Mar 10, 2026

Tired of conflicting information about why your GLP-1 medication stopped working? You are not alone. Thousands of researchers hit that wall. The scale freezes. The appetite suppression fades. The progress that felt inevitable three months ago now feels like a distant memory. And every forum post, every article, every well-meaning friend has a different theory about what went wrong.
Here is the truth. A GLP-1 reset is not some mythical protocol that magically restores everything overnight. It is a real, science-backed process that involves understanding how GLP-1 receptor agonists interact with your body at the cellular level, recognizing the difference between metabolic adaptation and genuine receptor desensitization, and then choosing the right strategy from a toolkit that includes everything from structured medication breaks to switching between medications to lifestyle interventions that actually move the needle. This guide covers every angle. The receptor biology. The practical protocols. The specific timelines. The strategies that experienced researchers use when they feel their GLP-1 response weakening. Whether you are on semaglutide, tirzepatide, or exploring retatrutide, SeekPeptides built this resource so you would never have to guess what comes next.
What a GLP-1 reset actually means
The term GLP-1 reset gets thrown around loosely in online communities. Some people use it to describe taking a break from medication. Others mean switching from one GLP-1 agonist to another. A few use it to describe any strategy that restarts stalled weight loss. These are all partially correct, but none capture the full picture.
A true GLP-1 reset is any deliberate intervention designed to restore or improve your body response to GLP-1 receptor agonist therapy. That might mean allowing downregulated receptors to recover their sensitivity. It might mean changing the agonist profile to engage slightly different receptor pathways. Or it might mean addressing the metabolic adaptations that make continued weight loss physiologically harder regardless of medication efficacy.
The confusion happens because people conflate three distinct phenomena.
First, there is receptor desensitization. This is the actual biological process where continuous stimulation of the GLP-1 receptor causes it to become less responsive. The receptor gets phosphorylated, internalized, and temporarily removed from the cell surface. This happens on a timescale of minutes to hours at the cellular level.
Second, there is metabolic adaptation. As you lose weight, your body requires fewer calories. Your metabolic rate adjusts. Hormones shift. The caloric deficit that produced steady weight loss at 250 pounds produces nothing at 210 pounds. The medication is still working. Your body simply adapted to the new energy balance.
Third, there is tachyphylaxis. This is progressive loss of medication effectiveness despite maintained dosing. True tachyphylaxis with GLP-1 receptor agonists remains controversial in the clinical literature. A 2020 study in the European Journal of Pharmacology found that tolerance does develop toward GLP-1 receptor agonist glucose-lowering effects in mice. But a study published in the Journal of Clinical Endocrinology and Metabolism by Buse and colleagues found no evidence that tolerance develops toward liraglutide glucose-lowering effects in humans. The distinction matters enormously because each phenomenon requires a different reset strategy.
Understanding which of these three issues you face is the first and most important step. Get it wrong, and you waste weeks on the wrong approach. Get it right, and the path forward becomes clear.
The science behind GLP-1 receptor desensitization
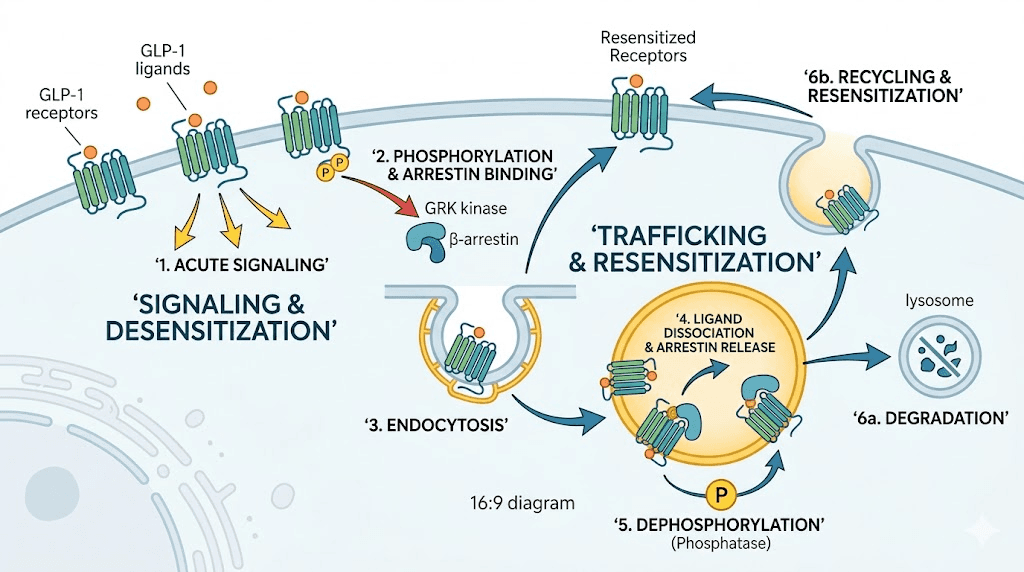
Before you can reset something, you need to understand what changed. The GLP-1 receptor is a G protein-coupled receptor that sits on the surface of cells throughout your body. When a GLP-1 agonist like semaglutide binds to it, the receptor activates a cascade of intracellular signaling events. These signals suppress appetite, slow gastric emptying, enhance insulin secretion, and promote satiety.
Simple enough. But cells are smart. They do not like being overstimulated.
How receptors respond to continuous stimulation
When a GLP-1 agonist binds continuously to the receptor, the cell initiates a protective response. Specific enzymes called GRKs, or G protein-coupled receptor kinases, phosphorylate the receptor at precise locations on its intracellular tail. Research has identified three critical serine doublets at positions 441/442, 444/445, and 451/452 that must be phosphorylated for full desensitization to occur.
This phosphorylation acts like a molecular off switch. Once these sites are tagged, the receptor can no longer efficiently activate its downstream G protein partners. The signal weakens. The appetite suppression becomes less pronounced. The satiety effects diminish.
The speed of this process is striking. Research published in Molecules measured the net desensitization half-life at just 2.99 minutes. The apparent desensitization half-life, which accounts for receptor recycling, was 19.27 minutes. In practical terms, the receptors on any given cell begin losing sensitivity within minutes of sustained agonist exposure.
But here is the critical nuance. The body compensates. New receptors are synthesized. Existing receptors are recycled back to the surface after dephosphorylation. In healthy physiology, there is a dynamic equilibrium between desensitization and resensitization that maintains overall receptor responsiveness despite continuous agonist presence.
Beta-arrestin recruitment and receptor internalization
Phosphorylation is just the first step. Once tagged, the receptor attracts proteins called beta-arrestins. These molecular chaperones bind to the phosphorylated receptor and serve two purposes. They physically block the receptor from interacting with G proteins, which terminates signaling. And they connect the receptor to the cell internalization machinery, specifically clathrin-coated pits that pull the receptor off the cell surface and into intracellular compartments called endosomes.
Once internalized, the receptor faces two possible fates. It can be dephosphorylated and recycled back to the cell surface, ready to signal again. Or, after prolonged or particularly intense stimulation, it can be routed to lysosomes for degradation. Research shows that 12-hour sustained stimulation leads to marked receptor downregulation, meaning the cell actually destroys receptors rather than recycling them.
This matters for reset protocols. Short-term desensitization through phosphorylation and internalization is rapidly reversible. Researchers at the University of Oxford found that beta-arrestin mediated desensitization in pancreatic beta cells recovered within six hours of agonist removal. But true receptor downregulation through lysosomal degradation requires the cell to synthesize entirely new receptors, a process that takes considerably longer.
Recent research has added another layer of complexity. A study published in the FEBS Journal found that GLP-1 receptor internalization can proceed through arrestin-independent pathways involving GRK, clathrin, and caveolae-dependent mechanisms. This means even when one desensitization pathway is blocked, backup systems exist. The cell really does not want to be overstimulated.
What this means for your response
So how does all of this translate to what you experience taking GLP-1 medications?
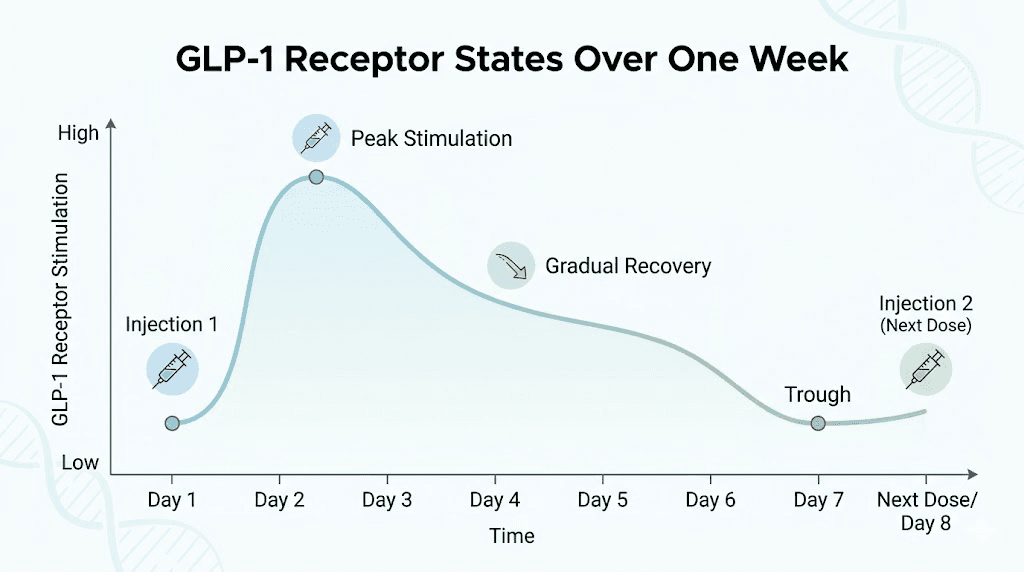
The weekly dosing schedule of medications like semaglutide and tirzepatide was designed with desensitization in mind. Drug levels naturally fluctuate between doses, creating periods of relatively lower receptor occupancy that allow partial receptor recovery. The pharmacokinetic half-life of semaglutide is approximately 168 hours, or one week. This means the drug does not hit peak levels and stay there permanently. There are natural ebbs and flows in receptor stimulation that support ongoing sensitivity.
However, at higher doses, the trough levels between injections may remain high enough that receptors never fully recover. This is one theoretical explanation for why dose escalation sometimes produces diminishing returns. The system never gets a meaningful break from stimulation.
Plateau vs true tolerance: the critical distinction
This is where most people go wrong. They hit a semaglutide plateau or notice their tirzepatide is not working anymore and immediately assume the medication has failed. They start googling how to reset their receptors when the actual problem has nothing to do with receptors at all.
Weight loss plateaus on GLP-1 medications are expected. Not just normal. Expected. The STEP clinical trials showed that weight loss on semaglutide 2.4 mg typically begins to plateau around week 60. A landmark physiology paper published in Obesity Reviews modeled the mathematics precisely. Semaglutide at maximum dose produces an intervention magnitude of approximately 1,300 kcal per day, with an expected plateau timeline of around 24 months. Tirzepatide at 10 mg produces roughly 1,560 kcal per day of intervention with a similar plateau timeline.
Signs you are experiencing a metabolic plateau
A metabolic plateau looks like this. Weight loss stalls or slows dramatically. But appetite suppression persists. You still feel full after smaller meals. You still notice reduced food noise. The medication is clearly doing something, just not producing weight loss anymore.
The reason is straightforward. Research from that same physiology paper found that semaglutide reduces the appetite feedback parameter to 49 kcal per day per kilogram of weight loss, compared to 82-83 kcal per day per kilogram during calorie restriction alone. This roughly 40 percent reduction in appetite feedback strength is why GLP-1 medications produce more weight loss than dieting alone. But eventually, the body metabolic adaptation catches up to even this reduced appetite drive.
Energy expenditure decreases. But here is a silver lining. The decrease is approximately 150 kcal per day less than predicted by standard metabolic models, suggesting GLP-1 medications partially protect against the severe metabolic slowdown seen with dieting alone. Your metabolism slows, but not as catastrophically as it would without medication.
If this is your situation, a GLP-1 reset through receptor recovery is not what you need. You need diet optimization, exercise strategies, or potentially a dose adjustment.
Signs of genuine receptor desensitization
True receptor desensitization presents differently. The key marker is loss of subjective medication effects, not just loss of weight loss. If your appetite suppression has noticeably weakened, if food noise has returned to pre-medication levels, if you can eat larger meals without discomfort, and if the characteristic feeling of the medication has faded, these point toward receptor level changes rather than simple metabolic adaptation.
Data from a study examining prior GLP-1 users versus naive users supports this distinction. Patients previously treated with GLP-1 medications lost 4.8 percent of body weight after 40 weeks on tirzepatide, compared to 7.5 percent for GLP-1 naive patients. That 2.7 percentage point gap suggests prior receptor exposure may genuinely reduce subsequent responsiveness.
Does this mean your receptors are permanently damaged? No. It means they need time and the right conditions to recover.
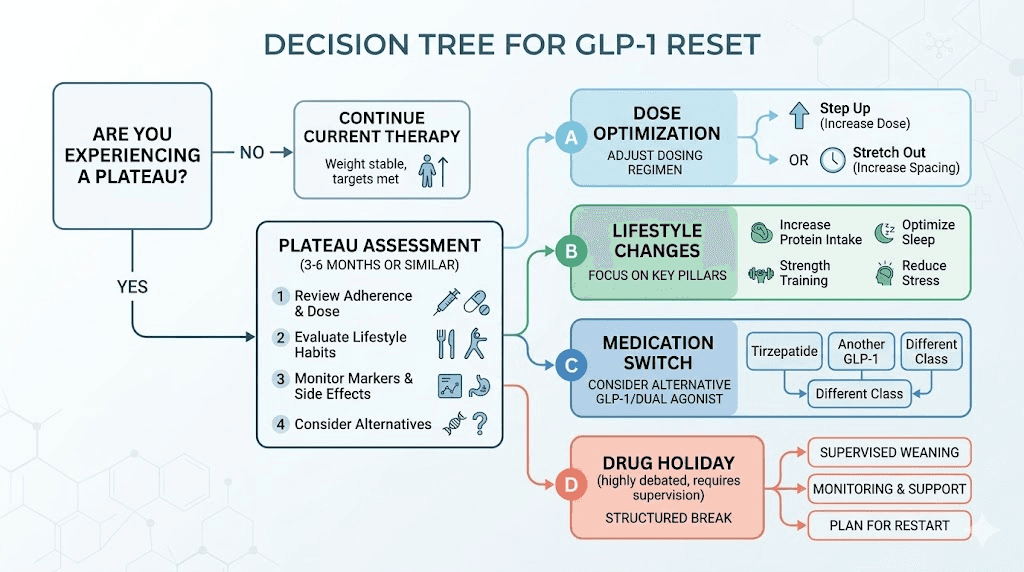
The drug holiday approach: structured medication breaks
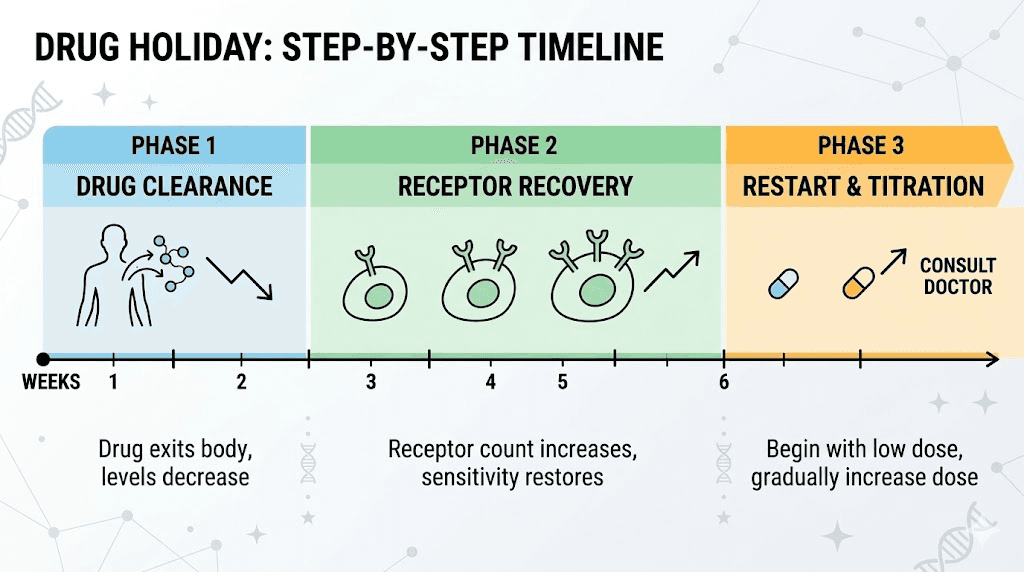
A drug holiday, sometimes called a structured medication break, is the most direct approach to a GLP-1 reset. The concept is simple. Stop the medication for a defined period. Allow receptors to recover their density and sensitivity. Then restart at a lower dose and titrate back up.
The recommended duration based on clinical guidance ranges from 4 to 8 weeks of complete discontinuation. This timeframe accounts for the pharmacokinetics of long-acting GLP-1 agonists. Semaglutide has a half-life of approximately one week, so it takes roughly five weeks for the drug to be essentially cleared from your system. Tirzepatide has a similar half-life of about five days. Only after the drug has substantially cleared can receptors fully recover without ongoing stimulation.
What happens during the first two weeks
The initial phase of a drug holiday is the hardest. As drug levels decline, appetite suppression weakens progressively. Most people notice increased hunger within 7-10 days of their last injection. Food noise returns. Portions that felt satisfying on medication suddenly feel inadequate.
This is not your imagination. The medication was actively suppressing appetite through multiple pathways. Slowed gastric emptying reverses. Central appetite suppression through hypothalamic signaling fades. Nausea-mediated appetite reduction, if present, disappears.
Semaglutide withdrawal symptoms can include increased hunger, cravings for high-calorie foods, and sometimes gastrointestinal changes as the gut readjusts to normal motility. The severity varies considerably between individuals.
Weeks three through six: receptor recovery
This is where the actual reset happens. With drug levels approaching negligible, GLP-1 receptors begin recovering in earnest. Internalized receptors are recycled back to the cell surface. New receptors are synthesized. The receptor density on target cells gradually returns toward pre-treatment levels.
There is no blood test that measures GLP-1 receptor sensitivity, so you cannot track this process directly. But the theory is supported by basic receptor pharmacology principles that apply across all G protein-coupled receptors. Remove the agonist, and the system resets. The timeline varies by tissue type and individual, but four to six weeks appears sufficient based on the pharmacokinetic clearance data and general GPCR biology.
Managing weight during a GLP-1 pause
This is the elephant in the room. Weight regain during medication breaks is real and often substantial. The STEP trial extension data showed that participants regained approximately 40 percent of lost weight within 28 weeks of stopping semaglutide. The SURMOUNT-4 trial found over 50 percent of tirzepatide weight loss rebounded over 52 weeks. A systematic review and meta-analysis published in eClinicalMedicine reported pooled mean weight regain of 5.63 kg and 5.81 percent of body weight.
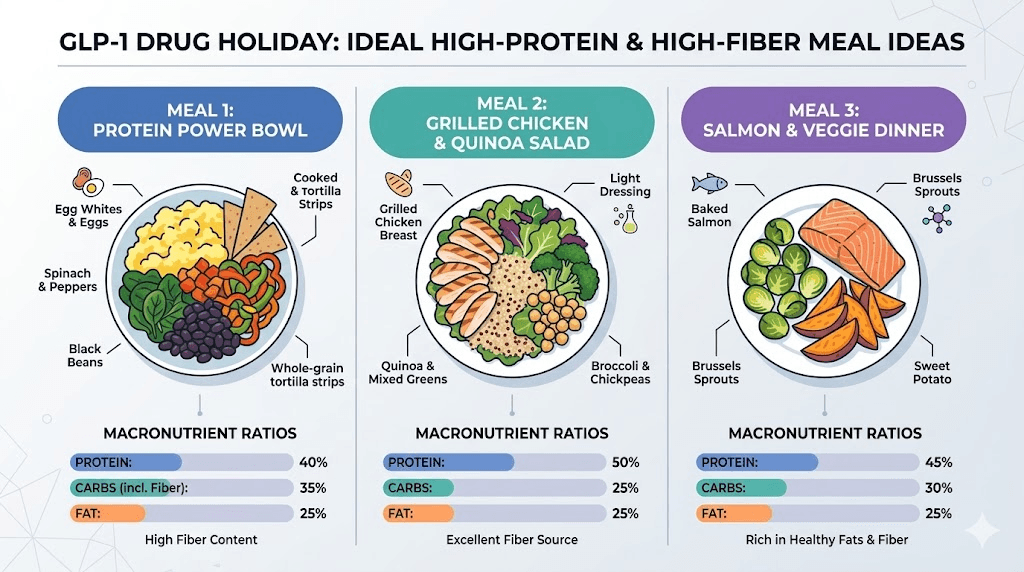
But a 4-8 week drug holiday is much shorter than the 28-52 week discontinuation periods in those studies. The key strategies for minimizing regain during a short break include maintaining a high protein intake of 1.6-2.2 grams per kilogram of body weight daily, continuing or increasing resistance training to preserve muscle mass, planning meals in advance so hunger does not drive impulsive food choices, monitoring weight weekly but not daily to avoid overreacting to normal fluctuations, and staying hydrated since the body may retain more water without GLP-1 mediated effects on fluid balance.
Some weight regain during the break is expected and acceptable. The goal is not to maintain exact weight. The goal is to keep regain minimal enough that the reset period provides net benefit when medication is restarted with restored sensitivity.
How to restart after a reset
Restarting after a drug holiday requires the same approach as initial dose titration. Do not jump back to your previous maintenance dose. This is critical. Your body has re-sensitized, which means the same dose that barely affected you before the break may now produce significant effects, including potentially severe gastrointestinal side effects.
For semaglutide, the standard restart protocol begins at 0.25 mg weekly for four weeks, then escalates through the standard titration schedule. For tirzepatide, restart at 2.5 mg weekly. If you previously reached maximum doses, you may find that a lower dose now produces the same or better effects than your pre-break maximum, which is exactly the point of the reset.
Some researchers find they never need to return to their pre-break dose. If you were on 2.4 mg semaglutide and experiencing diminishing returns, you might find that 1.7 mg after a reset produces stronger appetite suppression than 2.4 mg did before. This is the practical proof that the reset worked.
Switching between GLP-1 medications as a reset strategy
Not everyone wants to take a complete medication break. The weight regain risk, even for just 4-8 weeks, feels too high. There is an alternative. Switching to a different GLP-1 medication can provide a partial reset by engaging slightly different receptor profiles while maintaining continuous appetite suppression.
Semaglutide to tirzepatide: the most common switch
The most researched switch is from semaglutide to tirzepatide. This works because tirzepatide is not simply a stronger version of semaglutide. It is a fundamentally different molecule. Semaglutide is a pure GLP-1 receptor agonist. Tirzepatide is a dual agonist that activates both the GLP-1 receptor and the GIP receptor. This dual mechanism means tirzepatide engages pathways that were not being stimulated by semaglutide, providing a form of receptor novelty.
The clinical data supports this approach. In a large study of over 18,000 patients, those taking tirzepatide lost about 15.3 percent of body weight in one year compared to 8.3 percent with semaglutide. When patients specifically switched from semaglutide to tirzepatide, they continued losing weight. In one study, switchers lost an additional 2.15 kg in just 12 weeks, along with a 0.43 percent improvement in HbA1c and 7.83 mg/dL reduction in fasting glucose.
The switch process is straightforward. Research shows that transitioning within 3-10 days of the last semaglutide dose is well tolerated. No extended washout period is necessary. Most practitioners start tirzepatide at its lowest dose of 2.5 mg regardless of the previous semaglutide dose to minimize gastrointestinal side effects during the transition.
If you want the detailed conversion numbers, SeekPeptides maintains comprehensive dose conversion charts that map equivalent doses between the two medications.
Why dual agonists may overcome single-receptor tolerance
The GIP receptor pathway is distinct from GLP-1 signaling. GIP, or glucose-dependent insulinotropic polypeptide, influences adipose tissue metabolism, bone health, and central appetite regulation through mechanisms that differ from GLP-1. When semaglutide has maximally stimulated the GLP-1 pathway, adding GIP receptor activation through tirzepatide provides a genuinely new stimulus that desensitized GLP-1 receptors alone cannot explain away.
This is also why retatrutide generates such interest. As a triple agonist targeting GLP-1, GIP, and glucagon receptors, it engages even more pathways than tirzepatide. Researchers who have plateaued on dual agonists are exploring whether the switch from tirzepatide to retatrutide provides another level of receptor novelty and metabolic activation.
Tirzepatide to semaglutide: going the other direction
Some researchers switch from tirzepatide back to semaglutide. This might seem counterintuitive since tirzepatide is generally considered more effective. But the logic is sound. If your GIP receptors have desensitized alongside your GLP-1 receptors, switching to a pure GLP-1 agonist removes the GIP stimulus entirely, allowing those receptors to recover while you maintain GLP-1 mediated appetite suppression with a different agonist profile.
The tirzepatide to semaglutide switch requires careful dose conversion since the medications are not equivalent milligram for milligram. After a period on semaglutide, you can then switch back to tirzepatide and potentially experience renewed dual agonist benefits from recovered GIP receptors.
Some researchers take this a step further, alternating between semaglutide and tirzepatide in planned cycles. The evidence for this approach is entirely anecdotal at this point, but the receptor pharmacology logic supports the concept of periodic receptor novelty.
Lifestyle strategies that support receptor sensitivity
Medication strategies are only part of the equation. What you do outside of injections significantly influences how your receptors respond and how effectively any reset protocol works.
Protein: the non-negotiable foundation
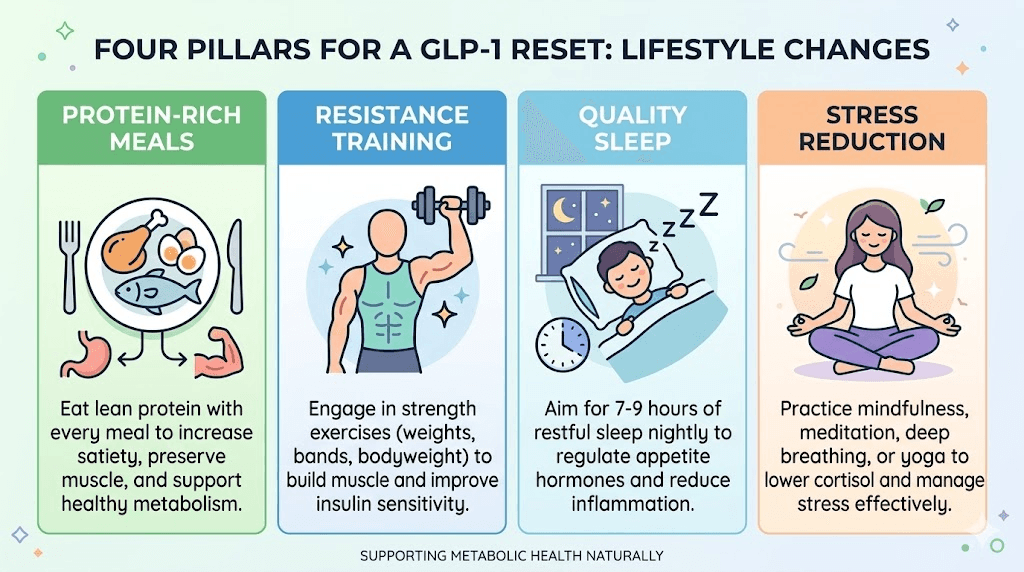
Protein intake during GLP-1 therapy, and especially during any reset period, deserves more attention than it typically receives. The recommended range for researchers on GLP-1 medications is 1.6-2.2 grams per kilogram of body weight daily. This is substantially higher than the standard dietary recommendation of 0.8 grams per kilogram.
Why does protein matter for a reset? Three reasons. First, adequate protein preserves lean muscle mass during weight loss. Concerning data from semaglutide trials showed substantially less fat loss than predicted, indicating greater lean mass loss than expected. Losing muscle reduces your metabolic rate, accelerates plateau formation, and makes any reset period less effective because you are fighting against a slower metabolism.
Second, protein has the highest thermic effect of any macronutrient. Your body burns approximately 20-30 percent of protein calories just processing them, compared to 5-10 percent for carbohydrates and 0-3 percent for fats. This matters during a drug holiday when you want to maximize calorie expenditure.
Third, protein promotes satiety independent of GLP-1 signaling. During a drug holiday when medication-driven appetite suppression fades, protein-rich meals become your primary tool for managing hunger. Check out our guides on the best foods to eat on semaglutide and what to eat on tirzepatide for specific meal ideas that prioritize protein.
Resistance training and metabolic rate preservation
Resistance training during GLP-1 therapy is not optional. It is essential. And during a reset period, it becomes even more critical. Every pound of muscle you preserve maintains roughly 6-10 additional calories of daily resting metabolic expenditure. That does not sound like much until you consider that losing 10 pounds of lean mass, which is entirely possible on GLP-1 medications without strength training, could reduce your daily calorie burn by 60-100 calories permanently.
The compounding effect matters. Over a year, that 60-100 calorie daily deficit represents 6-10 pounds of potential weight loss or, conversely, 6-10 pounds of easier weight regain during a drug holiday. Resistance training also improves insulin sensitivity independent of weight loss, which supports better metabolic function and may complement GLP-1 receptor resensitization.
For researchers specifically on peptides for fat loss, the combination of maintaining resistance training while implementing a GLP-1 reset creates the best possible conditions for continued progress when medication resumes.
Sleep: the overlooked reset amplifier
Poor sleep actively works against GLP-1 receptor sensitivity. Research consistently shows that sleep deprivation increases ghrelin (the hunger hormone), decreases leptin (the satiety hormone), impairs insulin sensitivity, and increases cortisol. All of these effects counteract the metabolic benefits you are trying to preserve during a reset.
During a drug holiday specifically, sleep quality becomes even more important because you have lost the medication-driven appetite suppression that previously compensated for suboptimal sleep habits. Seven to nine hours of quality sleep per night is the target. If you have been getting by on six hours because the medication suppressed your appetite regardless, that approach will fail during a reset period.
Practical sleep optimization includes consistent bed and wake times, cool sleeping environment around 65-68 degrees Fahrenheit, no screens for 60 minutes before bed, limiting caffeine after noon, and addressing any underlying insomnia or sleep disruption that may have developed during treatment.
Stress management and cortisol control
Chronic stress elevates cortisol, which promotes abdominal fat storage, increases insulin resistance, and drives cravings for high-calorie comfort foods. During a GLP-1 reset, elevated cortisol can accelerate weight regain and potentially interfere with receptor recovery processes.
The connection between stress and GLP-1 function runs deeper than most people realize. Cortisol directly impairs insulin signaling pathways that overlap with GLP-1 receptor cascades. Reducing cortisol through stress management is not just about feeling better. It creates a more favorable biochemical environment for receptor resensitization.
Practical approaches include daily walks of 20-30 minutes, meditation or breathing exercises for 10-15 minutes, reducing exposure to stressful news and social media, and maintaining social connections that provide emotional support during the challenging drug holiday period.
Dose optimization strategies before considering a full reset
Before committing to a drug holiday or medication switch, explore whether dose optimization can break the plateau. Sometimes the answer is simpler than a full receptor reset.
Dose escalation timing
Many researchers plateau because they have not yet reached their optimal dose. The standard semaglutide dosing protocol starts at 0.25 mg and escalates to 2.4 mg over 16-20 weeks. But some researchers titrate too slowly, sitting at sub-therapeutic doses for months. Others titrate too quickly, developing side effects that force dose reductions.
If you are on a moderate dose and experiencing a plateau, the first question is whether you have room to escalate. Check your current dose against the semaglutide dosage chart or tirzepatide dosing chart to see where you stand. The semaglutide dosage calculator on SeekPeptides can help determine your appropriate dose based on your current weight and response.
Microdosing approaches
On the opposite end of the spectrum, some researchers find success with microdosing tirzepatide or lower-dose protocols. The theory is that smaller, more frequent doses maintain receptor stimulation at a level that avoids heavy desensitization while preserving beneficial effects. A microdosing tirzepatide chart can help structure this approach.
Microdose protocols typically involve taking smaller amounts more frequently, such as dividing the weekly dose into two or three smaller injections. This creates a flatter pharmacokinetic curve with lower peak levels and higher trough levels, potentially reducing the intensity of receptor desensitization at peak concentrations while maintaining more consistent receptor occupancy throughout the week.
Split dosing
Related to microdosing but distinct is the concept of splitting your semaglutide dose or splitting your tirzepatide dose into twice-weekly administrations. Instead of one 2.4 mg injection weekly, you might take 1.2 mg twice weekly. The total dose remains the same, but the pharmacokinetic profile changes.
Split dosing can reduce side effects, provide more consistent appetite suppression throughout the week, and theoretically reduce peak receptor stimulation that drives desensitization. Some researchers report that split dosing broke their plateau without any change in total weekly dose.
Diet strategies during and after a GLP-1 reset
Your nutrition approach during a reset period requires deliberate planning. Without medication-driven appetite suppression, you are relying entirely on food choices, meal timing, and behavioral strategies to maintain control.
Pre-reset preparation
Start preparing your nutrition environment one to two weeks before beginning a drug holiday. Stock your kitchen with high-protein, high-fiber foods that promote satiety. Remove or reduce easy-access hyper-palatable foods that you know trigger overeating. Meal prep several days of meals in advance so that when hunger returns, healthy options are the path of least resistance.
Review the semaglutide diet plan and tirzepatide diet plan resources for structured meal frameworks. The food lists for semaglutide users still apply during a drug holiday since these foods were selected for their satiety-promoting properties, not their medication interactions.
During the drug holiday
Caloric needs will increase during the break as appetite returns. Accept this. Fighting extreme hunger with severe restriction will backfire, leading to binge episodes and potentially larger weight regain than a moderate approach. A reasonable target is maintenance calories for your current weight, not a caloric deficit. You are not trying to lose weight during the break. You are trying to minimize regain while allowing receptor recovery.
Prioritize meals that combine protein, fiber, and healthy fats for maximum satiety. Good options include lean meats with vegetables, Greek yogurt with berries and nuts, eggs with avocado and whole grain toast, and fish with complex carbohydrates. Avoid the same foods you avoided on medication since the reasons for avoiding them, rapid glucose spikes, low satiety, gastrointestinal distress, remain relevant even without the medication.
Supplements like fiber supplements, probiotics, and B vitamins can support digestive function and energy levels during the transition period. Some researchers add berberine during drug holidays for its blood sugar regulating properties, though this should be discussed with a healthcare provider.
Post-reset nutrition
When restarting medication after a reset, return to the same nutrition principles you followed during initial treatment. Start with smaller portions and see how your re-sensitized system responds. Many researchers find that the same meal that barely suppressed their appetite before the reset now feels substantially more filling. This is a positive sign that the reset achieved its goal.
Timeline expectations: what a realistic GLP-1 reset looks like
Setting realistic expectations prevents disappointment and premature abandonment of the reset protocol. Here is what a typical 6-week drug holiday timeline looks like based on pharmacokinetic data and clinical reports.
Week 1: Drug levels declining but still pharmacologically active. Minimal change in appetite or weight. You may not notice anything different. This is the easy part.
Week 2: Drug levels approaching sub-therapeutic range. Appetite begins returning. Hunger between meals increases. Withdrawal symptoms like increased cravings may appear. Weight may increase slightly, partly from water retention as GLP-1 mediated effects on fluid balance normalize. Some people experience gastrointestinal changes as gastric emptying rate returns to normal.
Weeks 3-4: Drug is essentially cleared from the system. Full appetite has returned. This is the most challenging period mentally and physically. Weight regain of 2-4 pounds is common, primarily from increased food intake and water/glycogen restoration. Receptor recovery is actively occurring during this window.
Weeks 5-6: Receptors approaching baseline sensitivity. Appetite is at pre-treatment levels. Weight may stabilize if nutrition and exercise are well managed. This is when the reset process is completing its work. Some people feel like they have fully returned to their pre-medication state.
Week 7 (restart): Begin medication at the initial starting dose. Within the first one to two injections, you should notice a return of appetite suppression that may feel as strong as when you first started treatment. If this happens, the reset was successful. Titrate up gradually based on response, and you may find your new effective dose is lower than your pre-reset dose.
Total expected weight regain during a 6-week holiday with proper nutrition management: 3-8 pounds. Expected timeline to return to pre-break weight after restarting: 4-8 weeks if the reset successfully restored receptor sensitivity.
When a GLP-1 reset is NOT the answer
Not every stall needs a reset. Sometimes the solution is simpler. Sometimes the problem is deeper. Knowing when NOT to attempt a reset is just as important as knowing how to do one.
When dose optimization is the real answer
If you have not yet reached your maximum tolerated dose, a reset is premature. Work through the full tirzepatide dosing guide or semaglutide dosing protocol before considering a drug holiday. Many plateaus break simply by increasing from a moderate to a higher dose.
Similarly, if your plateau started immediately after a dose reduction due to side effects, the plateau is dose-related, not receptor-related. Strategies for managing constipation, bloating, headaches, and fatigue can help you tolerate higher doses without needing to reduce.
When lifestyle factors are the bottleneck
If you are consuming excess calories despite appetite suppression (eating through fullness signals), not exercising, sleeping poorly, or under chronic stress, a receptor reset will not fix these issues. The medication could have perfect receptor binding and still not produce weight loss if the caloric balance equation does not favor it.
Before attempting a reset, honestly assess whether the following are optimized. Food choices. Portion awareness. Alcohol consumption. Physical activity level. Injection timing. Sleep duration and quality. Stress levels.
When something else is going on medically
Stalled weight loss can signal medical issues unrelated to GLP-1 receptor sensitivity. Thyroid dysfunction, hormonal imbalances, new medications with weight-promoting side effects, insulin resistance progression, and water retention from various causes can all masquerade as medication tolerance. A comprehensive medical evaluation should precede any self-directed reset protocol.
Additionally, some researchers notice menstrual cycle changes or hormonal shifts that coincide with apparent plateaus. These may be temporary and resolve without any medication changes.
Advanced reset strategies
For researchers who have tried basic approaches without success, several advanced strategies exist in the community.
Compound blends during transition periods
Some compounding pharmacies offer GLP-1 formulations blended with additional compounds like B12, glycine, L-carnitine, or niacinamide. While these blends do not directly address receptor desensitization, they may support metabolic function during reset periods.
B12 and methylcobalamin support energy production, which can help combat the fatigue many researchers experience during drug holidays. Glycine and B12 blends provide both amino acid support and neurological benefits. L-carnitine supports fat metabolism during periods when GLP-1 mediated fat oxidation effects are absent.
Combining with complementary peptides
Some researchers explore complementary peptides during reset periods. AOD 9604, a fragment of human growth hormone, targets fat metabolism through entirely different pathways than GLP-1 signaling. MOTS-c activates AMPK pathways that enhance metabolic function. 5-amino-1MQ inhibits NNMT enzyme activity, which may support fat metabolism.
These approaches remain largely experimental and should be discussed with a qualified healthcare provider. But for researchers who want to maintain some metabolic support during a GLP-1 drug holiday, peptide stacking offers potential options.
The retatrutide factor
For researchers who have plateaued on both semaglutide and tirzepatide, retatrutide represents the next frontier. As a triple agonist activating GLP-1, GIP, and glucagon receptors, it provides the most comprehensive receptor coverage available. The glucagon receptor component adds a thermogenic element that neither semaglutide nor tirzepatide can match, directly increasing energy expenditure.
Early clinical data shows retatrutide produces weight loss exceeding both semaglutide and tirzepatide in head-to-head comparisons. For researchers who have desensitized to dual agonist therapy, the addition of the glucagon receptor pathway provides genuinely novel stimulation. The retatrutide dosage chart and dosage calculator can help determine appropriate starting points.
Monitoring your reset: what to track
A GLP-1 reset without tracking is just a hope. Systematic monitoring helps you determine whether the reset worked and guides decisions about dose titration when restarting.
Before the break, document: Current dose. Current weight. Waist circumference. Subjective appetite rating on a 1-10 scale. Typical daily calorie intake. Exercise frequency and intensity. Any side effects present.
During the break, track weekly: Weight. Waist circumference. Appetite rating. Average daily calorie intake. Exercise adherence. Sleep quality. Stress level. Energy level. These markers create a baseline that you will compare against once medication restarts.
After restarting, monitor: Appetite suppression onset, specifically how quickly after the first injection do you notice effects? Food noise reduction. Portion size changes. Side effect profile, since a stronger restart response indicates successful resensitization. Rate of weight loss in the first 4-8 weeks. Dose at which full effects are achieved compared to pre-break dose.
The most telling indicator is dose response comparison. If you achieve the same appetite suppression at 1.7 mg semaglutide that previously required 2.4 mg, the reset objectively worked. Use the peptide calculator to track dose relationships over time.
Common mistakes that undermine a GLP-1 reset
Even well-planned resets can fail if these common errors are not avoided.
Mistake 1: Too short a break. A two-week medication pause is not enough. The drug has not fully cleared, and receptors have not had adequate time to recover. The minimum effective drug holiday appears to be four weeks, with six weeks providing a more complete reset based on pharmacokinetic clearance data.
Mistake 2: Restarting at your pre-break dose. This is potentially dangerous and almost certainly counterproductive. Re-sensitized receptors respond much more strongly to the medication. Starting at the full dose can cause severe nausea, vomiting, and other gastrointestinal effects that may force you to stop again. Always restart at the initial titration dose and work up.
Mistake 3: Unrestricted eating during the break. Some researchers view the drug holiday as a free pass to eat whatever they want. This undermines the reset in multiple ways. Excessive weight regain means you spend weeks after restarting just getting back to where you were. Inflammatory foods may worsen receptor function. And established poor habits are harder to break once medication restarts.
Mistake 4: Ignoring the psychological component. The return of hunger and food noise after months of suppression can be psychologically distressing. Researchers who do not prepare for this experience often panic, abandon the reset early, or develop unhealthy coping mechanisms. Mental preparation is as important as nutritional preparation.
Mistake 5: Not consulting a healthcare provider. Self-directed drug holidays carry risks, especially for people using GLP-1 medications for diabetes management where blood sugar control may deteriorate during the break. Always involve your prescribing physician in any decision to pause medication.
The future of GLP-1 reset strategies
The science of GLP-1 receptor pharmacology is advancing rapidly. Several developments may change how resets are approached in the coming years.
G protein-biased agonists represent one promising direction. These molecules are designed to activate beneficial signaling pathways while minimizing beta-arrestin recruitment that drives desensitization. Research published in the British Journal of Pharmacology suggests that biased agonists could maintain GLP-1 receptor efficacy over longer periods, potentially making resets unnecessary.
Oral formulations of GLP-1 agonists, including oral semaglutide and oral tirzepatide, create different pharmacokinetic profiles than injections. The shorter duration of action and different absorption patterns may naturally reduce receptor desensitization by creating more pronounced peaks and troughs in drug levels. Patch formulations offer yet another delivery profile.
The next generation of oral GLP-1 agents like orforglipron may also offer different receptor binding kinetics that reduce desensitization risk. As the field evolves, SeekPeptides will continue providing the latest evidence-based guidance on optimal protocols.
Frequently asked questions
How long does it take for GLP-1 receptors to reset?
Based on pharmacokinetic data, a minimum of 4 weeks of complete medication discontinuation allows for substantial drug clearance and receptor recovery. Most clinicians recommend 6-8 weeks for a more thorough reset. At the cellular level, receptor recycling begins within hours of reduced agonist exposure, but full receptor density restoration requires complete drug clearance first.
Will I regain all my weight during a drug holiday?
Not during a short 4-8 week break. Long-term studies show significant weight regain over 6-12 months of discontinuation, but a structured short break with proper weight maintenance strategies typically results in 3-8 pounds of regain, much of which is water weight and glycogen restoration that reverses quickly upon restarting medication.
Can I switch medications instead of taking a complete break?
Yes. Switching from semaglutide to tirzepatide provides receptor novelty through GIP receptor activation while maintaining continuous appetite suppression. This avoids the weight regain risk of a full drug holiday. The transition between medications is well-studied and generally well tolerated.
Is my plateau a sign the medication is not working anymore?
Usually not. Weight loss plateaus are a normal part of the process reflecting metabolic adaptation, not medication failure. The key distinction is whether you still feel appetite suppression. If satiety effects persist despite stalled weight loss, the medication is working. Your body has simply adapted to the new caloric equilibrium.
How do I know if my GLP-1 has truly stopped working?
True medication failure presents as loss of all subjective effects: appetite suppression gone, food noise returned, portion sizes increased, and characteristic medication sensations absent. This differs from a perceived plateau where weight loss stalls but appetite control remains intact. If your appetite is still suppressed, the medication is still working.
Should I tell my doctor about a planned drug holiday?
Absolutely. Self-directed medication breaks carry risks, especially for individuals with diabetes or other metabolic conditions. Blood sugar management may need adjustment during the break period. Your healthcare provider can also monitor for adverse effects and help structure the restart protocol safely.
Can I do a partial reset by just lowering my dose?
Dose reduction provides a less intense but potentially useful partial reset. Dropping from 2.4 mg to 1.0 mg semaglutide reduces receptor stimulation intensity while maintaining some appetite suppression. After 4-6 weeks at the reduced dose, titrating back up may produce improved effects. This is a middle-ground approach between a full drug holiday and no intervention.
What about GLP-1 tolerance for blood sugar control vs weight loss?
Interesting distinction. Clinical evidence suggests that tolerance to GLP-1 glucose-lowering effects does not develop in humans, despite occurring in animal models. Weight loss plateau mechanisms appear to be primarily metabolic adaptation rather than receptor tolerance. This means the medication continues protecting your blood sugar and metabolic health even when weight loss has stalled.
External resources
Physiology of the Weight Loss Plateau after GLP-1 Receptor Agonism - PMC
Tolerance Does Not Develop Toward Liraglutide Glucose-Lowering Effect - JCEM
For researchers serious about optimizing their GLP-1 protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your receptors stay sensitive, your plateaus stay temporary, and your progress stay consistent.