Feb 3, 2026

Tired of conflicting information about peptides for mental health? One source says Selank is the answer. Another swears by PE-22-28. A third dismisses the entire category as unproven. You have read the forums, skimmed the studies, and walked away more confused than when you started. Here is what actually works, what the research genuinely supports, and what remains speculative. The gap between promising peptide research and practical mental health application is not as wide as most sources make it seem, but it is not as simple as picking a peptide and hoping for the best either. Depression and anxiety involve multiple overlapping systems in the brain, from neurotransmitter imbalances to chronic neuroinflammation to disrupted gut-brain signaling. Traditional medications target one pathway. Peptides, by their very nature, tend to influence several.
That multi-target approach is precisely what makes them interesting to researchers studying mood disorders, and it is also what makes the topic so difficult to navigate without a comprehensive guide. This resource covers every peptide with meaningful research behind its mental health applications, including specific mechanisms, dosage protocols from clinical and preclinical studies, stacking strategies, and the honest limitations of current evidence.
Whether you are exploring peptides for anxiety for the first time or looking to refine an existing protocol, SeekPeptides built this guide to be the most thorough reference available. No hype. No overselling. Just the science, the practical details, and the context you need to make informed decisions about peptide research for mental health.
What happens in the brain during depression and anxiety
Before exploring how peptides interact with mood disorders, it helps to understand what goes wrong in the brain when depression or anxiety takes hold. The old explanation was simple. Too little serotonin. Take an SSRI. Problem solved. But decades of research have revealed a far more complex picture, one involving at least five interconnected systems that all contribute to mental health dysfunction.
The neurotransmitter imbalance theory still holds partial truth. Serotonin, dopamine, GABA, and norepinephrine all play roles in mood regulation, and disruptions in any of these systems can produce symptoms of depression or anxiety. Low serotonin correlates with depressive symptoms and obsessive thinking. Reduced GABA activity leaves the brain in an overexcited state, driving anxiety and panic. Dopamine deficits rob a person of motivation and pleasure. But neurotransmitters are only one piece of the puzzle, and targeting them alone, as conventional approaches to brain function often do, leaves many people without adequate relief.
The HPA axis, your body stress response system, plays an equally critical role. When the hypothalamic-pituitary-adrenal axis becomes dysregulated, cortisol levels spike and stay elevated. Chronic cortisol exposure damages hippocampal neurons, shrinks brain volume in key regions, and disrupts sleep architecture. This creates a vicious cycle where stress damages the very brain structures needed to regulate stress.
Neuroinflammation has emerged as perhaps the most significant factor in treatment-resistant depression. Pro-inflammatory cytokines like TNF-alpha, IL-1beta, and IL-6 cross the blood-brain barrier, activate microglia, and directly interfere with neurotransmitter synthesis. Research shows that people with elevated inflammatory markers respond poorly to standard antidepressants. The connection between inflammation and mental health represents one of the most active areas of psychiatric research, and it is where several peptides show their most compelling mechanisms.
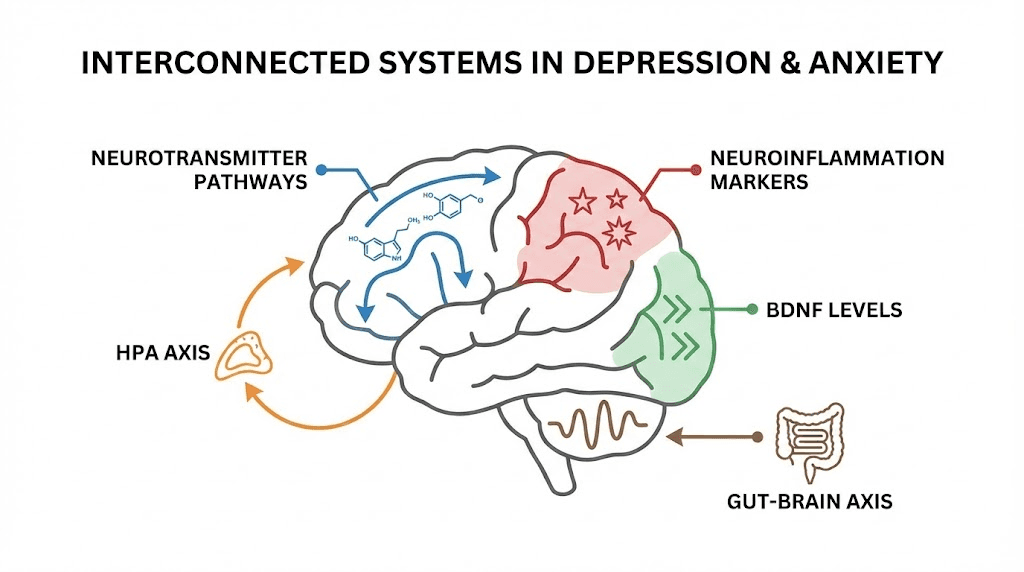
BDNF, brain-derived neurotrophic factor, acts as fertilizer for the brain. It promotes neurogenesis, strengthens synaptic connections, and supports neuronal survival. Depressed individuals consistently show reduced BDNF levels, particularly in the hippocampus and prefrontal cortex. Treatments that increase BDNF, whether pharmaceutical, behavioral, or peptide-based, tend to improve depressive symptoms. Several peptides discussed in this guide directly upregulate BDNF production, which partially explains their neurotrophic benefits.
The gut-brain axis adds yet another layer of complexity. Approximately 90% of the body serotonin is produced in the gut. Intestinal permeability, commonly called leaky gut, allows bacterial endotoxins into the bloodstream, triggering systemic inflammation that reaches the brain. Disrupted gut microbiome composition correlates strongly with both depression and anxiety. This is why peptides that heal the gut lining and reduce intestinal inflammation can produce unexpected improvements in mood, a connection explored extensively in gut health peptide research.
Understanding these five systems matters because it explains why single-target medications fail for so many people. And it reveals why peptides, which often influence multiple pathways simultaneously, have attracted serious research attention for mood disorders.
How peptides target depression and anxiety differently than traditional medications
Traditional antidepressants work by modifying a single neurotransmitter system. SSRIs block serotonin reuptake. SNRIs add norepinephrine to the equation. Benzodiazepines enhance GABA signaling. Each class picks one lock and turns one key. For many people, that is enough. For roughly 30% of depression patients, it is not.
Peptides operate differently.
Because peptides are short chains of amino acids that mimic natural signaling molecules, they tend to influence biological systems in ways that feel more native to the body. A peptide like Selank does not simply flood the brain with serotonin. It modulates GABA receptors allosterically, influences dopamine and serotonin receptor activity, enhances enkephalin levels, and reduces neuroinflammation, all through a single compound. That multi-pathway approach mirrors how the brain actually regulates mood, through coordinated activity across multiple systems rather than brute-force manipulation of one.
Side effect profiles in research also differ. Benzodiazepines produce sedation, cognitive impairment, physical dependence, and withdrawal symptoms. SSRIs cause sexual dysfunction, emotional blunting, weight gain, and discontinuation syndrome. The peptides studied for mood disorders generally show fewer of these issues in both animal and human trials, though the evidence base is admittedly smaller. Selank, for example, demonstrates anxiolytic effects comparable to benzodiazepines in clinical studies without the sedation, amnesia, or dependence that make benzodiazepines problematic for long-term use.
Neurogenesis represents another area where peptides diverge from conventional treatments. While SSRIs do promote some hippocampal neurogenesis over weeks to months, certain peptides demonstrate dramatically faster neurogenic effects. PE-22-28 induces measurable neurogenesis and synaptogenesis after just four days in animal models. Semax upregulates BDNF in specific brain regions. These brain repair mechanisms suggest that peptides may not just manage symptoms but actively rebuild neural architecture damaged by chronic depression.
The gut-brain connection provides perhaps the most unique advantage. No traditional antidepressant heals the intestinal lining or reduces gut permeability. BPC-157 does both while simultaneously modulating central neurotransmitter systems. KPV reduces intestinal inflammation through NF-kB inhibition while indirectly improving mood via reduced systemic inflammatory signaling. This dual-system approach, addressing both the gut and the brain simultaneously, is something no conventional medication offers. Researchers studying peptide solutions for complex health challenges find this multi-system modulation particularly compelling.
None of this means peptides are proven replacements for established psychiatric medications. They are not. But the mechanistic differences explain why researchers are increasingly interested in their potential for mood disorders, particularly for individuals who have not responded to conventional treatments. The peptide therapy landscape continues to evolve as more data becomes available.
The most researched peptides for depression
Not all peptides studied for mood disorders carry equal weight of evidence. Some have human clinical trial data. Others rely primarily on animal models. The following section covers the peptides with the most substantive research behind their antidepressant properties, presented in order of evidence strength and mechanistic interest. Each subsection includes the mechanism of action, key research findings, and practical protocol information drawn from published studies and clinical applications.
Selank for depression
Selank is a synthetic analog of tuftsin, an immunomodulatory peptide naturally produced by the spleen. Its sequence, Thr-Lys-Pro-Arg-Pro-Gly-Pro, was developed at the Institute of Molecular Genetics of the Russian Academy of Sciences. While Selank is better known for its anxiolytic properties, its antidepressant mechanisms deserve thorough examination.
The peptide influences mood through at least four distinct pathways. First, it modulates GABAA receptors allosterically, meaning it enhances GABA signaling without directly activating the receptor the way benzodiazepines do. This produces calming effects without sedation or cognitive impairment. Second, Selank modulates both dopamine and serotonin receptor activity, helping normalize the neurotransmitter imbalances that underlie depressive symptoms. Third, it increases levels of leu-enkephalin, a natural opioid peptide involved in pain relief and mood elevation. Fourth, it reduces neuroinflammation, addressing one of the root causes of treatment-resistant depression.
Clinical trials have evaluated Selank primarily through intranasal administration. A 14-day intranasal course demonstrated both anxiolytic and mood-stabilizing effects with good tolerability. Longer protocols, extending 8 to 12 weeks, show more pronounced cognitive and mood improvements. The compound has regulatory approval in Russia for anxiety and cognitive disorders. For a comprehensive breakdown of administration methods, see the Selank dosage guide.
Research on Selank combined with diazepam revealed an interesting finding. The peptide amplified the anxiolytic action of the benzodiazepine, suggesting potential as an adjunctive therapy that could allow lower doses of conventional anxiolytics. This combinatorial approach aligns with the multi-target philosophy that makes peptide research compelling for mood disorders.
Standard research protocols use subcutaneous administration once daily, with cycling patterns of four weeks on followed by four weeks off, or five days on with two days off. The intranasal route offers advantages for mood-related applications because it bypasses the blood-brain barrier more efficiently, delivering the peptide directly to central nervous system targets.
PE-22-28 for depression
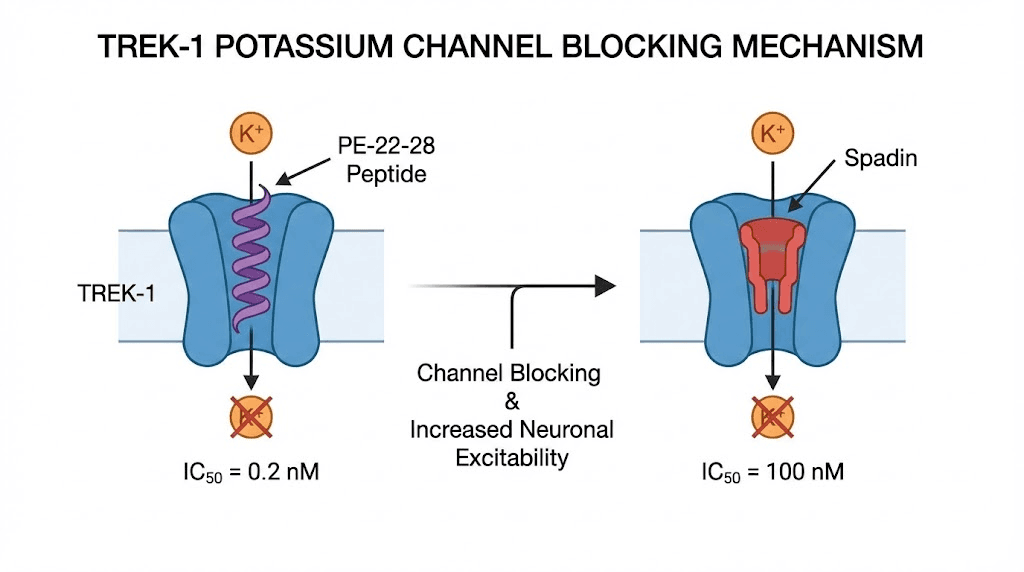
PE-22-28, sometimes called Mini-Spadin, may be the most exciting antidepressant peptide candidate in current research. This seven-amino-acid synthetic peptide was derived from spadin, itself a fragment of the sortilin protein. What makes PE-22-28 remarkable is not just its mechanism but its potency and speed of action.
The peptide works by blocking TREK-1 potassium channels. These channels, when overactive, are directly linked to depression. They hyperpolarize neurons in mood-regulating brain regions, essentially making those neurons harder to activate. By blocking TREK-1 channels, PE-22-28 restores normal neuronal excitability in circuits critical for mood regulation.
The numbers tell the story of potency. PE-22-28 inhibits TREK-1 channels with an IC50 of 0.12 nM, compared to 40-60 nM for its parent compound spadin. That makes PE-22-28 approximately 333 to 500 times more potent. In practical terms, this means dramatically lower doses achieve the same channel-blocking effect, reducing the risk of off-target interactions.
Speed matters in antidepressant research. SSRIs typically require four to six weeks to produce meaningful effects. PE-22-28 demonstrated antidepressant effects in mouse models after just four days. Even more impressive, it induced measurable neurogenesis and synaptogenesis within that same four-day window. New neurons. New synaptic connections. In four days. The complete PE-22-28 guide explores these mechanisms in greater detail.
The duration of action further distinguishes PE-22-28 from its predecessors. While spadin effects last approximately seven hours, PE-22-28 maintains its activity for up to 23 hours. This pharmacokinetic advantage means once-daily dosing provides near-continuous TREK-1 channel blockade.
PE-22-28 also activates serotonergic neurons in the dorsal raphe nucleus, the brain region that serves as the primary source of serotonin projections throughout the central nervous system. This activation occurs through a mechanism distinct from SSRIs, potentially explaining why TREK-1 channel blockers may help people who do not respond to conventional serotonin-based treatments.
Critically, animal studies show no evidence of hallucinations, dependence, or tolerance development with PE-22-28 administration. The rapid onset without psychomimetic effects places it in a different category from ketamine, another fast-acting antidepressant approach that carries significant abuse potential.
Anecdotal research protocols use approximately 400 mcg administered intranasally once daily, typically in the morning. However, human clinical trials are still limited, and optimal dosing in humans has not been formally established. Researchers should approach PE-22-28 with appropriate caution given the early stage of human evidence.
Semax for depression
Semax is a heptapeptide with the sequence Met-Glu-His-Phe-Pro-Gly-Pro. It is a synthetic derivative of ACTH(4-10), the fragment of adrenocorticotropic hormone responsible for neurotropic rather than hormonal effects. Developed in Russia, Semax has been studied extensively for cognitive enhancement, stroke recovery, and mood regulation.
The antidepressant properties of Semax center on its ability to upregulate BDNF in specific brain areas. This is not a diffuse, whole-brain effect. Semax increases BDNF expression in targeted regions relevant to mood, including the hippocampus and prefrontal cortex, the very areas where BDNF deficits are most pronounced in depressed individuals. It also increases plasma BDNF levels, providing a measurable biomarker of its neurotrophic activity.
Beyond BDNF, Semax normalizes anxiety and depression-like behavior through monoamine tuning. Rather than flooding synapses with a single neurotransmitter, it modulates the balance between serotonin, dopamine, and norepinephrine, nudging each toward optimal levels rather than artificially elevating one at the expense of others. This tuning mechanism may explain why Semax improves mood without the emotional blunting that SSRIs sometimes produce. The Semax dosage guide provides detailed protocol information for researchers.
Cognitive effects compound the mood benefits. Semax improves attention and short-term memory at doses of 250 to 1000 mcg per kg of body weight. Since cognitive dysfunction is a core feature of depression, often persisting even after mood improves, the cognitive enhancement properties of Semax provide additional therapeutic value. Researchers interested in broader brain function optimization frequently include Semax in their protocols.
In Russia, Semax has been used clinically for stroke treatment at doses of 6000 mcg per day for 10-day courses. For cognitive and mood applications in healthy individuals, the standard protocol uses a 0.1% solution, with one to two drops administered intranasally twice daily. The intranasal route is preferred because it delivers the peptide directly to the central nervous system through the olfactory mucosa.
Semax produces no sedative effects, making it suitable for daytime use. This distinguishes it from many anxiolytic compounds that impair alertness and cognitive performance. Combined with its BDNF-upregulating properties, Semax offers a compelling profile for researchers addressing the intersection of cognitive decline and mood disorders.
BPC-157 for depression
BPC-157, a 15-amino-acid peptide derived from human gastric juice, is most widely known for its tissue healing properties. But its effects on the central nervous system, particularly on neurotransmitter systems implicated in depression, deserve serious attention from researchers exploring mood disorder interventions.
The scope of BPC-157 neurotransmitter interactions is unusually broad. This single peptide interacts with the serotonin system, the dopamine system, the GABA system, the nitric oxide system, and the glutamate system. In rat studies, administration of 10 mcg per kg per day for seven days produced region-specific increases in serotonin synthesis. Not a global serotonin flood, but targeted increases in brain areas most relevant to mood regulation. This selectivity reduces the risk of the side effects associated with non-selective serotonin elevation.
BPC-157 demonstrates specific relevance to medication-related mood issues. It antagonizes amphetamine-induced anxiety in animal models, suggesting protective effects against stimulant-driven mood disturbances. Perhaps more significantly, it alleviates diazepam withdrawal symptoms, a finding with direct implications for individuals attempting to discontinue benzodiazepine therapy. Anyone who has experienced benzodiazepine withdrawal understands the severity of rebound anxiety and depression that can accompany discontinuation.
Neuroprotective properties add another dimension to the antidepressant profile. BPC-157 reduces hippocampal ischemia-reperfusion injuries in animal models, protecting the brain region most vulnerable to chronic stress damage. Since hippocampal atrophy is a hallmark of major depression, compounds that protect and potentially restore hippocampal tissue address a fundamental aspect of the disease process.
The gut-brain axis benefits of BPC-157 create a uniquely dual-action antidepressant mechanism. By healing the gut lining, reducing intestinal permeability, and modulating gut inflammation, BPC-157 addresses the peripheral inflammatory signaling that contributes to central neuroinflammation and depressive symptoms. This mechanism is explored further in the gut-brain section below, and the BPC-157 stacking guide covers how to combine it with complementary peptides.
Research protocols for BPC-157 typically use subcutaneous or oral administration. For researchers using the BPC-157 dosage calculator, standard protocols range from 200 to 500 mcg per day administered subcutaneously, though the optimal dose for neuropsychiatric applications may differ from tissue healing protocols. Proper reconstitution and correct storage are essential for maintaining peptide integrity.
Pinealon for depression
Pinealon, also known as EDR peptide (Glu-Asp-Arg), is a tripeptide that targets the pineal gland. Its antidepressant potential operates through a mechanism distinct from the other peptides discussed so far, focusing on serotonin synthesis regulation and circadian rhythm normalization.
The primary antidepressant mechanism involves promoting serotonin accumulation in the cerebral cortex. Pinealon achieves this by stimulating serotonin synthesis through regulation of the 5-tryptophan hydroxylase gene, the rate-limiting enzyme in serotonin production. Rather than blocking serotonin reuptake like SSRIs, Pinealon increases the actual production of serotonin, addressing deficiency at its source rather than recycling existing stores.
Circadian rhythm disruption is both a symptom and a driver of depression. Pinealon improves sleep quality and normalizes circadian rhythms through enhanced melatonin production. Since the pineal gland is the primary site of melatonin synthesis, and since Pinealon specifically targets pineal function, this effect is direct rather than incidental. Better sleep leads to better mood regulation, reduced cortisol, and improved cognitive function, creating a positive feedback loop that compounds over time.
The timeline of benefits follows a predictable pattern. Memory and cognitive improvements typically appear within one to two weeks. Mood enhancement becomes more pronounced at four to six weeks. This progression makes sense mechanistically, as cognitive effects from improved neural signaling appear before the structural and neurochemical changes underlying sustained mood improvement have fully developed. The complete Pinealon benefits guide covers these timelines in detail.
Perhaps the most intriguing aspect of Pinealon research involves its effects on cellular aging. Studies demonstrate that Pinealon extends cellular lifespans through telomere lengthening, a mechanism shared with Epitalon. While the direct relevance to depression may seem tangential, chronic depression accelerates cellular aging through telomere shortening. A peptide that addresses both mood and cellular aging simultaneously offers unique value for researchers studying the intersection of mental health and longevity.
Pinealon belongs to the bioregulator peptide category developed through Khavinson research. These short peptides were designed to regulate specific organ systems through gene expression modulation, and the Khavinson peptide framework provides the theoretical foundation for understanding how tripeptides can produce such targeted effects.
Peptides for anxiety specifically
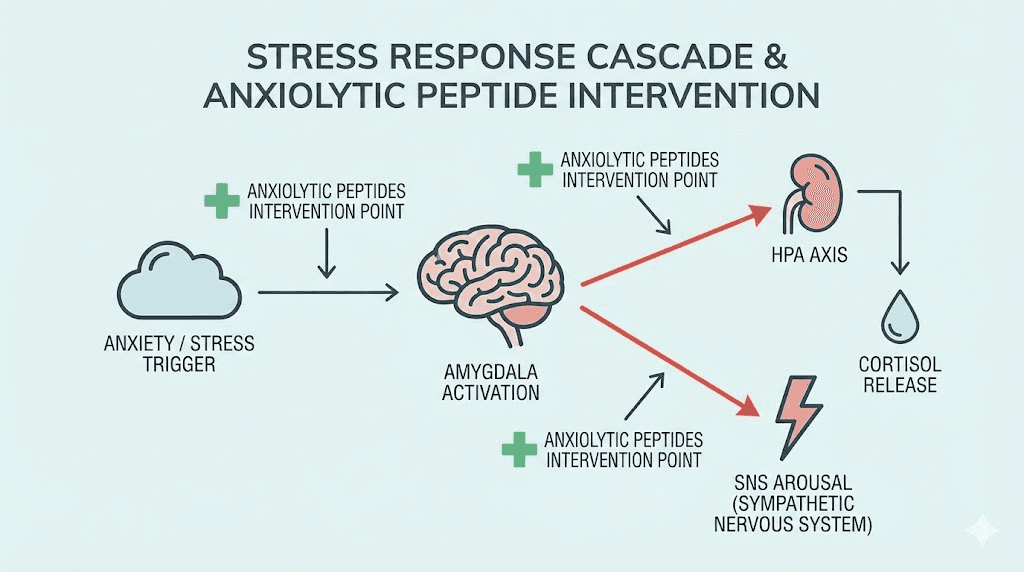
While depression and anxiety share overlapping neurobiology, anxiety involves distinct circuits and mechanisms that deserve separate discussion. The amygdala hyperactivation, excessive sympathetic nervous system arousal, and impaired fear extinction that characterize anxiety disorders respond to different peptide targets than the anhedonia, BDNF deficits, and hippocampal atrophy more central to depression. The following peptides show the strongest evidence for anxiolytic, specifically anxiety-reducing, applications.
Selank for anxiety
Selank earned its primary reputation as an anxiolytic, and the evidence supporting this application is stronger than for any other peptide in this guide. The comparison that matters most is this: Selank demonstrates anxiolytic effects comparable to benzodiazepines without producing sedation, amnesia, withdrawal symptoms, or physical dependence. That combination of efficacy and safety is what makes Selank exceptional.
The anxiolytic mechanism works through allosteric modulation of GABAA receptors. Unlike benzodiazepines, which bind directly to GABA receptors and force them open, Selank enhances the receptor response to naturally released GABA. This means the anxiolytic effect tracks with the brain own inhibitory signaling rather than overriding it. The result is anxiety reduction that feels natural rather than sedated, a distinction that matters enormously for daily functioning.
GABAergic enhancement is only part of the picture. Selank also reduces neuroinflammation, which emerging research identifies as a driver of pathological anxiety. By lowering inflammatory signaling in the brain, Selank addresses anxiety at the level of neuronal environment rather than just neurotransmitter balance. This dual mechanism, enhanced inhibition plus reduced inflammation, may explain why clinical response rates are strong.
The increase in leu-enkephalin levels adds another anxiolytic dimension. Enkephalins are natural opioid peptides that promote feelings of calm and well-being without the euphoria, respiratory depression, or addiction risk associated with exogenous opioids. Higher enkephalin tone contributes to emotional resilience and reduced reactivity to stressors.
Clinical protocols for anxiety-focused Selank use typically involve 14-day courses of intranasal administration. Research suggests that benefits accumulate over the treatment period, with peak anxiolytic effects observed toward the end of the two-week course and persisting for a period afterward. Longer protocols of eight to twelve weeks produce more durable changes in baseline anxiety levels. Detailed Selank protocols cover cycling, administration, and dosing specifics.
Combined administration with diazepam amplifies the anxiolytic action of both compounds. This finding has practical implications for researchers interested in reducing benzodiazepine doses while maintaining therapeutic efficacy, an approach that could mitigate the dependence and withdrawal risks inherent in long-term benzodiazepine use.
Oxytocin for anxiety
Oxytocin is a neuropeptide produced in the hypothalamus and released by the posterior pituitary gland. Known colloquially as the bonding hormone, its anxiolytic properties extend far beyond social attachment into direct modulation of fear and anxiety circuits.
The primary anxiolytic mechanism involves lowering amygdala reactivity. The amygdala serves as the brain threat detection center, and excessive amygdala activation is a hallmark of anxiety disorders, PTSD, and social phobia. Oxytocin reduces this hyperactivation, effectively raising the threshold for threat perception and reducing the intensity of fear responses. Neuroimaging studies show measurable decreases in amygdala activation following intranasal oxytocin administration.
Meta-analytic data quantifies the effect. Across multiple studies, intranasal oxytocin produces a Hedges g of 0.67 for anxiety and mood improvement, representing a moderately strong effect size. This is comparable to the effect sizes seen with established anxiolytic medications, lending credibility to oxytocin as a genuine therapeutic candidate rather than a marginal intervention.
Research shows oxytocin reduces symptoms across multiple anxiety-related conditions: generalized anxiety, social anxiety, OCD, and depression with anxious features. The breadth of efficacy across diagnostic categories suggests that oxytocin targets a fundamental anxiety mechanism rather than a disorder-specific pathway. The oxytocin dosage chart provides specific protocols based on clinical trial data.
Dosing protocol matters critically with oxytocin. The most common clinical trial dose is 24 IU administered intranasally. However, dose frequency significantly affects outcomes. Daily dosing may cause receptor desensitization, where oxytocin receptors downregulate in response to constant stimulation, reducing the peptide effectiveness over time. Every-other-day dosing maintained anxiolytic effects better than daily administration in comparative research. This finding is important for researchers planning longer-term protocols and is a detail that many sources overlook.
Oxytocin also promotes prosocial behavior and trust, which indirectly benefits anxiety by improving social functioning and reducing isolation. For individuals whose anxiety manifests primarily in social contexts, this combination of direct amygdala modulation and enhanced social confidence provides a dual-action mechanism.
Neuropeptide Y for anxiety and resilience
Neuropeptide Y, often abbreviated NPY, represents one of the most fascinating connections between stress resilience and peptide biology. The research linking NPY levels to anxiety resistance emerged from an unexpected source: studies of elite military personnel under extreme stress.
In studies of U.S. Special Forces soldiers, researchers found that individuals with higher NPY levels demonstrated dramatically better stress adaptation. They maintained cognitive function, emotional stability, and decision-making capacity under conditions designed to break them psychologically. This was not a small effect. NPY levels were among the strongest biological predictors of stress resilience measured in the study.
The clinical implications extend beyond military contexts. Research on depressed patients found that low NPY levels correlate with suicidal ideation, suggesting that NPY deficiency may identify particularly vulnerable individuals. Genetic variants in the NPY gene predict resilience versus vulnerability to mood disorders, further establishing NPY as a fundamental component of emotional regulation.
Animal model research has demonstrated that intranasal NPY administration reverses anxiety and depressive behavior in PTSD models. The anxiolytic effects appear mediated primarily in the hippocampal CA1 region and persist for remarkably long periods. In some studies, resilient behaviors persisted for up to eight weeks after treatment cessation, suggesting that NPY does not merely suppress anxiety but may induce lasting changes in stress-response circuitry.
The eight-week persistence of effects after treatment discontinuation is particularly noteworthy. Most anxiolytic compounds produce effects only during active administration. That NPY-induced resilience outlasts the treatment period by such a wide margin suggests neuroplastic changes, actual rewiring of anxiety circuits, rather than simple pharmacological suppression. This aligns with what researchers studying brain repair peptides have observed with other neuroplasticity-promoting compounds.
NPY is still in relatively early stages of clinical translation for psychiatric applications. Intranasal delivery appears to be the most promising route for CNS effects, and ongoing research continues to clarify optimal dosing and treatment duration for anxiety disorders.
KPV and the inflammation-anxiety connection
KPV, a tripeptide consisting of Lys-Pro-Val, may seem like an unusual inclusion in a discussion of anxiety peptides. It does not directly modulate GABA receptors, serotonin levels, or amygdala activity. Its anxiolytic potential operates through a completely different pathway: the reduction of systemic inflammation that drives neuroinflammation and, consequently, anxiety.
The mechanistic chain begins with NF-kB, the master regulator of inflammatory gene expression. KPV blocks NF-kB activation, suppressing the production of pro-inflammatory cytokines including TNF-alpha, IL-1beta, and IL-6. These same cytokines are consistently elevated in anxiety disorders and have been shown to directly increase anxiety-like behavior in animal models when injected peripherally or centrally.
Gut barrier integrity provides the critical link. KPV heals the intestinal epithelium and reduces colitis in inflammatory bowel disease models. By restoring gut barrier function, KPV prevents the translocation of bacterial endotoxins from the intestinal lumen into the bloodstream. This reduces the systemic inflammatory load that ultimately reaches the brain and activates neuroinflammatory pathways driving anxiety. The KPV benefits profile covers this mechanism comprehensively.
For individuals whose anxiety has an inflammatory component, and emerging research suggests this is a larger percentage than previously recognized, addressing inflammation may be as important as targeting neurotransmitters directly. KPV offers a way to do exactly that, working through the gut to influence the brain through a pathway that conventional anxiolytics do not touch. This approach connects directly with the broader understanding of how peptides address autoimmune and inflammatory conditions.
The indirect nature of KPV mood effects means it works best as part of a comprehensive protocol rather than as a standalone anxiolytic. Combining KPV with a direct-acting anxiolytic peptide like Selank addresses both the inflammatory drivers and the neurotransmitter imbalances contributing to anxiety. This stacking concept is explored further in the stacking strategies section below.
The gut-brain axis and how peptides bridge both systems
The gut-brain axis is not a metaphor. It is a bidirectional communication network involving the vagus nerve, the enteric nervous system, the immune system, and metabolic signaling pathways that physically connect intestinal health to brain function. Understanding this connection transforms how researchers approach mental health, and it explains why some of the most effective mood-modulating peptides are the same ones studied for gastrointestinal conditions.
The numbers are striking. Approximately 90% of the body serotonin resides in the gut, produced by enterochromaffin cells in the intestinal lining. Tryptophan, the amino acid precursor to serotonin, is absorbed through the intestinal epithelium and competes with other large neutral amino acids for transport across the blood-brain barrier.
When gut inflammation disrupts tryptophan metabolism, shunting it toward the kynurenine pathway instead of serotonin synthesis, the brain experiences a serotonin deficit even when dietary tryptophan intake is adequate.
Researchers interested in gut health peptides increasingly recognize this tryptophan-stealing mechanism as a key driver of inflammation-associated depression.
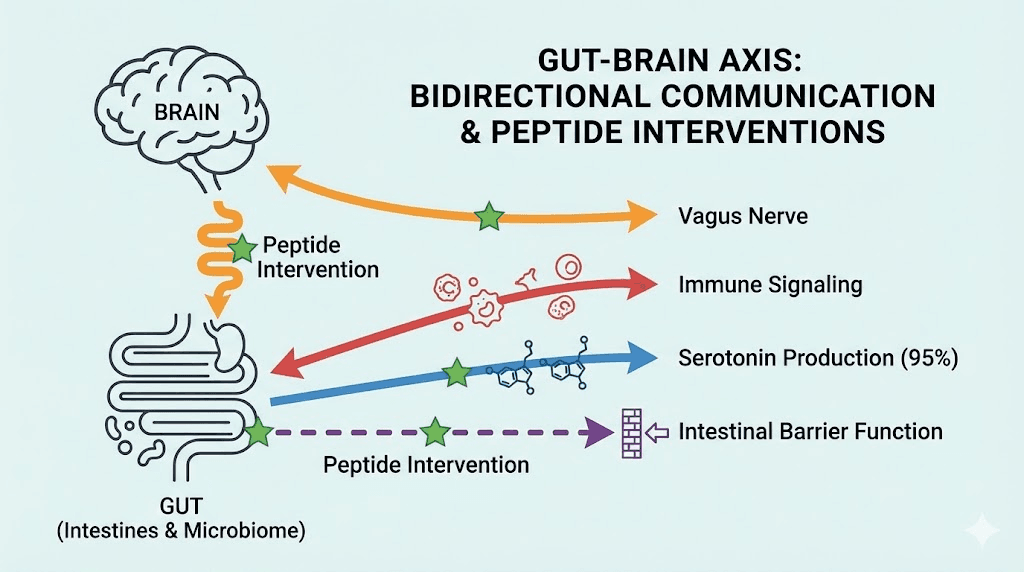
BPC-157 stands alone in its dual gut-brain action. On the gut side, it accelerates healing of the intestinal mucosa, reduces gut permeability, and promotes angiogenesis in damaged tissue. These effects are well-documented across multiple animal models of intestinal injury, ulcerative colitis, and inflammatory bowel disease. On the brain side, the same peptide modulates serotonin, dopamine, GABA, nitric oxide, and glutamate systems. The combination means BPC-157 simultaneously repairs the gut environment driving inflammatory depression while directly modulating the neurotransmitter systems producing depressive symptoms.
This is not a theoretical connection. Animal studies show that BPC-157 administration produces antidepressant-like behavior alongside gastrointestinal healing, with the two effects appearing in parallel rather than sequentially. The peptide does not heal the gut first and then improve mood. It does both simultaneously through overlapping signaling mechanisms. For researchers exploring BPC-157 stacking strategies, understanding this dual action is essential for protocol design.
KPV contributes to gut-brain axis modulation through inflammation reduction. By blocking NF-kB activation in intestinal tissue, KPV reduces the production and release of pro-inflammatory cytokines that would otherwise enter systemic circulation and cross into the brain. This reduces the inflammatory burden on the central nervous system without requiring a compound to cross the blood-brain barrier itself. The gut does the work. The brain reaps the benefits.
The vagus nerve serves as the primary communication highway between gut and brain. This cranial nerve carries sensory information from the intestinal environment directly to the brainstem, influencing mood, anxiety, and cognitive function in real time. Gut inflammation activates vagal afferents that signal distress to the brain, while healthy gut signaling promotes parasympathetic tone and emotional equilibrium. Peptides that reduce gut inflammation effectively change the messages traveling up the vagus nerve from alarm signals to calm-state signals.
For researchers designing mental health protocols, the gut-brain axis findings suggest that addressing gastrointestinal health is not peripheral to mood treatment. It may be central. A protocol that includes both a central-acting peptide like Selank or Semax and a gut-healing peptide like BPC-157 or KPV targets the mood disorder from both directions simultaneously. The peptide stacking guide provides frameworks for building multi-target protocols. Researchers can use the peptide stack calculator to plan combinations and verify compatibility.
Sleep, circadian rhythm, and mood
Sleep disruption and mood disorders exist in a bidirectional relationship so tight that untangling cause from effect is often impossible. Poor sleep worsens depression and anxiety. Depression and anxiety disrupt sleep. Breaking this cycle requires addressing both simultaneously, and several peptides offer mechanisms relevant to sleep architecture, circadian regulation, and their downstream effects on mood.
DSIP and sleep-mood connection
Delta Sleep-Inducing Peptide, abbreviated DSIP, was first isolated from rabbit brain tissue during induced sleep. Its name describes its primary function. DSIP promotes delta wave sleep, the deepest stage of non-REM sleep responsible for physical restoration, memory consolidation, and hormonal regulation.
The mood relevance of delta sleep cannot be overstated. During deep sleep, cortisol levels reach their daily nadir, growth hormone secretion peaks, and glymphatic clearance removes metabolic waste from the brain. When delta sleep is reduced, as it consistently is in depression, cortisol remains elevated through the night, growth hormone release is blunted, and inflammatory metabolites accumulate in the central nervous system. Each of these consequences independently worsens depressive symptoms.
DSIP normalizes cortisol patterns that become disrupted during chronic stress and depression. Rather than simply inducing sleepiness, it restructures sleep architecture to restore the normal cycling between sleep stages. This normalization of cortisol rhythm has downstream effects on mood, energy, appetite, and cognitive function that extend well beyond the sleep period itself. The DSIP benefits guide covers the full spectrum of effects, while the DSIP dosage guide provides specific protocol information.
For researchers whose mood disruption manifests primarily as sleep disturbance, addressing the sleep component directly may produce faster improvements in daytime mood than targeting neurotransmitters alone. DSIP offers this sleep-first approach with a mechanism distinct from conventional sleep medications, which tend to suppress deep sleep rather than promote it.
Pinealon and circadian regulation
Pinealon contribution to sleep extends beyond its serotonin-boosting effects described in the depression section. By targeting the pineal gland directly, this tripeptide enhances melatonin production and secretion, the primary hormonal signal that synchronizes circadian rhythms.
Circadian disruption is increasingly recognized as both a symptom and a cause of mood disorders. The suprachiasmatic nucleus, the brain master clock, coordinates the timing of neurotransmitter release, hormone secretion, body temperature, and cellular metabolism. When this timing system falters, as it does in depression and anxiety, every downstream process becomes dysregulated. Pinealon addresses this at the source by supporting the pineal gland capacity to produce the melatonin signal that synchronizes the entire circadian system. For researchers exploring pineal peptides for sleep, Pinealon represents the most targeted option available.
The combination of enhanced serotonin synthesis during the day and improved melatonin production at night creates a natural neurochemical rhythm that tracks with healthy mood regulation. Serotonin serves as the precursor to melatonin through the enzymatic pathway in the pineal gland, so Pinealon support of serotonin production also indirectly supports melatonin synthesis. This biochemical synergy is one reason why Pinealon effects on mood tend to become more pronounced over the four-to-six-week timeline, as the circadian system progressively normalizes.
Epitalon and the bigger picture
Epitalon, a tetrapeptide (Ala-Glu-Asp-Gly), does not function as a direct antidepressant. Its inclusion here reflects its role in the broader context of circadian health, cellular aging, and their connections to mood disorders.
Epitalon stimulates melatonin secretion from the pineal gland, supporting circadian rhythm normalization. More uniquely, it activates telomerase, the enzyme that maintains telomere length on chromosomes. Telomere shortening is accelerated in individuals with major depression, representing a measurable biological marker of the aging effect of chronic mood disorders. By supporting telomere maintenance, Epitalon may address one of the long-term consequences of depression at the cellular level.
The practical application of Epitalon for mood researchers is as a supporting compound rather than a primary intervention. It optimizes the circadian and cellular environment within which other, more directly acting mood peptides operate. When circadian rhythms are normalized and cellular stress is reduced, the brain becomes more responsive to interventions targeting neurotransmitters and neuroplasticity.
Peptide stacking strategies for mental health
Individual peptides target individual pathways. But depression and anxiety are multi-system disorders. Strategic stacking, combining peptides with complementary mechanisms, allows researchers to address multiple contributing factors simultaneously. The following stacking strategies are based on mechanistic logic and the available evidence base, though human clinical trials of specific combinations remain limited.
Stack 1: cognitive clarity and mood support (Semax + Selank)
This stack addresses the cognitive-emotional overlap that characterizes many mood disorders. Depression impairs concentration, working memory, and executive function. Anxiety disrupts attention and decision-making. Addressing both the emotional and cognitive dimensions simultaneously often produces better outcomes than targeting either alone.
Semax contributes BDNF upregulation, monoamine tuning, and cognitive enhancement. It sharpens attention, improves memory, and supports neuroplasticity in mood-relevant brain regions. Selank provides anxiolytic effects, GABAergic modulation, and anti-inflammatory action. Together, they address four of the five major systems disrupted in mood disorders: neurotransmitter balance, neuroinflammation, BDNF deficits, and HPA axis function.
Both peptides are commonly administered intranasally, which simplifies the protocol. Semax is typically used in the morning to leverage its cognitive-enhancing properties during waking hours. Selank can be administered once or twice daily depending on the severity of anxiety symptoms. The nasal spray peptide guide covers intranasal administration techniques in detail.
This combination has a track record in Russian clinical practice, where both peptides are approved medications. While Western clinical trial data on the specific combination is limited, the individual evidence bases for each peptide are substantial, and their mechanisms are complementary rather than redundant. Researchers can learn more about combining peptides safely in the peptide cycling guide.
Stack 2: gut-brain healing (BPC-157 + KPV)
This stack targets mood disorders through the gut-brain axis, making it particularly relevant for individuals whose depression or anxiety co-occurs with gastrointestinal symptoms, food sensitivities, or known inflammatory conditions.
BPC-157 heals the intestinal mucosa, reduces gut permeability, and simultaneously modulates central neurotransmitter systems. KPV blocks NF-kB-driven inflammation, reduces pro-inflammatory cytokine production, and supports gut barrier integrity. Together, they address gut inflammation from multiple angles while BPC-157 provides direct central nervous system benefits through its neurotransmitter interactions.
The synergy between these two peptides is mechanistic rather than additive. KPV reduces the inflammatory environment that damages the gut lining. BPC-157 repairs the damage and promotes tissue regeneration. With inflammation suppressed and tissue healing accelerated, the gut barrier normalizes faster than with either peptide alone, reducing the systemic inflammatory load that drives neuroinflammation.
Subcutaneous administration is standard for BPC-157 in this context, while KPV can be administered orally, subcutaneously, or even topically for intestinal applications. The peptide dosing guide provides frameworks for multi-peptide protocols, and the peptide calculator helps determine accurate dosing based on concentration and volume.
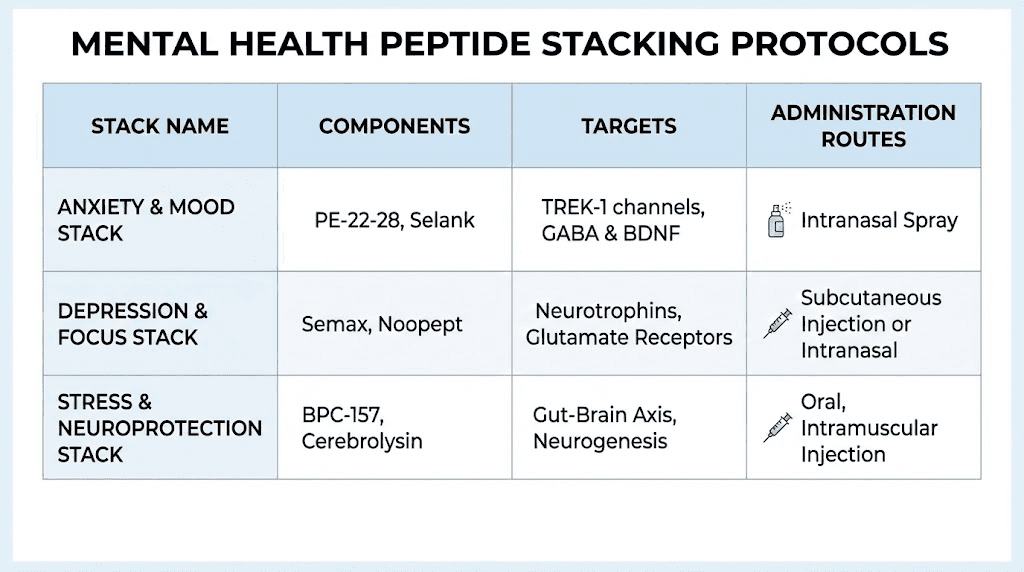
Stack 3: comprehensive mood protocol
For researchers seeking the most thorough multi-system approach, a comprehensive mood protocol might include elements targeting all five disrupted systems: neurotransmitter balance, HPA axis regulation, neuroinflammation, BDNF production, and gut-brain axis function.
A comprehensive approach might combine Selank for anxiolytic and anti-inflammatory effects, Semax for BDNF upregulation and cognitive support, BPC-157 for gut healing and neurotransmitter modulation, and Pinealon for serotonin synthesis and circadian normalization. This covers direct neurotransmitter modulation (Selank, Semax, BPC-157, Pinealon), neuroinflammation reduction (Selank, BPC-157), BDNF enhancement (Semax), gut-brain axis repair (BPC-157), and circadian rhythm normalization (Pinealon).
Important safety notes apply to any multi-peptide protocol. Start with one peptide at a time, adding each new compound after at least one to two weeks of stable response to the previous one. This allows researchers to identify which peptides produce specific effects and to recognize any adverse reactions attributable to individual compounds rather than combinations. The peptide cycle planning guide is essential reading for anyone considering multi-peptide protocols.
Cycling should be built into any stacking protocol. Not all peptides in a stack need to be cycled simultaneously. Staggering on-off periods can maintain continuous coverage while allowing receptor resensitization for individual compounds. The complete stacking guide covers these cycling strategies in depth.
Practical considerations for mental health peptide research
Understanding the science behind mood-modulating peptides is necessary but insufficient. Practical implementation involves decisions about administration routes, cycling protocols, storage, cost, and professional guidance that determine whether a research protocol succeeds or fails.
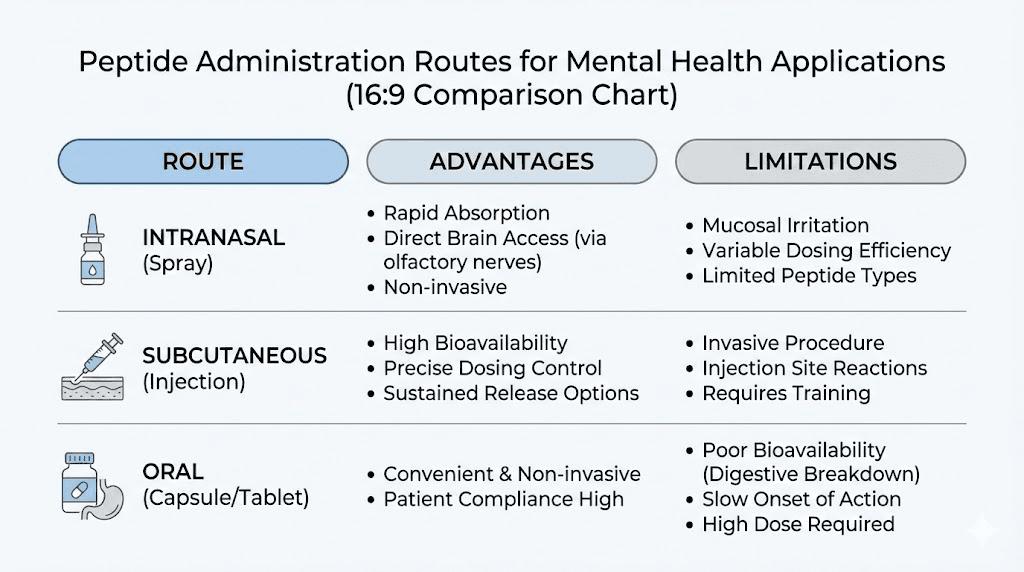
Administration routes for mood peptides
The route of administration significantly affects how a peptide reaches its target tissue, which is critically important for mood applications where the target is the central nervous system.
Intranasal administration is preferred for peptides targeting the brain directly. The olfactory mucosa provides a pathway that partially bypasses the blood-brain barrier, delivering peptides to the central nervous system more efficiently than peripheral routes. Selank, Semax, PE-22-28, and oxytocin are all commonly administered intranasally for mood applications. The nasal spray peptide guide covers proper technique, device selection, and dosing considerations specific to intranasal delivery.
Subcutaneous injection remains the standard for peptides like BPC-157 that need systemic distribution. While subcutaneous BPC-157 does reach the brain through peripheral circulation, its gut-healing effects require systemic presence. Researchers unfamiliar with injection technique should review the injectable peptides guide and consider using a peptide injection pen for more consistent and comfortable administration.
Oral administration works for select peptides, particularly small bioregulator peptides like Pinealon. These tripeptides are small enough to survive partial gastrointestinal degradation and still reach target tissues. The peptide capsules guide covers oral bioavailability considerations and which peptides are suitable for this route. Oral BPC-157 is also used, though bioavailability is lower than subcutaneous, and higher doses may be needed to achieve equivalent systemic effects. The injectable versus oral peptides comparison helps researchers evaluate the tradeoffs for their specific situation.
Cycling protocols for mood peptides
Cycling, alternating periods of peptide use with periods of abstinence, serves three purposes in mental health protocols: preventing receptor desensitization, allowing assessment of baseline mood without peptide support, and reducing the risk of developing tolerance.
Selank cycling typically follows a four-weeks-on, four-weeks-off pattern, or a five-days-on, two-days-off weekly cycle. The latter more closely mimics a medication schedule and may be easier to maintain consistently.
Oxytocin requires particular attention to cycling. Research shows that every-other-day dosing maintains anxiolytic effects better than daily administration, likely because daily dosing triggers receptor downregulation. This means more is not better with oxytocin, and restraint in dosing frequency actually produces superior outcomes.
PE-22-28, given its extended 23-hour duration of action, lends itself naturally to once-daily dosing. Cycling recommendations are less established due to the early stage of human research, but the general principle of periodic breaks applies. Detailed cycling strategies for various peptides are covered in the cycle planning guide, and the question of cycling different peptides is addressed with specific protocol examples.
The timeline for seeing results varies by peptide and should inform expectations. The guide to peptide timelines provides compound-specific benchmarks.
Storage and handling for peptide integrity
Peptides are fragile molecules. Improper storage degrades them, reducing or eliminating their biological activity. For mood-related peptides where consistent dosing is important for therapeutic effect, maintaining peptide integrity through proper handling is essential.
Lyophilized (freeze-dried) peptides should be stored in a freezer at -20 degrees Celsius or below until reconstitution. Once reconstituted with bacteriostatic water, peptides should be refrigerated at 2-8 degrees Celsius and used within a reasonable timeframe. The peptide storage guide covers optimal conditions in detail, and the guide on how long peptides last in the fridge provides specific stability data for commonly used compounds.
Reconstitution technique matters for dosing accuracy. The reconstitution guide walks through the process step by step, and the reconstitution calculator eliminates math errors that could lead to under- or over-dosing. For mood applications where dosing precision affects therapeutic outcomes, these practical details deserve as much attention as the science behind the peptides themselves.
Cost considerations
Mental health peptide protocols can range from relatively affordable to quite expensive depending on the compounds selected, the duration of use, and the source quality. The peptide therapy cost guide breaks down pricing across different categories.
Bioregulator peptides like Pinealon tend to be among the most affordable options, with small tripeptides costing less to synthesize than larger, more complex molecules. Selank and Semax fall in the moderate range. PE-22-28, as a newer and less widely produced compound, may carry premium pricing.
Source quality directly affects both safety and efficacy. Third-party testing for purity and identity is non-negotiable for any peptide intended for research use. The peptide testing labs guide identifies reputable testing services, and the peptide vial research guide covers what to look for when evaluating sources. Cheap peptides from untested sources are not a bargain if they contain degradation products, impurities, or incorrect compounds.
Working with healthcare providers
Mental health is serious. Peptides are research compounds. These two facts create a responsibility to involve qualified healthcare providers in any mental health protocol, regardless of the promising research behind individual peptides.
A psychiatrist or physician can provide proper diagnosis, rule out medical causes of mood symptoms, monitor for drug interactions with existing medications, and adjust treatment plans based on response. The online peptide therapy guide covers how to find providers knowledgeable about peptide research.
Never discontinue prescribed psychiatric medications to start a peptide protocol without medical supervision. Abrupt discontinuation of SSRIs, SNRIs, or benzodiazepines can produce dangerous withdrawal syndromes. Any transition should be gradual, medically supervised, and carefully monitored.
The legal status of peptides varies by jurisdiction. Understanding the regulatory framework in your location is important for both compliance and access.
What the research actually says (and what it does not)
Intellectual honesty demands acknowledging the limitations of current evidence. The peptides discussed in this guide range from those with human clinical trial data to those supported primarily by animal models and anecdotal reports. Understanding where each peptide falls on the evidence hierarchy helps researchers set appropriate expectations and make informed decisions.
Selank has the strongest clinical evidence base among the peptides discussed here. It has undergone human clinical trials in Russia, received regulatory approval for anxiety and cognitive disorders, and accumulated years of clinical use data. The trial methodology may not always meet the gold-standard requirements of Western regulatory agencies, but the breadth and consistency of positive findings across multiple studies provides meaningful confidence in its efficacy and safety.
Oxytocin also has substantial human data, with meta-analyses quantifying its effects on anxiety and mood. The moderately strong effect size (Hedges g = 0.67) across multiple randomized controlled trials places oxytocin research on relatively firm ground, though questions about optimal dosing, frequency, and long-term effects remain active areas of investigation.
Semax has extensive clinical use in Russia for stroke treatment and cognitive enhancement, with data supporting its mood effects primarily from preclinical research and clinical observation rather than large randomized trials specifically designed to test antidepressant efficacy. The BDNF upregulation has been documented in both animal and human studies, providing a plausible and measurable mechanism.
PE-22-28 sits in a different category. The preclinical data is extraordinarily promising, with rapid onset, high potency, neurogenesis induction, and a favorable safety profile in animal models. But human clinical trials are limited, and translating animal results to human outcomes is notoriously unreliable. Researchers should approach PE-22-28 with enthusiasm tempered by appropriate caution about the gap between mouse models and human depression.
BPC-157 has extensive animal data for both gastrointestinal and neurological effects but lacks published large-scale human clinical trials for depression specifically. The neurotransmitter modulation data comes entirely from preclinical models. The gut-healing effects, while well-documented in animals, also lack robust human trial data, though anecdotal reports from clinical use are consistently positive.
NPY research includes human observational data linking NPY levels to stress resilience, but therapeutic intranasal NPY administration for mood disorders remains primarily in the preclinical stage. The transition from observing natural NPY as a biomarker to using exogenous NPY as a treatment involves assumptions about dose-response relationships that have not been fully validated in human trials.
The Russian clinical trial context deserves specific mention. Many of the peptides discussed here, particularly Selank and Semax, were developed and tested primarily in Russia. Russian clinical trials have contributed valuable data, but methodological differences, including smaller sample sizes, different statistical approaches, and less rigorous blinding procedures compared to FDA standards, mean that Western regulatory agencies generally do not accept this data for drug approval. This does not mean the data is wrong, but it does mean it carries less weight in the global evidence hierarchy.
None of the peptides discussed in this guide have FDA approval for the treatment of depression or anxiety. This is a critical distinction between research evidence and regulatory approval, and it affects legal status, availability, and the framework within which these compounds can be used.
Managing expectations is essential. Peptides are not magic. They are research compounds with promising mechanisms and varying levels of evidence. They work within the context of overall health, including sleep, exercise, nutrition, social connection, and professional mental health support. Treating them as one component of a comprehensive approach, rather than a standalone solution, produces the most realistic and sustainable outcomes.
Additional peptides with mood-relevant mechanisms
Beyond the primary peptides discussed above, several additional compounds demonstrate mechanisms relevant to mental health, though their evidence bases for mood disorders specifically are less developed.
Dihexa is a hexapeptide with potent neurotrophic activity. It enhances hepatocyte growth factor signaling, which promotes synaptogenesis and cognitive function. Its effects on BDNF-related pathways and synaptic plasticity make it theoretically relevant to depression, though direct antidepressant research is limited. Researchers interested in cognitive aspects of mood disorders find Dihexa relevant because of its pronounced effects on learning and memory, functions consistently impaired in depression.
Cerebrolysin, a complex mixture of neuropeptides and amino acids derived from porcine brain tissue, has been studied for neurodegenerative conditions, stroke recovery, and traumatic brain injury. Its relevance to mood disorders stems from broad neurotrophic effects, including BDNF modulation and neuroprotection. Clinical use in Eastern Europe and Asia has included patients with comorbid depression and cognitive decline.
MOTS-c, a mitochondrial-derived peptide, influences cellular energy production and metabolic function. The connection to mood is indirect but meaningful. Mitochondrial dysfunction has been increasingly recognized as a contributor to depression, with impaired cellular energy production in mood-regulating brain regions correlating with depressive symptoms. By supporting mitochondrial function, MOTS-c may create a more favorable energy environment for neuronal health. The best peptides for energy guide covers MOTS-c and related compounds.
Thymalin and immune-modulating peptides influence mood through their effects on inflammatory signaling. Thymosin alpha-1, another immune peptide, reduces pro-inflammatory cytokine production, which may benefit individuals whose depression has a significant inflammatory component. The connection between immune dysfunction and mood disorders continues to strengthen in the research literature.
SS-31 (Elamipretide) targets the inner mitochondrial membrane, stabilizing cardiolipin and improving electron transport chain efficiency. Like MOTS-c, its mood relevance comes through mitochondrial support rather than direct neurotransmitter modulation. For researchers approaching mood disorders from a cellular energy perspective, SS-31 represents a highly targeted mitochondrial intervention.
Cortagen, a brain bioregulator peptide from the Khavinson framework, targets cerebral cortex function. Like other bioregulator peptides, it works through gene expression modulation rather than receptor binding, offering a fundamentally different mechanism from the neurotransmitter-focused peptides discussed earlier. The alpha peptides guide and Vesugen benefits guide cover related bioregulator peptides that support vascular and systemic health relevant to brain function.
Comparison table of all mental health peptides
The following table summarizes the key characteristics of each peptide discussed in this guide. Use it as a quick reference for comparing mechanisms, evidence levels, and practical considerations. The evidence level ratings reflect the current state of research specifically for mood and anxiety applications, not the peptide overall evidence base for other conditions.
Peptide | Primary target | Evidence level | Administration | Key mechanism |
|---|---|---|---|---|
Selank | Anxiety and mood | Strong (human trials) | Intranasal, subcutaneous | GABA modulation, enkephalin increase, anti-inflammatory |
PE-22-28 | Depression | Promising (animal models) | Intranasal | TREK-1 channel blockade, neurogenesis, serotonergic activation |
Semax | Mood and cognition | Moderate (clinical use) | Intranasal | BDNF upregulation, monoamine tuning |
BPC-157 | Gut-brain, neurotransmitters | Moderate (animal models) | Subcutaneous, oral | Multi-neurotransmitter modulation, gut healing |
Pinealon | Serotonin, circadian | Moderate (bioregulator research) | Oral, subcutaneous | Serotonin synthesis, melatonin support, telomere maintenance |
Oxytocin | Anxiety, social function | Strong (meta-analyses) | Intranasal | Amygdala modulation, prosocial effects |
NPY | Stress resilience | Moderate (observational + animal) | Intranasal | Hippocampal CA1 anxiolysis, lasting neuroplastic changes |
KPV | Inflammation-driven mood | Moderate (animal models) | Oral, subcutaneous | NF-kB inhibition, gut barrier repair, cytokine reduction |
DSIP | Sleep-mood connection | Moderate (clinical use) | Subcutaneous, intranasal | Delta sleep promotion, cortisol normalization |
Epitalon | Circadian, cellular aging | Moderate (bioregulator research) | Subcutaneous | Melatonin secretion, telomerase activation |
Dihexa | Cognition, neuroplasticity | Early (animal models) | Oral, subcutaneous | HGF signaling, synaptogenesis |
Cerebrolysin | Neuroprotection | Moderate (clinical use, neuro) | Injection | Broad neurotrophic support |
MOTS-c | Mitochondrial energy | Early (preclinical) | Subcutaneous | Mitochondrial optimization |
This table provides a starting point for evaluation, not a final answer. Evidence levels will shift as new research is published, and individual responses to specific peptides vary considerably. The peptide forum guide can help researchers connect with communities discussing real-world experiences with these compounds.
Demographic and situational considerations
Mood disorders do not present identically across different populations. Hormonal status, age, sex, and co-existing conditions all influence both the presentation of depression and anxiety and the likely response to peptide interventions.
Women over 40 face unique challenges as declining estrogen and progesterone levels affect serotonin receptor density, GABA sensitivity, and neuroinflammatory markers. The hormonal shifts of perimenopause and menopause frequently trigger or worsen depression and anxiety, even in women with no prior psychiatric history. Peptides that support hormonal balance may complement mood-specific peptides in this population. The safe peptides for women guide covers gender-specific considerations including interaction profiles and dosing adjustments.
Individuals dealing with chronic pain experience significantly higher rates of depression and anxiety. The bidirectional relationship between pain and mood means that peptides addressing both systems simultaneously, such as BPC-157, which heals tissue while modulating neurotransmitters, offer particular advantages for this group. The best peptides for pain guide and the more specific shoulder pain peptide guide cover analgesic applications that overlap with mood benefits.
Researchers focused on anti-aging and longevity often discover mood benefits as a secondary outcome. Anti-aging peptides like Epitalon and the bioregulator peptides influence circadian rhythms, cellular health, and inflammatory markers, all of which affect mood regulation. Growth hormone-releasing peptides like Ipamorelin and Sermorelin improve sleep quality and body composition, both of which correlate with mood improvements.
Body composition affects mood through multiple pathways, including inflammatory signaling from visceral adipose tissue, self-image, and hormonal regulation. Researchers exploring peptides for weight loss, including newer compounds like Cagrilintide, often report mood improvements alongside body composition changes. Similarly, those using peptides for muscle growth may experience mood benefits from improved testosterone levels, better sleep, and the well-documented antidepressant effects of regular resistance training facilitated by enhanced recovery.
Building a research framework
Approaching peptide research for mental health requires structure. Without a systematic framework, researchers risk wasting time, money, and emotional energy on poorly designed protocols that produce ambiguous results. The following framework provides a logical progression for evaluating and implementing mood-related peptide research.
Begin with assessment. Document baseline mood, anxiety levels, sleep quality, cognitive function, and any gastrointestinal symptoms using standardized self-report measures. The PHQ-9 for depression and GAD-7 for anxiety are freely available, validated instruments that provide quantitative baselines against which to measure changes. Keeping consistent records transforms subjective impressions into useful data.
Select a primary target. Is the primary issue depression, anxiety, sleep disruption, cognitive fog, or inflammation? While most people experience some combination, identifying the dominant concern guides initial peptide selection. Selank for primary anxiety. PE-22-28 or Pinealon for primary depression. DSIP for sleep-dominant presentations. BPC-157 plus KPV for inflammation-driven mood issues.
Start with a single peptide. The temptation to stack multiple compounds from the beginning is understandable but counterproductive. Starting with one peptide allows clear attribution of effects, both positive and negative. After establishing stable response over two to four weeks, a second peptide can be added if needed.
Track systematically. Daily mood and anxiety ratings on a simple 1-10 scale, weekly PHQ-9 and GAD-7 scores, sleep duration and quality notes, and any side effects or unexpected changes. This data reveals patterns that subjective memory would miss.
The dosing guide emphasizes the importance of systematic tracking for optimizing protocols.
Adjust based on data, not feelings. The worst day on a downward trend is still progress. A great day during a worsening trend is not success. Trends matter more than individual data points. Give each peptide at least four weeks before evaluating efficacy, unless adverse effects require earlier discontinuation.
Involve professionals. A psychiatrist or physician provides diagnostic accuracy, monitors for serious complications, manages interactions with existing medications, and offers perspective that self-directed research cannot provide. Peptide research is not a substitute for professional mental health care. It is a complement to it. SeekPeptides consistently emphasizes the importance of professional guidance alongside evidence-based peptide education.
Frequently asked questions
What is the best peptide for depression?
PE-22-28 shows the most exciting antidepressant mechanisms, with TREK-1 channel blockade producing rapid-onset effects and neurogenesis in animal models. However, Selank has the strongest human clinical evidence for mood improvement. For researchers prioritizing established safety data, Selank offers the most confidence. For those focused on mechanism and potency, PE-22-28 is the leading candidate. The PE-22-28 guide and Selank guide provide detailed protocol information for each.
Can peptides replace antidepressant medication?
No. Peptides are research compounds without FDA approval for treating depression or anxiety. They should not be used as replacements for prescribed psychiatric medications without medical supervision. Abrupt discontinuation of SSRIs, SNRIs, or benzodiazepines can cause dangerous withdrawal syndromes. Any changes to existing medication should be discussed with and supervised by a qualified healthcare provider.
How long do mental health peptides take to work?
Timelines vary by peptide. Selank shows anxiolytic effects within hours to days of first administration. PE-22-28 demonstrated antidepressant effects after four days in animal models. Semax cognitive effects appear within days, with mood effects developing over weeks. Pinealon cognitive improvements emerge at one to two weeks, with mood enhancement at four to six weeks. The peptide timeline guide covers expected response curves for specific compounds.
Are peptides for anxiety safe?
Safety profiles vary by peptide. Selank has the most extensive safety data, showing no sedation, dependence, or withdrawal in clinical use. Oxytocin is well-tolerated at standard intranasal doses. Most peptides discussed here show favorable safety profiles in available research, but long-term safety data is limited for many compounds. The peptide legality guide covers regulatory considerations.
Can you stack multiple mood peptides together?
Yes, with appropriate caution. Stacking peptides with complementary mechanisms, such as Semax plus Selank for cognitive-mood support, is common in research protocols. Start with one peptide, establish baseline response, then add compounds individually with at least one to two weeks between additions. The stacking guide and stack calculator provide frameworks for safe combination protocols.
Does BPC-157 help with depression through the gut?
BPC-157 demonstrates dual action: it heals the intestinal lining and reduces gut permeability while simultaneously modulating serotonin, dopamine, GABA, and other neurotransmitter systems in the brain. The gut-brain axis connection means that gut healing reduces systemic inflammation reaching the brain, while direct neurotransmitter effects address mood regulation centrally. Both mechanisms work in parallel. The gut health peptides guide covers this dual-action mechanism in detail.
What is the difference between Selank and benzodiazepines for anxiety?
Both reduce anxiety through GABAergic mechanisms, but they work differently. Benzodiazepines directly bind GABA receptors, producing sedation, amnesia, physical dependence, and withdrawal risk. Selank modulates GABA receptors allosterically, enhancing natural GABA signaling without forcing receptor activation. This produces anxiolytic effects without sedation, cognitive impairment, or dependence. The tradeoff is that Selank effects may be subtler than acute benzodiazepine effects, but the safety advantage is substantial.
How should I store mood peptides to maintain potency?
Store lyophilized peptides at -20 degrees Celsius until reconstitution. After mixing with bacteriostatic water, refrigerate at 2-8 degrees Celsius. Protect from light and avoid repeated freeze-thaw cycles. For intranasal peptides, nasal spray devices should be stored upright in the refrigerator. The storage guide provides compound-specific stability information.
External resources
PubMed - National Library of Medicine - Search for peer-reviewed peptide research studies
PubMed Central (PMC) - Free full-text research articles on neuropeptides and mood disorders
National Institute of Mental Health (NIMH) - Evidence-based information on depression and anxiety disorders
World Health Organization - Depression Fact Sheet - Global depression statistics and treatment information
ClinicalTrials.gov - Search for active and completed peptide clinical trials
For researchers serious about understanding and optimizing peptide protocols for mental health, SeekPeptides offers the most comprehensive resource available. Members access evidence-based protocol guides, detailed safety information, interaction databases, and a community of experienced researchers who have navigated these exact questions. When the science is complex and the stakes are personal, having access to structured guidance and peer support makes the difference between guessing and knowing.
In case I do not see you, good afternoon, good evening, and good night. May your neurotransmitters stay balanced, your research stay rigorous, and your protocols stay informed. Join SeekPeptides.