacies. The trade-off is larger injection volumes at higher doses. A full 2.4 mg dose requires 96 units (0.96 mL), which approaches the maximum capacity of a 1.0 mL syringe. For the full dosage breakdown at this concentration, see our semaglutide dosage chart in units.
Quick reference: 3.33 mg/mL concentration
Dose (mg) | Units | mL |
|---|---|---|
0.25 | 7.5 | 0.075 |
0.5 | 15 | 0.15 |
1.0 | 30 | 0.30 |
1.7 | 51 | 0.51 |
2.4 | 72 | 0.72 |
The 3.33 mg/mL concentration (common with 10 mg vials reconstituted with 3 mL of water) produces some slightly less clean unit numbers. The 0.5 mg dose at 15 units is still easy to measure. But 0.25 mg at 7.5 units requires hitting the midpoint between two syringe lines, which demands careful technique.
Semaglutide blends and how they affect unit calculations
Many compounding pharmacies now offer semaglutide blended with other ingredients. These additions can subtly affect the concentration and, by extension, your unit calculations.
Semaglutide with B12 (cyanocobalamin or methylcobalamin)
Semaglutide with B12 is one of the most popular compounded formulations. The B12 adds volume to the solution but the semaglutide concentration is calculated after accounting for the total volume. So if the label says 5 mg/mL, that is the semaglutide concentration regardless of how much B12 is in there. Your unit calculation stays the same.
The key is reading the label correctly. Some pharmacies list the semaglutide concentration separately from the B12 concentration. Others might list the total contents and volume. Use only the semaglutide concentration for your dosing calculation. Our B12 combination dosage chart covers the most common formulations and their exact unit conversions.
Other popular blends include semaglutide with glycine, semaglutide with L-carnitine, and semaglutide with niacinamide. In each case, the same rule applies: use the semaglutide concentration from the label for your unit calculation. The additional ingredients do not change the math.
B12 blend dosage charts by pharmacy
Different pharmacies formulate their blends at different concentrations. The semaglutide B12 dosage chart covers the most common pharmacy-specific formulations. If you are using a blend from Empower Pharmacy, Olympia Pharmacy, or another major compounder, our pharmacy-specific guides include the exact concentrations and unit conversions for their formulations.
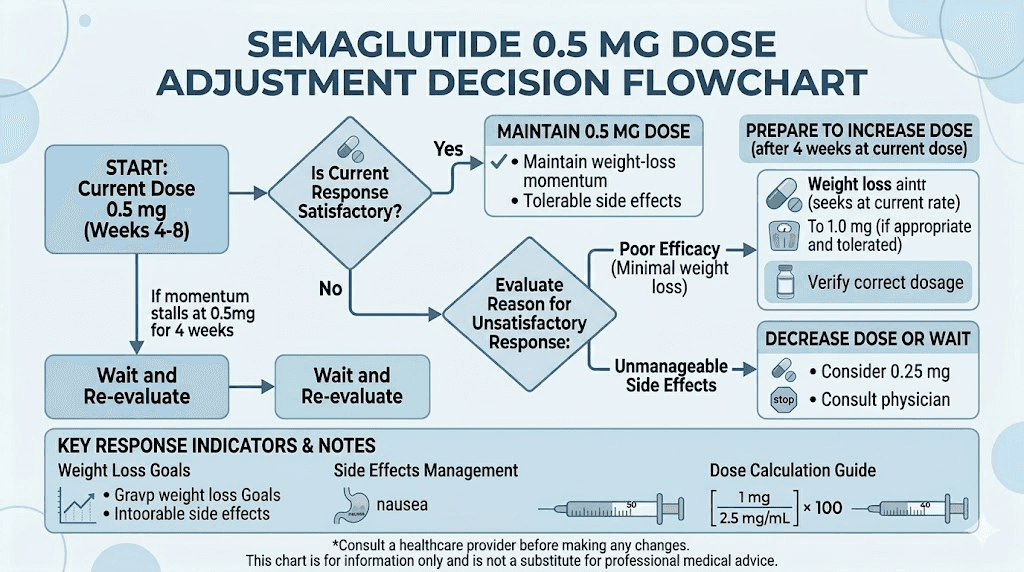
When to adjust beyond the standard 0.5 mg dose
Not everyone follows the textbook titration schedule. Understanding when and why practitioners adjust dosing helps you have informed conversations with your healthcare provider.
Signs you may need a higher dose
After 4 or more weeks at 0.5 mg, some indicators suggest your body may benefit from an increase to 1.0 mg.
Appetite suppression has faded. In the first week or two at 0.5 mg, you likely noticed reduced hunger. If that effect has diminished significantly and you are eating closer to pre-treatment amounts, your body may have partially adapted to this dose level. Some appetite return is normal, but if it is back to baseline, a dose increase may be warranted.
Weight loss has stalled. If you have been at 0.5 mg for 4+ weeks and the scale has stopped moving despite consistent dietary habits, a dose increase often restarts progress. Our guide on why weight loss stalls on semaglutide covers other factors to check before assuming you need more medication.
Side effects have fully resolved. If you tolerated 0.5 mg without any gastrointestinal effects, you likely have room to tolerate a higher dose. This is actually the intended signal that your body has adapted and is ready for the next step.
Signs you should stay at 0.5 mg longer
You are still losing weight at a satisfactory rate. If the scale is moving in the right direction, there is no clinical reason to increase dose just because the calendar says four weeks have passed.
You are still experiencing side effects. Persistent nausea, constipation, or other GI effects at 0.5 mg suggest your body needs more time to adapt before adding more medication.
Your appetite is well-managed. If you feel satisfied with meals, have minimal cravings, and are eating an appropriate amount, the current dose is working. More is not necessarily better.
Signs you may need to lower your dose
Severe or persistent side effects that interfere with daily life warrant a conversation about dose reduction. Some people find that 0.5 mg is too much and do better staying at 0.25 mg longer or even permanently. Others find that splitting the dose, as discussed earlier, manages side effects without reducing the total weekly amount.
If fatigue is overwhelming, if nausea prevents eating anything at all, or if you are experiencing significant dizziness, these are signals to discuss with your healthcare provider rather than push through.
Timing and administration tips at the 0.5 mg dose
Getting the units right is essential. But so is how and when you administer the dose.
Best day and time
Semaglutide is injected once per week, on the same day each week. The specific day does not matter pharmacologically, but it matters practically. Many people choose to inject on a day when potential side effects (mainly nausea) would be least disruptive. Injecting on a Friday evening means any nausea hits during the weekend rather than the workweek. For a detailed analysis of timing strategies, our best time to take semaglutide guide covers the options.
Consistency matters more than the specific day or time. Taking it every Monday at 8 AM is better than taking it randomly on different days. The 7-day half-life means the medication works best with regular, predictable dosing intervals.
Injection site rotation
Rotate between injection sites to prevent lipodystrophy (changes in fat tissue at the injection site). The three standard subcutaneous injection sites are the abdomen (at least 2 inches from the navel), the front of the thigh, and the back of the upper arm. For placement details and techniques, see our injection site guide.
Some people find that certain injection sites produce less nausea or discomfort than others. If you notice a pattern, there is nothing wrong with favoring a site that works best for you, as long as you still rotate within that area (for example, alternating between left and right sides of the abdomen).
What to eat (and avoid) at the 0.5 mg dose
The 0.5 mg dose often reduces appetite enough to change eating patterns. This is a feature, not a bug. But it means paying attention to nutrition becomes important. When you eat less overall, the quality of what you eat matters more.
Prioritize protein. Many researchers on semaglutide struggle to meet protein targets because appetite is suppressed. Protein preserves muscle mass during weight loss, and muscle loss is one of the main concerns with GLP-1 medications. For specific meal ideas, our guides on best foods to eat on semaglutide and foods to avoid provide practical guidance.
Hydration is equally critical. Semaglutide can cause constipation, and dehydration makes it worse. Aim for at least 64 ounces of water daily. More if you are active or in a warm climate.
Oral semaglutide versus injectable at the 0.5 mg dose
A note on oral semaglutide. The 0.5 mg dose discussed in this article refers to injectable semaglutide. Oral semaglutide (brand name Rybelsus) uses completely different dosing. The oral form comes in 3 mg, 7 mg, and 14 mg tablets because oral bioavailability is much lower than injectable. So 0.5 mg orally is not equivalent to 0.5 mg injected. These are fundamentally different dosing scales.
If you are interested in oral semaglutide options including sublingual drops and ODT formulations, see our dedicated guides. But do not attempt to convert between oral and injectable doses using the tables in this article. They apply exclusively to injectable semaglutide.
Using calculators and tools for accuracy
Manual calculation works. But technology makes it faster and eliminates arithmetic errors.
The SeekPeptides semaglutide dosage calculator lets you input your vial concentration and desired dose, then instantly shows the units to draw. It handles every concentration, every dose, and accounts for common vial sizes.
For reconstitution calculations specifically, the peptide reconstitution calculator tells you what concentration you will get for any combination of peptide amount and water volume. Use it before you add water to your vial so you know exactly what concentration to expect.
SeekPeptides provides these tools free of charge because accurate dosing is fundamental to safe peptide research. Calculation errors are the single most common source of dosing problems, and they are entirely preventable with the right tools.
For researchers who want even more comprehensive support, SeekPeptides members access personalized protocol builders, detailed titration guides, and expert-reviewed dosing resources that go well beyond basic calculators. The membership includes access to a community of experienced researchers who have navigated these exact dosing questions and can provide practical guidance based on real experience.
Frequently asked questions
Is 0.5 mg of semaglutide the same as 10 units?
Only if your vial concentration is 5 mg/mL. At 2.5 mg/mL, 0.5 mg equals 20 units. At 10 mg/mL, it equals 5 units. The unit count depends entirely on concentration. Always check your specific vial before drawing. Use our conversion chart to find the exact units for your concentration.
How do I know what concentration my semaglutide is?
Check the label on your vial. Pre-mixed formulations from compounding pharmacies will list the concentration (usually in mg/mL). If you reconstituted the vial yourself, divide the total peptide content by the amount of water you added. For example, 5 mg of peptide plus 2 mL of bacteriostatic water equals 2.5 mg/mL.
Can I use a regular syringe instead of an insulin syringe?
You can use a tuberculin (TB) syringe, which measures in milliliters instead of units. For a 0.5 mg dose from a 5 mg/mL vial, draw to 0.10 mL. From a 2.5 mg/mL vial, draw to 0.20 mL. Standard syringes (3 mL, 5 mL) are too large for accurate measurement of these small volumes and should not be used.
What if I accidentally took 1.0 mg instead of 0.5 mg?
A single dose of 1.0 mg is within the normal therapeutic range and is unlikely to cause serious harm. You may experience increased nausea, reduced appetite, or other side effects for a few days. Stay hydrated and eat bland foods. Do not skip your next dose to compensate. Resume your normal 0.5 mg dose the following week.
How many 0.5 mg doses can I get from a 5 mg vial?
Theoretically, 10 doses (5 mg total divided by 0.5 mg per dose). In practice, you will likely get 8-9 doses due to needle dead space and minor measurement losses. This means one vial covers approximately 8-10 weeks of weekly dosing at 0.5 mg. For cost planning, see our peptide cost calculator.
Is 0.5 mg enough for weight loss?
Clinical trials showed measurable weight loss at 0.5 mg compared to placebo. However, most weight loss protocols target higher maintenance doses (1.7 to 2.4 mg) for optimal results. The 0.5 mg dose is typically a transitional step, not a long-term maintenance dose for most people. See our guide on how fast semaglutide works for realistic timelines at each dose level.
Should I split my 0.5 mg dose into two injections?
Some practitioners recommend splitting the weekly dose (two injections of 0.25 mg) to reduce side effects and maintain more stable blood levels. This is not part of the standard protocol but may help if you experience significant nausea or appetite fluctuations throughout the week. Discuss with your healthcare provider before changing your dosing schedule. More details in our dose splitting guide.
How long should I stay on 0.5 mg before increasing?
The standard recommendation is at least 4 weeks at 0.5 mg before considering an increase to 1.0 mg. Some people stay at 0.5 mg for 6-8 weeks if they are responding well or still experiencing side effects. There is no benefit to rushing the titration. For the full timeline, see our week-by-week results guide.
External resources
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your concentrations stay accurate, your measurements stay precise, and your results stay consistent.