Mar 5, 2026

Some people draw up exactly 30 units of semaglutide every week and get perfect results. Others draw up the same 30 units, from a different vial, and end up on five times the dose they intended. Same number on the syringe. Wildly different outcomes. The difference is concentration, and it is the single most important variable that separates a safe, effective compounded semaglutide protocol from a dangerous dosing error.
Here is the short answer. At a 5 mg/mL concentration, 30 units equals 1.5 mg of semaglutide. At 2.5 mg/mL, those same 30 units equal only 0.75 mg. At 1 mg/mL, you are looking at just 0.3 mg. The number on your syringe tells you volume. It tells you nothing about the actual medication dose unless you know the concentration of the vial you are drawing from.
That distinction has caused real harm.
The FDA has documented cases where patients injected several times their intended dose because they assumed units and milligrams were interchangeable. They are not. And if you are reading this because you have a semaglutide vial measured in units and a prescription written in milligrams, you are already asking the right question. This guide will walk you through the complete math, cover every common concentration, provide reference charts you can bookmark, and explain the safety principles that prevent dosing mistakes. Whether you are on your first week or adjusting after months of treatment, the conversion process works the same way every single time.
Understanding the relationship between units, milliliters, and milligrams
Before touching the math, you need to understand what each measurement actually means. Units, milliliters, and milligrams measure three completely different things. Confusing them is where nearly every semaglutide dosing error begins.
Units measure volume on an insulin syringe. A standard insulin syringe holds 100 units total, which equals exactly 1 mL. So 30 units equals 0.3 mL of liquid. Always. Regardless of what medication is inside.
Milliliters (mL) also measure volume. The conversion between units and milliliters never changes. Divide units by 100 and you get milliliters. Thirty divided by 100 equals 0.3 mL. Simple.
Milligrams (mg) measure the actual amount of medication dissolved in that liquid. This is the number that determines your therapeutic dose. And this is where concentration enters the picture. A 5 mg/mL vial has five milligrams of semaglutide dissolved in every milliliter of solution. A 2 mg/mL vial has only two milligrams per milliliter. Same volume. Very different doses.
Think of it like coffee. A small cup of espresso and a small cup of weak drip coffee are the same volume. But the espresso contains far more caffeine per sip. Concentration is the caffeine equivalent in this analogy, and it changes everything about what 30 units actually delivers to your body.
The semaglutide dosage calculator on SeekPeptides automates this entire conversion. But understanding the manual math protects you from errors that no calculator can prevent if you enter the wrong concentration.
The conversion formula you need to memorize
One formula handles every semaglutide unit-to-mg conversion you will ever encounter. Learn it once and you never need to guess again.
Step 1: Convert units to milliliters.
Units divided by 100 equals milliliters. For 30 units: 30 / 100 = 0.3 mL.
Step 2: Multiply milliliters by concentration.
Milliliters multiplied by concentration (mg/mL) equals milligrams. For a 5 mg/mL vial: 0.3 mL x 5 mg/mL = 1.5 mg.
That is the entire formula. Two steps. No ambiguity.
You can also combine both steps into a single equation: (Units / 100) x Concentration = Dose in mg. For 30 units at 5 mg/mL: (30 / 100) x 5 = 1.5 mg. Memorize this formula and you can convert any unit measurement to milligrams for any semaglutide concentration in seconds.
The reverse formula works just as smoothly when your provider prescribes in milligrams and you need units. Dose in mg divided by concentration, then multiplied by 100, gives you units. For a 1.5 mg dose at 5 mg/mL: (1.5 / 5) x 100 = 30 units. Same numbers, same answer, opposite direction.
30 units of semaglutide converted for every common concentration
Compounding pharmacies prepare semaglutide in several standard concentrations. The concentration is always printed on the vial label, typically expressed as mg/mL. Here is what 30 units delivers at each one.
At 1 mg/mL concentration
Thirty units at 1 mg/mL equals 0.3 mg of semaglutide. This is below the standard starting dose for most weight management protocols. The typical starting dose is 0.25 mg per week, which would be 25 units at this concentration. If your provider prescribed 30 units from a 1 mg/mL vial, you are getting a slightly higher starting dose of 0.3 mg, which some clinics use as their initial titration point.
Math: (30 / 100) x 1 = 0.3 mg.
At 2 mg/mL concentration
Thirty units at 2 mg/mL equals 0.6 mg of semaglutide. This falls within the second phase of the standard dose escalation schedule. After four weeks at 0.25 mg, most protocols increase to 0.5 mg for another four weeks before moving to higher therapeutic doses. At 0.6 mg, you are slightly above the 0.5 mg tier but well below the 1 mg mark.
Math: (30 / 100) x 2 = 0.6 mg.
At 2.5 mg/mL concentration
Thirty units at 2.5 mg/mL equals 0.75 mg of semaglutide. This is a common maintenance dose for people who respond well to moderate levels and do not need to escalate further. Many researchers find their appetite suppression plateau around this range, making it a practical long-term target. The appetite suppression effects at 0.75 mg are substantial for most individuals.
Math: (30 / 100) x 2.5 = 0.75 mg.
At 3 mg/mL concentration
Thirty units at 3 mg/mL equals 0.9 mg of semaglutide. This sits just below the 1 mg threshold, which represents a meaningful escalation point in most dosing protocols. Some providers use 3 mg/mL vials specifically because they allow fine-grained dose adjustments between the 0.5 mg and 1 mg tiers without changing vials. If you are experiencing side effects at higher doses, staying at 0.9 mg can provide strong efficacy with better tolerability.
Math: (30 / 100) x 3 = 0.9 mg.
At 5 mg/mL concentration
Thirty units at 5 mg/mL equals 1.5 mg of semaglutide. This is a mid-to-high therapeutic dose. The standard protocol reaches 1.7 mg and eventually 2.4 mg for full weight management dosing. At 1.5 mg, you are past the initial titration phases and into territory where significant weight loss results typically become visible. The 5 mg/mL concentration is the most common from compounding pharmacies because its math is clean and predictable.
Math: (30 / 100) x 5 = 1.5 mg.
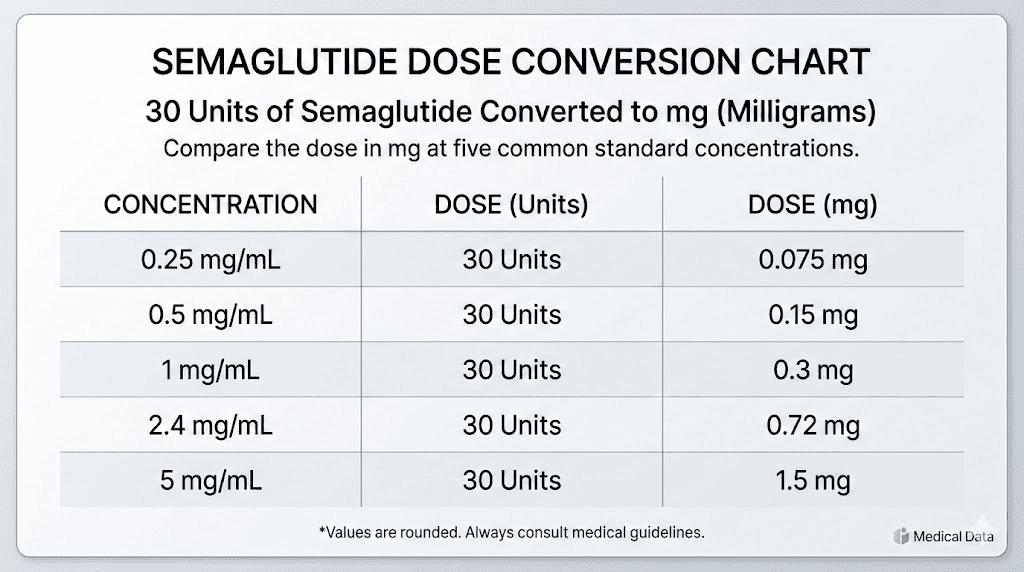
Complete conversion reference table
Bookmark this table. It covers 30 units alongside other common unit measurements at every standard concentration, so you have a single reference for all your semaglutide unit conversions.
Units | mL | 1 mg/mL | 2 mg/mL | 2.5 mg/mL | 3 mg/mL | 5 mg/mL |
|---|---|---|---|---|---|---|
5 | 0.05 | 0.05 mg | 0.10 mg | 0.125 mg | 0.15 mg | 0.25 mg |
10 | 0.10 | 0.10 mg | 0.20 mg | 0.25 mg | 0.30 mg | 0.50 mg |
15 | 0.15 | 0.15 mg | 0.30 mg | 0.375 mg | 0.45 mg | 0.75 mg |
20 | 0.20 | 0.20 mg | 0.40 mg | 0.50 mg | 0.60 mg | 1.00 mg |
25 | 0.25 | 0.25 mg | 0.50 mg | 0.625 mg | 0.75 mg | 1.25 mg |
30 | 0.30 | 0.30 mg | 0.60 mg | 0.75 mg | 0.90 mg | 1.50 mg |
35 | 0.35 | 0.35 mg | 0.70 mg | 0.875 mg | 1.05 mg | 1.75 mg |
40 | 0.40 | 0.40 mg | 0.80 mg | 1.00 mg | 1.20 mg | 2.00 mg |
50 | 0.50 | 0.50 mg | 1.00 mg | 1.25 mg | 1.50 mg | 2.50 mg |
60 | 0.60 | 0.60 mg | 1.20 mg | 1.50 mg | 1.80 mg | 3.00 mg |
80 | 0.80 | 0.80 mg | 1.60 mg | 2.00 mg | 2.40 mg | 4.00 mg |
100 | 1.00 | 1.00 mg | 2.00 mg | 2.50 mg | 3.00 mg | 5.00 mg |
The 30-unit row is bolded for quick reference. Notice how the milligram value changes dramatically across concentrations. At 1 mg/mL, 30 units is a conservative starting dose. At 5 mg/mL, those same 30 units represent a dose that most people do not reach until week 12 or later in their treatment timeline.
For reference tables covering other specific unit values, see our guides on 10 units of semaglutide, 20 units, 40 units, 50 units, and 100 units.
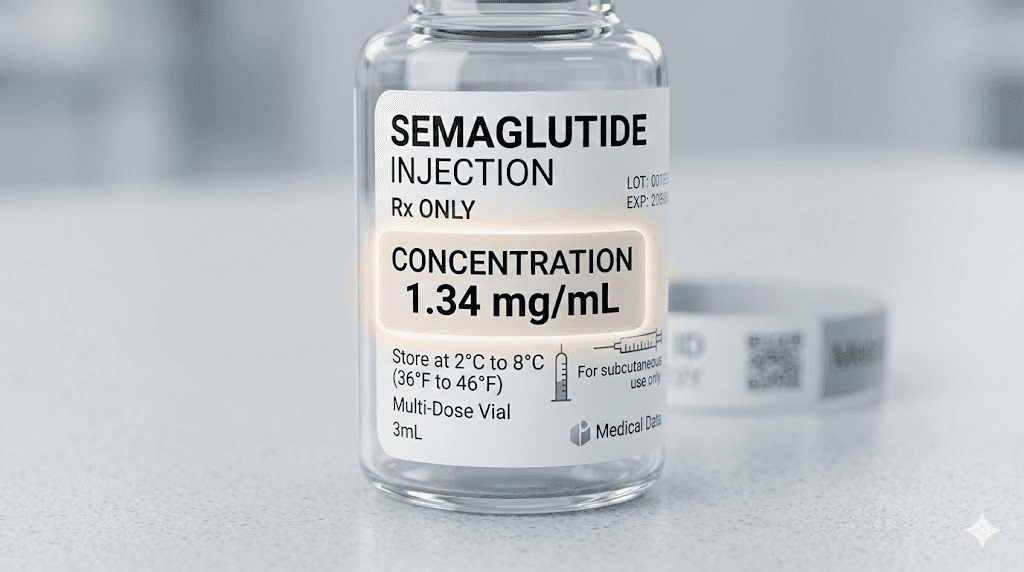
How to identify your vial concentration
The concentration is printed on the vial label. Every single time. But knowing where to look and how to read it prevents a surprising number of mistakes.
Reading compounding pharmacy labels
Compounded semaglutide labels vary by pharmacy, but they all include the concentration. Look for a number followed by mg/mL. Common formats include:
Semaglutide 5 mg/mL
Semaglutide 5mg/1mL
Semaglutide 25mg/5mL (this means 5 mg/mL, just expressed differently)
Semaglutide 2.5mg/mL
Some pharmacies also list the total content of the vial. A label reading "Semaglutide 25 mg / 5 mL" means the vial contains 25 mg total in 5 mL of solution, which works out to 5 mg per mL. Do not confuse the total vial content with the concentration per milliliter. That mistake turns a 1.5 mg dose into a 7.5 mg dose, and the consequences are severe.
If you receive vials from pharmacies like Empower Pharmacy or Olympia Pharmacy, each has slightly different label formats. Always verify the mg/mL concentration before your first draw.
Lyophilized powder vials
If you received a lyophilized (freeze-dried) semaglutide vial, the concentration depends on how much bacteriostatic water you add during reconstitution. A 5 mg vial reconstituted with 1 mL of bacteriostatic water creates a 5 mg/mL solution. The same 5 mg vial reconstituted with 2 mL creates a 2.5 mg/mL solution. You control the concentration through your reconstitution ratio.
For a 10 mg vial, adding 2 mL of bacteriostatic water gives you 5 mg/mL. Adding 4 mL gives you 2.5 mg/mL. The choice depends on your target dose and how many injections you want per vial. Higher concentrations mean smaller injection volumes but fewer total doses per vial. Lower concentrations mean larger injection volumes but more precise dose adjustments and more doses per vial.
Always write down the concentration you created during reconstitution. Label the vial immediately. Relying on memory weeks later is how errors happen.
Why 30 units is a common dosing point
Thirty units appears frequently in semaglutide protocols for several practical reasons. Understanding why helps you contextualize your own dosing and recognize whether your conversion makes clinical sense.
The 5 mg/mL sweet spot
At the most common compounded concentration of 5 mg/mL, 30 units delivers 1.5 mg per week. This dose sits in the middle of the standard escalation schedule. Most protocols begin at 0.25 mg for four weeks, increase to 0.5 mg for four weeks, then move to 1.0 mg, 1.7 mg, and eventually 2.4 mg. The 1.5 mg dose falls between the 1.0 mg and 1.7 mg tiers, making it a natural stopping point for people who respond well without needing full escalation.
Research consistently shows that significant appetite suppression and weight reduction occur at doses between 1.0 mg and 1.7 mg for most individuals. If you are experiencing strong appetite suppression at 1.5 mg with manageable side effects, many providers will keep you at this level rather than pushing higher.
The dose escalation bridge
Some providers prescribe 30 units at 5 mg/mL (1.5 mg) as a transitional dose between 1.0 mg and 1.7 mg. Instead of jumping directly from 1.0 mg to 1.7 mg, which represents a 70% increase, they insert a 1.5 mg step to reduce the risk of gastrointestinal side effects. This slower escalation approach often produces better tolerability and compliance than aggressive dose increases.
Lower concentration starting doses
At 1 mg/mL, 30 units delivers 0.3 mg, which some clinics use as their standard first dose. This is slightly above the typical 0.25 mg starting point but still conservative enough for initial titration. Clinics that compound at 1 mg/mL often prefer 30 units because the slightly higher starting dose can produce noticeable appetite changes earlier, helping with patient motivation during the first month.
At 2 mg/mL, 30 units gives 0.6 mg, which mirrors the second dose tier in most escalation protocols. This makes 30 units a convenient preset for patients transitioning from their initial four-week loading phase.
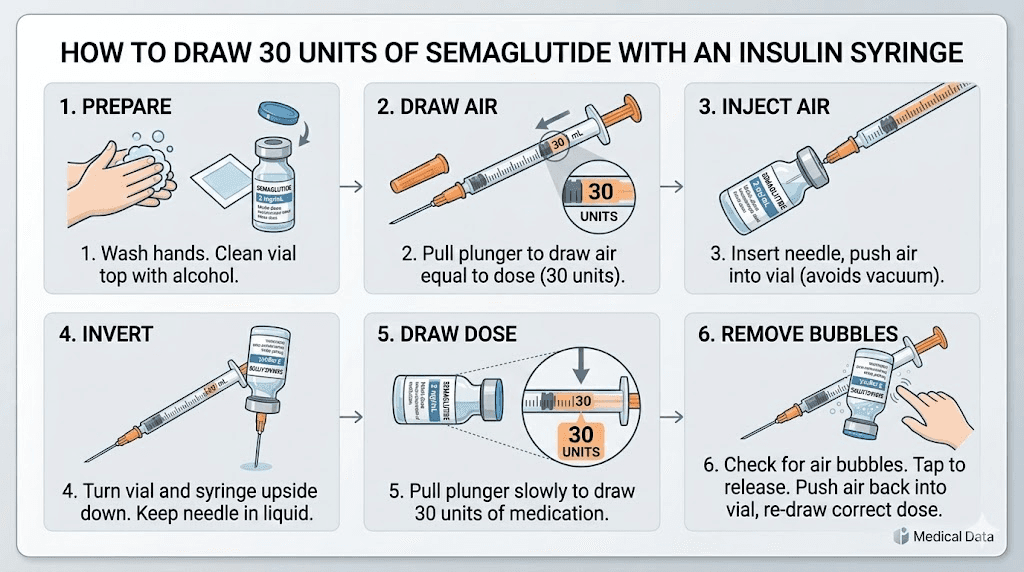
Step-by-step guide to drawing 30 units accurately
Getting the math right means nothing if you draw the wrong amount from the vial. The physical process of measuring 30 units on an insulin syringe requires attention to detail, especially with smaller syringes where graduation marks are close together.
Choosing the right syringe
Insulin syringes come in three common sizes: 30 units (0.3 mL), 50 units (0.5 mL), and 100 units (1 mL). For a 30-unit dose, you have options.
A 30-unit syringe fills completely to the top for a 30-unit dose. Each graduation mark represents 0.5 units, giving you extremely fine measurement precision. But drawing to the maximum capacity leaves zero room for air bubble adjustment. If you cannot fully eliminate air bubbles, your actual dose will be slightly less than 30 units.
A 50-unit syringe is often the best choice for 30 units. It provides enough space above your target line to manage air bubbles while still offering graduation marks at every 1 unit for precise measurement. You draw to the 30-unit line, which sits at 60% of the syringe capacity.
A 100-unit syringe works but offers less precision. Graduation marks typically appear every 2 units, making it harder to land exactly on 30. If 30 falls between two marks, you are estimating. For accurate semaglutide injection, a 50-unit syringe at 30 units is the ideal combination.
The drawing process
Clean the vial stopper with an alcohol swab. Let it dry completely. Pull back the syringe plunger to the 30-unit mark, filling the syringe with air. Insert the needle through the vial stopper. Push the air into the vial. This equalizes pressure and makes drawing easier.
Invert the vial so the stopper faces down. Pull the plunger back slowly past the 30-unit mark to about 35 units. Check for air bubbles. Tap the syringe barrel firmly with your finger to move bubbles toward the needle end. Push the plunger forward to expel the air and excess liquid until you reach exactly 30 units.
Hold the syringe at eye level to confirm the plunger edge aligns with the 30-unit graduation mark. The bottom edge of the plunger, not the middle or top, should sit squarely on the line. Remove the needle from the vial. You are ready to inject at your chosen site.
Where 30 units falls in standard dosing schedules
Knowing the milligram equivalent of 30 units is only half the picture. Understanding where that dose sits in the broader treatment timeline helps you evaluate whether your protocol is progressing appropriately.
Standard dose escalation schedule
The clinical dose escalation for semaglutide in weight management follows a structured pattern. Each dose tier lasts four weeks before the next increase.
Week | Target dose | Units at 5 mg/mL | Units at 2.5 mg/mL | Units at 2 mg/mL |
|---|---|---|---|---|
1-4 | 0.25 mg | 5 units | 10 units | 12.5 units |
5-8 | 0.5 mg | 10 units | 20 units | 25 units |
9-12 | 1.0 mg | 20 units | 40 units | 50 units |
13-16 | 1.7 mg | 34 units | 68 units | 85 units |
17+ | 2.4 mg | 48 units | 96 units | N/A |
At 5 mg/mL, 30 units (1.5 mg) falls between the week 9-12 tier and the week 13-16 tier. This is exactly where many providers insert an intermediate step. Rather than jumping from 20 units (1.0 mg) directly to 34 units (1.7 mg), they prescribe 30 units (1.5 mg) for two to four weeks as a bridge dose. This approach reduces the incidence of fatigue, dizziness, and gastrointestinal distress that commonly accompanies large dose jumps.
At 2.5 mg/mL, 30 units delivers 0.75 mg, which sits between the 0.5 mg and 1.0 mg tiers. Again, it serves as a bridge dose. At 2 mg/mL, 30 units gives 0.6 mg, just above the 0.5 mg starting tier, suitable for the early weeks of escalation.
Maintenance dosing at 30 units
Not everyone needs to reach the maximum 2.4 mg dose. Clinical data shows that a substantial percentage of patients achieve their target weight and maintain it at lower doses. If you have reached your weight loss goals at 30 units (1.5 mg from a 5 mg/mL vial), your provider may keep you at this level indefinitely. Maintenance dosing prioritizes the lowest effective dose, which minimizes side effects while sustaining results.
The question of how long to stay on semaglutide becomes especially relevant at maintenance doses. Many researchers and patients stay at moderate doses like 1.5 mg for months or even years with continued benefit. The withdrawal effects that some people experience when stopping semaglutide entirely make gradual, sustained dosing the preferred approach for most providers.
Common mistakes when converting 30 units to milligrams
Even with the formula memorized, specific errors repeat themselves across the semaglutide community. Knowing what to watch for is as important as knowing the math.
Mistake 1: assuming all vials are the same concentration
This is the most dangerous error. If you previously used a 2.5 mg/mL vial and your pharmacy switches you to a 5 mg/mL vial without clear communication, your 30 units goes from 0.75 mg to 1.5 mg overnight. That doubles your dose. Symptoms of overdosing include severe nausea, vomiting, and in extreme cases, dangerous gastrointestinal complications.
Every time you receive a new vial, check the concentration. Every time. Even if you order from the same pharmacy. Compounding pharmacies occasionally change formulations, and the label is your only safeguard.
Mistake 2: confusing total vial content with concentration
A vial labeled "Semaglutide 10 mg / 2 mL" contains 10 mg total in 2 mL of solution. The concentration is 5 mg/mL. If you mistakenly use 10 as your concentration in the formula, you calculate 30 units as 3.0 mg instead of the actual 1.5 mg. That is double the intended dose.
Always convert the label information to mg per mL before calculating. Total content divided by total volume gives you the concentration. 10 mg / 2 mL = 5 mg/mL.
Mistake 3: using the wrong syringe scale
Some syringes are marked in mL rather than units. A 1 mL syringe marked in 0.01 mL increments looks very different from a 100-unit insulin syringe. Drawing to the 0.30 mL line on a milliliter syringe gives you the correct volume for 30 units. But if you accidentally draw to 0.30 on a syringe that measures something else entirely, your dose is wrong.
Stick with standard insulin syringes for semaglutide injections. They are calibrated specifically for subcutaneous peptide injection and their unit markings eliminate the need for volume-to-unit mental math.
Mistake 4: not accounting for air bubbles
Air bubbles in the syringe reduce your actual dose. If you draw 30 units but 2 units worth of space is occupied by an air bubble, you are injecting 28 units of medication. Over time, small air bubble losses compound, and the last few doses from a vial contain more concentrated medication than expected. Remove all visible air bubbles before every injection.
How 30 units compares to other common unit doses
Placing 30 units in context with other frequently prescribed doses helps you understand the relative intensity of your protocol and what to expect as you move between dose tiers.
30 units vs 20 units
At 5 mg/mL, 20 units delivers 1.0 mg while 30 units delivers 1.5 mg. That is a 50% dose increase. If your provider moves you from 20 to 30 units, expect noticeably stronger appetite suppression within the first week. Side effects like mild nausea may briefly return or intensify before your body adjusts over 7 to 14 days.
The jump from 20 to 30 units at 5 mg/mL is one of the more substantial single-step increases in most protocols. If you have been tolerating 20 units well, the transition usually goes smoothly. But if you experienced significant side effects at 20 units, your provider might add an intermediate step at 25 units (1.25 mg) before reaching 30.
30 units vs 40 units
At 5 mg/mL, 40 units delivers 2.0 mg while 30 units delivers 1.5 mg. Moving from 30 to 40 represents a 33% increase. This step brings you close to the maximum maintenance dose of 2.4 mg (48 units at 5 mg/mL). Many people find that the difference between 1.5 mg and 2.0 mg is where diminishing returns begin, meaning the additional appetite suppression is modest compared to the potential increase in side effects.
30 units vs 50 units
At 5 mg/mL, 50 units equals 2.5 mg, which exceeds the standard maximum dose of 2.4 mg. Very few protocols call for 50 units at 5 mg/mL. The contrast with 30 units is dramatic: 2.5 mg versus 1.5 mg, a 67% increase. If you are currently at 30 units and your provider suggests jumping to 50, ask about intermediate steps. Such large increases strain the gastrointestinal system and often cause more problems than they solve.
30 units in the broader landscape
The question of whether any particular unit dose is too much depends entirely on concentration. Thirty units at 1 mg/mL (0.3 mg) is a gentle starting dose. Thirty units at 5 mg/mL (1.5 mg) is a moderate therapeutic dose. Thirty units from a theoretical 10 mg/mL concentration would deliver 3.0 mg, which exceeds the standard maximum. The unit number alone is meaningless without concentration context.
What to do if your dose changes but your units stay at 30
Sometimes providers change your vial concentration rather than your unit measurement. This happens when you switch pharmacies, when your pharmacy changes suppliers, or when a different concentration becomes available at a better price. If your units stay at 30 but your concentration changes, your actual dose changes too.
Scenario: moving from 2.5 mg/mL to 5 mg/mL
If you were drawing 30 units from a 2.5 mg/mL vial (0.75 mg) and receive a new 5 mg/mL vial, drawing the same 30 units now gives you 1.5 mg. Your dose just doubled. Your provider should reduce your unit measurement to 15 units to maintain the same 0.75 mg dose. Always confirm new unit measurements whenever your concentration changes.
Scenario: moving from 5 mg/mL to 3 mg/mL
If you were drawing 30 units from a 5 mg/mL vial (1.5 mg) and receive a 3 mg/mL vial, those same 30 units now deliver only 0.9 mg. Your dose dropped by 40%. To maintain 1.5 mg from a 3 mg/mL vial, you need 50 units. This kind of change often catches people off guard, leading to unexpected plateaus or mild withdrawal symptoms as the effective dose drops without their knowledge.
The golden rule
Any time your vial changes, recalculate. Use the formula. Use the semaglutide dosage calculator. Confirm with your provider. Do not assume that the same number of units means the same dose. It almost never does across different concentrations.
Semaglutide concentration and vial sizes from major compounding pharmacies
Different compounding pharmacies favor different concentrations. Knowing what to expect from the most common sources helps you prepare for the conversion before your vial even arrives.
Empower Pharmacy
Empower Pharmacy typically compounds semaglutide at multiple concentration tiers, often including 1 mg/mL, 2.5 mg/mL, and 5 mg/mL options. Their labeling usually displays the concentration prominently. At 5 mg/mL, your 30 units equals 1.5 mg.
Olympia Pharmacy
Olympia Pharmacy has been a popular source for compounded semaglutide. Their standard concentrations and vial sizes vary, so always check each new order carefully. Some Olympia formulations include additives like B12 or glycine, which do not change the semaglutide concentration but appear on the label and can cause confusion.
BPI Labs
BPI Labs offers compounded semaglutide in various configurations. As with any compounding pharmacy, verify the concentration on each vial rather than relying on what a previous order contained. Formulations and concentrations can change between batches.
Direct Meds and other providers
Direct Meds and similar telehealth providers often use their own compounding pharmacy partners, which means the concentration can vary depending on the supplier relationship at the time of your order. When you receive your vial, the first thing you do is read the label. The second thing you do is run the conversion.
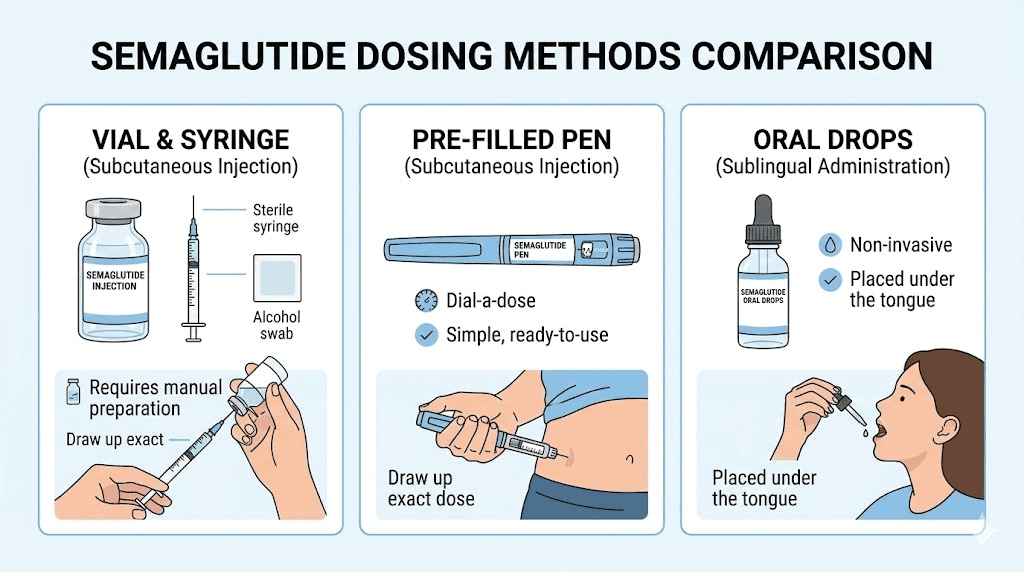
Semaglutide formulations that change the conversion math
Not all semaglutide products are liquid solutions measured in units. Some alternative formulations use different measurement systems entirely, and understanding these differences prevents dangerous cross-format confusion.
Pre-filled pens (brand-name products)
Brand-name semaglutide pens like Ozempic and Wegovy deliver preset doses in milligrams. You do not draw units from a vial. You dial the pen to the prescribed dose and click. If your provider switches you from a compounded vial to a brand-name pen, the concept of 30 units becomes irrelevant. The pen measures in milligrams directly. Understanding how GLP-1 brand products relate to compounded versions helps navigate these transitions.
Oral semaglutide
Oral semaglutide drops and sublingual formulations use completely different dosing scales. Oral semaglutide bioavailability is roughly 1% of injectable bioavailability, meaning oral doses are dramatically higher in milligrams to achieve similar blood levels. A 30-unit injection dose has absolutely no equivalency to an oral dose measured in milligrams. These are separate systems with separate calculations.
Semaglutide with additives
Compounded vials that include methylcobalamin (B12), glycine, or other additives still use the semaglutide concentration for dosing calculations. The additives do not change the mg/mL of semaglutide in the solution. A vial labeled "Semaglutide 5 mg/mL with B12 1 mg/mL" means you calculate semaglutide dose at 5 mg/mL. The B12 is a bonus, not a complicating factor for your semaglutide math.
Safety considerations specific to the 30-unit dose
Every dose level carries specific safety considerations. At 30 units, the concerns vary based on which concentration makes up your protocol.
At lower concentrations (0.3 to 0.75 mg)
If your 30 units delivers a dose below 1.0 mg, you are in the early titration phase. Side effects are typically mild. The most common include slight nausea during the first few days after injection, minor fatigue, and reduced appetite. These effects usually resolve within the first two to three weeks as your body adjusts to the GLP-1 receptor activation.
At these lower doses, the risk of serious adverse effects is minimal for most people. However, if you experience persistent vomiting, severe abdominal pain, or signs of dehydration, contact your provider regardless of dose level.
At moderate concentrations (0.9 to 1.5 mg)
The 0.9 to 1.5 mg range is where most therapeutic effects become pronounced. Appetite suppression strengthens considerably. Dietary considerations become more important because reduced food intake can lead to nutritional deficiencies if you are not deliberate about food choices.
At 1.5 mg specifically, ensure adequate protein intake. Semaglutide-driven weight loss can include muscle mass if nutrition is not optimized. Many providers recommend 0.7 to 1 gram of protein per pound of body weight during semaglutide treatment to preserve lean mass. Following a structured diet plan while on semaglutide significantly improves outcomes at this dose level.
Hydration matters more at moderate doses because nausea and reduced food intake can lower fluid consumption. Aim for at least 64 ounces of water daily, more if you exercise regularly.
Alcohol interactions
At any dose, alcohol and semaglutide interact in ways that increase nausea and reduce medication effectiveness. At the 1.5 mg level, these interactions become more pronounced. Many patients report that their alcohol tolerance drops significantly, and even small amounts of alcohol trigger intense nausea. This is not a safety emergency for most people, but it does affect quality of life and social situations.
Exercise at 30 units
Whether you can lose weight on semaglutide without exercise depends on your overall caloric deficit, but adding exercise improves outcomes at every dose level. At 1.5 mg, the combination of appetite suppression and regular physical activity typically produces the fastest and most sustainable results. If you have not been exercising, start with low-impact activities and increase gradually.
Storing your semaglutide vial to preserve potency at every dose
Improper storage degrades semaglutide over time, which means your 30 units might deliver less than the calculated milligrams if the peptide has lost potency. Protecting your investment requires consistent storage practices.
Refrigeration requirements
Semaglutide must be stored in a refrigerator at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). Both compounded semaglutide and brand-name versions require cold storage after opening. Place the vial in the main compartment of the refrigerator, not in the door where temperature fluctuates, and not near the back where it might freeze.
How long semaglutide lasts
Compounded semaglutide typically maintains potency for 28 to 90 days when properly refrigerated, depending on the compounding pharmacy formulation. Once reconstituted from lyophilized powder, most pharmacies recommend use within 28 days. Pre-mixed liquid formulations may last longer due to additional stabilizers.
If your vial accidentally gets left out overnight, brief temperature excursions usually do not destroy the peptide entirely, but repeated or prolonged exposure to room temperature reduces potency. When in doubt about a vial that has been temperature-compromised, contact your pharmacy rather than guessing.
Travel considerations
Traveling with semaglutide requires a cold pack or insulated medication bag. Airport security allows injectable medications with proper labeling. Keep your vial in a clear bag with your pharmacy label visible. The TSA and most international security agencies recognize insulin-style syringes and vials as medical supplies.
Expiration and potency
Using semaglutide after its expiration date is not recommended, though the peptide does not become toxic. It simply loses potency. If your vial is past its use-by date, the 1.5 mg you calculate from 30 units at 5 mg/mL might only deliver the equivalent of 1.0 mg or less. Expired semaglutide can lead to unexplained plateaus that have nothing to do with your body adapting and everything to do with degraded medication.
Comparing 30 units of semaglutide to equivalent tirzepatide doses
If you are considering switching from semaglutide to tirzepatide, or if your provider has mentioned the possibility, understanding cross-medication dose equivalency helps set expectations.
Semaglutide and tirzepatide are different peptides with different receptor profiles. Semaglutide activates the GLP-1 receptor exclusively. Tirzepatide activates both GLP-1 and GIP receptors, which produces somewhat different metabolic effects. Direct milligram-to-milligram comparisons are not meaningful because the two molecules have different potencies at their respective receptors.
That said, rough clinical equivalencies exist. A 1.5 mg semaglutide dose (30 units at 5 mg/mL) produces appetite suppression and weight loss roughly comparable to a 5 to 7.5 mg tirzepatide dose, according to clinical trial data comparing the two medications head-to-head. The semaglutide to tirzepatide conversion chart provides more detailed cross-reference values.
The side effect profiles differ between the two medications. Tirzepatide tends to produce more pronounced gastrointestinal effects at equivalent efficacy levels, while semaglutide produces more consistent appetite suppression at lower doses. The choice between them depends on individual response, tolerability, and provider recommendation.
For those interested in tirzepatide dosing specifics, tirzepatide also uses unit measurements with concentration-dependent conversions. The same formula applies: (Units / 100) x Concentration = Dose in mg. The tirzepatide dosage calculator handles the math for that peptide specifically.
When 30 units might not be the right dose for you
The fact that 30 units appears commonly in protocols does not mean it is universally appropriate. Several factors influence whether 30 units delivers the optimal therapeutic dose for your specific situation.
Body weight considerations
Semaglutide dosing in clinical trials was not weight-based. Everyone followed the same escalation schedule regardless of body weight. However, real-world evidence suggests that higher body weight individuals often need higher maintenance doses to achieve equivalent appetite suppression. If you weigh over 250 pounds and are on 30 units at 5 mg/mL (1.5 mg), you may benefit from continuing escalation to 1.7 mg or 2.4 mg. The BMI thresholds for GLP-1 therapy provide context on weight-based dosing considerations.
Side effect tolerance
If 30 units at your current concentration produces intolerable side effects, you may need to step back to a lower unit count and escalate more gradually. Common dose-limiting side effects include persistent nausea, constipation, excessive burping, and sleep disturbances. These effects usually resolve within two weeks of stabilizing at a new dose, but if they persist beyond that window, the dose may be too high for your current tolerance.
Medication interactions
Semaglutide interacts with several other medications. If you take phentermine alongside semaglutide, the combined appetite-suppressive effect can make even moderate semaglutide doses feel more potent. Phentermine and semaglutide work through different mechanisms, and their combination requires careful dose management. Similarly, semaglutide slows gastric emptying, which affects the absorption timing of oral medications. If you take time-sensitive medications, the delayed gastric emptying from a 1.5 mg dose (30 units at 5 mg/mL) may require schedule adjustments.
Post-surgical considerations
If you have had recent surgery, resuming semaglutide at your previous dose may not be appropriate. Many surgeons and anesthesiologists recommend stopping GLP-1 medications before surgery due to their gastric emptying effects. When resuming, most providers suggest restarting at a lower dose and re-titrating, even if you were previously stable at 30 units.
Using the SeekPeptides calculator for instant conversions
Manual math works. But when you need a quick answer and want to verify your calculations, the SeekPeptides semaglutide dosage calculator handles the conversion instantly. Enter your concentration, enter your units, and the calculator displays the milligram dose. No formula required. No room for arithmetic errors.
SeekPeptides also offers a peptide reconstitution calculator for those working with lyophilized powder, a peptide cost calculator for budgeting your protocol, and a general peptide calculator that works across multiple peptide types. These tools eliminate the most common source of dosing errors: mental math done in a hurry.
For researchers serious about optimizing their peptide protocols, SeekPeptides provides the most comprehensive resource available. Evidence-based guides, proven protocols, a complete calculator suite, and a community of thousands who have navigated these exact dosing questions. Members access detailed escalation schedules, side effect management strategies, and personalized protocol guidance that goes far beyond a simple unit-to-mg conversion.
Advanced conversion scenarios
Beyond the basic formula, certain real-world situations add complexity to the 30-unit conversion. Understanding these edge cases makes you a more confident and safer user.
Switching pharmacies mid-vial
If you run out of your current vial and your new vial from a different pharmacy has a different concentration, do not assume you can just continue drawing 30 units. Recalculate everything. Many people keep a small notebook or phone note with their current vial concentration, the date they started it, and the calculated dose per unit count. This simple habit prevents errors during transitions.
Dose splitting
Some providers recommend splitting weekly semaglutide doses into two smaller injections to reduce side effects. If your weekly dose is 30 units at 5 mg/mL (1.5 mg), a split protocol would have you injecting 15 units (0.75 mg) twice per week, typically spaced three to four days apart. The total weekly dose remains 1.5 mg. Split dosing can reduce nausea and provide more consistent blood levels throughout the week.
Microdosing scenarios
The growing interest in microdosing GLP-1 peptides means some researchers use very low unit counts from high-concentration vials. If you are drawing 30 units from a 0.5 mg/mL or 1 mg/mL vial for microdosing purposes (0.15 to 0.3 mg), the precision of your syringe becomes critical. At these low doses, even a 2-unit error represents a meaningful percentage change in your dose. Use the smallest available syringe for microdosing protocols.
Multi-peptide protocols
Researchers using semaglutide alongside other peptides sometimes draw from multiple vials in a single session. The 30-unit conversion applies only to your semaglutide vial. Do not carry concentration assumptions between different peptide products. Each vial has its own concentration, and each requires its own conversion calculation. The peptide stacking calculator can help manage multi-peptide protocols.
Tracking your dose over time
Documenting every injection creates a record that helps both you and your provider make informed dosing decisions. For 30 units specifically, tracking reveals patterns that guide future adjustments.
What to log
Record the date, time, unit count, vial concentration, calculated milligram dose, injection site, and any notable side effects or responses. This takes less than 30 seconds per injection and provides invaluable data over weeks and months.
Recognizing when 30 units stops working
If you have been stable at 30 units for several months and notice that appetite suppression is weakening, weight loss is stalling, or energy is declining, several factors could be at play. The most common is simple tolerance, where your body adapts to the current dose over time. Other possibilities include vial degradation from improper storage, a pharmacy formulation change, or metabolic adaptation to lower caloric intake.
Your injection log helps differentiate between these causes. If your vial is fresh, your technique is consistent, and your diet has not changed, tolerance is the most likely explanation and a dose increase discussion with your provider is warranted.
The role of patience
Weight loss on semaglutide is not linear. First month results vary enormously. Some people see dramatic changes at 30 units. Others see nothing for three weeks and then lose several pounds in week four. The medication builds cumulative effects over time, and judging effectiveness based on a single week at a single dose leads to premature adjustments. Give each dose level a minimum of four weeks before evaluating its effectiveness.
Frequently asked questions
Is 30 units of semaglutide the same as 30 mg?
No. Units and milligrams are completely different measurements. Thirty units equals 0.3 mL of liquid, regardless of concentration. The milligram dose depends on the concentration of your vial. At 5 mg/mL, 30 units equals 1.5 mg. At 1 mg/mL, 30 units equals only 0.3 mg. See the semaglutide units to mg conversion guide for the complete formula.
Can I use the same 30-unit dose when I switch semaglutide brands?
Only if both brands have the same concentration. Different brands and pharmacies compound semaglutide at different concentrations. Always check the mg/mL on the new vial label and recalculate your dose using the formula: (30 / 100) x concentration = mg dose.
How do I know if 30 units is too much or too little?
The answer depends on your concentration, your position in the dose escalation schedule, and your individual response. At 5 mg/mL, 30 units (1.5 mg) is a moderate therapeutic dose appropriate for people in weeks 9 through 16 of treatment. At lower concentrations, 30 units may be a starting dose. Understanding whether your dose is appropriate requires knowing your concentration and treatment timeline.
What happens if I accidentally inject 30 units from a higher concentration vial?
If you accidentally draw 30 units from a vial with a higher concentration than intended, you have taken a larger dose than planned. Monitor for increased nausea, vomiting, and other gastrointestinal symptoms. A single accidental overdose at moderate levels (up to 2x intended dose) is unlikely to cause serious harm but may produce uncomfortable side effects for 24 to 48 hours. Contact your provider if symptoms are severe or persistent.
Does the conversion change if my semaglutide contains B12 or glycine?
No. Additives like B12 or glycine do not change the semaglutide concentration. The mg/mL listed on the label refers to semaglutide specifically. Use that number for all your conversion calculations.
How many doses can I get from one vial at 30 units per dose?
Divide the total vial volume (in mL) by 0.3 mL. A 2 mL vial provides approximately 6 doses at 30 units each. A 3 mL vial provides approximately 10 doses. A 5 mL vial provides approximately 16 doses. Account for a small amount of waste liquid that cannot be drawn from the vial, typically 0.1 to 0.2 mL.
Should I switch to a different concentration to make 30 units more or less potent?
Your provider determines both your target dose in milligrams and the vial concentration. If you want a different milligram dose from 30 units, the simpler approach is usually to change the number of units drawn rather than switching vial concentrations. However, some people prefer 30 units as their standard draw because they are comfortable with the syringe measurement and would rather adjust concentration to change their dose. Discuss this preference with your provider.
Can I mix two partially used vials to get my full 30 units?
Only if both vials have the exact same concentration and are from the same pharmacy batch. Drawing 15 units from vial A and 15 units from vial B of the same concentration gives you a valid 30-unit dose. Mixing vials of different concentrations in a single injection is extremely dangerous and should never be done.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your conversions stay accurate, your concentrations stay labeled, and your doses stay consistent.