Mar 16, 2026

Sermorelin and semaglutide sound like they belong in the same conversation. They are both injectable peptides. They both show up in weight management discussions. They both promise body composition improvements that make people pay attention.
But these two compounds could not be more different in how they work, what they target, and who benefits most from using them.
One stimulates your pituitary gland to produce more growth hormone naturally. The other mimics a gut hormone that tells your brain you are full. One requires daily injections at bedtime. The other needs just one shot per week. One preserves muscle while slowly reshaping your body over months. The other delivers dramatic weight loss that shows up on the scale within weeks.
The confusion between them is understandable. Both appear in peptide therapy clinics. Both get recommended for people trying to lose fat. And both have passionate communities swearing by their results. But choosing between sermorelin and semaglutide without understanding the fundamental differences is like choosing between a marathon training plan and a sprint program without knowing what race you entered. The wrong pick does not just waste your time. It wastes months of injections, hundreds of dollars, and the opportunity to actually reach your goal.
This guide breaks down everything that separates these two peptides, from their molecular mechanisms to their real-world results, so you can make a decision based on evidence rather than hype. SeekPeptides has analyzed both compounds extensively, and the differences matter more than most guides admit.

What sermorelin actually does inside your body
Sermorelin is not growth hormone. This distinction matters more than anything else you will read about this peptide, because most of the confusion starts right here. Sermorelin is a growth hormone-releasing hormone analogue, a 29-amino-acid peptide that tells your pituitary gland to do its job better. It is the shortest synthetic fragment of GHRH that retains full biological activity, meaning researchers stripped it down to just the essential sequence needed to trigger growth hormone release.
Think of it this way. Your pituitary gland already knows how to make growth hormone. It has been doing it your entire life. But production declines with age, dropping roughly 14% per decade after age 30. By the time you reach 60, your growth hormone output may be a fraction of what it was at 25. Sermorelin does not replace what your body makes. It nudges the factory to produce more.
The pituitary feedback loop that keeps you safe
Here is where sermorelin gets interesting from a safety perspective. Unlike synthetic growth hormone injections that bypass your body regulatory systems entirely, sermorelin works through the same feedback loop your body already uses. When your pituitary releases enough growth hormone, a hormone called somatostatin steps in and says enough. This negative feedback mechanism means it is functionally difficult to overdose on sermorelin. Your body has a built-in ceiling.
A randomized study of adults aged 55 to 71 demonstrated this elegantly. Participants receiving nightly GHRH administration for 20 weeks showed significant increases in nocturnal growth hormone pulses and serum IGF-1 levels. But the increases stayed within physiological ranges. The body regulated itself. Men in the study experienced greater anabolic benefits, including improvements in insulin sensitivity and quality of life markers.
The practical result is a compound with one of the cleaner safety profiles among growth hormone-related peptides. Injection site reactions occur in about 1 in 6 users, usually mild redness or swelling that resolves quickly. Headaches happen occasionally. Flushing is possible. But the serious adverse event profile remains remarkably thin compared to direct growth hormone administration.
What growth hormone stimulation actually changes
When sermorelin successfully increases your natural growth hormone production, the downstream effects touch multiple systems. IGF-1 levels rise, which drives protein synthesis and muscle development. Fat metabolism shifts, with research showing improved breakdown of triglycerides stored in fat cells. Sleep quality often improves because growth hormone release naturally peaks during deep sleep, and sermorelin administered at bedtime aligns with this rhythm.
Recovery from exercise accelerates. Skin quality can improve over time. Energy levels tend to climb gradually. But none of this happens fast. Subjective improvements typically begin around weeks 3 to 6. Measurable changes in IGF-1 levels take 4 to 12 weeks. And the full body composition effects, the kind you can see in the mirror, usually require 3 to 6 months of consistent use.
This slow timeline is both the strength and weakness of sermorelin. The changes are sustainable and natural. But if you need visible results in 30 days, this is not the compound that delivers them.
The FDA approved sermorelin in 1997 for treating children with growth hormone deficiency. The original manufacturer discontinued production in 2008 for commercial reasons, not safety concerns. Today, sermorelin remains available through compounding pharmacies and is widely used in peptide therapy clinics for adult applications including anti-aging protocols and body composition optimization. For a deeper look at what sermorelin offers on its own, the sermorelin peptide benefits guide covers the full picture.
What semaglutide actually does inside your body
Semaglutide works through an entirely different biological system. It is a GLP-1 receptor agonist, meaning it mimics a hormone your gut naturally produces after you eat. When you consume food, your intestines release glucagon-like peptide-1. This hormone signals your brain that you are getting full, slows gastric emptying so food stays in your stomach longer, and helps regulate blood sugar by stimulating insulin release.
Natural GLP-1 breaks down within minutes. Semaglutide was engineered to last much longer, with a half-life of approximately 7 days. That extended duration is why semaglutide works as a once-weekly injection rather than requiring daily doses. The molecule was modified with a fatty acid chain that binds to albumin in your blood, protecting it from rapid degradation and allowing it to circulate and activate GLP-1 receptors continuously.
The appetite suppression mechanism
The weight loss from semaglutide comes primarily from reduced caloric intake. Users consistently report that their relationship with food fundamentally changes. Cravings diminish. Portion sizes shrink naturally. The constant mental chatter about food, what to eat next, when to snack, whether to have seconds, goes quiet.
Clinical trials tell the story in numbers. The STEP 1 trial showed participants lost an average of 14.9% of their body weight over 68 weeks at the 2.4mg dose. Some participants lost more than 20%. These are results that rival bariatric surgery outcomes, achieved through a weekly injection and lifestyle modifications.
But the mechanism goes beyond simple appetite control. Semaglutide affects reward pathways in the brain, reducing the hedonic drive to eat. It slows gastric emptying, so meals feel more satisfying for longer. And it improves glycemic control, which stabilizes energy levels and reduces the blood sugar crashes that trigger hunger. If you have ever wondered whether semaglutide suppresses appetite right away, the answer is usually yes, though the full effect builds over the dose escalation period.
Beyond weight loss
Semaglutide research has expanded well beyond obesity treatment. Cardiovascular outcomes trials have shown reduced rates of major adverse cardiac events. Studies suggest potential benefits for liver health, with improvements in non-alcoholic fatty liver disease markers. The compound is being investigated for kidney disease, Alzheimer disease, and addiction.
For most people considering semaglutide, though, the primary appeal remains fat loss. The compound delivers consistent, significant, and measurable weight reduction that often begins within the first week of treatment. Understanding how semaglutide makes you feel during those early days helps set realistic expectations. The week-by-week timeline shows how results typically unfold.

Mechanism comparison: two completely different biological targets
Placing sermorelin and semaglutide side by side reveals just how different these compounds are at the molecular level. They do not compete with each other. They do not even operate in the same biological neighborhood.
Feature | Sermorelin | Semaglutide |
|---|---|---|
Drug class | GHRH analogue | GLP-1 receptor agonist |
Primary target | Pituitary gland | GLP-1 receptors (gut, brain, pancreas) |
Hormone stimulated | Growth hormone (GH) | Mimics GLP-1 |
Downstream marker | IGF-1 increase | Reduced appetite, insulin secretion |
Primary effect | Body recomposition, recovery, anti-aging | Weight loss, glycemic control |
Feedback regulation | Yes (somatostatin limits GH) | Dose-dependent (no natural ceiling) |
Amino acid length | 29 amino acids | 31 amino acids (modified) |
The growth hormone pathway that sermorelin activates is fundamentally anabolic. It builds tissue. It repairs cells. It promotes lean mass development while encouraging fat breakdown as a secondary effect. This is why athletes and active individuals gravitate toward growth hormone peptides. The recovery benefits alone can transform training capacity.
The GLP-1 pathway that semaglutide activates is fundamentally catabolic in its practical effect. It reduces caloric intake. It shifts energy balance toward deficit. It drives weight loss through appetite modulation rather than metabolic acceleration. This is why people with significant fat to lose see dramatic results on semaglutide. The compound directly addresses the root challenge of overeating.
Where the pathways overlap
Despite targeting different systems, both pathways influence body composition. Both can reduce body fat percentage. Both affect energy levels, though through different mechanisms. And both interact with metabolic health markers like insulin sensitivity and lipid profiles.
Growth hormone, stimulated by sermorelin, improves insulin sensitivity through increased lean muscle mass and direct metabolic effects. Semaglutide improves insulin sensitivity through weight loss and direct pancreatic effects. The end result, better blood sugar control, looks similar on paper but arrives through entirely different routes.
This overlap is actually what makes the combination conversation interesting. More on that later. But understanding that these are complementary rather than competing pathways is critical for making an informed choice between them.
Weight loss outcomes: the numbers tell different stories
If your primary goal is seeing a lower number on the scale as quickly as possible, semaglutide wins this comparison decisively. The clinical evidence is overwhelming and consistent.
Semaglutide weight loss data
The STEP trial program, spanning multiple large-scale randomized controlled trials, established semaglutide as one of the most effective pharmacological weight loss interventions available. Key results include an average body weight reduction of 14.9% at the 2.4mg weekly dose over 68 weeks. Some participants achieved weight loss exceeding 20% of starting body weight. Significant reductions in waist circumference, blood pressure, and inflammatory markers accompanied the weight loss.
Most users begin noticing reduced appetite within the first one to two weeks. Measurable weight loss typically begins during the first week, with the most rapid phase occurring during months two through six. By month three, many users have lost 5 to 10% of their body weight. The one-month results already show meaningful progress for most people.
However, the weight lost on semaglutide is not exclusively fat. Studies consistently show that approximately 30 to 40% of weight lost on GLP-1 agonists comes from lean tissue, primarily muscle. This is a significant concern, especially for older adults and anyone who values strength and metabolic health alongside fat loss. The semaglutide tips guide covers strategies to mitigate this issue.
Sermorelin body composition changes
Sermorelin approaches body composition from the opposite direction. Rather than creating a large caloric deficit through appetite suppression, sermorelin stimulates growth hormone production that gradually shifts the ratio of lean mass to fat mass.
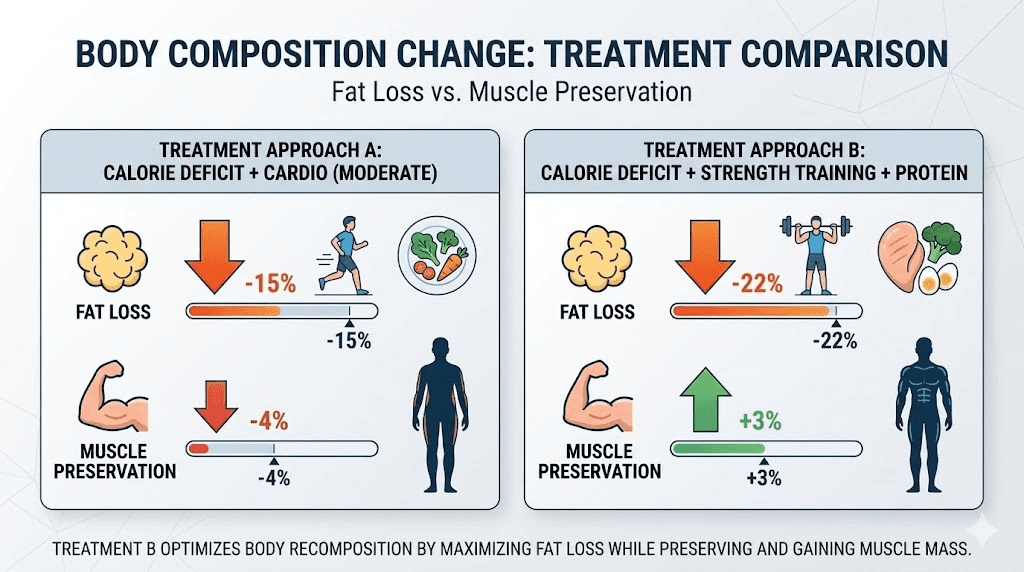
A pivotal study in older adults receiving nightly GHRH administration for 20 weeks showed reduced body fat and improved lean body mass. The total weight change on the scale was modest compared to semaglutide. But the composition of that change matters enormously. Participants gained muscle while losing fat, a true recomposition that semaglutide alone struggles to achieve.
The trade-off is speed. Where semaglutide users might lose 15 pounds in their first month, sermorelin users might see 3 to 5 pounds of fat loss over the same period, potentially offset by muscle gain that masks the fat loss on the scale. For someone focused exclusively on the scale number, this feels like failure. For someone focused on body composition and long-term metabolic health, it looks like exactly the right approach. If you want to see what the transformation actually looks like over time, the sermorelin before and after results provide visual evidence.
The muscle preservation question
This is where the comparison gets genuinely important for long-term health outcomes. Muscle mass is not just about aesthetics. It is the single strongest predictor of metabolic health, functional independence in aging, and all-cause mortality risk. Losing large amounts of muscle during weight loss creates a metabolic trap where your body requires fewer calories but your appetite eventually returns to previous levels.
Sermorelin directly addresses muscle preservation through growth hormone stimulation. GH promotes protein synthesis, supports muscle fiber repair, and maintains lean tissue even during caloric restriction. This is why peptides for weight loss and muscle gain often include growth hormone secretagogues as foundational compounds.
Semaglutide does not directly preserve muscle. The weight loss it produces follows standard caloric restriction patterns where both fat and muscle are lost. Resistance training and adequate protein intake can reduce muscle loss during semaglutide treatment, but they cannot eliminate it entirely. The diet recommendations during semaglutide treatment and food guides emphasize protein prioritization for exactly this reason.
Dosing protocols: daily commitment versus weekly convenience
The practical experience of using these compounds day-to-day differs substantially. Understanding the dosing requirements helps set realistic expectations for adherence and lifestyle impact.
Sermorelin dosing protocol
Sermorelin requires daily subcutaneous injections, typically administered at bedtime. The bedtime timing aligns with the natural peak in growth hormone release that occurs during deep sleep. By injecting sermorelin before bed, you amplify a process your body already initiates naturally.
Standard dosing ranges from 200 to 500mcg per day for most adult protocols. Some practitioners prescribe up to 1 to 2mg daily for specific research applications. The typical approach starts conservatively, often at 200 to 300mcg, and adjusts based on IGF-1 levels and clinical response over 4 to 12 weeks.
Some protocols incorporate cycling, using a 5-days-on, 2-days-off schedule to maintain pituitary sensitivity and prevent receptor downregulation. This cycling approach mimics natural hormonal rhythms and may optimize long-term results, though direct comparison data between continuous and cycled dosing remains limited. The sermorelin cost guide breaks down what to expect financially across different dosing strategies.
Phase | Dose | Duration | Goal |
|---|---|---|---|
Initiation | 200-300mcg daily at bedtime | Weeks 1-4 | Assess tolerance and response |
Optimization | 300-500mcg daily at bedtime | Weeks 5-12 | Achieve target IGF-1 levels |
Maintenance | 200-500mcg daily, possibly cycled | Months 3-6+ | Sustain benefits long-term |
For men specifically interested in pairing sermorelin with other growth hormone peptides, the sermorelin ipamorelin blend guide covers combination protocols that many clinics offer.
Semaglutide dosing protocol
Semaglutide follows a standardized dose escalation schedule designed to minimize gastrointestinal side effects while building toward the therapeutic dose. The once-weekly injection schedule is significantly more convenient than daily dosing.
Phase | Dose | Duration | Purpose |
|---|---|---|---|
Week 1-4 | 0.25mg weekly | 4 weeks | Tolerance building |
Week 5-8 | 0.5mg weekly | 4 weeks | Early therapeutic effect |
Week 9-12 | 1.0mg weekly | 4 weeks | Intermediate dose |
Week 13-16 | 1.7mg weekly | 4 weeks | Approaching full dose |
Week 17+ | 2.4mg weekly | Ongoing | Full therapeutic dose |
The dose escalation takes approximately 16 to 20 weeks to reach the full 2.4mg weekly dose. Some users achieve their weight loss goals at lower doses and never need the maximum. Others require the full dose for adequate appetite suppression. Understanding semaglutide dosage in units helps when working with compounded formulations where concentrations vary. The semaglutide dosage calculator makes conversion straightforward.
For those using compounded semaglutide, reconstitution is an additional step. The reconstitution guide covers the process, and the reconstitution calculator ensures accurate mixing. Proper storage matters too, as the semaglutide storage guide explains how long the compound remains viable.
Choosing the best time of day to take semaglutide is less critical than with sermorelin, since the weekly dosing means the compound is active continuously. Most users simply pick a consistent day and time that fits their schedule.
Side effect profiles: what to actually expect
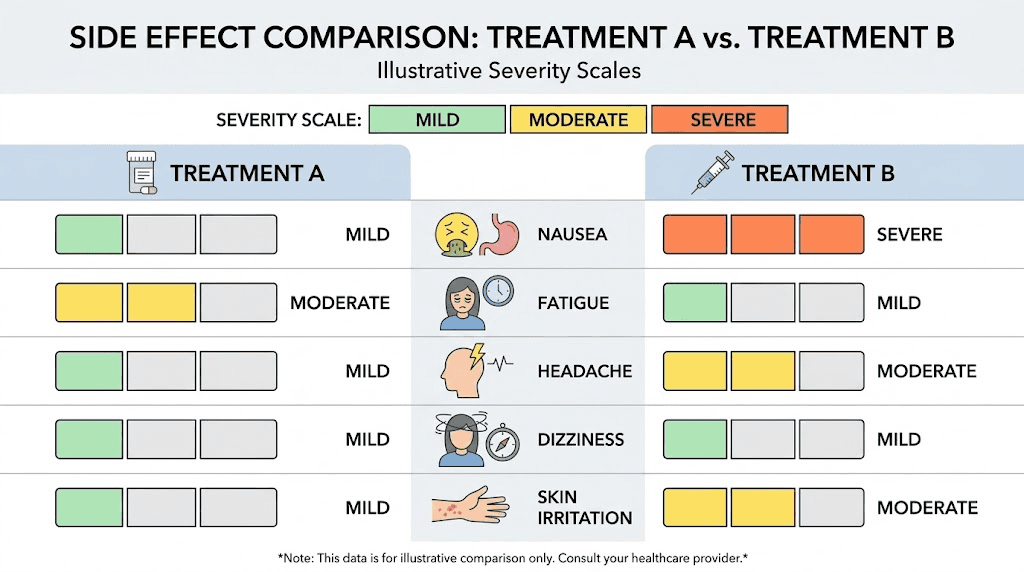
Side effects represent one of the starkest contrasts between these two compounds. Sermorelin is remarkably well tolerated. Semaglutide is effective but comes with a more demanding adjustment period.
Sermorelin side effects
The most common side effect of sermorelin is injection site irritation, occurring in roughly 1 out of every 6 users. This typically presents as mild redness, itching, or swelling at the injection site that resolves within hours. Beyond local reactions, some users report occasional headaches, flushing, or dizziness. These effects are generally transient and mild.
Rare side effects include difficulty swallowing, hives, and chest tightness, though these are uncommon enough that large-scale safety data has not linked sermorelin to clinically significant adverse events. The built-in somatostatin feedback mechanism provides a natural safety ceiling that exogenous growth hormone lacks.
Most users describe sermorelin as something they barely notice. The bedtime injection becomes routine quickly, and side effects are either absent or minor enough to ignore.
Semaglutide side effects
Semaglutide carries a more significant side effect burden, particularly during the early weeks and dose escalation phases. Gastrointestinal effects dominate the profile.
Nausea is the most commonly reported side effect, affecting up to 44% of users in clinical trials at the 2.4mg dose. It typically peaks during dose increases and gradually improves as the body adjusts. Acid reflux and bloating are common companions. Constipation and diarrhea can alternate, sometimes within the same week. The slowed gastric emptying that helps with appetite control also means food sits in the stomach longer than usual, contributing to these symptoms.
Fatigue affects a meaningful subset of users, particularly during caloric deficit. Dizziness can occur. Some users report sleep disruption. Hair thinning has been reported, likely related to rapid weight loss rather than the compound itself, as explored in the GLP-1 hair loss guide. And less commonly discussed effects like menstrual changes warrant attention for female users.
The good news is that most gastrointestinal side effects improve significantly after 4 to 8 weeks at a given dose. The dose escalation schedule exists specifically to minimize these effects by giving the body time to adapt. Understanding how long after taking semaglutide side effects appear helps set expectations.
Side effect | Sermorelin | Semaglutide |
|---|---|---|
Nausea | Rare, mild | Common (up to 44%), improves over time |
Injection site reaction | 1 in 6 users, mild | Occasional, mild |
Headache | Occasional | Occasional |
Constipation | Very rare | Common (24%) |
Diarrhea | Very rare | Common (30%) |
Fatigue | Rare (often improved energy) | Moderate (11%) |
Hair thinning | Not reported | Reported with rapid weight loss |
Sleep effects | Often improved sleep | Variable, possible disruption |
Severity overall | Minimal | Moderate, time-limited |
Timeline to results: patience versus speed
The timeline differences between these two compounds create entirely different user experiences. Understanding what to expect, and when to expect it, prevents premature abandonment of either approach.
When sermorelin starts working
Sermorelin operates on biological timescales that require patience. The compound must first stimulate your pituitary gland to increase growth hormone production. Then that growth hormone must circulate and produce its downstream effects through IGF-1 and other mediators. The cascade takes time.
Weeks 1 to 3: Most users notice improved sleep quality first. Deeper sleep, more vivid dreams, and easier time falling asleep are common early signs that sermorelin is working. Some report subtle energy improvements.
Weeks 3 to 6: Subjective improvements become more apparent. Better recovery from exercise. More consistent energy throughout the day. Some notice skin quality beginning to improve.
Weeks 6 to 12: Measurable changes start appearing. IGF-1 blood tests show increases. Body composition begins shifting, though the scale may not change dramatically because muscle gain can offset fat loss.
Months 3 to 6: The full benefits become evident. Visible changes in body composition. Improved muscle tone. Reduced body fat, particularly in stubborn areas. Enhanced exercise capacity and recovery. This is the timeline most peptides require to demonstrate their full potential.
When semaglutide starts working
Semaglutide delivers results on a dramatically compressed timeline. Most users notice effects within the first few days of their initial dose.
Days 1 to 7: Appetite reduction is often noticeable within the first week, even at the low starting dose. Some users report feeling full faster at meals and reduced between-meal hunger. Weight loss of 1 to 3 pounds may occur simply from eating less.
Weeks 2 to 4: The appetite suppression effect strengthens as the compound reaches steady-state levels. First-month results typically show 3 to 8 pounds of weight loss depending on starting weight and dose.
Months 1 to 3: Weight loss accelerates as doses increase through the escalation schedule. Most users are losing 1 to 2 pounds per week consistently. The week-by-week progression shows this pattern clearly.
Months 3 to 6: This is typically the period of maximum weight loss velocity. Users on the full 2.4mg dose can expect total weight loss of 10 to 15% of starting body weight by the six-month mark.
Months 6 to 12+: Weight loss continues but decelerates as the body approaches a new equilibrium. Some users hit a plateau and need strategy adjustments. Understanding how long to stay on semaglutide becomes relevant at this stage.
Milestone | Sermorelin | Semaglutide |
|---|---|---|
First noticeable effect | 1-3 weeks (sleep) | 1-7 days (appetite) |
Measurable body changes | 6-12 weeks | 2-4 weeks |
Significant results | 3-6 months | 2-4 months |
Peak benefit timeline | 6-12 months | 6-12 months |
Can you take sermorelin and semaglutide together
This is the question that comes up most frequently once people understand what each compound does individually. And the answer is more nuanced than a simple yes or no.
The complementary pathway argument
Because sermorelin and semaglutide operate through completely separate biological pathways, there is no direct pharmacological interaction between them. Sermorelin stimulates the pituitary gland through GHRH receptors. Semaglutide activates GLP-1 receptors in the gut, brain, and pancreas. These systems do not compete for the same receptors, and neither compound blocks or enhances the other at the receptor level.
The theoretical case for combining them is compelling. Semaglutide handles the heavy lifting for fat loss through appetite suppression and caloric deficit. Sermorelin addresses the biggest weakness of GLP-1 therapy by preserving and potentially building lean muscle mass through growth hormone stimulation. Together, they could deliver weight loss that is both substantial and composition-favorable.
What the evidence shows
Large-scale clinical trials specifically evaluating sermorelin and semaglutide in combination do not yet exist. The evidence comes primarily from clinical practice reports and studies examining GLP-1 agonists combined with muscle-protective agents more broadly.
What these clinical observations suggest is promising. Patients using both compounds tend to show superior body composition outcomes compared to either compound alone. Fat loss matches or exceeds semaglutide monotherapy. Lean mass preservation is significantly better than semaglutide alone. Recovery and energy levels are maintained despite the caloric deficit that semaglutide creates.
The timing works logistically as well. Semaglutide is injected once weekly at any time. Sermorelin is injected daily at bedtime. There is no scheduling conflict. Some practitioners recommend separating the injection sites when both are administered on the same day.
For researchers interested in peptide stacking strategies, this combination represents one of the more evidence-supported pairings. The peptide stack calculator can help evaluate compatibility. And for those already on semaglutide who want to understand related growth hormone peptides, resources on CJC-1295 and ipamorelin provide context on alternatives to sermorelin within the GH secretagogue class.
SeekPeptides members access detailed combination protocol guides that cover timing, dosing adjustments, and monitoring recommendations for multi-peptide approaches. This level of specificity matters when combining compounds that affect different hormonal systems.

Who should consider sermorelin
Sermorelin fits a specific profile that does not overlap much with the typical semaglutide candidate. Understanding whether you match this profile saves months of misaligned expectations.
Adults experiencing age-related growth hormone decline. If you are over 35 and noticing decreased recovery from exercise, reduced muscle tone despite consistent training, increased body fat that was not there before, or declining sleep quality, sermorelin addresses the potential root cause rather than masking symptoms.
Athletes and active individuals prioritizing recovery. The growth hormone stimulation from sermorelin accelerates tissue repair, reduces recovery time between training sessions, and supports joint and connective tissue health. For people who train hard, the recovery benefits often matter more than the body composition changes. Understanding the broader category of fat burning peptides for men and peptides for athletic performance helps contextualize where sermorelin fits.
People seeking body recomposition rather than weight loss. If your goal is building muscle while losing fat, and the number on the scale matters less than how you look and perform, sermorelin aligns with that objective. The gradual shift toward more muscle and less fat is exactly what recomposition means.
Those who want sustainable, natural hormonal optimization. Because sermorelin works through your own pituitary gland and is regulated by natural feedback mechanisms, the results integrate into your existing hormonal physiology rather than overriding it. People who prefer this approach over synthetic hormone replacement often gravitate toward sermorelin and similar hormone-balancing peptides.
Anyone concerned about the side effect burden of GLP-1 agonists. If the gastrointestinal effects of semaglutide are a dealbreaker, sermorelin offers a dramatically gentler experience. The mild injection site reactions that represent the most common side effect pale in comparison to the nausea, constipation, and digestive upheaval that accompanies GLP-1 therapy.
Who should consider semaglutide
Semaglutide addresses a different set of needs and fits a different profile. Its strengths lie precisely where sermorelin falls short.
People with significant weight to lose. If you need to lose 30, 50, or 100+ pounds, semaglutide delivers the magnitude of weight loss that makes a meaningful difference. Sermorelin simply cannot produce weight loss at this scale because it does not directly reduce caloric intake.
Those struggling with appetite control and food-related behaviors. Semaglutide uniquely addresses the psychological and neurological drivers of overeating. If your weight challenges stem primarily from difficulty controlling portions, constant food cravings, or an inability to feel satisfied after meals, semaglutide targets these specific mechanisms.
People with type 2 diabetes or prediabetes. The glycemic control benefits of semaglutide provide dual value for people managing blood sugar alongside weight. Sermorelin does not directly address glucose regulation in the same clinically validated way.
Anyone who values dosing convenience. Once-weekly injections are simply easier to maintain than daily injections. For people with busy schedules, travel demands, or injection fatigue, the weekly semaglutide protocol is more sustainable long-term.
Those who need visible results quickly to maintain motivation.
The rapid onset of appetite suppression and early weight loss on semaglutide provides positive feedback that keeps people engaged with their health goals. If you have historically abandoned programs because results came too slowly, semaglutide solves that problem. For those just starting out, understanding how fast semaglutide works and what to expect early on helps calibrate expectations.
For those exploring semaglutide options, understanding the difference between brand-name and compounded semaglutide matters for access and cost. And if semaglutide alone does not deliver the desired results, alternatives like tirzepatide represent the next step in GLP-1 therapy.
Making the right choice: a practical decision framework
Instead of asking which compound is better, ask which compound matches your specific situation. The decision framework below maps common goals to the compound most likely to deliver.
Your primary goal | Best choice | Why |
|---|---|---|
Lose 20+ pounds of fat | Semaglutide | Produces significant caloric deficit through appetite suppression |
Build muscle while losing fat | Sermorelin | GH stimulation promotes lean mass while fat decreases |
Improve recovery and performance | Sermorelin | GH directly enhances tissue repair and exercise adaptation |
Control blood sugar | Semaglutide | Direct glycemic control through GLP-1 pathway |
Anti-aging and longevity | Sermorelin | Restores declining GH levels through natural pituitary stimulation |
Minimize side effects | Sermorelin | Dramatically milder side effect profile |
Fastest visible results | Semaglutide | Noticeable appetite and weight changes within days to weeks |
Convenient dosing schedule | Semaglutide | Once weekly vs daily injections |
Maximize fat loss AND preserve muscle | Both (combination) | Complementary pathways address both goals simultaneously |
Notice that the last row suggests using both compounds together. For people with the budget and commitment, the combination approach may represent the optimal strategy. Semaglutide drives the caloric deficit and fat loss. Sermorelin protects lean tissue and supports recovery. Neither compound interferes with the other.
But if choosing one, the decision usually comes down to a single question. Is your primary challenge losing weight, or is it optimizing body composition and performance? Weight loss points toward semaglutide. Composition and performance point toward sermorelin.

Cost considerations
Budget plays a practical role in this decision that deserves honest discussion. Neither compound is cheap, and the ongoing nature of both treatments means costs accumulate over months.
Sermorelin through compounding pharmacies typically costs less per month than brand-name semaglutide. However, the daily dosing means you go through product faster. Monthly costs vary based on dosage and supplier, but the sermorelin cost breakdown provides current ranges.
Semaglutide costs depend heavily on whether you use brand-name products like Ozempic or Wegovy, which can exceed $1,000 monthly without insurance, or compounded versions that reduce costs significantly. The semaglutide buying guide covers sourcing options, and the peptide cost calculator helps estimate monthly expenses across different peptide protocols.
Insurance coverage adds another variable. Brand-name semaglutide may be partially covered for diabetes or obesity indications through some plans. Sermorelin is rarely covered by insurance for adult use. Compounded versions of both typically require out-of-pocket payment. Understanding GLP-1 insurance coverage helps navigate this landscape.
The combination approach doubles the financial commitment. Running both sermorelin and semaglutide simultaneously requires budgeting for two compounds, which may not be sustainable for everyone. If budget is a constraint, prioritizing based on your primary goal using the decision framework above makes more financial sense than trying to do both at a lower dose.
Storage, handling, and practical considerations
Both compounds require refrigeration and proper handling to maintain potency. The daily routine with sermorelin demands more frequent preparation than the weekly semaglutide protocol.
Sermorelin should be refrigerated after reconstitution and protected from light. Daily use means you interact with the vial every night, so maintaining sterile technique with each draw becomes habitual. Most sermorelin vials last 2 to 4 weeks when stored properly.
Semaglutide, whether in pen or vial form, also requires refrigeration. Compounded semaglutide has a limited shelf life after reconstitution, typically lasting several weeks in the fridge. Understanding storage requirements and what happens if the compound gets warm, as covered in the hot shipping guide and temperature exposure guide, prevents potency loss.
Travel presents different challenges for each compound. Daily sermorelin injections mean you must pack supplies for every night away from home. Semaglutide weekly dosing means you might be able to time your dose before or after travel. The traveling with semaglutide guide covers TSA rules, cold storage solutions, and scheduling strategies.
What happens when you stop
The sustainability of results after discontinuing each compound is a critical consideration that most comparison articles ignore entirely.
Stopping sermorelin gradually returns growth hormone production to pre-treatment levels. The muscle gained during treatment is maintainable through continued resistance training and adequate nutrition, even without sermorelin. The metabolic benefits persist as long as the lean mass is maintained. In other words, the structural changes sermorelin facilitates can outlast the treatment itself, provided you continue the lifestyle habits that support them.
Stopping semaglutide is more complicated. Research shows that weight regain is common and significant after discontinuation. A study published in the journal Diabetes, Obesity and Metabolism found that participants regained approximately two-thirds of the weight they had lost within one year of stopping semaglutide. The appetite suppression disappears. The cravings return. Caloric intake drifts back toward pre-treatment levels. Understanding semaglutide withdrawal symptoms and weight maintenance strategies becomes essential for anyone planning to eventually stop.
This difference in post-treatment sustainability is one of the strongest arguments for sermorelin in people who value long-term outcomes. It is also one of the strongest arguments for the combination approach, where sermorelin helps build the metabolic foundation (lean muscle mass, improved hormonal milieu) that makes weight maintenance possible even after semaglutide is discontinued.
Comparing sermorelin to other growth hormone peptides
If sermorelin interests you but you want to understand the full landscape, several related compounds deserve mention. Each stimulates growth hormone through slightly different mechanisms.
Ipamorelin is a growth hormone secretagogue that works through the ghrelin receptor rather than the GHRH receptor. It produces a cleaner GH pulse with fewer side effects than many alternatives. The sermorelin-ipamorelin combination is one of the most popular blends in peptide therapy clinics.
CJC-1295 is a modified GHRH analogue with a longer half-life than sermorelin. The ipamorelin vs CJC-1295 comparison breaks down how these two are often paired together.
Hexarelin is a more potent growth hormone secretagogue with additional cardiovascular benefits but stronger side effects and a tendency toward desensitization with prolonged use.
Each of these peptides approaches growth hormone stimulation from a different angle. The complete peptide reference guide covers all available options, and the peptide dosage chart provides dosing references across the category.
Comparing semaglutide to other GLP-1 options
Similarly, semaglutide is not the only GLP-1 option available. Understanding the alternatives provides context for whether semaglutide specifically is the right GLP-1 agonist for you.
Tirzepatide (brand name Mounjaro/Zepbound) is a dual GIP/GLP-1 receptor agonist that has shown even greater weight loss efficacy than semaglutide alone in head-to-head trials. The semaglutide vs tirzepatide comparison and the side-by-side effects analysis cover these differences in detail.
Retatrutide is a triple agonist (GIP/GLP-1/glucagon) currently in clinical development showing up to 24% weight loss. Articles on retatrutide pricing and retatrutide vs Ozempic explore this next-generation option.
Oral formulations of GLP-1 compounds represent an emerging alternative for people who dislike injections. The oral semaglutide guide and sublingual options review these approaches.
For anyone considering switching between GLP-1 options, the conversion charts and switching guides provide dosing equivalence information.
Lifestyle factors that influence your results with either compound
Neither sermorelin nor semaglutide works in a vacuum. Lifestyle factors significantly influence outcomes with both compounds, though the specific factors that matter most differ.
Nutrition considerations
With sermorelin, nutrition should emphasize adequate protein intake (1.0 to 1.6g per kg of body weight) to support the muscle-building processes that growth hormone facilitates. Without sufficient protein, the anabolic signal sermorelin creates goes unanswered. Caloric intake does not need to be restricted. In fact, slight caloric surpluses may enhance the muscle-building effects.
With semaglutide, the primary nutritional challenge is eating enough. The appetite suppression can be so strong that users undereat to the point of nutritional deficiency. Protein prioritization becomes critical to preserve muscle during weight loss. The diet plan for semaglutide users, recommended food lists, and foods to avoid provide specific guidance. The probiotic recommendations and protein shake options address common nutritional gaps.
Exercise considerations
With sermorelin, exercise is essentially required to capture the full benefits. Growth hormone stimulation without a training stimulus produces suboptimal results. Resistance training is particularly important because it provides the mechanical signal that directs growth hormone effects toward muscle building.
With semaglutide, exercise is strongly recommended for muscle preservation but not required for weight loss. Many users lose weight on semaglutide without exercise. However, the quality of weight loss (ratio of fat to muscle) improves dramatically with a structured resistance training program.
Sleep
Sleep quality interacts with both compounds in important ways. Sermorelin administered at bedtime enhances deep sleep phases, which in turn amplifies natural growth hormone release. Poor sleep undermines sermorelin effectiveness by disrupting the hormonal environment the compound is trying to optimize.
Semaglutide does not directly affect sleep, but the caloric restriction it creates can disrupt sleep patterns in some users. Conversely, weight loss itself often improves sleep quality by reducing sleep apnea risk and overall inflammation.
Supplements and companion compounds
Users of both compounds often explore complementary supplements. For semaglutide users, B12 supplementation, glycine, L-carnitine, and niacinamide are commonly discussed companions. For those exploring whether combining different classes of weight loss compounds makes sense, the phentermine and semaglutide combination guide and phentermine comparison cover that territory.
For sermorelin users, the supplement landscape focuses more on optimizing growth hormone release. Amino acids like arginine and glutamine, adequate zinc, and vitamin D all support healthy pituitary function and may enhance sermorelin response.
Understanding the broader peptide landscape
Both sermorelin and semaglutide exist within a larger ecosystem of legal peptides used for various health optimization goals. Knowing where these two compounds sit in the broader landscape helps inform decision-making.
Growth hormone peptides like sermorelin occupy one category, alongside compounds like MOTS-c for metabolic health, DSIP for sleep optimization, and AOD-9604 for targeted fat loss. These peptides work through diverse mechanisms but share the common thread of signaling your body to optimize its own processes.
GLP-1 agonists like semaglutide represent a different pharmaceutical category entirely. They are receptor agonists that mimic existing hormones rather than stimulating endogenous production. The distinction between research peptides and pharmaceutical-grade compounds becomes relevant here, as semaglutide has extensive FDA-approved clinical trial data behind it while sermorelin operates primarily in the compounding pharmacy space for adult applications.
For those interested in comparing across categories, the peptides vs TRT comparison and peptides vs SARMs comparison provide additional context. The general peptide cost guide helps budget across different protocols, and understanding drug testing implications matters for competitive athletes.
For researchers serious about understanding peptide protocols at a deeper level, SeekPeptides provides comprehensive guides, dosage calculators, and evidence-based protocol recommendations that go far beyond what free resources offer.
Injection technique and administration
Both sermorelin and semaglutide are administered via subcutaneous injection, but the practical details differ enough to warrant separate discussion.
Sermorelin is typically injected into the abdominal fat pad or the fatty tissue of the thigh, using an insulin syringe. The bedtime administration requires drawing the peptide from a reconstituted vial each evening. Proper reconstitution technique matters for maintaining potency. The peptide mixing guide and reconstitution calculator walk through this process step by step.
Semaglutide in pen form requires no reconstitution and minimal preparation. Compounded semaglutide in vial form requires reconstitution similar to sermorelin. Injection technique with a syringe is straightforward, and choosing the best injection site helps optimize absorption and minimize discomfort. Many users prefer the abdominal injection site for consistency.
For users new to self-injection, the peptide injection basics guide covers technique, equipment selection, and sterile protocol. The injection pen guide reviews pen devices that simplify the process for both compounds. Understanding proper storage after reconstitution prevents potency loss between doses.
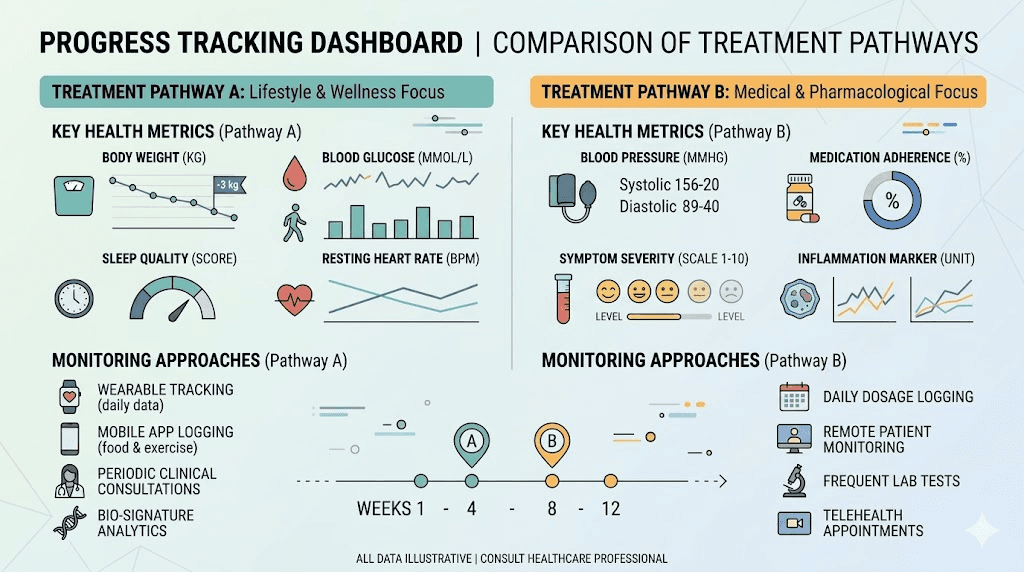
Monitoring your progress
Measuring whether your chosen compound is actually working requires different markers depending on which one you selected.
For sermorelin, the primary objective marker is serum IGF-1 levels. Baseline testing before starting sermorelin establishes your reference point. Follow-up testing at 6 to 12 weeks shows whether the compound is successfully stimulating growth hormone production. Body composition measurements through DEXA scans provide the most accurate picture of lean mass and fat mass changes. The scale alone is misleading with sermorelin because muscle gain can offset fat loss.
For semaglutide, monitoring is more straightforward. Body weight measured consistently under the same conditions provides the primary metric. Waist circumference adds a composition element. Blood work tracking HbA1c, fasting glucose, and lipid panels shows metabolic improvements. Understanding what semaglutide affects in blood work helps interpret results accurately.
Both compounds benefit from before-and-after progress photos taken under consistent lighting and conditions. For semaglutide users, the before and after gallery shows typical transformations. For sermorelin users, the sermorelin results documentation sets realistic visual expectations.
Special populations and considerations
Certain populations face unique considerations when choosing between these compounds.
Women of reproductive age should note that both compounds require careful consideration regarding pregnancy and breastfeeding. Semaglutide is contraindicated during pregnancy and should be stopped at least two months before conception. The effects on menstrual cycles can also affect fertility planning. Sermorelin similarly lacks safety data for use during pregnancy, and growth hormone modulation during pregnancy is generally avoided.
Older adults may benefit most from sermorelin precisely because age-related growth hormone decline is the primary condition it addresses. However, older adults with significant weight-related health conditions may need the more dramatic intervention that semaglutide provides.
People with thyroid conditions should be aware that growth hormone can influence thyroid hormone metabolism. Monitoring thyroid function during sermorelin therapy is advisable. Semaglutide does not directly affect thyroid function, though rapid weight loss can alter thyroid hormone requirements. For those researching GLP-1 interactions with thyroid conditions, the Hashimoto and GLP-1 guide provides specific insights.
People currently on hormone replacement therapy should discuss sermorelin with their provider as growth hormone optimization interacts with testosterone, estrogen, and thyroid replacement.
The peptides versus TRT analysis covers some of these interaction dynamics. Understanding how peptides affect testosterone specifically helps male users make informed decisions.
People with diabetes have a clearer path with semaglutide, which has extensive clinical data supporting its use in type 2 diabetes management. Sermorelin can affect insulin sensitivity and glucose metabolism, which may require monitoring and adjustment of diabetes medications.
The bottom line
Sermorelin and semaglutide are not interchangeable options on a spectrum. They are fundamentally different tools for fundamentally different jobs.
Sermorelin rebuilds. It restores declining growth hormone production, supports muscle development, enhances recovery, and promotes the kind of gradual body recomposition that serves long-term health. It works slowly. It demands daily commitment. And it delivers changes that are sustainable because they are built on your own hormonal physiology.
Semaglutide reduces. It suppresses appetite, creates caloric deficit, and drives substantial weight loss that transforms your body shape and metabolic health markers. It works quickly. It requires minimal dosing effort. And it delivers changes that are dramatic but require ongoing treatment to maintain.
The best choice depends entirely on what you need most right now. And for some people, the best choice is both.
For researchers who want personalized guidance on selecting the right peptide protocol, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, precision calculators, and a community of thousands who have navigated these exact decisions. SeekPeptides members access detailed protocol builders that account for individual goals, body composition, and compound interactions that generic guides cannot provide.
Frequently asked questions
Is sermorelin better than semaglutide for weight loss?
No. Semaglutide is significantly more effective for pure weight loss. Clinical trials show 14.9% average body weight reduction with semaglutide versus modest scale changes with sermorelin. However, sermorelin produces better body recomposition outcomes by preserving lean mass while reducing fat.
Can I switch from semaglutide to sermorelin?
Yes, though the transition requires planning. Stopping semaglutide typically leads to appetite returning and potential weight regain. Starting sermorelin simultaneously or before discontinuing semaglutide may help preserve lean mass during the transition. Work with a healthcare provider to time the switch appropriately.
How long does sermorelin take to show results?
Sleep improvements often appear within 1 to 3 weeks. Subjective energy and recovery improvements follow around weeks 3 to 6. Measurable body composition changes typically require 3 to 6 months of consistent daily dosing. The full benefits of sermorelin unfold over 6 to 12 months, which is significantly slower than semaglutide timelines.
Does sermorelin cause the same nausea as semaglutide?
No. Nausea is rare with sermorelin because it operates through the growth hormone pathway rather than the GLP-1 pathway that affects gastric motility. The most common side effect of sermorelin is mild injection site irritation in about 1 in 6 users. The GI side effects that characterize semaglutide treatment are largely absent with sermorelin.
Will I regain weight after stopping sermorelin?
The body composition improvements from sermorelin can be maintained through continued exercise and nutrition after discontinuation. Because sermorelin builds lean mass rather than simply suppressing appetite, the metabolic benefits persist as long as you maintain the muscle you gained. This differs from semaglutide, where discontinuation often leads to weight regain.
Is it safe to take sermorelin and semaglutide at the same time?
They operate through separate biological pathways with no known direct pharmacological interaction. Clinical observations of combination use suggest benefits for both fat loss and muscle preservation. However, combination protocols should always be supervised by a healthcare provider who can monitor hormonal levels and adjust dosing. The peptide stacking guide discusses combination safety principles.
Which is cheaper, sermorelin or semaglutide?
Compounded sermorelin typically costs less per month than brand-name semaglutide. However, compounded semaglutide can be price-competitive with sermorelin depending on the pharmacy. The peptide cost calculator helps compare expenses. Brand-name semaglutide (Ozempic, Wegovy) without insurance can exceed $1,000 monthly, making it substantially more expensive than either compounded option.
Does sermorelin help with anti-aging?
Yes. Sermorelin is one of the most popular peptides in anti-aging protocols because it directly addresses the age-related decline in growth hormone production. Benefits include improved skin quality, better sleep, enhanced recovery, increased lean mass, and reduced body fat, all markers associated with biological aging.
External resources
Sermorelin: A better approach to management of adult-onset growth hormone insufficiency (PMC)
PubMed: Sermorelin review for growth hormone deficiency treatment
In case I do not see you, good afternoon, good evening, and good night. May your hormones stay balanced, your protocols stay consistent, and your results stay worth the commitment.