Mar 20, 2026

You started retatrutide expecting to lose weight. Instead, you lost energy. The scale moved in the right direction, but your body felt like it was running on fumes. Coffee stopped working by noon. Afternoon meetings became endurance tests. And that couch? It started looking more inviting than the gym you paid for.
You are not imagining things. Retatrutide side effects are real, and fatigue ranks among the most commonly reported complaints in clinical trial participants. In the phase 2 NEJM trial, between 4% and 10% of people taking retatrutide reported feeling unusually tired, compared to just 4% in the placebo group. Those numbers might seem small on paper. They feel enormous when you are the one dragging through your day.
But here is the thing nobody tells you about retatrutide fatigue. It is almost always temporary. It is almost always manageable. And it is almost always caused by something specific that you can fix. The triple receptor agonist works on GLP-1, GIP, and glucagon pathways simultaneously, and that metabolic shift demands adjustment time. Your body is not broken. It is recalibrating. This guide covers exactly why retatrutide makes some people tired, how long the exhaustion typically lasts, which doses carry the highest fatigue risk, and the specific strategies that researchers use to get their energy back without compromising their results.
Why retatrutide causes fatigue in the first place
Understanding the root cause makes fixing the problem possible. Retatrutide does not cause fatigue through a single mechanism. Five distinct pathways contribute, sometimes individually, sometimes all at once, and identifying which ones apply to you determines the fastest route back to normal energy.
Reduced calorie intake is the primary driver
This one catches people off guard. Retatrutide is extraordinarily effective at suppressing appetite. Most people naturally eat 30% to 50% fewer calories than they consumed before starting treatment. That caloric deficit drives weight loss, which is the entire point. But your body interprets that sudden reduction as a signal to conserve energy.
Think about it. If you went from 2,200 calories per day to 1,300 calories per day overnight, your mitochondria would notice. They fuel every cell in your body, and they just got a significant budget cut. The result? Fatigue. Brain fog. That heavy feeling in your limbs when you climb stairs. The same process happens with semaglutide fatigue and tirzepatide tiredness, but retatrutide can amplify the effect because its triple receptor action suppresses appetite more aggressively than single or dual agonists.
Your body needs time to switch from burning dietary calories to efficiently mobilizing fat stores for energy. That metabolic transition typically takes two to four weeks.
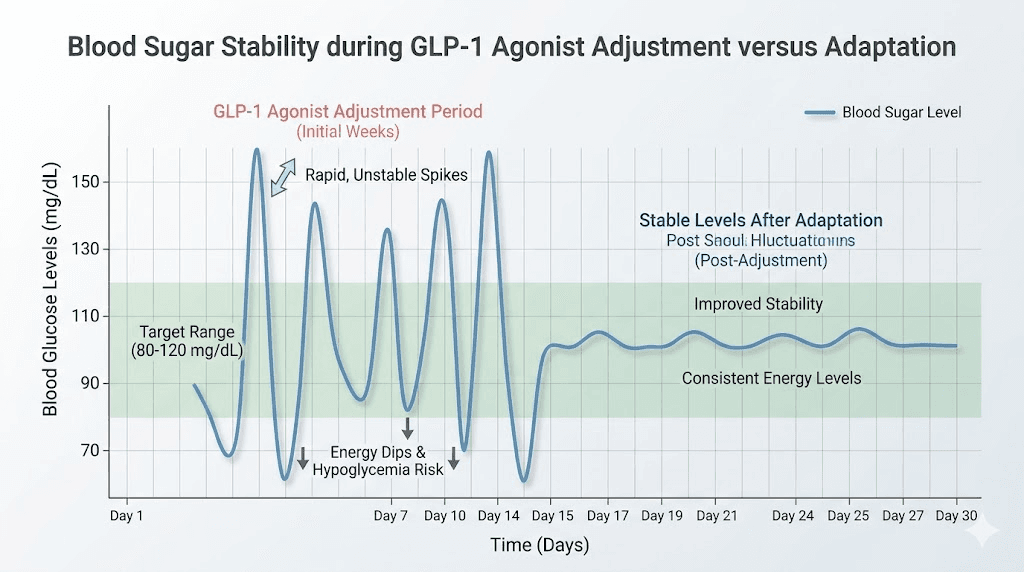
Blood sugar fluctuations during the adjustment period
Retatrutide activates both GLP-1 and GIP receptors, which dramatically improves insulin sensitivity. Excellent for long-term metabolic health. Challenging for short-term energy levels. During the first few weeks, your blood sugar may drop lower than your body expects, even when readings remain technically within normal ranges. That relative hypoglycemia produces a specific kind of tiredness, the foggy, unfocused, irritable exhaustion that makes you want to reach for sugar.
This mechanism differs from the caloric deficit fatigue described above. Blood sugar fatigue tends to hit in waves rather than as a constant background drain. You might feel fine in the morning, crash hard at 2 PM, then recover somewhat by evening. The pattern reflects your glucose curves adjusting to a new baseline. Researchers who track their blood sugar with continuous glucose monitors often discover these dips correspond precisely to their energy crashes.
Electrolyte depletion is the most underrecognized cause
Three electrolytes deserve your immediate attention. Sodium. Potassium. Magnesium. Each one plays essential roles in cellular energy production, muscle function, and nervous system signaling. Deplete any of them and fatigue arrives as one of the earliest warning signs.
Retatrutide depletes electrolytes through multiple mechanisms. Reduced food intake means fewer dietary electrolytes coming in. The GLP-1 pathway can increase urinary output, flushing electrolytes out faster. And if you experience any gastrointestinal side effects like diarrhea, electrolyte losses accelerate dramatically.
The symptoms mimic general tiredness so closely that most people blame the medication when the real culprit is a correctable mineral deficiency. Magnesium deficiency alone can cause fatigue, muscle weakness, and poor sleep quality, which compounds the exhaustion further.
Dehydration compounds every other fatigue mechanism
When nausea reduces your desire to drink fluids, and when you are eating less food (which normally provides 20% to 30% of daily water intake), dehydration sneaks in quietly. Even mild dehydration, losing just 1% to 2% of body water, reduces cognitive performance by 10% to 15% and increases perceived fatigue significantly.
Dehydration also worsens electrolyte imbalances, slows nutrient absorption, and reduces blood volume. Lower blood volume means your heart works harder to deliver oxygen to tissues. That circulatory strain manifests as tiredness, especially during physical activity. Many people who think retatrutide ruined their exercise capacity are actually just dehydrated.
Slowed gastric emptying changes how your body absorbs energy
Retatrutide, like other GLP-1 agonists, delays gastric emptying. Food sits in your stomach longer, which creates that prolonged feeling of fullness. But it also means nutrients enter your bloodstream more slowly. The sustained energy release sounds good in theory. In practice, it can leave you feeling like your tank is perpetually at one-quarter rather than cycling between full and empty.
This mechanism explains why some people on retatrutide never feel truly hungry but also never feel truly energized. The steady, low-level nutrient drip keeps you functional but not sharp. Combining strategic meal timing with the right macronutrient ratios can counteract this effect substantially.
What the clinical trials actually show about retatrutide and fatigue
Numbers matter here because they put your experience in context. The phase 2 trial published in the New England Journal of Medicine (Jastreboff et al., 2023) provides the most detailed data available on retatrutide fatigue.
Fatigue rates by dose
The data reveals something surprising. Fatigue does not increase linearly with dose.
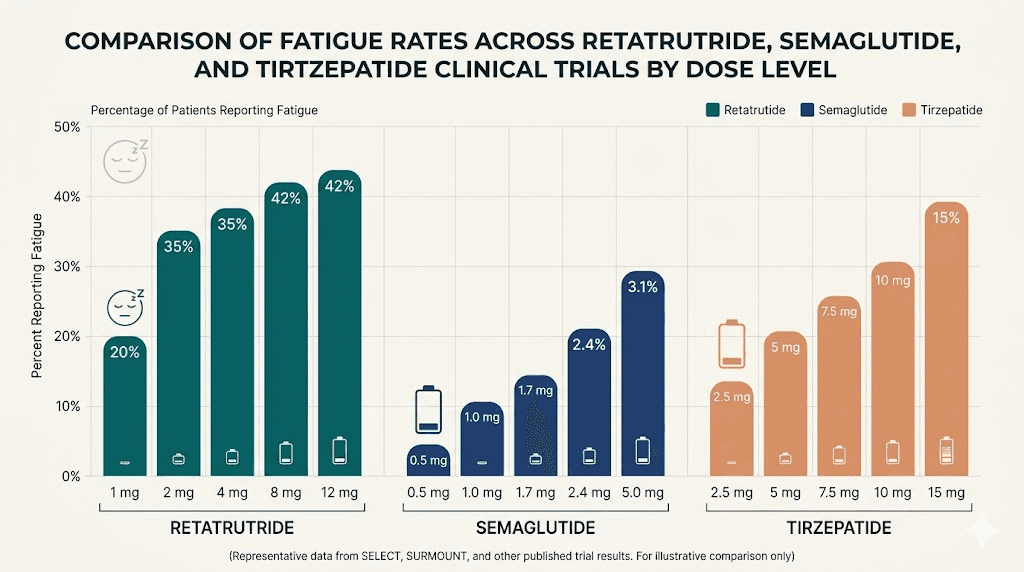
At 1 mg, 4% of participants reported fatigue. At 4 mg (starting from 2 mg), that number jumped to 12%. At 4 mg (starting from 4 mg), it dropped to 6%. At 8 mg (starting from 2 mg), just 3% reported fatigue. At 8 mg (starting from 4 mg), 9% experienced it. And at the maximum 12 mg dose, 10% reported feeling tired.
Notice the pattern. The starting dose and titration speed matter more than the final dose itself. Participants who started at 4 mg without a lower starting dose reported fatigue more often than those who titrated up gradually from 2 mg. This strongly suggests that the metabolic shock of rapid dose escalation, not the medication dose itself, drives most fatigue complaints.
Compare this to the placebo group, where 4% reported fatigue. That means some fatigue reports in the treatment group may simply reflect the experience of caloric restriction, lifestyle changes, or study participation itself.
How retatrutide fatigue compares to other GLP-1 medications
Context helps. Semaglutide and tirzepatide both produce fatigue in their clinical trials at comparable rates. Semaglutide trials report fatigue in approximately 5% to 11% of participants. Tirzepatide fatigue rates range from 4% to 7%. Retatrutide falls roughly in the same range at 3% to 12% depending on dose and titration.
The important takeaway is that retatrutide does not appear significantly worse for fatigue than its predecessors, despite activating an additional receptor pathway (glucagon). In fact, the glucagon receptor component theoretically supports energy expenditure through thermogenesis in brown fat tissue, which could partially offset the fatigue from caloric restriction.
The reassuring timeline from trial data
Here is what matters most. Fatigue is classified as mild to moderate in the overwhelming majority of cases. No participants discontinued the trial solely because of fatigue. And the symptom typically resolves within the first four to six weeks of treatment.
The pattern follows a predictable arc. Week one through two brings the sharpest fatigue, as the body encounters the metabolic shift for the first time. Weeks three through four show gradual improvement as metabolic adaptation occurs. By weeks five through eight, most people report energy levels returning to baseline or close to it. Some participants actually report improved energy after the adjustment period, likely because carrying less weight and having better metabolic health increases baseline vitality.
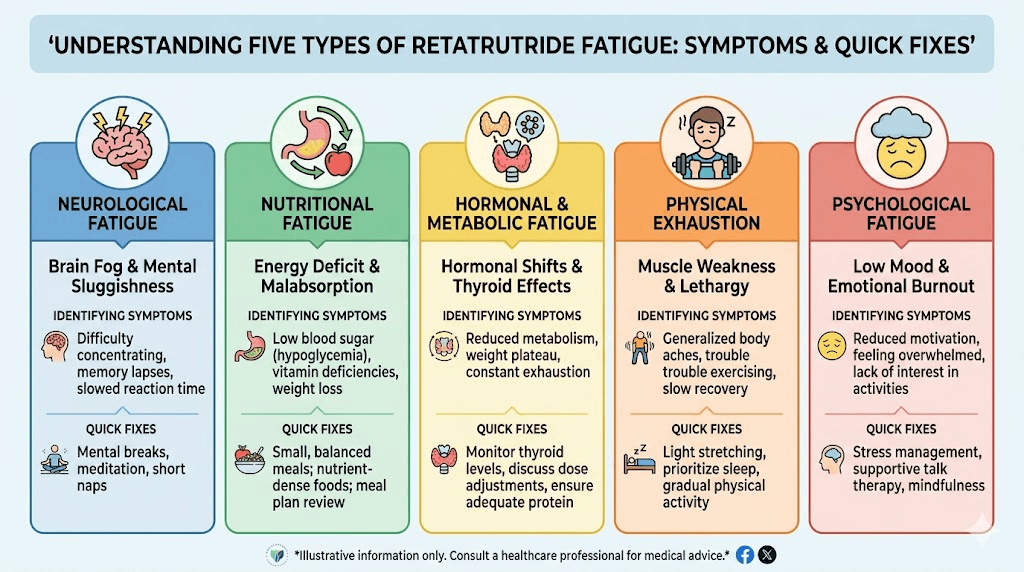
The five types of retatrutide fatigue and how to identify yours
Not all tiredness is created equal. The type you experience determines the fix.
Type 1: caloric deficit fatigue
What it feels like: A constant, low-grade drain. You are not exhausted enough to nap, but you never feel truly awake either. Everything requires slightly more effort than it should. You could describe it as moving through the day at 60% capacity.
When it hits: All day, every day, with minimal variation. Worse on days when you eat particularly little.
The fix: Strategic calorie distribution rather than restriction alone. Eating too few calories is counterproductive even on retatrutide for weight loss. You should aim for a moderate deficit (500 to 750 calories below maintenance) rather than the extreme deficits that appetite suppression can create. Protein should account for 30% to 40% of total intake. Use our peptide calculator tools alongside a food tracking approach to ensure adequate nutrition.
Type 2: blood sugar crash fatigue
What it feels like: Sharp energy drops that come and go in waves. You feel fine for a few hours, then hit a wall so hard you can barely think. Irritability often accompanies the crash. Concentration disappears. You might get shaky or slightly lightheaded.
When it hits: Two to four hours after meals, or during periods of extended fasting.
The fix: Smaller, more frequent meals with a focus on complex carbohydrates paired with protein and healthy fats. This combination slows glucose absorption and prevents the sharp spikes and crashes. The foods that work well with GLP-1 agonists also work well with retatrutide because the underlying metabolic mechanisms overlap. Avoid simple sugars, which cause rapid glucose spikes followed by insulin-driven crashes.
Type 3: electrolyte depletion fatigue
What it feels like: Muscle heaviness, mild cramping, and a specific kind of weakness that rest alone does not fix. You might notice heart palpitations or increased muscle twitching. The fatigue has a physical quality to it, not just mental fog but actual limb heaviness.
When it hits: Often worse in the morning (after overnight electrolyte losses) and after exercise (when sweating accelerates depletion).
The fix: Targeted supplementation. Magnesium glycinate (200 to 400 mg daily) addresses the most common deficiency. A quality electrolyte supplement with sodium, potassium, and magnesium taken twice daily can resolve this type of fatigue within 48 to 72 hours. The speed of improvement is a useful diagnostic clue. If electrolyte supplementation brings noticeable relief within two to three days, electrolyte depletion was likely your primary fatigue driver. Our guide on supplements to take with GLP-1 medications covers this topic in detail.
Type 4: dehydration fatigue
What it feels like: Headaches combined with tiredness, difficulty concentrating, and dry mouth. You might notice darker urine. Exercise feels disproportionately hard. Your skin might feel less elastic when pinched.
When it hits: Progressively throughout the day, especially if you did not drink enough in the morning. Worse in warm environments or after physical activity.
The fix: Structured hydration targets rather than drinking when thirsty. Thirst signals are often delayed, so if you feel thirsty you are already dehydrated. Aim for a minimum of 64 ounces of water daily, increasing to 80 to 100 ounces if you exercise. Set hourly reminders if needed. Flavored water (cucumber, citrus, berries) makes consumption easier when nausea or bloating reduce your desire to drink.
Type 5: sleep disruption fatigue
What it feels like: Classic sleep deprivation symptoms. Excessive yawning, difficulty focusing, emotional reactivity, and that gritty-eyed feeling of not having slept enough even when you technically got seven or eight hours.
When it hits: Worst in the morning, with slight improvement as the day progresses.
The fix: Retatrutide can disrupt sleep quality through several mechanisms, including nighttime nausea, blood sugar fluctuations during sleep, and changes to appetite-related hormones that influence circadian rhythm. Taking your dose at the optimal time of day matters. Most researchers find that morning dosing produces less sleep disruption than evening dosing. If insomnia accompanies your treatment, targeted sleep hygiene adjustments and potentially magnesium supplementation before bed can help significantly.
15 proven strategies to fight retatrutide fatigue
These strategies come from clinical guidance, user experience reports, and the underlying physiology of GLP-1/GIP/glucagon agonism. Start with the first five. They address the most common causes. Add more as needed.
Strategy 1: protect your protein intake
When appetite drops, protein is usually the first macronutrient people cut. That is a mistake. Protein maintains muscle mass during weight loss, supports neurotransmitter production (which directly affects energy and mood), and provides the most sustained energy release of any macronutrient. Aim for 0.7 to 1.0 grams of protein per pound of body weight daily. If that feels impossible on a suppressed appetite, prioritize protein at every eating opportunity. A high-protein food strategy works just as well for retatrutide users as it does for other GLP-1 medications.
Practical targets: 25 to 40 grams of protein at each meal. If you can only eat two meals, aim for 40 to 50 grams each. Greek yogurt, eggs, chicken breast, fish, and whey protein isolate are calorie-efficient protein sources that work well when appetite is limited. GLP-1 friendly protein shakes can fill gaps when solid food feels unappealing.
Strategy 2: supplement electrolytes proactively
Do not wait for symptoms. Begin electrolyte supplementation when you start retatrutide, not after fatigue appears. The three key minerals and their recommended daily targets:
Magnesium: 200 to 400 mg daily (magnesium glycinate or citrate, not oxide). Supports over 300 enzymatic reactions including energy production. Most adults are already mildly deficient before starting any medication.
Sodium: 2,000 to 3,000 mg daily from food plus supplementation. When you eat less food, you consume less sodium. Low sodium causes fatigue, headaches, and dizziness. Adding a pinch of high-quality salt to water or using electrolyte packets addresses this quickly.
Potassium: 2,500 to 3,400 mg daily from food sources primarily. Bananas, avocados, sweet potatoes, and spinach are potassium-rich foods that most people tolerate well on retatrutide. Potassium supplementation above food-derived amounts should involve medical supervision.
For a comprehensive approach to supplementation during peptide treatment, consider a daily electrolyte supplement designed for low-carb or fasting protocols, as these typically provide the right ratios.
Strategy 3: optimize your meal timing
When you eat matters almost as much as what you eat when managing retatrutide fatigue. The dosing schedule creates predictable patterns in appetite and energy. Eating three smaller meals plus two snacks throughout the day prevents the deep energy valleys that come with long fasting gaps.
A sample schedule that works for many people:
7:00 AM: Breakfast with protein and complex carbs (eggs with whole grain toast, or Greek yogurt with berries and nuts). 10:00 AM: Small snack (handful of almonds, cheese stick, protein bar). 12:30 PM: Lunch emphasizing protein and vegetables. 3:00 PM: Another small snack (apple with peanut butter, hard-boiled egg). 6:30 PM: Dinner with balanced macronutrients.
Even if appetite suppression makes some of these meals feel unnecessary, eating small amounts at regular intervals prevents the blood sugar crashes that drive the sharpest fatigue episodes. The foods to avoid during GLP-1 treatment apply here too, particularly simple sugars and highly processed carbohydrates that cause rapid glucose spikes.
Strategy 4: hydrate with intention
Set a specific daily water target and track it. This sounds basic. It works. Aim for at least half your body weight in ounces of water daily. A 200-pound person should target 100 ounces minimum. Keep a water bottle visible at all times. Set phone reminders every hour. Add flavor if plain water causes nausea or bloating.
Herbal tea counts toward your fluid target. Coffee counts partially but also increases urinary output, so it is less efficient for hydration. Alcohol dehydrates, so limiting alcohol during treatment helps energy levels on multiple fronts.
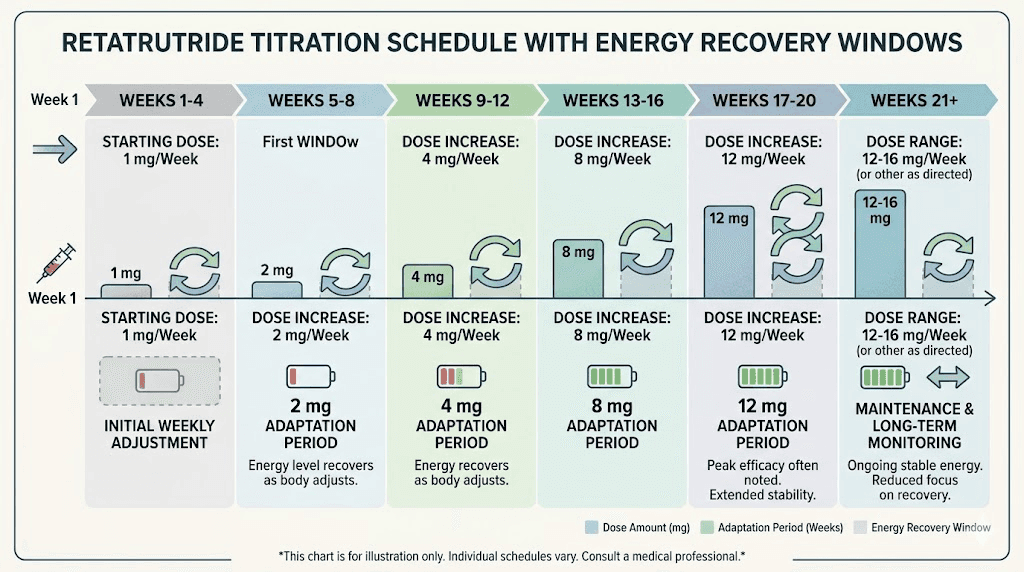
Strategy 5: titrate slowly
The clinical trial data showed that fatigue rates varied significantly based on titration speed. Participants who started at lower doses and titrated gradually reported less fatigue than those who jumped to higher doses quickly. If your retatrutide dosage protocol allows flexibility, ask about a slower titration. Starting at the lowest effective dose and increasing by the smallest available increment every two to four weeks gives your body maximum time to adapt.
The standard retatrutide dose schedule typically starts at 1 mg weekly for four weeks, then increases to 2 mg, then 4 mg, then 8 mg, and potentially 12 mg. If fatigue becomes problematic at any stage, holding at the current dose for an additional two to four weeks before increasing often resolves the issue.
Strategy 6: prioritize B12 and iron status
Reduced food intake can lead to deficiencies in B vitamins and iron, both of which are critical for energy production. B12 deficiency specifically causes fatigue, weakness, and cognitive fog that mimics the worst aspects of retatrutide tiredness. Iron deficiency produces similar symptoms through reduced oxygen-carrying capacity in the blood.
Ask for blood work checking B12, ferritin (iron stores), and folate levels within the first month of treatment. Supplementation with B12 or methylcobalamin can produce noticeable energy improvements within one to two weeks if deficiency is present. The vitamin and nutrient guide for GLP-1 users covers all the micronutrients worth monitoring.
Strategy 7: use strategic caffeine timing
Caffeine is not a solution to retatrutide fatigue, but when used strategically, it can bridge energy gaps during the adaptation period. The key is timing. Consume caffeine only in the morning or early afternoon (before 2 PM). Late caffeine disrupts sleep quality, which worsens fatigue the next day in a vicious cycle.
Limit intake to 200 to 400 mg daily (roughly two to four cups of coffee). If caffeine causes stomach irritation alongside retatrutide, green tea provides a gentler alternative with L-theanine, which smooths the energy curve. Avoid energy drinks, which often contain excessive sugar and can worsen GLP-1 headaches.
Strategy 8: incorporate light movement daily
This sounds counterintuitive when you are exhausted. But light physical activity, walking 15 to 30 minutes, gentle stretching, easy yoga, actually increases energy through improved circulation, enhanced mitochondrial function, and mood-boosting endorphin release.
The emphasis is on light. High-intensity exercise during the adaptation period can worsen fatigue because your body is already under metabolic stress. Save the intense workouts for after your energy stabilizes. Walking remains the single most accessible and effective energy-boosting activity during the first month of retatrutide. It supports muscle preservation without creating additional recovery demands that drain energy further. The peptides for fat loss resource covers how movement supports metabolic outcomes during treatment.
Strategy 9: optimize sleep environment and habits
Sleep quality matters more than sleep quantity during retatrutide treatment. Seven hours of deep, uninterrupted sleep beats nine hours of fragmented sleep for energy restoration. Key adjustments include keeping your bedroom cool (65 to 68 degrees Fahrenheit), eliminating screen exposure one hour before bed, maintaining consistent sleep and wake times even on weekends, and using blackout curtains.
Magnesium glycinate taken 30 to 60 minutes before bed serves double duty, replenishing electrolytes while promoting relaxation through GABA receptor activation. If sleep problems persist, a temporary low-dose melatonin supplement (0.5 to 1 mg, not the 5 to 10 mg doses commonly sold) can help reset circadian rhythm without creating dependence.
Strategy 10: track your symptoms
A simple daily log of energy levels (1 to 10 scale), meals eaten, water consumed, and sleep quality reveals patterns that are invisible otherwise. After two weeks of tracking, most people can clearly identify which days are worst and what they did differently. Maybe fatigue spikes on days you skip breakfast. Maybe it correlates with low water intake the previous day. Maybe dose days are consistently worse.
This data makes every other strategy more effective because you can target the actual cause rather than guessing. The timeline of retatrutide effects provides a useful reference for expected symptom patterns.
Strategy 11: manage stress actively
Cortisol, the stress hormone, directly increases fatigue and interferes with blood sugar regulation. If your body is already adjusting to retatrutide while dealing with work stress, sleep debt, and emotional strain, the combined load overwhelms your adaptive capacity. Something as simple as 10 minutes of deep breathing, meditation, or a walk in nature can lower cortisol levels measurably.
Stress also increases the likelihood of other retatrutide side effects, creating a cascade where multiple symptoms feed into each other. Managing stress is not a luxury during treatment. It is a practical necessity.
Strategy 12: consider dose timing adjustments
Most researchers take their retatrutide dose once weekly, but the time of day and day of the week matter. If fatigue peaks on dose day, try taking your injection in the evening so the worst of the metabolic adjustment happens while you sleep. If fatigue persists throughout the week, morning dosing might spread the adjustment more evenly.
Some researchers also find that taking their dose on a day when they can rest (like Friday evening or Saturday morning) allows recovery time before the work week. There is no single best approach. Finding the optimal injection timing requires experimentation.
Strategy 13: address gastrointestinal issues that worsen fatigue
Nausea, constipation, diarrhea, and bloating all contribute to fatigue indirectly. Nausea reduces food and fluid intake. Constipation creates discomfort that disrupts sleep. Diarrhea causes electrolyte and fluid losses. Bloating makes eating feel unpleasant, further reducing caloric intake.
Treating GI symptoms aggressively and proactively prevents the downstream fatigue they cause. Probiotics can help with GI discomfort. Fiber supplementation addresses constipation while supporting gut health. Ginger tea or capsules reduce nausea without medication interactions.
Strategy 14: get blood work done
If fatigue persists beyond six to eight weeks despite implementing the strategies above, blood work can identify underlying issues. Request a comprehensive metabolic panel including thyroid function (TSH, free T3, free T4), iron studies (ferritin, TIBC), B12, folate, vitamin D, magnesium (RBC magnesium, not serum), and fasting glucose with HbA1c.
Retatrutide can unmask pre-existing nutritional deficiencies that were previously compensated by higher food intake. Liver enzyme monitoring and blood work considerations during GLP-1 treatment provide additional context for interpreting results.
Strategy 15: consider temporary dose reduction
If fatigue significantly impairs your quality of life and does not respond to the strategies above, discuss a temporary dose reduction with your healthcare provider. Dropping back one tier for two to four weeks, then re-attempting the increase, often succeeds where pushing through fails. The microdosing approach to retatrutide provides a framework for finding the minimum effective dose that balances results with side effects.
Weight loss is not a sprint. Slowing titration to maintain energy and quality of life produces better long-term outcomes than pushing through severe fatigue, which often leads to treatment abandonment.
How long does retatrutide fatigue typically last
The timeline follows a consistent pattern across most users, though individual variation exists.
Week 1 through 2: the hardest stretch
The first two weeks bring the most noticeable fatigue. Your body is experiencing the metabolic shift for the first time, caloric intake has dropped, blood sugar regulation is adjusting, and electrolytes may already be depleting. This is when most people want to quit. Do not quit. The discomfort is temporary.
During this phase, energy levels typically drop to 50% to 70% of baseline. You can function, but everything feels harder. Mornings may be manageable, with progressive decline by afternoon. This mirrors what people experience with their first tirzepatide dose as well.
Week 3 through 4: gradual improvement
Most people notice measurable improvement by week three. Energy levels climb back to 70% to 85% of baseline. The blood sugar fluctuations stabilize as insulin sensitivity normalizes. If you have been supplementing electrolytes and maintaining adequate hydration, those benefits compound during this period.
Dose increases during this window can temporarily reset the fatigue cycle, which is why gradual titration matters so much. If you increase your retatrutide dose right as your body adapts to the current level, you may experience a smaller, briefer dip in energy rather than a return to week-one levels.
Month 2 through 3: near-normal energy
By the second month, the majority of users report energy levels at 85% to 95% of their pre-treatment baseline. Some report feeling better than before treatment started, because they have lost weight, improved metabolic markers, and are eating a more nutrient-dense diet (even if smaller in volume).
Residual fatigue at this stage usually points to an unaddressed nutritional deficiency, inadequate sleep quality, or excessive caloric restriction. Troubleshooting becomes easier because the acute metabolic adjustment is complete.
Month 3 through 4 and beyond: energy normalization
Research suggests that by month three to four, energy levels fully normalize for the vast majority of retatrutide users. The body has adapted to its new metabolic state. Fat oxidation efficiency has improved. Hormonal signaling has stabilized. Weight loss itself reduces the energy cost of daily movement, which creates a net energy gain.
Patients who implement proactive energy management strategies from the start report 60% to 70% reduction in fatigue severity compared to those who simply wait for symptoms to resolve on their own.
Retatrutide fatigue versus other GLP-1 medication fatigue
If you are switching from tirzepatide to retatrutide or considering retatrutide after trying other medications, understanding how fatigue profiles differ helps set realistic expectations.
Retatrutide versus semaglutide
Semaglutide is a pure GLP-1 receptor agonist. Retatrutide activates GLP-1, GIP, and glucagon receptors. This triple action means retatrutide suppresses appetite more aggressively, which can lead to larger caloric deficits and therefore more pronounced caloric-deficit fatigue. However, the glucagon component increases energy expenditure, which theoretically offsets some fatigue.
In practice, users switching from semaglutide to retatrutide report that the fatigue quality feels similar but may be slightly more intense during the first two weeks. The semaglutide fatigue experience provides a useful reference point.
Retatrutide versus tirzepatide
Tirzepatide is a dual GIP/GLP-1 agonist. Retatrutide adds glucagon activation on top of that. The additional receptor pathway creates more metabolic disruption during the adjustment period. However, the difference in reported fatigue between the two medications is modest in clinical data.
The bigger factor is typically dose and titration speed rather than the specific medication chosen. Someone on a well-titrated retatrutide protocol often experiences less fatigue than someone who escalated tirzepatide doses too quickly. For a broader comparison of side effect profiles, our three-way comparison guide covers the key differences.
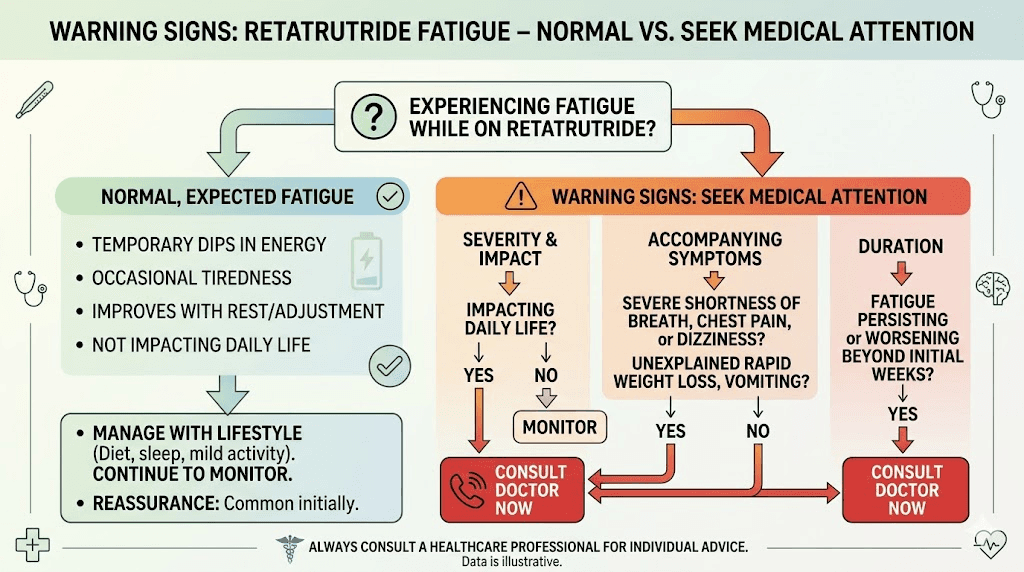
When retatrutide fatigue signals something more serious
Mild to moderate tiredness during the first few weeks of treatment is expected and manageable. But certain fatigue patterns warrant medical attention.
Red flags that require immediate evaluation
Contact your healthcare provider promptly if fatigue is accompanied by rapid heartbeat or heart palpitations that do not resolve with rest. Severe dizziness or fainting episodes are not normal side effects. Extreme weakness where you cannot perform basic daily activities goes beyond typical adjustment fatigue. Chest pain or shortness of breath with exertion needs immediate evaluation. Confusion or severe cognitive impairment is not an expected retatrutide effect.
These symptoms could indicate dehydration severe enough to affect cardiovascular function, electrolyte imbalances reaching dangerous levels, thyroid dysfunction, or other conditions that require medical intervention.
Persistent fatigue beyond 8 weeks
If you have implemented all 15 strategies described above and fatigue persists beyond eight weeks, comprehensive blood work is essential. Retatrutide can unmask or worsen pre-existing conditions including thyroid dysfunction, iron deficiency anemia, vitamin D deficiency, and adrenal insufficiency. These conditions cause fatigue independently and compound the metabolic adjustment fatigue from retatrutide.
Do not assume persistent fatigue is just how retatrutide works. Investigate. The goal is sustainable treatment, and sustainable means maintaining quality of life alongside weight loss.
Special considerations for specific populations
Retatrutide fatigue in people with type 2 diabetes
The Lancet published data from a phase 2 trial specifically examining retatrutide in people with type 2 diabetes (Rosenstock et al., 2023). Blood sugar regulation is already impaired in this population, and retatrutide dramatically improves insulin sensitivity while also reducing glucose output through glucagon modulation. The result is more pronounced blood sugar fluctuations during adjustment, which can intensify fatigue.
Careful glucose monitoring is essential. Working with your prescriber to adjust any existing diabetes medications (metformin, insulin, sulfonylureas) when starting retatrutide prevents the dangerous hypoglycemia that causes extreme fatigue, confusion, and potentially serious complications.
Retatrutide fatigue in people who exercise regularly
Active individuals notice fatigue more acutely because they have higher energy demands. The caloric deficit created by retatrutide appetite suppression is proportionally larger for someone who exercises regularly. A person burning 2,800 calories daily who drops to eating 1,500 calories faces a 1,300-calorie deficit, compared to a sedentary person burning 2,000 calories with the same food intake facing only a 500-calorie deficit.
Active users should pay particular attention to pre and post-workout nutrition, ensuring adequate carbohydrate intake around exercise sessions even if overall intake is reduced. Creatine supplementation can support exercise performance during the adjustment period without interfering with retatrutide mechanisms. Resistance training specifically helps preserve muscle mass during rapid weight loss.
Retatrutide fatigue in people over 50
Age-related changes in metabolism, hormone levels, and nutrient absorption make older adults more susceptible to retatrutide fatigue. B12 absorption naturally decreases with age, and reduced food intake on retatrutide compounds this. Thyroid function should be checked at baseline and monitored during treatment. Bone density considerations also come into play, as bone health during GLP-1 treatment requires adequate calcium and vitamin D intake.
The good news is that the weight loss and metabolic improvements from retatrutide often produce dramatic quality-of-life improvements in older adults, including increased mobility and reduced joint pain, that ultimately outweigh the temporary fatigue adjustment period.
Retatrutide fatigue compared to the fatigue of carrying excess weight
Perspective matters here. The fatigue from retatrutide is temporary. The fatigue from carrying 50, 80, or 100+ excess pounds is chronic. Obesity causes persistent fatigue through sleep apnea, chronic inflammation, insulin resistance, reduced cardiovascular capacity, and joint pain that limits activity. Every one of these factors improves with the weight loss that retatrutide facilitates.
Many people who push through the initial four to six weeks of adjustment fatigue report that their baseline energy levels after treatment are significantly higher than they were before starting, not because retatrutide gives you energy, but because losing weight removes the energy-draining burden of excess body mass.
The benefits beyond weight loss that apply to dual and triple agonists include improved sleep quality, reduced inflammation, better cardiovascular function, and enhanced insulin sensitivity. All of these translate directly into more daily energy.
Sample weekly energy management plan for your first month
Putting all 15 strategies together into a practical weekly plan makes implementation manageable rather than overwhelming.
Week 1: foundation building
Nutrition: Eat three meals and two snacks daily. Protein target 100+ grams. Do not try to restrict calories beyond what retatrutide naturally suppresses. Hydration: 64+ ounces water daily with electrolyte packets twice daily. Supplementation: Begin magnesium glycinate 200 mg at bedtime, B-complex vitamin with breakfast, and vitamin D3 2,000 IU daily. Movement: Walk 15 minutes daily, no intense exercise. Sleep: Strict 10 PM to 6 AM schedule, no screens after 9 PM.
Energy expectation: 50% to 65% of normal. This is the hardest week. Accept lower productivity.
Week 2: adjustment acceleration
Nutrition: Same framework, increase protein to 120+ grams if tolerated. Add glycine-containing foods or supplement. Hydration: Increase to 80+ ounces if tolerating well. Movement: Extend walks to 20 to 30 minutes. Add gentle stretching. Supplementation: Increase magnesium to 400 mg if sleep is still poor. Tracking: Begin daily energy, food, and water log.
Energy expectation: 60% to 75% of normal. Noticeable improvement from week 1.
Week 3: optimization phase
Nutrition: Use tracking data to identify energy-boosting meals. Lean into what works. Movement: Add light resistance training (bodyweight exercises, light weights) two to three times per week. Social: Resume normal social activities. Caffeine: If using, limit to morning only and track effect on sleep.
Energy expectation: 70% to 85% of normal. Significant improvement. Most daily activities feel manageable.
Week 4: return to baseline
Nutrition: Established routine should be solid. Movement: Resume moderate exercise if energy supports it. Assessment: Review your tracking log. If energy has not improved to 75%+ of baseline, consider blood work. Dose: If increasing dose this week, expect a minor two to three day energy dip that resolves faster than the initial adjustment.
Energy expectation: 80% to 95% of normal for most people.
The role of retatrutide glucagon activation in energy regulation
Retatrutide is unique among current GLP-1 medications because it activates the glucagon receptor. This deserves special attention regarding fatigue because glucagon has a complex relationship with energy.
Glucagon mobilizes stored glucose from the liver, which should theoretically prevent the low blood sugar episodes that cause fatigue. In animal models, glucagon receptor activation also increases energy expenditure by stimulating brown fat thermogenesis. This means your body burns more calories at rest, generating heat as a byproduct.
In practice, this glucagon effect means retatrutide users may experience a paradoxical combination of increased metabolic rate and reduced caloric intake. The body is burning more fuel while receiving less. During the adaptation period, this mismatch contributes to fatigue. After adaptation, it becomes a powerful advantage for weight loss and may actually support higher energy levels than pure GLP-1 agonists achieve.
This mechanism also explains why some users feel cold during treatment while others actually feel warmer. The glucagon-driven thermogenesis increases heat production, but the caloric deficit reduces the body insulation effect. The net result varies by individual.
For the deepest dive into how retatrutide mechanisms differ from other options, the retatrutide versus Mounjaro comparison and the cagrilintide versus retatrutide analysis provide detailed mechanism-by-mechanism breakdowns.
Frequently asked questions
Does retatrutide fatigue go away completely?
Yes, for the vast majority of users. Clinical trial data and user reports consistently show that retatrutide fatigue resolves within four to eight weeks. Most people describe their energy levels as equal to or better than pre-treatment levels by month three to four, particularly as weight loss reduces the physical burden of excess body mass.
Is retatrutide fatigue worse than semaglutide fatigue?
Not significantly. Clinical trial fatigue rates for retatrutide (3% to 12%) overlap substantially with semaglutide fatigue rates (5% to 11%). Individual experience varies more than the medication choice itself. Titration speed and supportive strategies have a larger impact on fatigue severity than which specific GLP-1 medication you use.
Can I take caffeine while on retatrutide?
Yes, moderate caffeine consumption (200 to 400 mg daily) is generally compatible with retatrutide. However, limit caffeine to morning and early afternoon to protect sleep quality. Avoid energy drinks with excessive sugar, as they worsen blood sugar instability.
Should I skip my workout if I am tired on retatrutide?
Replace intense workouts with light movement rather than skipping exercise entirely. Walking, gentle stretching, and light yoga maintain fitness and actually boost energy through improved circulation. Resume normal exercise intensity once energy stabilizes, typically by week three to four. Our muscle growth guide discusses exercise during peptide treatment.
Does the fatigue mean the medication is working?
Not directly. Fatigue is a side effect of the metabolic adjustment, not a sign of effectiveness. You can achieve excellent results from retatrutide with minimal fatigue if you manage nutrition, hydration, and supplementation proactively. Some people who experience zero fatigue still achieve significant weight loss.
What supplements help most with retatrutide fatigue?
Magnesium glycinate (200 to 400 mg daily), B12 or methylcobalamin, vitamin D3 (2,000 to 4,000 IU daily), and a comprehensive electrolyte supplement are the most impactful. The complete GLP-1 supplement guide covers additional options.
Can I switch from retatrutide to something else if the fatigue is unbearable?
Yes. If fatigue persists despite implementing all management strategies, other GLP-1 options may suit your physiology better. Semaglutide and tirzepatide both offer effective weight loss with potentially different side effect profiles for your body.
Does retatrutide fatigue get worse with higher doses?
Not linearly. The phase 2 trial data shows that fatigue rates varied more by titration speed than by final dose. The 10 mg dose and starting dose approach matter more than where you end up. Slow titration consistently produces less fatigue than rapid dose escalation.
External resources
For researchers serious about optimizing their retatrutide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides covering dosing protocols, dosage charts, injection techniques, and a community of thousands who have navigated these exact questions. SeekPeptides members access detailed protocols, expert guidance, and real-world experience reports that help you manage side effects while maximizing results.
In case I do not see you, good afternoon, good evening, and good night. May your energy levels stay high, your electrolytes stay balanced, and your retatrutide results stay consistent.