Mar 15, 2026

Before you increase your next dose, read this. Retatrutide is the most powerful weight loss peptide in clinical development right now, a triple agonist that hits GLP-1, GIP, and glucagon receptors simultaneously. And with that power comes a digestive system that may not appreciate the sudden change.
Diarrhea is one of the most commonly reported side effects in retatrutide clinical trials, affecting anywhere from 9% to 35% of participants depending on dose level and study phase. That is not a small number. And if you are currently dealing with it, or worried about dealing with it, you need real answers, not vague reassurance.
The good news is that clinical data tells us something encouraging. Most retatrutide-related diarrhea is mild to moderate, peaks during dose escalation, and resolves within 8 to 12 weeks for the majority of participants. The bad news is that those 8 to 12 weeks can feel miserable if you do not know how to manage them properly. This guide breaks down exactly what the Phase 2 and Phase 3 trials found, why retatrutide triggers diarrhea in the first place, and the specific dietary, hydration, and dosing strategies that can make the difference between pushing through successfully and abandoning your protocol entirely. SeekPeptides has analyzed every available clinical dataset to give you the most comprehensive breakdown available anywhere.
What the clinical trials actually found about retatrutide and diarrhea
Numbers matter here. Not vague claims about "some participants experienced GI issues." Real data from real trials with real participants. The most comprehensive evidence comes from three sources: the Phase 2 trial published in the New England Journal of Medicine, the Phase 3 TRIUMPH-4 trial, and a systematic review and meta-analysis that synthesized data from 878 total participants across three randomized controlled trials.
Phase 2 trial results
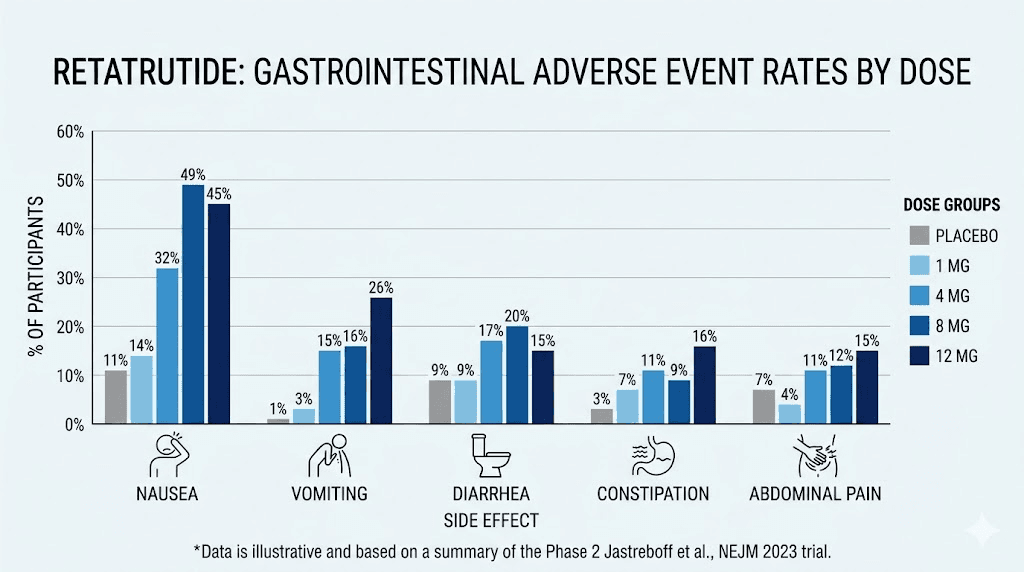
The Phase 2 trial established the dose-response pattern that researchers have been tracking ever since. Gastrointestinal adverse events were the most frequently reported side effects across all retatrutide dose groups, and they occurred primarily during the dose escalation phase of treatment. Diarrhea specifically affected 9% to 20% of participants across dose groups in Phase 2.
That range matters. It tells us something critical about how dose level influences digestive outcomes.
Participants receiving the 8 mg and 12 mg doses reported significantly higher rates of GI side effects than those on lower doses. And here is a detail that gets overlooked constantly: participants who received an initial starting dose of 4 mg experienced more GI symptoms than those who started at 2 mg. That one data point, that single difference in starting dose, changed the entire side effect profile for a meaningful percentage of trial participants. If you are wondering whether your dosage chart matters for digestive comfort, the answer is an unequivocal yes.
The Phase 2 trial also revealed that nausea, diarrhea, constipation, and vomiting were all more common in retatrutide groups than placebo. But unlike nausea, which followed a strictly linear dose-response pattern (more dose equals more nausea), diarrhea rates did not scale as predictably. Some participants at moderate doses experienced more diarrhea than those at the highest dose. This suggests that individual factors, including gut microbiome composition, dietary habits, and injection technique, play a meaningful role in who develops this particular side effect.
Phase 3 TRIUMPH-4 trial results
The Phase 3 TRIUMPH-4 trial enrolled 445 adults with obesity or overweight and knee osteoarthritis, testing 9 mg and 12 mg maintenance doses over 68 weeks. This longer duration gave researchers a clearer picture of how GI side effects evolve over time. The results were revealing.
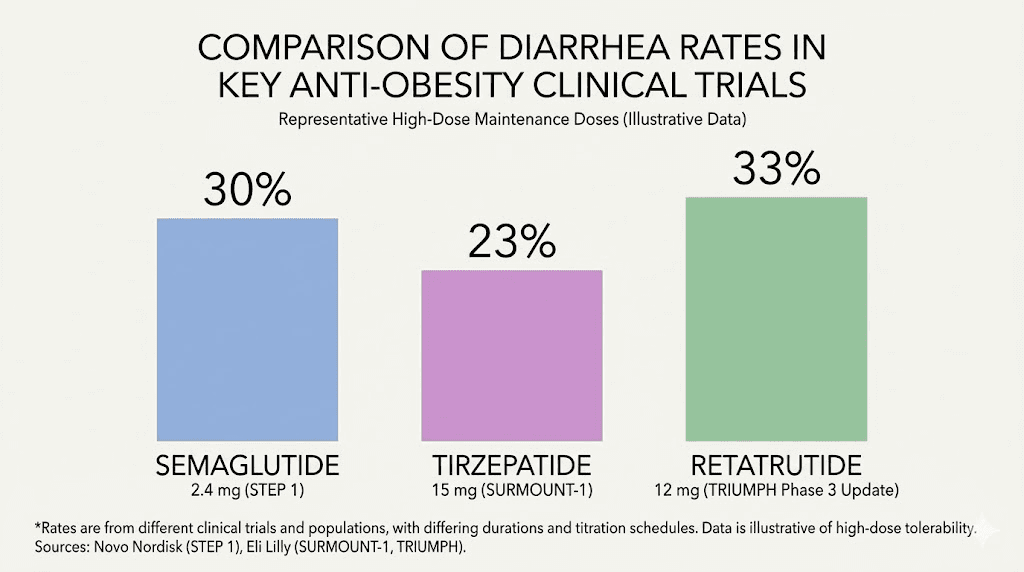
Diarrhea affected 33% to 35% of participants. That is significantly higher than the Phase 2 numbers, and it likely reflects the higher maintenance doses used in TRIUMPH-4 combined with the longer observation period. Nausea hit 38% to 43%. Constipation affected 22% to 25%. Vomiting occurred in 20% to 21% of participants. These are not insignificant numbers, and anyone starting a retatrutide protocol for weight loss needs to understand them upfront.
But context matters enormously. Despite these rates, discontinuation due to adverse events was comparable to other GLP-1 and GIP receptor agonists. Most participants who experienced diarrhea found it tolerable enough to continue treatment. Most saw it resolve or significantly improve after the initial adjustment period. The timeline for retatrutide to work and the timeline for side effects to resolve often overlap, which means the discomfort period frequently coincides with the period before you start seeing meaningful results.
Meta-analysis data: risk ratios by dose
The systematic review that synthesized all available trial data calculated specific risk ratios for diarrhea at each dose level compared to placebo. These numbers are essential for understanding your actual risk profile based on how much retatrutide you are taking.
At 4 mg, the relative risk of diarrhea was 1.64 compared to placebo, with a 95% confidence interval of 0.77 to 3.49. That P value of 0.2 means this increase was not statistically significant at the lowest dose. At 8 mg, the relative risk jumped to 2.51, with a confidence interval of 1.26 to 5.00 and a statistically significant P value of 0.009. At 12 mg, the relative risk was 2.04, with a confidence interval of 1.06 to 3.94 and a P value of 0.03.
Notice something interesting? The 8 mg dose actually showed a higher relative risk for diarrhea than the 12 mg dose. This non-linear pattern suggests that the body may develop some tolerance to the GI effects at higher maintenance doses, particularly after a proper titration schedule. It also reinforces why the dose schedule and dosage chart you follow matter so much for managing side effects.
Why retatrutide causes diarrhea in the first place
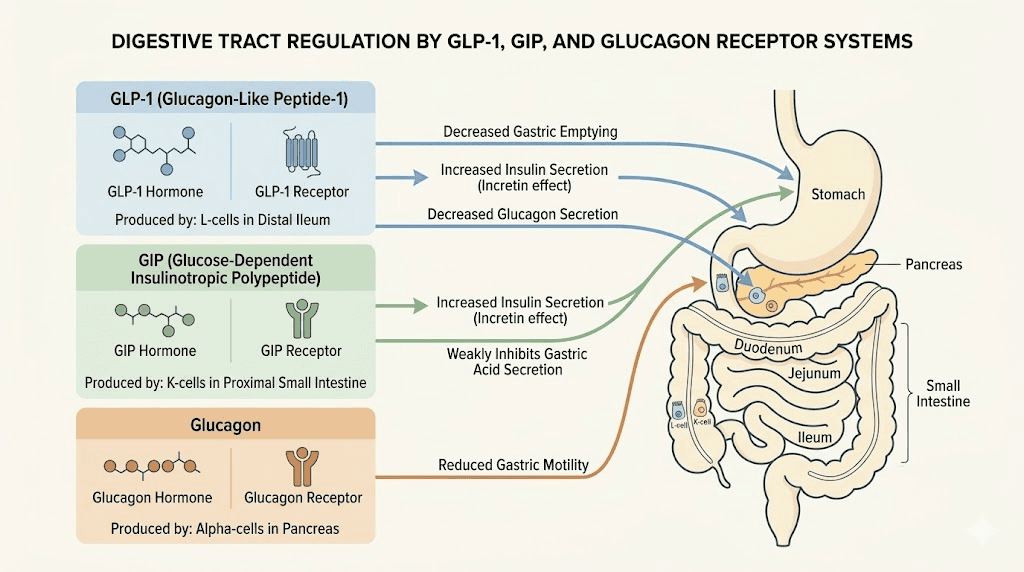
Understanding the mechanism helps you manage the symptom. Retatrutide is not just any peptide. It is a triple agonist that simultaneously activates three different receptor systems: GLP-1, GIP, and glucagon. Each of these receptor systems has distinct effects on the gastrointestinal tract, and the combination creates a unique digestive environment that your body needs time to adapt to.
The GLP-1 receptor effect on gut motility
GLP-1 receptor activation is the primary driver of gastrointestinal side effects in retatrutide, just as it is in pure GLP-1 agonists like semaglutide and dual agonists like tirzepatide. GLP-1 receptors are distributed throughout the enteric nervous system, which is the network of neurons that controls your entire digestive tract independently of your brain. When retatrutide activates these receptors, it fundamentally alters how your gut moves food through the system.
The most well-documented effect is delayed gastric emptying. Your stomach releases food into the small intestine much more slowly than normal. This is actually one of the mechanisms that drives weight loss, as slower gastric emptying means you feel full longer and eat less. But it also means that the normal rhythm of digestion gets disrupted.
Here is where the diarrhea paradox comes in. If GLP-1 agonists primarily slow things down, why does diarrhea occur at all? Should it not cause constipation instead? The answer is complicated, and researchers do not fully understand every mechanism yet. What they do know is that the slowed gastric emptying creates a cascade of downstream effects. Food that sits longer in the stomach can change in composition before reaching the intestines. The small intestine receives food in patterns it is not accustomed to. And in some people, the intestinal transit actually becomes irregular or accelerated as a compensatory response, leading to loose stools or outright diarrhea. If you have experienced diarrhea from tirzepatide or bloating from semaglutide, the mechanism is similar but amplified with retatrutide.
The glucagon receptor complication
What makes retatrutide unique is its glucagon receptor activation. Pure GLP-1 agonists and even dual GLP-1/GIP agonists do not activate this pathway. Glucagon has its own effects on the digestive system, including influences on bile secretion, hepatic glucose output, and gut motility patterns that differ from GLP-1 effects. This triple mechanism is what makes retatrutide different from semaglutide and tirzepatide in both efficacy and side effect profile.
The glucagon receptor stimulation may also raise heart rate slightly, which is a separate concern, but the digestive implications are what matter for diarrhea specifically. Glucagon influences bile acid metabolism, and altered bile acid patterns in the intestines are a well-known trigger for osmotic diarrhea. This may explain why some retatrutide users experience a different quality of diarrhea compared to what they experienced on semaglutide or tirzepatide alone.
The GIP receptor contribution
GIP receptor activation adds another layer. GIP, or glucose-dependent insulinotropic polypeptide, is naturally produced in the gut and plays roles in nutrient absorption and intestinal function. When retatrutide activates GIP receptors alongside GLP-1 and glucagon receptors, the combined effect on intestinal secretions, motility, and absorption patterns creates a complex new digestive environment. Some researchers theorize that the GIP component may actually help moderate some of the harsher GI effects of GLP-1 activation, which could partially explain why retatrutide compared to other agents does not always show proportionally worse GI profiles despite having three active mechanisms.
Gut microbiome changes
Emerging research suggests that GLP-1 receptor agonists may alter the composition of gut bacteria. These changes in the microbiome can influence stool consistency, frequency, and the overall digestive environment. While this research is still early, it may explain why some people develop diarrhea that persists beyond the typical 8 to 12 week adjustment window, and why probiotics have shown anecdotal benefit in managing GLP-1-related GI symptoms.
Diarrhea versus other retatrutide GI side effects
Diarrhea does not exist in isolation. Most people who experience it also deal with other gastrointestinal symptoms, and understanding the full picture helps you develop a comprehensive management strategy rather than treating each symptom individually.
The full GI side effect spectrum
Based on the meta-analysis data, here is how the major GI side effects compare across dose levels. Nausea is the most common, with relative risk ratios of 2.69 at 4 mg, 4.27 at 8 mg, and 4.00 at 12 mg compared to placebo. These rates are comparable to other GLP-1 agonist side effects but amplified by the triple mechanism.
Vomiting shows the steepest dose-response curve, with relative risks of 4.62 at 4 mg, 8.13 at 8 mg, and 8.98 at 12 mg. Constipation, interestingly, shows relatively flat rates across doses, with relative risks around 4.17 to 4.41 regardless of dose level. This suggests constipation is triggered by the baseline GLP-1 effect on gastric emptying rather than scaling with dose intensity.
And then there is diarrhea, with its unusual non-linear pattern: 1.64 at 4 mg, 2.51 at 8 mg, and 2.04 at 12 mg. The fact that diarrhea peaks at the middle dose and partially resolves at the highest dose tells us that adaptation is happening. Your body does adjust.
When diarrhea and constipation alternate
Some retatrutide users report alternating between diarrhea and constipation, sometimes within the same week. This is not unusual and reflects the complex interplay of slowed gastric emptying (which promotes constipation) and altered intestinal motility (which can trigger diarrhea). If you are experiencing this pattern, it is actually a sign that your gut is actively adapting to the medication. The alternation typically resolves as your system finds a new equilibrium, usually within the first 8 to 12 weeks of stable dosing.
Managing this alternating pattern requires a balanced approach. The strategies that help constipation from tirzepatide and constipation from semaglutide can make diarrhea worse if applied at the wrong time, and vice versa. The key is responding to your current symptom rather than trying to prevent both simultaneously.
Bloating and its relationship to diarrhea
Bloating frequently accompanies or precedes diarrhea episodes during retatrutide use. When gastric emptying slows, food ferments longer in the stomach and upper intestines, producing gas. This distension can trigger accelerated lower intestinal transit as your gut tries to make room, resulting in loose stools. If your diarrhea episodes are consistently preceded by significant bloating, the root cause is likely the delayed gastric emptying rather than a direct intestinal irritation. This distinction matters because the management approach differs. Understanding how bloating works with GLP-1 agonists can help you anticipate and prevent the diarrhea that follows it.
The timeline: when does retatrutide diarrhea start, peak, and resolve
Knowing what to expect week by week transforms a miserable experience into a manageable one. Here is what the clinical data tells us about the typical timeline.
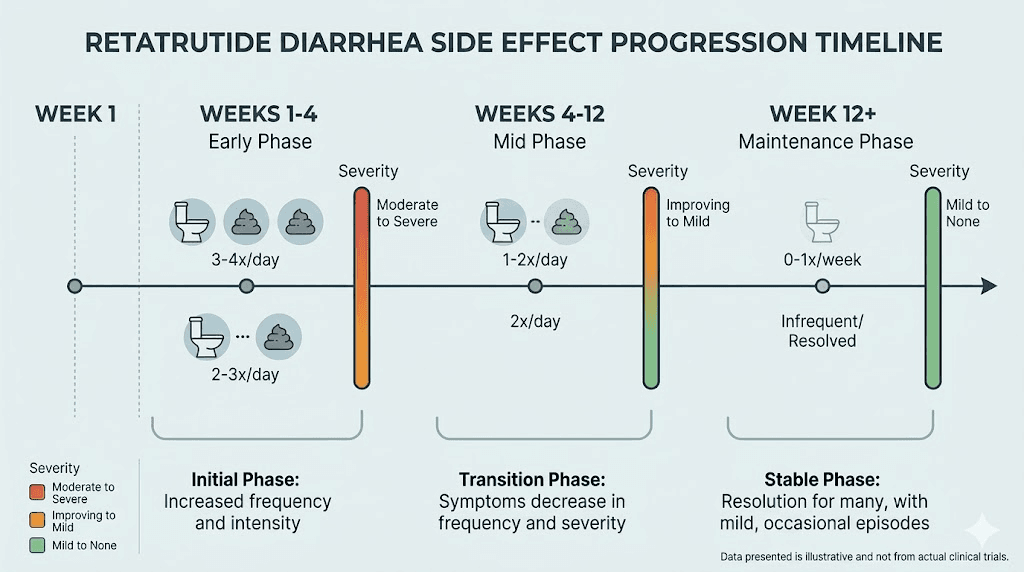
Week 1 to 4: the initiation phase
This is when most GI side effects first appear. If you are following a standard retatrutide dose schedule that starts at a low dose, you may experience mild digestive changes within the first few days. These often include softer stools rather than outright diarrhea, increased bowel frequency, and occasional urgency. Some people notice nothing at all during this initial phase, particularly those who start at the lowest recommended dose.
The severity during weeks 1 to 4 depends heavily on your starting dose. Clinical trial data clearly shows that participants starting at 2 mg experienced significantly fewer GI symptoms than those starting at 4 mg. If you have the option to begin at the lowest available dose, the data strongly supports doing so.
Week 4 to 8: the escalation peak
This is typically the worst period. Each dose increase during the titration phase can trigger a fresh round of GI symptoms, and diarrhea tends to peak during these escalation steps. The body needs approximately 2 to 3 weeks to adapt to each new dose level, so if you are increasing every 4 weeks (as most protocols recommend), you may feel like the symptoms are constant during this phase.
It is not constant. It is a repeating pattern of flare and partial resolution with each escalation step. Recognizing this pattern is crucial for maintaining adherence, because the temptation to quit is highest during this phase. You think it will never end. It does.
Week 8 to 12: the adaptation window
Clinical trials consistently show that most GI symptoms, including diarrhea, diminish significantly after 8 to 12 weeks, particularly in participants who followed gradual dose-escalation schedules. This is the light at the end of the tunnel. Your gut is adapting to the altered motility patterns, your microbiome is adjusting, and the compensatory mechanisms that initially caused diarrhea are finding a new baseline.
By week 12, most participants in the TRIUMPH-4 trial who initially reported diarrhea had either fully resolved or experienced only mild, infrequent episodes. This is also typically when the appetite suppression from retatrutide becomes most noticeable, so the timing works in your favor. The worst of the side effects fade just as the best of the benefits arrive.
Week 12 and beyond: maintenance phase
Once you reach your maintenance dose and have been stable for several weeks, diarrhea becomes much less common. It may still occur occasionally, particularly after dietary indiscretions (high-fat meals, excessive alcohol, or unusually large portions), but the chronic, frequent pattern of the escalation phase is typically over. Some people continue to have slightly looser stools than their pre-retatrutide baseline, which is a minor adaptation most find acceptable given the weight loss benefits.
Dose titration: your most powerful tool against diarrhea
If there is one takeaway from every clinical trial, every meta-analysis, and every researcher who has studied retatrutide GI side effects, it is this: gradual dose titration is the single most effective strategy for minimizing diarrhea. Participants who skipped titration steps experienced nearly double the GI symptom rates. Nearly double. That is not a subtle difference.
The standard titration approach
The clinical trials used specific escalation protocols designed to minimize GI disturbance while still reaching therapeutic dose levels. The general approach involves starting at the lowest dose, maintaining that dose for 4 weeks to allow adaptation, then increasing by one step. Each step gets its own 4-week adaptation window before the next increase. This slow, methodical approach is why the retatrutide dosage chart exists as a critical reference tool, not just a suggestion.
For a typical protocol targeting 8 mg or 12 mg maintenance, the escalation might look something like this. Weeks 1 through 4 at 2 mg. Weeks 5 through 8 at 4 mg. Weeks 9 through 12 at 8 mg. And for those targeting 12 mg, weeks 13 through 16 at 12 mg. Each step gives your digestive system time to adjust before the next challenge arrives. Use the retatrutide dosage calculator to determine your exact protocol based on your weight and goals.
When to slow down the titration
The trial protocols were designed for average responses. You are not average. You are an individual with a unique gut microbiome, unique dietary patterns, and unique sensitivity to GLP-1 receptor activation. If you are experiencing severe or persistent diarrhea at a given dose level, extending that dose period from 4 weeks to 6 or even 8 weeks before escalating is a legitimate strategy. The goal is reaching your target maintenance dose eventually, not reaching it on a rigid timeline.
Some signs that you should extend your current dose period before escalating include diarrhea that occurs more than 3 times daily, diarrhea that has not improved after 3 weeks at the current dose, significant dehydration symptoms (dark urine, dizziness, dry mouth), or diarrhea that is interfering with daily activities or work.
These signals suggest your gut has not yet adapted to the current dose level, and adding more stimulation will only make things worse.
Microdosing as a GI management strategy
Some researchers use an even more gradual approach, essentially micro-titrating by splitting doses or starting below the standard initial dose. While retatrutide microdosing has not been formally studied for GI mitigation specifically, the principle is sound based on the dose-response data from clinical trials. Lower doses produce fewer GI symptoms. Starting even lower and escalating even more gradually should theoretically produce even fewer symptoms, at the cost of a longer time to reach therapeutic levels.
Dietary strategies that actually work for retatrutide diarrhea
Diet is your second most powerful tool after titration. What you eat, when you eat it, and how much you eat at once all directly influence whether that dose of retatrutide triggers a diarrhea episode or passes without incident.
The BRAT protocol for acute episodes
When diarrhea hits, the BRAT diet remains the gold standard first response. Bananas, rice, applesauce, and toast. These foods are bland, low in fiber, low in fat, and gentle on an irritated digestive system. They help solidify stool by absorbing excess water in the intestines. They provide calories and basic nutrition without triggering additional GI stimulation.
But do not stay on BRAT for more than 48 to 72 hours. It is a temporary intervention, not a long-term dietary plan. Extended BRAT eating can actually worsen nutritional status and delay gut adaptation. Use it to get through acute episodes, then transition back to a more balanced eating pattern as symptoms subside.
Meal size and frequency
This is where most people go wrong. They eat their normal-sized meals and wonder why their gut rebels. Retatrutide has slowed your gastric emptying dramatically. That large meal is sitting in your stomach much longer than usual, fermenting, producing gas, and eventually hitting your intestines in a wave that your altered motility cannot handle smoothly.
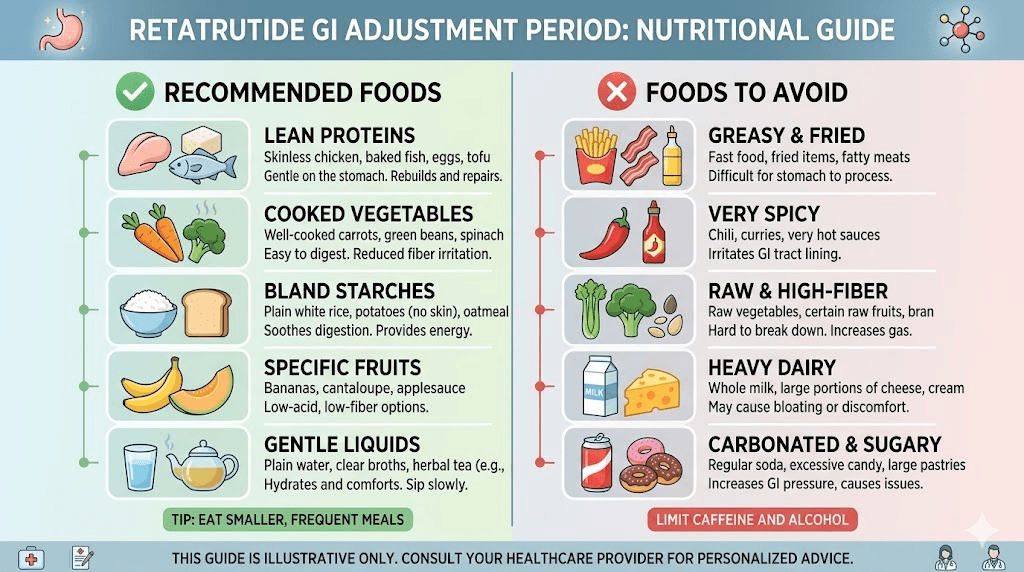
Smaller, more frequent meals. Five to six small meals instead of three large ones. This is not just generic advice. It is mechanistically targeted at the exact problem retatrutide creates. Smaller meals mean less volume for your slowed stomach to process at once, less fermentation, less gas, and a more gradual delivery of nutrients to the intestines. Your gut can handle a steady trickle. It cannot handle a flood. The same principle applies to eating on tirzepatide and eating on semaglutide, but it is even more critical with retatrutide because of the stronger combined receptor activation.
Foods to avoid during the titration phase
Certain foods are almost guaranteed to trigger or worsen diarrhea during the early weeks of retatrutide use. High-fat foods top the list. Fat takes the longest to digest, and when gastric emptying is already slowed, high-fat meals create a perfect storm of delayed processing and eventual intestinal flooding. Fried foods, creamy sauces, fatty cuts of meat, and full-fat dairy products should be minimized during dose escalation periods.
Greasy or oily foods are a particularly common trigger. The altered bile acid metabolism from glucagon receptor activation makes fat digestion less efficient, and undigested fats reaching the lower intestines cause osmotic diarrhea. This is a specific and somewhat unique aspect of retatrutide compared to foods to avoid on tirzepatide or foods to avoid on semaglutide, where the bile acid component is less significant.
Highly processed foods, excessive sugar, sugar alcohols (sorbitol, mannitol, xylitol), and large amounts of caffeine can all worsen diarrhea. Spicy foods are another common trigger during the sensitive escalation period. Alcohol deserves special mention because it acts as a GI irritant independent of retatrutide and can dramatically worsen diarrhea episodes when combined with the altered gut motility. If you must drink, understanding alcohol interactions with GLP-1 agonists is essential.
Foods that help manage diarrhea
On the positive side, certain foods actively help manage retatrutide-related diarrhea. Soft proteins like eggs, poultry, and white fish are easy to digest and provide essential amino acids without triggering GI distress. Soups and broths serve double duty by providing nutrition and hydration simultaneously. Plain yogurt with live cultures may help by supporting beneficial gut bacteria during the microbiome disruption that GLP-1 agonists can cause.
Rice, oatmeal, and plain potatoes provide starchy, binding carbohydrates that help solidify stool. Cooked vegetables (not raw) are easier to digest and less likely to trigger symptoms. Low-fat meals in general are your friend during the titration phase. Building your breakfast and dinner around these principles during dose escalation can make a significant difference in daily comfort.
The fiber balance
Fiber is tricky during retatrutide use. Too much insoluble fiber can worsen diarrhea by speeding intestinal transit. Too little fiber can worsen constipation on the days when your gut swings in that direction. The approach that works best for most people is focusing on soluble fiber sources (oats, bananas, apples without skin, white rice) while minimizing insoluble fiber sources (bran, raw vegetables, whole grains with intact husks) during acute diarrhea episodes.
Once your GI symptoms stabilize, you can gradually reintroduce more fiber. But during the active titration phase, keep fiber intake moderate and emphasize soluble over insoluble. This approach is consistent with what works for managing semaglutide diet protocols and tirzepatide diet plans as well.
Hydration and electrolyte management
Diarrhea causes dehydration. This is not a maybe. Every episode of diarrhea pulls water and electrolytes from your body, and if you are not actively replacing them, you will compound the problem with symptoms that mimic or worsen the diarrhea itself. Dehydration causes dizziness, fatigue, headaches, muscle cramps, and ironically, further GI disruption.
Water alone is not enough
This is the most common mistake. People experience diarrhea and drink more water. Good instinct, incomplete solution. When you lose fluids through diarrhea, you also lose essential electrolytes including sodium, potassium, chloride, and magnesium. Drinking plain water replaces volume but not the minerals your cells need to function properly. In fact, drinking large amounts of plain water without electrolytes can actually dilute your remaining mineral levels, making things worse.
Oral rehydration strategy
The most effective approach combines water with electrolyte replacement. Oral rehydration solutions (ORS) are specifically formulated to match the ratio of sodium, potassium, and glucose that optimizes intestinal water absorption. Commercial electrolyte drinks, electrolyte tablets or powders added to water, or even homemade solutions (a pinch of salt and a small amount of sugar in water) all work. The key is consistency. Do not wait until you feel dehydrated. Start replacing electrolytes at the first sign of loose stools.
Aim for at least 8 to 10 glasses of fluid daily during episodes, with at least half coming from electrolyte-containing sources. Coconut water is a natural option that provides potassium and some sodium. Bone broth provides sodium, potassium, and amino acids. Avoid excessive caffeine and alcohol, both of which are diuretics that accelerate fluid loss. The supplement strategies that work with tirzepatide apply equally well to retatrutide, with electrolytes being perhaps the most critical addition.
Signs of dehydration to watch for
Know these warning signs. Dark yellow or amber urine means you are already significantly behind on hydration. Decreased urination frequency is another early sign. Dry mouth, dry skin, sunken eyes, rapid heartbeat, and lightheadedness when standing are all signs that dehydration is progressing. Dizziness during GLP-1 agonist use is frequently a dehydration symptom rather than a direct drug effect, and correcting hydration often resolves it.
If you experience severe diarrhea (more than 6 episodes in 24 hours), bloody stools, inability to keep fluids down, or signs of severe dehydration, seek medical attention. These are not normal titration effects and may require medical intervention beyond self-management.
Over-the-counter and supplemental interventions
Beyond diet and hydration, several readily available interventions can help manage retatrutide diarrhea. These should complement, not replace, the dietary and titration strategies discussed above.
Probiotics
Given the emerging evidence that GLP-1 agonists alter gut microbiome composition, probiotics represent a logical intervention. While there are no randomized trials specifically testing probiotics for retatrutide-related diarrhea, the mechanistic rationale is strong. Multi-strain probiotics containing Lactobacillus and Bifidobacterium species have the most evidence for managing antibiotic-associated and medication-related diarrhea in general. Starting a probiotic before or simultaneously with retatrutide initiation may help maintain microbiome stability during the adjustment period. Probiotic recommendations for GLP-1 agonist users apply well here, though the glucagon receptor component of retatrutide may create somewhat different microbiome changes than pure GLP-1 agonists.
Digestive enzymes
Because retatrutide alters gastric emptying and potentially bile acid metabolism, supplemental digestive enzymes may help some people process meals more completely before food reaches the lower intestines. Lipase supplementation in particular may help with fat digestion, reducing the undigested fat that can cause osmotic diarrhea. Enzyme supplements are generally safe and well-tolerated, though they should be taken with meals rather than on an empty stomach.
Loperamide for severe episodes
Loperamide (the active ingredient in Imodium) slows intestinal motility and reduces stool frequency. It can be an effective rescue medication for severe diarrhea episodes, but it should not be used routinely during retatrutide treatment. Regular loperamide use can mask the natural adaptation process and may cause rebound constipation when stopped. Reserve it for situations where diarrhea is interfering with important activities or causing significant dehydration despite other management strategies.
Bismuth subsalicylate
Pepto-Bismol and similar bismuth subsalicylate products can help by coating the intestinal lining, reducing inflammation, and killing some bacteria that may contribute to diarrhea. They are generally safe for short-term use but can interact with certain medications and should not be used for extended periods. The characteristic black stool they produce is harmless but can be alarming if unexpected.
Ginger
Ginger has well-documented antiemetic (anti-nausea) properties and may also help with diarrhea through its anti-inflammatory effects on the GI tract. Ginger tea, ginger supplements, or fresh ginger added to meals can provide mild but genuine relief for overall GI discomfort during retatrutide use. It is a gentle intervention with minimal risk of side effects.
Retatrutide diarrhea compared to tirzepatide and semaglutide
If you are switching to retatrutide from another GLP-1 agonist, or choosing between them, understanding the comparative GI profiles helps set accurate expectations.
Semaglutide GI profile
Semaglutide versus retatrutide is a common comparison. Semaglutide, as a pure GLP-1 agonist, causes GI side effects primarily through delayed gastric emptying. Diarrhea rates in semaglutide trials typically range from 8% to 15% across dose levels, significantly lower than the 9% to 35% seen with retatrutide. However, semaglutide also produces less weight loss than retatrutide, so the higher GI burden comes with proportionally greater efficacy. Semaglutide withdrawal patterns also differ from what you might expect with retatrutide discontinuation.
Tirzepatide GI profile
Tirzepatide as a dual GLP-1/GIP agonist produces GI side effects somewhere between semaglutide and retatrutide in both rate and severity. The GIP receptor activation in tirzepatide may actually moderate some GLP-1-related GI effects, and many users report that tirzepatide is slightly better tolerated gastrointestinally than semaglutide despite being more effective. Retatrutide adds the glucagon receptor on top of this, which appears to increase GI side effect rates above tirzepatide levels. Those who have experienced tirzepatide diarrhea should expect a potentially more intense but similar duration pattern with retatrutide.
The trade-off calculation
Retatrutide produced up to 17.5% mean weight reduction at just 24 weeks in Phase 2, with some participants achieving over 24% body weight loss. That efficacy level exceeds both semaglutide and tirzepatide. The higher GI side effect rates are essentially the price of more powerful weight loss. For many people, 8 to 12 weeks of manageable diarrhea is an acceptable trade-off for significantly better outcomes. For others, a gentler approach with semaglutide or tirzepatide makes more sense. Understanding how these options compare overall helps inform that decision.
Switching from tirzepatide or semaglutide to retatrutide
If you are switching from tirzepatide to retatrutide, you have an advantage. Your GLP-1 and GIP receptors are already adapted to agonist stimulation, which means the GI adjustment to retatrutide may be less severe than starting from scratch. However, the glucagon receptor component is entirely new to your system, so some fresh GI adaptation should be expected. The dosage schedule when switching after high-dose tirzepatide accounts for this partial adaptation and can help minimize the transition diarrhea.
Injection timing and technique considerations
While the connection between injection practices and diarrhea might not be immediately obvious, how and when you inject retatrutide can influence GI tolerance.
Best time of day to inject
Many retatrutide users find that injection timing affects when GI symptoms peak. Injecting in the morning means that peak drug activity, and therefore peak GI effects, occurs during the daytime when you are active and can manage symptoms more easily. Injecting in the evening means peak effects may occur during sleep, which some people prefer because they sleep through the worst of the nausea, though nighttime diarrhea episodes can obviously disrupt sleep. The best time to take retatrutide often comes down to personal preference and symptom patterns, but starting with morning injections and adjusting based on your experience is a reasonable approach.
Injection site and technique
Proper injection technique ensures consistent drug absorption, which helps maintain stable blood levels and reduces the likelihood of absorption spikes that can trigger GI symptoms. Following proper injection site guidelines and injection technique is more than just a safety measure. Inconsistent absorption from poor technique can create mini-spikes in drug levels that provoke GI reactions. Rotate injection sites regularly, inject subcutaneously (not intramuscularly), and ensure proper reconstitution for consistent dosing accuracy.
Splitting doses
Some researchers experiment with splitting their weekly dose into two smaller injections given 3 to 4 days apart. The theory is that two smaller peaks are gentler on the digestive system than one large peak. While this has not been formally studied with retatrutide, the principle is supported by the dose-response data showing that lower individual doses produce proportionally fewer GI symptoms. If you are struggling with severe post-injection diarrhea, discussing dose splitting with a healthcare provider may be worthwhile. The concept is similar to splitting semaglutide doses, which some users have found helpful for GI management.
When to be concerned: red flags versus normal adjustment
Most retatrutide diarrhea is an annoyance, not a danger. But you need to know the difference between normal titration effects and signs that something more serious is happening.
Normal adjustment symptoms
These are expected and typically manageable: loose stools 1 to 3 times daily during dose escalation, mild abdominal cramping before bowel movements, increased urgency (needing to go sooner than usual), softer stool consistency without other alarming features, symptoms that correlate with recent dose increases, and gradual improvement over 2 to 4 weeks at a stable dose. These symptoms, while uncomfortable, are part of the normal adaptation process and are consistent with the clinical trial experience.
Warning signs that require medical attention
Seek medical evaluation if you experience any of the following. More than 6 watery stools in 24 hours. Blood or mucus in the stool. Severe abdominal pain (not just cramping). Fever accompanying diarrhea. Signs of significant dehydration despite oral rehydration efforts. Diarrhea that has not improved after 4 weeks at a stable dose. Dramatic, sudden worsening of symptoms without a dose change. Inability to keep any food or fluids down.
These signs may indicate something beyond normal drug adjustment, including infection, underlying gut conditions, or a severe medication reaction that needs professional management. Do not try to manage these at home with the strategies in this guide. They require proper medical evaluation.
Pancreatitis awareness
GLP-1 receptor agonists carry a theoretical risk of pancreatitis, though this has been rare in retatrutide trials specifically. Pancreatitis symptoms can include severe upper abdominal pain that radiates to the back, nausea and vomiting, and yes, diarrhea. If your diarrhea is accompanied by severe pain that is different in character from typical GI cramping, particularly pain that radiates to your back or worsens after eating, seek emergency medical attention. This is unlikely but important to know.
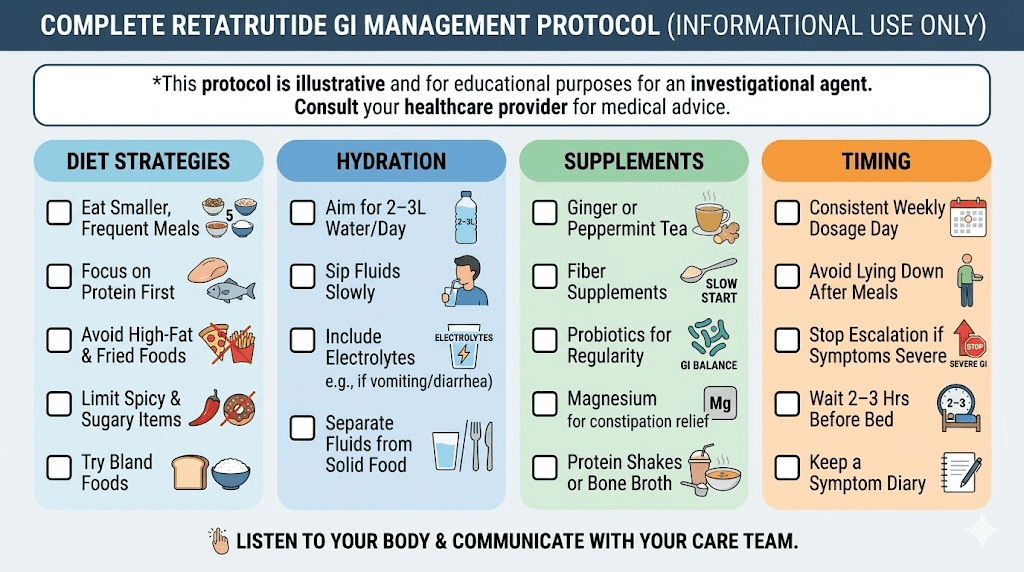
Building a complete GI management protocol
Rather than applying individual strategies randomly, build a systematic approach that addresses retatrutide diarrhea from multiple angles simultaneously.
Protocol 1: prevention-focused (start this before your first dose)
Goal: Minimize GI disruption from day one.
Two weeks before starting retatrutide: Begin a daily probiotic. Shift your diet toward smaller, more frequent meals. Reduce high-fat food intake. Start tracking your baseline bowel habits so you can identify changes early. Stock up on electrolyte solutions, ginger tea, and BRAT diet staples.
During titration: Take your probiotic daily with food. Eat 5 to 6 small meals instead of 3 large ones. Emphasize soft proteins, cooked vegetables, and low-fat preparations. Drink electrolyte fluids proactively, not just when symptomatic. Avoid trigger foods (high fat, greasy, spicy, excessive sugar). Consider digestive enzymes with meals if fat digestion seems problematic. Monitor hydration via urine color.
At each dose increase: Expect 1 to 2 weeks of increased GI sensitivity. Tighten your diet during this adjustment window. Increase electrolyte intake preemptively. If the previous dose caused significant issues, consider extending the current dose period before escalating.
Protocol 2: acute management (when diarrhea hits hard)
Goal: Rapid symptom control and dehydration prevention.
First 24 hours: Switch to BRAT diet. Begin oral rehydration solution immediately. Sip fluids constantly, not in large amounts. Consider loperamide if symptoms are severe and interfering with daily function. Avoid caffeine, alcohol, dairy, and high-fiber foods.
Days 2 to 3: Continue BRAT with gradual additions (plain chicken, white rice, cooked carrots). Maintain electrolyte replacement. Monitor urine color and frequency. If improving, slowly reintroduce your normal GLP-1 friendly diet.
Days 4 to 7: Resume normal eating patterns (small, frequent, low-fat). Continue probiotics and electrolytes. If not improving, contact your healthcare provider about potential dose adjustment or extended hold at current level.
Protocol 3: long-term maintenance (for persistent mild symptoms)
Goal: Comfortable long-term adherence with minimal GI disruption.
Daily habits: Maintain consistent meal timing and size. Take a daily probiotic. Include soluble fiber sources in each meal. Drink at least 2 liters of fluid daily, including some electrolyte sources. Avoid known personal trigger foods. Time high-fat meals strategically (not immediately after injection day). Exercise regularly, as physical activity promotes healthy gut motility.
Weekly check-ins: Monitor stool frequency and consistency. Track any foods that seem to trigger episodes. Assess hydration status. Note any new or worsening symptoms. Compare to the previous week to identify trends. If you are tracking your progress alongside your weight loss protocol, noting GI patterns can help optimize both outcomes.
The psychological component
Let us talk about something the clinical trials do not measure. The psychological burden of dealing with chronic diarrhea during retatrutide use.
Anxiety and anticipatory symptoms
Once you have had a few urgent diarrhea episodes, your brain starts anticipating them. You worry about being away from a bathroom. You stress about meals out with friends. You plan your day around bathroom access. This anxiety is completely normal and understandable, but it can also worsen the problem. The gut-brain connection is real and well-documented. Anxiety and stress activate the sympathetic nervous system, which can accelerate intestinal transit and actually cause the diarrhea you are afraid of having. Similar psychological patterns emerge with other GLP-1 agonist anxiety symptoms.
Strategies for managing the psychological burden
Know your timeline. Remind yourself that this is temporary. The 8 to 12 week adaptation window is not forever. Having a clear endpoint in mind makes the daily discomfort more bearable.
Prepare practically. Carry emergency supplies (wet wipes, change of underwear, loperamide) during the worst phase. This reduces anxiety about being caught unprepared. Plan activities around bathroom access during the first few weeks of each dose increase.
Reframe the experience. GI symptoms are actually a sign that the medication is working. The same mechanisms causing diarrhea are also driving weight loss. You are not suffering for nothing.
Connect with others. Online communities of people using GLP-1 agonists can provide reassurance and practical tips from people who have been through exactly what you are experiencing. Knowing that others survived the same phase and came out the other side is genuinely helpful.
Special populations and considerations
Not everyone experiences retatrutide diarrhea the same way. Certain factors can increase or decrease your risk and may require modified management approaches.
People with pre-existing IBS
If you have irritable bowel syndrome, particularly the diarrhea-predominant subtype (IBS-D), retatrutide can exacerbate your existing condition significantly. The altered motility patterns that retatrutide creates overlap with the motility dysfunction that defines IBS, and the combination can be challenging. Extra-gradual titration, proactive dietary management, and close communication with a gastroenterologist are essential for this population. You may also benefit from continuing any IBS-specific treatments (antispasmodics, low-FODMAP diet) alongside your retatrutide protocol.
People switching from other GLP-1 agonists
As mentioned earlier, if you are coming from tirzepatide or semaglutide, your GLP-1 receptors are already partially adapted. Your diarrhea risk with retatrutide may be lower than someone starting fresh, but the glucagon receptor activation is new territory for your gut. Expect some GI adjustment but potentially less severe than a completely naive start. The transition timeline from tirzepatide can help you plan for this adjustment period.
People on other medications
Certain medications can compound diarrhea risk. Metformin, a common diabetes medication, is notorious for causing GI side effects including diarrhea, and combining it with retatrutide can amplify digestive issues. Other medications that may worsen the situation include magnesium supplements (especially magnesium citrate), certain antibiotics, proton pump inhibitors, and some blood pressure medications. If you are on multiple medications, discuss potential GI interactions with your prescriber before starting retatrutide.
People with malabsorption concerns
Persistent diarrhea can raise concerns about nutrient malabsorption. If you are on retatrutide and experiencing chronic loose stools, monitor for signs of deficiency including fatigue, hair changes, brittle nails, muscle weakness, and difficulty concentrating. Some of these symptoms overlap with GLP-1 fatigue and semaglutide fatigue, making it important to distinguish between drug side effects and genuine nutritional deficiency. Blood work checking vitamin B12, vitamin D, iron, magnesium, and electrolyte levels can help identify any absorption issues that need targeted supplementation.
Frequently asked questions
How long does retatrutide diarrhea last?
Most retatrutide-related diarrhea improves significantly within 8 to 12 weeks of stable dosing, based on clinical trial data. The worst episodes typically occur during dose escalation phases and resolve 2 to 3 weeks after reaching a stable dose. Following proper titration schedules can shorten this adjustment period.
Is diarrhea from retatrutide worse than from semaglutide or tirzepatide?
Yes, diarrhea rates are higher with retatrutide (9-35% depending on dose and study) compared to semaglutide (8-15%) and tirzepatide (moderate rates between the two). The triple receptor mechanism of retatrutide, particularly the glucagon receptor component, contributes to higher GI side effect rates overall.
Can I take Imodium while on retatrutide?
Loperamide (Imodium) can be used as a rescue medication for severe diarrhea episodes, but it should not be taken routinely. Regular use can mask the natural adaptation process and may cause rebound constipation. Use it only when diarrhea is significantly interfering with daily activities or causing dehydration.
Does the diarrhea mean retatrutide is working?
GI side effects indicate that the drug is activating the receptors that drive weight loss. However, the absence of diarrhea does not mean the drug is not working. People respond differently, and some achieve excellent weight loss results without significant GI symptoms. The clinical data shows that efficacy and GI tolerance are not perfectly correlated.
Should I stop retatrutide if the diarrhea is severe?
Do not stop without consulting your healthcare provider. Severe diarrhea (more than 6 episodes daily, blood in stool, inability to stay hydrated) warrants medical evaluation, but the solution may be a dose reduction or extended hold at the current dose rather than complete discontinuation. In clinical trials, most participants who experienced even moderate GI symptoms were able to continue with appropriate management.
Will probiotics help with retatrutide diarrhea?
Probiotics may help by supporting gut microbiome stability during the adjustment period. While there are no retatrutide-specific probiotic studies, the mechanistic rationale is sound, and multi-strain formulations containing Lactobacillus and Bifidobacterium species have the most general evidence for medication-related diarrhea. Starting a probiotic before initiating treatment is a reasonable strategy.
Does what I eat really affect retatrutide diarrhea?
Diet has a massive impact. High-fat meals, greasy foods, excessive sugar, and large portions all significantly worsen retatrutide-related diarrhea. Switching to smaller, more frequent meals with low-fat proteins and cooked vegetables can reduce episode frequency substantially. The altered bile acid metabolism from glucagon receptor activation makes fat tolerance particularly important with retatrutide compared to other GLP-1 agonists.
Can I exercise with retatrutide diarrhea?
Light to moderate exercise is generally fine and may actually help regulate gut motility. However, high-intensity exercise can worsen diarrhea by redirecting blood flow away from the digestive system. During acute episodes, stick to walking or gentle movement. As symptoms stabilize, gradually return to your normal exercise routine while ensuring adequate hydration with protein and electrolyte supplementation.
External resources
PubMed Central - Retatrutide Systematic Review and Meta-Analysis
PubMed Central - Managing GI Side Effects of GLP-1 Receptor Agonists
PubMed Central - GI Adverse Effects of Anti-Obesity Medications Systematic Review
For researchers serious about managing their retatrutide protocols effectively, SeekPeptides offers the most comprehensive resource available, with evidence-based dosing guides, dosage calculators, side effect management protocols, and a community of thousands who have navigated these exact challenges. SeekPeptides members get access to detailed retatrutide protocols, weight loss dosing charts, and expert guidance for optimizing results while minimizing side effects like the diarrhea covered in this guide.
In case I do not see you, good afternoon, good evening, and good night. May your titration stay gradual, your hydration stay consistent, and your gut stay cooperative.