Apr 4, 2026

Tired of conflicting information about retatrutide dosing for women? You search for answers and find generic protocols written for a 200-pound man. You ask your doctor and get a shrug. You join forums and get seventeen different opinions. Here is what actually works, built on real clinical data, female-specific pharmacology, and the numbers that matter.
Retatrutide is not just a stronger version of semaglutide or tirzepatide. It is a triple agonist, activating GLP-1, GIP, and glucagon receptors simultaneously. That triple mechanism changes everything, including how it behaves differently in female bodies compared to male ones. The Phase 2 trial published in the New England Journal of Medicine confirmed what many women suspected: they respond to this drug in ways that are meaningfully different from men. Better outcomes on average. Stronger side effects at lower doses. Different hormonal interactions that nobody warns you about.
This guide exists because most dosing information ignores those differences entirely. You will find the full titration schedule here, the math to calculate exact syringe units for any vial size, the hormonal considerations your prescriber may not mention, and the specific management strategies that reduce GI side effects, which hit women at roughly 2.5 times the rate they hit men on equivalent doses.
SeekPeptides compiled this guide using Phase 2 and Phase 3 clinical data, pharmacokinetic research on sex-based drug clearance, and real-world titration experience. If you want a second opinion on your protocol or access to detailed female-specific dosing calculators, start there.
Read this before your next injection. The protocol matters more than the molecule.
Why women need a female-specific retatrutide dosing approach
Pharmacokinetics differ by sex
The assumption that one dose fits all has caused real harm in weight-loss pharmacology. Retatrutide was studied in mixed-sex populations, but the data inside those trials tells a different story when you separate it by sex. Women are not smaller men. Their metabolic physiology, hormonal environment, and drug clearance patterns differ in ways that directly affect how retatrutide moves through the body and what it does when it gets there.
Start with pharmacokinetics. Women clear GLP-1 agonists more slowly than men. The drug stays active longer between injections. That sounds like a benefit, and in terms of weight loss it partly is. But it also means that peak drug concentrations build higher relative to dose, which is the direct explanation for the elevated GI side effect burden women experience. A 6mg dose does not behave identically in a woman as it does in a man of equivalent weight. The exposure window is longer, the receptor activation is more sustained, and the nausea that results is not a psychological response to injections. It is a pharmacological consequence of pharmacokinetics.
Body composition and hormonal environment
Body composition adds another layer. Women carry a higher percentage of body fat than men at equivalent body weight. Fat tissue is metabolically active. It is also an endocrine organ that produces estrogen through aromatization. When retatrutide drives 20 to 30 percent body weight reduction, that reduction is not neutral hormonally. You are removing a significant estrogen-producing organ. The downstream effects on menstrual cycles, bone density signaling, and mood regulation are real and worth understanding before you start.
Response data: women outperform men consistently
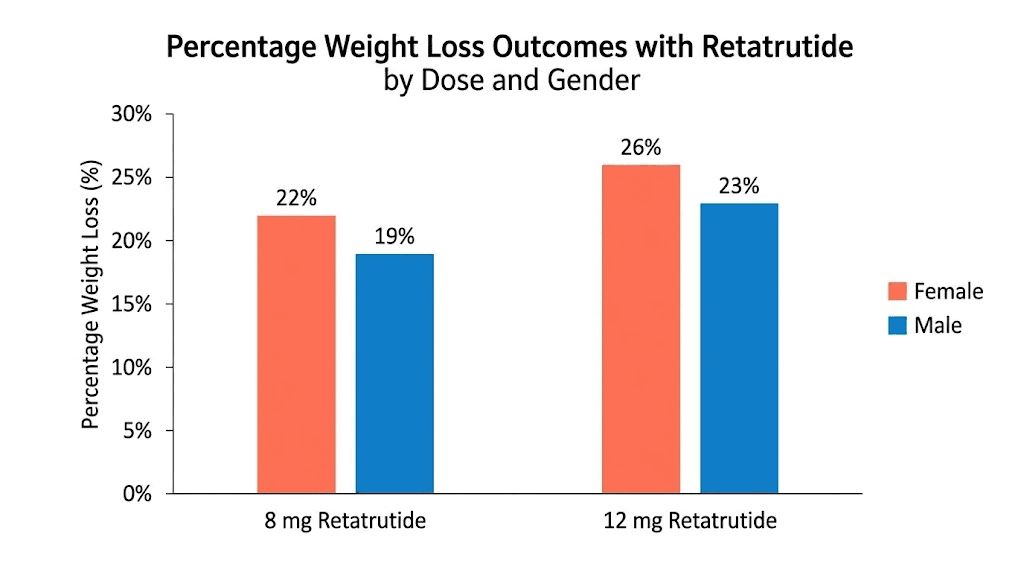
Then there is the response data itself. Across GLP-1 studies, women have achieved approximately 11 percent greater relative weight loss than men at equivalent doses. In the retatrutide Phase 2 trial, the sex difference was even more pronounced. Women in the highest dose groups lost 28.5 percent and 26.6 percent of body weight. Men in the same groups lost 19.8 percent and 21.9 percent. That is not a small difference. It suggests that standard doses may already be achieving near-maximal effect in women, which has implications for how aggressively you need to escalate. You can read more about how the retatrutide dosage calculator accounts for these sex-based response differences.
Female-specific conditions requiring protocol adjustments
Women also face hormonal considerations that simply do not apply to men. PCOS. Fertility planning. Hormone replacement therapy. Breastfeeding. These are not edge cases. They are common circumstances that require specific protocol modifications, and generic dosing guides never address them.
Understanding these differences is not about getting a smaller dose. It is about getting the right dose, escalating at the right pace, managing side effects before they become a reason to quit, and protecting hormonal health throughout the process. The complete retatrutide dose guide covers the general population framework. This guide covers the female-specific layer on top of that.
One more thing worth stating directly: women are not undertreated in peptide research because researchers do not care. They are undertreated because trial populations have historically skewed male. That is changing. The retatrutide data is among the best sex-stratified weight-loss trial data available. Use it.
What the clinical trials reveal about retatrutide and women
Phase 2 trial results: the headline numbers
The Phase 2 trial data is the foundation. Everything else builds on it.
Published in the New England Journal of Medicine, the trial tested retatrutide at doses of 1mg, 4mg, 8mg, and 12mg against placebo over 48 weeks. The primary endpoint was mean percentage weight change. At 48 weeks, the 12mg group achieved a mean weight reduction of 24.2 percent, representing 26.2 kilograms lost. At 24 weeks, the same group was already at 17.5 percent reduction, or 18.7 kilograms. Those are headline numbers. The sex-stratified data inside them is more interesting.
Sex-stratified outcomes: what the data shows women
Women in the 12mg dose groups lost 28.5 percent and 26.6 percent of body weight. Men in the same groups lost 19.8 percent and 21.9 percent. That means the best-performing women lost roughly 44 percent more weight than the best-performing men on identical protocols. This is not a marginal finding. It is a consistent signal that female metabolic response to triple agonism is stronger than male response at equivalent doses.
The responder analysis tells an equally compelling story. In the 12mg group, 100 percent of participants achieved at least 5 percent body weight loss. 93 percent achieved at least 10 percent. 83 percent achieved at least 15 percent. Those numbers held across sexes, but women reached those thresholds faster. In the 8mg group, 100 percent achieved 5 percent loss, 91 percent achieved 10 percent, and 75 percent achieved 15 percent.
Phase 3 data and practical implications for your protocol
Phase 3 data extended the timeline to 68 weeks and pushed peak weight loss to 28.7 percent, equivalent to 71.2 pounds or 32.3 kilograms in the highest-performing participants. Participant satisfaction was reported at 94.4 percent. These are numbers that no prior obesity medication has come close to matching.
What does this mean practically for women? It means you may reach your goal at a lower dose than the maximum. It means escalating to 12mg because that is the top of the scale may not be necessary or even advisable if you are already at your target at 8mg. It means the retatrutide dosage chart for weight loss should be read with your own response curve in mind, not the population average. You can also compare how these outcomes stack up against earlier drugs using the retatrutide vs semaglutide comparison and the retatrutide vs Mounjaro breakdown.
The GI side effect data is equally important. The trial documented nausea, vomiting, diarrhea, and constipation as the most common adverse events, with incidence peaking during dose escalation and declining at stable doses. Women experienced these at elevated rates. Understanding this in advance allows you to plan around it rather than abandoning the protocol during a rough week three.
One more clinical note: the trial used a gradual titration protocol specifically to manage tolerability. Participants did not start at 12mg. They stepped up over months. That design choice was not arbitrary. It reflects what the pharmacokinetic data shows about receptor adaptation and tolerability windows. Skipping steps does not save time. It increases dropout. The starting dose of retatrutide matters exactly because of this.
Complete retatrutide titration schedule for women
The four-week increment framework
The standard titration protocol moves in four-week increments. Each increment gives your body time to adapt before the next dose increase. For women, this pacing is not optional. It is the difference between tolerable and intolerable side effects during escalation.
Here is the complete week-by-week schedule:
Weeks | Dose | Frequency | Route | Notes |
|---|---|---|---|---|
1-4 | 2mg | Once weekly | Subcutaneous | Starting dose. Establish injection routine. |
5-8 | 4mg | Once weekly | Subcutaneous | First escalation. GI symptoms may increase briefly. |
9-12 | 6mg | Once weekly | Subcutaneous | Mid-escalation. Appetite suppression becomes significant. |
13-16 | 8mg | Once weekly | Subcutaneous | High therapeutic range. Assess response before proceeding. |
17+ | 10-12mg | Once weekly | Subcutaneous | Maximum range. Many women reach goals before this stage. |
Five rules women must know about this schedule
A few critical points about this schedule for women specifically.
First, you do not have to reach 12mg. The trial data showed that women achieved dramatically superior outcomes compared to men across all dose groups. If you have lost 20 percent of body weight at 8mg and your appetite is well-controlled, there is no clinical reason to escalate further. More drug is not always better drug. Review the retatrutide dosage chart and the 10mg retatrutide guide to understand what the higher dose range actually adds and whether that incremental gain is worth the added GI burden.
Second, the four-week increment is a minimum, not a maximum. If week four at any dose still feels rough, week five at the same dose is not failure. It is smart medicine. Extending any tier from four to six or eight weeks is a legitimate clinical strategy, particularly if you are experiencing nausea that is affecting nutrition intake, sleep, or work. See the retatrutide dose schedule for extended-pacing variations.
Third, injection day consistency matters more than most guides acknowledge. Because women clear GLP-1 agonists more slowly, trough concentrations before the next injection are higher relative to the starting point compared to men. This means the pharmacological gap between doses is narrower. Missing an injection by two or three days creates a sharper concentration fluctuation and can amplify nausea on the makeup dose. Pick one day per week and keep it. The best time to take retatrutide guide covers the timing considerations in detail.
Fourth, subcutaneous injection site rotation prevents localized tissue changes and ensures consistent absorption. Abdomen, thigh, and upper arm are all appropriate. Review where to inject retatrutide and how to inject retatrutide if you are new to self-injection. The best GLP-1 injection site for weight loss and how to inject GLP-1 guides provide additional technique guidance.
Fifth, if you are switching from tirzepatide to retatrutide, the starting dose and pacing logic is different. You likely have established GLP-1 receptor tolerance, which affects how you enter the retatrutide titration. See the retatrutide dosage schedule after high-dose tirzepatide for the transition-specific protocol.
The titration schedule above applies to research peptide use. If you are using pharmaceutical retatrutide through a clinical program, your prescriber will provide a protocol that may differ slightly. That protocol takes precedence.
How to calculate your exact retatrutide dose
Reconstitution basics: vials, BAC water, and insulin syringes
This section covers the math. It is not complicated once you understand the structure, but it does require precision. An error in reconstitution math means either underdosing or overdosing, neither of which serves you.
Retatrutide arrives as a lyophilized powder in vials. The most common research vial sizes are 5mg, 10mg, and 20mg. You reconstitute with bacteriostatic water, then draw doses using an insulin syringe calibrated in units (U-100 scale, where 100 units equals 1mL).
The peptide reconstitution calculator handles this math automatically and is the fastest way to get accurate unit counts for any vial and dose combination. If you prefer to understand the manual calculation, here is how it works.
The formula: Units to draw = (Dose in mg / Total mg in vial) x Total BAC water added in mL x 100
Worked examples for common vial and dose combinations
Walk through three common scenarios:
Scenario 1: 5mg vial, 2mg dose, 1mL BAC water added
(2 / 5) x 1 x 100 = 40 units. Draw to the 40-unit mark on your insulin syringe.
Scenario 2: 10mg vial, 4mg dose, 2mL BAC water added
(4 / 10) x 2 x 100 = 80 units. Draw to the 80-unit mark.
Scenario 3: 20mg vial, 8mg dose, 4mL BAC water added
(8 / 20) x 4 x 100 = 160 units. This exceeds a standard 1mL insulin syringe. Use two draws or a 2mL syringe.
Storage, shelf life, and cost management
The amount of BAC water you add does not change the dose you get. It changes the concentration of the solution, which changes how many units you draw. Adding more water means drawing more units for the same dose. Adding less water means drawing fewer units. Either approach works as long as the math is consistent. The how much BAC water for 10mg retatrutide guide shows the most common reconstitution ratios and their resulting concentrations.
For a consolidated visual reference, the retatrutide reconstitution chart and the retatrutide peptide dosage chart display pre-calculated unit values for the most common vial and water combinations. The retatrutide dose chart provides a quick-reference format for weekly doses across the titration schedule.
The retatrutide dosage calculator is the fastest tool for on-the-fly calculations when your vial size or water volume differs from standard scenarios. The peptide calculator works across all peptide types if you are managing multiple compounds simultaneously.
A note on storage after reconstitution. Reconstituted retatrutide must be refrigerated. It degrades at room temperature and is destroyed by freezing. Shelf life after reconstitution is typically two to four weeks under refrigeration. The how to store retatrutide guide covers temperature requirements, light exposure, and shelf life in detail. The does GLP-1 have to be refrigerated guide addresses the broader cold-chain question for travel and logistics.
If you are managing your budget alongside your protocol, the retatrutide cost and pricing guide covers the economics of different vial sizes and sourcing strategies. The peptide cost calculator helps you compare per-dose costs across different vial configurations.
Why women experience stronger GI side effects and how to manage them
The pharmacological reason women feel it harder
The nausea is real. The data is clear. Women experience gastrointestinal side effects at approximately 2.5 times the rate of men on equivalent retatrutide doses. This is not a tolerance issue or a psychological response to injections. It is pharmacology.
Here is the mechanism. Women clear GLP-1 agonists more slowly than men. Slower clearance means the drug stays active in the system longer. Longer active duration means higher sustained receptor stimulation between injections. GLP-1 receptors in the gut mediate gastric emptying, intestinal motility, and nausea signaling. When those receptors are stimulated more persistently, GI effects intensify.
The practical implication is straightforward: a dose that feels tolerable for a man may be genuinely too much for a woman of equivalent weight. This is not a reason to avoid retatrutide. It is a reason to escalate more slowly, to take GI management seriously from day one, and to understand that a rough week does not mean the drug is not working or is not right for you. The retatrutide diarrhea guide covers one of the most common and disruptive GI symptoms in detail.
Managing nausea from day one: timing, meals, and hydration
Managing GI side effects during titration starts before the injection.
Injection timing affects nausea intensity significantly. Many women find that evening injection before sleep reduces conscious nausea experience because peak drug activity occurs overnight. Some find morning injection preferable because they can eat a small meal two hours prior. There is no universal answer. The best time to take retatrutide discusses both approaches and helps you identify which pattern fits your physiology and schedule.
Meal composition matters enormously. High-fat meals dramatically worsen nausea on GLP-1 agonists because gastric emptying is already slowed by the drug. The gut is being asked to move food more slowly than normal, and rich fatty meals compound that effect. Small, low-fat, easily digestible meals spaced throughout the day are far better tolerated than two large meals. The GLP-1 friendly meals guide, GLP-1 breakfast ideas, and GLP-1 recipes for weight loss give you practical templates.
Hydration is consistently underappreciated. Dehydration worsens nausea independently of the drug. On retatrutide, reduced appetite means reduced fluid intake from food. Many women drink less water than usual because they are eating less. Electrolyte balance shifts when you are in significant caloric restriction. The best electrolytes for GLP-1 users guide covers the specific electrolyte needs during active weight loss phases.
Constipation, reflux, and when to hold your dose
For constipation, which hits a meaningful percentage of women on retatrutide due to slowed gastric motility, fiber supplementation is first-line management before any pharmaceutical interventions. The best fiber supplement for GLP-1 users reviews the options. The GLP-1 constipation relief guide covers the management hierarchy, and the semaglutide constipation treatment guide and tirzepatide constipation treatment guide provide comparative management frameworks that translate to retatrutide.
Acid reflux and bloating are common during escalation. The semaglutide acid reflux guide, semaglutide bloating guide, and heartburn on tirzepatide guide all describe mechanisms and management strategies that apply across GLP-1 class drugs including retatrutide. Sulfur burps, which many women report and find particularly distressing, are addressed in the sulfur burps on GLP-1 guide.
If nausea and GI symptoms feel unbearable at a particular dose level, the correct move is to hold at that dose longer, not to push through to the next escalation. The four-week increment is a minimum. Extending a tier to six or eight weeks while GI symptoms stabilize is clinically sensible and does not compromise long-term outcomes. The retatrutide microdosing guide explores an alternative approach of very gradual micro-increments for people with high GI sensitivity.
For women who experience significant fatigue alongside GI symptoms, which often occurs in the first two weeks after each escalation, the does retatrutide make you tired guide and GLP-1 fatigue complete guide explain the mechanism and offer practical management strategies.
Two symptoms deserve specific mention for women: dizziness and headaches. Both are more common during escalation, and both are frequently tied to dehydration and electrolyte shifts rather than direct drug toxicity. The semaglutide dizziness guide and GLP-1 headache complete guide address both in detail.
Hormonal considerations every woman should understand
Menstrual cycle, estrogen, and PCOS effects
This section is the one most women wish existed before they started. Hormonal effects of retatrutide are real, significant in some cases, and almost entirely manageable when you know what to expect.
Menstrual cycle changes
Menstrual disruption is among the most commonly reported female-specific effects of GLP-1 agonists as a class. Cycles may become shorter, longer, heavier, lighter, more irregular, or temporarily absent. The mechanism is multifactorial. Rapid weight loss alters sex hormone binding globulin levels, which affects free estrogen and progesterone availability. Caloric restriction, even moderate restriction, signals the hypothalamic-pituitary-ovarian axis to modulate reproductive function. And as body fat decreases, the peripheral estrogen production that fat tissue provides through aromatization decreases with it.
Most women normalize within three to six months, even if they continue losing weight. The first three months after starting or escalating retatrutide are the most likely period for disruption. Tracking your cycle carefully during this period gives you useful data. The does semaglutide affect your period guide and does tirzepatide affect your period guide document the same mechanisms across the GLP-1 class, and those findings translate directly to retatrutide.
Estrogen levels and body fat loss
Fat tissue is not inert storage. It actively converts androgens to estrogens through the enzyme aromatase. When you lose 20 to 30 percent of body weight on retatrutide, you are reducing a meaningful estrogen source. For postmenopausal women who are not on hormone replacement therapy, this reduction can accelerate some symptoms of estrogen deficiency: vaginal dryness, sleep disruption, skin changes, joint aches. The does semaglutide increase estrogen levels guide explores the estrogen-weight-loss relationship in depth.
If you are on hormone replacement therapy, the interaction is worth discussing with your prescriber. The HRT and GLP-1 together guide covers the pharmacological interactions, absorption considerations, and monitoring recommendations for women managing both simultaneously.
PCOS
Women with polycystic ovary syndrome represent one of the populations that may benefit most from retatrutide. PCOS is characterized by insulin resistance, elevated androgens, irregular ovulation, and often significant difficulty with weight management. GLP-1 agonists address the insulin resistance mechanism directly, and several studies have documented period regularization in women with PCOS on GLP-1 therapy. The PCOS and tirzepatide guide covers the mechanisms in detail using the most closely related molecule. Women with PCOS may find that their cycles become more regular on retatrutide, not less, particularly after the initial adjustment period. SeekPeptides has dedicated PCOS-specific protocol resources for women navigating retatrutide alongside insulin resistance management.
Fertility, contraception, breastfeeding, and libido
Fertility considerations
Retatrutide is not approved for use during pregnancy or while attempting to conceive. The practical complexity is that weight loss, insulin sensitivity improvements, and cycle regularization on GLP-1 agonists can increase fertility, sometimes unexpectedly. Women who had irregular cycles and assumed low fertility risk should not make that assumption on retatrutide. The semaglutide while trying to conceive guide and does semaglutide increase fertility guide are essential reading for any woman in reproductive years. The what happens if you get pregnant on tirzepatide guide addresses the real-world scenario of unintended pregnancy during GLP-1 use.
Contraceptive efficacy is a related consideration. GLP-1 agonists slow gastric emptying, which can reduce absorption of oral contraceptives. If you are relying on oral contraception while on retatrutide, barrier backup is a reasonable precaution, particularly during dose escalation periods when gastric motility effects are most pronounced.
Breastfeeding
Retatrutide has not been studied in breastfeeding women. By extension of GLP-1 class data, it is not recommended. The tirzepatide while breastfeeding guide, can you take GLP-1 while breastfeeding guide, and GLP-1 postpartum guide provide the current evidence base and clinical guidance for the postpartum period.
Libido and sexual function
Improved metabolic health, reduced inflammation, and weight loss itself generally improve sexual function and libido in women. The semaglutide and sex drive in women guide and tirzepatide sexual side effects guide document this pattern. However, in the early phases when GI side effects, fatigue, and caloric restriction are most significant, some women report temporary reductions in libido. This typically resolves as the body adapts and energy levels stabilize.
Breast cancer screening
Women with a personal or family history of hormone-sensitive cancers should discuss GLP-1 use with their oncologist. The GLP-1 and breast cancer guide covers the current evidence on the relationship between GLP-1 agonists and breast cancer risk, which is an area of active research.
Body composition and muscle preservation for women on retatrutide
Why muscle matters more than the number on the scale
Weight loss and fat loss are not the same thing. This distinction matters enormously for women on retatrutide because the scale will move faster than you expect, and some of what moves will be lean mass if you do not actively protect it.
In the Phase 2 trial, the majority of weight lost was fat mass. But lean mass loss occurred too, particularly in participants who did not maintain adequate protein intake or resistance training. For women, muscle preservation matters beyond aesthetics. Muscle mass directly supports insulin sensitivity, bone density signaling, metabolic rate, and functional capacity. Losing significant lean mass during a retatrutide course undermines the long-term metabolic benefit of the weight loss itself.
Think about what that means practically. A woman who loses 25 percent of body weight on retatrutide but loses 30 percent of that from lean mass will end the protocol with a compromised metabolic rate. She will burn fewer calories at rest. She will have less insulin-sensitive tissue. She will be at greater risk of weight regain when the drug stops. The does retatrutide cause muscle loss guide covers the mechanism and mitigation strategies in depth. The goal is not just smaller. The goal is metabolically healthier.
That means the conversation around retatrutide for women should always include protein, training, and supplementation from week one, not as an afterthought once the weight starts moving.
Protein targets and practical strategies when appetite is suppressed
Protein is the primary lever. The standard recommendation for weight-loss phases with GLP-1 agonists is 1.2 to 1.6 grams of protein per kilogram of target body weight per day. On retatrutide, appetite suppression is profound. Getting adequate protein when you are genuinely not hungry requires deliberate strategy. High-protein foods first at every meal, protein-forward snacks when you can tolerate them, and potentially protein shakes in formats that are easy on a nauseous stomach. The how much protein on semaglutide guide provides the framework that applies across GLP-1 compounds.
Practical examples matter here. A woman with a target body weight of 65 kilograms needs roughly 78 to 104 grams of protein daily at the 1.2 to 1.6 gram range. When appetite is heavily suppressed, that becomes a deliberate project rather than a natural outcome. Greek yogurt with 15 to 17 grams per serving, eggs with 6 grams each, cottage cheese with 25 grams per cup, and whey protein isolate with 25 to 30 grams per scoop are the most efficient delivery mechanisms. Front-loading protein at breakfast and lunch, before appetite suppression peaks later in the day, is a practical scheduling strategy many women find effective.
Tracking matters during the early titration phase. Not obsessively, but deliberately. Four weeks of protein logging gives you real data about whether you are actually hitting your target or just assuming you are. The gap between perceived intake and actual intake on significant caloric restriction is usually larger than most people expect. Once you have established reliable protein habits, tracking can be deprioritized. SeekPeptides members access female-specific nutrition protocols and protein target calculators designed specifically for the appetite suppression phases of GLP-1 titration.
Resistance training, bone density, and supplements
Resistance training is the second lever. You cannot fully protect lean mass through protein alone without the stimulus that tells the body to preserve it. Even two sessions per week of compound resistance movements is meaningfully better than none. The can you build muscle while on GLP-1 guide and semaglutide and exercise guide cover the training and nutrition interaction in the context of GLP-1 use. For women interested in body recomposition alongside weight loss, the retatrutide bodybuilding guide explores advanced protocols combining retatrutide with resistance training programs.
The specific training approach matters less than consistency. Two full-body sessions per week of compound movements such as squats, deadlifts, rows, and presses deliver more lean mass protection per hour than any isolation-focused routine. Women who are new to resistance training can start with bodyweight movements and progress to loaded versions as strength develops. The caloric deficit from retatrutide already does significant work for fat loss. Training does not need to add to the deficit. Its job is to signal lean mass preservation.
Creatine supplementation during a retatrutide course has genuine evidence behind it for lean mass preservation. It supports strength output during caloric restriction, which maintains training quality, which protects lean mass. The standard dosing of 3 to 5 grams daily of creatine monohydrate does not require loading. It is safe, inexpensive, and one of the most studied supplements in existence. The creatine and GLP-1 guide covers the evidence base and practical use.
For women specifically, the relationship between fat loss, estrogen reduction, and bone density deserves attention. Bone is sensitive to mechanical loading, managed with exercise, and estrogen levels, which change with fat loss as described in the hormonal section above. Weight-bearing exercise provides the mechanical loading signal. Calcium at 1,000 to 1,200 mg daily and vitamin D at 1,500 to 2,000 IU daily are baseline supplements for any woman in significant caloric restriction who is also reducing the estrogen-producing fat tissue. The supplements to take with GLP-1 guide provides the full evidence-ranked list of supplements worth considering during active retatrutide use.
Hair loss is a side effect that disproportionately distresses women and is worth addressing directly here. Telogen effluvium, the type of hair loss associated with GLP-1 agonists, is triggered by metabolic stress during rapid weight loss rather than by the drug directly. It is typically temporary. The GLP-1 hair loss complete guide and does retatrutide cause hair loss guide both explain the mechanism and the management approach, which centers on adequate nutrition and patience rather than stopping the medication.
Body composition tracking during retatrutide is more informative than scale weight alone. DEXA scans, bioelectrical impedance, or even consistent tape measurements give you a clearer picture of whether you are losing fat versus lean mass. Tracking this over time, alongside protein intake and training volume, gives you the data to adjust your protocol before significant lean mass loss occurs rather than after. A rough rule: if your scale weight is dropping faster than 1 percent of body weight per week over multiple weeks, investigate whether protein intake and training volume are adequate before concluding that faster is better.
Common dosing mistakes women make with retatrutide
Starting and escalation errors
Most protocol failures come from the same handful of errors. Knowing them in advance lets you avoid them.
Mistake 1: Starting too high because results feel urgent
The trial data is impressive enough that some women start at 4mg or 6mg to accelerate outcomes. The GI consequences are severe. Remember that women experience GI side effects at 2.5 times the rate of men on equivalent doses. Starting above 2mg dramatically increases the probability of nausea severe enough to compromise nutrition and cause early dropout. Start at 2mg. The four-week investment in tolerability pays dividends for the remaining 40+ weeks of your protocol. The starting dose of retatrutide guide walks through the reasoning in detail.
This is not a small risk. Women who begin at 4mg or higher frequently report nausea that lasts four to seven days after each injection, forcing them to eat far below any reasonable caloric floor. The resulting lean mass loss, dehydration, and fatigue create a negative feedback loop that leads many to abandon the protocol entirely in the first month. Starting at 2mg and spending four weeks building tolerance is not a concession. It is the strategy most likely to produce a successful 12-month outcome.
Mistake 2: Escalating on schedule regardless of symptoms
The four-week escalation schedule is a framework, not a mandate. If week three of any tier still brings meaningful nausea or GI disruption, extending that tier to five or six weeks is smarter than pushing to the next dose on schedule. The faster you escalate, the more likely you are to hit a dose that causes dropout. Slower is not failure. It is strategy. Review how much retatrutide to take for guidance on individual response-based dosing decisions.
Mistake 3: Assuming maximum dose means maximum results
Women in the Phase 2 trial outperformed men across all dose groups. Many women achieve their weight loss targets at 6mg or 8mg without needing to push to 12mg. Evaluating your response at each tier, rather than automatically escalating to the maximum, is both safer and potentially equally effective. The how long does retatrutide last guide helps you understand the pharmacokinetic window at each dose level.
A useful benchmark: if you have lost 20 percent or more of starting body weight, if your appetite is well-controlled, and if you are tolerating the current dose without significant GI burden, there is no clinical imperative to escalate further. Women who hold at 8mg for 20 weeks can achieve outcomes comparable to men at 12mg because of the superior female pharmacological response. More drug is not always better drug. It is always more side effects.
Nutrition, hormonal, and technique errors
Mistake 4: Not protecting lean mass
Appetite suppression is profound on retatrutide. Many women eat 600 to 900 calories daily during peak appetite suppression without trying to restrict. Severe caloric deficit without adequate protein is a reliable formula for muscle loss. Prioritize protein at every eating opportunity, even small ones. Track it if necessary. The how many calories on semaglutide guide gives you the floor caloric targets that prevent metabolic adaptation and lean mass loss.
The 600-calorie floor matters. Consistently eating below roughly 600 to 800 net calories triggers metabolic adaptation mechanisms that reduce resting metabolic rate and accelerate lean mass breakdown. Retatrutide does not protect against this. The drug suppresses appetite. It does not tell your body what to do with the resulting deficit. That is your job, managed through deliberate protein intake and resistance training even when hunger is essentially absent.
Mistake 5: Ignoring hormonal signals
Missed periods, significant cycle irregularity, or symptoms of estrogen deficiency during rapid weight loss should be communicated to a healthcare provider. They are not inevitable or irreversible, but they do warrant attention rather than being treated as an acceptable side effect to push through. A menstrual cycle absent for more than three consecutive months warrants a laboratory workup. This is the point where FSH, LH, estradiol, and thyroid markers give you the data to make an informed decision about whether to continue escalating, hold your dose, or modify your caloric intake to reduce the metabolic stress signal to the hypothalamic-pituitary-ovarian axis.
Women on retatrutide who are also managing thyroid conditions should be particularly attentive here. Rapid weight loss alters thyroid hormone binding and can shift free T3 and T4 levels in ways that require medication dose adjustment. If you are on levothyroxine or other thyroid medications, periodic thyroid panel checks during active weight loss phases are clinically prudent.
Mistake 6: Inconsistent injection timing
Because women clear GLP-1 agonists more slowly, the trough concentration before the next injection is higher relative to men. This means the concentration fluctuation from inconsistent timing is amplified. Inject on the same day each week, at roughly the same time. Use a tracking system. The how to track GLP-1 injections guide offers several tracking approaches for different organizational styles.
Mistake 7: Poor reconstitution technique
Errors in reconstitution math lead to dosing errors. Vigorous shaking degrades the peptide. Contamination from non-sterile technique compromises the vial. The retatrutide reconstitution chart and the retatrutide peptide dosage chart and the peptide reconstitution calculator eliminate math errors. Proper handling technique, including gentle swirling rather than shaking and sterile needle practice, eliminates the other failure modes.
Two technique specifics matter most. First, inject the BAC water slowly into the vial at an angle so it runs down the glass wall rather than hitting the powder directly. Direct streams create foaming that denatures the peptide. Second, allow the powder to dissolve by gravity and gentle swirling over two to three minutes. Do not rush it. A partially reconstituted vial produces an inconsistent concentration at every draw.
Mistake 8: Not planning for the skin sensitivity side effect
Skin sensitivity and injection site reactions are reported by a meaningful percentage of retatrutide users. The retatrutide skin sensitivity guide and GLP-1 injection site reaction guide cover management strategies. Rotating sites consistently and warming the injection area slightly before injecting both reduce local reactions.
When to hold, reduce, or increase your dose
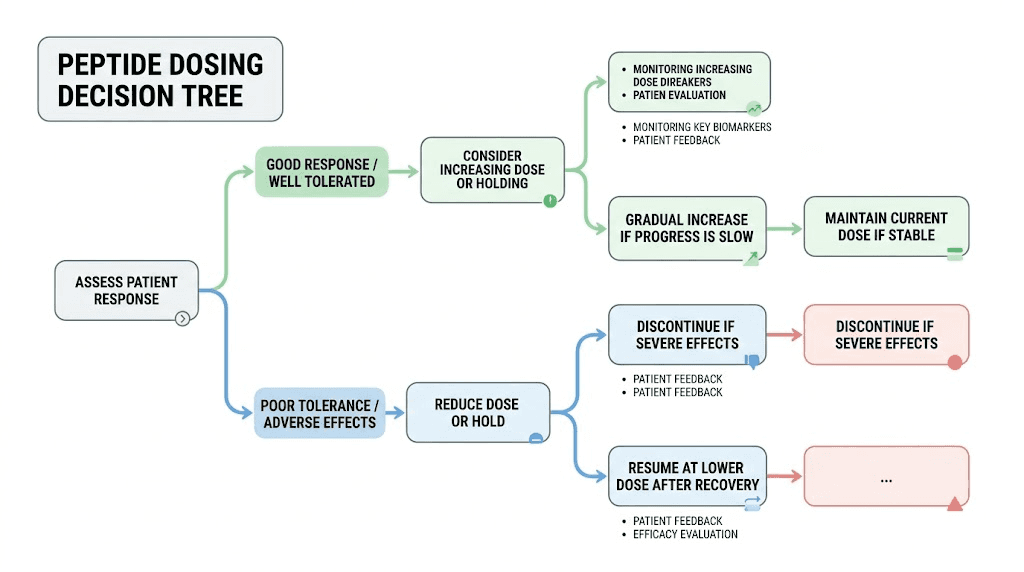
Hold and reduce scenarios: recognizing the signals
The titration schedule gives you a structure. Real life requires judgment calls within that structure. Here is how to make them.
When to hold your current dose (do not escalate yet)
Hold your current dose if nausea, vomiting, or diarrhea is interfering with your ability to eat adequate protein. Hold if GI symptoms are affecting sleep or work performance. Hold if you are in a high-stress period or have recently been ill, as these states exacerbate GI side effects. Hold if you have not been stable at the current dose for at least three weeks. Holding is not retreat. It is building the tolerability foundation for sustainable escalation.
A practical rule for the hold decision: if you are experiencing nausea that causes you to avoid food for more than 24 hours in a given week, that is a hold signal. If you are losing more than 2 percent of body weight per week over more than two consecutive weeks, that is a hold signal too, because the deficit is likely too aggressive for lean mass preservation regardless of how motivated you feel. The protocol needs to be sustainable for a year or more. Aggressive early escalation that compromises nutrition and produces dropout is not superior to gradual escalation that produces a completed 12-month course.
When to reduce your dose
Reduce if you have escalated and experienced persistent vomiting across more than four days. Reduce if you are unable to maintain adequate hydration or nutrition at the current dose. Reduce if you have experienced a medical event, surgery, or illness that has compromised your baseline state. A dose reduction of one tier, held for six to eight weeks before re-escalation, is a legitimate clinical approach. It is not failure and it does not indicate the drug is not working for you.
Dose reductions are underutilized. Women who push through unbearable side effects at a new dose tier often develop a negative psychological association with injections that undermines long-term adherence. Stepping back a tier and spending two extra months building tolerance before re-escalating produces better long-term outcomes than powering through three weeks of daily nausea. The clinical goal is the 12-month result, not the week-eight milestone.
The GLP-1 stall guide addresses the weight loss plateau scenario, which is distinct from the tolerability scenario but sometimes leads women to make dose changes for the wrong reasons. A stall in weight loss does not necessarily mean your dose is too low. Metabolic adaptation is the more common explanation, and dose escalation is not always the correct response. Before escalating to address a stall, audit protein intake, training volume, and overall caloric intake first. A stall at 1,500 calories daily with adequate protein is a different problem than a stall at 900 calories. They require different solutions.
Increase criteria and absolute hold situations
When to increase your dose
Increase when you have been stable at the current dose for at least four weeks with tolerable or no GI symptoms. Increase when appetite suppression has diminished significantly and weight loss has stalled for more than four weeks at an adequate caloric intake. Increase when you and your healthcare provider agree that incremental clinical benefit justifies the incremental side effect burden of a higher dose. Review the how long does retatrutide take to work guide and the how long for retatrutide to suppress appetite guide to calibrate your expectations about timeline before making escalation decisions based on impatience rather than data.
A note on the weight loss stall as an escalation trigger: stalls of two to three weeks in duration are extremely common during dose transitions and do not indicate inadequate dose. The body is recalibrating. A stall of six or more weeks at a stable caloric intake, after confirming protein targets are being met and training volume is consistent, is a more legitimate escalation signal. Chasing the scale week by week with dose increases is a pattern that usually ends in side effect overload rather than better outcomes. The GLP-1 average weight loss per month guide shows what realistic timelines look like across the full titration arc, and the GLP-1 maintenance dose guide covers the longer-term dose strategy once you reach your target weight.
Absolute hold situations
Pregnancy or suspected pregnancy is an absolute hold. Active pancreatitis is an absolute hold. Decompensated thyroid disease is an absolute hold. If you experience abdominal pain that radiates to the back, with or without nausea, seek immediate medical attention, as this is a potential sign of pancreatitis, which is a rare but serious adverse event associated with GLP-1 class medications.
Gallbladder disease is worth flagging separately. Rapid weight loss accelerates gallstone formation. GLP-1 agonists have an independent association with cholecystitis. Women are already at higher baseline risk for gallbladder disease than men. The combination of female sex, rapid weight loss, and GLP-1 use means right-upper-quadrant pain should prompt evaluation rather than self-management. If you have a known history of gallstones, discuss prophylactic ursodeoxycholic acid with your prescriber before beginning a retatrutide course.
The getting off GLP-1 guide covers the discontinuation process if you need to stop retatrutide for any reason, including tapering strategies that minimize weight regain and hormonal disruption.
Comparing retatrutide to other GLP-1 options for women
Retatrutide vs semaglutide and tirzepatide: the outcome gap
Understanding where retatrutide fits in the current landscape of weight-loss pharmacology helps you evaluate whether it is the right choice for your situation and what to expect if you are transitioning from another medication.
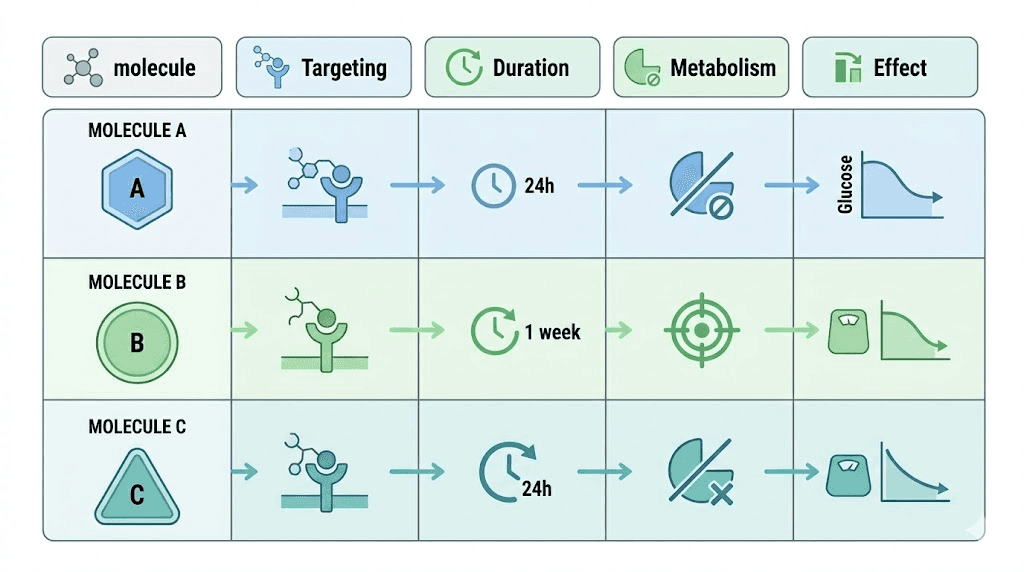
Retatrutide vs semaglutide
Semaglutide is a GLP-1 monoagonist. Retatrutide adds GIP and glucagon agonism to the GLP-1 mechanism. The weight loss outcomes are not comparable. Semaglutide achieves roughly 15 to 17 percent weight loss in phase 3 data. Retatrutide achieves up to 28.7 percent. For women specifically, this gap is even larger given the superior female response to triple agonism documented in the Phase 2 data. The retatrutide vs semaglutide comparison and semaglutide vs tirzepatide vs retatrutide guide break down the mechanism and outcome differences in depth. The semaglutide vs tirzepatide calculator and semaglutide dosage calculator are useful tools if you are comparing protocols.
For women who have already been on semaglutide and achieved the ceiling of their results, retatrutide offers a biologically distinct mechanism rather than just a higher dose of the same thing. The glucagon receptor component drives hepatic glucose production and lipolysis through a pathway that semaglutide does not touch. That is why the weight loss curves are genuinely different, not just incrementally better.
Retatrutide vs tirzepatide
Tirzepatide is a dual GLP-1 and GIP agonist. It is currently FDA-approved under the brand name Mounjaro for diabetes and Zepbound for obesity. Tirzepatide achieves 20 to 22 percent weight loss in phase 3 data, making it a more direct comparison to retatrutide than semaglutide. Retatrutide adds glucagon agonism, which contributes additional lipolysis and hepatic fat reduction beyond what tirzepatide achieves. The is retatrutide better than tirzepatide guide and retatrutide vs Mounjaro comparison analyze the outcome data and side effect profiles side by side.
For women who have plateaued on tirzepatide at 10 or 15mg, the transition to retatrutide is one of the most clinically rational next steps available. The GIP component already provides some receptor tolerance overlap, but the glucagon agonism is entirely new territory. Many women report meaningfully different hunger suppression patterns on retatrutide compared to tirzepatide, with particularly strong effects on food reward and cue-triggered eating rather than just basal appetite. If you are transitioning from tirzepatide, the starting dose and escalation strategy for retatrutide differs from naive initiation. The switching from tirzepatide to retatrutide guide, retatrutide dosage schedule after high-dose tirzepatide, and how long retatrutide takes to work after tirzepatide guide cover this transition in detail. The tirzepatide dosing guide provides the framework for where you would be starting from.
Retatrutide vs ozempic
Ozempic is the brand name for semaglutide in its injectable form. The mechanism comparison is identical to the semaglutide section above. The Ozempic vs retatrutide guide covers the practical comparison including approval status, availability, and cost differences.
Newer comparators and availability considerations
Cagrilintide and mazdutide are emerging candidates in the weight-loss pharmacology space. The cagrilintide vs retatrutide comparison and mazdutide vs retatrutide comparison cover the mechanism and early outcome data for both. Some protocols combine cagrilintide with retatrutide for additive effect. The cagrilintide dosage with retatrutide guide covers the combination protocol. The combining tesamorelin and retatrutide guide explores another advanced combination approach.
For women deciding between options in 2025 and 2026, the decision framework generally looks like this. Semaglutide is the entry point for women new to GLP-1 pharmacology who want an FDA-approved option with the longest safety record. Tirzepatide represents the step up when semaglutide results plateau or when insulin resistance is a primary concern given its GIP mechanism. Retatrutide is the logical choice for women who want maximum fat loss outcomes and are willing to manage a more demanding titration process with more assertive GI side effect management. SeekPeptides provides detailed comparison resources and calculators to help you work through which option fits your specific situation, history, and goals.
Retatrutide is not yet FDA-approved at the time this guide was written. It is available through research peptide channels. The retatrutide availability guide, retatrutide online guide, and retatrutide buying guide address sourcing. The best place to buy retatrutide and cheap retatrutide sourcing guide cover the economics. For larger quantity needs, the bulk retatrutide guide covers volume purchasing considerations.
For the broader context of peptide-based fat loss options beyond the GLP-1 class, the peptides for fat loss guide and best peptides for weight loss guide provide a comparative framework. The peptides for anti-aging guide is relevant for women interested in the longevity applications of peptide protocols alongside weight management.
Frequently asked questions
Dosing, timing, and calculation questions
What is the correct starting dose of retatrutide for a woman?
The correct starting dose is 2mg once weekly, subcutaneous injection. This is true regardless of body weight, prior GLP-1 experience, or how urgent your goals feel. Women experience GI side effects at approximately 2.5 times the rate of men on equivalent doses. Starting at 2mg builds the tolerability foundation that allows successful long-term escalation. See the starting dose of retatrutide guide for the complete rationale.
Do women lose more weight on retatrutide than men?
The Phase 2 trial data indicates yes. Women in the highest dose groups lost 28.5 percent and 26.6 percent of body weight at 48 weeks, compared to 19.8 percent and 21.9 percent for men in the same groups. This pattern is consistent with broader GLP-1 research showing women achieving approximately 11 percent greater relative weight loss than men across studies. The mechanism relates to slower drug clearance in women and potentially different receptor sensitivity patterns. The GLP-1 average weight loss per month guide shows timeline expectations.
Female-specific hormonal and health questions
Will retatrutide affect my menstrual cycle?
Possibly, particularly in the first three to six months. Cycles may become shorter, longer, heavier, lighter, irregular, or temporarily absent. The mechanism involves changes in sex hormone binding globulin from rapid weight loss, reduced peripheral estrogen production from fat tissue reduction, and hypothalamic-pituitary-ovarian axis response to caloric restriction. Most women normalize within three to six months. Women with PCOS often see improvements in cycle regularity. Consult your healthcare provider if cycles are absent for more than three months or if you are planning pregnancy. The does tirzepatide affect your period guide documents the same mechanism.
Can I take retatrutide while on birth control pills?
Retatrutide slows gastric emptying, which can reduce the absorption of oral contraceptives. This is a theoretical reduction in contraceptive efficacy. Barrier backup during dose escalation phases is a reasonable precaution. Discuss with your prescriber if you have concerns about contraceptive efficacy. Injectable or intrauterine contraceptive methods are not affected by gastric motility changes.
How do I calculate my dose in units?
The formula is: Units = (Dose in mg / Total mg in vial) x Total mL of BAC water added x 100. For example, a 4mg dose from a 10mg vial reconstituted with 2mL BAC water equals 80 units. The retatrutide dosage calculator and peptide reconstitution calculator handle this automatically for any vial and dose combination.
Is it safe to take retatrutide if I am on hormone replacement therapy?
There are no documented contraindications between retatrutide and HRT at present. The HRT and GLP-1 together guide covers the interaction data and monitoring recommendations. Discuss with your prescriber, particularly if you are on oral HRT, as gastric motility changes may affect absorption.
How long before retatrutide starts working for women?
Appetite suppression typically begins within the first week at the 2mg starting dose, though it is mild at this stage. Meaningful weight loss usually becomes apparent by weeks four to eight. The most significant appetite suppression effect develops as you escalate through the titration schedule. The how long for appetite suppression guide and how long GLP-1 takes to start working guide cover the timeline in detail.
Should I take retatrutide with food?
Retatrutide does not require food for absorption as a subcutaneous injection. However, injection timing relative to meals can affect nausea. Many women find that injecting in the evening before sleep minimizes conscious nausea experience. Others find small pre-injection meals helpful. The best time to take retatrutide guide explores both approaches. Avoid large fatty meals on or around injection day, as these dramatically worsen GI symptoms.
What happens to my results if I stop taking retatrutide?
Weight regain after stopping GLP-1 agonists is well-documented. The drug suppresses appetite and drives weight loss through pharmacological mechanisms that reverse when the drug is discontinued. The getting off GLP-1 guide covers tapering strategies and the lifestyle adjustments that minimize regain. The GLP-1 maintenance dose guide covers the option of low-dose maintenance to preserve results long-term.
Is the intranasal form of retatrutide an option for women who dislike injections?
Intranasal retatrutide is an area of active research but is not established as an equivalent alternative to subcutaneous injection in terms of pharmacokinetics or efficacy. The intranasal retatrutide guide covers the current evidence and status. Subcutaneous injection remains the standard delivery method with the documented efficacy data.
Nutrition, supplementation, and long-term use questions
What supplements should I take alongside retatrutide?
At minimum, protein optimization and electrolyte management are essential. Evidence-supported additions include fiber supplementation for GI motility, creatine for lean mass preservation, and a comprehensive multivitamin to address micronutrient gaps from reduced food intake. The supplements to take with GLP-1 guide provides an evidence-ranked list with dosing guidance.
Will I lose my hair on retatrutide?
Some women experience telogen effluvium, a diffuse shedding of hair triggered by metabolic stress during rapid weight loss. It is typically temporary and not caused directly by the drug itself. Most women see regrowth within three to six months of weight stabilization. Adequate protein intake is the primary mitigation strategy. The GLP-1 hair loss guide and does retatrutide cause hair loss guide cover the mechanism and management in detail.
Can I see before and after results from women specifically?
The Phase 2 and Phase 3 trial data provides population-level results. The before and after GLP-1 guide documents real-world outcome ranges across the GLP-1 medication class. Female-specific outcomes are embedded in the clinical data reviewed throughout this guide.
How does retatrutide interact with alcohol for women?
Alcohol consumption on retatrutide requires more attention than many women expect. First, gastric emptying is already slowed. Alcohol absorbed through a stomach that empties more slowly reaches the bloodstream differently than normal, and blood alcohol levels can be less predictable. Second, alcohol is a significant source of empty calories that bypasses the appetite suppression mechanism entirely. You can consume substantial calories from alcohol without triggering the satiety signaling that retatrutide enhances for food. Third, alcohol worsens nausea for many women on GLP-1 agonists, particularly during escalation phases. None of this means total abstinence is required. It means understanding the interaction and planning around it. Reducing alcohol during active escalation phases is the most practical approach, shifting to moderate consumption once you are stable at your maintenance dose.
What is the difference between retatrutide and CagriSema for women?
CagriSema is a combination of cagrilintide (an amylin analog) and semaglutide. It represents a different mechanistic approach than retatrutide, combining amylin and GLP-1 agonism rather than GLP-1, GIP, and glucagon agonism. Early Phase 3 data for CagriSema shows weight loss outcomes in the 22 to 25 percent range, which is closer to tirzepatide than retatrutide. For women specifically, the GIP and glucagon components in retatrutide appear to drive superior fat mass reduction compared to amylin-based combinations, based on available data. That said, CagriSema is further along the FDA approval pathway at the time of writing. The mechanistic differences, side effect profiles, and availability considerations all factor into the decision. For an updated comparison, the cagrilintide vs retatrutide comparison covers the head-to-head data.
Can I use the retatrutide peptide dosage chart to plan my full titration schedule in advance?
Yes, and doing so before you start is one of the best protocol preparation steps you can take. The retatrutide peptide dosage chart gives you pre-calculated unit values for every dose tier across common vial sizes. Planning your full titration sequence before starting, including the number of vials you will need for each tier, prevents the common problem of running out of supply mid-protocol and facing an unplanned gap in dosing. A complete 48-week protocol at standard titration pace requires roughly three to four 20mg vials at minimum, depending on how long you hold at each tier. Factor this into your supply planning from the beginning. The retatrutide reconstitution chart complements the dosage chart by showing the optimal BAC water volumes for each vial size to produce the most practical injection volumes.
External resources
Phase 2 Retatrutide Trial - New England Journal of Medicine, the primary clinical source for retatrutide efficacy and safety data including sex-stratified outcomes.
Sex differences in GLP-1 pharmacokinetics and response - PubMed, research documenting female-specific clearance rates and GI side effect burden across GLP-1 agonists.
Endocrine Society - Obesity and hormonal interactions, authoritative clinical guidance on endocrine changes during significant weight loss in women.
ACOG - Obesity and reproductive health, evidence-based guidance on weight management medications and reproductive considerations for women.
American Diabetes Association - GLP-1 receptor agonists, clinical framework for GLP-1 agonist use including monitoring recommendations.
Managing a protocol as powerful as retatrutide requires accurate information, and accurate information about female-specific dosing has been genuinely difficult to find. The data is clear that women respond exceptionally well to this medication. The data is equally clear that women need different titration pacing, proactive GI management, and hormonal awareness to use it safely and sustainably. SeekPeptides members get access to detailed female-specific protocols, dosing calculators, and updated guidance as the Phase 3 data continues to mature. If you are navigating retatrutide without a prescriber who understands GLP-1 pharmacology in women, the resources there can fill significant gaps in your knowledge base and your protocol confidence.
In case I do not see you, good afternoon, good evening, and good night. May your titration stay smooth, your results stay sustained, and your protocol stay working for you.