Jan 18, 2026

After analyzing hundreds of testosterone optimization protocols, one pattern keeps emerging. The researchers who see the best results aren't just using testosterone replacement. They're using peptides strategically to support their body's natural hormone production.
The difference matters more than most realize. Direct testosterone replacement shuts down natural production entirely. Your body stops making its own.
Fertility tanks. Testicular atrophy becomes inevitable. But peptides work differently.
They signal your body to produce more testosterone on its own, keeping the entire hormonal system intact while elevating levels naturally.
This guide covers every peptide that influences testosterone, from direct stimulators that act on the hypothalamic-pituitary-gonadal axis to growth hormone secretagogues that boost testosterone indirectly through improved body composition and metabolic function. You'll learn exact dosing protocols, understand the mechanisms behind each compound, and discover how to choose the right approach for your specific goals.
SeekPeptides members have access to detailed protocol databases and community insights that go far beyond what any single guide can cover. But this article provides the foundation you need to understand how peptides affect testosterone and which ones deserve your attention.
How peptides affect testosterone production
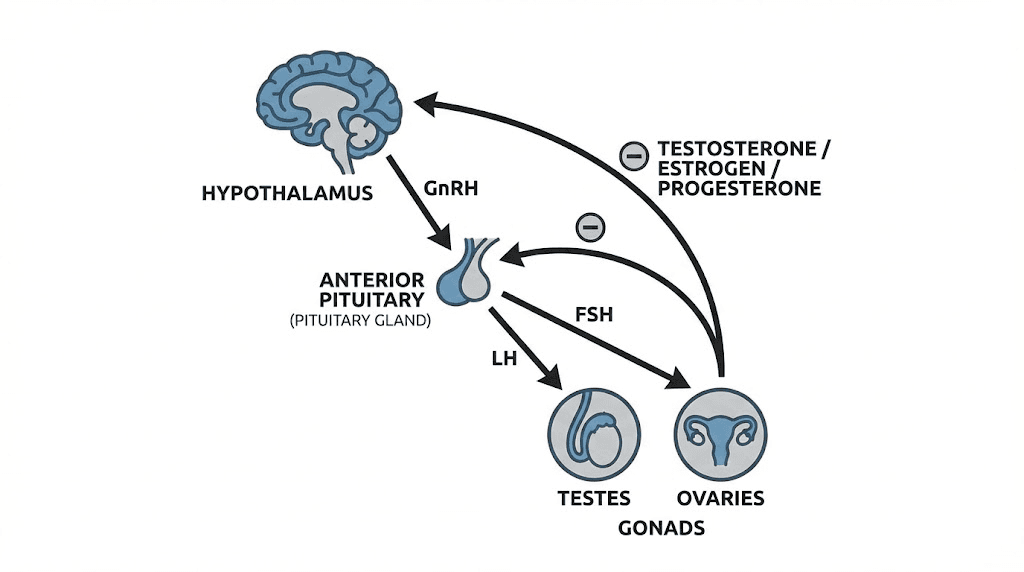
Understanding how peptides work requires grasping one fundamental concept: hormones operate through signaling cascades. Your brain releases signals that tell your pituitary gland what to do. Your pituitary then signals your testes (or ovaries) to produce sex hormones. Peptides can intervene at multiple points along this chain.
The hypothalamic-pituitary-gonadal axis controls testosterone production.
It starts in your hypothalamus, which releases gonadotropin-releasing hormone (GnRH).
This triggers your pituitary to release luteinizing hormone (LH) and follicle-stimulating hormone (FSH). LH then stimulates Leydig cells in the testes to produce testosterone.
Peptides that directly affect this axis can dramatically increase testosterone. Others work indirectly, improving factors like body composition, sleep quality, and metabolic health that influence hormone levels. Both approaches have their place in a comprehensive peptide protocol.
Direct HPG axis stimulation
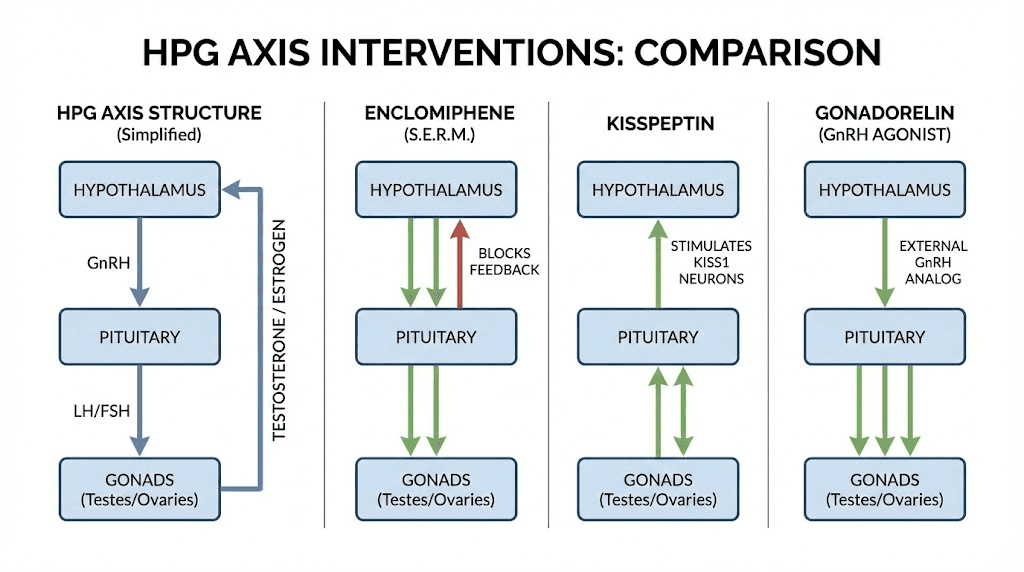
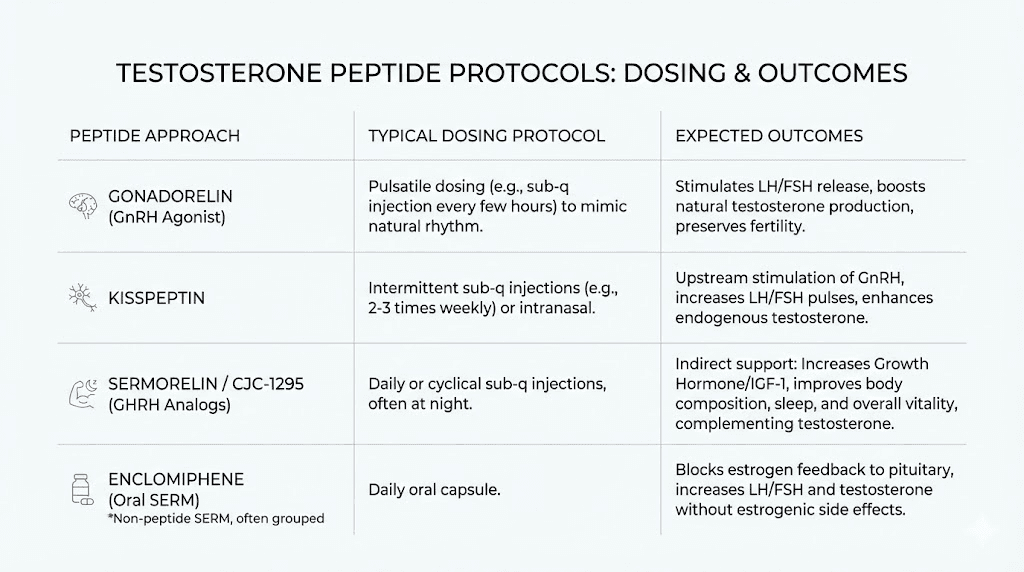
The most powerful testosterone-boosting peptides work directly on the HPG axis. Kisspeptin stimulates GnRH release from the hypothalamus. Gonadorelin mimics GnRH itself, directly triggering LH and FSH release. These peptides produce rapid, measurable increases in testosterone levels.
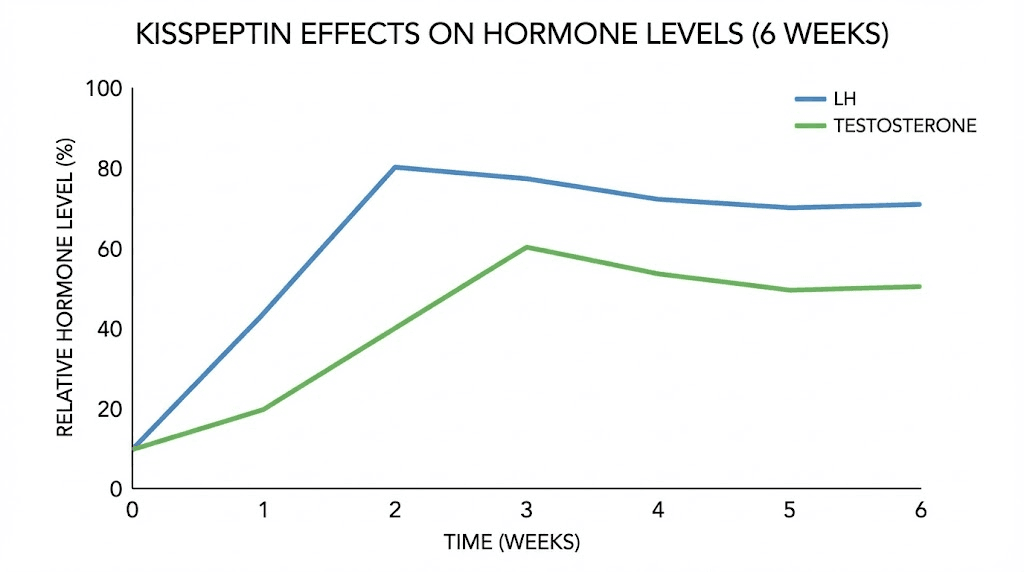
Clinical research demonstrates their potency. Kisspeptin-10 infusions increased LH from 5.4 to 20.8 IU/liter in healthy men, while testosterone rose from 16.6 to 24.0 nmol/liter. That's a 45% testosterone increase from a single compound acting on one pathway.
This direct approach preserves fertility, unlike exogenous testosterone. Your testes remain active, producing sperm alongside testosterone. For researchers concerned about reproductive function, direct HPG stimulation offers significant advantages.
Indirect testosterone support
Growth hormone secretagogues like CJC-1295, ipamorelin, and sermorelin don't directly stimulate testosterone production. They increase growth hormone, which creates downstream effects that support healthy testosterone levels.
The mechanism works through several pathways.
Growth hormone improves body composition, reducing visceral fat that converts testosterone to estrogen. Better sleep quality supports natural testosterone production cycles. Improved insulin sensitivity and metabolic function create an environment where testosterone thrives.
Researchers report 30-60% increases in testosterone levels within the first few months of growth hormone peptide therapy.
The effects take longer to manifest than direct stimulation, but they address root causes rather than just symptoms.
Combination approaches
Experienced researchers often combine direct and indirect approaches. A protocol might include kisspeptin for direct HPG stimulation alongside CJC-1295/ipamorelin for growth hormone benefits. This addresses testosterone from multiple angles while supporting overall hormonal health.
Understanding these mechanisms helps you choose the right peptides for your goals. Want rapid testosterone increases? Focus on direct HPG stimulators. Looking for sustainable, long-term optimization? Consider growth hormone secretagogues. Need both? A carefully designed stack can deliver.
Kisspeptin: the most potent natural testosterone stimulator
Kisspeptin represents the cutting edge of testosterone peptide research. This hypothalamic neuropeptide sits at the top of the reproductive hormone cascade, controlling the release of GnRH that ultimately drives testosterone production.
The research is compelling. Clinical studies show kisspeptin-10 boluses potently evoke LH secretion in men, while continuous infusion increases testosterone levels, LH pulse frequency, and pulse size. One study found infusion at 4 micrograms per kilogram per hour for 22.5 hours increased LH from 5.4 to 20.8 IU/liter and testosterone from 16.6 to 24.0 nmol/liter.
Think about what that means. A natural peptide, one your body already produces, can dramatically elevate testosterone without shutting down endogenous production. The implications for hormone optimization are significant.
How kisspeptin works
Kisspeptin binds to the KISS1R receptor in the hypothalamus. This binding directly stimulates GnRH release, which triggers the pituitary to release LH and FSH. Unlike synthetic GnRH analogs that can desensitize receptors with continuous use, kisspeptin works with your body's natural pulsatile hormone release pattern.
The peptide's role extends beyond just signaling. Research shows kisspeptin signaling is obligatory for normal pubertal maturation. Individuals with mutations in genes encoding kisspeptin or its receptor experience absent or disrupted pubertal development. This demonstrates how fundamental kisspeptin is to reproductive hormone function.
Some evidence suggests kisspeptin may also have direct effects on the testes. Studies found the Kiss1/Kiss1r system localized in testicular tissue, potentially contributing to local testosterone production.
However, other research questions whether these direct testicular effects are physiologically significant.
The primary mechanism remains central stimulation through the HPG axis.
Kisspeptin dosing protocols
Kisspeptin dosing varies based on administration method and research goals. The clinical studies used IV infusion, which isn't practical for most researchers. Subcutaneous administration requires different dosing considerations.
Typical research protocols range from 1-10 micrograms per kilogram of body weight. Lower doses produce subtle stimulation of the HPG axis. Higher doses create more dramatic LH and testosterone responses but may carry increased risk of receptor desensitization.
Most researchers start conservatively. A common approach uses 100-200 micrograms subcutaneously once or twice daily. Some protocols call for cycling, using kisspeptin for 4-6 weeks followed by a break. This prevents potential receptor downregulation while maintaining testosterone benefits.
The peptide dosage calculations matter here. Accurate reconstitution and measurement ensure consistent dosing. Use our peptide calculator to verify your math before administration.
What to expect from kisspeptin
Results from kisspeptin typically manifest within the first week of use. LH levels rise first, followed by testosterone increases over the subsequent days. Most researchers report noticeable effects on energy, libido, and mood within 2-3 weeks.
The timeline looks something like this. Days 1-3: minimal noticeable effects as LH begins rising. Days 4-7: initial testosterone increases become measurable. Weeks 2-4: subjective improvements in energy, motivation, and sexual function. Week 4 onward: sustained benefits with stable hormone levels.
Blood work confirms what researchers feel subjectively. LH increases of 50-300% are common. Testosterone typically rises 20-50% from baseline. These improvements maintain as long as administration continues, though the body may partially adapt over extended use.
Kisspeptin advantages and limitations
Kisspeptin offers several advantages over other testosterone-boosting approaches. It works with your body's natural hormone production rather than replacing it. Fertility remains intact because LH and FSH continue stimulating the testes normally. There's no testicular atrophy because the testes stay active.
The limitations exist too. Kisspeptin requires regular administration to maintain effects. It's less studied than some alternatives, with most research using IV rather than subcutaneous routes. And it won't help if the problem lies downstream of the hypothalamus, like primary hypogonadism where the testes themselves are dysfunctional.
For researchers with secondary hypogonadism or those wanting to enhance already-normal testosterone levels, kisspeptin represents one of the most promising options available. SeekPeptides members access detailed protocols and community experiences that help optimize kisspeptin use for individual goals.
Gonadorelin: synthetic GnRH for direct testosterone stimulation
Gonadorelin is a lab-made peptide with an identical structure to natural gonadotropin-releasing hormone. It acts directly on the pituitary gland, triggering the release of LH and FSH that stimulate testosterone production in the testes.
Unlike kisspeptin, which works one step higher in the cascade, gonadorelin skips the hypothalamus entirely. It directly tells the pituitary to release gonadotropins. This makes it useful for maintaining testicular function during testosterone replacement therapy, where the body's natural GnRH production becomes suppressed.
The peptide research community has extensively studied gonadorelin for both fertility preservation and testosterone support. The evidence supports its use in multiple contexts, though proper dosing and timing prove critical for success.
Gonadorelin mechanism of action
Gonadorelin binds to GnRH receptors on pituitary gonadotroph cells. This triggers the release of stored LH and FSH into the bloodstream. LH then travels to the testes, where it stimulates Leydig cells to produce testosterone.
The key to gonadorelin's effectiveness lies in pulsatile dosing. Natural GnRH releases in pulses, typically every 60-90 minutes. Continuous GnRH exposure actually suppresses LH and FSH release through receptor desensitization. This is how GnRH agonists used in prostate cancer treatment work, they flood the receptors constantly until they downregulate.
For testosterone support, gonadorelin must mimic natural pulsatile release. Brief periodic dosing preserves the signaling pattern.
Most protocols use injections 2-3 times weekly, spacing them to allow receptor recovery between doses.
This maintains the natural feedback loop while boosting overall gonadotropin output.
Gonadorelin dosing for testosterone
Typical gonadorelin doses range from 50-250 micrograms per injection, administered 2-3 times weekly. The response varies significantly between individuals. Some men experience robust LH and testosterone increases at lower doses. Others need higher amounts for meaningful effects.
A common starting protocol uses 100 micrograms subcutaneously three times weekly. After 4-6 weeks, blood work guides adjustments. If LH and testosterone haven't risen significantly, increasing to 150-200 micrograms may help. Doses above 200 micrograms per injection rarely provide additional benefit and may increase side effect risk.
Reconstitution typically uses bacteriostatic water to create a 1 mg/mL solution. At this concentration, a 100 microgram dose equals 0.1 mL, or 10 units on a standard insulin syringe. Proper storage after reconstitution maintains stability for 4-6 weeks refrigerated.
Timing matters for optimal results. Some researchers dose in the morning to support natural testosterone rhythms. Others prefer evening administration. The peptide injection guide provides detailed information on administration techniques and timing considerations.
Gonadorelin with TRT
Gonadorelin sees frequent use alongside testosterone replacement therapy. Exogenous testosterone suppresses natural production through negative feedback. LH and FSH plummet. The testes shrink from disuse. Sperm production crashes.
Adding gonadorelin during TRT maintains gonadotropin stimulation to the testes. This reduces or slows testicular atrophy, preserves some fertility potential, and may support intratesticular testosterone needed for optimal sperm production.
The protocol typically involves continued TRT dosing plus gonadorelin 100-150 micrograms 2-3 times weekly. Results vary. Some men maintain near-normal testicular size and sperm parameters. Others see minimal benefit even with optimal dosing. Individual response depends on factors like pre-TRT testicular function and duration of testosterone use.
Gonadorelin works less reliably than HCG for testicular maintenance during TRT. HCG directly mimics LH, binding to the same receptors and directly stimulating testosterone and sperm production in the testes. Gonadorelin works one step upstream, and the signal can get diluted by the time it reaches testicular tissue. Many TRT protocols now use gonadorelin since HCG became less accessible, but expectations should be tempered.
Gonadorelin standalone use
For researchers not on TRT, gonadorelin can boost testosterone as a standalone compound. It's particularly useful for men with secondary hypogonadism, where the problem lies in insufficient hypothalamic or pituitary signaling rather than testicular dysfunction.
Standalone protocols typically run 4-8 weeks, followed by reassessment. During this time, researchers monitor for testosterone increases and symptom improvement. Successful protocols may continue with periodic breaks to prevent receptor adaptation.
The advantages of standalone gonadorelin include preserved fertility and natural hormone production. Unlike TRT, stopping gonadorelin doesn't leave you worse off than before. Your body's natural production wasn't suppressed, so there's no recovery period needed.
The disadvantages include less predictable results compared to direct testosterone administration. Some men respond excellently. Others experience minimal testosterone increases despite appropriate dosing. Blood work before and during treatment helps identify responders early.
Enclomiphene: the SERM for testosterone and fertility
Enclomiphene citrate isn't technically a peptide, but it deserves discussion in any comprehensive testosterone optimization guide. This selective estrogen receptor modulator (SERM) works by blocking estrogen feedback to the hypothalamus and pituitary, triggering increased LH and FSH release.
The mechanism differs from peptides but achieves similar goals. By blocking estrogen receptors in the brain, enclomiphene tricks the body into thinking estrogen levels are low. The response? Increased gonadotropin release and elevated testosterone production.
Clinical trials demonstrate impressive results. After 6 weeks at 25 mg daily, men achieved mean testosterone levels of 604 ng/dL. More importantly, sperm counts remained above 75 million/mL in all participants, compared to severe oligospermia in men using testosterone therapy. This preservation of fertility makes enclomiphene particularly valuable.
How enclomiphene differs from clomiphene
Clomiphene citrate has been used for decades to boost testosterone and treat male infertility. But it's a mixture of two isomers: enclomiphene and zuclomiphene. The zuclomiphene component has estrogenic effects that can cause side effects and partially negate the testosterone-boosting benefits.
Enclomiphene is the purified, active isomer. It provides the anti-estrogenic effects that boost testosterone without the estrogenic activity of zuclomiphene. Users typically report fewer side effects, particularly the visual disturbances and emotional changes sometimes associated with clomiphene.
The distinction matters for practical use. Clomiphene works, but the side effect profile limits its appeal for long-term testosterone optimization. Enclomiphene offers a cleaner experience with potentially better results.
Enclomiphene dosing protocols
Standard enclomiphene dosing ranges from 12.5-50 mg daily. Most protocols start at 25 mg, adjusting based on response. Clinical trials used 25 mg with excellent results, making this a reasonable starting point.
Lower doses like 12.5 mg work well for maintenance or for men who respond strongly. Higher doses up to 50 mg may benefit those with stubborn hypogonadism or poor initial response. Blood work at 4-6 weeks guides dose optimization.
Enclomiphene can be taken daily long-term or used cyclically. Some researchers prefer 5 days on, 2 days off to allow for receptor sensitivity maintenance. Others use continuous dosing without apparent issues. The optimal approach varies by individual.
Enclomiphene for testosterone versus TRT
The choice between enclomiphene and TRT depends on your priorities. TRT produces more reliable, predictable testosterone increases. Inject testosterone, testosterone levels rise. Simple. But you sacrifice natural production and fertility, potentially permanently.
Enclomiphene preserves everything. Natural production continues. Testicular function persists. Fertility remains viable. For young men concerned about future family planning, this matters enormously.
The testosterone boosters versus peptides comparison explores these tradeoffs in detail. The short version: if maximum testosterone is the only goal and fertility doesn't matter, TRT is more effective. If you want testosterone optimization while maintaining natural function, enclomiphene (or peptides like kisspeptin and gonadorelin) makes more sense.
Combining enclomiphene with peptides
Some protocols combine enclomiphene with peptides for synergistic effects. Enclomiphene blocks estrogen feedback while kisspeptin or gonadorelin directly stimulates the axis. The combination can produce greater testosterone increases than either compound alone.
A typical combination protocol might use enclomiphene 25 mg daily plus gonadorelin 100 mcg three times weekly. The enclomiphene removes estrogen-mediated suppression while the gonadorelin provides direct stimulation. Blood work guides adjustments and monitors for excessive elevation.
These combinations require more careful monitoring. More compounds mean more variables and more potential for issues. SeekPeptides provides protocols and community support for researchers exploring these advanced approaches.
Growth hormone peptides and testosterone
Growth hormone secretagogues represent a different approach to testosterone optimization. CJC-1295, ipamorelin, sermorelin, and tesamorelin don't directly stimulate testosterone production. They increase growth hormone, creating downstream effects that support healthy testosterone levels.
The connection between growth hormone and testosterone is well established. Men with growth hormone deficiency often have low testosterone. Growth hormone therapy frequently improves testosterone levels as a secondary benefit. The mechanisms involve improved body composition, better sleep, enhanced metabolic function, and direct effects on gonadotropin secretion.
For researchers seeking comprehensive hormone optimization rather than just testosterone, growth hormone peptides offer significant value.
They address multiple aspects of health and performance while supporting testosterone production indirectly.
CJC-1295 and ipamorelin
This combination represents the most popular growth hormone peptide stack. CJC-1295 is a growth hormone releasing hormone (GHRH) analog that extends the hormone's half-life. Ipamorelin mimics ghrelin to stimulate additional growth hormone release. Together, they produce sustained elevations in growth hormone and IGF-1.
The testosterone effects are indirect but meaningful. Research shows that improved GH and IGF-1 levels may modulate gonadotropins, potentially supporting testosterone production. More significantly, the body composition improvements from GH peptides reduce visceral fat, which is a major converter of testosterone to estrogen through aromatase activity.
Typical protocols use CJC-1295 100-300 mcg combined with ipamorelin 100-300 mcg, administered subcutaneously once or twice daily. Many researchers prefer nighttime dosing to amplify the natural GH surge during sleep. The peptide stacking guide covers optimal combination strategies.
Results take longer to manifest than with direct HPG stimulators. Most researchers notice body composition changes within 4-8 weeks. Sleep quality often improves within the first week. Testosterone benefits typically become apparent after 2-3 months of consistent use as body fat decreases and metabolic health improves.
Sermorelin for testosterone support
Sermorelin is a synthetic version of naturally occurring GHRH. It stimulates your pituitary to produce more growth hormone, which then affects testosterone through several pathways.
The research suggests sermorelin produces small acute rises in FSH and LH alongside its GH effects. This finding implies potential for direct HPG axis stimulation, not just the indirect benefits from improved body composition. The mechanisms need more study, but the clinical observations are intriguing.
Practically, sermorelin users report benefits that overlap with testosterone improvement: better energy, improved mood, stronger workouts, enhanced libido. These effects likely result from both the GH benefits and any direct hormonal effects on testosterone production.
Standard sermorelin dosing uses 200-500 mcg subcutaneously once daily, usually before bed. Some protocols use twice-daily dosing. Results build gradually over weeks to months. Patience is required, but the comprehensive benefits justify the timeline for many researchers.
Tesamorelin: FDA-approved GH peptide
Tesamorelin stands apart as an FDA-approved GHRH analog. Originally developed for HIV-associated lipodystrophy, it's gained attention for its potent effects on visceral fat and body composition.
The testosterone connection with tesamorelin works primarily through fat reduction. Visceral fat contains high concentrations of aromatase, the enzyme that converts testosterone to estrogen. Reducing visceral fat means less testosterone conversion, resulting in higher circulating testosterone levels.
Studies show tesamorelin decreases visceral adipose tissue by approximately 15% compared to placebo. Some research found relative hepatic fat reductions of 40%. These changes create a hormonal environment more favorable for testosterone production and utilization.
Standard dosing is 2 mg subcutaneously daily.
The newer Egrifta WR formulation delivers 1.28 mg daily with equivalent efficacy. Results appear within 4-6 weeks for fat reduction, with significant body composition changes over 3-6 months. Testosterone benefits parallel these body composition improvements.
GH peptides versus direct testosterone stimulation
The choice between growth hormone peptides and direct testosterone stimulators depends on your goals and timeframe. Direct stimulators like kisspeptin and gonadorelin produce faster testosterone increases. GH peptides take longer but address broader aspects of hormonal and metabolic health.
Many researchers use both. A comprehensive protocol might include gonadorelin for direct testosterone stimulation plus CJC-1295/ipamorelin for growth hormone benefits. This approach optimizes multiple hormone axes simultaneously, creating synergistic improvements in body composition, energy, recovery, and sexual function.
The best peptide for your situation depends on specific deficiencies and goals. Blood work identifying which hormones are suboptimal helps guide protocol design. SeekPeptides members get access to detailed assessment frameworks and personalized protocol recommendations.
Supporting peptides that indirectly affect testosterone
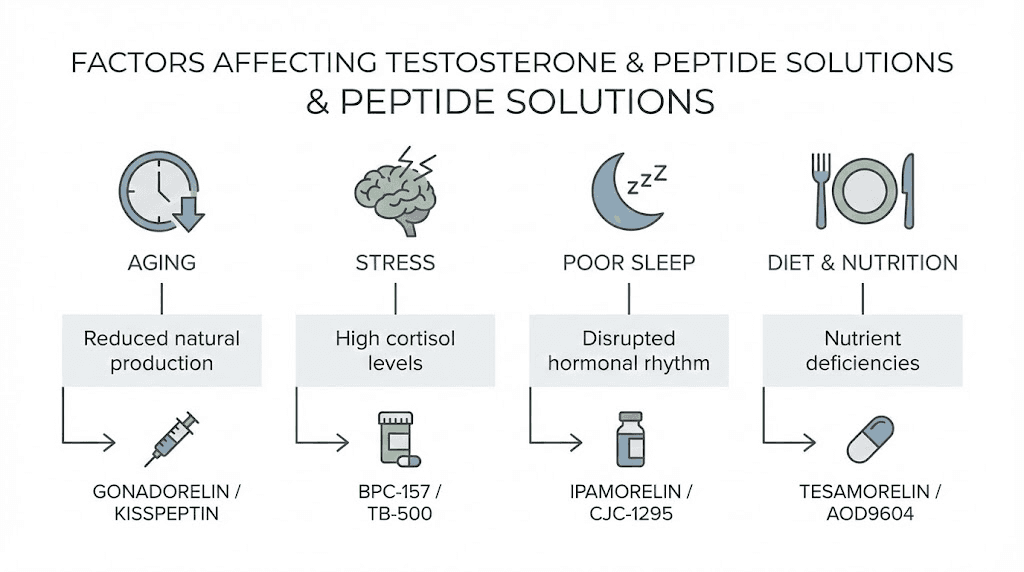
Several peptides don't directly influence testosterone but create conditions that support healthy hormone levels. These compounds address recovery, inflammation, gut health, and cellular function in ways that contribute to optimal testosterone production.
Understanding these indirect effects helps build comprehensive protocols. Testosterone doesn't exist in isolation. Inflammation suppresses it.
Poor sleep reduces it. Chronic stress tanks it. Peptides that address these factors create an environment where testosterone thrives.
BPC-157 and testosterone
BPC-157 is primarily known for its healing properties, but its influence extends to hormonal health. While BPC-157 doesn't directly increase testosterone, its effects on recovery, inflammation, and gut health create conditions that support hormone production.
Chronic inflammation suppresses testosterone. The body prioritizes dealing with inflammation over reproductive function. By reducing systemic inflammation, BPC-157 removes one barrier to optimal testosterone levels. Researchers recovering from injuries often notice their testosterone symptoms improve alongside healing.
Gut health also influences hormones. The gut produces and regulates numerous compounds that affect the HPG axis. BPC-157's protective effects on the gastrointestinal lining may improve nutrient absorption and gut-brain signaling in ways that benefit testosterone production.
Some theories suggest BPC-157 may upregulate neurotransmitters correlated with testosterone, specifically dopamine. The evidence for this specific mechanism remains limited, but the general relationship between dopaminergic function and testosterone is well established.
Standard BPC-157 protocols use 200-300 mcg twice daily. Most researchers incorporate it as part of broader stacks rather than using it specifically for testosterone. Its healing benefits provide value regardless of any hormonal effects.
TB-500 for recovery and testosterone support
TB-500 shares similarities with BPC-157 in promoting recovery and reducing inflammation. Its benefits for tissue healing create conditions favorable for testosterone production through similar mechanisms.
The connection works through stress reduction. Physical stress from injuries, chronic inflammation, or overtraining suppresses the HPG axis. Cortisol, the primary stress hormone, directly inhibits testosterone production. By accelerating recovery and reducing physical stressors, TB-500 removes barriers to healthy testosterone levels.
Many researchers combine BPC-157 and TB-500 in their protocols. The combination addresses recovery comprehensively while creating a hormonal environment more supportive of testosterone production. The comparison between these peptides helps identify which might be more appropriate for specific situations.
MOTS-c and metabolic testosterone support
MOTS-c is a mitochondrial-derived peptide that affects metabolic function. It improves insulin sensitivity, promotes fat oxidation, and enhances cellular energy production. These metabolic improvements create conditions favorable for testosterone production.
Poor metabolic health, particularly insulin resistance and obesity, significantly impairs testosterone. Visceral fat converts testosterone to estrogen. Insulin resistance disrupts hormonal signaling. By improving metabolic function, MOTS-c addresses root causes of suboptimal testosterone rather than just treating symptoms.
Research on MOTS-c and testosterone specifically is limited. The theoretical basis for benefits is strong, but direct clinical evidence for testosterone increases from MOTS-c use remains sparse. Researchers typically use MOTS-c for its metabolic and anti-aging benefits, with any testosterone effects being secondary.
Peptides versus testosterone replacement therapy
The fundamental question many researchers face: should you use peptides to support natural testosterone or go straight to TRT? Both approaches have merits. Neither is universally superior. Understanding the tradeoffs helps make informed decisions.
TRT works. There's no question about that. Inject exogenous testosterone, and your levels rise predictably. The comparison between peptides and steroids highlights this reliability as TRT's main advantage.
But that reliability comes with significant costs.
The TRT tradeoffs
Exogenous testosterone suppresses natural production through negative feedback. Your hypothalamus sees high testosterone and reduces GnRH release. Your pituitary reduces LH and FSH. Your testes, no longer receiving stimulation, atrophy and stop producing testosterone and sperm.
This suppression is often permanent or semi-permanent. Men who use TRT for extended periods may never fully recover natural production after stopping. Some require lifelong TRT because their natural system no longer functions adequately.
Fertility becomes severely compromised during TRT. Sperm production requires intratesticular testosterone at concentrations 50-100 times higher than blood levels. Only local production in the testes achieves this. Exogenous testosterone can't reach these concentrations intratestically, so sperm production crashes.
Additional TRT considerations include cardiovascular effects, estrogen conversion requiring management with aromatase inhibitors, and the psychological aspects of lifelong hormone dependence. None of these are necessarily dealbreakers, but they deserve consideration.
Peptide advantages
Peptides that stimulate natural testosterone production avoid most of TRT's downsides. Your body continues making its own testosterone. The HPG axis stays active. Fertility remains intact. Testicular atrophy doesn't occur.
Stopping peptides doesn't leave you worse off than before. Since your natural production was never suppressed, there's no recovery period.
Your baseline testosterone returns to where it started, not to suppressed levels below your starting point.
Peptides also address testosterone as part of broader hormonal health. Growth hormone secretagogues improve GH alongside supporting testosterone. The comprehensive benefits exceed what testosterone alone provides.
The comparison between HGH alternatives illustrates how peptides can replace or complement traditional hormone therapy while maintaining natural function. The approach requires more patience but preserves long-term options.
When peptides might not be enough
Peptides work best for secondary hypogonadism, where the problem lies in insufficient signaling rather than testicular dysfunction. If your testes can produce testosterone when properly stimulated, peptides can provide that stimulation.
Primary hypogonadism, where the testes themselves are damaged or dysfunctional, responds poorly to peptides. You can send all the LH you want, but if the testes can't respond, testosterone won't increase. These cases require TRT.
Severely low testosterone might also warrant TRT initially. If levels are in the truly hypogonadal range with significant symptoms, getting them up quickly with TRT while simultaneously addressing underlying causes might make sense.
Some researchers then transition from TRT to peptide-based protocols once they've stabilized.
Blood work helps identify which category applies. LH levels distinguish primary from secondary hypogonadism. If LH is high but testosterone is low, the problem is testicular. Peptides won't help much. If LH is low or normal with low testosterone, the problem is signaling. Peptides can address that.
Complete testosterone peptide protocols
Putting together effective protocols requires understanding how different compounds interact and matching them to specific goals. The following protocols represent common approaches used by researchers at various stages of testosterone optimization.
Remember that individual response varies significantly. What works excellently for one person may provide minimal benefit for another.
Blood work before, during, and after protocols helps identify what's working and guides adjustments. SeekPeptides members access community experiences and expert guidance that help optimize protocols for individual situations.
Protocol 1: Direct HPG stimulation (moderate approach)
Goal: Boost testosterone through natural pathway stimulation while preserving fertility
Components:
Gonadorelin: 100 mcg subcutaneously three times weekly (Monday, Wednesday, Friday)
Implementation:
Morning administration to support natural testosterone rhythm
Reconstitute with bacteriostatic water to 1 mg/mL concentration
Store reconstituted solution refrigerated
Use insulin syringes for accurate dosing
Duration: 8-12 weeks initial protocol
Expected results:
LH increase: 30-80% above baseline
Testosterone increase: 20-40% above baseline
Maintained or improved sperm parameters
Timeline:
Week 1-2: Minimal noticeable effects, LH beginning to rise
Week 3-4: Testosterone increases become measurable
Week 4-8: Subjective improvements in energy and libido
Week 8-12: Stable improvements, assess for continuation
Protocol 2: Comprehensive HPG and GH support (aggressive approach)
Goal: Maximize testosterone while also boosting growth hormone for body composition and recovery
Components:
Kisspeptin-10: 200 mcg subcutaneously once daily (morning)
CJC-1295 no DAC: 100 mcg subcutaneously once daily (evening)
Ipamorelin: 200 mcg subcutaneously once daily (evening)
Implementation:
Kisspeptin in morning for HPG axis stimulation throughout day
CJC-1295/Ipamorelin before bed to amplify natural GH pulse during sleep
Can combine CJC and ipamorelin in same syringe if both reconstituted with bacteriostatic water
Maintain consistent timing daily
Duration: 12-16 weeks
Expected results:
Testosterone increase: 30-50% above baseline
GH/IGF-1 increases: 50-100% above baseline
Body composition improvements: fat loss, muscle gain
Enhanced recovery and sleep quality
Timeline:
Week 1: Improved sleep from GH peptides
Week 2-4: Energy and recovery improvements
Week 4-8: Measurable testosterone and body composition changes
Week 8-16: Continued optimization and stabilization
Protocol 3: Testosterone support with fertility preservation
Goal: Optimize testosterone specifically while maintaining or enhancing fertility
Components:
Enclomiphene: 25 mg orally once daily
Gonadorelin: 100 mcg subcutaneously twice weekly
Implementation:
Enclomiphene taken with morning meal for consistent absorption
Gonadorelin on non-consecutive days (Tuesday, Saturday)
Monitor for visual disturbances, a rare side effect of SERMs
Regular sperm analysis if fertility is a primary concern
Duration: Ongoing or cycled (8 weeks on, 4 weeks off)
Expected results:
Testosterone increase: 40-70% above baseline
LH and FSH increases: 50-150% above baseline
Maintained or improved sperm parameters
Preserved testicular size and function
Timeline:
Week 2: LH/FSH increases begin
Week 4-6: Testosterone increases measurable on blood work
Week 6-12: Subjective symptom improvement stabilizes
Protocol 4: Recovery-focused with testosterone support
Goal: Address healing and recovery while creating conditions favorable for testosterone
Components:
BPC-157: 250 mcg subcutaneously twice daily
TB-500: 2.5 mg subcutaneously twice weekly
Sermorelin: 300 mcg subcutaneously before bed
Implementation:
BPC-157 morning and evening for consistent anti-inflammatory effects
TB-500 on set days (Monday and Thursday) for tissue repair
Sermorelin before bed to support GH and recovery during sleep
Can combine BPC-157 and sermorelin in evening dose if convenient
Duration: 6-8 weeks for acute recovery, ongoing at maintenance doses for chronic support
Expected results:
Accelerated healing from injury or overtraining
Reduced inflammation and associated testosterone suppression
Improved sleep and recovery
Indirect testosterone support through stress reduction
Timeline:
Week 1: Improved sleep, reduced inflammation
Week 2-4: Accelerated healing of damaged tissues
Week 4-8: Systemic inflammation reduction, improved hormonal environment
Dosing calculations and reconstitution
Accurate dosing makes the difference between effective and ineffective protocols. Most peptides come as lyophilized (freeze-dried) powder requiring reconstitution before use. Getting this right ensures consistent results.
Standard reconstitution process
The general process applies to most testosterone-related peptides:
Allow the peptide vial to reach room temperature
Wipe the vial stopper with an alcohol swab
Draw the desired amount of bacteriostatic water into a syringe
Insert needle through stopper at an angle
Slowly release water against the vial wall, not directly on the powder
Allow the peptide to dissolve naturally, don't shake
Once dissolved, store refrigerated
The amount of water determines concentration. More water means a more dilute solution, requiring larger injection volumes for the same dose. Less water creates a concentrated solution, allowing smaller injection volumes.
Common reconstitution calculations
For a 2 mg gonadorelin vial:
Add 2 mL bacteriostatic water = 1 mg/mL = 1000 mcg/mL
Each 0.1 mL (10 units on insulin syringe) = 100 mcg
For a 5 mg BPC-157 vial:
Add 2.5 mL bacteriostatic water = 2 mg/mL = 2000 mcg/mL
Each 0.1 mL (10 units) = 200 mcg
Each 0.125 mL (12.5 units) = 250 mcg
For a 10 mg kisspeptin vial:
Add 2 mL bacteriostatic water = 5 mg/mL = 5000 mcg/mL
Each 0.04 mL (4 units) = 200 mcg
The peptide calculator handles these calculations automatically. Input your vial size, reconstitution volume, and desired dose to get exact syringe units.
Storage after reconstitution
Reconstituted peptides are less stable than lyophilized powder. Proper storage maintains potency:
Always refrigerate at 2-8°C (35-46°F)
Avoid freezing reconstituted solutions
Keep away from light
Use within 4-6 weeks for most peptides
Don't repeatedly warm and cool the solution
How long peptides last depends on the specific compound, reconstitution solution, and storage conditions. Bacteriostatic water provides longer stability than sterile water due to the preservative benzyl alcohol.
Side effects and safety considerations
Peptides affecting testosterone carry potential side effects that warrant understanding before use. While generally well-tolerated compared to exogenous testosterone, these compounds aren't without risks.
Peptide safety requires attention to both compound-specific effects and general injection-related concerns. The following covers what researchers commonly experience and how to manage issues.
Kisspeptin side effects
Kisspeptin is generally well-tolerated. Reported side effects include:
Facial flushing, particularly with higher doses
Headache, usually mild and transient
Injection site reactions, minor and temporary
Potential for receptor desensitization with continuous use
Most side effects resolve quickly and don't require stopping the protocol. Flushing typically decreases as the body adjusts over the first few days. Headaches respond to standard over-the-counter analgesics.
The main concern with kisspeptin is the limited long-term safety data. Most studies used short-term administration. The effects of extended use remain less well characterized. Cycling protocols with periodic breaks may reduce any theoretical long-term risks.
Gonadorelin side effects
Gonadorelin carries similar side effect risks:
Headache, the most commonly reported effect
Nausea, usually mild
Abdominal discomfort
Injection site reactions
Potential for HPG axis suppression with excessive or continuous dosing
The critical safety consideration with gonadorelin is dosing pattern. Continuous or excessive GnRH agonist exposure suppresses rather than stimulates the HPG axis. This paradoxical effect requires maintaining pulsatile dosing patterns.
Never exceed recommended doses or injection frequency with gonadorelin. More is not better and can actually worsen testosterone levels through receptor desensitization.
Growth hormone peptide side effects
CJC-1295, ipamorelin, sermorelin, and similar compounds share common side effects:
Water retention, typically mild and transient
Joint pain or stiffness from fluid shifts
Numbness or tingling in extremities (carpal tunnel-like symptoms)
Increased hunger (particularly with ghrelin-mimetics like ipamorelin)
Fatigue or lethargy in some users
Headache
These effects generally indicate the peptides are working, as they're associated with GH elevation. Reducing dose often resolves excessive symptoms while maintaining benefits.
Long-term GH elevation raises theoretical concerns about insulin resistance, cardiovascular effects, and potential cancer risk. The evidence for these concerns with peptide-level GH elevation (as opposed to supraphysiological HGH doses) is limited but warrants awareness.
General injection safety
All injectable peptides carry injection-related risks:
Infection at injection sites (prevented by sterile technique)
Bruising or bleeding (minor, self-limiting)
Nerve irritation if injection technique is poor
Allergic reactions to the peptide or diluent (rare)
Sterile technique prevents most injection complications. Clean the injection site with alcohol. Use a fresh needle for each injection. Never share needles or peptide supplies.
Rotating injection sites prevents localized tissue irritation. Subcutaneous injections can be administered in the abdomen, thigh, or upper arm. Moving between sites each day or week allows tissue recovery.
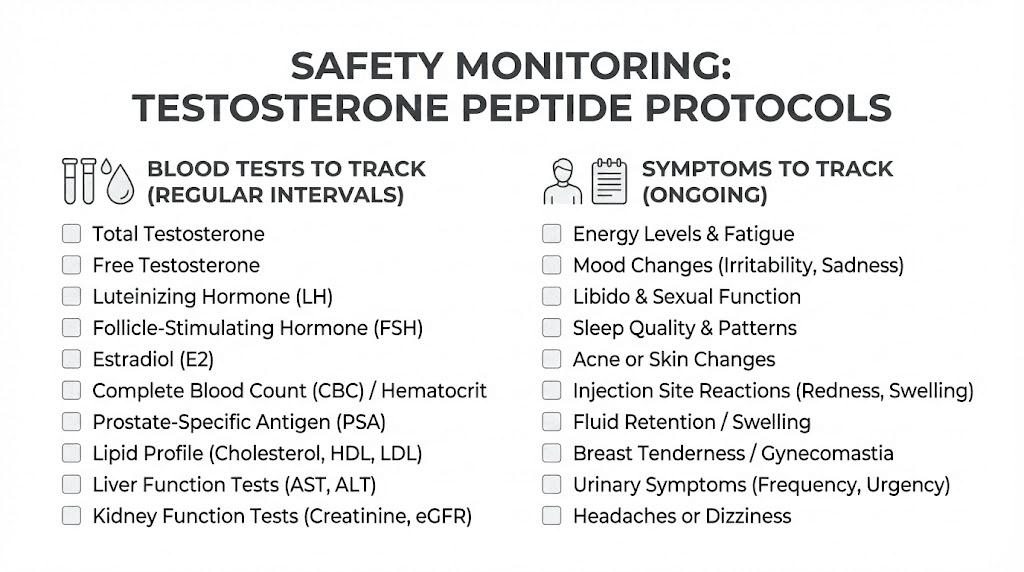
Monitoring recommendations
Blood work before and during peptide protocols helps identify issues early:
Baseline testosterone, LH, FSH before starting
Repeat testing at 4-6 weeks to assess response
Monitor estrogen, as increased testosterone can increase estrogen
Check IGF-1 if using growth hormone peptides
Consider fasting glucose and insulin if using GH peptides long-term
Symptom tracking complements blood work. Note energy levels, libido, mood, sleep quality, and any side effects. Subjective improvements often precede blood work changes and help confirm the protocol is working.
Legal and regulatory considerations
The legal status of peptides varies by jurisdiction and intended use. Understanding the regulatory landscape helps researchers make informed decisions about their protocols.
Research chemical status
Most testosterone-related peptides are sold as research chemicals, not for human consumption. This designation means:
They're legal to purchase for research purposes in most jurisdictions
Quality varies significantly between vendors
No regulatory oversight ensures purity or potency
Use on humans technically falls outside approved purposes
This gray area creates both opportunities and risks. Researchers can access peptides that would otherwise require prescriptions. But they also bear responsibility for verifying quality and accepting risks of unregulated compounds.
Peptide regulation news keeps evolving. Recent changes have affected availability of some compounds. Staying informed about regulatory developments helps researchers adapt their approaches.
Finding quality peptides
Without regulatory oversight, peptide vendors vary dramatically in quality. Third-party testing, COAs (certificates of analysis), and reputation become critical for identifying reliable sources.
Look for vendors that:
Provide current COAs with each batch
Use third-party testing laboratories
Have established reputations in research communities
Respond appropriately to quality concerns
Display transparent business practices
Price alone doesn't indicate quality. Some cheap peptides are fine. Some expensive ones are underdosed or impure. Testing and reputation matter more than price point.
Sports and competition considerations
Many testosterone-affecting peptides are prohibited by WADA and other sports organizations. Tesamorelin, for example, is specifically banned. GH secretagogues fall under prohibited substance categories.
Athletes subject to drug testing should assume all testosterone and GH-related peptides are prohibited unless specifically cleared by their governing body. The consequences of positive tests can be career-ending.
Even researchers not subject to testing should understand these classifications. They indicate how seriously regulatory bodies view these compounds' performance-enhancing potential.
Frequently asked questions
Do peptides directly increase testosterone?
Some peptides directly stimulate testosterone production. Kisspeptin triggers the HPG axis cascade that leads to testosterone release. Gonadorelin mimics GnRH to directly stimulate LH and FSH. Others like CJC-1295 and ipamorelin work indirectly through growth hormone pathways that support testosterone production.
How long do testosterone peptides take to work?
Direct HPG stimulators like kisspeptin and gonadorelin produce measurable testosterone increases within 1-2 weeks. Growth hormone peptides take longer, typically 2-3 months for noticeable testosterone benefits as body composition improves. Subjective improvements in energy and libido often precede blood work changes.
Can I use testosterone peptides with TRT?
Yes, compounds like gonadorelin are specifically used alongside TRT to maintain testicular function. Adding peptides to TRT can preserve fertility potential and reduce testicular atrophy. However, the combination requires careful management and monitoring.
Are testosterone peptides safer than TRT?
Peptides that stimulate natural testosterone production maintain the HPG axis and preserve fertility, avoiding the shutdown associated with TRT. This makes them "safer" in terms of maintaining natural function. However, peptides have less long-term safety data than testosterone, which has been used for decades. Both approaches carry risks and benefits that require individual assessment.
Which testosterone peptide is most effective?
Kisspeptin produces the most dramatic acute testosterone increases in research settings.
For practical use, the combination of enclomiphene plus gonadorelin often produces the best sustained results. CJC-1295/ipamorelin provides broader benefits beyond just testosterone.
The "best" choice depends on specific goals and circumstances.
Do I need a prescription for testosterone peptides?
In most jurisdictions, testosterone-affecting peptides are available as research chemicals without prescription. Some, like enclomiphene, are available through compounding pharmacies with a prescription. Regulations vary by location and change over time, so verify current rules in your jurisdiction.
Can women use testosterone peptides?
Women can use certain testosterone-affecting peptides, though the goals and dosing differ from men. Peptides for women often focus on optimizing hormones for energy, libido, and body composition rather than maximizing testosterone. Growth hormone peptides benefit both sexes similarly. Direct testosterone stimulators require more careful consideration in women.
How do I know if testosterone peptides are working?
Blood work provides objective confirmation. Before and after testing shows LH, FSH, and testosterone changes. Subjective markers include improved energy, enhanced libido, better mood, increased strength, and improved body composition. Most researchers notice subjective changes before blood work confirms the mechanism.
External resources
For researchers serious about optimizing testosterone through peptides, SeekPeptides provides the most comprehensive resource available. Members access detailed protocols, community experiences from thousands of researchers, expert guidance, and tools that take the guesswork out of peptide optimization. Whether you're exploring kisspeptin, building a GH peptide stack, or designing a comprehensive hormone optimization protocol, the platform delivers evidence-based guidance that goes far beyond what any single article can offer.