Mar 15, 2026

Something feels wrong with your skin. Not painful exactly, but not right either. A light brush against your arm sends signals that feel too loud, too intense, like the volume got turned up on every nerve ending at once. You started retatrutide a few weeks ago. The weight loss results have been promising. But now your skin is behaving like it belongs to someone else, reacting to bedsheets, clothing seams, even a gentle touch from another person.
You are not imagining this.
Retatrutide skin sensitivity is a real, documented side effect that shows up in roughly 7% of clinical trial participants. That is not a small number. For a triple-receptor agonist that targets GLP-1, GIP, and glucagon receptors simultaneously, the neurological ripple effects are still being studied, still being understood. And if you are sitting here searching for answers because your own skin suddenly feels like a stranger, you need more than a generic paragraph telling you to "talk to your doctor." You need to understand what is happening, why it is happening, and exactly what you can do about it.
This guide breaks down the full clinical picture of retatrutide skin sensitivity. The mechanisms driving it. The timeline for resolution. The specific management strategies that work. And the critical difference between skin sensitivity that will resolve on its own and symptoms that demand medical attention. SeekPeptides has compiled the most comprehensive resource available on this topic, pulling from Phase 2 trial data published in the New England Journal of Medicine, emerging case series on GLP-1 allodynia, and practical management protocols from researchers navigating this exact situation.
What retatrutide skin sensitivity actually is
Skin sensitivity from retatrutide is not a simple allergic reaction. It is not a rash that appears and fades. The condition involves your nervous system misinterpreting normal sensory input as abnormal, sometimes painful, sometimes just deeply uncomfortable. Understanding the distinction matters because the treatment approach changes entirely based on what type of skin response you are experiencing.
There are three primary categories of altered skin sensation associated with retatrutide and other GLP-1 receptor agonists.
Hyperesthesia
This is heightened sensitivity to normal stimuli. Touch feels stronger than it should. Pressure registers as more intense. Temperature changes feel amplified. Your clothing might feel rough when it never did before. A handshake might feel uncomfortably firm. This is the most common form of retatrutide skin sensitivity, accounting for the majority of the 7% incidence rate reported in clinical trials.
Allodynia
This is the more severe form. Normal, non-painful stimuli actually trigger pain responses. A bedsheet draped across your legs hurts. The seam of a shirt pressing against your shoulder creates genuine discomfort. Running water across your skin stings. Allodynia represents a neurological misfiring where your central nervous system has, temporarily, lost the ability to correctly categorize incoming sensory data. Researchers studying allodynia with semaglutide have documented similar patterns across the entire GLP-1 drug class.
Dysesthesia
This covers abnormal sensations that do not fit neatly into pain or sensitivity categories. Tingling without an obvious cause. Burning sensations on skin that is not warm. A crawling feeling. Numbness alternating with sharp awareness. Dysesthesia is less common than hyperesthesia but more distressing for those who experience it because the sensations are harder to describe and harder to predict.
In the Phase 2 trial published in the New England Journal of Medicine, researchers documented cutaneous hyperesthesia in approximately 7% of retatrutide participants compared to just 1% in the placebo group. None of these events were classified as severe. None led to treatment discontinuation. But that 7% represents real people dealing with real symptoms that affect daily life, and the clinical data alone does not capture what it actually feels like to live with altered skin sensation for weeks.
Why retatrutide causes skin sensitivity
The honest answer is that researchers do not fully understand the mechanism yet. But the evidence points in several directions, and understanding these potential pathways helps explain why the symptoms manifest the way they do, and why they typically resolve.
GLP-1 receptor expression in the nervous system
GLP-1 receptors are not limited to the pancreas and gut. They exist throughout the central and peripheral nervous system. When retatrutide activates these receptors, it does not just affect insulin secretion and appetite. It modulates neuronal signaling in ways that are still being mapped. The skin is densely innervated with sensory neurons, many of which express GLP-1 receptors. When these receptors get activated by a potent triple agonist like retatrutide, the result can be altered sensory processing.
Think of it this way. Your nervous system has a volume dial for sensory input. Retatrutide can turn that dial up. Not permanently. Not dangerously. But enough that normal sensations feel amplified until your nervous system recalibrates.
The triple-receptor factor
Retatrutide is unique among weight loss peptides because it activates three receptors simultaneously. GLP-1. GIP. And glucagon. This triple activation is what makes it so effective for fat loss, with Phase 2 data showing up to 24% body weight reduction. But it also means retatrutide interacts with a broader range of neural pathways than single or dual agonists.
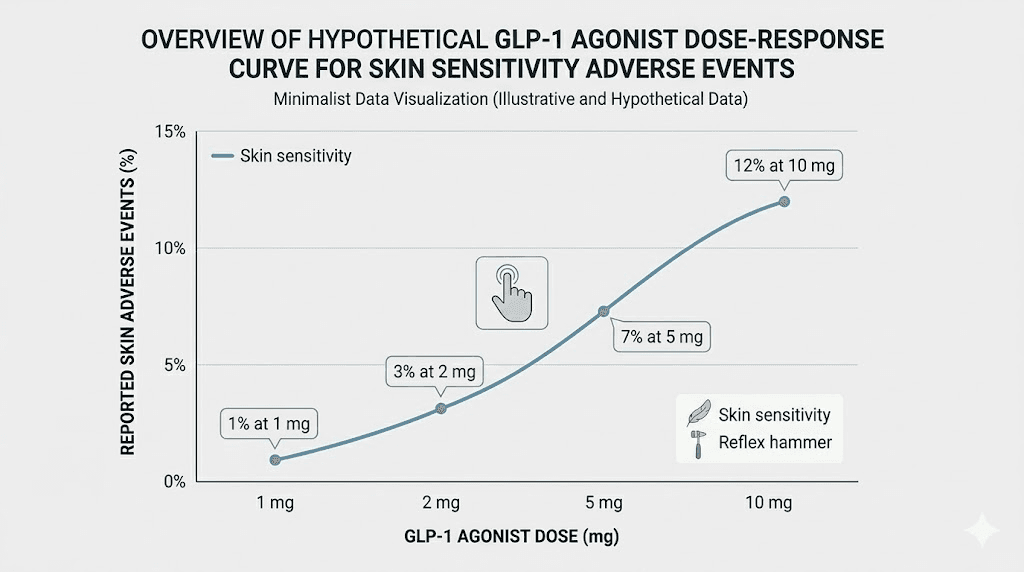
When you compare the skin sensitivity rates across the GLP-1 drug class, an interesting pattern emerges. Semaglutide, a pure GLP-1 agonist, shows lower rates of skin sensitivity. Tirzepatide, a dual GIP/GLP-1 agonist, shows intermediate rates. And retatrutide, the triple agonist, shows the highest rates. This dose-response relationship across receptor activation suggests that the more pathways you stimulate, the higher the likelihood of neurological side effects including skin sensitivity.
Dose-dependent relationship
The STEP UP trial for oral semaglutide provides compelling parallel evidence. Dysesthesia occurred in 22.9% of participants at the 7.2mg dose versus only 6% at the 2.4mg dose and 0.5% with placebo. This massive dose-dependent gap strongly suggests that higher drug exposure increases the probability of altered skin sensation. With retatrutide dosing, the same principle applies. Higher doses correlate with higher rates of skin sensitivity. This is actually useful information because it means dose adjustment is a viable management strategy.
Microvascular effects
One emerging hypothesis involves changes to small blood vessels in the skin. GLP-1 receptor activation affects vascular function, and changes in microvascular blood flow could alter how sensory nerves in the skin behave. Increased blood flow to certain skin areas might sensitize local nerve endings. Decreased flow to others might create numbness or tingling. This vascular theory would explain why skin sensitivity often affects different body regions at different times, and why it can fluctuate throughout the day.
Long-term potentiation of sensory nerves
The most technically accurate explanation involves a phenomenon called long-term potentiation, or LTP. This is a process where repeated stimulation of neural pathways makes them more responsive over time. Normally, LTP is associated with learning and memory formation in the brain. But it can also occur in sensory nerve pathways. When retatrutide continuously activates GLP-1 receptors on sensory neurons, those neurons can become "trained" to fire more easily, lowering the threshold for what triggers a sensory response. The good news: this potentiation is reversible once the stimulus (the drug) is removed or the nervous system adapts.
When skin sensitivity starts and how long it lasts
Timing matters. If you know when to expect symptoms, you can prepare. If you know how long they typically last, you can make informed decisions about whether to continue, adjust, or pause your retatrutide protocol.
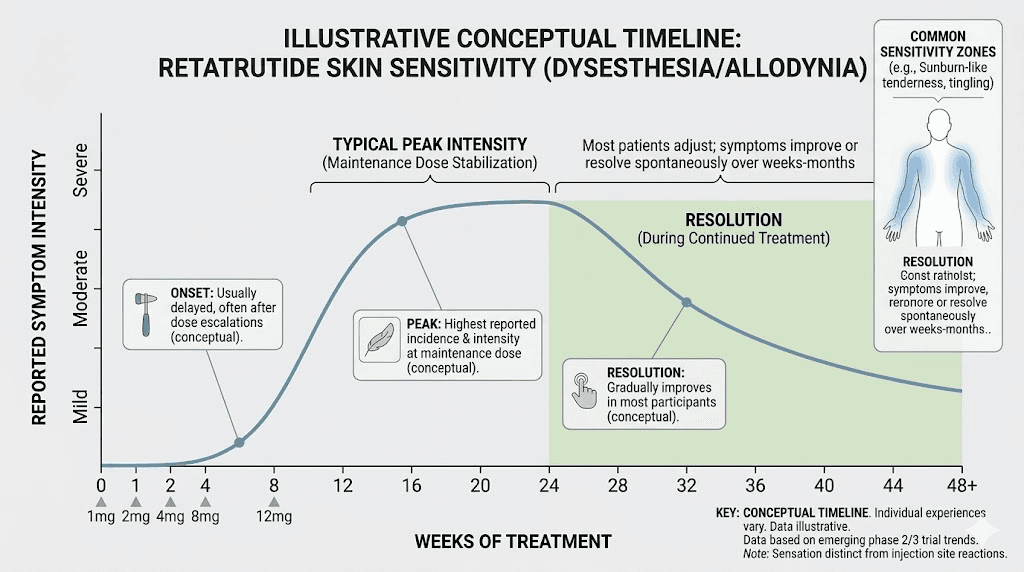
Onset timeline
Most cases of retatrutide skin sensitivity appear within the first 2 to 6 weeks of starting treatment, often coinciding with dose escalation phases. The standard dose schedule involves gradual increases, and many people first notice skin changes when they step up to a higher dose. Some experience sensitivity from the very first injection. Others do not notice anything until reaching the 4mg or 8mg dose range. The variability is significant.
There is also a subset of users who experience delayed onset, with skin sensitivity appearing after 8 to 12 weeks of stable dosing. This delayed presentation may relate to cumulative receptor activation and gradual changes in neural sensitivity thresholds.
Duration and resolution
Here is the most important number in this entire article. For approximately 70 to 80% of affected individuals, skin sensitivity improves significantly within 2 to 4 weeks. The body adapts. The nervous system recalibrates. The volume dial gradually turns back down to normal.
That means most people who develop this side effect can expect meaningful improvement without changing anything about their protocol. Just time.
For the remaining 20 to 30%, symptoms may persist longer, sometimes throughout the entire treatment period, though typically at reduced intensity compared to the initial onset. A small percentage find that symptoms only fully resolve after discontinuing the medication.
The adaptation curve
Understanding the adaptation curve helps manage expectations and reduces anxiety, which itself can worsen the perception of skin sensitivity. Here is what the typical progression looks like:
Week 1 to 2: Initial onset. Symptoms feel most intense during this window because your nervous system has not yet begun adapting. This is when many people panic and want to stop immediately.
Week 2 to 4: Peak and plateau. Symptoms may peak around weeks 2 to 3, then begin a gradual decline. The decline is often irregular, with good days and bad days rather than a smooth improvement curve.
Week 4 to 8: Significant improvement. Most people report that symptoms have decreased by 50 to 70% by this point. The sensitivity becomes more predictable and easier to manage.
Week 8 and beyond: Resolution or stabilization. For the majority, symptoms have resolved or reduced to a level that does not meaningfully impact daily life. For a minority, residual sensitivity persists but becomes their new normal.
Skin sensitivity versus injection site reactions
These are two completely different things, and confusing them leads to wrong management decisions. Understanding the distinction is critical for anyone on a retatrutide injection protocol.
Injection site reactions
These are localized responses at the exact spot where the needle entered your skin. Redness, slight swelling, itching, or a small nodule at the injection site. They are caused by the physical act of injection plus local immune response to the injected substance. Injection site reactions occurred in 5 to 15% of retatrutide trial participants and are generally mild, resolving within 24 to 72 hours.
Management is straightforward. Rotate injection sites. Apply a cool compress. Use proper injection technique. These reactions are not neurological. They are local tissue responses.
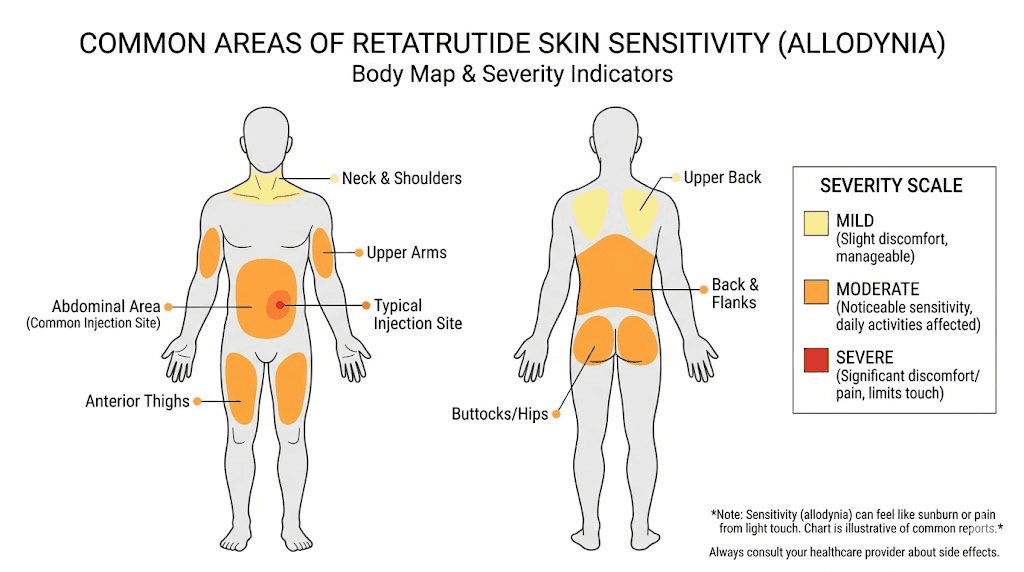
Systemic skin sensitivity
This is the topic of this article. Systemic skin sensitivity affects areas far from the injection site. It involves altered nerve signaling, not local immune response. It does not look like a rash or redness. It feels like changed perception, heightened awareness, amplified sensation. You might feel it on your arms, legs, back, face, or anywhere on your body, and the affected areas can shift.
The key differentiator: injection site reactions are visible and localized. Systemic skin sensitivity is invisible and widespread. If someone looks at your skin and sees nothing unusual, but you feel everything differently, that is systemic sensitivity.
Who is most at risk
Not everyone on retatrutide will develop skin sensitivity. Understanding risk factors helps you assess your own likelihood and prepare accordingly.
Higher dose users
The dose-response relationship is clear. People on higher doses of retatrutide are more likely to experience skin sensitivity than those on lower doses. If you are on the maximum dose range (8 to 12mg), your risk is higher than someone on microdoses. This is consistent across the GLP-1 class, as the STEP UP trial showed dramatically higher dysesthesia rates at higher semaglutide doses.
Rapid dose escalation
People who increase their dose quickly, skipping steps in the recommended dose schedule, appear more likely to develop skin sensitivity. Gradual escalation gives the nervous system time to adapt incrementally. Jumping from a low dose to a high dose can overwhelm sensory pathways.
History of neuropathic conditions
People with pre-existing conditions involving nerve sensitivity, such as fibromyalgia, diabetic neuropathy, or chronic pain syndromes, may be at elevated risk. Their nervous systems are already operating at a heightened baseline, and the additional stimulus from retatrutide can push them past their tolerance threshold.
Female sex
While the trial data does not provide a definitive gender breakdown for skin sensitivity specifically, studies on allodynia and dysesthesia across the GLP-1 class suggest women may be slightly more susceptible than men. This aligns with broader pain research showing sex-based differences in pain perception and sensitization.
Concurrent medications
Certain medications that affect nerve function, including some antidepressants, gabapentinoids, and other neuroactive drugs, might interact with retatrutide in ways that increase skin sensitivity risk. If you are combining medications, discuss potential interactions with your healthcare provider.
Comparing retatrutide skin effects to other GLP-1 medications
If you are considering switching between GLP-1 medications due to skin sensitivity, understanding the comparative landscape helps inform that decision.
Medication | Receptor targets | Skin sensitivity rate | Severity | Resolution timeline |
|---|---|---|---|---|
Retatrutide | GLP-1 + GIP + Glucagon | ~7% | Mild to moderate | 2-4 weeks typical |
GLP-1 only | ~2-6% (dose-dependent) | Mild to moderate | Weeks to months | |
GLP-1 + GIP | ~3-5% | Mild | 2-6 weeks | |
Amylin receptor | Data limited | Mild | Variable |
The pattern supports the receptor-load hypothesis. More receptor targets equals more neurological modulation equals higher likelihood of skin sensitivity. However, individual variation is enormous. Some people on maximum-dose retatrutide have zero skin issues, while others develop sensitivity on low-dose semaglutide. Your personal neurology matters more than population averages.
SeekPeptides members can access detailed comparison tools to help evaluate which medication aligns best with their tolerance profile and goals.
Specific symptoms and what they mean
Not all skin sensitivity is the same. Identifying your specific symptoms helps determine the most effective management strategy.
Sensitivity to touch
Clothes feel rough. Bedsheets feel heavy. A handshake feels too firm. Light touch registers as moderate pressure. This is classic hyperesthesia and is the most commonly reported symptom among retatrutide users experiencing skin sensitivity. It is uncomfortable but not typically painful.
What it means: Your tactile sensory neurons have a lowered activation threshold. They are firing in response to stimuli that normally would not trigger a strong signal. This usually responds well to time and does not indicate anything structurally wrong with your skin or nerves.
Pain from non-painful stimuli
This is allodynia. Different from heightened sensitivity because the response is actually painful. Water from a shower stings. The weight of a blanket creates aching pressure. Even air moving across skin can feel sharp. If you have experienced this, you understand why it is distressing.
What it means: Your central nervous system is misclassifying sensory input. Signals that should register as "touch" are being routed through pain pathways. This is more significant than hyperesthesia and warrants closer monitoring. Read the full allodynia guide for deeper context on this condition across GLP-1 medications.
Burning or tingling sensations
A burning feeling on skin that is not hot. Tingling that resembles the "pins and needles" of a limb falling asleep, but without an obvious cause. These dysesthetic symptoms can occur anywhere on the body and may migrate, appearing on arms one day and legs the next.
What it means: Sensory nerve signaling is disordered. The nerves are generating sensory reports without appropriate external stimuli. While disconcerting, this pattern typically resolves as the nervous system adapts to retatrutide.
Temperature sensitivity
Feeling cold when the room is warm. Feeling hot when the temperature is normal. Water temperature in the shower feels much hotter or colder than it actually is. Some retatrutide users report similar patterns to those seen in people who experience cold sensitivity on tirzepatide or semaglutide.
What it means: Thermoregulatory nerve fibers are affected. This can overlap with the metabolic changes retatrutide creates (increased fat burning and metabolic rate changes can independently affect temperature perception).
Skin sensitivity to pressure
Sitting in a chair feels harder than usual. Wearing a belt or watch feels uncomfortable. Pressure from leaning on an elbow creates disproportionate discomfort. This baroesthetic sensitivity specifically affects mechanoreceptors that detect pressure.
What it means: Deep pressure sensors in the skin and underlying tissue have become hypersensitive. This tends to resolve more slowly than surface touch sensitivity but responds well to desensitization techniques.
Proven management strategies
You do not have to simply endure skin sensitivity and wait for it to pass. Multiple management approaches can meaningfully reduce symptoms while your body adapts. Start with the simplest interventions and escalate if needed.
Strategy 1: Temperature management
Cool compresses applied to sensitive areas for 10 to 15 minutes can temporarily reduce nerve firing and provide relief. The cold slightly numbs sensory nerve endings, turning that volume dial back down for a while. Avoid ice directly on skin, as this can cause damage. Use a cloth-wrapped cold pack or a cool, damp towel.
For temperature sensitivity specifically, avoid extreme temperature changes. Lukewarm showers instead of hot. Gradual temperature transitions rather than sudden shifts. Layer clothing so you can adjust to temperature changes without dramatic swings.
Strategy 2: Over-the-counter antihistamines
Non-sedating antihistamines like cetirizine (Zyrtec) or loratadine (Claritin) can reduce skin sensitivity for some users. While skin sensitivity from retatrutide is not an allergic reaction per se, antihistamines modulate histamine receptors in the skin that can amplify sensory signals. Taking a daily antihistamine during the adaptation period has been reported to reduce symptom intensity by 30 to 50% in some cases.
Sedating antihistamines like diphenhydramine (Benadryl) can be used at night if skin sensitivity is disrupting sleep, but they should not be relied on long-term.
Strategy 3: Clothing and fabric choices
This sounds simple, but it makes a significant difference. During periods of heightened skin sensitivity, switch to soft, seamless fabrics. Cotton and bamboo tend to be best tolerated. Avoid synthetic materials that create friction. Loose-fitting clothes reduce the amount of fabric-to-skin contact. Tagless clothing eliminates one common irritation point.
For bedding, consider smooth, high-thread-count sheets. Some people find that a silk or satin pillowcase dramatically reduces facial skin sensitivity at night.
Strategy 4: Dose adjustment
Given the clear dose-response relationship, reducing your retatrutide dose temporarily can reduce skin sensitivity. This does not mean abandoning your protocol. It means stepping back one dose level, allowing your nervous system to adapt, and then cautiously resuming escalation after 2 to 4 weeks. Use the retatrutide dosage calculator to determine appropriate adjustment levels.
Many researchers have found that a slower, more gradual dose escalation eliminates skin sensitivity entirely. What triggers symptoms at a fast escalation rate may produce no symptoms at all when the same total dose is reached more slowly.
Strategy 5: Topical treatments
For localized skin sensitivity, topical lidocaine (available over-the-counter in most countries) can provide temporary numbing relief. Apply a thin layer to the most sensitive areas. Capsaicin cream, paradoxically, can help with chronic skin sensitivity by gradually desensitizing nerve endings. It works by depleting substance P, a neurotransmitter involved in pain signaling. The initial application may briefly increase sensitivity before the desensitizing effect kicks in.
Aloe vera and calamine lotion can soothe surface-level irritation that sometimes accompanies the deeper neurological sensitivity.
Strategy 6: Stress management
Stress amplifies pain perception. That is not opinion. It is neuroscience. Cortisol and adrenaline lower sensory thresholds, making already-sensitive skin feel even more reactive. If you are anxious about your skin sensitivity (understandable), that anxiety itself worsens the sensation.
Mindfulness, meditation, deep breathing exercises, and adequate sleep all help regulate the neurological systems involved in sensory processing. This is not a dismissive "just relax" suggestion. It is a clinically supported intervention that can meaningfully reduce how intensely you perceive skin sensitivity.
Strategy 7: Gentle desensitization
Deliberately exposing sensitive skin to controlled, gentle stimulation can help recalibrate nerve responses. Light massage with smooth tools. Gentle brushing with a soft-bristle brush. Progressive exposure to textures that trigger mild sensitivity. The principle is the same as exposure therapy, gradually teaching your nervous system that the stimulus is not threatening.
Start with barely-perceptible stimulation and gradually increase intensity over days. This should never be painful. If a stimulus causes pain, you are pushing too hard.
Retatrutide skin rash and allergic reactions
Separate from the neurological skin sensitivity discussed above, some retatrutide users experience actual dermatological reactions. These involve visible skin changes rather than altered sensation.
Rash
A small percentage of trial participants developed skin rashes, typically presenting as small red patches or bumps. These are distinct from injection site reactions because they can appear anywhere on the body. Most rashes are classified as mild and self-limiting, resolving without specific treatment within 1 to 2 weeks.
Pruritus (itching)
Generalized itching without visible skin changes is reported by some retatrutide users. This may overlap with the neurological sensitivity (your skin "thinks" it itches because of altered nerve signaling) or may represent a mild immune-mediated response. Antihistamines are the first-line treatment and are usually effective.
Urticaria (hives)
Raised, itchy welts on the skin. Less common than rash or itching alone. Urticaria typically indicates a histamine-mediated immune response. If hives are widespread or accompanied by other symptoms (swelling of the face or throat, difficulty breathing, rapid heartbeat), seek emergency medical attention immediately. However, isolated, mild hives are manageable with antihistamines and do not necessarily require stopping retatrutide.
What about anaphylaxis?
No cases of anaphylaxis or life-threatening allergic reactions have been reported in the retatrutide trial literature. This is reassuring. While theoretically possible with any injectable peptide, the risk appears to be extremely low.
Skin sensitivity and the retatrutide dose escalation schedule
The relationship between dose timing and skin sensitivity has practical implications for how you structure your retatrutide protocol.
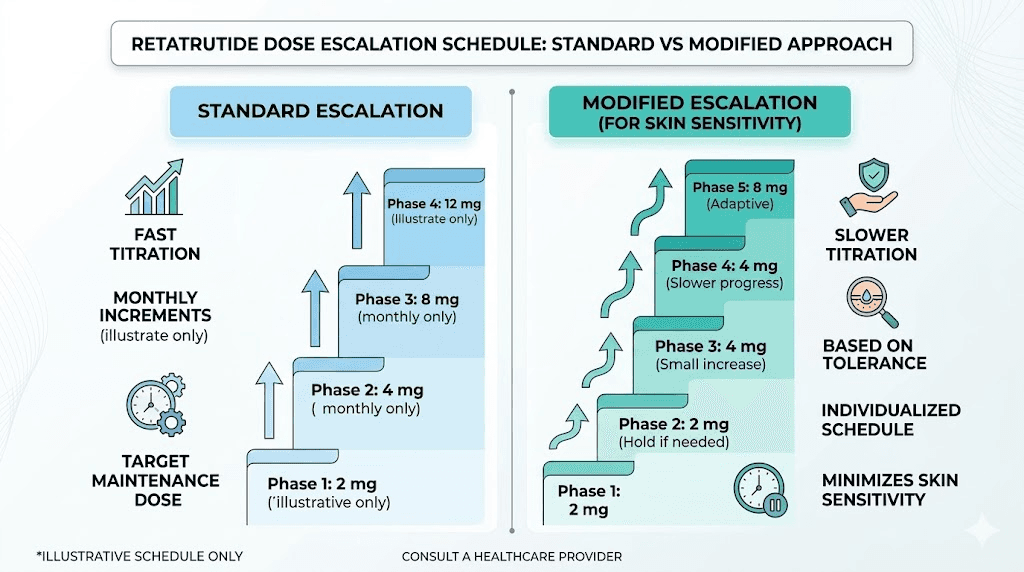
Standard escalation approach
The typical retatrutide dose escalation starts low and increases over several weeks. Each step up represents a new level of receptor activation, and each step is a potential trigger point for skin sensitivity onset. If you are following the standard dosage chart, pay close attention to how your skin responds at each new dose level.
Modified escalation for skin-sensitive individuals
If you have a history of skin sensitivity, neuropathic conditions, or have already experienced sensitivity at lower doses, consider a modified approach. Instead of standard dose increases, use smaller increments. Extend the time at each dose level from the typical schedule to double the usual duration. This gives your nervous system more adaptation time at each exposure level.
For example, if the standard protocol calls for increasing from 2mg to 4mg after 4 weeks, a skin-sensitive individual might go from 2mg to 3mg, hold for 4 weeks, then move to 4mg. The final dose achieved is the same, but the pathway there is gentler on the nervous system. Explore retatrutide microdosing strategies for more granular dose adjustment options.
Timing your dose
Some users report that skin sensitivity peaks in the 24 to 48 hours after injection, then gradually improves until the next dose. If this pattern applies to you, timing activities around this cycle can help. Schedule high-comfort-demand activities (massages, physical therapy, social events) for the latter half of your dosing cycle when sensitivity is lowest. The best time to take retatrutide may also factor into your symptom management strategy.
The connection to rapid weight loss
Retatrutide produces substantial weight loss. Phase 2 trials showed up to 24% body weight reduction. This magnitude of weight loss itself can affect skin and nerve function, independent of the direct pharmacological effects.
Loose skin and nerve repositioning
As subcutaneous fat decreases, the skin that previously stretched over that fat tissue becomes relatively loose. Nerve endings that were previously cushioned by fat are now closer to the surface, potentially more exposed to external stimuli. This physical repositioning of nerve fibers can contribute to altered sensation. It is a mechanical explanation that complements the pharmacological one.
Nutritional factors
Rapid weight loss can lead to nutritional deficiencies that affect nerve function. Vitamin B12 deficiency, in particular, is associated with peripheral neuropathy and altered skin sensation. Many GLP-1 medications reduce appetite significantly, and people on retatrutide may eat substantially less, increasing the risk of micronutrient deficiencies. Ensuring adequate nutrition, particularly B vitamins, is an important part of managing and preventing skin sensitivity.
Several companion compounds like semaglutide with B12 and tirzepatide with B12 have emerged specifically to address this concern. Supplementation strategies designed for GLP-1 users can help maintain nerve health during treatment.
Dehydration
GLP-1 medications can cause dehydration through reduced fluid intake (you are simply drinking less) and increased fluid loss (particularly if GI side effects are present). Dehydration affects skin turgor and nerve function. Staying well-hydrated is one of the simplest interventions for reducing skin sensitivity.
How skin sensitivity compares to other retatrutide side effects
Putting skin sensitivity in context with other retatrutide side effects helps you understand where it falls on the severity and management spectrum.
Side effect | Frequency | Severity | Duration | Management difficulty |
|---|---|---|---|---|
Nausea | ~25-40% | Mild to moderate | 2-4 weeks | Easy |
~15-25% | Mild to moderate | 1-3 weeks | Easy | |
Skin sensitivity | ~7% | Mild to moderate | 2-4 weeks | Moderate |
Injection site reactions | ~5-15% | Mild | 24-72 hours | Easy |
~3-5% | Mild | Variable | Moderate | |
~10-15% | Mild to moderate | 2-6 weeks | Moderate |
Skin sensitivity is less common than the classic GI side effects but can be more psychologically distressing because it is less understood and less frequently discussed. Many people expect nausea on GLP-1 medications. Few expect their skin to feel fundamentally different.
When to continue, when to adjust, and when to stop
The decision to push through skin sensitivity versus modifying your protocol versus stopping entirely depends on several factors.
Continue without changes when
Symptoms are mild. Your daily life is not significantly impacted. The sensitivity has been stable or improving. You are still in the first 4 weeks (the adaptation window). You have not needed any pain medication. Under these circumstances, the evidence strongly supports waiting. Most cases resolve.
Adjust your protocol when
Symptoms are moderate and interfering with daily activities, specifically sleep, work, or exercise. Simple management strategies (cool compresses, antihistamines) provide partial but not complete relief. Symptoms have not improved after 4 weeks. You are on a higher dose and have room to step down temporarily. In these cases, discuss dose reduction or slower escalation with your healthcare provider. Use the dosage calculator to map out a modified schedule.
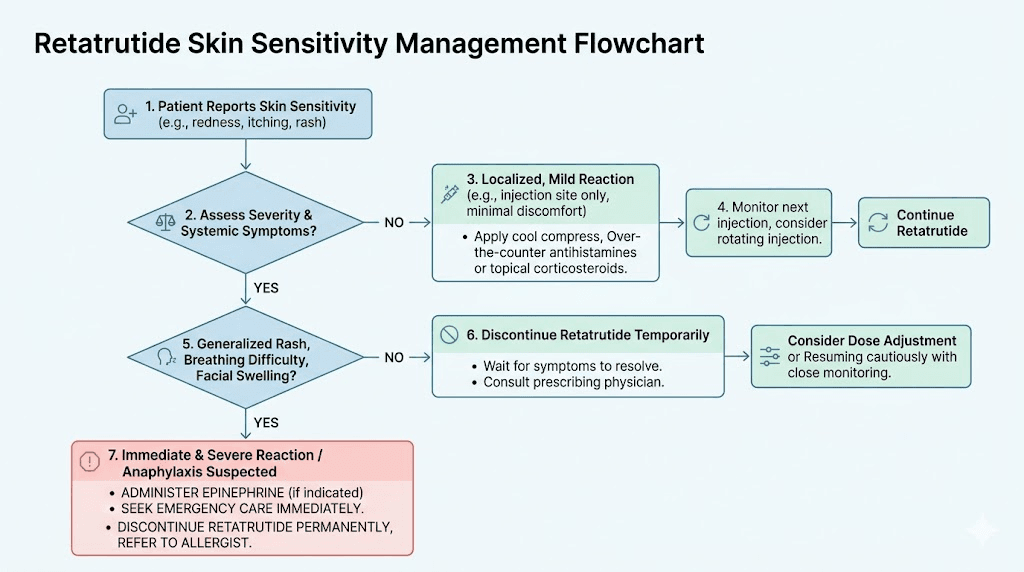
Stop and seek medical evaluation when
You experience severe pain from normal touch (significant allodynia). Symptoms are getting progressively worse rather than stabilizing. You develop widespread rash with systemic symptoms (fever, swelling, breathing difficulty). Numbness or weakness accompanies the sensitivity (possible nerve damage rather than sensitivity). Symptoms are severely impacting your quality of life despite management efforts.
Stopping retatrutide typically results in complete resolution of skin sensitivity. Published case data shows symptoms resolve within days to weeks of discontinuation. This reversibility is reassuring and is consistent with a functional (nerve sensitization) rather than structural (nerve damage) mechanism.
The psychological impact of skin sensitivity
Clinical trials measure severity on standardized scales. They do not capture what it feels like to flinch when your partner touches your arm. They do not measure the frustration of being uncomfortable in your own clothing. They do not quantify the anxiety of wondering whether something is seriously wrong.
The psychological burden of skin sensitivity is real and valid. Acknowledging it is not weakness. It is an appropriate response to your body behaving in unfamiliar ways.
Anxiety amplification cycle
Here is the trap many people fall into. Skin sensitivity causes anxiety. Anxiety increases cortisol. Cortisol lowers sensory thresholds. Lower thresholds make skin sensitivity worse. Worse sensitivity causes more anxiety. The cycle accelerates.
Breaking this cycle requires conscious intervention. Remind yourself that this side effect is well-documented, temporary in most cases, and not indicative of serious harm. Seek support from communities of people who have experienced the same thing. SeekPeptides offers access to a community of experienced researchers who have navigated these exact challenges and can provide perspective that clinical data alone cannot.
Sleep disruption
Skin sensitivity frequently disrupts sleep. The pressure of a mattress, the weight of blankets, the texture of sheets, things you never noticed before suddenly demand attention. Poor sleep then worsens pain perception, creating another negative cycle.
Prioritize sleep hygiene during this period. Consider a lighter blanket. Use smooth, high-thread-count sheets. Sleep in minimal clothing. A cool bedroom temperature (65 to 68 degrees Fahrenheit) can help because cooler temperatures slightly reduce nerve firing rates.
Long-term outlook and what the research shows
Retatrutide is still in clinical development, with Phase 3 trials ongoing. The long-term skin sensitivity data is therefore limited to Phase 2 trial duration plus emerging real-world reports.
What we know
Skin sensitivity in Phase 2 trials was classified as mild to moderate in all reported cases. No participant discontinued treatment due to skin sensitivity alone. The 7% incidence rate was consistent across dose groups, though higher doses trended toward higher rates. Resolution occurred for the majority within the trial period. No cases of permanent nerve damage or lasting skin changes were reported.
What we do not know yet
Long-term incidence rates over 1 to 2+ years of continuous use. Whether tolerance develops completely in all users. Whether intermittent dosing protocols affect skin sensitivity patterns. The exact mechanism, which means current management strategies are symptom-based rather than targeted.
The GLP-1 class context
Skin sensitivity is emerging as a recognized class-wide effect of GLP-1 receptor agonists. As semaglutide and tirzepatide have been used by millions of people worldwide, the data on skin-related side effects has grown substantially. A case series published in the American Journal of Health-System Pharmacy documented allodynia specifically associated with semaglutide, and a Cureus publication detailed dysesthesia and allodynia with both semaglutide and tirzepatide. This growing body of evidence suggests that as retatrutide reaches wider use, our understanding of its skin effects will deepen significantly.
Practical protocol for managing retatrutide skin sensitivity
Here is a structured, step-by-step approach to follow if you develop skin sensitivity on retatrutide. This protocol combines the clinical evidence with practical experience from researchers who have managed this side effect successfully.
Week 1: Assessment and baseline management
Document your symptoms. Write down exactly what you feel, where you feel it, how intense it is on a 1 to 10 scale, and when it started relative to your last dose. This baseline becomes your comparison point for tracking improvement.
Start simple interventions. Cool compresses for acute discomfort. Switch to soft, loose clothing. Begin a daily non-sedating antihistamine. Ensure adequate hydration (minimum 2 liters of water daily).
Check your nutrition. Are you eating enough? Specifically, are you getting adequate B vitamins, omega-3 fatty acids, and magnesium? These nutrients support nerve function. Consider a B-complex supplement. Review dietary recommendations for GLP-1 users and apply the same principles.
Do not change your dose yet. Give the simple interventions time to work. Panicking and immediately dropping your dose may not be necessary if your body was going to adapt on its own.
Week 2: Evaluation and escalation
Compare to baseline. Has the sensitivity stayed the same, improved, or worsened? If improved even slightly, that is a positive sign suggesting adaptation is occurring.
If stable or improved: Continue baseline management. Begin gentle desensitization exercises. Maintain your current retatrutide dose.
If worsening: Add topical lidocaine for the most affected areas. Consider sedating antihistamine at bedtime if sleep is affected. Contact your healthcare provider to discuss potential dose adjustment.
Week 3 to 4: Decision point
If symptoms are improving: Stay the course. Most cases resolve by week 4. Continue all management strategies. You may begin to gradually reduce antihistamine use.
If symptoms are persistent but manageable: Consider a temporary dose reduction of one step in the escalation schedule. Maintain reduced dose for 2 to 4 weeks before attempting re-escalation.
If symptoms are persistent and significantly impacting quality of life: Discuss with your healthcare provider whether continued treatment is appropriate. Explore alternative GLP-1 medications with potentially lower skin sensitivity profiles. Switching protocols between different GLP-1 agents is well-documented.
Week 4 and beyond: Maintenance
For those whose symptoms have resolved or significantly improved, you can gradually resume dose escalation if you had stepped down. Increase slowly. If sensitivity returns at a specific dose, that is your current threshold, and you may need to hold at the dose below it for a longer period before attempting another increase.
Natural remedies and supportive approaches
Beyond pharmaceutical interventions, several natural approaches can support nerve health and reduce skin sensitivity.
Omega-3 fatty acids
EPA and DHA from fish oil have well-documented anti-inflammatory and neuroprotective properties. Doses of 2 to 4 grams daily of combined EPA/DHA may help modulate nerve sensitivity. These fatty acids are incorporated into nerve cell membranes and influence how neurons signal.
Alpha-lipoic acid
Used extensively in Europe for diabetic neuropathy, alpha-lipoic acid at 600mg daily has shown benefits for peripheral nerve function. It acts as an antioxidant specifically in neural tissue and may help reduce the sensitization process that underlies retatrutide skin sensitivity.
Magnesium
Magnesium plays a critical role in nerve signal transmission. Deficiency can exacerbate nerve sensitivity. Magnesium glycinate at 200 to 400mg daily is well-absorbed and may help regulate the excitability of sensory neurons. Many people on calorie-restricted GLP-1 diets are not getting enough magnesium from food alone.
B-complex vitamins
B1 (thiamine), B6 (pyridoxine), and B12 (methylcobalamin) are all critical for nerve health. The combination of GLP-1 medication with reduced food intake creates a perfect storm for B-vitamin depletion. A high-quality B-complex supplement or specific methylcobalamin formulations can help maintain the nerve function that protects against excessive skin sensitivity.
Epsom salt baths
Magnesium sulfate absorbed through the skin during a warm (not hot) bath can provide both magnesium supplementation and temporary sensory relief. The warm water provides gentle, uniform sensory input that can help "reset" sensitized nerve pathways. Twenty to thirty minutes, 2 to 3 times per week.
Acupuncture
While the evidence base is mixed, acupuncture has shown benefits for various neuropathic pain conditions. The mechanism likely involves modulation of pain signaling pathways and endorphin release. Some retatrutide users report meaningful improvement in skin sensitivity following acupuncture sessions.
What to tell your doctor
If you are discussing retatrutide skin sensitivity with a healthcare provider, clear communication helps ensure you get appropriate care.
Information to provide
When the sensitivity started relative to starting retatrutide or changing your dose. Exactly where on your body you feel it and whether it moves. What triggers the sensation (touch, pressure, temperature, nothing). How intense it is on a scale of 1 to 10. Whether it is getting better, worse, or staying the same. What you have tried and what has or has not helped. Any other medications you are taking. Any history of nerve-related conditions.
Questions to ask
Should I continue my current dose? Would a temporary dose reduction be appropriate? Are there any tests you recommend to rule out other causes? Is this consistent with what you have seen in other patients on GLP-1 medications? At what point should I consider switching to a different medication?
Red flags that require immediate medical attention
Severe, worsening pain that does not respond to any management. Facial swelling, throat tightness, or difficulty breathing (potential anaphylaxis). Numbness or weakness in limbs (potential nerve damage). Skin changes accompanied by fever (potential allergic reaction or infection). Rapid onset of widespread hives with systemic symptoms.
Retatrutide skin sensitivity in the context of your overall protocol
Skin sensitivity does not exist in isolation. It is one factor among many when evaluating whether retatrutide is the right choice for your goals.
Weighing benefits against side effects
Retatrutide has demonstrated the most potent weight loss efficacy of any GLP-1 medication studied to date. Up to 24% body weight reduction in Phase 2 trials. For people with significant fat loss goals, this level of efficacy may justify tolerating temporary skin sensitivity. The key word is "temporary." If you are in the 70 to 80% whose symptoms resolve within weeks, a brief period of discomfort may be a reasonable trade-off.
Optimizing other aspects of your protocol
While managing skin sensitivity, do not neglect other protocol components. Understanding your results timeline helps set expectations. Maintaining proper reconstitution and storage ensures you are getting the full dose you expect. Proper injection technique minimizes local reactions that can compound systemic sensitivity.
Considering alternatives
If skin sensitivity is severe or persistent, exploring alternatives is reasonable. Retatrutide versus semaglutide and retatrutide versus tirzepatide (Mounjaro) comparisons can help you evaluate whether a dual or single agonist might achieve acceptable results with fewer neurological side effects. Some researchers have had success transitioning between medications to find the best balance of efficacy and tolerability.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers comprehensive safety guides, interaction databases, and a community of experienced researchers who have navigated these exact decisions. The depth of member resources available goes well beyond what any single article can provide.
Frequently asked questions
How common is skin sensitivity with retatrutide?
Approximately 7% of participants in the Phase 2 clinical trial experienced skin sensitivity, compared to 1% in the placebo group. This makes it a relatively uncommon but well-documented side effect. The rate appears to be higher than with single-receptor GLP-1 agonists like semaglutide.
Will retatrutide skin sensitivity go away on its own?
For 70 to 80% of affected individuals, skin sensitivity improves significantly within 2 to 4 weeks without any dose changes. The body adapts to the medication, and nerve sensitivity returns toward baseline. A smaller percentage may require dose adjustments or longer adaptation periods.
Is retatrutide skin sensitivity dangerous?
No. All cases reported in clinical trials were classified as mild to moderate. No serious adverse events related to skin sensitivity were documented, and no participants discontinued treatment solely because of this side effect. However, if you experience severe pain, numbness, or weakness, seek medical evaluation to rule out other causes.
Does the dose of retatrutide affect skin sensitivity?
Yes. Clinical evidence across the GLP-1 drug class shows a clear dose-response relationship. Higher doses are associated with higher rates and greater severity of skin sensitivity. This is why gradual dose escalation is recommended and why dose reduction can be an effective management strategy.
Can I take antihistamines with retatrutide for skin sensitivity?
Over-the-counter antihistamines like cetirizine and loratadine are commonly used to manage retatrutide skin sensitivity and are generally safe to combine with the medication. They do not interfere with retatrutide effectiveness. As always, discuss any new medications with your healthcare provider.
Is skin sensitivity from retatrutide different from semaglutide allodynia?
The underlying mechanism appears similar across GLP-1 medications. Retatrutide skin sensitivity and semaglutide allodynia both involve altered nerve signaling and heightened sensory processing. The key difference is that retatrutide, as a triple-receptor agonist, activates more neural pathways and shows a slightly higher incidence rate.
Should I stop retatrutide if I develop skin sensitivity?
Not necessarily. Most cases resolve without stopping. The recommended approach is to try conservative management strategies first (cool compresses, antihistamines, clothing changes), then consider dose adjustment if symptoms persist beyond 4 weeks, and only discuss discontinuation if symptoms are severe and unresponsive to other interventions.
Can nutritional deficiencies worsen retatrutide skin sensitivity?
Yes. B12 deficiency, magnesium deficiency, and omega-3 deficiency can all worsen nerve sensitivity. Because retatrutide reduces appetite significantly, nutritional gaps are common. Proper supplementation is important for nerve health during treatment.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your nerve endings stay calm, your skin stay comfortable, and your protocols stay effective.