Mar 1, 2026

Some people feel it within days. A quiet shift. Food just stops calling to them the way it used to. Others spend three weeks on retatrutide wondering if they received a placebo, feeling every bit as hungry as before, still thinking about lunch before breakfast is finished. The difference between these two experiences is not random. It is not luck. And it is not because one person responds to peptides better than another.
It comes down to dose, timing, individual biology, and something most guides never bother explaining: how a triple receptor agonist actually reshapes appetite signaling across three separate hormonal pathways simultaneously. That process does not happen overnight. But when it does happen, the effect is unlike anything semaglutide or tirzepatide can produce alone.
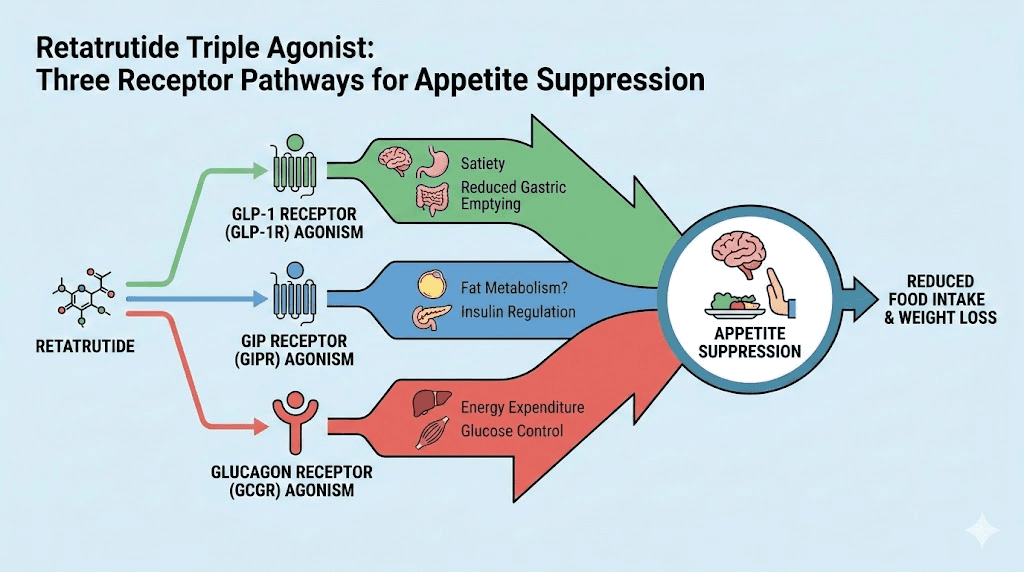
Retatrutide does not just reduce hunger. It recalibrates the entire relationship between your brain, your gut, and your fat tissue. It targets GLP-1 receptors, GIP receptors, and glucagon receptors all at once, creating a cascade of metabolic changes that affect appetite from multiple angles. Understanding the timeline of those changes, what happens in week one versus week eight versus week twenty-four, is the difference between realistic expectations and premature frustration.
This guide breaks down exactly when retatrutide suppresses appetite based on clinical trial data, phase 2 study findings on eating behavior, and the mechanisms that drive appetite reduction at each dose level. Whether you are considering retatrutide, already on it and wondering why results have not appeared yet, or switching from another GLP-1 medication, the answer to your question lives in the details that follow.
What retatrutide actually does to your appetite
Before you can understand the timeline, you need to understand the mechanism. And the mechanism behind retatrutide is fundamentally different from every other weight loss peptide currently available.
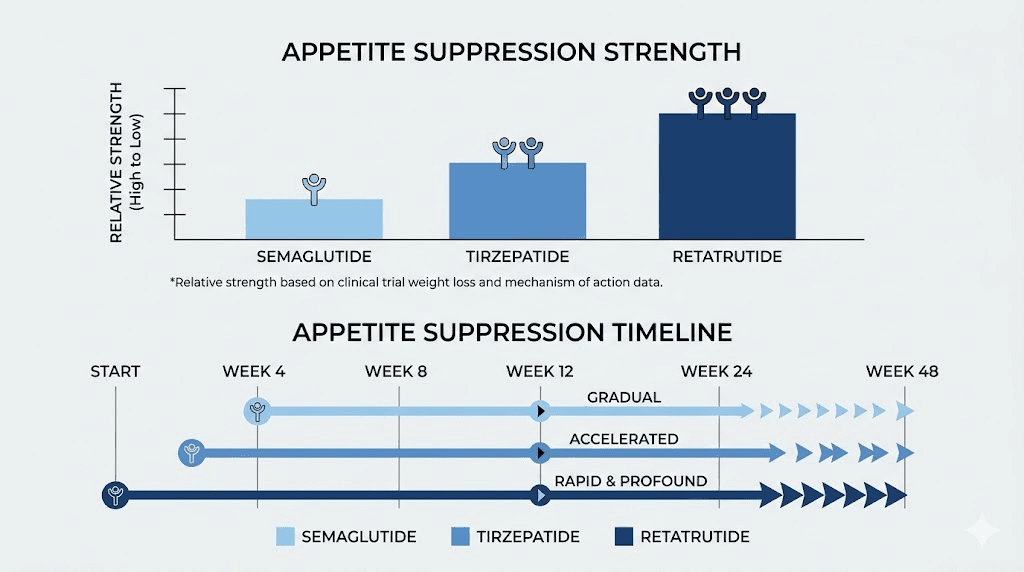
Most GLP-1 medications target one receptor. Semaglutide activates GLP-1 receptors. That is it. One pathway. Tirzepatide goes further, activating both GLP-1 and GIP receptors. Two pathways. Retatrutide activates three: GLP-1, GIP, and glucagon receptors. This triple activation is not just marketing language. It produces qualitatively different appetite suppression through three distinct biological mechanisms working in concert.
The GLP-1 pathway: slowing the gut and signaling satiety
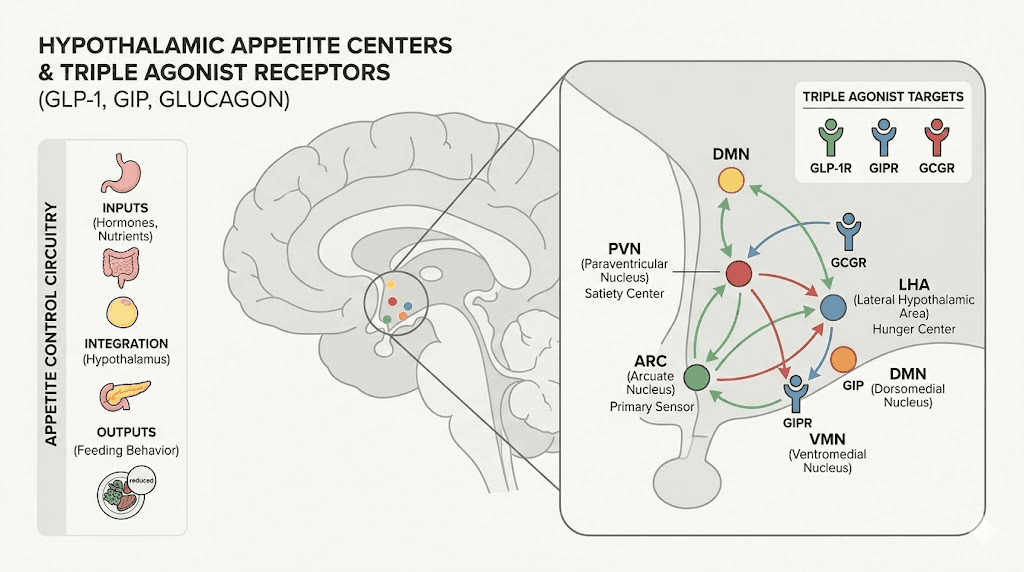
When retatrutide activates GLP-1 receptors, it triggers the same appetite-reducing effects you see with semaglutide. Gastric emptying slows down, meaning food stays in the stomach longer. You feel full faster. You stay full longer. Meanwhile, GLP-1 receptor activation in the hypothalamus, specifically in the arcuate nucleus and paraventricular nucleus, directly suppresses hunger signals by activating satiety-promoting POMC/CART neurons while inhibiting hunger-promoting NPY/AgRP neurons.
This is the pathway most people are familiar with.
But it is only one third of what retatrutide does.
The GIP pathway: enhancing insulin response and reducing cravings
GIP receptor activation reduces appetite through a mechanism that works alongside GLP-1 but through different cellular pathways. GIP slows gastric motility, enhances insulin release from the pancreas, and contributes to satiety signaling in ways that are additive to GLP-1 effects. Research suggests that GIP activation may play a particularly important role in reducing cravings for specific food types, especially high-fat and high-sugar foods.
This dual activation is why tirzepatide outperforms semaglutide for appetite suppression. And retatrutide includes this same dual activation plus something more.
The glucagon pathway: the metabolic accelerator
Here is where retatrutide separates itself from everything else. Glucagon receptor activation does not directly suppress appetite in the way GLP-1 does. Instead, it shifts the metabolic environment in ways that indirectly reduce hunger and dramatically accelerate fat loss.
Glucagon decreases lipogenesis, the creation of new fat. It induces lipolysis, the breakdown of existing fat. It promotes thermogenesis in brown adipose tissue, meaning your body burns more calories as heat. And it reduces gastrointestinal motility, further slowing food transit through the digestive system.
The combined effect of all three pathways creates appetite suppression that is both stronger and more multidimensional than what any single-receptor or dual-receptor agonist can achieve. In animal studies, retatrutide produced the largest decreases in food intake compared to semaglutide, tirzepatide, and liraglutide individually.
The week-by-week appetite suppression timeline
Now for the question you came here to answer. When does it actually work?
The short answer: most people notice meaningful appetite changes between weeks 2 and 8. But the full picture is more nuanced than that, and the specific timeline depends heavily on your dose, your titration schedule, and your individual biology.
Weeks 1 to 2: the adjustment period
During the first one to two weeks on retatrutide, you are typically on the starting dose of 2mg per week. At this dose, the primary goal is allowing your body to adjust to the medication, not producing dramatic appetite changes.
Some people notice subtle shifts during this period. Portions might feel slightly more satisfying. The urge to snack between meals might decrease modestly. But these changes are often mild enough to question whether they are real or just expectation bias.
What you will likely notice more during weeks 1-2 are side effects. Mild nausea is common. Fatigue can occur. Some people experience headaches. These symptoms indicate that the medication is active in your system, even if appetite changes have not become obvious yet.
Do not mistake the absence of dramatic appetite suppression at 2mg for the medication failing.
It is not failing. It is building.
Weeks 3 to 4: the first real shifts
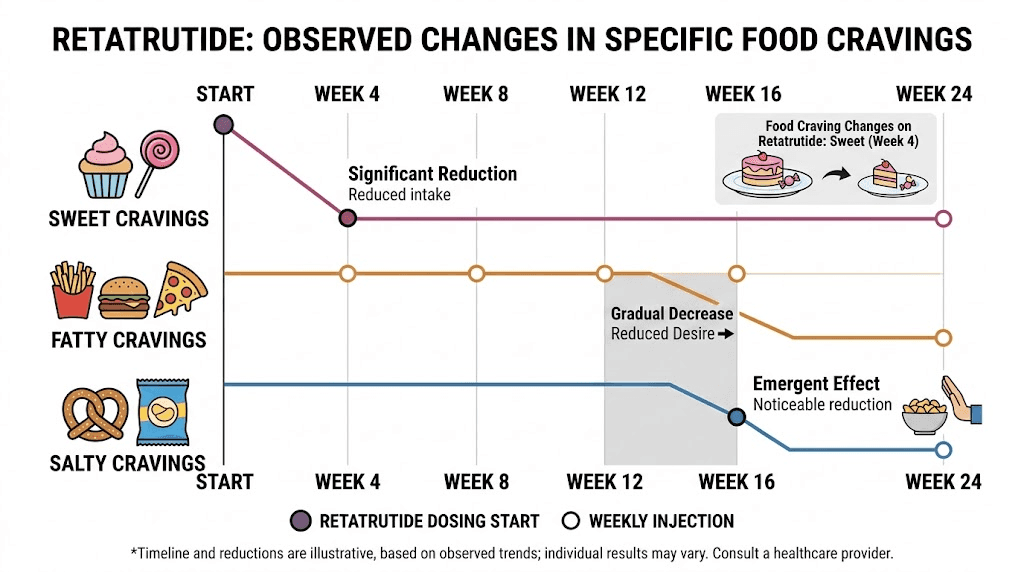
By weeks 3-4, most people are either still on 2mg or have just escalated to 4mg. This is where appetite changes typically become noticeable for the first time. Clinical trial data from the phase 2 study shows that retatrutide at 4mg and above produces statistically significant reductions in desire for sweet foods by week 4, with participants reporting 14 to 19.5 point improvements on appetite visual analog scales compared to placebo.
What this feels like in practice:
You finish a meal and genuinely do not want more
The thought of dessert becomes less compelling
You might forget about a snack you normally would have reached for automatically
Portion sizes naturally decrease without conscious effort
These are not dramatic transformations. They are subtle recalibrations. But they are real, measurable, and consistent across the clinical data.
Weeks 5 to 8: appetite suppression solidifies
This is the period where most people on retatrutide describe a clear before-and-after shift in their relationship with food. By week 5-8, you are typically on 4mg or transitioning to 8mg, and the triple receptor activation has had enough time to produce measurable changes across all three pathways.
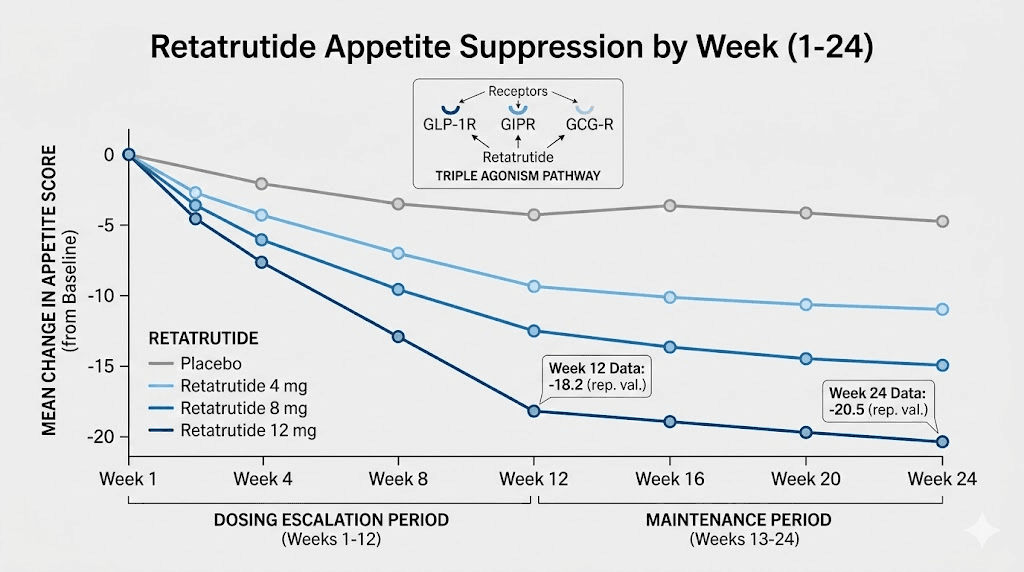
Phase 2 clinical data shows that by week 8, retatrutide at 4mg reduced hunger scores by 10.4 points versus placebo on appetite visual analog scales. At 8mg, the reduction reached 11.4 points by week 12. These are clinically significant reductions that translate to meaningful daily differences in how hungry you feel and how much you eat.
In the eating behavior sub-study, 31 of 36 retatrutide-treated participants reported noticeable changes in eating behaviors within the first 8 weeks. They described eating less frequently, consuming smaller portions, feeling hungry less often, feeling fuller after eating, having different food preferences, and feeling more in control of their eating choices.
That last point matters. Appetite suppression is not just about feeling less hungry. It is about a fundamental shift in how food occupies your mental space. The constant background noise of food thoughts, what researchers call food noise, begins to quiet during this period for most people.
Weeks 9 to 12: dose-dependent acceleration
By weeks 9-12, people on higher doses (8mg or transitioning to 12mg) typically experience the strongest appetite suppression they have felt to date. The dose escalation to maintenance levels means all three receptor pathways are being activated at therapeutic concentrations.
The clinical data supports this acceleration. Retatrutide at 8mg showed hunger reductions of 11.4 points versus placebo at week 12. Desire for salty foods decreased by 16.6 points. Desire for fatty foods decreased by 14.5 points. These are not subtle changes. They represent a genuine shift in how your brain responds to food cues.
During this phase, many people report experiences like:
Genuinely forgetting to eat meals
Looking at foods they once craved and feeling neutral or even slightly repulsed
Feeling physically unable to finish portions they would have easily consumed before
Reduced interest in snacking entirely
Choosing different foods instinctively, gravitating toward protein and away from processed carbohydrates
This is also the period where weight loss begins accelerating noticeably. The combination of reduced caloric intake from appetite suppression, increased energy expenditure from glucagon receptor activation, and improved metabolic efficiency from GIP pathway activation creates a powerful synergy.
Weeks 13 to 24: full therapeutic effect
Once you reach your maintenance dose and have been on it for several weeks, the full appetite-suppressing effects of retatrutide become established. The phase 2 study measured appetite outcomes at week 24 and found that all retatrutide doses of 4mg and above produced approximately 15-16 point reductions in hunger versus placebo.
Perceived hunger at week 24 decreased by 1.4 to 1.5 points on the Eating Inventory scale across the 4mg, 8mg, and 12mg groups. Disinhibition, the tendency to overeat in response to emotional or environmental triggers, also improved significantly at all doses above 0.5mg.
By this point, appetite suppression feels less like a medication effect and more like a new normal. The constant negotiation with food, the willpower battles, the guilt cycles, these largely fade. Not because you are forcing them down, but because the biological drives that created them have been recalibrated.
At the 24-week mark in clinical trials, mean body weight reduction ranged from 7.2% at 1mg to 17.5% at 12mg, compared to 1.6% with placebo. The relationship between appetite suppression and weight loss was statistically significant, with reductions in perceived hunger and disinhibition directly correlated with reductions in body weight.
Weeks 25 to 48: sustained and deepening effects
The appetite suppression does not plateau at week 24. Retatrutide continues producing weight loss beyond the 24-week mark, suggesting that appetite-related effects also continue deepening or at minimum remain stable.
At week 36, the eating behavior data showed even stronger results than at week 24 for higher doses. Perceived hunger reductions at 8mg and 12mg reached 1.9 to 2.4 points versus placebo. Disinhibition improvements reached 2.1 to 2.6 points. Dietary restraint, the ability to consciously control food intake, increased by 3.3 points at 12mg.
By week 48, participants on 12mg had lost an average of 24.2% of their body weight. This represents the highest weight loss achieved by any GLP-1 class medication in clinical trials, and it would not be possible without sustained, powerful appetite suppression throughout the treatment period.
How retatrutide compares to semaglutide and tirzepatide for appetite suppression
Context matters. Understanding how quickly retatrutide suppresses appetite means understanding how it stacks up against the alternatives you may have tried or considered.
Semaglutide: the single-receptor comparison
Semaglutide typically begins suppressing appetite within the first 1-2 weeks for some people, with most users noticing clear effects by weeks 4-8. Peak appetite suppression usually occurs around weeks 12-14. A 12-week trial at 1.0mg showed semaglutide reduced energy intake by approximately 35% versus placebo.
The appetite suppression from semaglutide is real and well-documented. But it operates through only one receptor pathway. The 68-week STEP 1 trial showed 14.9% mean body weight reduction at 2.4mg, compared to retatrutide hitting 17.5% at just 24 weeks with the 12mg dose.
The timeline comparison is illuminating. Where semaglutide might take 12-14 weeks to reach peak appetite suppression, retatrutide achieves clinically significant appetite changes by week 8 at therapeutic doses, and continues deepening those effects well beyond the point where semaglutide typically plateaus.
Tirzepatide: the dual-receptor comparison
Tirzepatide adds GIP receptor activation to GLP-1, creating appetite suppression that is faster and stronger than semaglutide alone. Most tirzepatide users report appetite changes within the first 2-4 weeks, with many describing significant shifts by week 6-8.
In clinical trials, tirzepatide achieved up to 18% weight loss compared to semaglutide at 12%. The SURPASS trials demonstrated greater appetite reduction and more dramatic shifts in food preferences compared to GLP-1-only medications.
Retatrutide builds on everything tirzepatide does and adds the glucagon receptor component. In direct comparison animal studies, retatrutide produced the largest decreases in food intake compared to all other GLP-1 class medications. The human data reflects this advantage, with retatrutide achieving 24.2% weight loss at 48 weeks compared to tirzepatide reaching approximately 21% at 72 weeks in the SURMOUNT trials.
Head-to-head appetite comparison table
Factor | Semaglutide | Tirzepatide | Retatrutide |
|---|---|---|---|
Receptors targeted | GLP-1 only | GLP-1 + GIP | GLP-1 + GIP + Glucagon |
First appetite changes | Weeks 1-2 | Weeks 1-3 | Weeks 2-4 |
Clear appetite suppression | Weeks 4-8 | Weeks 3-6 | Weeks 4-8 |
Peak effect | Weeks 12-14 | Weeks 8-12 | Weeks 12-24+ |
Max weight loss (trials) | 14.9% (68 wks) | 21% (72 wks) | 24.2% (48 wks) |
Appetite depth | Moderate | Strong | Strongest in class |
One pattern worth noting: retatrutide may appear slightly slower to produce initial appetite effects compared to semaglutide. This is likely because retatrutide protocols typically start at 2mg, which has minimal appetite-suppressing activity, and the dose escalation takes time. But once therapeutic doses are reached, the appetite suppression is deeper, more sustained, and covers more dimensions of eating behavior than either single or dual receptor agonists.
Factors that affect how quickly retatrutide suppresses your appetite
Two people can start retatrutide on the same day, follow the same protocol, and have completely different appetite experiences during the first month. Understanding why helps set realistic expectations and troubleshoot if results are not appearing on the expected timeline.
Starting dose and titration speed
This is the single biggest variable. The dose escalation schedule directly determines when you reach appetite-suppressing levels of the medication.
In clinical trials, participants who started at 2mg and escalated every 4 weeks through 4mg, 8mg, and finally 12mg experienced a gradual onset of appetite suppression. Those who started at 4mg saw faster initial appetite effects but also experienced higher rates of nausea and other gastrointestinal side effects.
The data is clear on this tradeoff. Starting at 2mg reduces nausea rates significantly compared to starting at 4mg, but it also delays the onset of meaningful appetite suppression by approximately 4 weeks. For most people, the slower start is worth it because better tolerability leads to better adherence, and adherence is ultimately what produces results.
Body weight and composition
Higher body weight typically means it takes longer for retatrutide to reach effective concentrations in the body. This is a simple pharmacokinetic reality. More body mass means the medication is distributed across a larger volume, resulting in lower peak concentrations at any given dose.
This does not mean retatrutide is less effective for heavier individuals. The clinical trials included participants across a wide BMI range and showed consistent benefits. But it does mean that someone with a BMI of 45 might not experience the same appetite suppression at 4mg that someone with a BMI of 32 feels at the same dose.
Previous GLP-1 medication use
If you are switching from tirzepatide to retatrutide or from semaglutide, your body has already adapted to GLP-1 receptor activation. This prior exposure may slightly blunt the initial appetite-suppressing effects of retatrutide GLP-1 component, though the additional GIP and glucagon pathways will still be novel.
Some people transitioning from high-dose tirzepatide or semaglutide report a temporary period where appetite suppression feels weaker before retatrutide glucagon receptor effects begin contributing meaningfully. This is normal and usually resolves within 4-6 weeks as the full triple receptor activation establishes itself.
Metabolic health status
People with type 2 diabetes may experience somewhat different appetite timelines compared to those without diabetes. The phase 2 study in type 2 diabetes patients showed significant appetite reductions, but the overall weight loss was slightly lower than in the obesity-only trial (16.9% versus 24.2% at the highest doses over comparable timeframes).
Insulin resistance, chronic inflammation, and disrupted hunger hormone signaling can all influence how quickly appetite changes become noticeable. This does not mean retatrutide is less effective for people with metabolic conditions. It means expectations around timing should account for these variables.
Diet and lifestyle factors
What you eat while on retatrutide affects how noticeable the appetite suppression feels. A diet high in processed carbohydrates and sugar can partially counteract the appetite-suppressing effects by creating insulin spikes and blood sugar crashes that drive hunger independent of GLP-1 signaling.
People who combine retatrutide with a protein-focused diet, adequate hydration, and regular physical activity tend to notice appetite changes earlier and more dramatically than those who make no dietary modifications.
Sleep quality also matters. Poor sleep disrupts ghrelin and leptin levels, the primary hunger and satiety hormones, which can partially offset GLP-1 mediated appetite suppression. Stress has similar effects through cortisol elevation.
Individual genetic variation
GLP-1 receptor density, GIP receptor sensitivity, and glucagon receptor expression vary between individuals. These genetic differences explain why some people are hyperresponders who feel appetite suppression from the very first dose, while others require several weeks of dose escalation before noticing meaningful changes.
There is no way to predict which category you will fall into before starting the medication. The clinical trials demonstrate that the vast majority of participants eventually achieve significant appetite suppression, but the timeline to get there varies by several weeks between individuals.
The dose escalation schedule and how appetite changes at each level
Understanding the dose escalation protocol is essential because appetite suppression is fundamentally dose-dependent with retatrutide. Each dose level produces qualitatively different appetite effects.
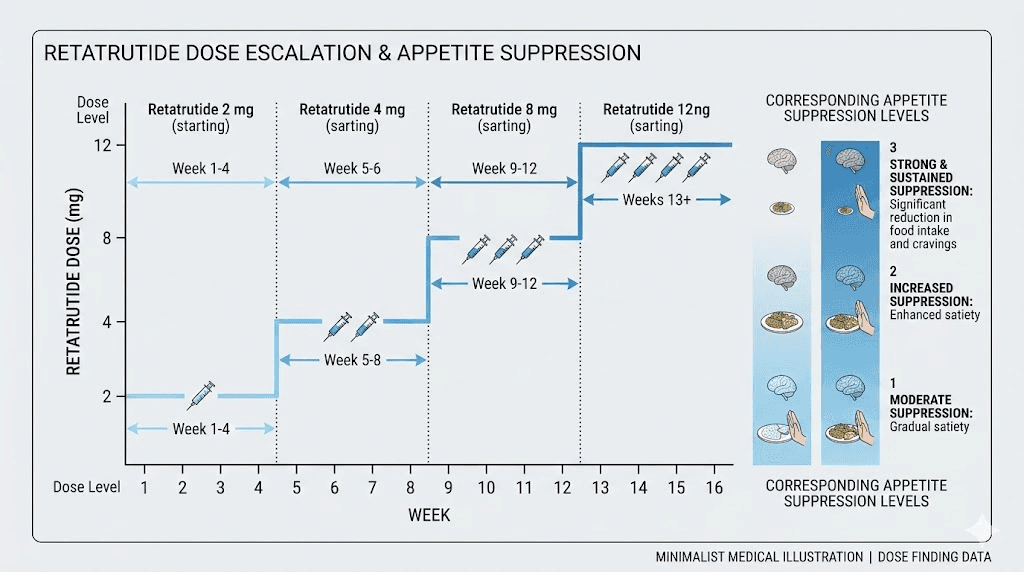
2mg weekly: the foundation (weeks 1-4)
The 2mg starting dose has minimal appetite-suppressing activity. In clinical trials, the 0.5mg and 1mg doses showed no statistically significant difference from placebo for appetite outcomes. While 2mg is higher than these sub-therapeutic doses, it is still below the threshold where most people experience clear appetite changes.
Purpose of this phase: allow your body to adjust to the medication, establish tolerance, and minimize gastrointestinal side effects that would otherwise be more severe at higher starting doses.
What to expect: possibly subtle appetite changes, but do not count on them. Focus on tolerability.
4mg weekly: appetite suppression begins (weeks 5-8)
At 4mg, retatrutide crosses the threshold into clinically meaningful appetite suppression for most people. The phase 2 study showed statistically significant hunger reductions beginning at this dose level.
Hunger scores decreased by 10.4 points versus placebo at week 8 on 4mg. Desire for sweet foods decreased by 14.0 to 19.5 points as early as week 4 after reaching this dose. Disinhibition, the tendency to overeat in response to triggers, improved significantly.
This is typically the dose where people first say, I notice a difference. Meals become more satisfying. The mental pull toward food between meals weakens. Cravings for specific foods, particularly sweet and high-calorie options, begin to fade.
8mg weekly: strong appetite suppression (weeks 9-12+)
The transition from 4mg to 8mg typically produces a noticeable step-change in appetite suppression. Clinical data at this dose level shows:
Hunger reduction of 11.4 points versus placebo at week 12
Significant decreases in desire for salty foods (16.6 points) and fatty foods (14.5 points) at week 16
Perceived hunger on the Eating Inventory decreased by 1.9 points at week 36
Disinhibition improved by 2.1 points at week 36
At 8mg, many people describe appetite suppression as effortless. It is not that they are fighting hunger and winning. The hunger simply is not there, or is so muted that it barely registers. Food preferences shift noticeably. The gravitational pull toward calorie-dense foods weakens substantially.
Weight loss accelerates at this dose level. In the phase 2 trial, the 8mg group achieved approximately 17.3% weight reduction at 24 weeks, a rate of loss that would not be possible without profound appetite suppression driving significant caloric deficit.
12mg weekly: maximum therapeutic effect (weeks 13+)
The 12mg maintenance dose represents the highest studied dose and produces the strongest appetite effects. By week 24, hunger reductions reached approximately 15-16 points versus placebo, and dietary restraint increased by 2.0 points, indicating not just reduced hunger but improved ability to consciously manage food intake.
At week 36, the 12mg group showed the most dramatic eating behavior changes:
Perceived hunger decreased by 2.4 points versus placebo
Disinhibition improved by 2.6 points
Dietary restraint increased by 3.3 points
100% of participants achieved at least 5% body weight loss by week 48
83% achieved 15% or greater weight loss
Mean weight reduction reached 24.2% at 48 weeks
These numbers represent the strongest weight loss and appetite-related outcomes ever recorded in clinical trials for any GLP-1 class medication. The 12mg dose does not simply suppress appetite. It fundamentally alters the metabolic and neurological environment in which appetite operates.
Managing side effects during the appetite adjustment period
Appetite suppression and side effects often arrive together. Understanding this relationship helps you distinguish between the medication working as intended and the medication causing problems that need addressing.
Nausea: the most common early experience
Nausea is the most frequently reported side effect with retatrutide, occurring in 14% of participants at 1mg up to 60% at 12mg in clinical trials. The nausea is not a separate issue from appetite suppression. It is partially a manifestation of the same mechanisms that reduce hunger, specifically the delayed gastric emptying and altered gut signaling that GLP-1 and GIP receptor activation produce.
The timing of nausea follows a predictable pattern. It peaks during the first 1-2 weeks at each new dose level and typically resolves within 4-8 weeks as receptor adaptation occurs. The phase 2 trial found that starting at 2mg rather than 4mg significantly reduced nausea rates during escalation, validating the conservative titration approach.
Practical management strategies:
Eat smaller meals more frequently rather than large meals
Avoid high-fat and greasy foods during dose escalation periods
Stay well hydrated throughout the day
Time your injection when minor nausea will be least disruptive
Consider avoiding foods that commonly trigger nausea (spicy, acidic, very sweet)
Decreased appetite versus loss of appetite
There is an important distinction between healthy appetite suppression and appetite loss that crosses into problematic territory. Retatrutide should reduce your drive to eat and help you feel satisfied with smaller portions. It should not make you unable to eat at all or cause you to go entire days without any food intake.
If you are experiencing complete appetite absence to the point where you cannot maintain minimum caloric intake (generally below 1,200 calories per day for women or 1,500 for men), this may indicate that your current dose is too high or that escalation happened too quickly. This is particularly important because inadequate protein intake during rapid weight loss can lead to muscle loss and hair thinning, both of which are avoidable with proper nutritional management.
Gastrointestinal adaptation timeline
Beyond nausea, other gastrointestinal effects follow their own timelines:
Diarrhea affects some users and typically appears during dose escalation periods. It usually resolves within 2-3 weeks at each dose level.
Constipation can occur as gastric emptying slows significantly. Adequate fiber, hydration, and in some cases magnesium supplementation help manage this.
Bloating and abdominal discomfort are common during the first few weeks and typically improve as the body adjusts to delayed gastric emptying.
The overall pattern is consistent: most gastrointestinal side effects peak during dose escalation, diminish within weeks, and become minimal at stable maintenance doses. Meanwhile, appetite suppression persists and often deepens over time. The side effects are temporary. The appetite changes are sustained.
The science behind why triple receptor activation changes appetite differently
Understanding the neuroscience helps explain why retatrutide appetite suppression feels qualitatively different from single-receptor medications. This is not academic. It is practical. If you know what is happening in your brain, you can better interpret and work with the appetite changes as they develop.
Central nervous system effects
All three receptor types activated by retatrutide have targets in the central nervous system that influence appetite regulation.
GLP-1 receptors in the hypothalamus and nucleus tractus solitarius (NTS) mediate direct satiety signaling. When retatrutide activates these receptors, it increases the production of satiety-promoting neuropeptides while suppressing hunger-promoting ones. This is the same mechanism that semaglutide uses, and it produces the familiar sensation of feeling full sooner and staying full longer.
GIP receptors in the brain contribute to reward processing and food motivation. Activation of these receptors may reduce the hedonic drive to eat, the pleasure-seeking component of appetite that makes you want to eat even when you are not physically hungry. This helps explain why people on tirzepatide and retatrutide often report that food just becomes less interesting, a phenomenon that goes beyond simple hunger reduction.
Glucagon receptors influence energy homeostasis through effects on hepatic glucose production and systemic energy balance. When glucagon pathways are activated, the body shifts toward catabolic metabolism, breaking down stored energy rather than seeking new energy from food. This metabolic shift may contribute to appetite suppression indirectly by reducing the biological signals that drive hunger when energy stores are being depleted.
Peripheral effects on gut signaling
The gut is sometimes called the second brain, and retatrutide affects it through multiple mechanisms simultaneously. Delayed gastric emptying means food stays in the stomach longer, providing sustained signals of fullness to the brain via the vagus nerve. Reduced gastrointestinal motility throughout the digestive tract prolongs the period during which nutrient sensors in the gut wall send satiety signals.
The glucagon component adds something unique: reduced lipogenesis in the liver means the body is less efficient at converting dietary fat into stored fat, which alters the metabolic feedback loops that regulate hunger. When the body is burning stored fat for energy through glucagon-mediated lipolysis, the signals driving you to consume more calories are naturally attenuated.
The reward pathway recalibration
Perhaps the most fascinating aspect of retatrutide appetite suppression is its effect on food reward processing. Research on GLP-1 receptor agonists shows that these medications reduce activation in brain regions associated with food reward, including the insula, amygdala, and orbitofrontal cortex. A recent study on semaglutide specifically demonstrated that the medication reduces appetite while simultaneously increasing dopamine reward signaling in the brain, suggesting that it does not simply blunt pleasure but rather redirects it.
With retatrutide adding GIP and glucagon activation on top of this, the reward recalibration may be even more comprehensive. Anecdotal reports from clinical trial participants describe not just reduced hunger but a fundamental shift in how they think about and relate to food. This is not willpower. It is neurochemistry.
What to do when appetite suppression is not happening on schedule
Not everyone follows the textbook timeline. If you are several weeks into retatrutide and not feeling the appetite suppression you expected, here are the most common reasons and solutions.
You are still on the starting dose
The 2mg starting dose produces minimal appetite effects for most people. If you are in weeks 1-4 and wondering where the appetite suppression is, the answer is straightforward: it has not arrived yet because your dose is not high enough. The clinical data is clear that meaningful appetite suppression begins at 4mg and above.
Solution: be patient through the titration period. The starting dose exists for tolerability, not efficacy.
Your titration schedule is too conservative
While slower titration reduces side effects, an excessively conservative approach can delay appetite suppression unnecessarily. If you have been on 2mg for 6+ weeks without progressing to 4mg and are tolerating the medication well, the delay in escalation is likely postponing the appetite benefits you are seeking.
Solution: discuss titration timing with your healthcare provider. The standard protocol in clinical trials escalated doses every 4 weeks.
Caloric compensation is masking the effects
Sometimes appetite suppression is occurring, but dietary habits are compensating without you realizing it. You might be eating less at meals but drinking more calories. You might have naturally reduced portion sizes but added an extra meal. You might feel less hungry during the day but eating more in the evening out of habit rather than hunger.
Solution: track food intake for a few days to objectively assess whether your total caloric consumption has actually changed. Many people discover the appetite suppression is working but their eating patterns have not adjusted to match.
High-carb diet is fighting the medication
Diets high in refined carbohydrates and sugar create insulin spikes and subsequent blood sugar crashes that trigger hunger independent of GLP-1 signaling. If your diet consists primarily of processed foods, the medication may be working on the GLP-1, GIP, and glucagon pathways while insulin-mediated hunger is still driving eating behavior through a different mechanism entirely.
Solution: shift toward a protein-focused diet with complex carbohydrates, healthy fats, and adequate fiber. This aligns dietary approach with the medication mechanisms and allows appetite suppression to express itself more fully.
Sleep deprivation or chronic stress
Inadequate sleep elevates ghrelin (the hunger hormone) and reduces leptin (the satiety hormone). Chronic stress elevates cortisol, which drives appetite, particularly for high-calorie comfort foods. Both of these hormonal disruptions can partially counteract GLP-1 mediated appetite suppression.
Solution: prioritize 7-9 hours of sleep and implement stress management practices. These are not optional lifestyle tweaks. They are biological prerequisites for optimal medication response.
Unrealistic expectations
Some people expect retatrutide to eliminate hunger entirely. That is not what it does, and it is not what you want it to do. Healthy appetite suppression means reduced hunger, smaller portions feeling satisfying, fewer cravings, and less food noise. It does not mean zero interest in food or inability to eat.
If you are experiencing moderate appetite reduction and eating 20-30% fewer calories than before, the medication is working. That level of reduction, sustained over months, produces the dramatic weight loss seen in clinical trials.
Long-term appetite effects and what happens after month six
The question is not just when appetite suppression starts. It is how long it lasts and what happens over extended treatment periods.
Does appetite suppression fade over time?
Based on available data, appetite suppression with retatrutide does not appear to diminish significantly over the treatment period studied. The eating behavior data at week 36 actually showed stronger effects than at week 24 for the 8mg and 12mg groups, suggesting that appetite-related benefits may continue deepening rather than fading.
This contrasts with some concerns about GLP-1 receptor desensitization. While some receptor adaptation does occur (explaining why gastric emptying effects attenuate over time even as doses increase), the central appetite-suppressing effects appear to be maintained through mechanisms that do not rely solely on gastric motility.
The glucagon receptor component may contribute to sustained appetite suppression through metabolic mechanisms that are less susceptible to tolerance. Continued lipolysis, thermogenesis, and metabolic shifting create an ongoing environment of energy availability that reduces hunger signals independent of GLP-1 receptor adaptation.
Weight loss trajectory and appetite at different phases
Weight loss with retatrutide follows a characteristic pattern:
Months 1-3: Slow start during dose escalation, transitioning to accelerating weight loss as appetite suppression establishes. Average weight loss in this period is approximately 5-8% of body weight at therapeutic doses.
Months 3-6: Peak rate of weight loss as full therapeutic dose is maintained and appetite suppression is maximized. The 12mg group lost approximately 17.5% by week 24 (month 6).
Months 6-12: Continued weight loss at a gradually decelerating rate. By week 48 (approximately month 12), the 12mg group had lost 24.2%, with 93% achieving at least 10% total body weight reduction.
The decelerating weight loss in months 6-12 does not indicate failing appetite suppression. It reflects the body reaching a new equilibrium where metabolic rate has adjusted to the lower body weight and caloric intake stabilizes at a sustainable level. Appetite suppression remains active but is balanced by the reduced caloric needs of a smaller body.
What happens to appetite if you stop retatrutide
This is a critical question that does not have definitive answers from retatrutide-specific studies yet, but data from semaglutide and tirzepatide trials provides relevant context.
Studies with semaglutide show that discontinuation leads to appetite returning to baseline levels and weight regain of approximately two-thirds of the lost weight within one year. Similar patterns are expected with retatrutide, as the underlying biological drivers of appetite are being managed by the medication, not permanently altered.
This does not mean the medication is a failure. It means retatrutide, like all GLP-1 class medications, works best as a sustained treatment rather than a temporary intervention. The appetite suppression lasts as long as the medication is active in your system.
Retatrutide appetite suppression for specific goals
Different people use retatrutide for different reasons, and the appetite suppression timeline may feel different depending on what you are trying to achieve.
For significant weight loss (50+ pounds)
If your goal involves losing 50 or more pounds, the appetite suppression timeline with retatrutide is actually encouraging. The phase 2 trial showed that participants on 12mg lost an average of 57.8 pounds (26.2 kg) by week 48. The phase 3 TRIUMPH-4 trial recently reported average weight loss of up to 71.2 pounds.
For this level of weight loss, expect appetite suppression to build gradually over the first 8-12 weeks, then sustain at a high level throughout the treatment period. The key is patience during the dose escalation phase and consistency once you reach maintenance dosing.
For metabolic health improvement
If your primary concern is metabolic health rather than the scale number, appetite suppression serves a different but equally important role. Reduced caloric intake improves insulin sensitivity, reduces liver fat, and lowers inflammatory markers. The phase 2 study showed HbA1c reductions of up to 2.02% at 24 weeks, outcomes that are partially mediated by the same appetite suppression that drives weight loss.
For metabolic goals, even moderate appetite suppression at lower doses (4-8mg) can produce meaningful health improvements without requiring maximum dosing.
For body composition optimization
If you are focused on losing fat while preserving lean mass, the appetite suppression from retatrutide needs to be paired with strategic nutrition. The glucagon component of retatrutide preferentially targets fat tissue through lipolysis, which is advantageous for body composition. However, adequate protein intake (generally 0.7-1.0 grams per pound of body weight) is essential to support muscle preservation during weight loss.
Appetite suppression can make hitting protein targets challenging. Many people find that appetite suppression reduces interest in all food categories, including protein sources. Proactive meal planning that prioritizes protein at every eating occasion helps ensure that the caloric deficit created by appetite suppression comes primarily from fat and carbohydrate reduction rather than protein deficit.
The role of food preferences and cravings in the appetite timeline
Appetite suppression is not just about hunger levels. The phase 2 study on retatrutide eating behaviors revealed that the medication changes what you want to eat, not just how much.
Sweet food cravings
Desire for sweet foods showed the earliest response to retatrutide. By week 4 on doses of 4mg and above, participants showed 14.0 to 19.5 point reductions in sweet food desire compared to placebo. This is one of the first appetite-related changes most people notice, often before general hunger levels decrease significantly.
The reduction in sweet cravings is particularly valuable because sugar and processed carbohydrate consumption drives insulin-mediated hunger cycles that can perpetuate overeating independent of actual energy needs. Breaking this cycle early creates a positive feedback loop where reduced sugar intake leads to more stable blood sugar, which further reduces hunger and cravings.
Salty food cravings
Desire for salty foods decreased significantly by week 16, with reductions of 16.6 points versus placebo in clinical data. This later onset compared to sweet cravings may reflect different neurological mechanisms for salt preference versus sugar preference.
Fatty food cravings
Similarly, desire for fatty and greasy foods decreased by 14.5 points versus placebo, with the most significant changes appearing around weeks 12-16. This reduction aligns with the timing of glucagon receptor effects becoming fully established, which makes sense given that glucagon activation specifically reduces lipogenesis and promotes fat oxidation.
Food preference shifts
Beyond reduced cravings, many people on retatrutide and other GLP-1 medications report qualitative shifts in food preferences. Foods that were previously irresistible become neutral or even unappealing. Meanwhile, simpler, whole foods like lean proteins, vegetables, and fruits become more satisfying. This is not a conscious dietary choice. It appears to be a neurochemical shift in how the brain processes food reward signals.
In the phase 2 study, participants specifically described having different food preferences as one of the key behavioral changes they experienced within the first 8 weeks of treatment. This preference shift supports the theory that GLP-1 class medications fundamentally alter food reward processing in the brain, not just hunger signaling.
Combining retatrutide with lifestyle changes for faster appetite results
Retatrutide is not a standalone solution. The clinical trials that produced 24.2% weight loss included lifestyle modification components, and the appetite suppression works best when supported by complementary habits.
Protein-first eating
Prioritizing protein at every meal enhances appetite suppression through two mechanisms. First, protein is the most satiating macronutrient, producing stronger fullness signals per calorie than carbohydrates or fat. Second, adequate protein intake prevents muscle loss during rapid weight loss, preserving metabolic rate and ensuring that weight lost is primarily fat.
Aim for 25-40 grams of protein at each meal. If appetite suppression makes this difficult, consider liquid protein sources like shakes, which are generally easier to consume when appetite is low.
Hydration
Dehydration can mimic hunger, and GLP-1 medications can increase dehydration risk through reduced fluid intake (when you eat less, you also consume less water from food). Staying well hydrated helps the appetite-suppressing effects of retatrutide work optimally and prevents false hunger signals from being confused with thirst.
Regular physical activity
Exercise has complex effects on appetite. Acute vigorous exercise temporarily suppresses appetite through exercise-induced anorexia. Regular moderate exercise improves insulin sensitivity, which synergizes with retatrutide GLP-1 and GIP effects. Resistance training preserves muscle mass during weight loss, maintaining metabolic rate and preventing the metabolic adaptation that can stall progress.
The combination of retatrutide appetite suppression and regular exercise creates a more sustainable caloric deficit than either approach alone.
Meal timing and structure
Many people on retatrutide find that their natural eating patterns shift. Three large meals per day may become two smaller meals and a snack. Some people gravitate toward intermittent fasting patterns naturally because they genuinely are not hungry in the morning.
Rather than fighting these shifts, working with them can enhance the appetite suppression effect. If you are not hungry at breakfast, you do not need to force breakfast. If you find that two meals per day adequately sustains you, that pattern can work well as long as those two meals contain sufficient protein and essential nutrients.
Frequently asked questions
How long does it take for retatrutide to suppress appetite?
Most people notice initial appetite changes between weeks 2 and 4 on retatrutide, with clear appetite suppression typically establishing between weeks 4 and 8. The exact timeline depends on your dose escalation schedule, as the starting dose of 2mg produces minimal appetite effects and meaningful suppression begins at 4mg and above.
Is retatrutide appetite suppression stronger than semaglutide?
Clinical data suggests yes. Retatrutide targets three receptor pathways (GLP-1, GIP, and glucagon) compared to semaglutide targeting only GLP-1. In animal studies, retatrutide produced the largest decreases in food intake compared to semaglutide and other GLP-1 medications. The 24.2% weight loss at 48 weeks with retatrutide exceeds semaglutide 14.9% at 68 weeks, suggesting deeper and more sustained appetite suppression.
Does retatrutide reduce food cravings?
Yes. The phase 2 study specifically measured cravings and found significant reductions in desire for sweet foods (as early as week 4), salty foods (by week 16), and fatty foods (by weeks 12-16) at doses of 4mg and above compared to placebo. Many participants also reported spontaneous shifts in food preferences toward simpler, whole foods.
What if I do not feel appetite suppression after 4 weeks on retatrutide?
If you are on the 2mg starting dose at week 4, lack of appetite suppression is expected. The 2mg dose is primarily for tolerability, not appetite reduction. Appetite effects typically begin at 4mg and above. If you are already at 4mg or higher and not noticing changes, factors like diet composition, sleep quality, stress, and individual biology may be influencing your response.
Can I take retatrutide with other appetite-suppressing peptides?
Combining retatrutide with other GLP-1 medications is not recommended as it could increase side effect risk without proportional benefit. However, supportive peptides that target different pathways (such as BPC-157 for gut health or MOTS-c for metabolic optimization) may complement retatrutide through non-overlapping mechanisms. Always consult a healthcare provider before combining medications.
Does the appetite suppression from retatrutide wear off?
Based on available clinical data through 48 weeks, appetite suppression does not appear to diminish over time. The eating behavior data at week 36 actually showed stronger effects than at week 24 for the 8mg and 12mg groups. However, if you stop taking retatrutide, appetite is expected to return to baseline levels, similar to patterns seen with semaglutide discontinuation.
How does retatrutide appetite suppression compare to tirzepatide?
Retatrutide adds glucagon receptor activation to the dual GLP-1/GIP activation that tirzepatide provides. This additional pathway produces appetite suppression through metabolic mechanisms (increased lipolysis, thermogenesis) that tirzepatide does not directly access. In clinical trials, retatrutide achieved 24.2% weight loss at 48 weeks versus tirzepatide approximately 21% at 72 weeks, suggesting stronger overall appetite and metabolic effects.
What should I eat while waiting for retatrutide appetite suppression to start?
During the dose escalation period, focus on a protein-rich diet with complex carbohydrates and healthy fats. Avoid excessive sugar and processed foods that create insulin-mediated hunger cycles independent of GLP-1 signaling. This dietary approach supports the medication mechanisms and may help appetite suppression become noticeable sooner.
External resources
Appetite, eating attitudes, and eating behaviours during treatment with retatrutide (PubMed Central)
Retatrutide: A Game Changer in Obesity Pharmacotherapy (PubMed Central)
Weight Loss and Maintenance Related to GLP-1 Receptor Agonists (PubMed Central)
How Fast Do GLP-1 Drugs Suppress Appetite (Cleveland Clinic)
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions. SeekPeptides members access detailed retatrutide dosing protocols, dosage calculators, and expert guidance for navigating the appetite suppression timeline with confidence.
In case I do not see you, good afternoon, good evening, and good night. May your appetite stay manageable, your protocols stay consistent, and your results stay rewarding.