Mar 3, 2026

Nausea kills more semaglutide protocols than anything else. Not the cost. Not the injections. Not the waiting. The relentless, rolling waves of nausea that hit during dose escalation drive roughly 10-17% of users to abandon treatment entirely, according to data from the STEP clinical trials. And for the people who push through, the discomfort often leads to skipped doses, slower titration schedules, and ultimately, diminished results.
That is the problem pyridoxine aims to solve.
Pyridoxine, the active form of vitamin B6, has decades of clinical evidence supporting its anti-nausea properties. Obstetricians have prescribed it for morning sickness since the 1940s, and the American College of Obstetricians and Gynecologists still recommends it as a first-line treatment for pregnancy-related nausea. When compounding pharmacies began adding pyridoxine to compounded semaglutide formulations, the logic was straightforward. If B6 can calm the nausea centers in the brainstem during pregnancy, it might do the same for the gastrointestinal distress triggered by GLP-1 receptor agonists. The early reports from providers and patients suggest this reasoning holds up in practice, with many users reporting smoother dose escalation and better day-to-day tolerance when pyridoxine is included in their compound.
This guide breaks down exactly how pyridoxine works alongside semaglutide, what the research actually supports, how the dosing works, and whether this formulation makes sense for your situation. Whether you are just starting semaglutide and dreading the nausea, or you have already tried the standard formulation and struggled with side effects, the information here will help you have a more informed conversation with your healthcare provider about your options.
What is pyridoxine and why is it added to semaglutide
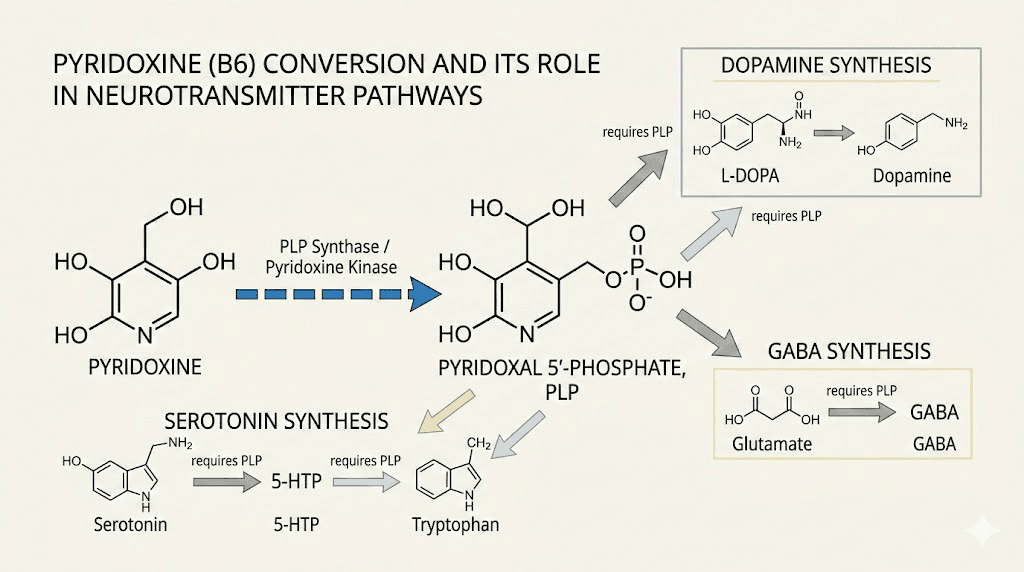
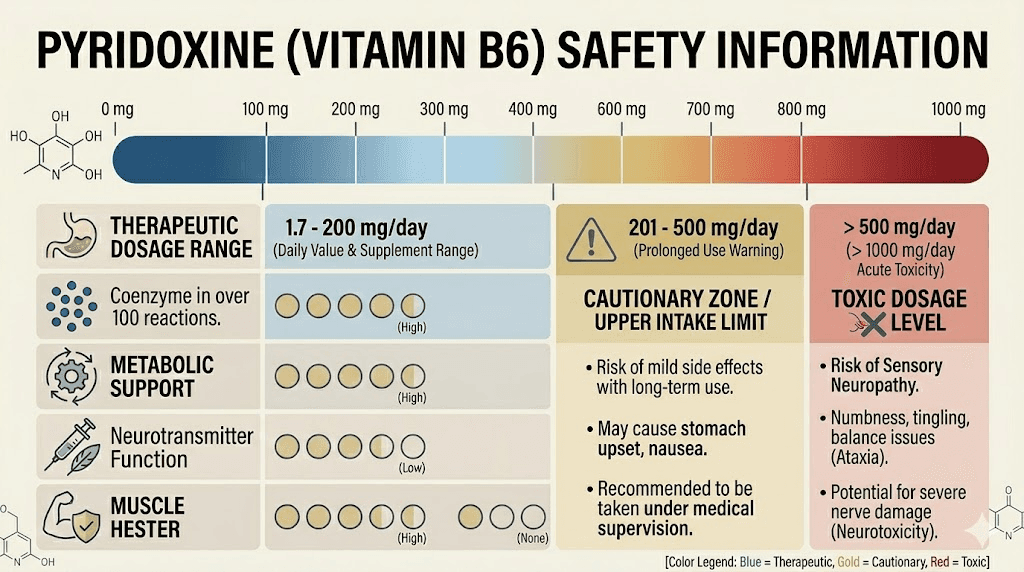
Pyridoxine is one of six chemical forms of vitamin B6, a water-soluble nutrient the body cannot produce on its own. It serves as a coenzyme in over 100 enzymatic reactions, most of them involving amino acid metabolism, neurotransmitter synthesis, and glycogen breakdown. The body converts pyridoxine into its active form, pyridoxal 5-phosphate (PLP), which then participates in the production of serotonin, dopamine, GABA, and norepinephrine. These neurotransmitters regulate everything from mood and sleep to appetite and, critically, the nausea response.
When compounding pharmacies add pyridoxine to semaglutide injections, the primary goal is nausea management. But the benefits extend beyond that single symptom.
Vitamin B6 supports protein metabolism at a time when preserving lean muscle mass matters most. People on semaglutide weight loss protocols often eat significantly less protein than they need, and B6 helps the body process whatever protein it does receive more efficiently. It also supports immune function, red blood cell formation, and the conversion of stored glycogen into usable glucose for energy, which becomes especially relevant during the caloric deficit that semaglutide naturally creates.
The typical pyridoxine dose in compounded semaglutide formulations ranges from 5 to 10 milligrams per injection. This is well within the safe therapeutic range and far below the 100-milligram daily ceiling that most clinical guidelines recommend as a long-term maximum.
How semaglutide causes nausea in the first place
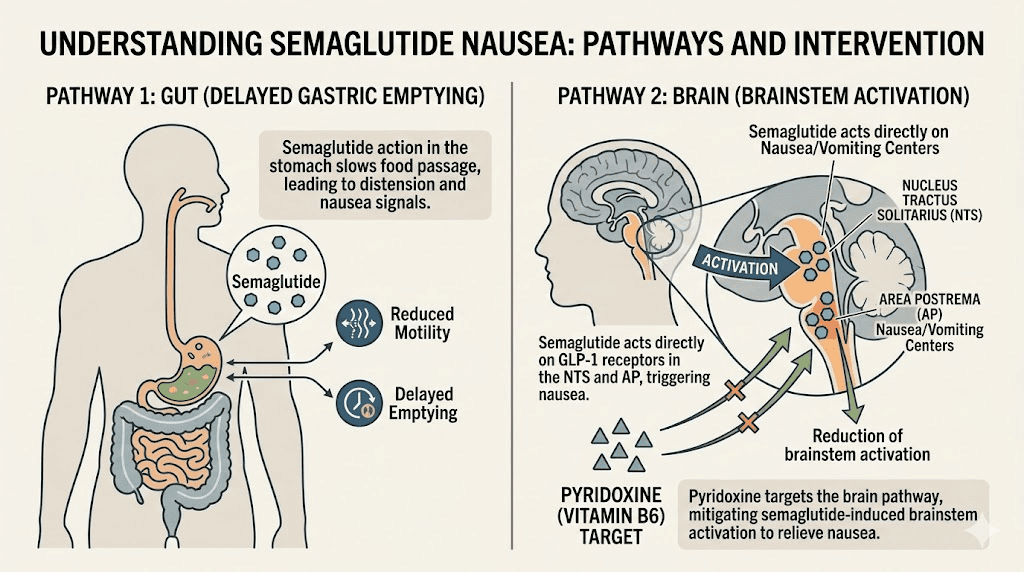
Understanding why semaglutide makes people nauseous requires looking at two separate mechanisms working simultaneously. The first involves the gut. The second involves the brain. Together, they create the characteristic GI distress that plagues so many users during the first weeks and months of treatment.
The gastric emptying effect
Semaglutide is a GLP-1 receptor agonist, meaning it mimics the incretin hormone GLP-1 that the body naturally produces after eating. If you are wondering whether GLP-1 and Ozempic are the same thing, the short answer is that Ozempic is one brand name for semaglutide. One of GLP-1 primary effects is slowing gastric emptying, the rate at which food moves from the stomach into the small intestine. This delay is actually part of how the medication works for weight loss. Food sits in the stomach longer, which signals fullness to the brain, reduces appetite, and lowers caloric intake.
But when gastric emptying slows too much, especially during the early dose escalation phase, the stomach essentially holds food longer than the body expects. This creates a sensation of persistent fullness, bloating, and nausea. Some users describe feeling like they ate a massive meal when they only had a few bites. The sensation can persist for hours or even the entire day following an injection.
Research from the STEP 1 trial showed that nausea affected 44.2% of participants on the 2.4 mg maintenance dose, compared to 17.4% on placebo. Most episodes were mild to moderate, and the median duration of individual nausea episodes was approximately 8 days. But for the people experiencing them, those days feel endless.
The brainstem pathway
The second mechanism is central. GLP-1 receptors exist throughout the brainstem, including in the area postrema and the nucleus tractus solitarius, two regions that form part of the vomiting reflex circuit. When semaglutide activates these receptors, it can directly trigger nausea signals independent of what is happening in the stomach. This central nausea is why some people feel nauseous even on an empty stomach, or why bloating and nausea can persist even when dietary adjustments successfully manage the gastric emptying component.
This dual mechanism, peripheral and central, is exactly why pyridoxine is such a logical addition to the formulation. Vitamin B6 works primarily through the central pathway, targeting the brainstem nausea centers through neurotransmitter modulation. It addresses the piece of the puzzle that dietary changes alone cannot fix.
How pyridoxine fights GLP-1 induced nausea
Pyridoxine does not simply mask nausea. It intervenes at the neurochemical level, modulating the same pathways that semaglutide inadvertently activates when it triggers the nausea response.
Neurotransmitter regulation
The nausea response depends heavily on serotonin signaling. The area postrema, the brainstem region most responsible for drug-induced nausea, is packed with serotonin receptors. When semaglutide activates GLP-1 receptors in this region, it can dysregulate local serotonin signaling and trigger the emetic reflex. Pyridoxine helps by supporting balanced serotonin synthesis. As a cofactor for the enzyme aromatic L-amino acid decarboxylase, pyridoxine is directly involved in converting 5-hydroxytryptophan to serotonin. Adequate B6 levels help maintain steady serotonin production rather than the surges and dips that contribute to nausea.
The same applies to GABA, the primary inhibitory neurotransmitter. GABA has a dampening effect on the vomiting center. Pyridoxine serves as a cofactor for glutamic acid decarboxylase, the enzyme that converts glutamate to GABA. Higher GABA activity in the brainstem can reduce the sensitivity of the area postrema to nausea triggers, effectively raising the threshold for how much GLP-1 stimulation is needed before nausea occurs.
This is not theoretical. It is the same mechanism that makes pyridoxine effective for pregnancy nausea, chemotherapy-induced nausea, and motion sickness. The brainstem pathways involved are remarkably similar regardless of the nausea source.
The pregnancy nausea evidence
The strongest evidence for pyridoxine anti-nausea effects comes from obstetric research. The American College of Obstetricians and Gynecologists recommends vitamin B6 at doses of 10-25 mg three times daily as a first-line treatment for nausea and vomiting during pregnancy. Multiple randomized controlled trials have demonstrated its effectiveness.
A landmark study published in Obstetrics & Gynecology found that women taking 25 mg of pyridoxine every 8 hours experienced a significant reduction in nausea severity compared to placebo. The improvement was most pronounced in cases of moderate nausea, which aligns closely with the type of nausea most semaglutide users experience.
The FDA-approved combination of pyridoxine and doxylamine (marketed as Diclegis) remains one of only a few medications specifically approved for pregnancy nausea, with pyridoxine as the cornerstone ingredient. While the specific mechanism may differ slightly between pregnancy-related and GLP-1-related nausea, the brainstem pathways targeted are substantially similar, which provides a reasonable pharmacological basis for using B6 alongside semaglutide.
Semaglutide with pyridoxine dosage and formulation details
The dosing of semaglutide in compound formulations follows the same escalation schedule as brand-name versions. What changes is the addition of pyridoxine and the specific concentrations used by different compounding pharmacies.
Typical semaglutide escalation with pyridoxine
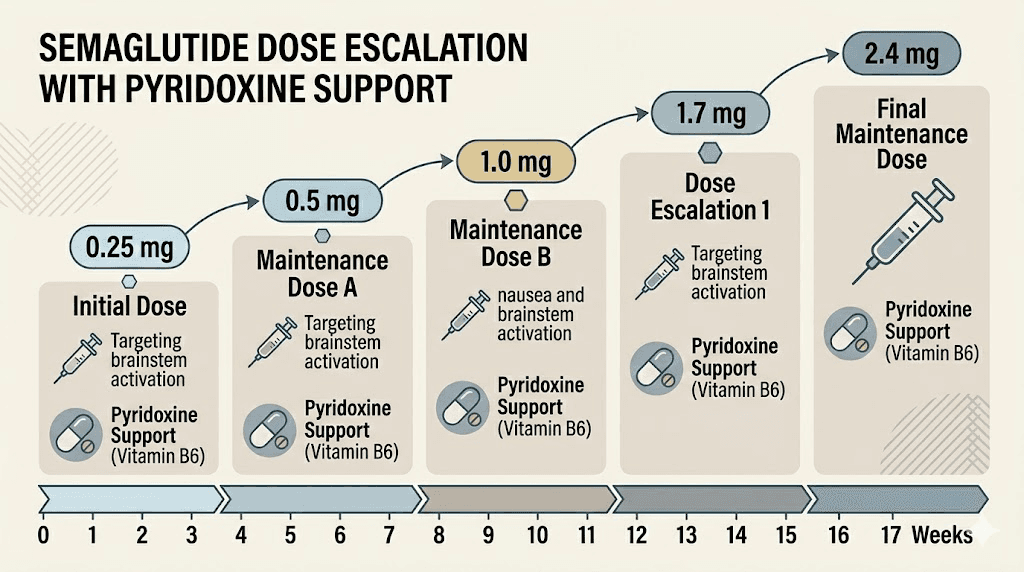
Most providers follow a standard titration schedule when prescribing semaglutide with pyridoxine. The semaglutide dose increases gradually while the pyridoxine dose typically stays constant throughout treatment.
Weeks 1-4: 0.25 mg semaglutide + 5-10 mg pyridoxine, injected subcutaneously once weekly
Weeks 5-8: 0.5 mg semaglutide + 5-10 mg pyridoxine, injected subcutaneously once weekly
Weeks 9-12: 1.0 mg semaglutide + 5-10 mg pyridoxine, injected subcutaneously once weekly
Weeks 13-16: 1.7 mg semaglutide + 5-10 mg pyridoxine, injected subcutaneously once weekly
Week 17 and beyond: 2.4 mg semaglutide + 5-10 mg pyridoxine, injected subcutaneously once weekly
Some providers modify this schedule based on individual tolerance. If a patient handles the first four weeks without any nausea, the provider may accelerate the escalation. If nausea is significant even with pyridoxine, the escalation may slow, holding at each dose for six or eight weeks instead of four.
Concentration and vial information
Compounding pharmacies typically provide semaglutide with pyridoxine in multi-dose vials. A common formulation is 5 mg/mL semaglutide combined with pyridoxine, though concentrations vary between pharmacies. The injectable solution should be clear and colorless. Any cloudiness, discoloration, or particulate matter indicates a problem with the compound and it should not be used.
To calculate your specific injection volume, you can use the SeekPeptides semaglutide dosage calculator. If your vial concentration is 5 mg/mL, then 0.25 mg equals 5 units on a standard insulin syringe, 0.5 mg equals 10 units, 1.0 mg equals 20 units, and so on. These conversions become second nature after the first few injections, but getting them right from the start prevents dosing errors that can cause unnecessary side effects.
Injection technique for the compound
The injection technique for semaglutide with pyridoxine is identical to standard semaglutide injections. Administer subcutaneously in the abdomen, upper arm, or thigh. Rotate injection sites with each dose to prevent lipodystrophy. The most popular injection sites are the abdomen (two inches away from the navel) and the upper outer thigh.
Clean the injection site with an alcohol swab, pinch the skin, insert the needle at a 45-90 degree angle depending on body composition, inject slowly, hold for 5-10 seconds, and withdraw. If you are new to self-injection, our step-by-step semaglutide injection guide walks through every detail including needle selection and proper disposal. You can also review our broader guide on how to inject GLP-1 medications and learn about the best GLP-1 injection sites for weight loss.
What to expect when starting semaglutide with pyridoxine
The first week sets the tone for the entire treatment course. Knowing what to expect helps you distinguish normal adjustment effects from genuine problems that need medical attention.
Week 1: the adjustment period
At 0.25 mg, semaglutide is at its lowest therapeutic dose. Many people feel very little during the first week on semaglutide. The pyridoxine component may further reduce whatever mild GI symptoms would otherwise occur. You might notice a slight decrease in appetite, particularly in the 24-48 hours following your injection. Some people report feeling "less interested" in food rather than actively nauseous. The timeline for semaglutide appetite suppression varies, but most people notice changes within the first few days.
Weight loss during week one is typically 0-2 pounds. Do not be discouraged. This is a sub-therapeutic dose designed to let your body adjust. The real work begins at higher doses. If you want a detailed breakdown of what the initial period looks like, our guide on when you start losing weight on semaglutide covers the realistic timeline.
Weeks 2-4: building tolerance
By the end of the first month, most people on the 0.25 mg dose have established a baseline tolerance. The appetite suppression effects become more consistent. You may find yourself leaving food on your plate without thinking about it, skipping snacks that used to feel automatic, or simply forgetting to eat at your usual times.
The pyridoxine advantage becomes most apparent during the first dose increase, from 0.25 mg to 0.5 mg. This is traditionally the point where nausea spikes for many users on standard semaglutide. Users on the pyridoxine compound often report a smoother transition, with milder and shorter-duration nausea episodes.
Weeks 5-8: dose escalation begins
At 0.5 mg, the weight loss effects of semaglutide start to become noticeable. Average weight loss by week 8 is approximately 3-5% of starting body weight, though individual results vary widely. The appetite suppression is now consistent enough that most people naturally reduce their caloric intake by 20-40% without consciously dieting.
Nausea at this dose, for those on the pyridoxine formulation, tends to be mild and episodic rather than constant. You might feel slightly nauseous for a few hours after eating a larger meal, or experience brief waves of queasiness in the first 24 hours after injection day. These episodes typically resolve within a day or two and become less frequent as your body adjusts.
Weeks 9-16: reaching therapeutic doses
The jump from 0.5 mg to 1.0 mg is the largest percentage increase in the titration schedule, doubling the dose. This is another critical point where pyridoxine provides the most benefit. The 1.0 mg to 1.7 mg and 1.7 mg to 2.4 mg transitions are smaller relative increases, but cumulative GI adaptation means they usually feel less dramatic than earlier escalations.
By week 12-16, most users on the pyridoxine compound have settled into a manageable routine. The nausea that does occur is predictable, usually tied to overeating, high-fat meals, or the first 24 hours post-injection. Knowing your triggers and managing them with proper food choices makes a significant difference at this stage.
Week 17 and beyond: maintenance
At the 2.4 mg maintenance dose, weight loss continues steadily. The STEP 1 trial showed an average weight loss of 14.9% of body weight at 68 weeks. The pyridoxine formulation does not change the weight loss outcomes; it simply makes the journey there more tolerable. By this point, most GI side effects have either resolved or become manageable with dietary modifications. For a complete visual reference of how semaglutide doses translate across different vial concentrations, see our semaglutide 5mg/mL dosage chart and units-to-mg conversion guide.
Pyridoxine compared to other semaglutide compound additives
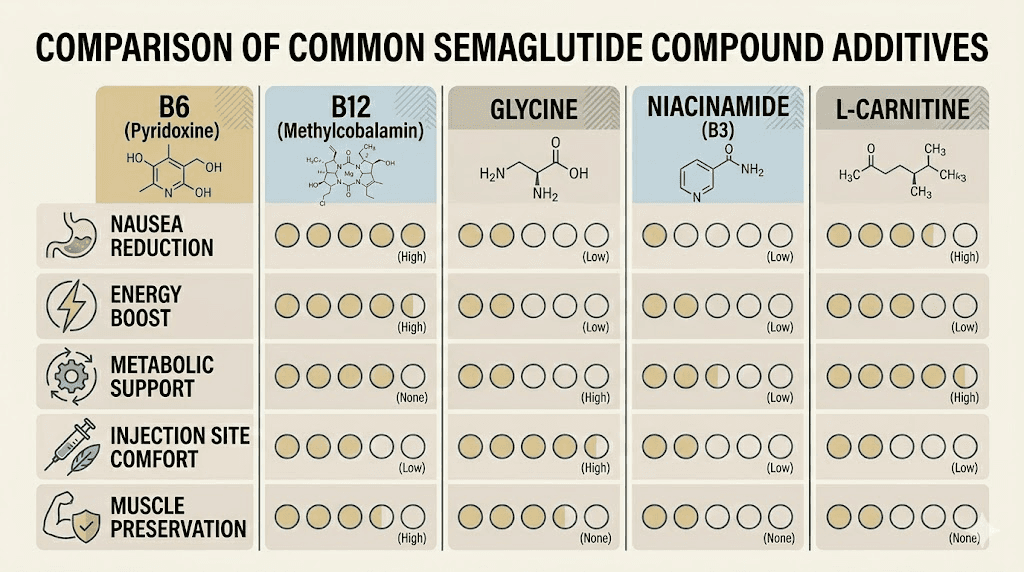
Pyridoxine is not the only additive used in compounded semaglutide. Several vitamins, amino acids, and cofactors are commonly paired with semaglutide to address different aspects of GLP-1 therapy. Understanding the differences helps you choose the formulation that best matches your needs.
Pyridoxine (B6) vs cyanocobalamin (B12)
Semaglutide with B12 is probably the most widely available compound formulation. Cyanocobalamin (vitamin B12) supports energy production, red blood cell formation, and neurological function. Its primary benefit in the semaglutide context is combating the fatigue and low energy that many users experience during significant caloric restriction.
The key difference: B12 does not have anti-nausea properties. If your primary concern is nausea during dose escalation, pyridoxine is the more targeted choice. If your primary concern is fatigue and low energy, B12 makes more sense. Some providers prescribe formulations containing both, addressing multiple side effects simultaneously.
Pyridoxine vs glycine
Semaglutide with glycine takes a different approach. Glycine is an amino acid that supports collagen synthesis, connective tissue health, and sleep quality. It also acts as an inhibitory neurotransmitter in the central nervous system, which can have mild calming effects. For semaglutide users concerned about muscle preservation and joint health during rapid weight loss, glycine offers benefits that pyridoxine does not. But glycine lacks the specific anti-nausea evidence that pyridoxine carries.
Pyridoxine vs methylcobalamin
Semaglutide with methylcobalamin uses the active, methylated form of vitamin B12 rather than cyanocobalamin. Methylcobalamin is bioavailable immediately, requiring no liver conversion. It supports nerve health, cognitive function, and methylation pathways. Like cyanocobalamin, it addresses fatigue rather than nausea, but it may be better absorbed and utilized than the synthetic form.
Pyridoxine vs niacinamide
Semaglutide with niacinamide (vitamin B3) targets a different set of concerns entirely. Niacinamide supports cellular energy metabolism, skin health, and insulin sensitivity. It can complement semaglutide effects on blood sugar regulation, which makes it appealing for users with insulin resistance or type 2 diabetes. However, niacinamide has no significant anti-nausea properties.
Pyridoxine vs L-carnitine
Semaglutide with L-carnitine focuses on fat metabolism. L-carnitine transports fatty acids into mitochondria for energy production, theoretically enhancing the fat-burning effects of caloric restriction during semaglutide therapy. Users who prioritize maximizing fat loss efficiency may prefer this formulation. Again, L-carnitine does not address nausea.
The triple blend: semaglutide, glycine, and B12
The semaglutide glycine B12 blend combines multiple additives to address fatigue, muscle preservation, and energy simultaneously. This is one of the most popular multi-additive formulations. If your provider offers it but you are primarily concerned about nausea, asking about adding or substituting pyridoxine may be worthwhile.
Quick comparison table
Additive | Primary benefit | Anti-nausea | Energy support | Muscle preservation | Best for |
|---|---|---|---|---|---|
Pyridoxine (B6) | Nausea reduction | Strong | Moderate | Moderate | Users who struggle with nausea |
Cyanocobalamin (B12) | Energy and nerve health | None | Strong | Low | Users with fatigue |
Methylcobalamin | Active B12, nerve health | None | Strong | Low | Users wanting bioavailable B12 |
Glycine | Muscle and joint support | Mild | Low | Strong | Users concerned about muscle loss |
Niacinamide (B3) | Metabolic and skin health | None | Moderate | Low | Users with insulin resistance |
L-Carnitine | Fat metabolism | None | Moderate | Moderate | Users maximizing fat loss |
Who benefits most from semaglutide with pyridoxine
Not everyone needs pyridoxine in their semaglutide compound. Some people tolerate standard semaglutide with minimal nausea. Others breeze through dose escalation without any GI issues at all. The pyridoxine formulation makes the most sense for specific populations.
People with a history of medication-related nausea
If you have experienced nausea with other medications in the past, whether antibiotics, pain medications, birth control, or supplements, your brainstem nausea centers may be more reactive than average. This heightened sensitivity predicts a higher likelihood of semaglutide-related nausea, and it also predicts a stronger response to pyridoxine anti-nausea effects.
People who have tried semaglutide before and quit due to nausea
This is the most obvious candidate group. If you started semaglutide or a brand-name equivalent and discontinued because the nausea was intolerable, the pyridoxine compound offers a legitimate reason to try again. The mechanism of action has not changed, only the addition of a nausea-dampening cofactor that may make the critical early weeks and dose escalation phases manageable.
Some people in this situation also benefit from a slower titration schedule combined with the pyridoxine formulation. Instead of increasing every four weeks, extending each dose level to six or eight weeks allows the body more time to adapt while the pyridoxine handles the acute nausea component. Talk to your provider about whether a modified schedule makes sense. You can learn more about alternative dosing approaches in our guide to split semaglutide dosing. Understanding how long semaglutide takes to work at each dose level helps set appropriate expectations for the slower schedule.
People prone to motion sickness
Motion sickness susceptibility correlates with increased sensitivity to all forms of nausea, including drug-induced nausea. The vestibular system and the brainstem nausea centers share overlapping neural pathways. People who get carsick, seasick, or nauseous on amusement rides typically have a lower threshold for GLP-1-induced nausea as well. Pyridoxine targets the central pathway that both motion sickness and semaglutide nausea share.
People with vitamin B6 deficiency
B6 deficiency is more common than most people realize. Groups at higher risk include older adults, people with kidney disease, people with autoimmune conditions, heavy alcohol consumers, and people taking certain medications that deplete B6 stores (including some oral contraceptives and isoniazid). A B6-deficient person starting semaglutide faces a double problem: their neurotransmitter synthesis is already compromised, and semaglutide further disrupts the GI and central nervous system pathways that depend on adequate B6 levels. For these individuals, the pyridoxine compound addresses both the deficiency and the medication side effects simultaneously.
People who want to escalate doses faster
Some providers and patients prefer an accelerated titration schedule to reach the therapeutic dose sooner. The logic is simple: faster escalation means less time at sub-therapeutic doses and earlier onset of meaningful weight loss. The risk is increased nausea during the rapid increases. Pyridoxine can serve as a buffer, allowing faster dose escalation while keeping nausea within tolerable limits. This approach requires close communication with your provider and is not appropriate for everyone.
Side effects and safety considerations
Pyridoxine is generally safe when dosed appropriately, but it is not without risks. Understanding the safety profile helps you and your provider make informed decisions about the compound.
Pyridoxine toxicity: the dose matters
The most significant risk associated with pyridoxine is peripheral neuropathy at high doses. Chronic intake above 200 mg daily has been associated with sensory neuropathy, characterized by numbness, tingling, and loss of sensation in the hands and feet. The risk increases with both dose and duration.
At the 5-10 mg per injection used in compounded semaglutide, the risk of toxicity is extremely low. Even with weekly injections for a full year, the cumulative weekly B6 dose from the compound alone ranges from 5 to 10 mg, far below the levels associated with neuropathy. The tolerable upper intake level set by the Institute of Medicine is 100 mg per day for adults, and the compounded dose is a small fraction of that.
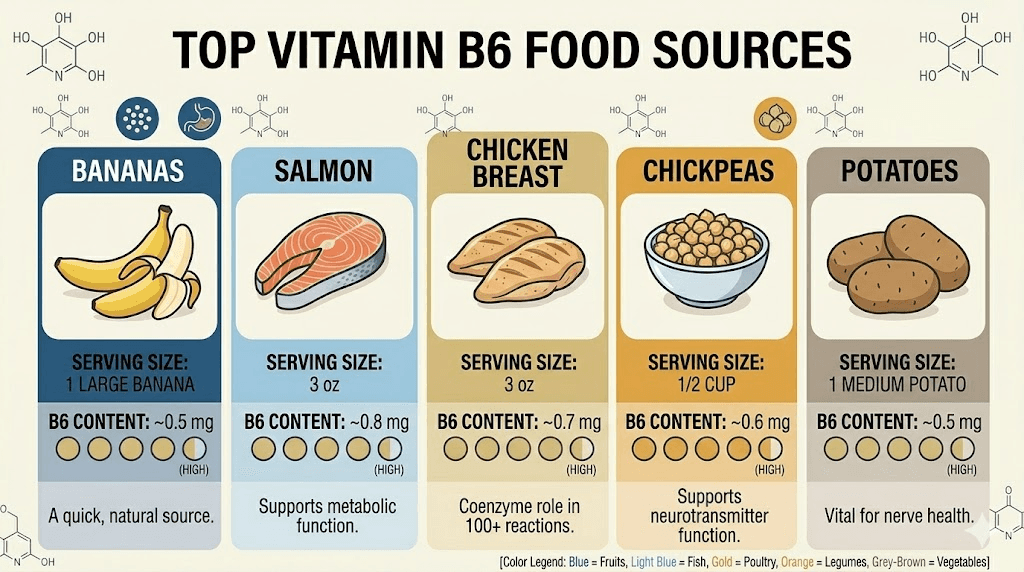
That said, you should inform your provider about all sources of B6 in your regimen. If you are also taking a B-complex supplement, a multivitamin, and eating B6-rich foods like poultry, fish, potatoes, and chickpeas, the total adds up. Your provider can assess your complete B6 intake and adjust the compound or your supplement regimen accordingly.
Semaglutide side effects remain
Pyridoxine addresses nausea specifically. It does not eliminate all semaglutide side effects. You may still experience:
Constipation affects 24% of semaglutide users in clinical trials. Slowed gastric motility extends throughout the GI tract, reducing bowel movement frequency. Adequate water intake, fiber, and in some cases stool softeners help manage this.
Dizziness occurs in some users, particularly during the first weeks. It may relate to blood sugar fluctuations or reduced caloric intake. Eating regular, balanced meals and staying hydrated minimize the risk.
Fatigue is common during caloric restriction. The body is adapting to lower energy intake. This is where a B12 additive might complement pyridoxine, if your provider offers a multi-additive formulation.
Hair thinning can occur with rapid weight loss from any cause, not just semaglutide. Adequate protein intake and nutritional supplementation help mitigate this.
Injection site reactions including redness, itching, or mild pain at the injection site affect a small percentage of users. Rotating injection sites and proper technique minimize these.
Drug interactions
Pyridoxine interacts with a few medications worth noting. Levodopa (used for Parkinson disease) effectiveness can be reduced by high-dose B6 unless combined with carbidopa. Phenytoin and phenobarbital (seizure medications) can be less effective at high B6 doses. Isoniazid and cycloserine (tuberculosis drugs) actually deplete B6, so the compound would be beneficial in those cases.
At the low doses used in compounded semaglutide (5-10 mg), clinically significant interactions are unlikely. But disclosure to your provider is always the right approach, especially if you take prescription medications.
Storage, handling, and shelf life
Compounded semaglutide with pyridoxine requires the same careful storage as standard compounded semaglutide. The compound is a protein-based medication, and improper storage degrades both the semaglutide and the pyridoxine.
Refrigeration requirements
Refrigeration is essential. Store the vial at 36-46 degrees Fahrenheit (2-8 degrees Celsius) at all times when not in use. The back of the refrigerator, away from the door, provides the most stable temperature. Do not freeze the compound. Freezing can cause the proteins to denature, rendering the medication ineffective.
If your compound is accidentally left out of the fridge, brief periods at room temperature (up to a few hours) are generally acceptable. Extended exposure to warmth, especially above 77 degrees Fahrenheit, can degrade the semaglutide component. If your semaglutide arrived warm during shipping, contact the pharmacy before using it.
Shelf life of the compound
Compounded semaglutide formulations typically have a beyond-use date (BUD) assigned by the compounding pharmacy, usually 30-90 days from the date of compounding depending on the pharmacy stability testing. This is shorter than the shelf life of brand-name semaglutide products because compounded medications do not undergo the same extensive stability testing.
Check the label on your vial for the specific BUD. Do not use the medication past this date. If you have concerns about whether your vial is still good, our guides on semaglutide shelf life and compounded semaglutide expiration cover the details.
Traveling with the compound
If you need to travel with your semaglutide, use an insulated medication travel case with cold packs. Keep the compound in your carry-on luggage, never checked baggage where temperature extremes are common. TSA allows injectable medications with proper documentation. A letter from your prescribing provider or the pharmacy label is usually sufficient. If your medication was exposed to heat during travel, check with your pharmacy before using it.
How to reconstitute semaglutide with pyridoxine
Most compounding pharmacies provide semaglutide with pyridoxine as a ready-to-inject solution. If your pharmacy provides it in lyophilized (freeze-dried) form requiring reconstitution, the process follows standard peptide reconstitution protocols.
You will need bacteriostatic water, an appropriate syringe, and alcohol swabs. The amount of bacteriostatic water to add depends on the desired final concentration, which your pharmacy or provider should specify. Our semaglutide reconstitution guide provides step-by-step instructions, and the peptide reconstitution calculator helps you determine exact volumes based on your vial potency and desired concentration.
When reconstituting, direct the bacteriostatic water along the inside wall of the vial rather than directly onto the powder. Swirl gently. Do not shake. Vigorous agitation can damage the semaglutide peptide chains and reduce potency. The solution should be clear and colorless once fully dissolved. If it appears cloudy or contains particles, do not use it.
Optimizing results on semaglutide with pyridoxine
The compound handles the nausea component. But maximizing your overall results requires attention to diet, timing, and lifestyle factors that many guides overlook.
Dietary strategies that complement the compound
Even with pyridoxine reducing nausea, certain dietary habits make or break the semaglutide experience. Protein intake is the single most important nutritional factor. Aim for 0.7-1.0 grams of protein per pound of body weight daily. This is difficult when your appetite is suppressed, which is why protein-dense food choices matter so much. Chicken, fish, Greek yogurt, eggs, and protein shakes become dietary staples.
Small, frequent meals work better than large ones. The delayed gastric emptying means your stomach processes food more slowly. Three smaller meals with two protein-rich snacks typically produce less GI discomfort than two or three large meals. Plan your GLP-1 friendly breakfasts to include both protein and fiber, setting a nutritional foundation for the day.
Hydration matters more than most people realize. Semaglutide can reduce thirst signals alongside appetite signals. Dehydration worsens nausea, constipation, and fatigue. Aim for at least 64 ounces of water daily, more if you exercise or live in a warm climate.
Timing your injection for minimal side effects
The best time of day to inject semaglutide varies by individual, but most people find that injecting in the evening or before bed minimizes the impact of any post-injection nausea. You sleep through the peak nausea window and wake up with the worst already passed. Others prefer morning injections to get it over with and manage any symptoms during the day.
Consistency matters more than the specific time. Inject on the same day each week, at roughly the same time. This maintains steady blood levels and reduces the peaks and troughs that can trigger breakthrough nausea. If you need to change your injection day, you can shift by a day or two as long as you maintain at least 48 hours between doses.
Exercise considerations
Exercise during semaglutide therapy preserves lean muscle mass, which is critical during rapid weight loss. Resistance training two to three times per week prevents the muscle loss that can accompany caloric deficit. Cardiovascular exercise supports metabolic health and mood. Some people find that semaglutide works even without exercise, but adding movement accelerates results and preserves the metabolic rate.
If nausea limits your exercise tolerance, particularly in the first hours after injection, schedule workouts for non-injection days or later in the day when nausea has subsided. The pyridoxine in your compound should help reduce this limitation, but listening to your body remains important.
Compounding pharmacies and the regulatory landscape
Understanding the regulatory context of compounded semaglutide with pyridoxine helps you make informed decisions about where to source your medication and what questions to ask your provider.
503A vs 503B pharmacies
Compounding pharmacies fall into two regulatory categories. 503A pharmacies compound medications based on individual prescriptions for specific patients. 503B pharmacies are outsourcing facilities that can compound larger batches without patient-specific prescriptions. Both types can produce semaglutide with pyridoxine, but 503B pharmacies typically undergo more rigorous FDA oversight, including regular inspections and batch testing requirements.
When evaluating a compounding pharmacy, look for accreditation from the Pharmacy Compounding Accreditation Board (PCAB) or state board of pharmacy compliance. Ask about their sterility testing protocols, beyond-use dating methodology, and whether they conduct potency testing on their semaglutide compounds. These questions are not unreasonable. They are the bare minimum for injectable medication safety.
FDA regulatory status
Compounded semaglutide with pyridoxine is not FDA-approved as a combination product. The FDA has approved semaglutide as a standalone medication (branded as Ozempic for diabetes and Wegovy for weight management), but the compounded versions containing additional ingredients like pyridoxine have not undergone FDA review for safety or efficacy as a combination.
This does not mean the combination is unsafe. Compounding pharmacies have legally produced customized medication formulations for decades under state pharmacy board regulation and FDA guidance. Many commonly used medications are compounded with additional ingredients to improve tolerability, adjust dosing, or address individual patient needs. However, the lack of FDA-specific approval means the combination has not been subjected to the controlled clinical trials that brand-name medications undergo.
Finding a provider who prescribes the compound
Not all providers are familiar with the semaglutide-pyridoxine combination. Telehealth weight management platforms, functional medicine practitioners, and obesity medicine specialists are most likely to be aware of and willing to prescribe compound formulations. When discussing this option with your provider, come prepared with information about the formulation, the evidence for pyridoxine anti-nausea effects, and why you believe it is appropriate for your situation.
If your current provider is unfamiliar with compounding, our guide on how to qualify for semaglutide and what to say when requesting GLP-1 options can help you navigate the conversation.
B6-rich foods that complement the compound
While the injectable pyridoxine provides a direct, controlled dose of vitamin B6, dietary sources complement the compound and support overall nutritional status during weight loss.
Top food sources of pyridoxine
The richest dietary sources of vitamin B6 include chicken breast (0.5 mg per 3 oz serving), salmon (0.6 mg per 3 oz serving), tuna (0.9 mg per 3 oz serving), chickpeas (1.1 mg per cup), potatoes (0.4 mg per medium potato), and bananas (0.4 mg per medium banana). Fortified cereals can provide the full daily recommended intake in a single serving.
Notice that many of the best B6 sources are also high in protein, which aligns perfectly with the dietary priorities during semaglutide therapy. Building meals around chicken, fish, and legumes simultaneously supports protein needs, B6 status, and the appetite-suppressing effects of the medication.
The recommended daily intake
The recommended dietary allowance (RDA) for vitamin B6 is 1.3 mg per day for adults aged 19-50, rising to 1.5 mg for women and 1.7 mg for men over age 50. Most Americans meet this requirement through diet alone. The pyridoxine in your semaglutide compound adds a supplemental dose on top of dietary intake, which provides a comfortable margin, particularly useful during periods of reduced food intake when dietary B6 may decrease.
If you are curious about your B6 status, a simple blood test measuring pyridoxal 5-phosphate (PLP) levels can confirm whether you are deficient, adequate, or well-supplied. Levels below 20 nmol/L indicate deficiency, while levels above 30 nmol/L are considered adequate.
What happens if you switch from standard semaglutide to the pyridoxine compound
If you are currently on standard compounded semaglutide or a brand-name version and want to switch to the pyridoxine formulation, the transition is straightforward. You do not need to restart from the lowest dose. Continue at your current dose level, simply switching to the pyridoxine-containing compound at your next injection.
Some people notice an improvement in nausea within the first one to two injections after switching. Others may not see a significant change if their nausea has already resolved through adaptation. The benefit is most pronounced for people who are still actively struggling with GI side effects or who are about to escalate to a higher dose.
If you are considering switching between different GLP-1 medications entirely, such as moving from tirzepatide to semaglutide or vice versa, discuss the transition plan with your provider. The dosing equivalencies are not straightforward, and our conversion chart provides general guidance on equivalent doses.
Semaglutide with pyridoxine versus tirzepatide with B6
Tirzepatide (the active ingredient in brand-name Mounjaro and Zepbound) is a dual GIP/GLP-1 receptor agonist that has shown even greater weight loss efficacy than semaglutide in head-to-head trials. Compounding pharmacies also produce tirzepatide with vitamin B6, using the same pyridoxine additive strategy.
The nausea profile differs between the two medications. Tirzepatide causes nausea in approximately 25-33% of users depending on dose, compared to 44% for semaglutide at 2.4 mg. The GIP receptor activation in tirzepatide may partially offset some of the GLP-1 mediated nausea. This means pyridoxine may provide proportionally greater benefit for semaglutide users than tirzepatide users, simply because the baseline nausea burden is higher. If you are weighing the two medications, you may also find our tirzepatide vs semaglutide dosage chart and semaglutide before and after results helpful for comparison.
If you are deciding between the two medications, our semaglutide vs tirzepatide comparison and side effects comparison guide provide detailed head-to-head analyses.
Managing expectations and tracking progress
Pyridoxine improves tolerance. It does not accelerate weight loss. Setting realistic expectations prevents frustration and keeps you committed for the long-term treatment course that meaningful weight loss requires.
Realistic weight loss timelines
Based on clinical trial data and real-world experience, here is what to expect at each phase of treatment:
Month 1 (0.25-0.5 mg): 2-5 pounds of weight loss, primarily from reduced caloric intake and some water weight. First month results are modest for most people.
Month 2-3 (0.5-1.0 mg): An additional 4-8 pounds. The pace picks up as the dose increases and appetite suppression becomes more consistent. Results vary based on starting weight, dietary choices, and activity level.
Month 4-6 (1.0-2.4 mg): This is typically the steepest weight loss phase. Many people lose 5-10% of their starting body weight by month 6. The week-by-week semaglutide results become increasingly visible.
Month 6-12 (2.4 mg maintenance): Weight loss continues but gradually slows. Most people reach their maximum benefit between 12-18 months. The STEP trials showed average losses of 14.9% of body weight at 68 weeks.
Beyond 12 months: Weight maintenance becomes the focus. Some people reach a plateau that requires dietary adjustments, exercise modifications, or discussions with their provider about dose optimization.
When the compound is not working
If you have been on semaglutide with pyridoxine for four or more weeks at a given dose and are still experiencing significant nausea, several possibilities exist. The dose may be too high for your current tolerance, and holding at the current level for additional weeks may help. The nausea may have a different primary cause, such as acid reflux, gastroparesis, or a food sensitivity unrelated to the medication. Or the pyridoxine dose in your specific compound may be insufficient for your needs.
Discuss these possibilities with your provider. Adjustments can include slowing the titration schedule, increasing the pyridoxine component, adding ondansetron for breakthrough nausea, or switching to a different GLP-1 medication if semaglutide fundamentally does not agree with your system.
If weight loss specifically has stalled despite good adherence, our guides on why semaglutide is not working and four weeks on semaglutide with no weight loss address the most common reasons and solutions.
Long-term considerations
Semaglutide therapy is typically a long-term commitment. Understanding what the extended timeline looks like helps you plan and prepare.
Duration of treatment
Most weight management protocols recommend continuing semaglutide for at least 12-18 months to reach full weight loss potential. Many providers recommend continued treatment beyond this point to maintain results, as stopping semaglutide is associated with weight regain in approximately two-thirds of patients within one year of discontinuation. For those wondering about the full picture, our guide on how long to stay on semaglutide covers the clinical recommendations. Some users who have been off treatment and want to resume should review the guidelines for restarting semaglutide after a break, as dosing protocols may differ from the initial start.
The pyridoxine component becomes less critical over time as the body adapts to semaglutide and nausea resolves naturally for most users. Some providers discontinue the pyridoxine additive once the patient has been stable on the maintenance dose for several months without GI issues. Others continue it throughout treatment as a preventive measure and for its general nutritional benefits.
Cost considerations
Compounded semaglutide with pyridoxine is typically priced similarly to standard compounded semaglutide. The addition of pyridoxine adds minimal cost to the formulation. The actual price varies widely between pharmacies, geographic regions, and provider markup structures. Be cautious of extremely low-priced options, which may indicate lower quality standards or less rigorous testing protocols.
Compare pricing between multiple compounding pharmacies and telehealth platforms. The major compounding pharmacies like Olympia, Belmar, and Elevate each have different pricing structures and formulation options. Some telehealth platforms bundle the consultation, prescription, and compound into a single monthly fee.
Monitoring and bloodwork
Regular monitoring during semaglutide therapy is standard practice regardless of the formulation. Most providers recommend baseline bloodwork before starting treatment, followed by periodic checks every 3-6 months. Key markers include fasting glucose, HbA1c (especially for diabetic patients), thyroid function (semaglutide carries a boxed warning about thyroid C-cell tumors in rodent studies), liver function, kidney function, lipid panel, and a complete metabolic panel.
If your provider is not already checking vitamin B6 levels, requesting a pyridoxal 5-phosphate (PLP) test at your next lab draw provides useful baseline data. This is especially relevant if you are supplementing B6 from multiple sources or if you have risk factors for B6 deficiency or toxicity.
Special populations and pyridoxine semaglutide
Certain groups require extra consideration when evaluating the semaglutide-pyridoxine combination. Your individual health profile, medications, and life circumstances all factor into whether this formulation is the right choice.
Women of reproductive age
Semaglutide is contraindicated during pregnancy and should be discontinued at least two months before a planned pregnancy. The pyridoxine component does not change this guidance. However, for women who may become pregnant unexpectedly, the fact that their semaglutide compound already contains B6 provides an incidental benefit. Pyridoxine is one of the first supplements recommended during early pregnancy for morning sickness management, so having adequate B6 stores from the compound could be protective during the transition period.
If you are using semaglutide for weight loss and considering pregnancy in the future, discuss timeline planning with your provider. The effects of semaglutide on menstrual cycles are worth understanding, as some women experience changes in cycle regularity during treatment.
People with kidney or liver conditions
Pyridoxine is primarily metabolized by the liver and excreted by the kidneys. In people with significant kidney or liver impairment, B6 clearance may be reduced, potentially leading to accumulation at standard doses. If you have chronic kidney disease, liver disease, or are taking medications that affect kidney or liver function, your provider may need to adjust the pyridoxine dose in your compound or monitor B6 levels more frequently.
Semaglutide itself requires caution in patients with a history of pancreatitis, severe GI disease, or medullary thyroid carcinoma. These contraindications exist regardless of whether pyridoxine is included in the formulation. The kidney safety profile of semaglutide is something to discuss with your provider if you have pre-existing renal concerns.
People taking psychiatric medications
Several psychiatric medications interact with vitamin B6 metabolism. MAO inhibitors, certain antipsychotics, and some antidepressants can affect B6 levels or be affected by supplemental B6. The doses used in semaglutide compounds are generally too low to cause clinically significant interactions, but disclosure is essential. Your prescribing provider and pharmacist should both be aware of all medications in your regimen.
The mood-supporting effects of adequate B6 levels, through serotonin and GABA synthesis, can actually complement psychiatric treatment rather than interfere with it. Some providers view the B6 component as an added benefit for patients who experience mood changes during significant weight loss and caloric restriction.
Older adults
Adults over 65 have increased B6 requirements (1.5-1.7 mg RDA compared to 1.3 mg for younger adults) and are more likely to have suboptimal B6 status. They also tend to experience more pronounced nausea with GLP-1 medications. The pyridoxine formulation may be particularly beneficial for this age group, addressing both the increased nausea susceptibility and the higher nutritional needs simultaneously.
However, older adults are also more susceptible to B6-related peripheral neuropathy, and they may already have neuropathy from other causes such as diabetes or vascular disease. Careful monitoring and a lower threshold for checking B6 levels is appropriate in this population.
Building your support protocol around the compound
The semaglutide-pyridoxine compound works best as part of a comprehensive approach. The medication handles appetite and the B6 handles nausea, but everything else, protein intake, hydration, movement, sleep, and stress management, determines how much benefit you actually extract from the treatment.
The protein priority
Protein preservation is the single most underestimated factor in GLP-1 weight loss. Rapid weight loss without adequate protein leads to muscle loss, reduced metabolic rate, and the "skinny fat" outcome that so many semaglutide users fear. Aim for a minimum of 100 grams of protein daily, spread across three to four meals. This is challenging when your appetite is suppressed. It requires intentional meal planning.
Start every meal with protein. If you can only eat half a plate, make sure the protein gets eaten first. Greek yogurt, cottage cheese, chicken breast, fish, eggs, and whey protein shakes are high-density protein sources that deliver significant protein in relatively small volumes. Our complete food guide for semaglutide provides meal-by-meal recommendations tailored to reduced appetites.
Hydration protocol
Dehydration is the silent saboteur of GLP-1 therapy. Semaglutide reduces thirst alongside appetite. Many users do not realize they are dehydrated until they develop headaches, constipation, or worsened nausea. All three symptoms improve with adequate water intake.
Track your water intake for at least the first month. Aim for half your body weight in ounces as a starting target. If you weigh 200 pounds, that is 100 ounces daily. Set reminders if necessary. Herbal teas, sparkling water, and water-rich foods like cucumbers and watermelon count toward your total. Caffeinated beverages have a mild diuretic effect and should not be your primary hydration source.
Sleep and recovery
Sleep quality often improves on semaglutide as weight decreases, particularly for people with obstructive sleep apnea. But the medication itself can occasionally cause insomnia in some users, especially when injecting later in the day. The B6 in your compound supports melatonin production through the serotonin-to-melatonin conversion pathway, which may provide a slight sleep benefit. But if insomnia becomes an issue, consider shifting your injection to the morning and discussing it with your provider.
Prioritize 7-9 hours of sleep nightly. Sleep deprivation increases cortisol, which promotes fat storage and increases appetite, directly counteracting what semaglutide is trying to do. Good sleep is not optional during weight loss. It is a foundational requirement that amplifies every other intervention.
Common misconceptions about semaglutide with pyridoxine
Several myths circulate about this compound formulation. Addressing them prevents poor decision-making based on inaccurate information.
Myth: pyridoxine makes semaglutide work better for weight loss
Pyridoxine does not enhance the weight loss mechanism of semaglutide. It does not increase GLP-1 receptor activation, amplify appetite suppression, or boost metabolism. Its role is purely supportive, reducing a side effect that would otherwise interfere with treatment adherence. The weight loss comes from semaglutide. The pyridoxine helps you stay on semaglutide long enough for it to work.
Myth: you can just take oral B6 instead of the compound
You can take oral vitamin B6 supplements alongside standard semaglutide, and some people do. However, there are potential advantages to the injectable route. Injectable pyridoxine bypasses the GI tract, which is important because semaglutide delayed gastric emptying can interfere with oral supplement absorption. The co-injection ensures that the B6 reaches systemic circulation at the same time as the semaglutide, providing nausea coverage right when it is most needed.
That said, oral B6 supplementation at 10-25 mg daily is a reasonable, lower-cost alternative for people who cannot access the compound formulation. Discuss both options with your provider.
Myth: more B6 means less nausea
The anti-nausea benefit of pyridoxine does not scale linearly with dose. There is a therapeutic window. Below a certain threshold, you get insufficient nausea relief. Above a certain point, additional B6 provides no further benefit and begins to carry toxicity risk. The 5-10 mg range used in most compounds sits comfortably within the effective and safe zone. Asking your pharmacy to double or triple the pyridoxine dose is not advisable and unlikely to produce better outcomes.
Myth: the compound is just as regulated as brand-name semaglutide
This is not accurate. Compounded medications, including semaglutide with pyridoxine, are regulated differently than FDA-approved brand-name drugs. They do not undergo the same pre-market review, clinical trials, or post-market surveillance. They are regulated primarily at the state level through boards of pharmacy, with additional federal oversight for 503B outsourcing facilities. This does not make them inherently dangerous, but it does mean the quality assurance depends heavily on the specific pharmacy producing the compound.
The role of SeekPeptides in your semaglutide journey
Navigating compounded semaglutide formulations, dosing schedules, and additive options is overwhelming. SeekPeptides exists to cut through that confusion. Members access evidence-based protocol guides, dosage calculators, comprehensive compound comparison resources, and a community of researchers who have navigated these exact decisions.
Whether you are trying to determine the right additive for your semaglutide compound, understand dosage chart conversions, or troubleshoot side effects that are not responding to standard approaches, SeekPeptides provides the depth of information that generic health sites simply do not offer. The platform was built specifically for people serious about peptide research, with protocols informed by clinical literature and real-world experience from thousands of users.
Combining semaglutide with pyridoxine and other interventions
Semaglutide does not exist in isolation. Many people combine it with other medications, supplements, or lifestyle interventions. Understanding how pyridoxine-containing semaglutide interacts with common combinations helps you and your provider optimize your protocol.
Semaglutide with pyridoxine and metformin
Metformin is one of the most commonly co-prescribed medications with GLP-1 agonists, particularly for patients with type 2 diabetes or insulin resistance. The combination is generally well-tolerated, though both medications can cause GI side effects. Metformin own nausea potential is well-documented, and adding it to semaglutide increases the cumulative GI burden. The pyridoxine in the semaglutide compound may help offset some of this combined nausea load, though clinical data on this specific three-way interaction is limited.
Semaglutide with pyridoxine and phentermine
Some providers prescribe phentermine alongside semaglutide for enhanced appetite suppression, particularly in the early weeks before semaglutide reaches full effect. Phentermine is a sympathomimetic amine that stimulates the central nervous system. It does not typically cause nausea, so the pyridoxine component of your semaglutide compound does not interact meaningfully with phentermine pharmacology.
Semaglutide with pyridoxine and berberine
Berberine and semaglutide together is a combination that has gained popularity for its potential synergistic effects on blood sugar regulation and metabolic health. Berberine can cause its own GI side effects, including nausea and diarrhea. The pyridoxine in your semaglutide compound may provide some cross-protective benefit against berberine-induced nausea, though this has not been specifically studied.
Alcohol considerations
Alcohol interacts with semaglutide in ways that affect both efficacy and side effects. Drinking on semaglutide can intensify nausea, worsen dehydration, slow weight loss progress, and increase the risk of hypoglycemia. The pyridoxine in your compound does not mitigate these alcohol-related effects. If you choose to drink, moderation is essential, and timing your consumption away from injection day minimizes complications.
Practical tips from people who have used the compound
Clinical data tells one story. Real-world experience tells another. Here are the practical insights that emerge from user communities and provider feedback about the semaglutide-pyridoxine combination.
Injection day strategies
Most users on the pyridoxine compound report that injection day nausea, while reduced compared to standard semaglutide, can still be noticeable at higher doses. Successful strategies include: injecting in the evening around 7-8 PM so the initial nausea peak occurs during sleep. Eating a light, protein-rich meal 2-3 hours before injection rather than injecting on an empty stomach. Having ginger tea, peppermint tea, or ginger chews available for the first 24 hours post-injection. Keeping meals small and bland for the first day after injection, then gradually returning to normal eating by day two or three.
Managing the dose escalation transitions
The transitions from 0.5 mg to 1.0 mg and from 1.7 mg to 2.4 mg are the two points where nausea most commonly spikes. Some users on the pyridoxine compound preemptively eat lighter in the 24 hours leading up to their dose escalation injection. Others use over-the-counter anti-nausea options like ginger supplements or bismuth subsalicylate as a temporary backup during the first week at a new dose.
If nausea becomes severe despite pyridoxine, ondansetron (Zofran) is a prescription anti-nausea medication that many providers prescribe as a rescue option. It works through a different mechanism (5-HT3 receptor antagonism) that complements pyridoxine serotonin-modulating effects.
Signs your compound is working properly
A well-formulated semaglutide with pyridoxine compound should produce consistent appetite suppression within 24-48 hours of injection, with gradual onset rather than sudden onset. Nausea, if present, should be mild and brief, typically resolving within 1-2 days of injection. Weight loss should follow the expected trajectory for your dose level. The compound should remain clear, colorless, and particulate-free throughout its shelf life. If any of these markers are missing, discuss with your provider or pharmacy about potential formulation issues.
Understanding blood work changes on the compound
Semaglutide therapy produces measurable changes in blood work that both you and your provider should monitor. The pyridoxine component adds a layer to watch as well.
Expected metabolic improvements
Weight loss from semaglutide typically produces favorable changes in fasting glucose (decreases), HbA1c (decreases), triglycerides (decreases), LDL cholesterol (modest decrease), HDL cholesterol (modest increase), blood pressure (decreases with weight loss), and inflammatory markers like C-reactive protein (decreases). These improvements are driven by the weight loss itself and the direct metabolic effects of GLP-1 receptor activation.
B6-related markers to watch
If you are receiving pyridoxine through the compound and also supplementing orally or through diet, your PLP levels may be higher than the reference range. This is not necessarily concerning at therapeutic doses. However, if PLP levels exceed 200 nmol/L or if you develop numbness or tingling in the extremities, discuss with your provider about potential B6 accumulation.
Some providers also check homocysteine levels, as B6 (along with B12 and folate) plays a role in homocysteine metabolism. Elevated homocysteine is associated with cardiovascular risk, and adequate B6 helps keep levels in check. The pyridoxine in your compound may contribute positively to this marker.
Future of GLP-1 compound formulations
The landscape of compounded GLP-1 medications continues to evolve. Understanding where things are headed helps you plan your treatment approach.
Multi-additive formulations are becoming more sophisticated. Some pharmacies now offer compounds with three or four additives, semaglutide with pyridoxine plus B12 plus glycine, for example, attempting to address nausea, fatigue, and muscle preservation simultaneously in a single injection. The clinical evidence for these multi-additive combinations is limited, but anecdotal reports from providers and patients are generally positive.
Oral compound formulations are also emerging. Some pharmacies offer oral semaglutide drops or sublingual semaglutide that include pyridoxine. The bioavailability of oral semaglutide is lower than injectable, and the addition of B6 to these oral formulations is even less studied. If considering an oral route, weigh the convenience against the potentially reduced efficacy and discuss the tradeoffs with your provider.
For researchers serious about optimizing their GLP-1 protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
Frequently asked questions
Does pyridoxine in semaglutide completely eliminate nausea?
No. Pyridoxine reduces the severity and duration of nausea for most users, but it does not eliminate it entirely. Most people on the compound report milder, shorter nausea episodes compared to standard semaglutide, particularly during dose escalation. Individual responses vary based on sensitivity, dose level, and other factors.
Can I add pyridoxine to my existing semaglutide compound?
Not at home. Combining medications requires sterile compounding conditions. Ask your prescribing provider to switch your prescription to a semaglutide-pyridoxine formulation, which the compounding pharmacy will prepare. Alternatively, you can take oral vitamin B6 supplements (10-25 mg daily) alongside your current semaglutide, though injectable delivery may be more effective.
Is semaglutide with pyridoxine more expensive than standard compounded semaglutide?
Generally, the price difference is minimal. Pyridoxine is an inexpensive ingredient, and the additional compounding steps are straightforward. Expect no more than a 5-15% increase in cost compared to standard compounded semaglutide, if any. Some pharmacies price them identically.
How long should I stay on the pyridoxine formulation?
Most providers recommend continuing the pyridoxine formulation at least through the full dose escalation phase (approximately 16-20 weeks). After reaching and stabilizing on the maintenance dose, your provider may suggest switching to standard semaglutide if nausea has fully resolved. Others continue the pyridoxine formulation long-term for its general nutritional benefits during extended treatment.
Can I take a separate B6 supplement while on the pyridoxine compound?
Technically yes, but monitor your total B6 intake. The compound provides 5-10 mg per week. If you are also taking a B-complex or multivitamin with B6, plus eating B6-rich foods, the total could add up. Stay below 100 mg total daily from all sources to maintain a safe margin. Inform your provider about all supplement use.
Is the pyridoxine compound available in pre-filled pens?
Most compounding pharmacies provide the compound in multi-dose vials rather than pre-filled pens. You will need insulin syringes to draw and inject the medication. Brand-name pre-filled pens (Ozempic, Wegovy) do not contain pyridoxine and are separate products entirely.
What if I experience tingling or numbness in my hands or feet?
Tingling or numbness could indicate B6 accumulation or other causes including nerve compression, B12 deficiency, or semaglutide side effects. Report these symptoms to your provider immediately. They may check your B6 levels, adjust the formulation, or investigate other causes. At standard compound doses, B6-related neuropathy is extremely unlikely, but monitoring is important.
Does the pyridoxine affect semaglutide shelf life or stability?
The addition of pyridoxine should not significantly affect the shelf life of the compound. Follow the beyond-use date assigned by your compounding pharmacy and store according to their instructions. The stability of the combination depends on the pharmacy specific formulation and testing protocols.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your nausea stay mild, your dose escalation stay smooth, and your protocols stay effective.