Mar 18, 2026

Three weeks into her semaglutide protocol, Jen noticed something strange. Not nausea. Not the appetite changes she had been expecting. A burning sensation when she used the bathroom. Then urgency. Then frequency. She wondered if her injection was somehow responsible, and a quick search confirmed she was not alone in asking the question.
The relationship between semaglutide and urinary tract infections is more nuanced than a simple yes or no. Clinical trials involving thousands of participants did not flag UTIs as a significant adverse event. The FDA prescribing information for Ozempic, Wegovy, and Rybelsus does not list urinary tract infections among common side effects. Yet anecdotal reports persist, forum threads multiply, and researchers continue investigating possible indirect connections that could explain why some people develop UTIs after starting GLP-1 therapy.
This guide breaks down what the clinical evidence actually shows, explains the indirect mechanisms that could raise your risk, identifies who is most vulnerable, and provides actionable prevention strategies you can start using today. Whether you are already on semaglutide and worried about a recent UTI, or considering starting treatment and want to understand your risk profile, every question gets answered here. SeekPeptides has analyzed the research so you do not have to piece it together from scattered forum posts and conflicting blog articles.
What the clinical evidence actually says about semaglutide and UTIs
Start with the data. The SUSTAIN trial program, which evaluated semaglutide for type 2 diabetes across multiple Phase 3 studies enrolling thousands of participants, did not identify urinary tract infections as a statistically significant adverse event compared to placebo. The STEP trial program, which studied semaglutide 2.4 mg for weight management, told the same story. UTIs showed up in both treatment and control groups at roughly comparable rates.
That matters.
It means the highest quality evidence available, randomized controlled trials with large sample sizes, does not support a direct causal link between semaglutide and urinary tract infections. The FDA reviewed this data before approving Ozempic, Wegovy, and Rybelsus, and UTIs are not listed in the prescribing information as a common or even uncommon adverse reaction. If you are researching semaglutide tips for getting started, understanding what the medication does and does not cause is an important foundation.
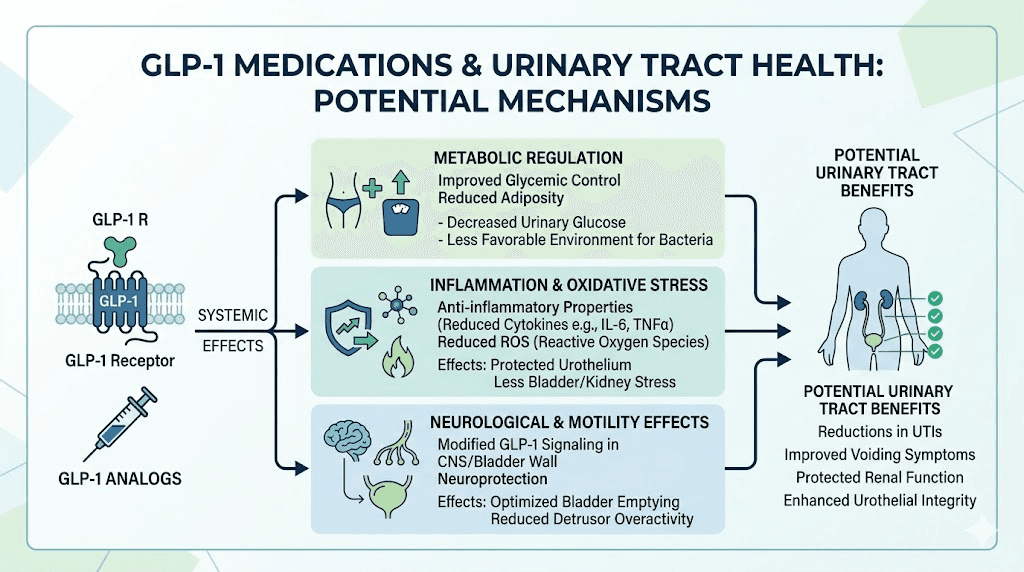
A study published in the Journal of Urology examined semaglutide utilization in weight management and its implications for urinary tract infections and urolithiasis specifically. The findings suggested that semaglutide use for weight management in non-diabetic individuals did not increase the risk of kidney stones and actually decreased the risk of UTI. This is a critical finding that often gets lost in the noise of anecdotal reports.
But clinical trials have limitations. They run for defined periods. They exclude certain populations. They track predefined endpoints. The real-world picture, where millions of people with varying health histories use semaglutide for months or years, sometimes tells a different story. This is where the conversation gets interesting, and where understanding how semaglutide makes you feel day to day becomes relevant to the UTI question.
How semaglutide might indirectly increase UTI risk
If semaglutide does not directly cause UTIs, why are people reporting them? The answer lies in a chain of indirect mechanisms that, when you trace them carefully, create a plausible pathway from your weekly injection to a urinary tract infection.
The dehydration pathway
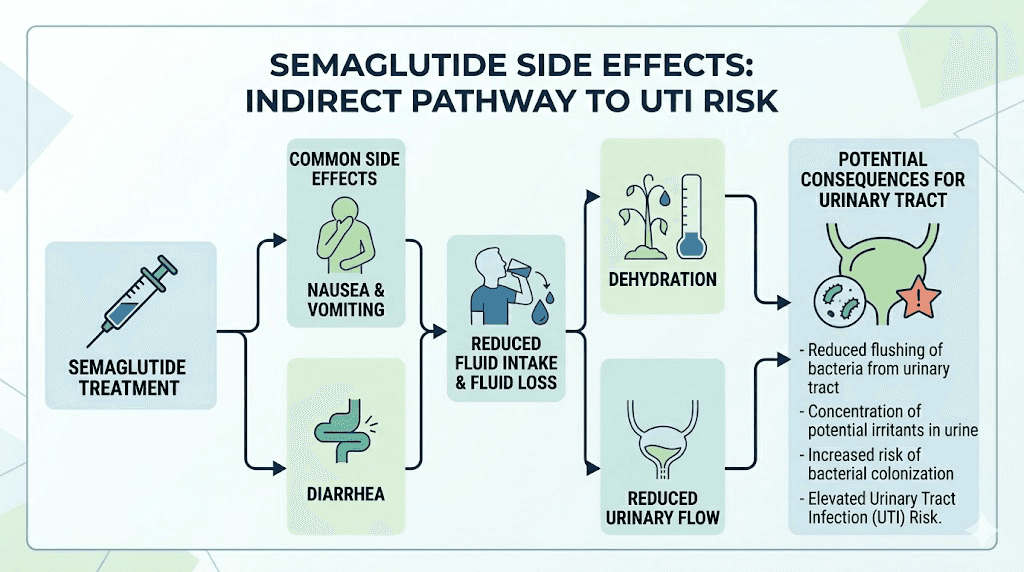
This is the big one. Semaglutide causes gastrointestinal side effects in a significant percentage of users. Clinical trial data shows nausea affects approximately 44% of users, diarrhea hits about 30%, and vomiting is common especially during dose escalation. Overall, around 73% of trial participants experienced some form of GI side effect.
Each of these side effects pulls water from your body. Vomiting and diarrhea cause direct fluid loss. Nausea reduces fluid intake because people simply do not feel like drinking when they feel sick. And here is something most guides miss entirely: GLP-1 medications can suppress your natural thirst cues, much like they reduce appetite. So your body needs more water than usual, but your brain is telling you that you need less.
Concentrated urine from dehydration creates an environment where bacteria thrive. Normally, adequate hydration flushes bacteria from the urinary tract before they can establish an infection. When urine becomes concentrated, that natural flushing mechanism weakens. Bacteria that would otherwise be washed away now have time to colonize, multiply, and cause infection. If you are managing semaglutide constipation, dehydration compounds both problems simultaneously.
This is not theoretical. It is well established in urology that dehydration is a modifiable risk factor for UTIs. The mechanism becomes especially concerning for semaglutide users who do not realize they need to dramatically increase their water intake to compensate for GI losses and suppressed thirst signals.
The constipation connection
Constipation is a recognized side effect of semaglutide and GLP-1 receptor agonists broadly. When stool remains in the colon for extended periods, it creates pressure on the bladder and can impair complete bladder emptying. Residual urine sitting in the bladder becomes a breeding ground for bacteria.
Additionally, the proximity of the rectum to the urethra (particularly in women) means that prolonged constipation increases the bacterial load near the urinary opening. E. coli, the bacterium responsible for roughly 80-90% of UTIs, originates in the intestinal tract. More time, more pressure, more bacterial migration. Managing your GLP-1 related constipation is not just about comfort. It is directly relevant to UTI prevention.
Appetite suppression and reduced fluid intake
People on semaglutide eat less. That is the point. But they often drink less too, and this gets overlooked. When you are eating smaller meals or skipping meals entirely, you lose the fluid that normally comes from food. Fruits, vegetables, soups, and other water-rich foods can contribute 20-30% of daily fluid intake. Cut your food consumption in half and you have just eliminated a significant water source without even realizing it.
Understanding what foods to eat on semaglutide includes choosing water-rich options that support both your nutritional needs and your hydration status. A proper semaglutide diet plan accounts for fluid intake as a core component, not an afterthought.
Blood sugar changes and immune function
For people using semaglutide to manage type 2 diabetes, the relationship between blood sugar and UTI risk is bidirectional. Poorly controlled diabetes impairs immune function and increases glucose in the urine, both of which promote bacterial growth. Semaglutide lowers blood sugar, which should theoretically reduce UTI risk over time.
But during the transition period, as blood sugar levels adjust, the immune system is adapting too. Some researchers hypothesize that the metabolic shifts during early treatment could temporarily affect immune surveillance in the urinary tract. This remains speculative, but it could explain why some users report UTIs specifically during the first few months of treatment, during the early weeks on semaglutide when the body is adjusting most dramatically.
It is important to note that semaglutide is fundamentally different from SGLT-2 inhibitors like empagliflozin or dapagliflozin, which work by increasing glucose excretion through urine. SGLT-2 inhibitors have a well-documented association with UTIs and genital infections because they literally create a sugar-rich environment in the urinary tract. Semaglutide does not do this. It works through GLP-1 receptor agonism, affecting insulin secretion and appetite signaling, not urinary glucose levels.
Who faces the highest UTI risk on semaglutide
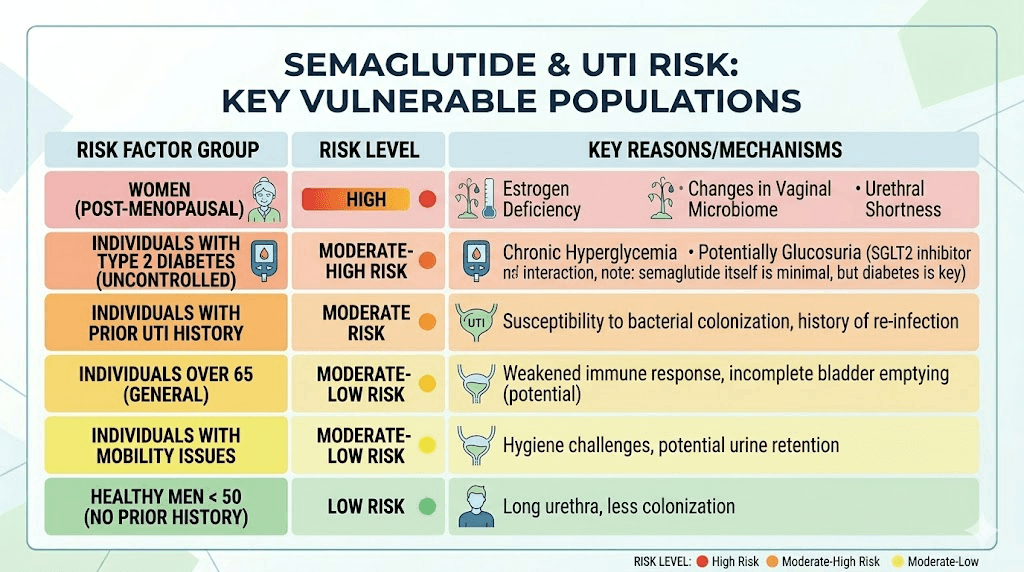
Not everyone on semaglutide faces equal risk. Several factors compound the indirect pathways described above, creating significantly higher vulnerability in certain populations.
Women
Approximately 50-60% of women experience at least one UTI during their lifetime, compared to roughly 12% of men. The shorter female urethra (about 4 cm versus 20 cm in men) provides less distance for bacteria to travel before reaching the bladder. Hormonal factors, especially declining estrogen during perimenopause and menopause, thin the urethral lining and reduce protective lactobacilli. Women taking semaglutide who are already in a higher risk demographic need to be especially vigilant about hydration and prevention strategies.
If you are also concerned about how semaglutide affects your period, understanding the hormonal context of your UTI risk becomes even more relevant. Hormonal fluctuations throughout your cycle can independently affect UTI susceptibility.
People with diabetes
Diabetes independently increases UTI risk through multiple mechanisms: impaired immune function, diabetic neuropathy affecting bladder sensation and emptying, and higher urinary glucose levels in poorly controlled disease. Adding semaglutide to this baseline risk creates a situation where any additional dehydration or constipation can tip the balance toward infection. The good news is that as semaglutide improves glycemic control over time, the diabetes-related UTI risk factors may actually decrease.
People experiencing severe GI side effects
If you are in the group dealing with significant nausea, vomiting, or diarrhea, your dehydration risk is substantially higher than someone with mild or no GI symptoms. This is especially true during the early period after starting semaglutide and during dose escalation phases. People who experience semaglutide bloating may also reduce their fluid intake simply because they feel uncomfortably full.
People with a history of recurrent UTIs
If you have had three or more UTIs in a year or two or more in six months, you already have underlying factors that predispose you to infection. These might include anatomical differences, immune deficiencies, or persistent bacterial colonization. Adding the dehydration and constipation effects of semaglutide to an already vulnerable system requires proactive prevention, not reactive treatment.
Older adults
Age-related changes in bladder function, immune response, and kidney function create higher baseline UTI risk. Older adults are also more susceptible to dehydration from GI side effects because they may have reduced kidney function and less physiological reserve. Understanding semaglutide fatigue is particularly important in this population, as fatigue can reduce motivation to maintain adequate fluid intake.
Semaglutide versus other GLP-1 medications: UTI risk comparison
How does semaglutide compare to other medications in the same class? This matters because if you are choosing between GLP-1 options, or considering switching from tirzepatide to semaglutide or vice versa, understanding the relative UTI risk profile helps inform that decision.
A network meta-analysis examining 105 randomized controlled trials with 219,283 participants found no significant association between GLP-1 receptor agonists as a class and increased infection risk, including UTIs. No significant associations were found between any individual GLP-1 receptor agonist and risk of sepsis, abscess, gangrene, or other serious infections.
The key distinction remains between GLP-1 receptor agonists and SGLT-2 inhibitors. While SGLT-2 inhibitors have documented associations with both UTIs and genital mycotic infections (yeast infections), GLP-1 drugs like semaglutide do not share this mechanism. If you have previously experienced UTIs on an SGLT-2 inhibitor and are now considering semaglutide, this is genuinely good news. The semaglutide versus tirzepatide comparison page offers more detail on how these GLP-1 options differ.
Medication Class | UTI Risk | Mechanism | Key Difference |
|---|---|---|---|
Semaglutide (GLP-1 RA) | No direct increase | Does not affect urinary glucose | Indirect risk through dehydration only |
Tirzepatide (dual GIP/GLP-1) | No direct increase | Does not affect urinary glucose | Similar indirect risk profile |
SGLT-2 inhibitors | Documented increase | Increases urinary glucose | Creates sugar-rich urinary environment |
Metformin | No significant increase | Works on hepatic glucose | Minimal urinary tract effects |
Insulin | No direct increase | Does not affect urinary composition | Hypoglycemia risk instead |
An interesting finding from a recent retrospective cohort study examined patients receiving botulinum toxin for overactive bladder. Those who were concurrently using GLP-1 receptor agonists had a 48% lower rate of UTIs (8.8% versus 13.3%) and a 74% lower rate of urinary retention compared to those not on GLP-1 therapy. While this was a specific clinical population and the findings are hypothesis-generating rather than definitive, it suggests GLP-1 drugs may actually have protective urinary effects in certain contexts.
Researchers exploring semaglutide versus tirzepatide side effects find broadly similar GI profiles between the two medications. If UTI risk from dehydration concerns you with one, switching to the other is unlikely to make a meaningful difference. Both require the same hydration vigilance.
Recognizing UTI symptoms while on semaglutide
One complication with identifying UTIs during semaglutide treatment is that some symptoms overlap with or get masked by semaglutide side effects. Knowing what to look for matters.
Classic UTI symptoms
A burning sensation during urination (dysuria) is the hallmark symptom. Increased frequency, where you feel the need to urinate much more often than usual but pass only small amounts each time. Urgency, the sudden intense need to urinate that feels difficult to delay. Cloudy, dark, or strong-smelling urine. Pelvic pressure or lower abdominal discomfort. Blood in the urine (hematuria) in some cases.
Symptoms that require immediate medical attention
Fever of 100.4 degrees Fahrenheit or higher. Chills or shaking. Flank pain, which is pain in the sides of your lower back below the ribs. Nausea and vomiting combined with urinary symptoms (this can indicate the infection has reached the kidneys). These suggest a possible kidney infection (pyelonephritis), which requires prompt treatment with antibiotics.
The overlap problem
Nausea and abdominal discomfort are common semaglutide side effects. If you develop a UTI while on semaglutide, you might dismiss urinary symptoms as just more medication side effects. This delay in recognition can allow a simple bladder infection to progress to a more serious kidney infection. The key differentiator is the urinary-specific symptoms: burning with urination, frequency, urgency, and changes in urine appearance or smell. These are not semaglutide side effects and should prompt evaluation.
If you are already managing semaglutide acid reflux or semaglutide dizziness, adding urinary symptoms to the mix can feel overwhelming. But distinguishing between expected side effects and new symptoms that require medical attention is critical for staying safe on your protocol.
Prevention strategies that actually work
Prevention is always better than treatment, and the good news is that the indirect UTI risk from semaglutide is almost entirely preventable with the right approach. These strategies are not generic wellness advice. They are specific to the unique challenges semaglutide users face.
Hydration protocol for semaglutide users
Forget the generic "drink 8 glasses of water" advice. Semaglutide users need a more structured approach.
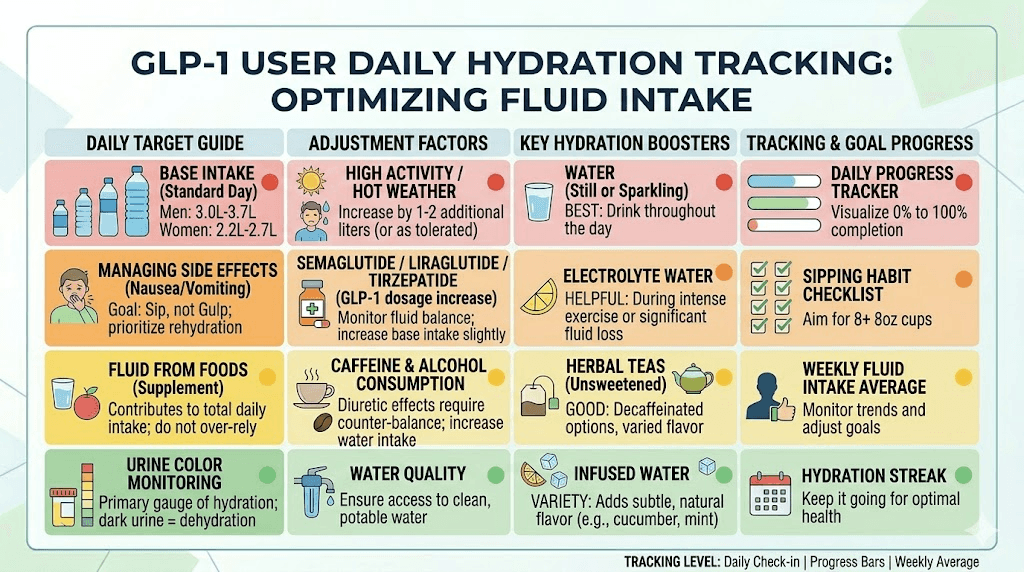
Baseline target: Start with half your body weight in ounces daily. A 180-pound person needs approximately 90 ounces (about 2.7 liters) as a baseline. But this is the minimum.
Adjustment for GI symptoms: Add 8-16 additional ounces for every episode of vomiting or significant diarrhea. If you are in a dose escalation phase with persistent nausea, increase your baseline by 20-30% even if you are not actively vomiting, because reduced food and fluid intake from nausea creates a slow dehydration that builds over days.
Electrolyte considerations: Plain water is not always enough. When you lose fluids through GI side effects, you also lose electrolytes. Adding a small amount of mineral-rich salt (like pink Himalayan or Redmond salt, about half a teaspoon) to water twice daily can help your body retain fluid more efficiently. This supports the recommendations in our supplements to take with GLP-1 medications guide.
Timing strategy: Sip water throughout the day rather than gulping large amounts at once. Large volumes can trigger nausea in semaglutide users. Set a timer if needed. Keep water visible and accessible at all times. Drink a full glass within 30 minutes of waking, before the day's distractions begin.
Hydration markers: Monitor your urine color. Pale yellow indicates adequate hydration. Dark yellow or amber signals dehydration and increased UTI risk. If your urine consistently looks concentrated, increase your intake immediately regardless of what your thirst cues are telling you.
Manage constipation proactively
Do not wait for constipation to become a problem. Start preventive measures from day one of your semaglutide protocol.
Fiber intake is foundational. Aim for 25-30 grams daily from food sources: vegetables, fruits, legumes, and whole grains. If your appetite suppression makes eating enough fiber-rich food difficult, a psyllium husk supplement can help. Our guide on the best foods to eat on semaglutide includes high-fiber options that work well even with reduced appetite.
Magnesium citrate or magnesium oxide at bedtime can support regular bowel movements. Start with 200-400 mg and adjust based on response. Physical activity, even walking for 20-30 minutes daily, stimulates intestinal motility. Do not ignore the urge to have a bowel movement, as delaying can worsen constipation over time.
Urination habits
Urinate when you feel the urge. Do not hold it. This is simple advice that many people ignore, especially at work or during activities. Holding urine allows bacteria more time to multiply in the bladder. Empty your bladder completely each time, taking an extra moment to ensure you have fully voided.
Urinate within 30 minutes after sexual activity. This is one of the most evidence-supported prevention strategies for sexually active individuals and it helps flush any bacteria that may have entered the urethra during intercourse.
Hygiene practices
Women should always wipe from front to back after using the bathroom. This prevents E. coli from the rectal area from reaching the urethra. Avoid douches, feminine sprays, and scented products in the genital area. These disrupt the normal protective flora and can actually increase infection risk. Wear cotton underwear and avoid tight-fitting clothing that traps moisture.
Dietary support
Cranberry products (juice or supplements) have mixed evidence for UTI prevention, but some studies suggest D-mannose, a naturally occurring sugar found in cranberries, may help prevent E. coli from adhering to the urinary tract lining. If you choose to try cranberry supplements, look for products standardized for proanthocyanidin content rather than drinking sugar-laden cranberry juice cocktail. Our best probiotic for semaglutide guide covers how maintaining healthy gut flora can support overall immune function, which has downstream effects on UTI resistance.
Probiotics containing Lactobacillus strains may support urinary tract health by maintaining the vaginal and periurethral microbiome. This is particularly relevant for women on semaglutide, as the medication's effects on the gut microbiome are still being studied.
What to do if you get a UTI while on semaglutide
First and most important: do not stop taking semaglutide without consulting your healthcare provider. A UTI does not mean semaglutide caused it, and stopping the medication abruptly can create its own set of problems. Understanding what happens when you stop semaglutide suddenly is important context for why a measured approach to any medication changes matters.
Immediate steps
Contact your healthcare provider for evaluation and treatment. UTIs typically require antibiotics, and the sooner treatment begins, the less likely the infection is to spread to the kidneys. While waiting for your appointment, dramatically increase your water intake. Aim for clear or very pale urine. This helps dilute bacteria and reduce symptoms.
Over-the-counter phenazopyridine (brand name AZO) can provide temporary relief from burning and urgency while you wait for antibiotics to take effect. Note that this medication turns urine bright orange, which is normal and expected. It treats symptoms only, not the infection itself.
Antibiotic considerations
Most uncomplicated UTIs respond well to short courses of antibiotics like trimethoprim-sulfamethoxazole (3 days), nitrofurantoin (5 days), or fosfomycin (single dose). There are no known significant drug interactions between semaglutide and common UTI antibiotics. However, always inform your prescriber about all medications you are taking, including semaglutide.
One practical consideration: antibiotics can worsen GI symptoms in some people, and if you are already dealing with semaglutide-related nausea or diarrhea, this overlap can be uncomfortable. Taking antibiotics with food (when appropriate for the specific antibiotic) and maintaining your hydration protocol can help minimize additional GI distress.
After the infection clears
Use the UTI as a signal to audit your prevention practices. Are you drinking enough water? Has constipation been an issue? Are you urinating frequently enough? Sometimes a UTI is the wake-up call that prompts better adherence to the prevention strategies that should have been in place from the start.
If you experience recurrent UTIs (two or more within six months), discuss with your provider whether prophylactic strategies like low-dose antibiotics or D-mannose supplementation make sense for your situation. Recurrent UTIs while on semaglutide warrant a more thorough urological evaluation to rule out other contributing factors.
Semaglutide, kidney health, and the bigger urinary picture
Understanding UTI risk in the context of semaglutide requires a broader look at how the medication affects the urinary system overall. The news is largely positive.
Kidney function effects
Data from the STEP 1, 2, and 3 trials showed that semaglutide had favorable effects on albuminuria (protein in the urine, a marker of kidney damage) and kidney function in people with overweight or obesity. Weight loss itself improves kidney function by reducing the metabolic burden on the kidneys, lowering blood pressure, and improving insulin sensitivity.
However, the FDA prescribing information includes a warning about acute kidney injury (AKI) in patients who experience severe gastrointestinal adverse reactions. The mechanism is straightforward: severe vomiting and diarrhea cause dehydration, which reduces blood flow to the kidneys. This is another reason why aggressive hydration during GI side effects is not just about preventing UTIs. It protects your kidneys too. If you are concerned about kidney health, our guide on semaglutide and kidney stones covers another important aspect of urinary health on this medication.
Weight loss and urinary health
There is a genuinely encouraging finding here. Research shows that a modest 10% weight loss can reduce urinary incontinence symptoms by up to 47% through decreased bladder pressure and improved urethral function. Since semaglutide typically produces weight loss in the 10-15% range, many users actually experience improved urinary health over time, even if they face some indirect risk during the initial adjustment period.
The weight loss benefits extend beyond incontinence. Reduced abdominal fat decreases pressure on the bladder and pelvic floor, potentially improving bladder emptying and reducing the residual urine volume that contributes to UTI risk. For people tracking their semaglutide results week by week, improved urinary symptoms may be one of the less celebrated but genuinely meaningful outcomes.
Yeast infections versus UTIs
Some people confuse UTIs with yeast infections, and it is worth clarifying the difference. If you are experiencing vaginal itching, thick white discharge, or external irritation rather than burning urination and frequency, you may have a yeast infection rather than a UTI. Our guide on why semaglutide can cause yeast infections explains the different mechanism involved. The treatment approaches are completely different, so getting the right diagnosis matters.
Managing side effects that contribute to UTI risk
Since the primary pathway from semaglutide to UTIs runs through GI side effects and dehydration, managing those side effects effectively is itself a UTI prevention strategy.
Nausea management
Eat smaller, more frequent meals. Avoid greasy, spicy, or heavily seasoned foods, especially during dose escalation. Ginger tea or ginger supplements may provide mild antiemetic effects. Some people find that sipping cold liquids is easier to tolerate than room temperature water when nauseous. Peppermint tea can also help. The foods to avoid on semaglutide guide covers triggers in more detail.
Diarrhea management
Diarrhea is a significant fluid-loss event that directly increases dehydration and UTI risk. Use oral rehydration solutions (not just plain water) to replace both fluids and electrolytes. Avoid caffeine and alcohol, which have diuretic effects and can worsen dehydration. The BRAT diet (bananas, rice, applesauce, toast) can help firm stools during acute episodes. If diarrhea persists for more than a few days, contact your healthcare provider.
Timing your dose to minimize side effects
Some people find that taking their semaglutide injection at a specific time reduces GI side effects. Our guides on the best time of day to take semaglutide and general injection technique can help you optimize your protocol. Some users report fewer GI issues when injecting in the evening so they sleep through the worst of any nausea. Others prefer morning injections. Experiment to find what works for your body.
Dose escalation and patience
GI side effects are typically worst during the first few weeks and during dose increases. Following the prescribed titration schedule (starting low and increasing gradually) minimizes these effects and, by extension, minimizes the dehydration that drives UTI risk. If your GI symptoms are severe enough that you cannot maintain adequate hydration despite your best efforts, talk to your prescriber about slowing the escalation.
Understanding how quickly semaglutide works helps set realistic expectations. The medication builds in your system over weeks, and pushing too fast on dose escalation in hopes of faster results often backfires with more severe side effects.
Special considerations for different semaglutide formulations
Semaglutide comes in several forms, and the UTI risk profile may differ slightly between them based on their side effect profiles.
Injectable semaglutide (Ozempic, Wegovy)
The injectable forms deliver semaglutide directly into the bloodstream via subcutaneous injection. GI side effects are common but generally manageable with proper dose titration. The best injection site for semaglutide can affect absorption and potentially influence the severity of side effects. Proper reconstitution technique matters for compounded versions to ensure accurate dosing, which directly impacts side effect severity and by extension dehydration risk.
Oral semaglutide (Rybelsus)
Oral semaglutide has a different absorption profile and may produce somewhat different GI side effect patterns. It must be taken on an empty stomach with minimal water (no more than 4 ounces), which creates a unique hydration challenge. If you are on oral semaglutide, you need to be especially intentional about catching up on hydration after the required fasting period. The sublingual semaglutide guide covers alternative oral delivery methods and their considerations.
Compounded semaglutide
Users of compounded semaglutide should apply all the same UTI prevention strategies. Compounded versions may have different excipients or concentrations, but the active ingredient works through the same mechanisms. Ensuring proper dosage accuracy with compounded preparations is especially important for managing side effects predictably. Use the semaglutide dosage calculator to verify your doses.
The role of other medications and supplements
Many semaglutide users take other medications or supplements concurrently, and some of these can independently affect UTI risk.
Metformin
Metformin is commonly prescribed alongside semaglutide for type 2 diabetes. While metformin itself does not significantly increase UTI risk, it can cause GI side effects (especially diarrhea) that compound the dehydration problem. If you are on both medications, your hydration needs are even higher. Our guide on combining metformin with GLP-1 medications discusses managing overlapping side effects.
Supplements that may help
Vitamin C can acidify urine, creating a less hospitable environment for bacteria. D-mannose supplementation (500-2000 mg daily) has shown promise in preventing recurrent UTIs by interfering with E. coli adhesion to the urinary tract lining. B12 supplementation is commonly recommended for semaglutide users for other reasons, but it does not directly affect UTI risk.
Probiotics, particularly strains of Lactobacillus, may support both gut health (improving GI side effects) and vaginal/urinary flora (reducing UTI risk). This dual benefit makes them worth considering for semaglutide users, especially women. Choosing the right supplements to support your GLP-1 protocol can address multiple concerns simultaneously.
Alcohol
Alcohol is a diuretic that worsens dehydration. Combining alcohol with semaglutide, which already creates dehydration risk through GI side effects and suppressed thirst, significantly increases the concentration of urine and UTI vulnerability. If you choose to drink, our guide on drinking on semaglutide covers harm reduction strategies. Match every alcoholic drink with at least one full glass of water.
Long-term outlook: does UTI risk change over time on semaglutide
The trajectory of UTI risk while on semaglutide likely follows a pattern that mirrors the side effect timeline.
Weeks 1-8 (highest risk period): GI side effects are at their peak during initial dose escalation. Dehydration risk is highest. Your body is adjusting to the medication. This is when most semaglutide-associated UTI reports seem to cluster.
Months 2-4 (decreasing risk): Most people develop tolerance to GI side effects. Fluid intake habits stabilize. Constipation management strategies are in place. The initial adjustment period ends.
Months 4+ (potentially protective): Weight loss is progressing, which reduces bladder pressure and improves urinary function. Blood sugar control has improved (for diabetic users), reducing a key UTI risk factor. GI side effects have largely resolved. The net effect may actually be a lower UTI risk than before starting semaglutide, particularly for people who have lost significant weight.
This is encouraging news for anyone who is planning their long-term semaglutide protocol. The highest risk period is finite and manageable with proper prevention, while the long-term benefits for urinary health are genuine.
When to talk to your doctor
Schedule a conversation with your healthcare provider if you experience any of the following while on semaglutide.
Any UTI symptoms (burning, frequency, urgency, cloudy urine). Do not try to self-treat and do not assume it will resolve on its own. UTIs require antibiotics.
Recurrent UTIs (two or more within six months). This pattern warrants investigation beyond simple treatment of individual episodes.
Severe GI side effects that prevent you from maintaining adequate hydration despite your best efforts. Your provider may adjust your dose or prescribe antiemetic medication.
Signs of kidney infection (fever, chills, flank pain, nausea with urinary symptoms). This is a medical urgency that requires same-day evaluation.
Blood in your urine, even without other symptoms. While this can occur with UTIs, it can also indicate other conditions that need evaluation.
If your provider is not familiar with the indirect connections between GLP-1 therapy and urinary health, sharing the research discussed in this article can facilitate a more informed conversation. SeekPeptides members have access to detailed guides on managing every aspect of their GLP-1 protocols, including the side effect management strategies that make the difference between a smooth experience and a difficult one.
Frequently asked questions
Does semaglutide directly cause urinary tract infections?
No. Clinical trials including the SUSTAIN and STEP programs did not identify UTIs as a significant adverse event associated with semaglutide. The FDA prescribing information for Ozempic, Wegovy, and Rybelsus does not list UTIs among common side effects. However, semaglutide can indirectly increase UTI risk through dehydration from GI side effects like nausea, vomiting, and diarrhea.
Should I stop semaglutide if I get a UTI?
No. Do not stop semaglutide without consulting your healthcare provider. A UTI can be treated with antibiotics while continuing your semaglutide protocol. There are no significant drug interactions between semaglutide and common UTI antibiotics. Stopping semaglutide abruptly can cause withdrawal-like effects and weight regain.
How much water should I drink on semaglutide to prevent UTIs?
Start with half your body weight in ounces as a daily baseline. Add 8-16 ounces for every episode of vomiting or diarrhea. During dose escalation when GI side effects peak, increase your baseline by 20-30%. Monitor urine color. Pale yellow indicates adequate hydration. Dark yellow means you need to drink more immediately.
Is the UTI risk different between injectable and oral semaglutide?
The indirect UTI risk mechanism (dehydration from GI side effects) applies to both forms. However, oral semaglutide requires fasting with minimal water for absorption, creating a brief period where hydration is restricted. Be intentional about catching up on fluid intake after the fasting window.
Are UTIs more common during dose escalation?
Anecdotal reports suggest UTI risk is highest during the initial weeks and during dose increases, which aligns with when GI side effects (and therefore dehydration risk) are most pronounced. Following the prescribed titration schedule and maintaining aggressive hydration during these periods provides the best protection.
Can semaglutide help with urinary incontinence?
Yes, indirectly. Research shows that 10% weight loss can reduce urinary incontinence symptoms by up to 47%. Since semaglutide typically produces 10-15% weight loss, many users experience significant improvement in urinary symptoms over time. One study even found that GLP-1 receptor agonist users had lower rates of urinary retention and UTIs in certain clinical settings.
Is semaglutide safer than SGLT-2 inhibitors for UTI-prone people?
Yes. SGLT-2 inhibitors (like empagliflozin and dapagliflozin) increase urinary glucose levels, creating conditions that promote bacterial growth and have documented associations with UTIs and genital infections. Semaglutide does not affect urinary glucose and has a fundamentally different mechanism. If you have a history of UTIs, this distinction is clinically significant.
Do probiotics help prevent UTIs while on semaglutide?
Probiotics containing Lactobacillus strains may support urinary tract health by maintaining protective flora. They also support gut health, potentially reducing the GI side effects that drive dehydration. While evidence is not definitive for UTI prevention specifically, the dual benefit makes them a reasonable addition for semaglutide users. See our best probiotic for semaglutide guide for specific strain recommendations.
External resources
Diabetes Care: Semaglutide Effects on Kidney Function (STEP Trials)
Journal of Urology: Semaglutide and Urinary Tract Implications
For researchers serious about optimizing their GLP-1 protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. From practical semaglutide tips to detailed dosage calculators, the tools and guidance you need are all in one place.
In case I do not see you, good afternoon, good evening, and good night. May your hydration stay consistent, your urinary tract stay clear, and your semaglutide protocol stay on track.