Mar 5, 2026

Experienced researchers know something about retatrutide that most dosing guides completely ignore. The official answer to "when should I take it?" is deceptively simple: any time that works for you, once per week. And technically, that is correct. Retatrutide has an approximate half-life of six days, which means the compound maintains relatively stable blood levels regardless of whether you inject at dawn or midnight. But the researchers who have been through multiple GLP-1 protocols, who have tried semaglutide, tirzepatide, and now retatrutide, will tell you something different. Timing does not change the drug. Timing changes your experience with the drug.
The difference between injecting at the right time versus the wrong time is not measured in pounds lost or receptor activation. It is measured in nausea managed, sleep preserved, workouts maintained, and social events enjoyed. When you are dealing with a triple-receptor agonist that hits GLP-1, GIP, and glucagon pathways simultaneously, the side effect profile during those first 24 to 48 hours after injection matters enormously. Understanding how incretin-class side effects work provides useful background. And how you navigate those hours depends entirely on when you choose to start the clock.
This guide covers every angle of retatrutide timing that actually affects your daily life. From the pharmacokinetics that explain why once-weekly dosing works, to the practical strategies for aligning injections with your schedule, meals, exercise routine, and sleep patterns. SeekPeptides members have shared hundreds of protocol adjustments over time, and injection timing remains one of the simplest changes that yields the biggest improvements in tolerability. Whether you are just starting your first retatrutide dose or adjusting timing mid-protocol, the information here applies across every dose in the retatrutide dosage chart.
Understanding retatrutide pharmacokinetics and why timing is flexible
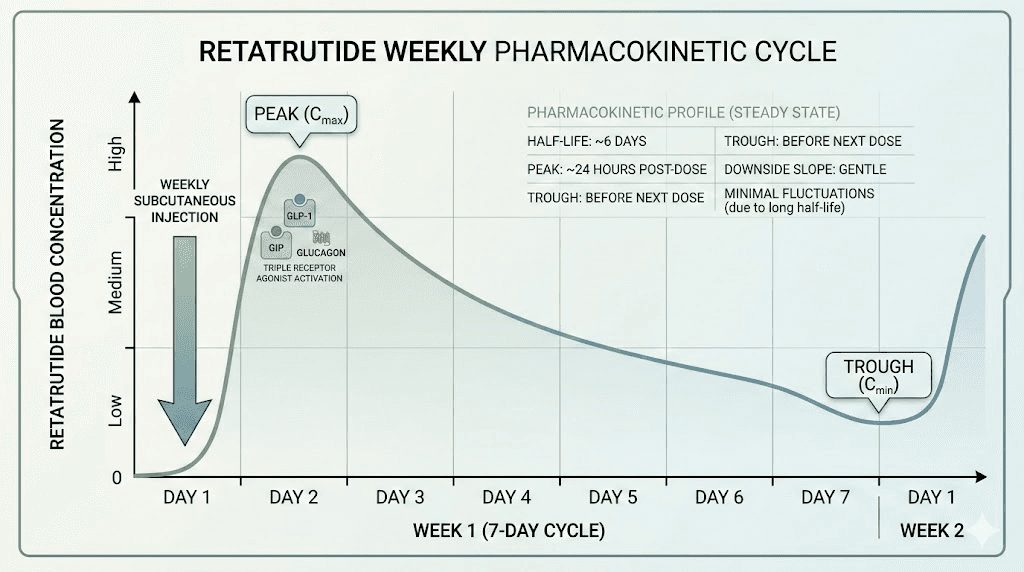
Before diving into practical timing strategies, it helps to understand why retatrutide allows such flexibility in the first place. Unlike medications that require precise timing around meals or sleep, retatrutide operates on a pharmacokinetic profile designed for once-weekly administration. The compound reaches peak plasma concentration approximately 12 to 72 hours after subcutaneous injection, then gradually declines over the following days. With a half-life of roughly six days, each weekly injection builds upon residual levels from previous doses until steady state is achieved around weeks four to five.
This is important.
It means that by the time you have completed your first month of injections, your body maintains a relatively consistent level of retatrutide throughout the entire week. The distinction between "injection day" and "day seven" becomes less dramatic over time, though most people still notice a pattern of stronger effects in the first 48 hours after each dose. This pharmacokinetic profile is explained thoroughly in the how long retatrutide lasts guide. The timeline for retatrutide results depends more on your dose escalation schedule than on what time of day you inject.
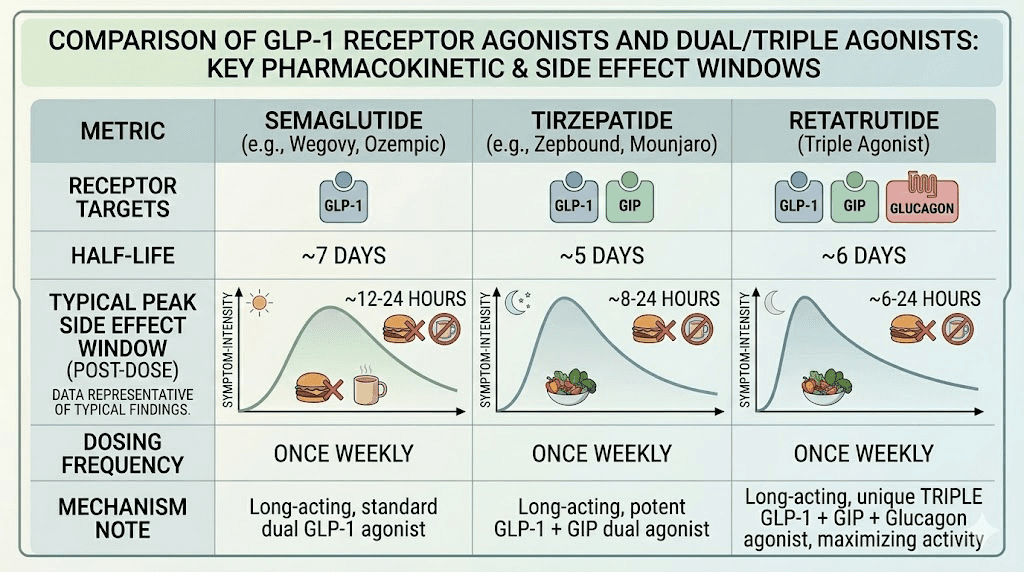
Retatrutide is a triple agonist, meaning it simultaneously activates three receptor types that single-target drugs like semaglutide do not touch. GLP-1 receptor activation suppresses appetite and slows gastric emptying. GIP receptor activation enhances insulin sensitivity and may contribute to fat metabolism in ways researchers are still mapping. Glucagon receptor activation increases energy expenditure and promotes hepatic fat oxidation. This triple mechanism, explained thoroughly in the GLP-3 (triple agonist) peptide guide, explains why retatrutide produced weight reduction of up to 24.2% at 48 weeks in phase 2 trials, numbers that exceeded both semaglutide and tirzepatide weight loss outcomes at similar timepoints.
The glucagon component, which makes retatrutide fundamentally different from semaglutide and tirzepatide, is what makes retatrutide unique among GLP-1 class medications, and it is also what makes the side effect profile slightly different. Some researchers report more energy fluctuation and thermogenic effects compared to tirzepatide alone. These effects can influence how you experience the hours immediately following injection, which is exactly why timing strategy matters even though the pharmacokinetics technically do not require it.
Morning injections: the case for starting your day with retatrutide
Morning injection is the most popular timing choice among GLP-1 users generally, and for good reason. When you inject retatrutide between 6 AM and 10 AM, you gain several practical advantages that extend through the rest of your day and week.
The primary benefit is awareness. Side effects from retatrutide, particularly nausea, typically emerge within two to six hours after injection. By injecting in the morning, you experience the peak side effect window during waking hours when you can actively manage symptoms. You can adjust food intake, stay hydrated, take anti-nausea measures if needed, and monitor how your body responds. This is especially valuable during the early weeks of treatment when you are still learning your personal response pattern at each retatrutide dose level.
Morning dosing also aligns with natural cortisol rhythms. Cortisol peaks shortly after waking, typically between 6 AM and 8 AM, and this natural hormonal surge supports the body in managing metabolic stress. Since retatrutide introduces significant metabolic activity through its triple-receptor mechanism, injecting during the cortisol peak may help your body integrate the compound more comfortably. Research on circadian rhythm and glucose metabolism consistently shows that insulin sensitivity is highest in the morning hours, which theoretically supports better metabolic response to GLP-1 and GIP receptor activation during this window.
There is also the routine factor. Most people find it easier to remember a morning injection because it can be paired with existing habits, brushing teeth, making coffee, checking messages. The retatrutide dose schedule requires weekly consistency, and anything that reduces the chance of forgetting an injection or taking it at wildly different times supports better outcomes.
Morning injection protocol
If you choose morning timing, here is a practical framework based on what experienced researchers report works best. Wake at your normal time and eat a light meal first, something with protein and minimal fat. Eggs, Greek yogurt, or a protein shake are popular choices. Wait 30 to 60 minutes after eating, then administer your injection. The small amount of food in your stomach can buffer the initial nausea response that some people experience on an empty stomach. Our guide on how to inject retatrutide covers the full technical process.
After injecting, plan for a low-key morning. Do not schedule intense workouts, heavy meals, or high-stress activities within the first two to three hours. Let the compound settle. By midday, most people report that the initial side effect wave has passed, and the appetite suppression has settled into a comfortable, manageable state. You can resume normal activity from there.
Morning injection works particularly well for people who experience fatigue as a side effect. The energy dip that sometimes accompanies the first 24 hours post-injection happens during the day when you can manage it with light activity, caffeine if tolerated, and strategic eating. By bedtime, the initial response has typically mellowed. If fatigue is a significant concern, the strategies discussed in our GLP-1 and energy levels guide translate well to retatrutide protocols.
Who should consider morning injections
Morning timing tends to work best for people who experience moderate nausea and want to monitor it. It suits those with regular morning routines and consistent wake times. If you are someone who prefers to get things done early and not think about medical protocols later in the day, morning injection removes the task from your mental load. The getting started with peptides guide emphasizes this kind of routine-building as critical for adherence. People who exercise in the afternoon or evening also benefit, since the injection site has several hours to settle before physical activity.
Evening injections: sleeping through the worst of it
The evening injection strategy follows a completely different logic. Instead of monitoring side effects during waking hours, you sleep through them.
This approach has become increasingly popular in GLP-1 communities, and the reasoning is straightforward. If the most uncomfortable period falls within the first four to eight hours after injection, and you inject at 8 PM or 9 PM, then the peak discomfort window aligns with your sleeping hours. You might feel slightly off as you fall asleep, but by morning, the acute phase has passed. Many researchers who switched from morning to evening injection report dramatically improved quality of life, not because the side effects disappeared, but because they simply did not experience them consciously.
This strategy is especially compelling for people dealing with significant nausea during dose escalation. The retatrutide dosage chart for weight loss involves titrating from low starting doses up through 8 mg or 12 mg maintenance, and each dose increase can temporarily intensify GI symptoms. If you know that dose-escalation weeks hit you hard, timing the injection for evening means you wake up the next morning past the worst of it.
Evening injection also offers a social advantage that morning dosing does not. If you inject on a Friday evening, the strongest appetite suppression and potential GI effects fall on Saturday morning when your schedule is typically more flexible. You are not fighting nausea at your desk or trying to eat a business lunch when food repulses you. By Saturday afternoon or Sunday, the acute effects have subsided, and you can enjoy the weekend normally. For those who enjoy alcohol on weekends, our guide on alcohol and GLP-1 medication interactions provides important context on how timing intersects with social drinking.
Evening injection protocol
For evening timing, eat your last meal of the day at least two hours before injection. A moderate dinner with protein and vegetables works well. Avoid large, heavy, or high-fat meals, since retatrutide will slow gastric emptying and you do not want a full stomach sitting stagnant overnight. After eating, let things settle, then inject between 7 PM and 10 PM depending on your bedtime.
Keep water by your bed. Some people wake briefly during the night feeling mildly nauseated or thirsty. Small sips of water or ginger tea can help. If you are prone to sulfur burps or acid reflux, sleeping with your upper body slightly elevated can make a meaningful difference on injection night. Understanding GLP-1 bloating management helps with nighttime comfort as well. The injection site selection matters here too. Abdominal injections while lying down shortly after can be uncomfortable, so consider the thigh or upper arm for evening doses. The full injection technique guide covers site rotation and proper subcutaneous technique.
By morning, you should feel the appetite suppression without the acute nausea. Eat a light breakfast, hydrate well, and proceed with your day. The timing effectively compresses your "adjustment period" into unconscious hours.
Who should consider evening injections
Evening timing is ideal for people who experience strong nausea or GI distress during the first hours after injection. It works well for those with demanding morning schedules, early gym sessions, or physically active jobs where feeling unwell is not an option. If you have tried morning injection and found the side effects disruptive to your workday, switching to evening can feel like a revelation. People who want appetite suppression to kick in by morning also benefit from this approach.
The weekend strategy: timing injections around your lifestyle
Choosing between morning and evening is only half the equation. The day of the week you inject matters just as much, and this is where most dosing guides fall short. They tell you to pick a day and stick with it, which is correct. But they rarely explain how to choose that day strategically.
The weekend strategy is simple. Inject on Friday evening or Saturday morning so that the first 24 to 48 hours of peak effects fall on days when you have more control over your schedule. No meetings to power through. No commutes where nausea is miserable. No work lunches where food aversion becomes awkward. This approach gives your body the weekend to adjust to each weekly dose before you return to the demands of your work week.
This strategy becomes especially important during the dose escalation phase. Phase 2 clinical trials for retatrutide used a gradual titration protocol, starting at 2 mg and increasing every four weeks up to the target dose. Each dose increase can bring a temporary return of side effects, sometimes stronger than what you experienced at the previous level. Planning those escalation weeks to coincide with weekends gives you a built-in buffer.
This aligns well with the first dose experience that many GLP-1 users describe, where that initial adjustment period benefits from scheduling flexibility. Some researchers take this a step further and use specific dose timing around their social calendar. If you know you have a dinner event on Saturday, inject on Sunday instead so that peak appetite suppression and GI sensitivity do not coincide with a meal you want to enjoy. This kind of flexibility is completely safe. The key constraint is consistency, not precision. Injecting within a window of plus or minus one day does not meaningfully affect drug levels at steady state. Users who need flexibility in their dosing schedule might also explore how taking GLP-1 injections a day early affects the weekly cycle. The retatrutide reconstitution chart helps ensure your doses remain accurate regardless of which day you choose.
Choosing your injection day
Ask yourself three questions. First, which day of the week do you have the most flexibility and the least obligations? That is your ideal injection day. Second, which day allows you to have a quiet next morning? Because the morning after injection is typically when effects are strongest. Third, which day is easiest to remember consistently? Many people find that anchoring to a specific day of the week, the same way you might always do laundry on Sunday, creates a natural rhythm that prevents missed doses.
For people who track their protocols carefully, and SeekPeptides provides tools that make this easy, logging injection day and time alongside side effects and appetite levels reveals patterns within two to three weeks. You might discover that injecting Thursday evening gives you the best balance of weekday productivity and weekend comfort. Or that Saturday morning works because you can rest if needed and still enjoy Saturday evening out. There is no universal best day. There is only your best day.
Meal timing and retatrutide: before food, after food, or does it matter?
Since retatrutide is a subcutaneous injection, food in your stomach does not directly affect absorption. The drug enters your bloodstream through subcutaneous tissue, not through the digestive tract. This is fundamentally different from oral medications where food timing affects bioavailability. Whether you inject on an empty stomach or after a three-course meal, the same amount of retatrutide reaches your system at the same rate.
But that does not mean meal timing is irrelevant. Far from it.
The indirect relationship between meals and injection timing revolves around nausea management. Retatrutide slows gastric emptying significantly, and this effect begins within hours of injection. If you inject on a full stomach, that food will sit in your stomach much longer than usual. For some people, this creates a heavy, bloated, nauseated feeling that persists for hours. For others, having food already in the stomach actually buffers the nausea and prevents the waves of queasiness that come with an empty stomach plus a GLP-1 agonist.
The split is roughly 50/50 based on community reports. There is no right answer that applies to everyone. But here are the patterns that have emerged from thousands of GLP-1 protocols:
Injecting on a mostly empty stomach
Some people find that injecting two to three hours after a light meal, when the stomach is mostly empty but not completely vacant, produces the least nausea. The reasoning is that an empty stomach gives the GLP-1 receptor activation less material to slow down. There is no food being held hostage in your gut, so the delayed gastric emptying does not create that heavy, stuck sensation. The retatrutide dosing guidance does not specify food requirements, but personal experimentation is valuable.
If you choose this approach, plan a light snack 30 to 60 minutes after injection if nausea hits. Keeping GLP-1 compatible snack options on hand makes this much easier. Crackers, toast, ginger chews, or a handful of almonds can settle the stomach without adding significant volume. Stay hydrated throughout. Dehydration worsens every GI side effect that GLP-1 agonists can produce.
Injecting after a moderate meal
Other researchers prefer injecting about 30 to 60 minutes after a moderate meal containing protein and some healthy fats. The food provides a buffer, and the argument is that your stomach was going to process a meal anyway, so having the gastric emptying slow down with food already present feels more natural. The key word is moderate. Large meals before injection are almost universally reported as a bad idea. Your stomach needs room to work, and a massive meal plus slowed motility equals misery.
This approach pairs well with morning injection schedules. Eat breakfast, wait 30 to 60 minutes, inject. Or for evening protocols, eat dinner on the earlier side, let it partially digest, then inject before bed. Resources covering optimal foods for GLP-1 users apply to retatrutide as well, since the gastric emptying mechanism is similar across the class.
What to avoid on injection day
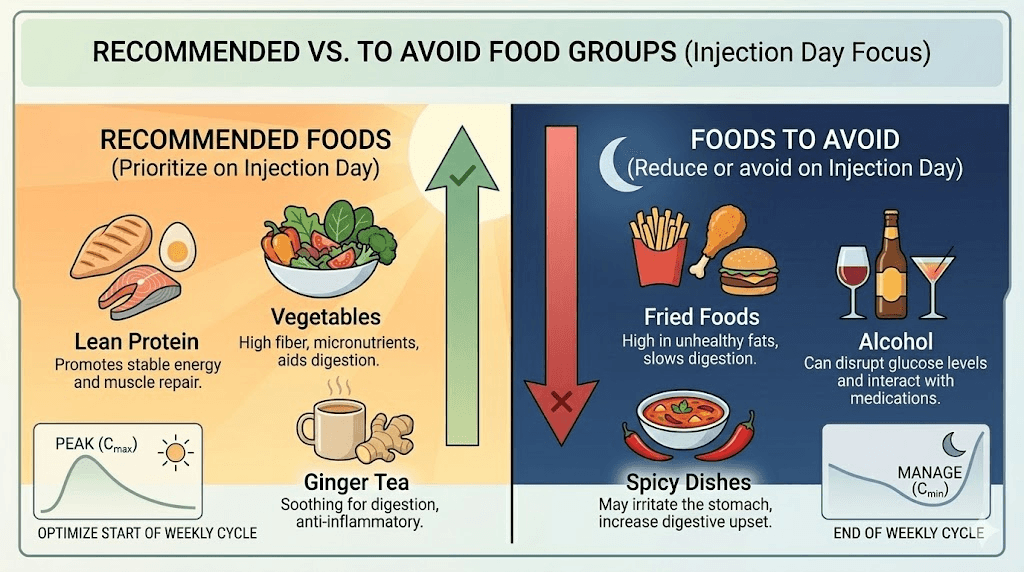
Regardless of whether you eat before or after injection, certain foods consistently worsen the experience. High-fat meals are the biggest offender. Fat takes the longest to digest under normal circumstances, and when you add GLP-1 mediated gastric slowing on top, fat can sit in your stomach for an absurdly long time. Fried foods, heavy sauces, creamy dishes, and fatty cuts of meat should be minimized on injection day. Similar guidance applies to those managing foods to avoid on GLP-1 medications.
Spicy foods can irritate an already sensitive stomach. Carbonated beverages add gas to a GI system that is already moving slowly. Alcohol is a poor choice on injection day for several reasons, not least because it dehydrates you and can compound nausea. Sugar-heavy meals cause blood sugar spikes that the GIP and glucagon receptor activation will then aggressively address, potentially causing uncomfortable blood sugar swings. Users dealing with GLP-1 compatible breakfast options find that protein-focused, low-fat meals produce the smoothest injection day experience.
Exercise timing around retatrutide injections
Physical activity and retatrutide interact in ways that are worth planning around. Exercise increases blood flow to subcutaneous tissue, which can accelerate absorption at the injection site. Exercise also creates its own metabolic demands, energy expenditure, glucose utilization, and hormonal responses, that layer on top of what retatrutide is already doing in your body.
The practical question is not whether to exercise on retatrutide. The answer to that is emphatically yes. Exercise preserves lean mass during weight loss, which is critically important when you are potentially losing 20% or more of your body weight over a protocol period. The question is how to schedule workouts relative to your injection.
The two-hour buffer rule
A widely followed guideline, consistent with general peptide injection best practices, is to separate injection and exercise by at least two hours. If you inject in your thigh, this buffer becomes especially important. During exercise, blood flow to the legs increases dramatically, which can accelerate retatrutide absorption beyond the intended rate. Faster absorption does not necessarily mean better results, but it can mean stronger side effects, particularly nausea and GI discomfort. If you exercise shortly after injection, the compound hits your system faster and harder than if you allow time for gradual absorption at rest.
For abdominal injections, the two-hour rule still applies but is less critical since core blood flow changes during exercise are less extreme than in the legs. The retatrutide injection site guide covers the full range of appropriate sites and their respective considerations.
Best workout timing on injection day
If you inject in the morning, schedule your workout for the afternoon or evening. This gives the injection site time to settle and allows the initial side effect window to pass before you add physical stress. If you inject in the evening, exercise earlier that day, ideally in the morning or afternoon, well before injection time.
Many researchers find that their energy levels follow a predictable pattern throughout the week relative to injection day. Days one and two after injection often bring the most fatigue and strongest appetite suppression. By days three through five, energy returns and workouts feel more productive. Days six and seven, as the dose wears down before the next injection, some people notice a slight rebound in appetite and energy.
Tracking this pattern allows you to schedule your most demanding workouts for the days when you feel strongest, typically mid-week if you inject on weekends, or towards the end of your weekly cycle regardless of injection day. Light walking, yoga, or low-intensity movement works well for the first day or two after injection when energy may be lower and GI sensitivity higher. The exercise and weight maintenance strategies that apply to tirzepatide translate directly to retatrutide protocols.
Preserving muscle mass during rapid weight loss
Retatrutide produces some of the most aggressive weight loss numbers ever documented in clinical trials. Phase 2 data showed 24.2% mean body weight reduction at the 12 mg dose over 48 weeks. That kind of rapid loss almost always includes some lean muscle tissue unless you actively work to prevent it. Resistance training at least two to three times per week is not optional on retatrutide. It is essential. The same principles covered in our muscle preservation with peptides guide apply here.
Protein intake needs to stay high, typically 0.7 to 1.0 grams per pound of body weight per day, even when appetite is suppressed. The peptides for weight loss overview emphasizes this point across all GLP-1 class compounds. This is where meal timing becomes strategically important. On injection day, front-load your protein intake before the appetite suppression fully kicks in. Have a protein-rich meal within the first few hours, then use GLP-1 compatible protein shakes later in the day when solid food becomes less appealing. Tracking your BMI progress on GLP-1 medications helps quantify whether your nutritional strategy is preserving lean mass.
How to handle the first 48 hours after each injection
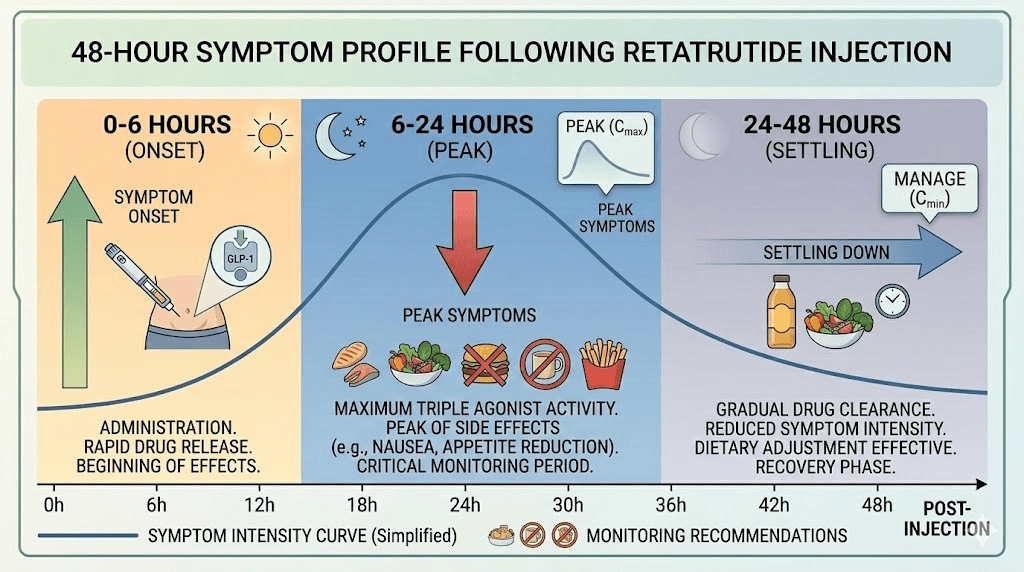
The first 48 hours after injecting retatrutide are consistently reported as the most eventful part of the weekly cycle. This is when blood levels are rising toward their peak, when GI effects are most pronounced, and when your body is most actively adjusting to the compound. Understanding what to expect during this window, and having a strategy for navigating it, makes the entire protocol significantly more manageable.
Hours 0 to 6: the onset window
In the first six hours, you may feel very little. Many people report no immediate effects at all, especially at lower doses. Others notice a subtle reduction in appetite starting around hour two or three. Some experience mild nausea around hours four to six. This is the window where your timing choice matters most. If you injected in the morning, you are still in your workday and need to function. If you injected in the evening, you are winding down and heading to bed.
Stay hydrated during this window regardless. Small sips of water, herbal tea, or electrolyte-enhanced beverages keep your system moving. Do not try to eat a large meal during hours two through six unless you are genuinely hungry. The gastric emptying slowdown is beginning, and heavy food will sit uncomfortably. If you struggle with hydration, electrolyte drinks and clear fluids work better than trying to force plain water. Understanding how GLP-1 medications affect your body helps set realistic expectations for this window.
Hours 6 to 24: the peak response
This is typically the strongest period. Appetite suppression is in full effect. Nausea, if you experience it, tends to peak somewhere in this window. Some people report feeling unusually warm or notice slight increases in heart rate, which aligns with the glucagon receptor activation increasing energy expenditure. The phase 2 trials noted dose-dependent increases in heart rate that peaked around 24 weeks and declined thereafter, suggesting the body adapts over time.
During this window, eat small meals if you can. Even when appetite is minimal, getting protein and fluids in is important. The food lists designed for GLP-1 users prioritize easily digestible, protein-rich options that work well even when nothing sounds appetizing. Broth-based soups, smoothies, and soft proteins like yogurt or cottage cheese are often better tolerated than solid meals during this peak window.
Avoid making any dose adjustment decisions during this window. What feels intense at hour 12 often mellows significantly by hour 36. People who panic and reduce their dose during the peak window often regret it when the effects normalize. The GLP-1 side effect timeline confirms this pattern across the medication class. The retatrutide results timeline shows that the body adapts progressively, and what feels overwhelming during your first few weeks at a new dose usually becomes manageable by week two or three at that same level.
Hours 24 to 48: settling in
By the second day after injection, most people report that the acute side effects have diminished considerably. Appetite suppression remains strong but feels less like revulsion and more like a natural lack of interest in food. Energy levels typically begin recovering. GI symptoms calm down, though some residual constipation may linger. This is when the medication starts feeling like it is working for you rather than against you.
Use this window to catch up on nutrition you may have missed during the first 24 hours. Get a full protein serving. Eat vegetables. Take your supplements, including any vitamins recommended for GLP-1 users. If you skipped a workout on injection day, this is a good time for moderate exercise. The general peptide dosing principles about consistency apply here as much as they do to any other compound.
Dose escalation and timing adjustments
Retatrutide dose escalation follows a structured titration protocol. The phase 2 clinical trial used a starting dose of 2 mg, increasing every four weeks through 4 mg, 6 mg, 8 mg, and potentially up to 12 mg depending on the treatment arm. Each dose increase essentially resets your side effect expectations because your body needs to adjust to the higher level of receptor activation.
This is where timing becomes strategically important again. Many researchers adjust their injection timing specifically for dose escalation weeks. The strategy is simple: on the week you increase your dose, take extra precautions with timing. If you normally inject on a weekday, consider shifting to Friday evening or Saturday morning for that first injection at the new dose. If you normally inject in the morning, consider switching to evening for the escalation week so you can sleep through the initial response.
You can return to your normal timing the following week once you know how the new dose affects you. This one-week adjustment prevents unnecessary disruption to your routine while giving your body the gentlest possible introduction to each new dose level.
When to extend time at a dose level
The phase 2 trial protocols allowed participants to remain at their current dose for an extra two to four weeks before increasing if they experienced significant nausea. This flexibility did not reduce long-term effectiveness. The detailed retatrutide dose chart maps out all standard escalation paths. The retatrutide dose schedule is a guideline, not a rigid requirement. If a dose increase hits you harder than expected, staying at that level for an additional two weeks before trying again is a legitimate and evidence-supported strategy.
Timing can help here too. If your first attempt at a dose increase produced intolerable side effects despite evening injection, weekend timing, and dietary preparation, consider splitting the difference. Some researchers step up to an intermediate dose, for example going from 4 mg to 6 mg via two weeks at 5 mg, using their retatrutide dosage calculator to get the exact measurements right.
Comparing timing strategies with other GLP-1 medications
If you have previously used semaglutide or tirzepatide, your timing experience with those medications provides useful but imperfect guidance for retatrutide. The pharmacokinetic profiles differ enough that what worked for one may need adjustment for the other.
Retatrutide versus semaglutide timing
Semaglutide has a half-life of approximately seven days, slightly longer than retatrutide. The side effect profiles overlap heavily in the GI department, nausea, constipation, reduced appetite, but semaglutide lacks the glucagon receptor activation that gives retatrutide its thermogenic edge. People who experienced semaglutide fatigue often report that retatrutide produces a different kind of energy fluctuation, more of a metabolic revving sensation rather than pure tiredness. Those who found that semaglutide appetite suppression kicked in quickly should expect retatrutide to feel similarly rapid but potentially more intense due to the triple mechanism. The retatrutide vs semaglutide comparison covers the full spectrum of differences.
If you timed semaglutide injections in the evening to sleep through nausea, the same strategy likely works for retatrutide. If you found morning semaglutide injections comfortable, you might find that retatrutide needs an evening shift during dose escalation but can return to morning timing at maintenance doses.
Retatrutide versus tirzepatide timing
Tirzepatide is a dual GLP-1/GIP agonist with a half-life of about five days, shorter than retatrutide. Many researchers who transition from tirzepatide to retatrutide find the side effect timing quite similar since both medications share the GIP pathway. The main difference is the glucagon component in retatrutide, which can produce more noticeable energy shifts and temperature changes in the first 24 hours. Our guide on switching from tirzepatide to retatrutide covers the transition in detail.
If you had a well-established timing routine with tirzepatide, particularly one referenced in our best time to take tirzepatide guide, start with that same timing for retatrutide and adjust from there. Most people find they need minimal changes. The retatrutide vs tirzepatide dosage chart helps compare where you were on tirzepatide versus where you will start on retatrutide, and the mazdutide vs retatrutide comparison provides context for another emerging triple agonist.
Transition timing considerations
When switching between GLP-1 medications, timing your last dose of the old medication relative to your first dose of the new one matters. The retatrutide kickin timeline after tirzepatide suggests waiting at least one half-life of the previous medication before starting retatrutide. For tirzepatide, that means roughly five days. For semaglutide, roughly seven days. This prevents overlapping receptor activation that could intensify side effects beyond what either drug would produce alone.
Managing specific side effects through timing
Different side effects respond to different timing strategies. Rather than applying a one-size-fits-all approach, experienced researchers learn to match their timing to their primary side effect concern.
Nausea
Nausea is the most common retatrutide side effect and the one most responsive to timing optimization. Evening injection is the strongest single strategy for nausea management because you sleep through the peak onset window. Combining evening injection with a two-hour food buffer before injection and ginger tea before bed covers most cases. For persistent nausea that extends beyond the first night, our GLP-1 side effect management guides cover additional strategies.
If evening injection alone does not fully resolve nausea, the next adjustment is dietary. Eat smaller, more frequent meals throughout injection day. Avoid anything heavy, greasy, or strongly flavored. Some researchers keep bland snacks, crackers, rice cakes, or plain bread, within arm is reach for the first 24 hours. The goal is to never let your stomach be completely empty or completely full.
Fatigue and energy fluctuations
The triple-receptor mechanism of retatrutide creates a unique energy profile that differs from pure GLP-1 agonists. The glucagon receptor activation increases metabolic rate, which can feel like a strange combination of tiredness and internal heat. Some describe it as "tired but wired," a sensation also reported in the tirzepatide energy effects literature though often less pronounced with dual agonists. If fatigue is your primary concern, morning injection may actually work better than evening. You can manage the energy dip with light activity and caffeine during the day, and by bedtime, you are genuinely tired rather than artificially fatigued.
For researchers who experience significant post-injection fatigue, pairing injection day with a lighter schedule, fewer obligations, more rest time, makes the entire protocol more sustainable. The fatigue typically improves as your body adjusts to each dose level. Resources about GLP-1 fatigue provide deeper coverage of this specific issue.
Constipation and GI slowdown
Delayed gastric emptying is a feature of all GLP-1 agonists, and retatrutide is no exception. The timing strategy for constipation is less about when you inject and more about what you do in the 48 hours after injection. Stay aggressively hydrated. Walk after meals. Include fiber from whole food sources rather than supplements, which can worsen the feeling of fullness. If constipation becomes a recurring issue, the dedicated guide on GLP-1 constipation management applies equally to retatrutide.
One timing-specific strategy that helps with constipation is front-loading fiber and hydration before injection rather than after. On injection day, prioritize vegetables, water, and gentle movement earlier in the day. By the time you inject and gastric motility slows, you have already given your digestive system a head start.
Injection site reactions
Some people experience redness, swelling, or itching at the injection site. While this is not strictly a timing issue, the way you use the injection site in the hours after injection matters. If you inject in the thigh and then go for a run, increased blood flow to the area can worsen local reactions. Similarly, injecting in the abdomen and then wearing a tight waistband creates friction that aggravates the site. Plan your injection location around your post-injection activities. Our comprehensive guide on GLP-1 injection site reactions covers treatment options.
Special timing situations
Travel across time zones
If you travel frequently across time zones, retatrutide timing requires some flexibility. The good news is that once-weekly dosing provides significant wiggle room. Injecting 12 to 24 hours earlier or later than your usual time to accommodate travel does not meaningfully affect drug levels at steady state. The traveling with injectable medications guide covers storage, TSA considerations, and schedule adjustment strategies that apply to retatrutide.
A practical approach is to inject at your destination is local time equivalent of your usual injection time. If you normally inject at 8 PM Eastern and fly to California, inject at 8 PM Pacific. The three-hour difference is negligible for a drug with a six-day half-life. For larger time zone shifts, gradual adjustment over two to three weeks works well. Shift your injection time by two to three hours per week until you reach the new desired time.
Illness and skipped doses
If you are sick with a stomach virus, food poisoning, or anything that already causes nausea and vomiting, adding a retatrutide injection on top is generally a poor idea. It is acceptable to delay your injection by one to three days until GI symptoms from the illness resolve. A short delay will not derail your protocol. Your blood levels will dip slightly below steady state but will quickly recover once you resume.
If you completely miss a dose and more than five days have passed since your scheduled injection, most guidance suggests taking the missed dose as soon as you remember and then resuming your regular schedule the following week. Do not double up on doses to compensate. The retatrutide availability landscape means supply consistency can sometimes vary, so having a strategy for missed doses is important. The retatrutide duration and half-life information helps you understand how blood levels respond to timing shifts.
Stacking retatrutide with other compounds
Researchers who use retatrutide alongside other peptides or supplements need to consider timing interactions. If you are stacking with tesamorelin or cagrilintide, separate the injections by at least a few hours and use different injection sites. This prevents local tissue overload and allows you to identify which compound causes any specific side effect.
For oral supplements, timing is simpler. Take vitamins, minerals, and other oral supplements during the window when your stomach is handling food most comfortably, typically the second day after injection rather than the first. Some researchers also explore cagrilintide alongside retatrutide as a stacking strategy, though this requires careful timing coordination. If you are using supplements common in GLP-1 protocols, morning administration on non-injection days generally works well since gastric function is closest to normal toward the end of your weekly cycle.
Building your personalized retatrutide timing protocol
The best timing protocol is the one you actually follow consistently. And the only way to find it is through systematic experimentation over four to six weeks. Here is a framework for developing your own optimized schedule.
Week one: establish your baseline
Choose a starting time based on your best guess. If you have never used a GLP-1 agonist before, evening injection on a Friday or Saturday is a safe default. If you have experience with semaglutide timing or GLP-1 injection timing, start with whatever worked for those medications.
After your first injection, log the following on a simple spreadsheet or notes app:
Time of injection. What you ate in the four hours before injection. When nausea started (if at all). When nausea peaked. When nausea resolved. Sleep quality that night. Energy level the next morning on a 1 to 10 scale. When appetite returned. Any other notable side effects.
Week two: assess and maintain
Inject at the same time, same conditions as week one. Compare your notes. Some variation is normal, but consistent patterns will emerge. If nausea peaked at the same window both weeks, that confirms your timeline. If sleep was disrupted both weeks, that might signal a timing change is worth trying.
Week three: adjust if needed
If weeks one and two revealed a consistent problem, such as nausea ruining your mornings, this is the week to make one change. Shift from morning to evening, or vice versa. Keep everything else the same, same day of week, same meal timing relative to injection, same activities. Isolating one variable at a time is the only way to know what actually helped.
Weeks four through six: refine
By now you are into your second dose level if following standard escalation. The timing strategies that worked at the lower dose may need small adjustments at the higher dose. Continue logging and refining. Most researchers find their optimal timing within this window and maintain it for the remainder of their protocol. The retatrutide peptide dosage chart helps you anticipate what each dose level will feel like, and the peptide calculator for weight loss can help with precise measurements.
Summary of timing variables to experiment with
Here is a quick reference table for the variables you can adjust:
Variable | Option A | Option B | Best for |
|---|---|---|---|
Time of day | Morning (6-10 AM) | Evening (7-10 PM) | Evening for nausea, morning for monitoring |
Day of week | Weekday | Weekend | Weekend for dose escalation flexibility |
Food timing | Empty stomach | After moderate meal | Personal preference, test both |
Exercise timing | Before injection (2+ hours) | Next day | Next day for heavy workouts |
Injection site | Abdomen | Thigh or upper arm | Thigh for evening, abdomen for morning |
What the clinical trial data tells us about timing
The phase 2 retatrutide trial published in the New England Journal of Medicine enrolled 338 participants and tested doses ranging from 1 mg to 12 mg over 48 weeks. The trial protocol did not specify a particular time of day for injections, which is itself an informative data point. If timing significantly affected efficacy, the trial design would have controlled for it.
What the trial did reveal about timing-adjacent factors is more useful. Participants who started at 2 mg (lower starting dose) experienced fewer GI side effects than those who started at 4 mg, even when both groups eventually reached the same maintenance dose. This suggests that the body needs time to adjust to receptor activation, and giving it that time through gradual escalation reduces discomfort regardless of when during the day you inject.
The trial also showed that GI side effects were "mostly mild to moderate in severity" and were "partially mitigated with a lower starting dose." This means that many of the side effects people try to manage through timing can also be addressed through dose adjustment. Both strategies work. The most successful researchers use both, optimizing their timing while also ensuring their dose escalation is appropriately gradual.
At 48 weeks, participants in the 12 mg group achieved a mean weight reduction of 24.2% compared to 2.1% for placebo. The 8 mg group achieved 22.8%. These results, discussed in detail in our retatrutide dosage chart and competitive landscape analysis, did not correlate with injection time because the study was not designed to measure that variable. But the consistency of results across hundreds of participants injecting at various times of day strongly supports the conclusion that efficacy is time-independent, while tolerability is time-dependent. The retatrutide 10 mg dosing guide and 20 mg dosing information provide context for understanding different dose levels.
Circadian rhythm and metabolic timing
There is a growing body of research on how circadian rhythms affect drug metabolism and metabolic function. While no study has directly examined retatrutide timing relative to circadian patterns, the broader literature on GLP-1 biology and circadian rhythm provides some interesting context.
Natural GLP-1 secretion in the body follows a circadian pattern. Endogenous GLP-1 tends to peak in the late afternoon and evening, roughly between 5:30 PM and 6 PM, with lowest levels occurring at night. Morning GLP-1 and GIP release tends to be more pronounced after eating compared to afternoon release. This suggests that the incretin system, which retatrutide mimics and amplifies, is naturally more active at certain times of day.
Insulin sensitivity also follows a circadian rhythm. It peaks in the morning and declines throughout the day. Glucose tolerance is measurably worse in the evening compared to the morning. Since retatrutide activates GIP receptors that enhance insulin sensitivity, some researchers theorize that morning injection could synergize with the natural morning insulin sensitivity peak to produce slightly better metabolic outcomes.
However, this theory remains speculative for retatrutide specifically. The exogenous drug operates at much higher concentrations than natural incretin hormones, and its six-day half-life means it is active around the clock regardless of when it peaks. Any circadian advantage from morning injection would be modest at best and has not been demonstrated in controlled studies. The peptide research landscape continues to evolve on these timing questions. Practical considerations like nausea management and lifestyle compatibility almost certainly matter more than circadian optimization for the vast majority of users. For a broader look at how peptides work at the molecular level, our foundational guide covers the receptor-binding mechanisms that underpin all GLP-1 class medications.
Retatrutide timing for specific goals
Your primary goal with retatrutide, whether weight loss, metabolic health improvement, or body recomposition, can influence which timing approach makes the most sense. While the pharmacokinetics remain the same regardless of your goal, the practical considerations shift.
Timing for maximum weight loss
If your primary goal is aggressive weight loss, your timing strategy should prioritize two things: maximizing the appetite-suppressive window during your most vulnerable eating hours, and ensuring you can maintain adequate protein intake despite reduced hunger.
For most people, the danger zone for overeating falls in the evening. Stress eating, boredom snacking, social eating. All of these happen after 6 PM for the majority of the population. If you inject Friday or Saturday morning, the strongest appetite suppression hits within 6 to 24 hours, covering that evening window and extending through the weekend. By Monday, the suppression has moderated to a manageable level that still reduces appetite but does not make eating impossible.
The counterargument is that morning injection means you lose your appetite during the hours when you should be eating protein-rich meals to preserve muscle mass. If you find that morning injection kills your appetite to the point where you cannot eat lunch or dinner on injection day, front-load your protein before injecting. Eat a substantial, protein-heavy breakfast, then inject 30 to 60 minutes later. You have already gotten a significant chunk of your daily protein before appetite suppression fully kicks in.
Timing for metabolic health
For researchers focused on metabolic markers, blood sugar regulation, GLP-1 pathway optimization, and overall metabolic improvement, morning injection has a theoretical edge. Insulin sensitivity peaks in the morning, and the GIP receptor activation from retatrutide may synergize with this natural morning peak to produce slightly better glucose handling. Research on chronobiology and drug timing suggests that hormonal therapies often work best when aligned with the body is natural rhythms, and retatrutide is fundamentally a hormonal intervention.
That said, the effect size of this circadian alignment is likely small compared to the overall impact of the drug itself. If morning injection causes you so much nausea that you skip meals, miss workouts, or dread injection day, the metabolic costs of that stress and disruption far outweigh any circadian benefit. Practical tolerability trumps theoretical optimization every time. The metabolic effects of GLP-1 class medications operate around the clock regardless of injection timing.
Timing for body recomposition
Body recomposition, losing fat while building or at minimum preserving muscle, demands the most careful timing strategy. You need to balance appetite suppression (which helps with fat loss) against nutritional adequacy (which prevents muscle loss). This means your injection timing should work with your training and eating schedule, not against it.
A popular approach for recomp-focused researchers is to inject in the evening after completing their most important meal of the day. Train in the morning or afternoon, eat a large post-workout meal rich in protein and carbohydrates within two hours of training, then inject in the evening. The appetite suppression hits overnight and into the next morning, creating a natural fasting window that supports fat loss. By the afternoon of the following day, appetite returns enough to eat another training-focused meal.
This approach to peptide-supported fat loss creates a cycling of fed and fasted states within the weekly injection cycle, not dissimilar to intermittent fasting, except the fasting windows are pharmacologically supported rather than forced through willpower. The key is ensuring you never go more than 24 hours without a meaningful protein serving, even when appetite is at its lowest. Peptide stacking strategies for weight loss often incorporate similar timing principles.
Reconstitution timing and injection preparation
For researchers working with lyophilized retatrutide powder, the timing of reconstitution relative to injection is an additional consideration. Properly reconstituted retatrutide stored in the refrigerator, following the same principles outlined in the peptide storage after reconstitution guide, maintains stability for a reasonable period, but freshly reconstituted solutions may behave slightly differently than solutions that have been sitting for days.
The standard practice is to reconstitute a vial using the correct amount of bacteriostatic water and then allow the solution to sit in the refrigerator for at least 15 to 30 minutes before drawing your first dose. This allows the peptide to fully dissolve and stabilize. Rushing from reconstitution to injection can result in uneven concentration if the powder has not completely dissolved. The guide to mixing peptides with bacteriostatic water covers the proper technique for all peptide types.
Once reconstituted, store the vial upright in the refrigerator and draw your weekly dose at your scheduled injection time. Avoid leaving the reconstituted vial at room temperature for extended periods. If you are traveling and the vial needs to be out of refrigeration, the same principles that apply to warm peptide storage apply to retatrutide. Our retatrutide reconstitution chart provides the exact water-to-powder ratios for accurate dosing.
The general peptide storage guide and reconstituted peptide storage protocols provide comprehensive information on maintaining potency. For retatrutide specifically, cold storage is essential. Room temperature exposure degrades the compound, and repeated temperature cycling (cold to warm and back) can reduce potency faster than consistent refrigeration. The bacteriostatic water guide covers water quality requirements for reconstitution, and the peptide refrigerator shelf life guide provides storage duration data.
Tracking your timing data for optimal results
The difference between a good retatrutide protocol and a great one often comes down to data. Researchers who track their timing, side effects, energy levels, and appetite patterns consistently outperform those who wing it. The tracking does not need to be elaborate. A simple daily log with four data points captures everything you need.
First, record your injection time and any pre-injection meals. Second, note side effects during the first 24 hours using a simple 1 to 10 severity scale. Third, log your energy level each morning and evening. Fourth, track whether you hit your protein target for the day. After three to four weeks, patterns emerge that no amount of general advice can replicate.
For example, you might discover that injecting at 7 PM produces less nausea than injecting at 9 PM because you are further from your last meal. Or that injection day protein intake consistently drops below 80 grams unless you front-load breakfast. Or that your best workout days are consistently three and four days after injection. These are personal insights that optimize your protocol in ways that generic timing advice cannot. Members of SeekPeptides access protocol tracking tools designed specifically for this kind of self-experimentation with peptides.
The retatrutide dosage calculator pairs well with a timing log. When you know exactly what dose you are taking and exactly when you are taking it, correlating those numbers with your side effect and energy data becomes straightforward. Over time, you build a personal database that makes each dose escalation and timing adjustment more informed than the last.
Community data from GLP-1 forums and research communities consistently shows that tracked protocols produce better adherence and better outcomes. When you can see your progress charted over weeks, the temporary discomfort of side effects feels more manageable because you can see the trend improving. Tools like the GLP-1 plotter help visualize this progress. Researchers who understand the retatrutide results timeline are better equipped to maintain patience during the early adjustment phase.
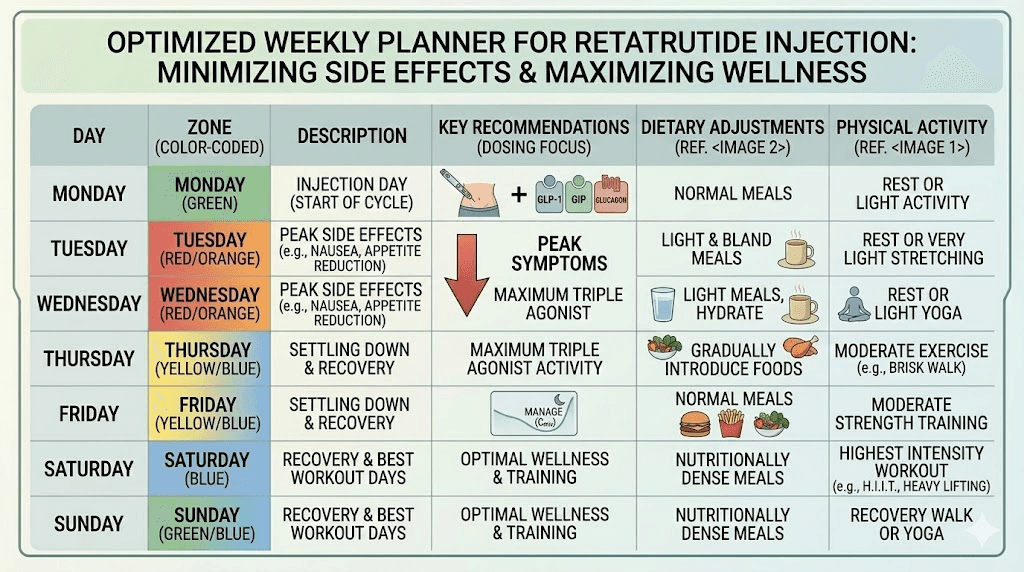
Understanding the weekly side effect cycle
One of the most valuable pieces of timing knowledge for retatrutide users is understanding how side effects and benefits cycle throughout the week. This predictable pattern allows you to plan your entire week around your injection schedule rather than being surprised by fluctuations.
Days one and two (injection day and the day after)
This is the highest impact window. Appetite suppression is strongest. GI side effects are most likely. Energy may fluctuate. Some researchers report feeling slightly warm or flushed as the glucagon receptor activation increases metabolic rate. This is the window where timing strategy matters most, and where evening injection provides the biggest advantage for those who struggle with nausea.
Nutritionally, these are the hardest days. Food may not sound appealing. Portions naturally shrink. The challenge is getting enough nutrition despite low appetite. Smoothies, broth-based soups, and easy-to-digest protein sources are your best allies. Our guide to what to eat on GLP-1 medications provides a comprehensive food list. Do not force yourself to eat large meals, but do make every bite count nutritionally.
Days three and four (the productive middle)
By mid-week in your injection cycle, the acute effects have softened into a comfortable steady state. Appetite suppression remains but feels more natural, like simply not being very hungry rather than the complete food aversion that can characterize days one and two. Energy levels normalize or even improve. This is when most researchers feel their best and when intense workouts, social meals, and demanding work schedules are most manageable.
If you are planning important events, schedule them for these days relative to your injection. A dinner out on day four feels completely different from a dinner out on day one, much like the first week on semaglutide feels dramatically different from week four. You can eat, enjoy the experience, and make reasonable food choices without the compound fighting you every step of the way.
Days five through seven (the taper)
As blood levels decline toward the end of the weekly cycle, some people notice a gradual return of appetite. Hunger increases slightly. Cravings may surface, particularly for carbohydrate-rich foods. Energy is typically stable. Side effects are at their weekly minimum.
This taper period is where adherence gets tested. The temptation to overeat during the taper can undermine the caloric deficit achieved during the first half of the week. Planning meals for these days, having healthy options readily available, maintaining the same eating patterns even as appetite increases, separates successful protocols from struggling ones. Similar patterns are documented in our semaglutide plateau guide and the why am I not losing weight on semaglutide troubleshooting resource. The GLP-1 compatible diet planning resources help structure these later-in-cycle days.
Some researchers strategically increase their caloric intake slightly during days five through seven, focusing on protein and complex carbohydrates, to fuel recovery and maintain muscle while still staying in an overall weekly deficit. This cyclical approach to nutrition mirrors the cyclical nature of the drug is effects and can feel much more sustainable than trying to eat the same restricted diet every single day.
Common timing mistakes to avoid
After reviewing thousands of GLP-1 protocol reports and community discussions, certain timing mistakes appear repeatedly. Avoiding these saves you weeks of unnecessary discomfort.
Changing everything at once
When side effects are bad, the temptation is to change injection time, injection day, meal timing, and exercise schedule simultaneously. This makes it impossible to identify what actually helped. Change one variable at a time and give each change at least two weeks before evaluating. This methodical approach mirrors the peptide cycle planning principles that apply to any research compound.
Injecting before a big meal or social event
Retatrutide will make that dinner party uncomfortable. The appetite suppression and potential nausea make it difficult to enjoy food socially. Plan injections for at least 24 hours before any event centered around eating. Better yet, plan events for days four through seven of your weekly cycle when appetite is closest to normal.
Inconsistent weekly timing
Injecting Monday morning one week, Wednesday evening the next, and Friday afternoon the week after creates unpredictable drug level fluctuations. While the half-life provides some buffer, consistent timing promotes consistent blood levels and consistent side effect patterns you can plan around. If you need to shift your injection day, do it gradually. Move by one day per week until you reach the new desired day. The common peptide mistakes beginners make often include inconsistent dosing schedules, and GLP-1 agonists are no exception.
Ignoring post-injection hydration
This is not strictly a timing mistake, but it is so strongly correlated with injection day that it belongs here. Dehydration amplifies every GLP-1 side effect. Nausea gets worse. Constipation gets worse. Fatigue gets worse. Headaches appear. Dizziness creeps in. On injection day and the day after, aim for at least 80 to 100 ounces of water. More if you exercise or live in a warm climate. The retatrutide hair loss concerns can also be exacerbated by dehydration and nutritional deficits during aggressive weight loss phases.
Not tracking patterns
Trying to optimize timing from memory is unreliable. Your perception of how bad Tuesday was can be colored by Wednesday is improvement. A simple log, even just three lines per day noting energy, appetite, and any side effects, reveals patterns within two to three weeks that you would never notice otherwise.
Frequently asked questions
Can I take retatrutide at different times each week?
Minor variations of an hour or two are fine and will not affect results. Larger shifts, like switching from morning to evening, should be done deliberately as a timing experiment rather than randomly. Consistent timing helps you predict and manage side effects. The retatrutide dosing schedule emphasizes weekly consistency as the primary timing requirement. If you are purchasing retatrutide, the buying guide covers sourcing considerations, and our best places to buy retatrutide review evaluates current vendors.
Is it better to take retatrutide on an empty stomach or with food?
Since retatrutide is a subcutaneous injection, food does not affect absorption. However, the timing of meals relative to injection affects your GI comfort. Most people find either a mostly empty stomach or a moderate meal 30 to 60 minutes before injection works best. Test both approaches and note which produces less nausea for you personally.
What if I miss my usual injection time by several hours?
Take it when you remember. A delay of 6, 12, or even 24 hours has minimal impact on a drug with a six-day half-life. Do not skip the dose entirely. Just take it and resume your normal schedule the following week. If you want to shift back to your original time, do so gradually over two to three weeks.
Should I change injection time when I increase my dose?
Many researchers temporarily switch to evening injection and weekend timing for dose escalation weeks, then return to their usual schedule once they have adjusted to the new dose. This is a smart precautionary strategy that reduces the impact of potentially stronger side effects at the higher dose. The retatrutide dosage chart for weight loss provides the standard escalation schedule.
How long after injection should I wait to exercise?
A minimum of two hours between injection and exercise is widely recommended. This is especially important if you inject in your thigh, since increased blood flow during leg exercise can accelerate absorption and intensify side effects. Light walking is fine immediately after injection, but save intense workouts for at least two hours post-injection, or better yet, schedule them for the following day.
Does the time of day I inject affect how much weight I lose?
No. Clinical trials did not control for injection time because it does not significantly affect the drug is efficacy. Weight loss outcomes depend on dose, diet, exercise, and adherence to the protocol. Timing affects your experience and comfort, not the drug is fundamental metabolic effects. For context on expected results, the retatrutide results timeline covers what to expect at each stage. The ozempic vs retatrutide comparison also shows how weight loss outcomes compare across the GLP-1 class.
Can I take retatrutide before bed without side effects?
Many people inject before bed specifically to avoid side effects during waking hours. While some experience mild sleep disruption on injection night, the majority report that sleeping through the initial onset window makes the overall experience much more tolerable. Keep water and ginger tea nearby in case you wake with mild nausea.
What is the best day of the week for retatrutide injections?
The best day is whichever day gives you the most flexibility for the 24 to 48 hours following injection. For most working professionals, Friday evening or Saturday morning works well because the peak side effect window falls on the weekend. But any day works if it fits your schedule consistently. Our retatrutide online sourcing guide covers delivery timing so you can plan around your injection day, and the retatrutide microdosing guide offers an alternative approach for those who prefer more frequent, smaller doses.
External resources
New England Journal of Medicine: Retatrutide Phase 2 Trial Results
PubMed Central: Systematic Review of Retatrutide Weight and Metabolic Markers
Nature Medicine: Retatrutide for Metabolic Dysfunction-Associated Liver Disease
For researchers serious about optimizing every aspect of their retatrutide protocol, SeekPeptides provides the most comprehensive resource available. Members access detailed protocols, dosing calculators, community-shared timing strategies, and evidence-based guides that cover exactly these kinds of nuanced decisions. When the difference between a good protocol and a great one comes down to details like injection timing, having the right tools and community makes all the difference.
In case I do not see you, good afternoon, good evening, and good night. May your injection timing stay consistent, your side effects stay manageable, and your results stay on track.