Mar 22, 2026

Some researchers draw exactly 5 units from a semaglutide vial and get their target dose. Others draw the same 5 units and end up with double what they intended. Same syringe. Same number on the barrel. Completely different amounts of active peptide entering the body.
The difference comes down to one number printed on the vial label. Concentration. That single variable transforms 5 units from a precise microdose into a potentially problematic overdose, or from an effective starting point into a dose so small it does nothing at all. And the confusion is not accidental. Compounded semaglutide arrives in concentrations ranging from 1 mg/mL all the way up to 5 mg/mL, with several options in between. Each concentration produces a different milligram dose when you draw 5 units on an insulin syringe.
This guide breaks down every possible answer to the question. You will learn the exact milligram value of 5 units at every common concentration, understand the formula behind the conversion, and walk away confident that you are measuring correctly. Whether you are starting a compounded semaglutide protocol for the first time or double-checking your math before your next injection, the numbers here will keep you safe and accurate.
The quick answer for every concentration
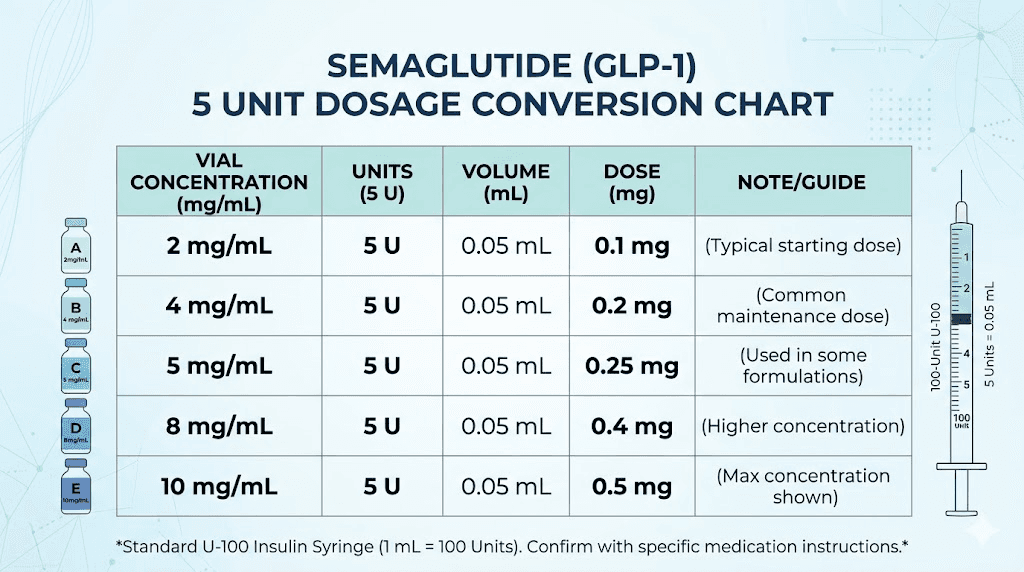
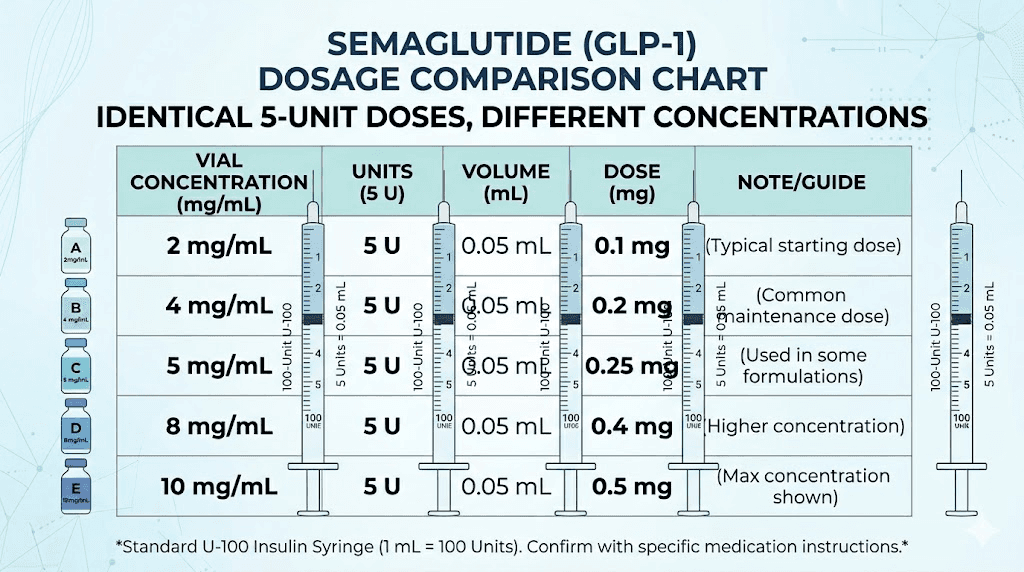
Five units on a standard U-100 insulin syringe equals 0.05 mL of liquid. That volume never changes regardless of what is inside the vial. What changes is how much semaglutide is dissolved in that 0.05 mL.
Here is the complete breakdown.
Vial concentration | 5 units equals | Volume drawn |
|---|---|---|
1 mg/mL | 0.05 mg | 0.05 mL |
2 mg/mL | 0.10 mg | 0.05 mL |
2.5 mg/mL | 0.125 mg | 0.05 mL |
3 mg/mL | 0.15 mg | 0.05 mL |
5 mg/mL | 0.25 mg | 0.05 mL |
Notice the pattern. The volume stays constant at 0.05 mL every single time. But the milligram dose ranges from 0.05 mg at the lowest concentration to 0.25 mg at the highest. That is a fivefold difference from the same syringe reading. If you are using our semaglutide dosage calculator, it handles this math automatically. But understanding the numbers yourself is essential for safe dosing.
The most common concentration you will encounter is 5 mg/mL. Most compounding pharmacies favor this concentration because it makes the math clean, with each 5-unit increment corresponding to exactly 0.25 mg. At this concentration, 5 units delivers 0.25 mg, which happens to be the standard starting dose for most semaglutide protocols.
Understanding the conversion formula
The math behind semaglutide unit conversion is straightforward once you understand three variables. You need the number of units you are drawing, the total units in your syringe (always 100 for a U-100 insulin syringe), and the concentration printed on your vial.
The formula looks like this:
Dose in mg = (units drawn / 100) x concentration in mg/mL
For 5 units from a 5 mg/mL vial:
(5 / 100) x 5 = 0.05 x 5 = 0.25 mg
Simple. Clean. No guesswork.
But here is where people get confused. The word "units" on an insulin syringe does not refer to units of semaglutide. It refers to units of volume. A U-100 insulin syringe was originally designed for insulin, where 100 units equals 1 mL. When you repurpose that syringe for semaglutide, the unit markings simply tell you how much liquid you are drawing. They say nothing about the actual drug dose until you factor in concentration.
This distinction trips up even experienced researchers. If you have used our semaglutide units to mg conversion guide, you already know this. But it bears repeating every time you prepare a dose, because a moment of inattention with the wrong concentration can mean injecting two or three times what you intended.
Why U-100 syringes became the standard
U-100 insulin syringes dominate the compounded peptide space for practical reasons. They are widely available at any pharmacy. The markings are precise enough for small doses. And the needle gauge, typically 29 to 31 gauge, is thin enough for comfortable subcutaneous injection.
The 100-unit scale also makes percentage-based calculations intuitive. Drawing 5 units means drawing 5% of 1 mL, which equals 0.05 mL. Drawing 10 units means drawing 10%, or 0.10 mL. The math scales linearly, so once you understand one conversion, you understand them all.
Some researchers prefer tuberculin syringes marked in milliliters rather than units. These syringes display 0.01 mL increments directly, eliminating one step in the conversion process. For a 5-unit dose, you would draw to the 0.05 mL line on a tuberculin syringe. The result is identical. Only the markings differ.
Working the formula in reverse
Sometimes you know the milligram dose you want and need to figure out how many units to draw. The reverse formula is equally simple:
Units to draw = (desired mg / concentration in mg/mL) x 100
If your provider prescribed 0.25 mg and you have a 5 mg/mL vial:
(0.25 / 5) x 100 = 5 units
If you have a 2.5 mg/mL vial instead:
(0.25 / 2.5) x 100 = 10 units
Same dose. Different unit count. Different concentration. This is exactly why checking your vial label matters every single time. Our peptide calculator handles both forward and reverse conversions, but knowing the formula gives you a built-in safety check whenever the numbers on a calculator seem off.
Concentration-by-concentration breakdown
Each semaglutide concentration tells a different story when you draw 5 units. Some concentrations make 5 units a meaningful starting dose. Others make it a micro amount barely worth injecting. Understanding where your vial falls on this spectrum determines whether 5 units is right for your protocol.
5 mg/mL concentration (the most common)
At 5 mg/mL, 5 units delivers exactly 0.25 mg of semaglutide. This is the standard starting dose in most compounded semaglutide dosing schedules. Compounding pharmacies prefer this concentration because the math works out to clean numbers at every standard dose level.
Here is why 5 mg/mL dominates the compounded market. At this concentration, the standard titration schedule aligns perfectly with easy-to-read syringe markings:
Dose | Units to draw | Titration phase |
|---|---|---|
0.25 mg | 5 units | Starting dose (weeks 1-4) |
0.50 mg | 10 units | First increase (weeks 5-8) |
1.0 mg | 20 units | Second increase (weeks 9-12) |
1.7 mg | 34 units | Third increase (weeks 13-16) |
2.4 mg | 48 units | Maintenance dose |
Every dose falls on a clearly visible syringe marking. No squinting between lines. No estimating half-marks. For the starting dose specifically, 5 units sits right on a major graduation line on most insulin syringes, making it nearly impossible to mismeasure.
If you are working with a 5 mg/mL vial and wondering about the full 5 mg/mL dosage chart, our complete guide covers every increment from 5 units through 50 units with the corresponding milligram values.
3 mg/mL concentration
At 3 mg/mL, 5 units equals 0.15 mg. This falls below the standard 0.25 mg starting dose, making 5 units at this concentration suitable primarily for microdosing protocols or for researchers who want to start even more conservatively than the standard titration schedule recommends.
The 3 mg/mL concentration appears less frequently in the compounded semaglutide market. When it does appear, the arithmetic becomes slightly less convenient. To reach the standard 0.25 mg starting dose, you would need approximately 8.3 units, a number that falls between graduation marks on most syringes. This imprecision is one reason most pharmacies have moved toward the cleaner 5 mg/mL formulation.
That said, 0.15 mg is not a useless dose. Some providers specifically prescribe sub-therapeutic starting doses to minimize gastrointestinal side effects during the initial adjustment period. If nausea, constipation, or sulfur burps have been a concern, starting at 0.15 mg and titrating slowly can help the body adapt more gently.
2.5 mg/mL concentration
At 2.5 mg/mL, 5 units equals 0.125 mg. This is exactly half the standard starting dose. Some older compounded formulations and certain pre-filled vials use this concentration.
The math at 2.5 mg/mL creates a straightforward relationship. To reach 0.25 mg, you need 10 units instead of 5. To reach 0.5 mg, you need 20 units. Everything doubles compared to the 5 mg/mL concentration. This can actually be advantageous for precision at very low doses. Drawing 10 units for a 0.25 mg dose gives you more room on the syringe barrel compared to drawing just 5 units, reducing the chance of mismeasurement.
However, the tradeoff is injection volume. Higher doses at 2.5 mg/mL require drawing significantly more liquid. A 2.4 mg maintenance dose would require 96 units, nearly filling the entire syringe. At that point, the injection volume (0.96 mL) can cause more discomfort at the injection site compared to the 0.48 mL you would inject at 5 mg/mL for the same dose.
2 mg/mL concentration
At 2 mg/mL, 5 units delivers only 0.10 mg of semaglutide. This is a genuinely small dose. Less than half the standard starting amount. Less than what most clinical protocols consider a therapeutic starting point for weight management.
You might encounter 2 mg/mL concentrations from certain compounding pharmacies that specialize in ultra-low-dose formulations. Some providers use this concentration specifically for patients who have experienced significant dizziness or fatigue at standard starting doses and need to begin even lower.
At 0.10 mg, the GLP-1 receptor activation is minimal but not zero. Research suggests that even sub-therapeutic doses can begin priming receptor sensitivity, potentially making the transition to higher doses smoother when the time comes. Think of it as a pre-loading phase rather than a treatment phase.
1 mg/mL concentration
At 1 mg/mL, 5 units equals just 0.05 mg. This is one-fifth of the standard starting dose and represents the absolute minimum that most researchers would consider drawing. At this dose level, you are operating firmly in microdose territory.
The 1 mg/mL concentration is uncommon in the compounded semaglutide market for weight management. When it does appear, it is typically in research contexts or in formulations designed specifically for split-dose protocols where very small amounts are administered multiple times per week rather than a larger dose once weekly.
One practical advantage of this concentration at 5 units is precision. Drawing 5 units from a 1 mg/mL vial puts you at a clearly marked line on the syringe. If you needed 0.05 mg from a 5 mg/mL vial, you would need just 1 unit, a marking so small that accurate measurement becomes nearly impossible without magnification.
How to read your semaglutide vial label
The concentration is printed on every vial. Finding it takes seconds once you know where to look. But reading it wrong can mean dosing errors that compound over weeks of treatment.
Look for one of these formats on the label:
5 mg/mL (five milligrams per milliliter)
5mg/1mL (same thing, written differently)
12.5 mg/2.5 mL (total contents divided by total volume, equals 5 mg/mL)
The third format causes the most confusion. When a vial says 12.5 mg/2.5 mL, the concentration is still 5 mg/mL because 12.5 divided by 2.5 equals 5. But some researchers see "12.5 mg" and think they have a higher concentration product. They do not. The label is simply telling you the total amount of semaglutide in the entire vial, not the concentration per milliliter.
Here is a quick reference for common vial labeling and what the concentration actually is:
Label says | Actual concentration | 5 units equals |
|---|---|---|
5 mg/mL | 5 mg/mL | 0.25 mg |
5 mg/1 mL | 5 mg/mL | 0.25 mg |
10 mg/2 mL | 5 mg/mL | 0.25 mg |
12.5 mg/2.5 mL | 5 mg/mL | 0.25 mg |
2.5 mg/mL | 2.5 mg/mL | 0.125 mg |
5 mg/2 mL | 2.5 mg/mL | 0.125 mg |
7.5 mg/3 mL | 2.5 mg/mL | 0.125 mg |
Always divide the total milligrams by the total milliliters to find your concentration. Then apply the formula. If the math does not feel right, verify with your pharmacist or use a dosage calculator before drawing your dose.
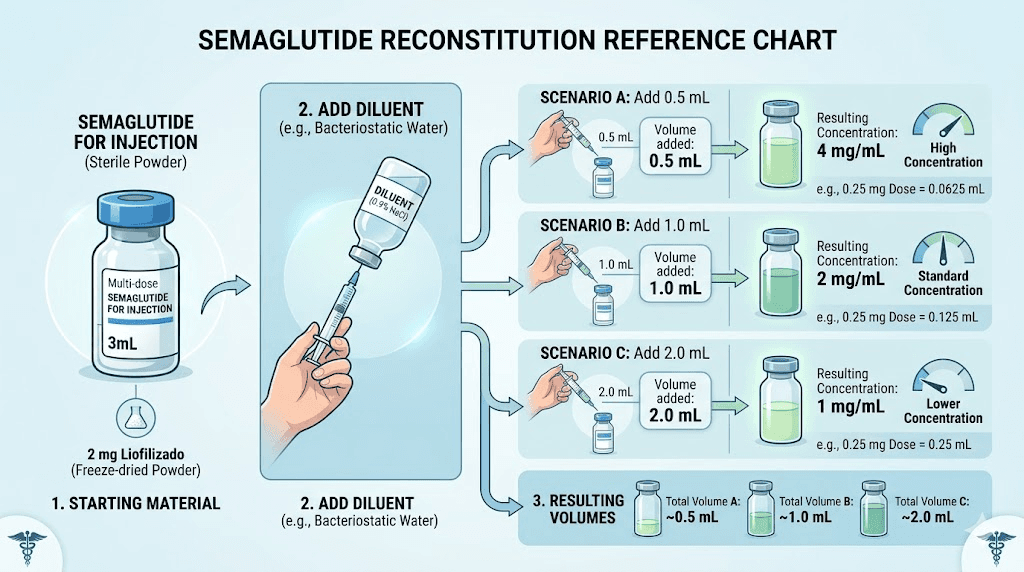
Some vials also list the concentration after reconstitution. If you received lyophilized (freeze-dried) semaglutide powder and reconstituted it yourself with bacteriostatic water, the concentration depends entirely on how much water you added. Adding 1 mL of water to 5 mg of powder creates a 5 mg/mL solution. Adding 2 mL creates 2.5 mg/mL. The amount of water you used during reconstitution is the concentration-defining variable.
Drawing exactly 5 units with an insulin syringe
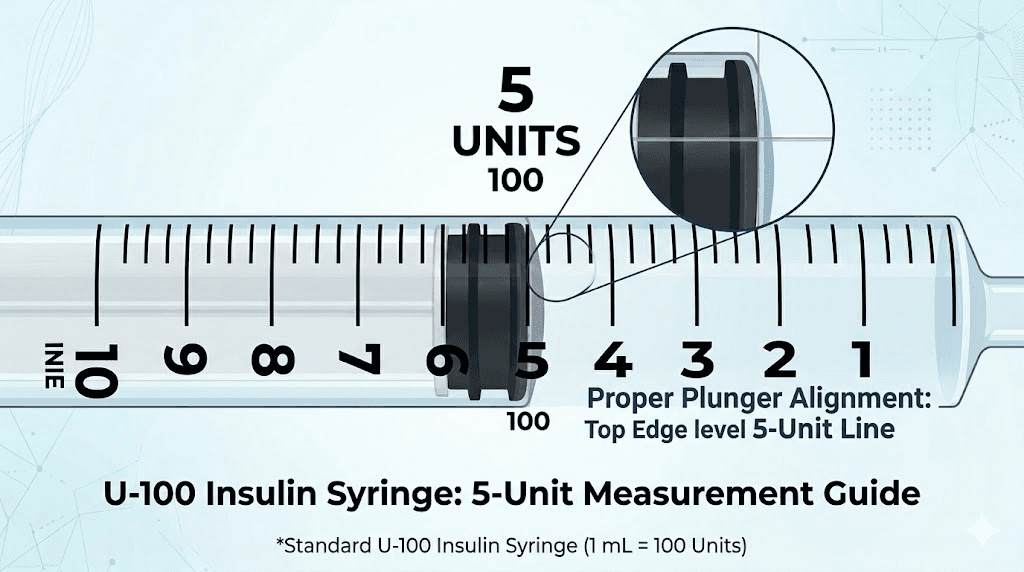
Five units is a small volume. Really small. On a 1 mL (100-unit) insulin syringe, 5 units occupies the very bottom of the barrel, just one major graduation mark above zero. Getting it right requires attention to technique.
Choosing the right syringe size
Standard insulin syringes come in three sizes. The 1 mL (100-unit) syringe covers the full range from 0 to 100 units. The 0.5 mL (50-unit) syringe covers 0 to 50 units with more widely spaced markings. And the 0.3 mL (30-unit) syringe covers 0 to 30 units with the most detailed graduation marks.
For a 5-unit dose, the 0.3 mL syringe offers the best precision. Each unit marking on a 30-unit syringe is approximately twice as wide as the markings on a 100-unit syringe, making it much easier to identify exactly where 5 units falls. If you are consistently dosing at 5 units, investing in 0.3 mL syringes will improve your accuracy significantly.
However, the 0.5 mL and 1 mL syringes work perfectly fine for 5 units as well. The 5-unit line appears as a clearly marked graduation on all standard insulin syringes. You do not need to estimate between lines, which is where most measurement errors occur. For detailed guidance on using your syringe correctly, our injection guide walks through the process step by step.
Step-by-step technique for drawing 5 units
Clean the vial stopper with an alcohol swab and let it dry. Pull the syringe plunger back to the 5-unit mark, drawing air into the barrel. Insert the needle through the vial stopper and push the air in. This equalizes pressure inside the vial and makes drawing liquid easier.
Now flip the vial upside down with the syringe still inserted. Pull the plunger back slowly past the 5-unit mark. You want to overdraw slightly. Tap the syringe barrel gently to move any air bubbles to the top, near the needle. Then push the plunger forward carefully until the bottom of the plunger gasket sits exactly on the 5-unit line.
Read the syringe at eye level. Hold it horizontally with the markings facing you. The bottom edge of the rubber gasket, not the top, indicates your volume. This detail matters more at small volumes like 5 units where even a half-unit error represents a 10% dosing change.
Remove the syringe from the vial. If you see a small bubble trapped in the liquid, flick the barrel gently and push the bubble out by advancing the plunger slightly. Then re-verify your volume. Air bubbles at 5 units can displace a meaningful percentage of your dose. At 20 units or higher, a tiny bubble matters less proportionally. At 5 units, it matters a lot.
Air bubbles and dead space
Every syringe has a small amount of dead space, the volume of liquid that remains in the needle hub after you push the plunger all the way down. For most insulin syringes, dead space holds approximately 0.5 to 1 unit of liquid. At a 5-unit dose, that dead space represents 10% to 20% of your intended dose that never gets injected.
Low dead space syringes reduce this loss to nearly zero. If you are dosing consistently at 5 units, consider switching to low dead space models. The cost difference is minimal, and the dosing accuracy improvement is substantial at these small volumes.
Air bubbles present a different challenge. A bubble sitting in the middle of your drawn liquid effectively reduces the volume of semaglutide in the syringe. A 1-unit air bubble in a 5-unit draw means you only have 4 units of actual solution. That is a 20% underdose. Always eliminate visible bubbles before injecting, and always recheck your volume after removing them.
When 5 units is the right starting dose
For the majority of people beginning semaglutide with a 5 mg/mL vial, 5 units (0.25 mg) is the correct starting dose. This aligns with both the FDA-approved Wegovy titration schedule and the protocols most compounding pharmacies recommend.
The logic behind starting at 0.25 mg is simple. Semaglutide activates GLP-1 receptors throughout the body, affecting appetite regulation, gastric emptying, and insulin signaling simultaneously. Starting low gives these systems time to adjust. Jumping straight to a higher dose dramatically increases the risk of gastrointestinal side effects that make people want to quit before the medication has a chance to work.
Most protocols keep the dose at 0.25 mg (5 units from a 5 mg/mL vial) for four weeks. Four weeks is not arbitrary. It typically takes 4 to 5 half-lives for semaglutide to reach steady-state blood levels, and with a half-life of approximately 7 days, that works out to about 4 weeks. By the end of week 4, your body has adapted to the GLP-1 receptor activation, and appetite suppression typically becomes noticeable.
Who might start below 5 units
Not everyone begins at the standard 0.25 mg. Some individuals benefit from starting even lower. This includes people with a history of severe gastrointestinal sensitivity, those who have previously tried semaglutide and stopped due to side effects, and researchers exploring sub-therapeutic doses for non-weight-related applications.
With a 5 mg/mL vial, going below 5 units means drawing between 1 and 4 units. At 2.5 units, you get 0.125 mg. At 1 unit, just 0.05 mg. These micro-amounts are difficult to measure accurately on standard syringes. If sub-0.25 mg dosing is part of your protocol, using a lower concentration vial (2.5 mg/mL or 3 mg/mL) or a smaller syringe will improve precision.
Some providers recommend starting at 0.125 mg for the first week or two, then moving up to 0.25 mg. This creates an even gentler on-ramp. If your first week on semaglutide produces significant nausea or discomfort, this approach can help. The tradeoff is a slower path to effective doses, but for people who have quit other GLP-1 medications due to side effects, slower often means sustainable.
Who should not stop at 5 units
Five units at 0.25 mg is a starting dose, not a destination. Clinical trials establishing semaglutide effectiveness for weight management used doses up to 2.4 mg weekly. The 0.25 mg starting dose showed minimal weight loss on its own. The real results came at higher doses after proper titration.
If you have been at 5 units for more than 4 weeks and are not seeing weight loss results, the dose is likely too low. The standard protocol increases to 0.5 mg (10 units from a 5 mg/mL vial) at week 5, then continues titrating upward every 4 weeks until reaching the target maintenance dose.
Staying at the starting dose indefinitely is one of the most common mistakes researchers make. It feels safe. Side effects are minimal. But the therapeutic benefits are also minimal. The week-by-week results data shows clearly that meaningful outcomes require titration to effective doses.
Titration schedules starting from 5 units
Starting at 5 units is just the beginning. Where you go from there depends on your protocol, your tolerance, and your goals. Here are the most common titration paths, all assuming a 5 mg/mL vial concentration.
Standard clinical titration
The standard schedule follows the FDA-approved Wegovy titration. It moves upward every 4 weeks, giving the body time to adapt at each level. This is the approach most providers recommend and the one with the strongest clinical evidence behind it.
Weeks | Dose | Units (5 mg/mL) | What to expect |
|---|---|---|---|
1-4 | 0.25 mg | 5 units | Mild appetite changes, possible nausea |
5-8 | 0.5 mg | 10 units | Noticeable appetite reduction |
9-12 | 1.0 mg | 20 units | Significant appetite suppression |
13-16 | 1.7 mg | 34 units | Strong appetite control, weight loss accelerates |
17+ | 2.4 mg | 48 units | Maintenance dose, maximum effect |
Each increase doubles or nearly doubles the previous dose for the first three steps. The jump from 0.25 to 0.5 is a 100% increase. From 0.5 to 1.0 is another 100% increase. After that, the increments become proportionally smaller (70% from 1.0 to 1.7, then 41% from 1.7 to 2.4). This gradual flattening of the escalation curve is intentional, reducing the risk of severe side effects as doses climb higher.
For detailed conversion charts at every dose level, our complete semaglutide dosage conversion guide covers every concentration and every common dose.
Conservative titration
Some researchers prefer a slower approach, especially those who experienced nausea or other side effects during initial dosing. A conservative schedule might look like this:
Weeks | Dose | Units (5 mg/mL) |
|---|---|---|
1-4 | 0.25 mg | 5 units |
5-8 | 0.25 mg | 5 units (extended) |
9-12 | 0.5 mg | 10 units |
13-16 | 0.5 mg | 10 units (extended) |
17-20 | 1.0 mg | 20 units |
21-24 | 1.7 mg | 34 units |
25+ | 2.4 mg | 48 units |
This schedule takes nearly twice as long to reach the maintenance dose. But for people who are highly sensitive to GLP-1 agonists, the slower ramp prevents the kind of severe nausea and gastrointestinal distress that leads to premature discontinuation. Staying on the medication at a lower dose beats quitting at a higher one.
The key question is whether to extend the starting phase or move forward. If 5 units produces no side effects at all after 2 weeks, there is no pharmacological reason to stay there for 8 weeks. The extended timeline serves people who need it, not everyone. Your body will tell you which schedule fits. Listen to it.
Microdosing approach
A newer approach gaining attention involves staying at very low doses for extended periods rather than titrating to standard therapeutic levels. This is sometimes called GLP-1 microdosing, and it targets anti-inflammatory and metabolic benefits rather than maximum weight loss.
At 5 units from a 5 mg/mL vial (0.25 mg), the dose is already at the lower end of clinical dosing. True microdosing protocols might stay here or go even lower, using 2 to 3 units (0.10 to 0.15 mg) for weeks or months. The evidence base for this approach is still emerging, but anecdotal reports suggest benefits for autoimmune conditions, systemic inflammation, and long-term metabolic maintenance after achieving weight loss at higher doses.
Common mistakes when measuring 5 units
Small doses amplify small errors. A mistake that would barely matter at 40 units becomes clinically significant at 5 units. Here are the most frequent errors and how to avoid them.
Confusing concentration with dose
This is the number one mistake. A researcher switches from a 5 mg/mL vial to a 2.5 mg/mL vial and continues drawing 5 units, assuming they are getting the same dose. They are not. They just cut their dose in half without realizing it.
The reverse scenario is more dangerous. Switching from a 2.5 mg/mL vial to a 5 mg/mL vial while drawing the same number of units doubles the dose. If someone was stable at 0.125 mg (5 units from 2.5 mg/mL) and suddenly receives 0.25 mg (5 units from 5 mg/mL), the jump can trigger significant appetite suppression and gastrointestinal side effects.
Every time you open a new vial, read the concentration. Every single time. Even if you think it is the same as your last vial. Pharmacies can change formulations between orders. Verify before you draw.
Reading the syringe at the wrong part of the plunger
The rubber gasket at the end of the plunger has a dome shape. The top of the dome and the bottom of the dome can be 0.5 to 1 unit apart. At 5 units, reading from the top instead of the bottom means a 10% to 20% error in every dose.
Always read from the top edge of the rubber gasket where it contacts the barrel wall. This is the true measurement point. If your syringe has a flat-tipped gasket (some newer designs do), the reading is the same from both edges, but always confirm which measurement standard your syringe manufacturer recommends.
Ignoring dead space waste
Over the course of a multi-dose vial, dead space waste adds up. If each injection leaves 0.5 units of solution in the needle hub, and you take one injection per week from a vial that should last 4 weeks, you lose 2 units total. That is nearly half a dose of 5 units wasted.
With larger vials containing 10 mg or more, this waste is proportionally small. With a 5 mg vial that should provide 20 doses at 0.25 mg each, losing 2 units per dose means losing 40 units over the vial lifetime, equivalent to 2 full doses. The solution is low dead space syringes or, for those comfortable with the technique, an air-lock method where a small air bubble behind the liquid pushes all the medication out of the needle.
Not accounting for reconstitution volume
If you reconstituted your own semaglutide powder with bacteriostatic water, the concentration depends entirely on how much water you added. This seems obvious, but errors happen more often than you would expect. Adding 1.1 mL of water instead of 1.0 mL to a 5 mg vial changes the concentration from 5 mg/mL to 4.55 mg/mL. At 5 units, that is the difference between 0.25 mg and 0.23 mg. Small, but it compounds over weeks of dosing.
Use our peptide reconstitution calculator to determine the exact amount of water needed for your desired concentration. And measure the water with the same precision you apply to measuring the final dose. The reconstitution step is where concentration is set. Getting it wrong means every subsequent dose is wrong too.
5 units compared to other common doses
Context helps. Knowing that 5 units equals 0.25 mg from a 5 mg/mL vial is useful. But understanding where that dose sits relative to other common doses gives you a much clearer picture of what to expect.
Units (5 mg/mL) | Dose (mg) | Phase | Typical effects |
|---|---|---|---|
5 units | 0.25 mg | Starting | Mild appetite changes, body adjusting |
10 units | 0.50 mg | Early titration | Noticeable appetite reduction |
20 units | 1.0 mg | Mid titration | Significant appetite suppression, weight loss begins |
34 units | 1.7 mg | Late titration | Strong appetite control, accelerating results |
48 units | 2.4 mg | Maintenance | Maximum therapeutic effect |
At 5 units, you are at the very beginning. Most people do not notice dramatic changes at this dose. Some report subtle decreases in food cravings or slight nausea after meals. Others feel nothing at all. Both responses are normal. The medication is building in your system, and noticeable effects typically appear as the dose increases and blood levels reach steady state.
If you want detailed breakdowns for each dose level, we have specific guides for 10 units, 20 units, 25 units, 30 units, 40 units, 50 units, and 100 units. Each covers the specific conversion math, expected effects, and dosing considerations for that unit count.
How 5 units of semaglutide compares to tirzepatide
Researchers sometimes switch between semaglutide and tirzepatide or wonder how the doses compare. The short answer is that they do not convert directly. Semaglutide and tirzepatide are different molecules with different potencies, different receptor binding profiles, and different dose-response curves.
Semaglutide at 0.25 mg is a GLP-1 receptor agonist only. Tirzepatide at its starting dose of 2.5 mg activates both GLP-1 and GIP receptors. The starting doses are not equivalent in milligrams, and they are not equivalent in effect. For anyone considering switching between the two, our conversion chart provides approximate equivalencies based on clinical response data rather than milligram-to-milligram comparison.
The semaglutide versus tirzepatide comparison is one of the most researched topics in the GLP-1 space. Both medications produce significant weight loss. Tirzepatide has shown slightly greater average weight loss in head-to-head trials. But individual response varies widely, and what works best depends on factors beyond the molecule itself.
Reconstitution and how it determines your 5-unit dose
If your semaglutide arrived as a pre-mixed liquid from a compounding pharmacy, your concentration is fixed. The pharmacist determined it during manufacturing. You just need to read the label.
But if you received lyophilized semaglutide powder and need to reconstitute it yourself, you control the concentration. This is both empowering and potentially dangerous. The amount of bacteriostatic water you add determines every dose you will draw from that vial for its entire usable life.
Reconstitution math for common vial sizes
Here is what happens when you add different amounts of water to a 5 mg vial of semaglutide powder:
Water added | Resulting concentration | 5 units equals |
|---|---|---|
1.0 mL | 5 mg/mL | 0.25 mg |
1.5 mL | 3.33 mg/mL | 0.167 mg |
2.0 mL | 2.5 mg/mL | 0.125 mg |
2.5 mL | 2 mg/mL | 0.10 mg |
5.0 mL | 1 mg/mL | 0.05 mg |
And for a 10 mg vial:
Water added | Resulting concentration | 5 units equals |
|---|---|---|
2.0 mL | 5 mg/mL | 0.25 mg |
3.0 mL | 3.33 mg/mL | 0.167 mg |
4.0 mL | 2.5 mg/mL | 0.125 mg |
The pattern is consistent. More water means lower concentration, which means less semaglutide per unit drawn. For a 10 mg vial, doubling the water from 2 mL to 4 mL cuts the dose per unit in half. Our reconstitution calculator takes the guesswork out of this process.
Getting the reconstitution right
Reconstitution errors cascade through every subsequent dose. If you add 10% too much water, every dose from that vial will be 10% too low. If you add 10% too little, every dose will be 10% too high. Over a 4-week supply, those small errors accumulate into meaningful dosing inconsistencies.
The technique matters. Direct the stream of bacteriostatic water against the wall of the vial, not directly onto the powder cake. Let the water flow gently down the glass and dissolve the powder gradually. Do not shake the vial. Swirl it gently in a circular motion until the solution is clear. Vigorous shaking can damage the peptide structure and reduce potency.
For a complete walkthrough of the reconstitution process, our semaglutide reconstitution guide covers everything from water selection to mixing technique to post-reconstitution storage.
Getting this step right is arguably more important than any subsequent dosing decision, because the concentration it establishes governs every dose you take from that vial.
Storage considerations that affect your dose accuracy
Even perfect measurement technique cannot compensate for degraded semaglutide. If the peptide in your vial has lost potency due to improper storage, drawing 5 units gives you 0.25 mg on paper but less than that in actual active compound.
Temperature requirements
Reconstituted semaglutide requires refrigeration at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). At room temperature, the peptide degrades progressively. Studies suggest that compounded semaglutide can tolerate brief excursions to room temperature (up to 86 degrees Fahrenheit or 30 degrees Celsius) for limited periods, but extended exposure accelerates degradation.
If you are wondering how long compounded semaglutide lasts in the fridge, most formulations remain stable for 28 to 42 days when properly refrigerated. Some compounding pharmacies assign longer beyond-use dates based on stability testing, but 28 days is the conservative standard.
What happens if your semaglutide gets warm? Brief exposure (a few hours) during transport is generally acceptable. Extended warmth (overnight or longer) may compromise potency. If your semaglutide arrived hot or you accidentally left it out overnight, the safest course is to contact your pharmacy about a replacement.
Vial lifespan and dose consistency
A 5 mg vial reconstituted to 5 mg/mL (1 mL of water) contains 100 units of solution. At 5 units per dose (once weekly), that vial should last 20 weeks. However, most beyond-use dating limits reconstituted semaglutide to 4-6 weeks. This creates a mismatch: the vial contains far more doses than the expiration date allows.
The practical solution is matching your vial size to your dosing schedule. If you are staying at 5 units (0.25 mg) long-term, a smaller vial might be more appropriate to minimize waste. For information on vial lifespan and shelf life, our storage guides provide detailed timelines for various formulations.
Does semaglutide change appearance as it degrades? Sometimes. Normal semaglutide solution is clear and colorless to slightly yellowish. If it turns cloudy, develops particles, or changes color significantly, discard it. These visual changes indicate degradation or contamination that no amount of careful measuring can compensate for.
What to expect after injecting 5 units of semaglutide
Expectations at the starting dose should be calibrated. Five units (0.25 mg from a 5 mg/mL vial) is not going to produce dramatic weight loss. It is not designed to. It is designed to introduce the medication to your system gradually.
First week experiences
After your first injection of 5 units, some people feel subtle changes within 24 to 48 hours. Slightly less interest in food. A vague sensation of fullness that was not there before. Perhaps some mild nausea, especially in the first day or two.
Others feel absolutely nothing. This is equally normal. Semaglutide has a half-life of approximately one week, meaning it takes about 4 to 5 weeks of weekly injections for blood levels to reach steady state. Your first week represents the very beginning of this accumulation process.
How semaglutide makes you feel varies enormously between individuals. Some people are highly sensitive to GLP-1 receptor activation and notice appetite changes even at 0.25 mg. Others require doses of 1.0 mg or higher before feeling any meaningful effect. Neither response pattern predicts long-term outcomes. The slow responders at starting doses often achieve similar results once they reach their effective dose through proper titration.
Side effects at the starting dose
The most common side effects at 0.25 mg are gastrointestinal. Nausea tops the list, followed by constipation, bloating, and occasionally dizziness. These effects are typically mild at the starting dose and often resolve within the first week or two as the body adjusts.
Fatigue is another commonly reported effect during the initial weeks. The mechanism is not fully understood, but it may relate to metabolic adjustment as the body adapts to altered glucose regulation and reduced caloric intake. For most people, the fatigue is transient and resolves as the body reaches a new equilibrium.
Less common but worth monitoring: changes in menstrual patterns, mild sleep disturbances, and sulfur burps. If any side effect at the starting dose feels severe, do not increase the dose on schedule. Stay at 5 units for an additional 2 to 4 weeks, or consult your provider about splitting the dose into two smaller injections per week.
When results actually begin
Meaningful weight loss at the starting dose is uncommon. Clinical trials show average weight loss of 1 to 2 percent of body weight during the first month at 0.25 mg. Some participants lost nothing. A few lost more. The median was modest.
The real results begin during and after titration. By the time researchers reach 1.0 to 1.7 mg, weight loss becomes clinically significant. At the 2.4 mg maintenance dose, clinical trials showed average weight loss of 15% to 17% of body weight over 68 weeks.
Understanding this timeline prevents discouragement. If you are 4 weeks in with no weight loss, that is entirely expected at the starting dose. The medication is working, building up in your system, preparing your body for the higher doses where results actually happen. Patience during the starting phase is not optional. It is part of the protocol.
Injection technique for small doses
Injecting 5 units follows the same basic technique as any subcutaneous injection. But the small volume introduces a few considerations worth addressing.
Choosing the injection site
The standard injection sites for subcutaneous semaglutide are the abdomen (at least 2 inches from the navel), the front of the thigh, and the upper arm. All three sites provide adequate subcutaneous tissue for proper absorption. Our guide on the best injection site for semaglutide compares absorption rates and comfort levels across all three locations.
At 5 units, you are injecting just 0.05 mL of liquid. This tiny volume absorbs quickly regardless of site. Some researchers prefer the abdomen for its larger subcutaneous tissue area and easier access. Others prefer the thigh because they can see the injection site more clearly. There is no evidence that injection site significantly affects efficacy at any dose level.
Rotate injection sites between doses. Even though 0.05 mL causes minimal tissue disruption, consistent injection in the exact same spot can lead to lipodystrophy over time, small changes in the fat tissue that may affect absorption. Pick a different spot within the same general area each week. For guidance on GLP-1 injection technique and site rotation patterns, our injection guides cover the details.
Timing your injection
Semaglutide is a once-weekly injection. The best time to inject is whenever you will remember to do it consistently. Pick a day and approximate time, then stick with it.
Some researchers find that injecting in the evening reduces nausea because they sleep through the initial hours when GI effects are most likely. Others inject in the morning to align with their routine. At the 5-unit starting dose, timing matters less than consistency. The medication has a 7-day half-life, so the exact hour of injection has minimal impact on blood levels between doses.
What happens if you take your dose a day early or a day late? At 5 units, the impact is negligible. The starting dose produces such low blood levels that a 24-hour shift in timing barely affects the pharmacokinetics. Just get back on your regular schedule the following week.
Enhancing your semaglutide protocol at 5 units
While the starting dose does its work building up in your system, you can optimize other factors that influence results. These complementary strategies do not replace proper titration, but they set the foundation for better outcomes once you reach effective doses.
Nutrition at the starting dose
Even at 0.25 mg, many people notice subtle changes in food preferences or appetite patterns. Leaning into these changes rather than fighting them can amplify the early benefits. Our guide to foods while on semaglutide covers specific food choices that work with the medication rather than against it.
High-protein meals become more important once you start any GLP-1 agonist. Semaglutide can reduce total caloric intake, and without adequate protein, the body may lose muscle mass along with fat. Aim for at least 0.7 to 1.0 grams of protein per pound of lean body mass. This applies even at the starting dose, because the dietary habits you build now carry forward through your entire protocol.
Foods to avoid on semaglutide include high-fat meals that worsen nausea, highly processed carbohydrates that spike blood sugar, and large portion sizes that overwhelm slowed gastric emptying. Our semaglutide diet plan and best foods guide provide specific meal frameworks designed for GLP-1 users. Some researchers also find GLP-1-friendly breakfast ideas particularly helpful during the adjustment period.
Supplements that complement semaglutide
Several supplements can support your semaglutide protocol from the very beginning. B12 supplementation addresses potential absorption changes that GLP-1 agonists can cause. Glycine supports gut health and may help with sleep quality. Probiotics can help maintain gut microbiome balance during the metabolic shift.
Some compounded semaglutide formulations include these additives pre-mixed. Semaglutide with methylcobalamin (active B12) is one of the most popular combination formulations. Glycine and B12 blends combine multiple supportive compounds in a single vial. L-carnitine combinations target fat oxidation alongside appetite reduction. And niacinamide blends support cellular energy metabolism during caloric restriction.
Whether these additions provide meaningful benefit at the 5-unit starting dose is debatable. The base semaglutide dose is doing very little clinically at 0.25 mg, and the additive effects of supplements are similarly modest at this level. The real value of starting supplements early is establishing the habit so they are already part of your routine when you reach doses where they matter more.
Exercise and activity
Can you lose weight on semaglutide without exercise? Yes. The clinical trials demonstrated significant weight loss without mandated exercise programs. But adding exercise, even at the starting dose, improves outcomes in multiple ways. It preserves muscle mass during weight loss. It improves insulin sensitivity independently of semaglutide. And it establishes movement habits before higher doses potentially reduce energy and appetite to the point where starting an exercise routine feels harder.
Resistance training is particularly valuable during any GLP-1 protocol. The appetite-suppressing effects of semaglutide can lead to inadvertently low protein intake, which combined with caloric deficit puts muscle mass at risk. Resistance training signals the body to preserve muscle even during weight loss, and starting while you are still at the 5-unit dose (when energy levels are most normal) is easier than starting later at higher doses.
Pharmacy and sourcing considerations
Where your semaglutide comes from affects what 5 units actually delivers. Not all compounded semaglutide is created equal, and the sourcing decision has real implications for dosing accuracy.
Compounding pharmacy quality
Compounded semaglutide is not FDA-approved. Each compounding pharmacy produces its own formulation, and quality varies. Reputable pharmacies test their products for potency, sterility, and endotoxin levels. Less reputable operations may skip these quality checks, resulting in vials where the labeled concentration does not match the actual concentration.
If your vial says 5 mg/mL but actually contains 4 mg/mL, your 5-unit dose delivers 0.20 mg instead of 0.25 mg. You would never know from the syringe reading alone. This is why sourcing from a 503B outsourcing facility matters. These facilities operate under stricter regulatory oversight and are required to test their products more rigorously than traditional 503A pharmacies.
Several compounding pharmacies have established strong reputations in the GLP-1 space. Our reviews of Empower Pharmacy, Olympia Pharmacy, Belmar Pharmacy, and BPI Labs cover the sourcing options in detail.
Pre-filled pens versus vials
Brand-name semaglutide products like Ozempic and Wegovy come in pre-filled pens with fixed dose settings. These pens do not use the unit system described in this article. Instead, they deliver precise pre-measured doses selected by clicking a dial. Five units on an insulin syringe is not the same as any setting on an Ozempic pen.
If you are using a pre-filled pen, the unit conversion math in this guide does not apply to you. The pen handles dosing internally. For researchers wondering about the relationship between these delivery systems, our guide on GLP-1 versus Ozempic clarifies the terminology and product differences.
The unit conversion information in this article applies specifically to compounded semaglutide drawn from multi-dose vials using insulin syringes. This is the most common format for researchers using compounded formulations, and the format where understanding your concentration and doing the math correctly matters most.
Long-term planning beyond the starting dose
Five units is where you begin. But planning ahead helps you navigate the months of treatment that follow. Understanding what comes after the starting dose prepares you for a smoother journey.
How long to stay on semaglutide
Clinical evidence suggests that semaglutide benefits continue as long as you take the medication. Studies show that long-term semaglutide use maintains weight loss, while discontinuation leads to regain for most people within 12 months.
This creates important planning considerations. If you start at 5 units and titrate to a maintenance dose, how long do you plan to continue? What happens when you want to stop? Our guide on semaglutide withdrawal symptoms covers what to expect when discontinuing, and stopping cold turkey versus tapering produces very different experiences.
Some researchers find success with a maintenance protocol that uses lower doses long-term. After reaching target weight at higher doses, they taper back down, sometimes returning to the starting dose of 5 units as a maintenance dose. This approach uses less medication while potentially maintaining metabolic benefits. The evidence is still emerging, but the concept of dose reduction for maintenance rather than complete discontinuation shows promise.
Dealing with plateaus
Weight loss plateaus on semaglutide are common and expected. They typically occur at transition points between dose increases or after the initial rapid weight loss phase. If you have been at the same dose for more than 4 to 6 weeks without progress and have not yet reached the maximum dose, the standard response is to titrate upward.
Our semaglutide plateau guide covers the full range of strategies for breaking through stalls. Dose increases, dietary adjustments, exercise modifications, and supplement additions can all play a role. For people who have hit a wall with weight loss, understanding why it happens is the first step toward fixing it.
Considering alternatives
Not everyone responds optimally to semaglutide. Some researchers find better results with tirzepatide, which activates both GLP-1 and GIP receptors for potentially greater weight loss. Others explore retatrutide, the triple agonist that adds glucagon receptor activation to the mix. Our three-way comparison breaks down the differences in detail.
The question of whether tirzepatide works if semaglutide does not comes up frequently. The answer is often yes, because the dual receptor mechanism provides additional pathways for appetite suppression and metabolic improvement. But the decision to switch should be made after giving semaglutide a fair trial at adequate doses, not based on the starting dose experience alone.
For researchers serious about optimizing their peptide protocols, SeekPeptides provides the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact dosing questions. Whether you are just starting at 5 units or planning your titration strategy months ahead, SeekPeptides members access detailed calculators, concentration-specific charts, and expert-reviewed protocols that take the uncertainty out of every dose.
Safety considerations at the 5-unit dose
The starting dose is the safest dose. By design. But "safest" does not mean "zero risk." Understanding what to watch for, even at 5 units, helps you respond appropriately if something unexpected occurs.
Contraindications
Semaglutide is contraindicated in individuals with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). This applies at all doses, including the starting dose. The medication is also contraindicated in individuals with known hypersensitivity to semaglutide or any component of the formulation.
Certain medications may interact with semaglutide. If you are taking oral medications that require precise absorption timing, semaglutide delayed gastric emptying can affect their bioavailability. Discuss your full medication list with your provider before starting, even at the low 5-unit dose. Our guide on combining semaglutide with other medications covers some of the most common interaction questions.
Monitoring during the starting phase
At the starting dose, most providers recommend basic monitoring. Track your weight weekly (same time, same conditions). Note any side effects and their severity. Keep a simple food log if possible, as it helps identify patterns between eating habits and side effects.
Some providers order baseline bloodwork before starting semaglutide and repeat it at 3 and 6 months. Common panels include fasting glucose, HbA1c, lipid panel, liver function, and kidney function. Semaglutide can affect several metabolic markers, and tracking these changes helps assess both safety and efficacy over time. If you are curious whether semaglutide shows up in blood work, our guide explains what standard panels will and will not detect.
When to contact your provider
At the 5-unit starting dose, most side effects are mild and self-limiting. However, certain symptoms warrant immediate medical attention at any dose. Severe abdominal pain that does not resolve (possible pancreatitis). Signs of allergic reaction including swelling, difficulty breathing, or widespread rash. Symptoms of blood clots or severe kidney-related symptoms. Gallbladder symptoms including right upper quadrant pain, especially after eating fatty foods.
Do not wait to see if serious symptoms resolve on their own. GLP-1 agonists affect multiple body systems, and while serious adverse events at the starting dose are rare, they are not impossible. Better to contact your provider unnecessarily than to ignore a signal that needed attention.
Alcohol and lifestyle interactions at the starting dose
Lifestyle factors interact with semaglutide in ways worth understanding before you begin. Even at the starting dose, some interactions matter.
Alcohol and semaglutide have a complicated relationship. Many people report dramatically reduced alcohol tolerance after starting GLP-1 agonists. Even at the 0.25 mg starting dose, some researchers notice that one drink feels like two or three. This may relate to altered gastric emptying, changes in liver metabolism, or direct effects on reward pathways in the brain.
The practical advice is straightforward. If you drink alcohol, reduce your intake during the initial adjustment period and pay close attention to how your body responds. The combination of slowed gastric emptying, potential nausea, and reduced alcohol tolerance can make even moderate drinking uncomfortable at best and potentially risky at worst.
Travel with semaglutide requires some planning. You need to maintain the cold chain for your vial, which means a small cooler or insulated pouch for transport. Our travel guide for semaglutide covers TSA regulations, temperature management, and tips for maintaining your injection schedule across time zones.
Frequently asked questions
Is 5 units of semaglutide a lot?
No. Five units from a 5 mg/mL vial equals 0.25 mg, which is the standard starting dose. It is the lowest dose in the recommended titration schedule. Most people need to increase to higher doses over time for full therapeutic benefit. For perspective, 20 units (1.0 mg) is still considered a moderate dose, and the maintenance dose of 2.4 mg requires 48 units from the same vial.
Can I take 5 units of semaglutide twice a week?
Some protocols do involve splitting semaglutide doses into two smaller injections per week rather than one larger weekly dose. At 5 units twice weekly from a 5 mg/mL vial, you would be getting 0.50 mg per week total, equivalent to a single 10-unit weekly dose. This approach may reduce side effects for some people by maintaining more stable blood levels. Discuss with your provider before altering the standard once-weekly schedule.
How long will a vial last at 5 units per week?
A 5 mg vial reconstituted to 1 mL (5 mg/mL) contains 100 units total. At 5 units per week, the vial contains enough solution for 20 weekly doses. However, most compounded semaglutide has a beyond-use date of 28 to 42 days after reconstitution, meaning you should use it within 4 to 6 weeks regardless of remaining volume. Check your vial expiration date and plan accordingly.
What if I accidentally inject more than 5 units?
Accidentally injecting 6, 7, or even 10 units when you intended 5 is unlikely to cause serious harm at these low doses. You would be getting 0.30, 0.35, or 0.50 mg instead of 0.25 mg, all still within the lower end of the therapeutic range. You might experience slightly more nausea than usual. Do not take an additional dose to "compensate" or skip your next scheduled dose. Simply resume your normal 5-unit dose at the next scheduled injection and mention the error to your provider.
Does the brand of semaglutide affect the 5-unit conversion?
Pre-filled brand-name pens (Ozempic, Wegovy) do not use the unit system discussed here. For compounded semaglutide from vials, the brand or pharmacy does not change the math. Five units always equals 0.05 mL of liquid, and the milligram dose always depends on concentration. As long as you know your vial concentration, the conversion formula applies universally regardless of source.
Should I worry about the needle size when drawing 5 units?
Needle gauge (thickness) does not affect dosing accuracy. A 29-gauge, 30-gauge, or 31-gauge needle draws the same volume at 5 units. Thinner needles (higher gauge numbers) cause less injection discomfort. For the small 0.05 mL volume at 5 units, a 31-gauge needle provides the most comfortable experience with no loss of accuracy. The injection site and depth matter more than needle gauge for proper absorption.
Can I combine semaglutide with other peptides at the starting dose?
Many researchers combine semaglutide with other compounds. Berberine with semaglutide, phentermine with semaglutide, and semaglutide with tirzepatide are among the most common combinations discussed. Starting any combination at the lowest effective dose of each compound is standard practice. Do not combine multiple GLP-1 agonists without specific guidance from your provider, as the overlapping receptor activity can amplify side effects unpredictably.
What happens if my semaglutide vial has no concentration label?
Do not inject from a vial without a clear concentration label. Contact your pharmacy immediately for clarification. Without knowing the concentration, the 5-unit conversion could represent any dose from 0.05 mg to 0.25 mg or higher. Guessing is not acceptable when it comes to injectable medications. A quick phone call to your pharmacy resolves the question in minutes.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your conversions stay accurate, your concentrations stay verified, and your starting dose stay exactly where you intended it.