Apr 4, 2026

Something shifts in your body around your late thirties or early forties. It is quiet at first. The scale creeps up a pound or two. Your jeans fit differently. Sleep gets patchy. And the strategies that worked for years, the calorie cuts, the morning runs, the discipline that once felt effortless, they stop producing results. This is not a failure of willpower. This is perimenopause rewriting your metabolic rules, and your body is responding exactly the way declining estrogen and progesterone tell it to.
Semaglutide has entered this conversation with force. Originally developed for type 2 diabetes management, this GLP-1 receptor agonist has shown remarkable weight loss results across clinical trials. But here is the question most resources skip entirely: does semaglutide work differently during perimenopause? Does the hormonal chaos of this transition change how effectively it suppresses appetite, burns fat, or preserves muscle? The answer is more nuanced than most articles admit, and the research emerging from studies on postmenopausal women paints a picture that is both encouraging and complicated.
This guide covers everything researchers and women navigating perimenopause need to know about semaglutide during this specific life stage. We will dig into the hormonal mechanisms that make perimenopausal weight gain uniquely stubborn, examine what clinical data actually shows about semaglutide effectiveness in this population, explore the synergy between hormone replacement therapy and GLP-1 medications, and provide practical protocols that account for the biological realities of the menopausal transition. SeekPeptides has compiled the most current research to help you navigate this intersection of hormonal health and peptide science with clarity.
Why perimenopause makes weight loss so difficult
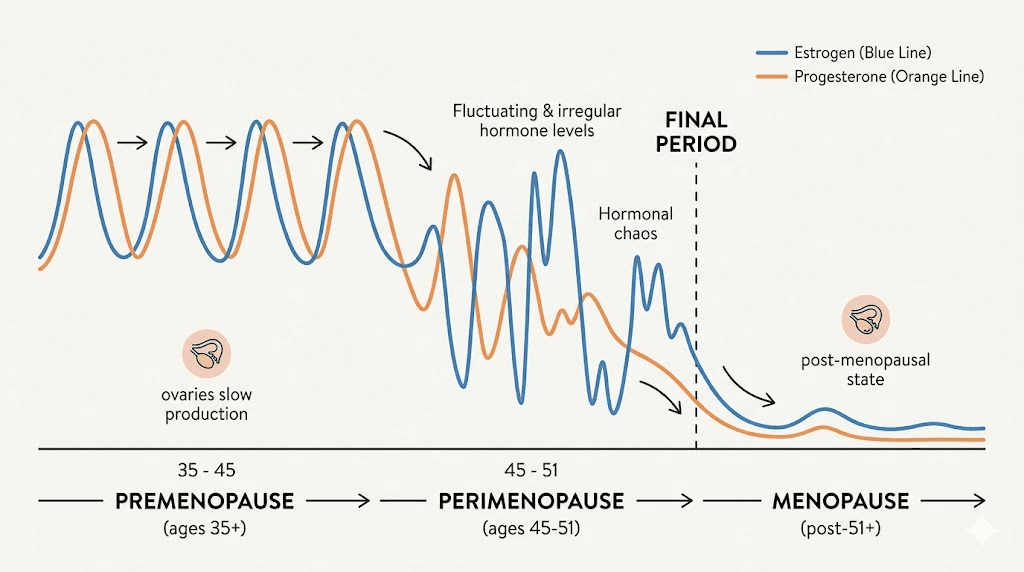
Perimenopause is not a single event. It is a transition that can last anywhere from four to ten years before your final menstrual period. During this time, estrogen does not simply decline in a straight line. It fluctuates wildly, sometimes spiking to levels higher than your reproductive peak before crashing to near-menopausal lows within the same month. Progesterone, meanwhile, drops more consistently and earlier. This hormonal rollercoaster creates metabolic disruptions that go far beyond what most people realize.
The weight gain is real. Research shows women gain an average of 1.5 pounds per year during midlife, with a study published in the International Journal of Obesity documenting an average weight gain of 12 pounds within eight years of reaching menopause. But the number on the scale only tells part of the story.
What changes is not just how much fat you carry but how your entire metabolic system operates. Your resting metabolic rate drops. Your body preferentially stores energy as fat rather than burning it. And the mechanisms that used to respond predictably to calorie reduction and exercise become less reliable. Understanding exactly why this happens is the first step toward knowing why semaglutide can be particularly useful during this window.
The four phases of perimenopausal metabolic change
Perimenopause does not unfold uniformly. Researchers generally break it into distinct phases, each with different metabolic implications.
Early perimenopause begins when cycle length starts varying by seven or more days. Estrogen levels may actually be higher than normal during this phase, while progesterone begins its decline. Many women notice water retention, bloating, and mood changes before significant weight gain begins.
Mid perimenopause is when the metabolic disruption intensifies. Estrogen swings become more dramatic. Cycles may skip months entirely. Insulin resistance begins to develop or worsen. This is often when women notice the classic nothing works anymore pattern with their weight management strategies. GLP-1 therapy started during this phase can intercept the metabolic decline before it fully establishes.
Late perimenopause involves longer gaps between periods and more consistently low estrogen. The metabolic changes are well established by this point. Visceral fat accumulation is typically noticeable, and blood sugar markers like fasting insulin and HbA1c may show concerning trends.
Early postmenopause (the first few years after your final period) is when bone loss accelerates most rapidly and metabolic changes stabilize at their new baseline. Women who begin semaglutide during perimenopause and continue into postmenopause often see sustained benefits because they addressed the metabolic dysfunction before it became deeply entrenched.
The insulin resistance connection
Here is what most articles about perimenopausal weight gain miss entirely. Estrogen plays a direct role in insulin sensitivity. When estrogen levels drop, your cells become less responsive to insulin. Your body compensates by producing more insulin, which drives fat storage, particularly visceral fat around the midsection. This is not the same subcutaneous fat you might have carried on your hips and thighs in your twenties and thirties. Visceral fat is metabolically active, producing inflammatory compounds that further worsen insulin resistance. A vicious cycle forms.
Semaglutide interrupts this cycle. As a GLP-1 receptor agonist, it enhances insulin secretion when blood glucose is elevated and suppresses glucagon release. For perimenopausal women dealing with new or worsening insulin resistance, this mechanism targets the root metabolic dysfunction, not just the appetite.
The distinction matters. Many weight loss approaches only address caloric intake. Semaglutide addresses the hormonal and metabolic machinery that is actively working against you during perimenopause.
Where fat is stored changes everything
Before perimenopause, estrogen directs fat storage toward the hips, thighs, and buttocks. This is the classic gynoid fat distribution pattern. As estrogen declines, fat redistribution shifts toward the abdomen, creating the android pattern more commonly associated with male fat storage. This visceral fat accumulation is not cosmetic. It is a cardiovascular risk factor, a driver of metabolic dysfunction, and a contributor to systemic inflammation.
Clinical research shows semaglutide reduces visceral fat more effectively than subcutaneous fat in many patients. For perimenopausal women, this preferential targeting of the most metabolically dangerous fat is particularly significant.
The health implications extend beyond appearance. Visceral fat produces interleukin-6, tumor necrosis factor-alpha, and other inflammatory markers that contribute to cardiovascular disease, type 2 diabetes, and even certain cancers. Women who successfully reduce visceral fat during perimenopause, whether through semaglutide, lifestyle changes, or both, measurably reduce their risk profile for decades to come. The window matters. The metabolic patterns you establish during this transition tend to persist.
The leptin resistance problem
Leptin is the hormone that tells your brain you have enough stored energy and do not need to eat more. In theory, women with excess fat should have plenty of leptin signaling fullness. In practice, chronic excess body fat leads to leptin resistance, where the brain stops responding to the signal. It is like living next to a noisy highway. Eventually you stop hearing it.
Perimenopause worsens leptin resistance through multiple pathways. Inflammation from visceral fat impairs leptin signaling. Sleep disruption reduces leptin sensitivity. And estrogen normally helps maintain proper leptin and appetite signaling, so its decline during perimenopause compromises this system further.
Semaglutide works through a different appetite regulation pathway (GLP-1) that bypasses the broken leptin system. This is one reason it can be so effective for women who have been unable to lose weight through willpower alone. The problem was never willpower. It was a biological signaling failure that semaglutide corrects from a different angle.
The cortisol amplifier
Perimenopause does not happen in isolation. Sleep disruption from night sweats and hormonal fluctuations elevates cortisol. Elevated cortisol promotes visceral fat storage. Poor sleep also increases ghrelin (the hunger hormone) and decreases leptin (the satiety hormone), creating appetite dysregulation on top of the metabolic changes already in progress.
Semaglutide acts on the appetite regulation system in the brain, helping to normalize the hunger signals that cortisol and sleep disruption have thrown off course. This is why many perimenopausal women describe the effect of semaglutide as turning off the food noise, a reduction in the constant background thinking about food that intensifies during this transition.
How semaglutide works during perimenopause
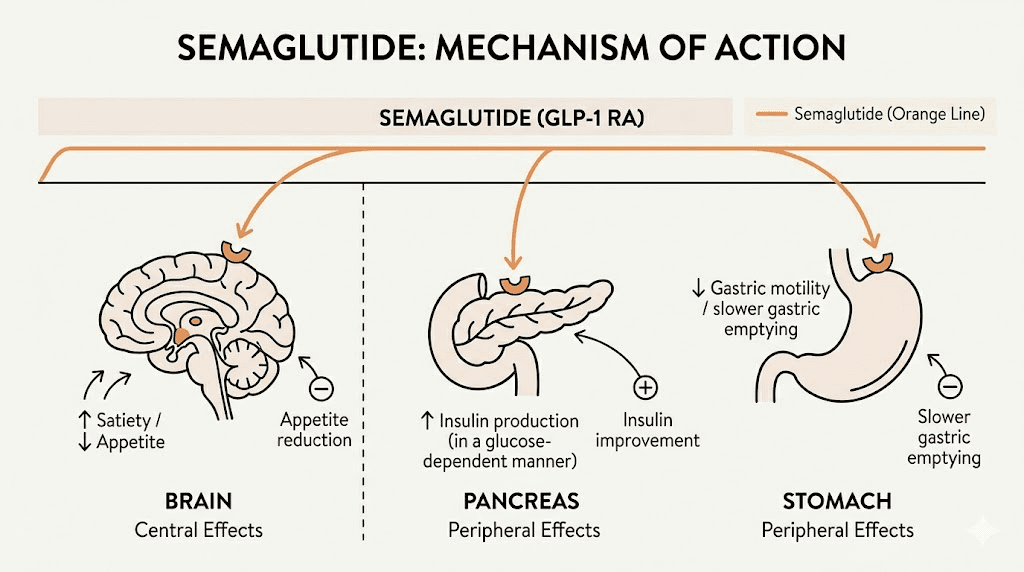
Semaglutide mimics GLP-1, a hormone your gut naturally produces after eating. It binds to GLP-1 receptors in the brain, pancreas, and gastrointestinal tract. The effects cascade through multiple systems simultaneously.
Appetite suppression and food noise reduction
The hypothalamus contains GLP-1 receptors that regulate hunger and satiety. Semaglutide activates these receptors, reducing appetite at a neurological level. But it goes further than simple appetite suppression. Research suggests semaglutide also influences the mesolimbic dopamine pathway, the brain reward system. This means it does not just make you less hungry. It reduces the psychological drive toward food, the cravings, the food fixation, the emotional eating patterns that often intensify during hormonal transitions.
For perimenopausal women, this dual mechanism is critical. Hormonal fluctuations during perimenopause directly affect neurotransmitter levels, including serotonin and dopamine. Many women experience increased cravings for carbohydrates and sugar during this time, driven by the brain seeking serotonin boosts. Semaglutide helps regulate these pathways from a different angle.
Insulin sensitivity improvement
Semaglutide enhances glucose-dependent insulin secretion and suppresses inappropriately elevated glucagon. For perimenopausal women whose insulin sensitivity is declining due to estrogen loss, this correction addresses a fundamental metabolic shift that diet and exercise alone cannot fully counteract.
A study published in the journal Menopause found that after four months of semaglutide 1 mg treatment, fat mass loss and total weight loss were comparable between postmenopausal and premenopausal women. Despite postmenopausal women starting with greater initial weight and fat mass, they responded to semaglutide at similar rates. This finding challenges the assumption that hormonal status inherently limits semaglutide effectiveness.
Gastric emptying and satiety signaling
Semaglutide slows gastric emptying, meaning food stays in the stomach longer. This prolongs feelings of fullness after meals and reduces the tendency to overeat. For women dealing with the increased appetite that often accompanies perimenopause, this mechanical effect complements the neurological appetite suppression. The result is that smaller portions feel genuinely satisfying rather than restrictive.
Understanding when appetite suppression begins helps set realistic expectations. Most women notice reduced appetite within the first one to two weeks, with full effects developing over four to eight weeks as the dose is gradually increased.
Anti-inflammatory effects
Chronic low-grade inflammation is a hallmark of perimenopause. Declining estrogen reduces the body natural anti-inflammatory defenses while increasing visceral fat pumps out pro-inflammatory cytokines. This inflammatory state does more than make you feel lousy. It actively promotes weight gain, worsens insulin resistance, and accelerates aging.
Semaglutide demonstrates anti-inflammatory properties independent of weight loss. It reduces C-reactive protein (CRP), a key marker of systemic inflammation, and decreases levels of inflammatory cytokines. For perimenopausal women, this means semaglutide is not just helping with the symptom (weight gain) but addressing one of the underlying drivers (inflammation) that makes perimenopausal weight gain so stubborn and metabolically dangerous.
The anti-inflammatory effect also partially explains why some women on semaglutide report improvements in joint pain, skin sensitivity, and general achiness during perimenopause. These symptoms are often driven by the same inflammatory processes that semaglutide helps modulate.
GLP-1 receptors in the brain: beyond appetite
GLP-1 receptors are not limited to the gut and pancreas. They exist throughout the brain, including areas involved in learning, memory, emotion regulation, and neuroprotection. This is relevant for perimenopausal women because estrogen also plays a neuroprotective role, and its decline contributes to the brain fog, memory lapses, and mood changes common during this transition.
Emerging research suggests that GLP-1 receptor activation may provide some of the neuroprotective benefits that declining estrogen once provided. Clinical trials are actively investigating semaglutide for neurodegenerative conditions, and while the research is early, the theoretical basis for cognitive benefits during perimenopause is compelling. Some women report improved mental clarity on semaglutide, which may reflect both the metabolic improvements (more stable blood sugar means more stable brain fuel supply) and the direct effects of GLP-1 receptor activation in the brain.
What the clinical research actually shows
Let us look at the data specifically relevant to perimenopausal and menopausal women. The research is growing, and the findings deserve careful attention.
The Menopause journal study on semaglutide and HRT
A pivotal study published in the journal Menopause examined weight loss responses to semaglutide in postmenopausal women with and without concurrent hormone therapy use. The results were striking. Women using hormone therapy alongside semaglutide achieved approximately 30% more weight loss than those using semaglutide alone. At the 12-month mark, women on hormone therapy reached 16% total body weight loss, comparable to the weight loss seen in the major pivotal trials for semaglutide.
This is a significant finding. It suggests that replacing the declining estrogen through hormone therapy may restore some of the metabolic environment in which semaglutide works most effectively. The combination of HRT and GLP-1 therapy is an area of active research and represents a potentially powerful approach for perimenopausal women.
Low-dose semaglutide efficacy in menopausal women
A study published in Metabolic Syndrome and Related Disorders specifically examined low-dose semaglutide (1 mg) in menopausal women. After four months, participants showed significant reductions in both total body weight and fat mass. The study noted that fat mass loss was proportionally similar to what premenopausal women achieved, despite the metabolic disadvantages of the menopausal transition.
This is encouraging because it means lower doses of semaglutide may still be effective for this population, potentially reducing the side effect burden while delivering meaningful results.
The STEP trials and female subgroup analysis
The landmark STEP trials demonstrated that adults receiving weekly 2.4 mg semaglutide injections for approximately 15 months lost an average of 15% of their body weight, compared to 2.4% in the placebo group. Subgroup analyses from these trials confirmed that semaglutide produced clinically meaningful weight loss in female participants regardless of menopausal status. A presentation at the Obesity Society conference further validated these findings across different menopausal groups.
The data is clear. Semaglutide works for weight loss during perimenopause and menopause. The question is not whether it works, but how to optimize its use within the context of hormonal transition.
Semaglutide dosing considerations for perimenopausal women
Dosing semaglutide during perimenopause follows the same general titration schedule used for all patients, but there are specific considerations that matter for this population.
Standard titration protocol
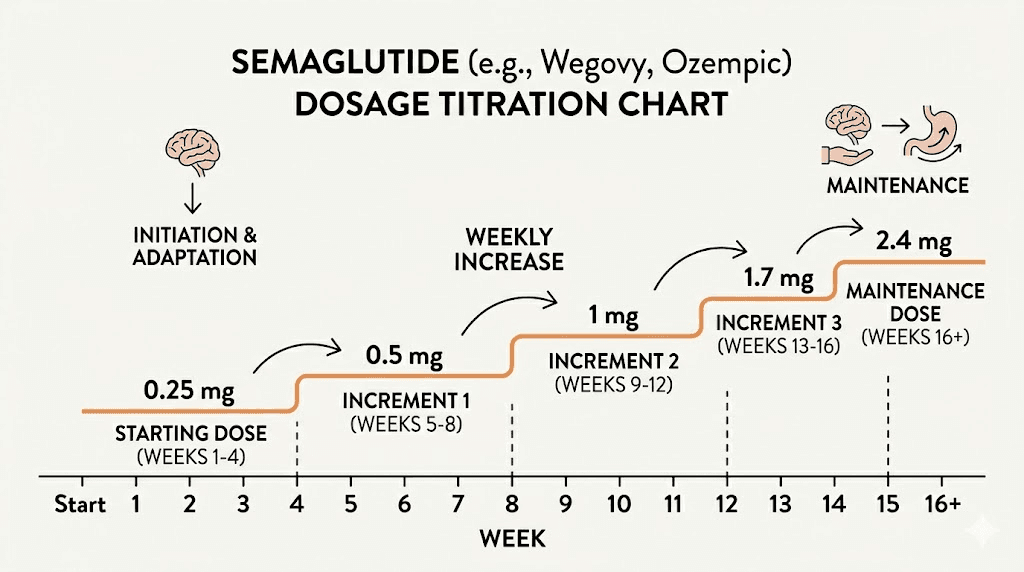
The standard approach starts low and increases gradually to minimize gastrointestinal side effects:
Weeks 1 through 4: 0.25 mg once weekly. This is the tolerance-building phase. Most women experience minimal side effects at this dose, though some notice mild nausea. The appetite-suppressing effects may be subtle but present.
Weeks 5 through 8: 0.5 mg once weekly. Appetite suppression becomes more noticeable. Many women report a significant reduction in food noise during this phase. Appetite changes typically become more pronounced here.
Weeks 9 through 12: 1.0 mg once weekly. This is where substantial weight loss acceleration often begins. The study in menopausal women showing comparable fat loss to premenopausal women used this 1 mg dose.
Weeks 13 through 16: 1.7 mg once weekly, if tolerated and if additional weight loss is desired.
Week 17 onward: 2.4 mg once weekly, the maximum therapeutic dose. Not all women need to reach this level. Some achieve excellent results at 1.0 or 1.7 mg.
You can use the SeekPeptides semaglutide dosage calculator to determine your exact unit measurements based on your vial concentration.
Perimenopause-specific dosing considerations
Perimenopausal women may experience more pronounced gastrointestinal side effects initially due to the existing hormonal influence on gut motility. Estrogen and progesterone affect gastric emptying rates, and the fluctuations of perimenopause can make bloating and nausea more variable.
Some practitioners recommend an extended titration for perimenopausal patients. Instead of increasing every four weeks, some women benefit from spending six to eight weeks at each dose level. This slower approach reduces side effects while still allowing the medication to build to therapeutic levels.
Timing relative to the menstrual cycle also matters. Some women find that semaglutide side effects are more intense during the luteal phase (the two weeks before menstruation) when progesterone is higher and gut motility naturally slows. Adjusting injection day to fall during the follicular phase (the two weeks after menstruation) may help reduce overlapping GI symptoms.
When to consider dose adjustments
Perimenopausal women should monitor their response carefully. If weight loss stalls after initial progress, it may indicate hormonal shifts rather than semaglutide failure. Estrogen fluctuations can cause temporary water retention and metabolic slowdowns that mask ongoing fat loss. Measuring waist circumference and body composition, not just scale weight, gives a more accurate picture of progress.
If you hit a semaglutide plateau, consider whether the timing coincides with hormonal shifts. Some women find that their weight loss follows a cyclical pattern during perimenopause, with more loss in some weeks and temporary stalls in others.
The semaglutide and hormone therapy synergy
The research on combining semaglutide with hormone replacement therapy deserves its own section because the implications are significant for perimenopausal women considering their options.
Why HRT amplifies semaglutide results
Estrogen replacement restores insulin sensitivity. When you add semaglutide to a body that has regained some of its estrogen-mediated metabolic function, the GLP-1 receptor agonist works in a more favorable metabolic environment. Think of it this way: semaglutide is a powerful tool, but it works best when the underlying hormonal foundation supports its mechanisms.
The study showing 30% more weight loss with HRT combination suggests that estrogen replacement addresses the metabolic resistance that would otherwise partially blunt semaglutide effects. Women on hormone therapy with GLP-1 medications also reported better mood, sleep quality, and energy levels, all factors that support sustainable weight management.
Estrogen types and delivery methods that matter
Not all hormone therapy is equal in this context. Transdermal estradiol (patches, gels, or sprays) avoids the first-pass liver metabolism that oral estrogens undergo. This is relevant because oral estrogens can affect liver-produced proteins involved in metabolism and may increase triglycerides, potentially interacting with semaglutide gastrointestinal effects.
Bioidentical progesterone (micronized progesterone) is generally preferred over synthetic progestins for women with an intact uterus. Some synthetic progestins can worsen insulin resistance, which would partially counteract the metabolic benefits of both HRT and semaglutide.
Timing and coordination
Starting HRT and semaglutide simultaneously can make it difficult to distinguish which is causing which effects, both positive and negative. Many practitioners recommend establishing one therapy first, typically HRT for at least two to three months, before adding semaglutide. This allows the hormonal environment to stabilize before introducing the GLP-1 agonist.
However, women already on stable HRT who add semaglutide often see accelerated results compared to women starting semaglutide alone. The combination addresses perimenopausal weight gain from multiple angles: hormonal restoration, appetite regulation, insulin sensitivity improvement, and metabolic optimization.
Managing side effects during perimenopause
The side effect profile of semaglutide does not fundamentally change during perimenopause, but certain side effects may feel more intense or overlap with perimenopausal symptoms.
Gastrointestinal effects
Nausea is the most common semaglutide side effect, reported by approximately 44% of users in clinical trials. During perimenopause, GI sensitivity may already be heightened due to hormonal fluctuations. Constipation, another common side effect, can worsen during the luteal phase when progesterone naturally slows gut transit.
Practical management strategies include eating smaller, more frequent meals, avoiding high-fat foods immediately after injection, staying well hydrated, and considering a quality probiotic to support gut health during both transitions. Some women find that acid reflux worsens on semaglutide, particularly during perimenopause when reflux is already more common.
Fatigue and energy changes
Fatigue on semaglutide can overlap with perimenopausal fatigue in confusing ways. Reduced caloric intake from semaglutide appetite suppression can lower energy, especially in the first few weeks. Combined with the sleep disruptions and energy fluctuations of perimenopause, some women feel significantly more tired during the initial adjustment period.
The solution is not to push through on willpower. Adequate protein intake is essential, aiming for 1.0 to 1.2 grams per kilogram of body weight daily. Understanding caloric needs on semaglutide prevents excessive restriction that worsens fatigue. Nutrient-dense foods become even more important when appetite is reduced and the body is already under hormonal stress.
Mood and cognitive effects
Perimenopause is already associated with mood changes, brain fog, and increased anxiety for many women. Semaglutide effects on brain GLP-1 receptors are being actively researched, with some evidence suggesting improvements in mood and cognitive function. However, the caloric restriction that comes with reduced appetite can temporarily worsen brain fog if blood sugar drops too low.
Maintaining steady blood sugar through regular, balanced meals and adequate protein helps mitigate this. Some women report that once they adjust to semaglutide, their brain fog actually improves, possibly because reduced blood sugar spikes and crashes lead to more stable cognitive function throughout the day.
Hair thinning concerns
Rapid weight loss from any cause can trigger telogen effluvium, a temporary shedding of hair that typically begins two to three months after significant weight loss begins. Perimenopause already increases the risk of hair changes due to shifting estrogen and testosterone ratios. The combination of rapid semaglutide-driven weight loss and perimenopausal hormonal changes means hair thinning deserves attention.
Adequate protein intake, iron levels, and biotin supplementation can help. A slower rate of weight loss, achieved through lower semaglutide doses, reduces the risk of significant hair shedding. Most women who experience telogen effluvium see regrowth within six to twelve months as the body adjusts to its new weight.
Bone density considerations
Estrogen decline during perimenopause accelerates bone loss. Rapid weight loss, regardless of method, can further reduce bone density because the mechanical load on bones decreases. This makes bone health monitoring particularly important for perimenopausal women on semaglutide.
Weight-bearing exercise, adequate calcium (1,200 mg daily for women over 50), vitamin D (at least 1,000 IU daily), and monitoring through DEXA scans help protect bone health. If you are taking supplements with your GLP-1 medication, calcium and vitamin D should be priorities for perimenopausal women.
Muscle preservation during perimenopausal weight loss
This is arguably the most important and most overlooked aspect of using semaglutide during perimenopause. Muscle loss accelerates during the menopausal transition due to declining estrogen and testosterone. Semaglutide-driven weight loss, if not managed carefully, can compound this problem.
The muscle loss math
In the STEP trials, approximately 30 to 40% of weight lost on semaglutide was lean mass (including muscle). For a woman losing 30 pounds, that could mean 9 to 12 pounds of muscle loss. During perimenopause, when muscle is already declining at approximately 3 to 8% per decade after age 30 (accelerating during the menopausal transition), this additional loss is concerning.
Sarcopenia, the age-related loss of muscle mass and function, is a significant health risk for women post-menopause. It reduces metabolic rate, increases fall risk, worsens insulin resistance, and diminishes quality of life. Any weight loss strategy during perimenopause must actively counteract muscle loss.
The resistance training requirement
Resistance training is not optional for perimenopausal women on semaglutide. It is a medical necessity. Progressive resistance training two to three times per week has been shown to preserve and even build muscle mass during weight loss. The exercises do not need to be complicated. Compound movements like squats, deadlifts, rows, and presses stimulate the most muscle groups efficiently.
Research shows that combining GLP-1 medications with structured resistance training significantly improves the ratio of fat loss to muscle loss. Women who train while using semaglutide lose proportionally more fat and less muscle than those who rely on the medication alone. Building muscle while on GLP-1 medications is absolutely possible with the right approach.
Protein requirements increase
The standard protein recommendation of 0.8 grams per kilogram of body weight is insufficient for perimenopausal women losing weight on semaglutide. Current research supports 1.2 to 1.6 grams per kilogram, with some experts recommending even higher intakes for women over 40 actively trying to preserve muscle. Protein intake on semaglutide requires deliberate planning because reduced appetite makes it easy to under-eat protein.
Distributing protein across three to four meals of at least 25 to 30 grams each optimizes muscle protein synthesis. Protein shakes can help fill gaps when appetite is low, but whole food protein sources should make up the majority of intake.
Creatine as a complementary supplement
Creatine supplementation alongside semaglutide has gained attention for its potential to support muscle preservation. Creatine monohydrate at 3 to 5 grams daily supports muscle energy production and may help maintain strength during caloric deficit. For perimenopausal women, creatine also shows emerging evidence of supporting cognitive function, a welcome bonus during a time when brain fog is common.
Nutrition strategies for semaglutide during perimenopause
When appetite is reduced and nutritional demands are heightened by both hormonal transition and weight loss, every bite counts. The standard advice to just eat healthy is not specific enough.
Priority nutrients for perimenopausal women on semaglutide
Protein sits at the top. We have covered why. But several other nutrients deserve attention.
Calcium and vitamin D protect bones during a time of accelerated bone loss. Dairy products, fortified foods, sardines, and leafy greens contribute calcium. Vitamin D supplementation is almost universally recommended because food sources rarely provide adequate amounts.
Omega-3 fatty acids support cardiovascular health (increasingly important as estrogen cardioprotective effects decline) and may help reduce the inflammation associated with both perimenopause and visceral fat. Fatty fish twice weekly or a quality fish oil supplement covers this need.
Fiber becomes especially important on semaglutide due to the tendency toward constipation. Aim for 25 to 30 grams daily from vegetables, fruits, legumes, and whole grains. Managing constipation on GLP-1 medications often starts with adequate fiber and hydration.
Iron deserves monitoring, especially for women still menstruating (which you are during perimenopause). Irregular and sometimes heavy periods during this transition can deplete iron stores. Reduced appetite from semaglutide may further limit iron intake.
Meal timing and structure
Three to four small meals tend to work better than the traditional three large meals for perimenopausal women on semaglutide. Smaller portions are better tolerated given the slowed gastric emptying, and more frequent protein distribution supports muscle preservation. Planning a complete diet approach prevents the nutritional gaps that lead to fatigue and muscle loss.
Breakfast should prioritize protein and healthy fats. A protein-rich morning meal stabilizes blood sugar and supports the metabolic foundation for the day. Evening meals should be lighter but still include adequate protein, as overnight muscle protein synthesis is important for preservation.
Some women on semaglutide skip meals entirely because they simply are not hungry. During perimenopause, this is risky. Undereating, even unintentionally, accelerates muscle loss, worsens fatigue, and can disrupt already-unstable hormones. If appetite is extremely suppressed, nutrient-dense smoothies and GLP-1 friendly recipes can help meet minimum nutritional needs.
Foods to prioritize and avoid
Prioritize: lean proteins, fatty fish, eggs, Greek yogurt, berries, leafy greens, cruciferous vegetables (which support estrogen metabolism), nuts, seeds, and legumes. The complete food list for semaglutide provides detailed options, but perimenopausal women should emphasize phytoestrogen-containing foods like flaxseeds and soy, which provide mild estrogenic support.
Foods to avoid on semaglutide include highly processed items, excessive sugar, fried foods, and alcohol. Alcohol deserves special mention because it worsens hot flashes, disrupts sleep, impairs liver metabolism of hormones, and can intensify semaglutide nausea. Understanding alcohol and semaglutide interactions is important for all users, but particularly for perimenopausal women already dealing with sleep and thermoregulation challenges.
The gut-hormone axis during perimenopause
The gastrointestinal system and the hormonal system communicate constantly through what researchers call the gut-hormone axis. During perimenopause, this communication becomes disrupted in ways that directly affect how semaglutide works and why it can be particularly beneficial.
Estrogen and the gut microbiome
Your gut microbiome contains a collection of bacteria collectively called the estrobolome, microbes that metabolize estrogen. As estrogen levels fluctuate during perimenopause, the estrobolome is affected, which in turn impacts estrogen recycling and elimination. This creates a feedback loop where hormonal changes alter gut bacteria, which further disrupts hormonal balance.
Semaglutide slows gastric emptying and changes gut transit time, which can shift the composition of the gut microbiome. While research on this interaction is still early, some preliminary evidence suggests that the gut microbiome changes associated with GLP-1 therapy may actually support healthier estrogen metabolism. A quality probiotic may complement this effect by supporting beneficial bacterial populations.
Gut motility changes compound during perimenopause
Progesterone naturally slows gut motility. During the luteal phase of the menstrual cycle (and particularly during early perimenopause when progesterone levels are still fluctuating), many women experience constipation and bloating. Semaglutide also slows gastric emptying. The combination can make GI side effects more pronounced during certain phases of the perimenopausal cycle.
This is why timing matters. Women who inject semaglutide during the follicular phase (when progesterone is lowest) often report fewer GI complaints than those who inject during the luteal phase. Tracking your cycle, even when it is irregular, can help optimize your injection timing and reduce the overlap of gut-slowing effects.
Fiber supplementation, adequate hydration (aim for at least 64 ounces of water daily, more if you are active), and movement after meals all help counteract the doubled gut-slowing effect. Magnesium citrate in the evening can address both constipation and the magnesium deficiency that is common during perimenopause.
Bile acid changes and fat digestion
Estrogen influences bile acid production and composition. During perimenopause, changes in bile acids can affect fat digestion and absorption, contributing to the bloating and digestive discomfort many women experience. Semaglutide effect on the GI tract interacts with these bile acid changes, which is one reason some perimenopausal women experience more acid reflux or sulfur burps than younger users.
Eating smaller, more frequent meals with moderate fat content (rather than large, high-fat meals) helps manage this. Bile acids adapt to dietary patterns, and consistent eating schedules help maintain more predictable digestion even amid hormonal chaos.
Semaglutide versus tirzepatide for perimenopause
Women navigating perimenopausal weight gain often ask whether semaglutide or tirzepatide is the better choice. Both are GLP-1 receptor agonists, but tirzepatide also activates GIP receptors, making it a dual agonist.
Head-to-head comparison for perimenopausal women
Factor | Semaglutide | Tirzepatide |
|---|---|---|
Mechanism | GLP-1 agonist only | GLP-1 + GIP dual agonist |
Average weight loss | 15-16% body weight | 20-22% body weight |
Insulin sensitivity | Significant improvement | Greater improvement (dual mechanism) |
Research in menopausal women | More published data | Less menopause-specific data |
HRT synergy data | Published research available | Limited data |
GI side effects | 44% nausea rate | Similar nausea profile |
Muscle preservation | Similar lean mass loss ratio | Similar lean mass loss ratio |
Tirzepatide produces greater average weight loss in clinical trials. Its dual mechanism may offer advantages for perimenopausal women with significant insulin resistance. However, semaglutide has more published research specifically in menopausal populations, particularly regarding the HRT combination data. The side effect profiles differ somewhat, and individual tolerance varies.
For women who do not respond adequately to semaglutide, switching to tirzepatide is a reasonable option. The conversion chart between the two medications helps guide dose translation.
Retatrutide as a future option
Looking ahead, retatrutide represents the next generation of weight loss peptides. As a triple agonist (GLP-1, GIP, and glucagon receptors), it has produced even greater weight loss in clinical trials, with some participants losing over 24% of body weight. While not yet approved, it is in active development and may eventually offer perimenopausal women another powerful option.
Lifestyle factors that amplify semaglutide results during perimenopause
Semaglutide is not a standalone solution. For perimenopausal women, the lifestyle foundations become even more important than for younger users.
Exercise beyond resistance training
We covered resistance training for muscle preservation. But cardiovascular exercise and flexibility work also matter during perimenopause. Exercise on semaglutide should include a mix of strength training (two to three times weekly), moderate cardio (150 minutes weekly), and flexibility or balance work (two to three times weekly).
Walking is underrated. A daily 30-minute walk improves insulin sensitivity, supports cardiovascular health, reduces cortisol, and does not require recovery time that might interfere with resistance training. For perimenopausal women on semaglutide, this combination of structured exercise and daily movement creates a foundation for sustainable weight management.
High-intensity interval training (HIIT) deserves careful consideration during perimenopause. While effective for fat loss, excessive HIIT can elevate cortisol and worsen the adrenal stress that many perimenopausal women already experience. Two sessions per week is generally the maximum recommended, with adequate recovery between sessions. Low-impact options like swimming, cycling, or elliptical training provide cardiovascular benefits with less joint stress, which matters as estrogen-related joint protection declines.
Yoga and tai chi offer unique benefits for this population. Both reduce cortisol, improve balance (reducing fall risk as bone density changes), support sleep quality, and provide the stress management that is so critical during hormonal transition. Some research suggests yoga may even help moderate hot flash frequency and severity, complementing the indirect thermoregulatory benefits of semaglutide-driven weight loss.
Sleep optimization
Poor sleep is both a symptom of perimenopause and a driver of weight gain. Night sweats, insomnia, and disrupted sleep architecture all worsen during this transition. Semaglutide may help some women sleep better by reducing sleep apnea symptoms associated with excess weight, but it does not directly address hormonal sleep disruption.
Sleep hygiene becomes critical: consistent bedtime, cool bedroom temperature (especially important for hot flashes), limiting screens before bed, and considering magnesium glycinate supplementation, which supports both sleep and muscle function. Understanding the relationship between semaglutide and sleep helps distinguish medication effects from perimenopausal symptoms.
Stress management
Cortisol is the enemy of perimenopausal weight loss. Chronic stress elevates cortisol, which promotes visceral fat storage, worsens insulin resistance, increases appetite, and disrupts sleep. Semaglutide cannot override a chronically stressed system.
Practical stress management for perimenopausal women includes regular movement, mindfulness practices (even 10 minutes daily shows measurable cortisol reduction), social connection, and boundaries around energy expenditure. Many women in perimenopause are in their peak career and caregiving years, making stress reduction a practical challenge that requires deliberate prioritization.
Body composition versus scale weight during perimenopause
This distinction is critical and frequently misunderstood. During perimenopause, the scale is an unreliable measure of progress for several reasons.
Why the scale lies during perimenopause
Hormonal fluctuations cause significant water retention changes. Estrogen spikes (which happen unpredictably during perimenopause) increase water retention. A woman can gain three to five pounds of water weight overnight during an estrogen surge, completely masking a week of fat loss. This leads to frustration and the false conclusion that semaglutide is not working.
Additionally, if you are building muscle through resistance training while losing fat on semaglutide, the scale may not change much even as your body composition transforms dramatically. A woman who loses five pounds of fat and gains three pounds of muscle has only lost two pounds on the scale but has made significant health and metabolic improvements.
Better measures of progress
Track waist circumference. Visceral fat reduction shows up here before it shows on the scale. A loss of even one to two inches at the waist represents meaningful visceral fat reduction.
Track how clothes fit. This subjective measure often captures body composition changes that the scale misses.
Consider body composition testing. DEXA scans provide accurate measurements of fat mass, lean mass, and bone density. For perimenopausal women, DEXA scans serve the dual purpose of tracking weight loss progress and monitoring bone density.
Track energy levels, sleep quality, and mood. These markers often improve before scale weight changes and indicate that semaglutide and lifestyle modifications are working at the metabolic level.
When semaglutide might not be the right choice during perimenopause
Semaglutide is not appropriate for every perimenopausal woman. Several factors warrant careful consideration.
Contraindications and cautions
Women with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 should not use semaglutide. Those with a history of pancreatitis should use it with caution. Cardiovascular considerations should be discussed with a healthcare provider, particularly for women with existing risk factors that may be amplified by the cardiovascular changes of perimenopause.
Women with a history of eating disorders require careful evaluation. Semaglutide powerful appetite suppression can be problematic for those with restrictive eating patterns. During perimenopause, when body image concerns and mood instability may already be elevated, this risk deserves thoughtful discussion.
When underlying issues need addressing first
Thyroid dysfunction is common during perimenopause and causes weight gain independent of caloric intake. Hashimoto thyroiditis and GLP-1 medications can interact, and undiagnosed hypothyroidism should be treated before attributing weight gain solely to perimenopause or expecting semaglutide to compensate.
Severe sleep disorders, unmanaged depression, and significant nutritional deficiencies all impair semaglutide effectiveness and may need to be addressed as foundational steps before starting GLP-1 therapy.
Cost and sustainability considerations
Semaglutide is not a short-term solution. Research consistently shows that stopping semaglutide leads to weight regain for most users. For perimenopausal women, this raises questions about long-term commitment and cost planning. Understanding how long to stay on semaglutide requires weighing the metabolic benefits against practical considerations.
Some women use semaglutide during the most metabolically challenging phase of perimenopause and then transition to a maintenance dose or taper off as they establish new lifestyle habits and potentially begin HRT. This approach treats semaglutide as a bridge rather than a permanent commitment.
Practical protocols for perimenopausal women
Based on the research and clinical experience, here are two evidence-based approaches.
Protocol 1: Semaglutide alone (no HRT)
Goal: Weight loss and metabolic improvement without hormone therapy
Dosing: Standard titration (0.25 mg increasing to tolerance), consider extended titration if GI symptoms are significant
Nutrition: 1.2 to 1.4 g protein per kg body weight, 25 to 30 g fiber daily, calcium 1,200 mg, vitamin D 1,000 to 2,000 IU, omega-3 supplementation
Exercise: Resistance training 2 to 3 times weekly, 150 minutes moderate cardio weekly, daily walking
Monitoring: Monthly waist circumference, quarterly bloodwork (fasting insulin, HbA1c, lipids, thyroid, iron), annual DEXA scan
Expected results: 10 to 15% body weight loss over 12 months, improved insulin sensitivity, reduced visceral fat
Timeline: Appetite suppression weeks 1 to 2, noticeable weight loss by week 4 to 6, significant results by month 3 to 4
Protocol 2: Semaglutide with HRT (optimized approach)
Goal: Maximum weight loss with comprehensive hormonal support
Step 1: Begin HRT under medical supervision (transdermal estradiol plus micronized progesterone if uterus intact)
Step 2: After 2 to 3 months on stable HRT, begin semaglutide titration
Dosing: Standard titration, potentially achieving results at lower maximum doses due to improved metabolic environment
Nutrition: 1.2 to 1.6 g protein per kg body weight, all supplements from Protocol 1, phytoestrogen-rich foods
Exercise: Same as Protocol 1, with added emphasis on high-impact exercise for bone health (if appropriate)
Monitoring: Same as Protocol 1, plus hormone levels (estradiol, progesterone, FSH) quarterly
Expected results: 15 to 20% body weight loss over 12 months, improved body composition, better sleep, mood stability, reduced hot flashes
Both protocols require regular medical supervision. Healthcare providers recommend check-ins every two to three months to monitor progress, adjust doses, and screen for complications.
Real expectations and timelines
Setting accurate expectations prevents the frustration that leads many women to abandon effective treatment prematurely.
Month-by-month guide
Month 1: Reduced appetite, possible nausea and GI adjustment, minimal scale change (0 to 3 pounds). Some women notice reduced food noise almost immediately. Others need more time. The first week on semaglutide varies enormously between individuals.
Month 2: Appetite suppression more consistent, weight loss becoming visible (3 to 7 pounds total). GI side effects typically improving. Energy may still be adjusting.
Month 3: Noticeable body composition changes, clothes fitting differently, 5 to 10% of the eventual weight loss achieved. Early results become motivating.
Months 4 through 6: Accelerated fat loss phase, particularly if dose has been titrated to therapeutic levels. Waist circumference decreasing. Energy often improving as the body adapts. This is when the before-and-after transformation becomes evident.
Months 6 through 12: Continued fat loss at a potentially slower rate. Body composition continuing to improve with consistent resistance training. Metabolic markers (blood sugar, insulin, lipids) showing significant improvement.
Month 12 onward: Approaching maximum weight loss for most women. The focus shifts to maintenance, body composition optimization, and sustainable lifestyle habits.
The perimenopause wild card
Hormonal fluctuations during perimenopause make this timeline more variable than for premenopausal women. Expect weeks where the scale goes up despite doing everything right. Expect periods (sometimes literally) where water retention masks fat loss. Expect that some months will show dramatic progress and others will feel like nothing is happening.
This variability does not mean semaglutide is failing. It means perimenopause is adding noise to the signal. Track trends over months, not weeks. The overall trajectory matters far more than any individual weigh-in.
Semaglutide and specific perimenopausal symptoms
Beyond weight loss, semaglutide may influence several common perimenopausal symptoms.
Hot flashes
Some preliminary evidence suggests that weight loss itself reduces hot flash frequency and severity. Visceral fat acts as an insulator and disrupts thermoregulation. As semaglutide reduces visceral fat, some women report improvement in vasomotor symptoms. However, this is an indirect effect of weight loss rather than a direct pharmacological action of semaglutide.
Joint pain
Perimenopausal women often develop new joint pain due to declining estrogen effects on cartilage and inflammation. Weight loss from semaglutide reduces mechanical stress on joints. For every pound lost, the force on the knee during walking decreases by approximately four pounds. A 20-pound weight loss translates to 80 pounds less force with every step.
Cardiovascular risk
Estrogen is cardioprotective. As it declines during perimenopause, cardiovascular risk increases. Semaglutide has demonstrated cardiovascular benefits independent of weight loss in the SELECT trial, including reduced rates of major adverse cardiovascular events. For perimenopausal women whose cardiovascular risk is rising due to hormonal changes, this additional benefit is meaningful.
Mood and anxiety
The relationship between semaglutide and mood during perimenopause is complex. Weight loss itself improves mood and self-esteem for many women. The reduction in food preoccupation frees mental bandwidth. However, the caloric restriction and rapid hormonal adjustments can temporarily worsen anxiety in some individuals. Monitoring mood and having open conversations with healthcare providers helps navigate this nuanced territory.
Semaglutide delivery options for perimenopausal women
Semaglutide is available in multiple formats, and the choice of delivery method matters more during perimenopause than many realize.
Injectable semaglutide
Subcutaneous injection remains the most common and most studied delivery method. Weekly injections are administered in the abdomen, thigh, or upper arm. For perimenopausal women, the injection site can affect absorption rates slightly. Abdominal injections are typically absorbed most consistently, while thigh injections may be absorbed more slowly. Rotating sites prevents lipodystrophy (localized fat changes at injection sites).
Many women find that the injection process becomes routine within two to three weeks. If needle anxiety is a concern, learning proper technique with insulin syringes provides finer dose control than auto-injector pens, which is valuable during the titration phase when smaller dose adjustments may be needed.
Oral semaglutide
Oral semaglutide drops and sublingual semaglutide offer needle-free alternatives. However, oral bioavailability is significantly lower than injectable, meaning higher doses are needed to achieve equivalent blood levels. For perimenopausal women who need precise dosing and predictable absorption, injectable semaglutide generally provides more consistent results.
Semaglutide troches are another option available through compounding pharmacies. These dissolve in the mouth and absorb through the oral mucosa. Some women prefer this approach for its simplicity, though absorption can be variable depending on technique and individual factors.
Compounded versus brand-name semaglutide
Compounded semaglutide is available at a fraction of the cost of brand-name options. For perimenopausal women who may be on treatment for an extended period, cost is a legitimate factor. Compounded formulations are available from 503B compounding pharmacies and may include added ingredients like vitamin B12, glycine, or niacinamide.
B12 supplementation is particularly relevant for perimenopausal women because B12 deficiency becomes more common with age, and methylcobalamin (active B12) supports energy production, neurological function, and mood, all of which are already under stress during the menopausal transition. A compounded semaglutide with B12 addresses two common perimenopausal needs in a single injection.
Understanding the compounded semaglutide dosage chart and proper reconstitution procedures is essential for compounded formulations. The semaglutide dosage calculator on SeekPeptides helps with the math.
Preparing to start semaglutide during perimenopause
If you are considering semaglutide during perimenopause, preparation improves outcomes.
Baseline testing
Before starting, get comprehensive bloodwork: fasting glucose, fasting insulin, HbA1c, complete thyroid panel (TSH, free T4, free T3, thyroid antibodies), complete metabolic panel, lipid panel, iron studies, vitamin D, and complete blood count. For perimenopausal women, add FSH, estradiol, and progesterone to understand your current hormonal status.
A baseline DEXA scan establishes starting bone density and body composition measurements against which future changes can be tracked.
Setting up your support system
Find a healthcare provider who understands both GLP-1 therapy and menopause management. These are often different specialists, and coordination between them improves outcomes. Consider whether qualifying for semaglutide through your insurance or exploring compounded options through a compounding pharmacy better fits your situation.
Learn how to properly administer injections. Understanding injection site selection and injection technique reduces anxiety around the process. The timing of your injection can also affect side effect management.
Storage and handling
Proper storage preserves potency. Understand how long semaglutide lasts in the refrigerator and what happens if it gets warm. If you travel, a travel guide for semaglutide helps maintain the cold chain and keep your medication effective.
SeekPeptides members access detailed storage protocols, reconstitution guides, and dosing tools designed to take the guesswork out of peptide management. For perimenopausal women juggling multiple health considerations, having reliable reference materials makes the process considerably less overwhelming.
Common mistakes perimenopausal women make with semaglutide
Knowing what not to do is as valuable as knowing the right approach. These mistakes are common and avoidable.
Mistake 1: Relying on the scale as the primary measure
We covered this above, but it bears repeating because it is the number one reason women abandon effective treatment prematurely. Hormonal water retention during perimenopause can mask weeks of genuine fat loss. A woman losing half a pound of fat per week while retaining two pounds of hormonally-driven water will see the scale go up and conclude semaglutide has stopped working. It has not. Track waist circumference, body composition, and how clothes fit. These measures tell the truth when the scale lies.
Mistake 2: Eating too little protein
When appetite drops on semaglutide, many women eat whatever sounds good in the moment, which is usually not protein. They end up consuming 40 to 60 grams of protein daily when they need 90 to 120 grams or more. The result is accelerated muscle loss that worsens the metabolic slowdown perimenopause already initiates. Plan protein first at every meal. If you can only eat one thing, make it protein. Tracking protein intake for even a few weeks establishes the habits that protect muscle long-term.
Mistake 3: Skipping resistance training
Cardio feels productive. You sweat, your heart rate rises, you feel like you did something. But for perimenopausal women on semaglutide, resistance training is non-negotiable. Without it, you will lose muscle along with fat, your metabolism will slow further, and you will end up at a lower weight but with a worse body composition and lower metabolic rate than before. Two to three sessions per week of progressive resistance training is the minimum. This does not mean light dumbbells. It means challenging weight that you struggle to complete by the final rep.
Mistake 4: Ignoring sleep
Sleep is when your body repairs, builds muscle, regulates hormones, and processes fat. Perimenopausal sleep disruption is common and often dismissed as something to push through. But chronic sleep deprivation of even one to two hours per night increases cortisol by 37%, reduces insulin sensitivity by 25%, and increases hunger hormones dramatically. Semaglutide cannot overcome these effects. Prioritize sleep hygiene, consider melatonin or magnesium supplementation, and address hot flashes through cooling strategies or HRT if appropriate.
Mistake 5: Starting semaglutide without baseline bloodwork
Without baseline numbers, you cannot measure progress beyond scale weight. More importantly, you cannot identify underlying conditions that need treatment first. Undiagnosed hypothyroidism, iron deficiency anemia, vitamin D deficiency, and pre-diabetes all affect how you respond to semaglutide. Get the bloodwork done before your first injection. It turns your treatment from guesswork into science.
Mistake 6: Comparing your results to younger users
The timeline and trajectory of semaglutide results during perimenopause will not match what a 28-year-old with straightforward excess weight experiences. The hormonal complexity adds variability. The metabolic resistance adds time. The competing demands on your body add complications. Your results are valid even if they are slower or more irregular than someone else. Consistency over months matters more than speed over weeks.
Mistake 7: Neglecting electrolyte balance
Reduced food intake on semaglutide, combined with the fluid shifts of perimenopause, can deplete electrolytes. Magnesium, potassium, and sodium all need attention. Symptoms like leg cramps, dizziness, and lightheadedness are often electrolyte issues rather than semaglutide side effects per se. A quality electrolyte supplement, particularly one with magnesium glycinate, can resolve these issues quickly.
Blood testing and monitoring during treatment
Perimenopausal women on semaglutide benefit from more comprehensive monitoring than the general population. Here is what to track and when.
Baseline panel (before starting semaglutide)
Complete metabolic panel, fasting glucose, fasting insulin, HbA1c, lipid panel, complete thyroid panel (TSH, free T4, free T3, anti-TPO antibodies), iron studies (ferritin, serum iron, TIBC), vitamin D 25-hydroxy, complete blood count, liver enzymes, kidney function markers, FSH, estradiol, and progesterone.
Three-month check
Repeat fasting glucose, fasting insulin, HbA1c, lipid panel, liver enzymes, and complete metabolic panel. Compare to baseline to assess metabolic improvement. If liver enzymes are elevated, this needs evaluation before continuing titration.
Six-month comprehensive panel
Full repeat of the baseline panel, including hormonal markers. This is important because perimenopausal hormone levels shift over time, and what was normal at baseline may have changed. Thyroid function should be rechecked because both semaglutide-driven weight loss and perimenopausal changes can affect thyroid requirements.
Annual assessment
Full bloodwork plus DEXA scan for bone density and body composition. The DEXA scan is arguably the most valuable monitoring tool for perimenopausal women on semaglutide because it tracks three critical variables simultaneously: fat mass, lean mass, and bone density. All three are in flux during this life stage, and knowing exactly what is happening with each allows for targeted adjustments to exercise, nutrition, and supplementation.
The bigger picture: perimenopause as a metabolic reset opportunity
Here is a perspective that reframes the entire conversation. Perimenopause is disruptive. It is uncomfortable. It changes your body in ways you did not consent to. But it is also a window of opportunity.
The metabolic dysfunction that perimenopause exposes, the insulin resistance, the visceral fat accumulation, the muscle loss, these processes were happening slowly before perimenopause accelerated them. Estrogen was masking some of the metabolic damage from years of suboptimal sleep, chronic stress, and sedentary patterns. Perimenopause pulls back the curtain.
Semaglutide, combined with the right lifestyle modifications, can help you not just lose weight but fundamentally improve your metabolic health at a critical juncture. The habits you build now, the muscle you preserve, the insulin sensitivity you restore, the bone density you protect, these investments compound for decades.
Women who navigate perimenopause with deliberate metabolic optimization often emerge healthier than they were in their thirties. Not in spite of the transition, but because it forced them to address issues that would have worsened silently for years.
For researchers and women serious about making the most of this window, SeekPeptides provides evidence-based protocols, community support from women navigating similar transitions, and expert-reviewed guidance that accounts for the complexity of hormonal health and peptide science working together.
Frequently asked questions
Does semaglutide work less effectively during perimenopause?
No. Research shows that semaglutide produces comparable fat mass and weight loss in postmenopausal women as in premenopausal women after four months of treatment at 1 mg. The hormonal changes of perimenopause do not prevent semaglutide from working. However, the fluctuating hormones may cause more variable week-to-week results. Combining semaglutide with hormone therapy may enhance results by approximately 30%.
Can semaglutide help with hot flashes?
Indirectly, yes. Weight loss, particularly visceral fat reduction, has been associated with reduced frequency and severity of hot flashes in some studies. Semaglutide does not directly treat vasomotor symptoms, but the weight loss it facilitates may improve them. For direct hot flash treatment, hormone therapy remains the most effective option.
Will semaglutide make perimenopausal mood swings worse?
For most women, no. Many report improved mood as weight decreases and food preoccupation diminishes. However, the initial caloric reduction can temporarily affect mood and energy. Ensuring adequate nutrition, especially protein and complex carbohydrates, helps stabilize both blood sugar and mood. If you experience significant mood changes on semaglutide, discuss them with your healthcare provider.
Should I start HRT before or alongside semaglutide?
Starting HRT first (two to three months before semaglutide) is generally preferred. This allows your body to adjust to hormone replacement and establishes a more stable metabolic environment before adding semaglutide. Women already on stable HRT who add semaglutide often see better initial results than those starting both simultaneously.
How much muscle will I lose on semaglutide during perimenopause?
Without intervention, approximately 30 to 40% of weight lost on semaglutide may be lean mass. With progressive resistance training two to three times weekly and adequate protein intake (1.2 to 1.6 g per kg body weight), this ratio improves significantly. Building muscle while on GLP-1 medications is achievable with deliberate effort.
Is compounded semaglutide safe for perimenopausal women?
Compounded semaglutide is available through licensed compounding pharmacies. The safety profile depends on the pharmacy quality standards. Key considerations include proper reconstitution, appropriate storage, and working with a reputable provider. Compounded formulations sometimes include added B12 or glycine, which may offer additional benefits.
Can I take semaglutide if I am still having periods?
Yes. Perimenopause is defined by irregular cycles, not absence of periods. Semaglutide can be used during this transitional phase. However, be aware that semaglutide may affect menstrual cycles, and weight loss can increase fertility. If pregnancy is not desired, contraception remains important during perimenopause until menopause is confirmed (12 consecutive months without a period).
What happens if I stop semaglutide during perimenopause?
Research shows that most people regain weight after discontinuing semaglutide. During perimenopause, the metabolic challenges that contributed to weight gain remain, potentially making regain even more likely. Some women transition to a lower maintenance dose rather than stopping entirely. Others use the weight loss window to establish strong exercise and nutrition habits that partially buffer against regain.
External resources
In case I do not see you, good afternoon, good evening, and good night. May your hormones find balance, your metabolism find its rhythm, and your health find its strongest chapter yet.