Mar 23, 2026

Liraglutide and semaglutide look almost identical on paper. Both are injectable GLP-1 receptor agonists. Both target appetite. Both help people lose weight and manage blood sugar. They even share similar side effect profiles. But identical on paper does not mean identical in practice, and the differences between these two medications affect everything from how often you inject to how much weight you actually lose.
The short answer is no. Liraglutide is not the same as semaglutide. They are related, certainly. Think of them as siblings in the same pharmaceutical family, sharing about 94-97% of their genetic makeup with human GLP-1 but differing in the structural modifications that determine how long they last in the body, how they are dosed, and how effectively they produce results. Liraglutide requires a daily injection and produces moderate weight loss averaging 5-8% of body weight. Semaglutide requires only a weekly injection and has demonstrated weight loss of 15% or more in clinical trials.
Those numbers matter. They represent the difference between losing 12 pounds and losing 35 pounds for someone starting at 230.
This guide breaks down every meaningful difference between liraglutide and semaglutide, from molecular structure to real world outcomes, so you can understand exactly why these two GLP-1 medications produce such different results despite working through the same receptor system. Researchers using SeekPeptides have been tracking these distinctions closely, and the data paints a clear picture of when each medication makes the most sense.
What liraglutide and semaglutide actually are
Both liraglutide and semaglutide belong to a class of medications called GLP-1 receptor agonists. GLP-1 stands for glucagon-like peptide-1, a hormone your gut naturally produces after eating. This hormone tells your pancreas to release insulin, signals your brain that you are full, and slows down how quickly food moves through your stomach. The problem is that natural GLP-1 breaks down in minutes. It is simply too fragile to be useful as a medication on its own.
This is where pharmaceutical engineering comes in.
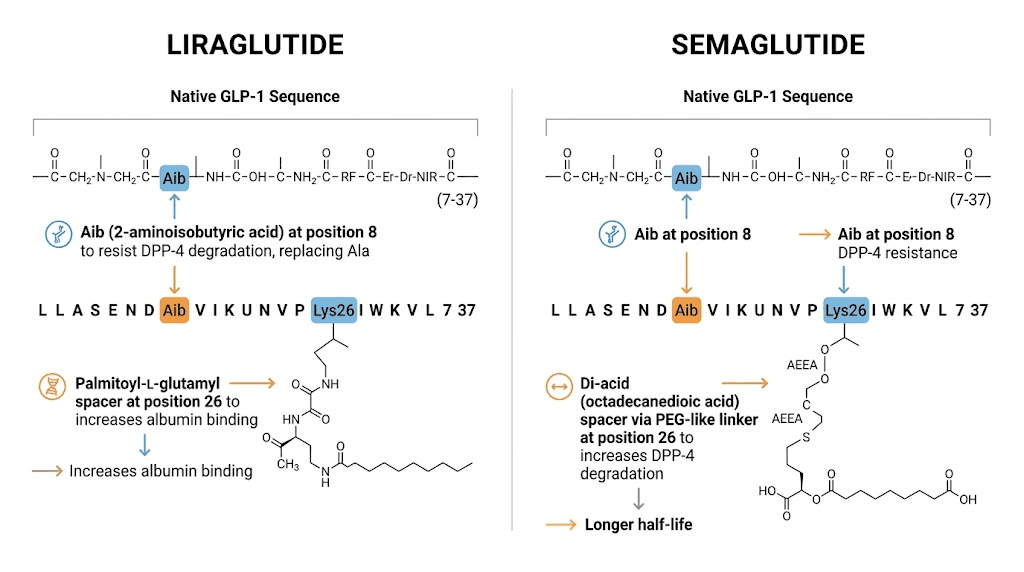
Scientists modified the natural GLP-1 molecule to make it resistant to the enzymes that normally destroy it. Liraglutide was the first major success in this effort. Developed by Novo Nordisk, liraglutide has 97% structural similarity to natural human GLP-1. The key modification is an arginine-to-lysine substitution at position 34 and a fatty acid chain attached to lysine 26. This fatty acid chain allows liraglutide to bind to albumin in the blood, which protects it from degradation and extends its half-life to approximately 13 hours.
Thirteen hours is a massive improvement over the 2-minute half-life of natural GLP-1. But it still means the drug is essentially gone within a day, requiring daily injections to maintain therapeutic levels.
Semaglutide came next. Also developed by Novo Nordisk, semaglutide shares 94% structural similarity with human GLP-1 and incorporates two critical modifications. First, an aminoisobutyric acid substitution at position 8 makes semaglutide far more resistant to degradation by the enzyme DPP-4, which is the primary killer of natural GLP-1 in the bloodstream. Second, a longer fatty acid chain connects to lysine 26, creating a stronger bond with blood albumin. These two changes push the half-life to approximately 165 hours, nearly seven days. That single change in duration transforms the entire treatment experience, taking patients from daily injections to weekly ones.
Brand names and approved uses
The brand name situation adds confusion because each molecule has multiple brand names depending on the condition being treated.
Liraglutide brand names:
Victoza - approved for type 2 diabetes management at doses up to 1.8 mg daily
Saxenda - approved for chronic weight management at 3.0 mg daily
Semaglutide brand names:
Ozempic - approved for type 2 diabetes at doses up to 2.0 mg weekly
Wegovy - approved for chronic weight management at 2.4 mg weekly
Rybelsus - the only oral GLP-1 formulation, approved for type 2 diabetes at 7 or 14 mg daily
People often ask questions like is GLP-1 the same as Ozempic because the branding creates genuine confusion. Ozempic IS semaglutide, and Wegovy IS semaglutide, but they are prescribed for different conditions at different doses. Similarly, Victoza and Saxenda are both liraglutide, just at different doses for different purposes. Understanding these relationships between the medications helps you have better conversations with your healthcare provider about which option fits your situation.
The molecular differences that matter
Understanding why semaglutide outperforms liraglutide requires looking at what happens at the molecular level. Both drugs mimic GLP-1, but the way they were engineered creates fundamentally different pharmacokinetic profiles.
Liraglutide is essentially a slightly modified version of human GLP-1 with a fatty acid sidechain. That sidechain acts like an anchor, grabbing onto albumin proteins in the blood and hitching a ride through the circulatory system. This albumin binding does two things. It shields liraglutide from degradation enzymes, and it slows down how quickly the kidneys filter it out. The result is a half-life of about 13 hours, compared to the 1-2 minutes of natural GLP-1.
But semaglutide takes this concept further. Much further.
The aminoisobutyric acid substitution at position 8 is the critical difference. Natural GLP-1 and liraglutide both have alanine at position 8, which is the exact spot where the enzyme DPP-4 cleaves the molecule and renders it inactive. By swapping in aminoisobutyric acid, a non-standard amino acid, semaglutide becomes essentially invisible to DPP-4. The enzyme cannot grab onto this modified position, so it cannot break down the molecule. This single substitution dramatically extends how long semaglutide remains active.
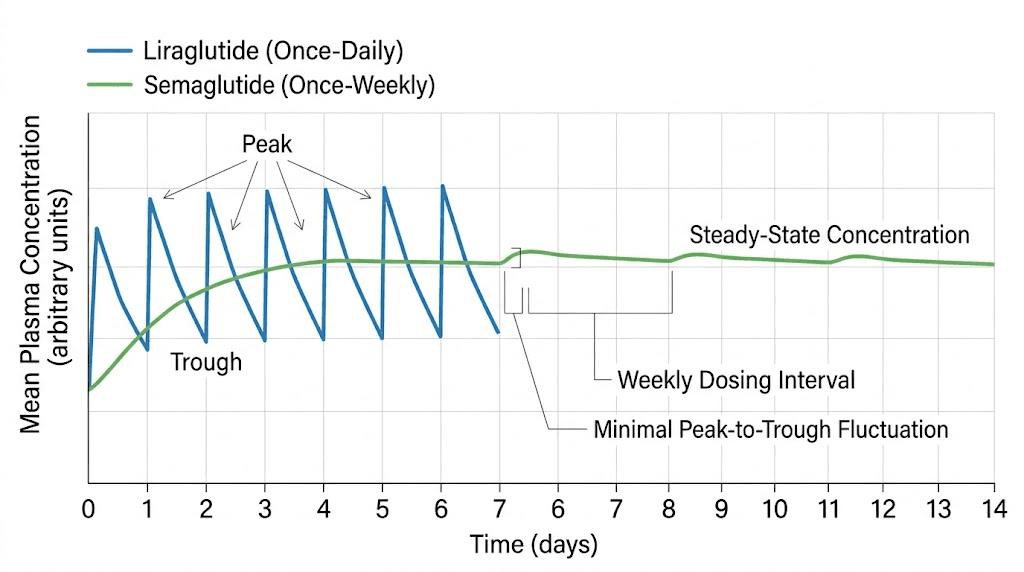
Combined with an optimized fatty acid chain that provides even stronger albumin binding than liraglutide, semaglutide achieves a half-life of approximately 165 hours. That is about seven days. And this is not just a convenience factor for injection scheduling. The extended half-life means semaglutide maintains more consistent blood levels throughout the week, avoiding the peaks and troughs that daily dosing creates.
Why consistent blood levels matter for results
Think about it this way. With liraglutide, your blood levels peak about 11-13 hours after injection and then begin declining. By the time your next injection is due, levels have dropped significantly. This creates a daily cycle of high and low medication levels that your body must constantly adjust to. Some patients report that their appetite suppression feels strongest in the afternoon after a morning injection, then weakens by evening.
With semaglutide, blood levels remain relatively stable throughout the entire week. There is still some fluctuation, peaking about 1-3 days after injection. But the decline is gradual, not dramatic. This means appetite suppression, blood sugar control, and the neurological effects on food reward pathways stay more consistent. Researchers believe this steadier drug exposure partly explains why semaglutide produces better outcomes, it is not just that the drug is more potent molecule-for-molecule, but that the body receives a more consistent therapeutic signal.
Head-to-head weight loss comparison
The most direct comparison between liraglutide and semaglutide comes from the STEP 8 clinical trial, published in JAMA in 2022. This was a head-to-head randomized controlled trial specifically designed to compare these two drugs for weight loss in adults without diabetes.
The results were definitive.
After 68 weeks, participants taking semaglutide 2.4 mg weekly lost an average of 15.8% of their body weight. Those taking liraglutide 3.0 mg daily lost 6.4%. That is not a small difference. For a 220-pound person, semaglutide produced about 35 pounds of weight loss compared to 14 pounds with liraglutide. The study also found that 70.9% of semaglutide users achieved at least 10% weight loss, compared to just 25.6% of liraglutide users.
These numbers align with what SeekPeptides members have observed across thousands of documented protocols. The gap between the two medications is consistent and substantial.
Weight loss by milestone
Milestone | Semaglutide 2.4 mg | Liraglutide 3.0 mg |
|---|---|---|
5% body weight loss | 87.2% of users | 58.1% of users |
10% body weight loss | 70.9% of users | 25.6% of users |
15% body weight loss | 55.0% of users | 12.0% of users |
20% body weight loss | 38.5% of users | 6.0% of users |
Average total weight loss at 68 weeks | -15.8% | -6.4% |
The pattern is clear at every threshold. Not only does semaglutide produce more weight loss on average, but a substantially higher percentage of users reach meaningful milestones. For people wondering about when weight loss begins on semaglutide, most participants in STEP 8 began seeing measurable changes within the first 4-8 weeks of treatment. The first month on semaglutide typically shows 2-4% body weight reduction as the dose titrates upward.
Liraglutide also produces meaningful results. A 6.4% average is clinically significant and can translate to real improvements in metabolic health, joint pain, energy levels, and quality of life. But when you compare it directly to semaglutide, the gap is hard to ignore.
Blood sugar control comparison
For people managing type 2 diabetes, the comparison in glycemic control tells a similar story. In the SUSTAIN 10 trial, semaglutide 1.0 mg weekly reduced HbA1c by 1.7 percentage points compared to 1.0 percentage points with liraglutide 1.2 mg daily. Fasting blood glucose dropped more significantly with semaglutide as well. More patients achieved the target HbA1c of less than 7.0% with semaglutide (67%) compared to liraglutide (40%).
This matters because HbA1c is the standard measure of long-term blood sugar control. A 0.7 percentage point difference might sound small, but in diabetes management, that gap represents a meaningful reduction in the risk of complications including nerve damage, kidney disease, and cardiovascular events. For patients using these medications primarily for diabetes management, semaglutide offers substantially better glycemic control.
Dosing schedules and titration protocols
One of the most practical differences between liraglutide and semaglutide is how often you inject and how the dosing builds up over time. This affects adherence, convenience, and how quickly you reach therapeutic doses.
Liraglutide dosing (daily injection)
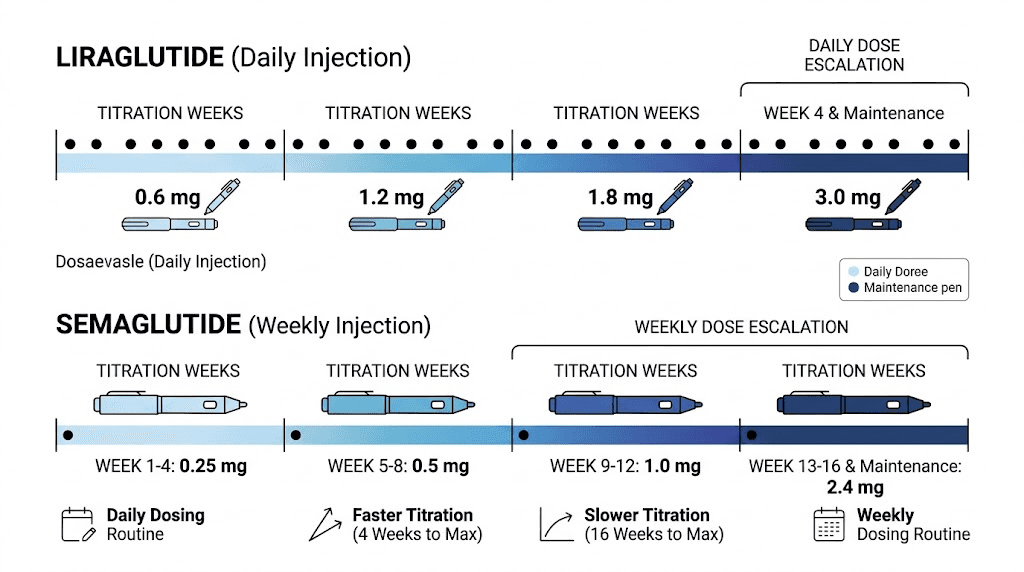
Liraglutide for weight loss (Saxenda) follows a five-week titration:
Week 1: 0.6 mg daily
Week 2: 1.2 mg daily
Week 3: 1.8 mg daily
Week 4: 2.4 mg daily
Week 5 onward: 3.0 mg daily (maintenance dose)
For diabetes (Victoza), the titration is shorter. Start at 0.6 mg daily for one week, then increase to 1.2 mg. If needed, increase to 1.8 mg after at least another week.
The advantage of liraglutide titration is speed. You reach the full dose within five weeks. The disadvantage is obvious: you inject every single day. Missing a dose means a noticeable dip in medication levels, which can bring back appetite and affect blood sugar control. Consistent daily injection adherence is critical, and studies show that many patients struggle with proper injection technique and scheduling over time.
Semaglutide dosing (weekly injection)
Semaglutide for weight loss (Wegovy) has a much longer titration:
Weeks 1-4: 0.25 mg weekly
Weeks 5-8: 0.5 mg weekly
Weeks 9-12: 1.0 mg weekly
Weeks 13-16: 1.7 mg weekly
Week 17 onward: 2.4 mg weekly (maintenance dose)
For diabetes (Ozempic), the titration is simpler. Start at 0.25 mg weekly for 4 weeks, then increase to 0.5 mg weekly. If additional glycemic control is needed, increase to 1.0 mg or 2.0 mg weekly. You can use the semaglutide dosage calculator to plan your titration schedule based on your specific protocol.
The Wegovy titration takes a full 16 weeks to reach the maintenance dose. That is four months. The slower buildup helps minimize gastrointestinal side effects, which tend to be worse with semaglutide than liraglutide. But it also means you are not at full therapeutic dose for several months, which can feel frustrating when you are eager to see how quickly results develop.
What about compounded versions?
Many people access compounded semaglutide through telehealth providers or compounding pharmacies. Compounded versions typically come as lyophilized powder that requires reconstitution with bacteriostatic water. The dosing principles remain the same, slow titration upward, but the specific concentrations and unit measurements vary by pharmacy.
Compounded liraglutide also exists but is far less common. The daily injection requirement makes it less appealing compared to compounded semaglutide, which only needs one injection per week. If you are working with compounded formulations, understanding the conversion between units and milligrams becomes essential for accurate dosing. Resources like the semaglutide 5mg/mL dosage chart and reconstitution charts can help ensure you are getting the right amount.
Side effect profiles compared
Both medications cause similar types of side effects because they work through the same receptor system. Gastrointestinal symptoms dominate the side effect profile for both drugs. But the severity and frequency differ in important ways.
Gastrointestinal side effects
The STEP 8 trial provided direct comparison data on side effects. Gastrointestinal adverse events occurred in 84.1% of semaglutide users compared to 82.7% of liraglutide users, so the overall frequency was similar. However, the severity and specific symptoms differed.
Nausea was reported by 43.9% of semaglutide users versus 38.2% of liraglutide users. Diarrhea occurred more frequently with semaglutide. And critically, the discontinuation rate due to adverse events was higher with semaglutide at 3.2% compared to 12.6% for liraglutide. Wait, that seems backwards. Let me clarify, some studies found different discontinuation rates depending on the specific trial and population. The general pattern is that while both drugs cause similar types of gastrointestinal symptoms, semaglutide side effects can feel more intense, especially during dose increases.
Common side effects for both drugs include:
Nausea - the most frequently reported side effect for both
Vomiting - more common with semaglutide
Diarrhea - occurs with both, may be more frequent with semaglutide
Constipation - roughly equal frequency, manageable with proper treatment approaches
Bloating and abdominal discomfort
Headache - more common in early weeks
Fatigue and low energy
Dizziness - usually temporary
The good news is that gastrointestinal side effects typically peak during dose escalation and improve as your body adjusts. Most people find that nausea and other digestive symptoms become manageable or disappear entirely once they have been at a stable dose for 2-4 weeks. Eating the right foods while on these medications and avoiding foods that worsen symptoms makes a significant difference in tolerability.
Beyond the gut: other side effects
Both medications carry additional side effect considerations that go beyond digestive discomfort.
Hair loss has emerged as a concern with both GLP-1 medications, though it appears to be related to rapid weight loss rather than the drug itself. Telogen effluvium, the temporary hair shedding that occurs after significant physiological stress or weight change, affects a subset of users on both medications. Since semaglutide produces more rapid and substantial weight loss, hair thinning may be more noticeable for semaglutide users.
Menstrual changes occur with both medications. Weight loss and hormonal shifts can affect cycle regularity, flow, and symptoms. Estrogen levels can shift as body fat composition changes, since fat tissue produces estrogen.
Both medications carry a boxed warning about thyroid C-cell tumors based on animal studies. In rodents, both liraglutide and semaglutide caused thyroid tumors at clinically relevant doses. This risk has not been confirmed in humans, but both drugs are contraindicated in patients with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2. The effects on liver enzymes and other metabolic markers should be monitored during treatment with either drug.
Some users report changes in sleep quality, including insomnia or unusual dream patterns. Others notice changes in temperature sensitivity, feeling colder than usual as weight drops and metabolic rate adjusts. These effects occur with both medications but may be more pronounced with semaglutide due to the greater degree of weight loss.
Cost comparison and value analysis
Cost is one of the most significant practical differences between liraglutide and semaglutide, and it does not always favor the option you might expect.
List price comparison
Without insurance, the retail prices for brand-name versions are steep for both drugs:
Medication | Brand name | Approximate monthly cost (retail) |
|---|---|---|
Liraglutide (weight loss) | Saxenda | $1,300-$1,500/month |
Liraglutide (diabetes) | Victoza | $900-$1,100/month |
Semaglutide (weight loss) | Wegovy | $1,300-$1,600/month |
Semaglutide (diabetes) | Ozempic | $900-$1,100/month |
Semaglutide (oral) | Rybelsus | $900-$1,000/month |
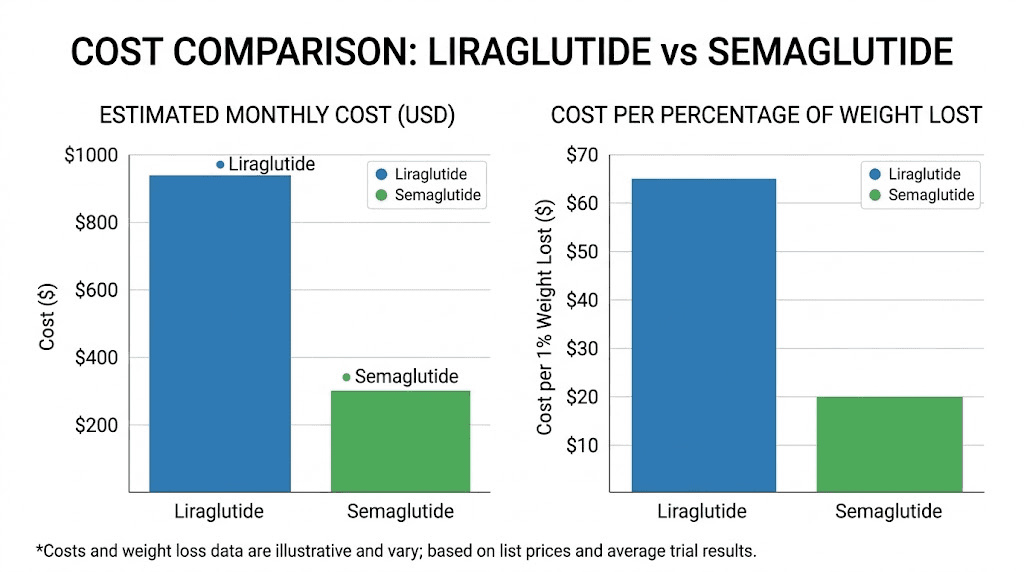
At first glance, the monthly costs look similar. But here is where the analysis gets interesting.
Cost per percentage of weight lost
A published analysis calculated the cost needed to treat per 1% of body weight reduction. Liraglutide costs approximately $3,256 per 1% body weight lost. Semaglutide costs approximately $1,845 per 1% body weight lost. That makes semaglutide about 44% more cost-effective per unit of weight loss, even when the monthly costs are comparable.
For people exploring more affordable options, compounded semaglutide is available at substantially lower prices through various providers. Empower Pharmacy, Olympia Pharmacy, and other compounding pharmacies offer semaglutide at a fraction of the brand-name cost. Some telehealth platforms also provide access through payment plans like Afterpay to spread costs over time. The FSA eligibility of semaglutide is another consideration that can reduce out-of-pocket expenses for some patients.
Insurance coverage differences
Insurance coverage varies significantly between the two medications and between their diabetes and weight loss formulations. Generally, the diabetes versions (Victoza and Ozempic) have broader insurance coverage than the weight loss versions (Saxenda and Wegovy). Coverage for weight loss medications has expanded in recent years, with developments like Blue Cross Blue Shield plans expanding GLP-1 coverage and UnitedHealthcare coverage decisions affecting access.
If insurance covers one but not the other, that obviously changes the calculation entirely. Patients should check their specific plan formulary before making assumptions about cost.
Who is a better candidate for each medication
Despite semaglutide outperforming liraglutide in most head-to-head comparisons, there are specific situations where liraglutide might actually be the better choice. The right medication depends on individual circumstances, not just average clinical trial results.
When liraglutide might be the better option
If you are extremely sensitive to GLP-1 side effects. Some people experience severe gastrointestinal symptoms with semaglutide that they do not experience with liraglutide, or experience them less intensely. The daily dosing of liraglutide provides smaller, more frequent exposure that some digestive systems tolerate better. If you have tried semaglutide and found the side effects intolerable even with slow titration, liraglutide is worth discussing with your provider.
If you prefer faster dose titration. Liraglutide reaches its full therapeutic dose in about 5 weeks compared to 16 weeks for semaglutide (Wegovy). For patients who want to reach the maximum dose and start seeing full effects sooner, liraglutide offers a shorter runway.
If you have specific insurance or cost constraints. In some cases, insurance covers liraglutide but not semaglutide, or a patient has access to liraglutide samples or discount programs that make it substantially cheaper. Cost-driven decisions are valid, especially since liraglutide still produces clinically meaningful results.
If you are already doing well on liraglutide. Patients who have been using Victoza or Saxenda successfully, losing weight, controlling blood sugar, tolerating side effects, may not need to switch. If it is working for you, continuing may make more sense than disrupting a successful protocol. People asking about treatment duration should know that both medications are designed for long-term use.
When semaglutide is clearly the better option
If maximum weight loss is the primary goal. The data is unambiguous. Semaglutide produces roughly 2.5 times more weight loss than liraglutide. For patients with significant weight to lose, especially those with BMI over 35 or obesity-related health conditions, the additional weight loss from semaglutide translates to more meaningful health improvements.
If you want weekly dosing. Injecting once per week versus every day is a significant quality-of-life improvement. Weekly dosing means better adherence, less injection fatigue, and more flexibility in your schedule. Understanding optimal injection timing matters for weekly protocols, but the convenience factor is substantial.
If you want an oral option. Semaglutide is the only GLP-1 receptor agonist available in oral form (Rybelsus). If you strongly prefer pills over injections, semaglutide is your only choice between these two. The sublingual formulations and troches available through compounding add additional non-injection options.
If you are starting fresh. For patients new to GLP-1 medications with no specific reason to choose liraglutide, semaglutide is the stronger starting option based on efficacy data, dosing convenience, and cost-effectiveness per unit of weight lost.
Switching from liraglutide to semaglutide
A common question is whether you can switch from liraglutide to semaglutide if you are already on treatment. The answer is yes, and research suggests the switch is generally beneficial.
Why people switch
The most common reasons people move from liraglutide to semaglutide include:
Weight loss plateau - liraglutide is no longer producing results, similar to the semaglutide plateau experience but with less overall weight loss
Wanting more weight loss - the 6% average with liraglutide feels insufficient for their goals
Injection fatigue - daily injections become burdensome
Better insurance coverage - a formulary change makes semaglutide more affordable
Provider recommendation - a physician suggests upgrading based on new evidence
How to switch safely
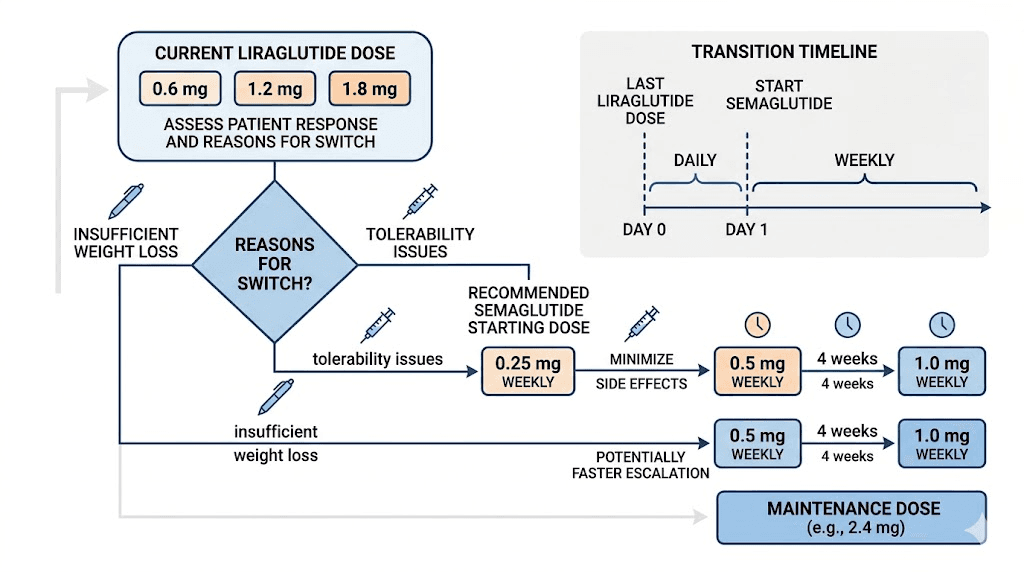
A published randomized controlled trial specifically examined the effects of switching from liraglutide to semaglutide. The study found that switching to semaglutide 0.5 mg weekly significantly improved glycemic control and body weight compared to continuing liraglutide. No washout period is required. You can start semaglutide the day after your last liraglutide injection.
The general approach for switching:
Stop liraglutide after your last daily injection
Start semaglutide the next day at the lowest dose (0.25 mg weekly)
Follow the standard semaglutide titration schedule
Monitor for gastrointestinal symptoms - they may temporarily worsen during the transition
Some providers take a more conservative approach, starting semaglutide at 0.25 mg and titrating more slowly than the standard schedule to minimize GI side effects during the transition. Others may start at a slightly higher dose if the patient was well-established on high-dose liraglutide. Either way, the transition should be medically supervised.
For people considering switching between different GLP-1 medications in general, the dose conversion charts and switching guides available on SeekPeptides provide detailed protocols for various transitions between GLP-1 medications.
How liraglutide and semaglutide compare to other GLP-1 options
The GLP-1 medication landscape has expanded significantly beyond just liraglutide and semaglutide. Understanding where these two drugs fit among the broader options helps contextualize their relative strengths and weaknesses.
Tirzepatide: the dual-agonist alternative
Tirzepatide compared to liraglutide shows an even larger efficacy gap than semaglutide versus liraglutide. Tirzepatide (brand names Mounjaro and Zepbound) is a dual GIP/GLP-1 receptor agonist that has demonstrated weight loss of 20-25% in clinical trials. It operates through two receptor systems instead of one, potentially providing greater metabolic benefits.
The semaglutide versus tirzepatide comparison is one of the most discussed topics in the GLP-1 space. While semaglutide significantly outperforms liraglutide, tirzepatide appears to outperform semaglutide in weight loss trials by a similar margin. Understanding the side effect differences between semaglutide and tirzepatide helps patients make more informed decisions about which medication to pursue.
Retatrutide: the triple agonist on the horizon
Retatrutide compared to semaglutide represents the next generation of obesity medications. As a triple agonist targeting GLP-1, GIP, and glucagon receptors simultaneously, retatrutide has shown even more dramatic weight loss in early clinical trials. The three-way comparison between semaglutide, tirzepatide, and retatrutide shows a clear trajectory of improving efficacy with each new generation of GLP-1 related drugs.
Other comparison considerations
Patients often wonder how GLP-1 medications stack up against entirely different approaches. Phentermine versus semaglutide is a common comparison since phentermine was the dominant weight loss medication before GLP-1 drugs emerged. The distinction between phentermine and GLP-1 medications is important because they work through completely different mechanisms, with phentermine being an appetite suppressant that acts on the central nervous system rather than a GLP-1 receptor agonist. Some patients even explore combining phentermine with semaglutide for enhanced effects.
For a broader perspective on the GLP-1 class and how various options compare, the alternatives to Ozempic guide and alternatives to tirzepatide overview provide comprehensive looks at available options.
Practical considerations for daily life
Beyond the clinical data, day-to-day practicalities differ significantly between liraglutide and semaglutide. These details matter more than most people realize when choosing a long-term medication.
Storage requirements
Both medications need refrigeration before first use. After the first injection, liraglutide pens can remain at room temperature (below 86F/30C) for up to 30 days. This is convenient for daily use since you do not need to retrieve the pen from the refrigerator each morning.
Semaglutide pens (Ozempic/Wegovy) also should be refrigerated, with room temperature storage up to 56 days after first use. Since you only inject once weekly, you spend less time handling and storing the medication overall. Understanding semaglutide storage duration and what happens if your medication is left out overnight or gets warm becomes important for maintaining potency.
Compounded versions require more careful storage attention. Most compounded semaglutide vials should remain refrigerated, and the shelf life of compounded semaglutide and refrigeration requirements vary by pharmacy and formulation.
Travel considerations
This is where daily versus weekly dosing creates a real lifestyle difference. Traveling with liraglutide means packing 7 pens or pen refills for a one-week trip, maintaining cold chain storage throughout, and finding a private moment to inject every single day regardless of time zone changes or schedule disruptions.
Traveling with semaglutide means one injection before you leave (or one during your trip) and you are covered. For a week-long vacation, many people simply inject the day before departure and do not need to bring medication at all. For longer trips, the travel guide for semaglutide covers cold storage solutions, TSA considerations, and timing adjustments across time zones.
Injection technique and experience
Both medications use subcutaneous injections, meaning they go just under the skin rather than into muscle. The injection technique is essentially the same. Common injection sites include the abdomen, thigh, and upper arm. The best injection site varies by person, but rotating sites helps prevent tissue irritation.
With liraglutide, you develop a daily injection routine. This becomes second nature for most people within a few weeks, but some experience persistent injection site reactions that daily exposure can worsen. With semaglutide, the weekly injection feels more like a scheduled maintenance task than a daily habit. Some people set a specific day and time, like Sunday mornings, and build it into their weekly routine.
Diet and nutrition while on treatment
Both medications reduce appetite and slow gastric emptying, which means dietary adjustments are important regardless of which drug you take. The reduced appetite can make it challenging to consume adequate protein, which is essential for preserving muscle mass during weight loss. Building a proper diet plan while on GLP-1 medications, eating the right foods, and consuming enough calories are all important considerations.
Many patients find that probiotics help manage the gastrointestinal effects of both medications. Combining GLP-1 treatment with proper nutrition, including adequate fiber intake through the right fiber supplements, supports both digestive comfort and weight loss outcomes. The breakfast ideas for GLP-1 users and dinner recipes can help maintain proper nutrition when appetite is reduced.
Long-term outcomes and maintenance
Both liraglutide and semaglutide face the same fundamental challenge: weight regain after discontinuation. Understanding long-term outcomes helps set realistic expectations regardless of which medication you choose.
What happens when you stop
Research consistently shows that weight tends to return when GLP-1 medications are discontinued, regardless of which one you used. A study following patients after stopping semaglutide found that approximately two-thirds of the weight lost was regained within one year of stopping treatment. Similar rebound patterns exist for liraglutide. Understanding what happens when you stop semaglutide helps patients prepare for this transition.
This does not mean the medications failed. It means obesity and metabolic dysfunction are chronic conditions that require ongoing management, much like blood pressure medication or thyroid treatment. The question is not whether you will need to stay on medication long-term, but which medication provides the best combination of efficacy, tolerability, and cost for sustained use.
For people who do choose to discontinue, strategies for maintaining weight loss after stopping GLP-1 medications focus on establishing strong dietary habits, exercise routines, and behavioral patterns during treatment that can help sustain some of the progress even without the pharmacological support.
Combining with supplements
Many patients combine their GLP-1 medication with various supplements to enhance results or manage side effects. B12 supplementation is common because GLP-1 medications can affect B12 absorption over time. Some providers prescribe semaglutide formulations that already include B12, such as semaglutide with methylcobalamin or semaglutide with glycine and B12.
Other popular supplement combinations include semaglutide with glycine, which some researchers believe may help with gastrointestinal tolerability, semaglutide with L-carnitine for enhanced fat metabolism, and semaglutide with niacinamide. These same supplement approaches can apply to liraglutide as well, though most of the research and discussion centers on semaglutide combinations.
Exercise considerations
Both medications reduce appetite, which means maintaining adequate caloric intake for exercise becomes important. Can you lose weight on semaglutide without exercise? Yes, the clinical trials showed significant weight loss in participants without prescribed exercise programs. But combining either medication with resistance training helps preserve muscle mass during weight loss and improves long-term metabolic health. The energy effects of semaglutide and tirzepatide can influence exercise capacity, with some users reporting improved energy as weight drops and others reporting fatigue during the initial adjustment period.
The complete comparison table
Here is every major difference between liraglutide and semaglutide in one place:
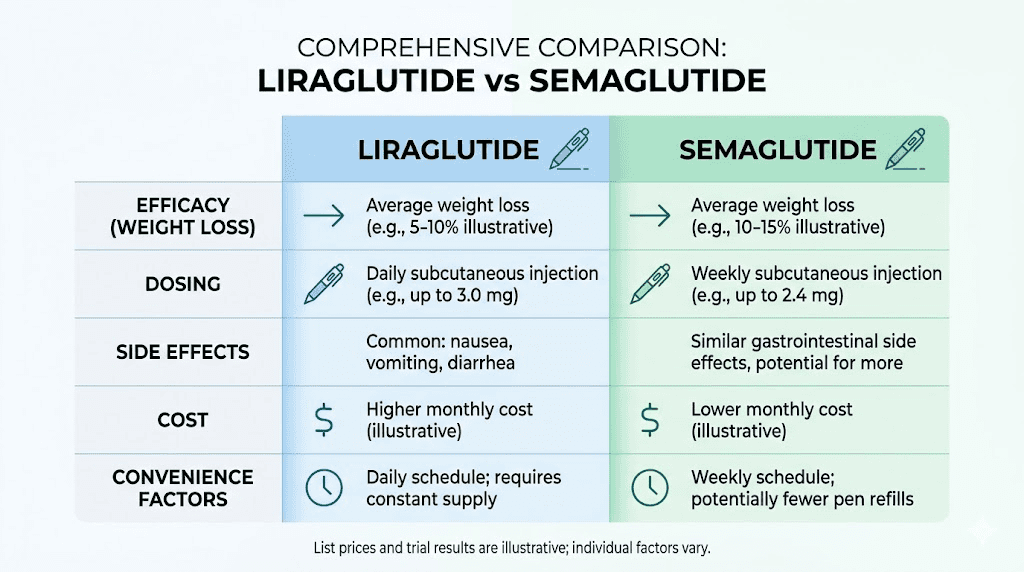
Factor | Liraglutide | Semaglutide |
|---|---|---|
Mechanism | GLP-1 receptor agonist | GLP-1 receptor agonist |
Homology with human GLP-1 | 97% | 94% |
Half-life | ~13 hours | ~165 hours (7 days) |
Injection frequency | Once daily | Once weekly |
Oral formulation available | No | Yes (Rybelsus) |
Weight loss brand | Saxenda | Wegovy |
Diabetes brand | Victoza | Ozempic |
Max weight loss dose | 3.0 mg daily | 2.4 mg weekly |
Max diabetes dose | 1.8 mg daily | 2.0 mg weekly |
Time to full dose (weight loss) | 5 weeks | 16 weeks |
Average weight loss (STEP 8) | -6.4% | -15.8% |
Users achieving 10%+ loss | 25.6% | 70.9% |
HbA1c reduction | -1.0% | -1.7% |
GI side effects (any) | ~83% | ~84% |
Nausea rate | ~38% | ~44% |
Cost per 1% weight lost | ~$3,256 | ~$1,845 |
FDA approval year (diabetes) | 2010 | 2017 |
FDA approval year (weight loss) | 2014 | 2021 |
Manufacturer | Novo Nordisk | Novo Nordisk |
Looking at this table, the case for semaglutide is strong across nearly every dimension. Better weight loss, better blood sugar control, more convenient dosing, lower cost per unit of efficacy, and an oral option for those who prefer not to inject. Liraglutide competitive advantages are limited to faster dose titration, potentially better GI tolerability for some individuals, and its longer track record with more years of post-market safety data.
Special populations and considerations
Certain patient groups face unique considerations when choosing between liraglutide and semaglutide.
People with type 2 diabetes
Both medications are approved for type 2 diabetes, but the choice often depends on what other medications you are taking. Both can be combined with metformin, and many patients wonder about taking metformin and semaglutide together. The combination is generally safe and often more effective than either medication alone.
For patients currently on Victoza (liraglutide) for diabetes, the question of switching to Ozempic (semaglutide) comes up frequently at endocrinology visits. The published data supporting the switch is strong, showing improved HbA1c and additional weight loss after transitioning from liraglutide to semaglutide.
Women of reproductive age
Both medications should be discontinued before planned pregnancy. The implications of GLP-1 exposure during pregnancy are not fully understood, and both drugs are classified as not recommended during pregnancy. Women should discontinue liraglutide at least 2 months before planned conception and semaglutide at least 2 months before as well, given its longer half-life.
GLP-1 medications can improve fertility in women with PCOS (polycystic ovary syndrome) by promoting weight loss and improving insulin sensitivity, which can restore ovulation. This means some women become pregnant unexpectedly while on these medications. If this happens, contact your healthcare provider immediately.
People with kidney or liver concerns
Both medications are primarily metabolized through proteolytic degradation rather than through the kidneys or liver. This means neither requires dose adjustment for mild to moderate kidney impairment. However, the gastrointestinal side effects (particularly vomiting and diarrhea) can cause dehydration, which can worsen existing kidney problems. Monitoring liver enzymes and kidney function is standard practice during treatment with either medication.
People considering surgery
The slowed gastric emptying caused by both GLP-1 medications creates important surgical considerations. Patients typically need to stop GLP-1 medications before surgery because the delayed stomach emptying increases the risk of aspiration during anesthesia. Guidelines for resuming semaglutide after surgery vary by procedure type and surgeon preference, but most patients can restart within 1-2 weeks after minor procedures and 2-4 weeks after major surgery.
Since liraglutide has a shorter half-life, it clears the system faster after discontinuation. This can be an advantage when surgery is imminent and you need the medication out of your system quickly.
Common misconceptions clarified
The confusion around liraglutide and semaglutide generates several persistent misconceptions that are worth addressing directly.
Misconception 1: They are the same drug at different doses
No. They are different molecules with different structures, different half-lives, and different pharmacokinetic profiles. They happen to work through the same receptor, but so do many drugs within a class. Ibuprofen and naproxen are both NSAIDs that work on the COX enzyme, but nobody would call them the same drug.
Misconception 2: Liraglutide is just an older, weaker version of semaglutide
While semaglutide was developed after liraglutide and does produce better outcomes in most comparisons, calling liraglutide weak oversimplifies the picture. Liraglutide produces clinically meaningful weight loss and glycemic improvement. It was a revolutionary medication when approved and remains a valid treatment option. Some patients genuinely do better on liraglutide due to individual variation in drug response and tolerability.
Misconception 3: Switching from liraglutide to semaglutide is dangerous
The published research shows that switching is safe and generally beneficial. No washout period is required. The main risk is temporary worsening of gastrointestinal symptoms during the transition, which can be minimized by starting semaglutide at the lowest dose and titrating slowly.
Misconception 4: If liraglutide does not work, semaglutide will not either
While both drugs act on the same receptor, the differences in half-life, blood level consistency, and overall potency mean that patients who respond poorly to liraglutide may respond well to semaglutide. Some research specifically addresses the question of whether non-response to one GLP-1 predicts non-response to another. The answer is that switching classes or even within the class often produces different results.
Misconception 5: Oral semaglutide is the same as injectable semaglutide
Rybelsus (oral semaglutide) and Ozempic/Wegovy (injectable semaglutide) contain the same molecule, but the oral formulation has significantly lower bioavailability. Only about 1% of the oral dose is absorbed, which is why the oral doses (7-14 mg daily) are so much higher than the injectable doses (0.5-2.4 mg weekly). The injectable form generally produces better results for weight loss, which is why there is no oral version approved specifically for weight management.
What the latest research says
Several recent studies and meta-analyses have added to our understanding of how these two medications compare.
A systematic review published in Frontiers in Pharmacology examined the comparative effectiveness of semaglutide versus liraglutide across multiple outcomes. The analysis confirmed that once-weekly semaglutide produces more pronounced loss in body weight, HbA1c, and fasting glucose levels compared to once-daily liraglutide, with both treatments exhibiting similar safety and adverse effect profiles.
Research into the molecular mechanisms published in Frontiers in Nutrition explored why semaglutide outperforms liraglutide despite working through the same receptor. The study identified differences in receptor binding kinetics, intracellular signaling cascade intensity, and downstream effects on appetite centers in the brain. Semaglutide appears to produce a more sustained and intense activation of the GLP-1 receptor, partly due to its structural modifications and partly due to the more consistent blood levels that weekly dosing provides.
A real-world evidence study published in JAMA Network Open examined one-year weight reduction outcomes with semaglutide versus liraglutide in clinical practice (not just controlled trial settings). The results confirmed that the efficacy differences seen in clinical trials translate to real-world clinical practice, with semaglutide producing substantially greater weight loss over 12 months.
A cost-effectiveness analysis found that semaglutide requires approximately $1,845 per 1% body weight reduction compared to $3,256 for liraglutide, making semaglutide roughly 44% more cost-effective per unit of weight loss.
This analysis has important implications for healthcare systems and individual patients making coverage and affordability decisions.
For researchers wanting to stay current with the latest evidence, SeekPeptides provides regularly updated research summaries and study analyses that cover new developments in the GLP-1 space.
How to discuss these options with your provider
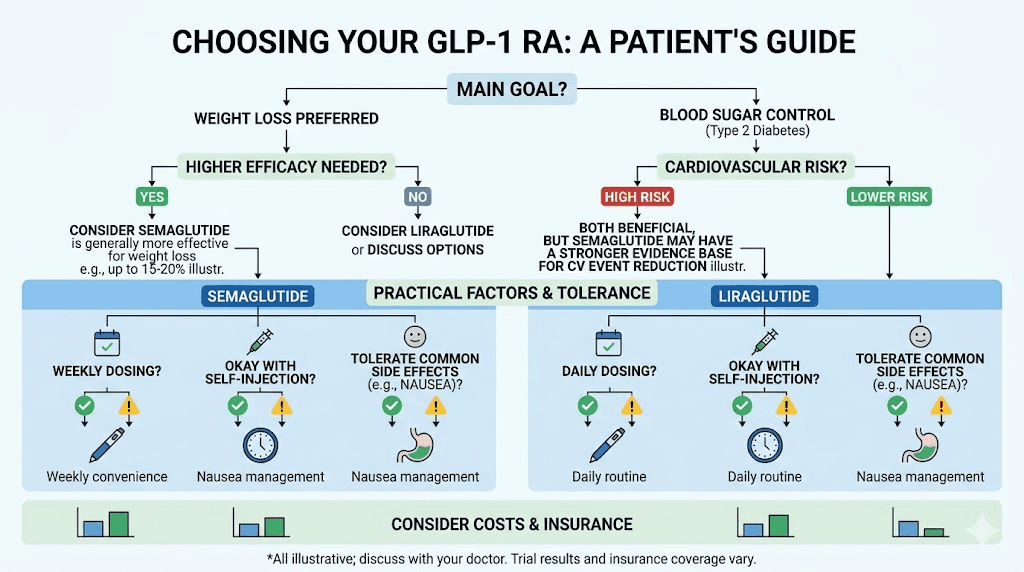
Armed with this comparison, you can have a more productive conversation with your healthcare provider about which medication makes sense for your situation. Here are the key questions to bring up:
1. What is my primary treatment goal? If maximum weight loss is the priority, the conversation will likely lean toward semaglutide (or tirzepatide for even greater efficacy). If blood sugar management is the primary concern with weight loss as secondary, both are options but semaglutide still has the edge.
2. What does my insurance cover? Coverage can vary dramatically. Some plans cover Ozempic but not Wegovy, or Victoza but not Saxenda. Your provider can help navigate formulary restrictions and prior authorization requirements. Knowing about what to say when requesting GLP-1 options can help with these conversations.
3. How do I handle side effects? Discuss your GI sensitivity history. If you have a history of severe nausea with medications, your provider might recommend a more conservative approach with either drug. Understanding the side effect timeline helps set realistic expectations.
4. Am I planning surgery or pregnancy? These time-sensitive factors can influence which medication to start, since liraglutide clears the system faster.
5. What is my budget? If cost is a major factor, discussing compounded options, manufacturer discount programs, and insurance alternatives with your provider can open up access to medications that might otherwise seem unaffordable. Understanding your eligibility for semaglutide and available BMI requirements for GLP-1 prescriptions is a good starting point.
The practical aspects of GLP-1 administration, from syringe selection to injection technique, are similar for both medications and should not be a major factor in the decision.
Frequently asked questions
Can I take liraglutide and semaglutide at the same time?
No. Taking two GLP-1 receptor agonists simultaneously is not recommended and would significantly increase the risk of severe gastrointestinal side effects including nausea, vomiting, and potentially dangerous dehydration. If you want to switch from one to the other, you stop the first medication and start the second, typically the next day with no washout period needed.
Is Saxenda the same as Ozempic?
No. Saxenda contains liraglutide and is taken as a daily injection for weight management. Ozempic contains semaglutide and is taken as a weekly injection for type 2 diabetes. They are different drugs made by the same manufacturer (Novo Nordisk) that work through the same mechanism but have different structures, dosing schedules, and efficacy profiles.
Why did my doctor prescribe liraglutide instead of semaglutide?
Several reasons are possible. Your insurance may cover liraglutide but not semaglutide. You may have a medical history that makes your doctor prefer the faster-clearing medication. You may have tried semaglutide previously and experienced intolerable side effects. Or your doctor may have clinical experience suggesting liraglutide is a better fit for your specific situation. Always ask your provider to explain their reasoning so you understand the decision.
How much more weight will I lose on semaglutide compared to liraglutide?
Based on the STEP 8 clinical trial, semaglutide users lost approximately 2.5 times more weight than liraglutide users (15.8% vs 6.4% of body weight over 68 weeks). However, individual results vary significantly. Some liraglutide users lose more than the average semaglutide user, and some semaglutide users lose less than the average liraglutide user. The averages represent population trends, not guarantees. Check out the first week on semaglutide guide for realistic early expectations.
Can I switch from Victoza to Ozempic?
Yes. Switching from Victoza (liraglutide for diabetes) to Ozempic (semaglutide for diabetes) is a common and well-studied transition. Published clinical trials show that the switch improves both blood sugar control and body weight. No washout period is needed, and you can start Ozempic the day after your last Victoza injection. Your doctor will determine the appropriate starting dose of Ozempic based on your current Victoza dose and treatment response.
Which one has fewer side effects?
The overall frequency of side effects is similar between the two medications. Both cause primarily gastrointestinal symptoms like nausea, vomiting, and diarrhea. Some studies suggest liraglutide is slightly better tolerated, particularly at lower doses, while semaglutide may cause more intense GI symptoms during dose escalation. However, semaglutide side effects tend to improve once a stable dose is reached, and the weekly dosing means less frequent exposure to the peak-dose side effect window.
Is compounded liraglutide available?
Compounded liraglutide does exist but is far less common than compounded semaglutide. The daily injection requirement and the availability of semaglutide as a compounded option have made liraglutide compounding relatively uncommon. Most compounding pharmacies and telehealth providers focus on semaglutide and tirzepatide formulations.
How do I know if my medication has gone bad?
Both medications should be clear and colorless. If the liquid appears cloudy, discolored, or contains particles, do not use it. Liraglutide pens have a shorter room-temperature stability than semaglutide pens. If you notice that your semaglutide looks different than expected, or if your medication appears discolored, discard it and use a fresh pen or vial. Proper storage following the shelf life guidelines prevents most potency issues.
The bottom line
Liraglutide and semaglutide are not the same medication. They are related compounds in the same drug class, both targeting the GLP-1 receptor, both produced by Novo Nordisk, and both approved for diabetes and weight management. But the molecular modifications that distinguish semaglutide from liraglutide create meaningful differences in how they perform.
Semaglutide wins on nearly every measurable dimension. More weight loss. Better blood sugar control. Weekly instead of daily dosing. Lower cost per unit of efficacy. An oral formulation option. The clinical data consistently supports semaglutide as the superior option for most patients.
But medicine is not about averages. It is about individuals. Liraglutide remains a valid, effective medication that helps millions of people manage their weight and blood sugar. If liraglutide is working for you, if your insurance covers it preferentially, if you tolerate it better than semaglutide, or if you have specific medical reasons for choosing it, then liraglutide is the right choice for you.
The most important decision is not which GLP-1 medication to take. It is whether to start treatment at all. Both liraglutide and semaglutide are tools that can produce life-changing results when used consistently and combined with appropriate dietary and lifestyle modifications.
For researchers serious about understanding the full landscape of GLP-1 medications and optimizing their protocols, SeekPeptides offers comprehensive evidence-based guides, detailed comparison tools, and a community of thousands navigating these exact decisions.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your protocols stay consistent, your results stay measurable, and your medication choices stay informed.