Feb 23, 2026

What if the real reason your GLP-1 oral liquid is not working has nothing to do with the formula itself, but everything to do with how often you take it?
This is the question that frustrates thousands of people every month. They fill their prescription. They measure their dose. They place the drops under their tongue. And then they wait. Nothing happens. Or worse, they get hit with nausea so intense they want to quit entirely. The missing piece is almost always dosing frequency, the timing between doses, and the specific protocol that matches their formulation type.
GLP-1 oral liquid is not one product. It includes FDA-approved tablets like Rybelsus, compounded sublingual drops from pharmacies, and even newer formulations hitting the market. Each one has a completely different dosing frequency. Take the wrong one at the wrong interval and you are either wasting your medication or making side effects worse than they need to be. Oral semaglutide drops work on a daily schedule. Tirzepatide drops follow their own separate protocol. And the sublingual formulations that compounding pharmacies produce have absorption characteristics that change everything about when and how often you should dose.
This guide covers every GLP-1 oral liquid formulation, the exact dosing frequencies for each, week-by-week titration schedules, the best time of day to take them, what happens when you miss a dose, and the absorption tricks that make or break your results. Whether you are on compounded semaglutide drops or considering oral tirzepatide, the dosing frequency information here will help you get the most from every single drop.
Understanding GLP-1 oral liquid formulations
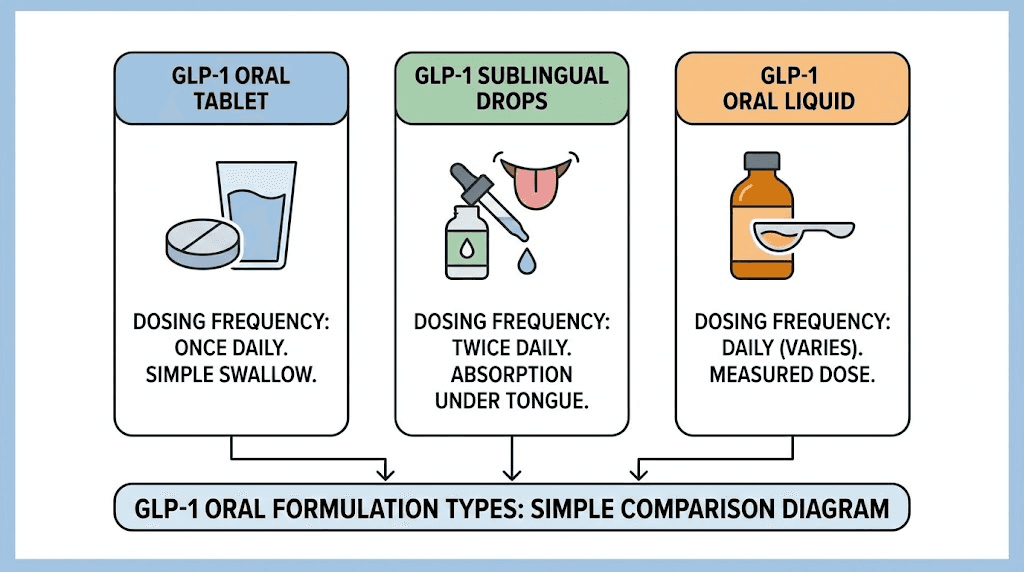
Before diving into dosing frequency, you need to understand which type of GLP-1 oral liquid you are actually taking. This matters because the formulation determines the frequency. Get this wrong and everything downstream falls apart.
FDA-approved oral GLP-1 tablets
Rybelsus is the most well-known FDA-approved oral semaglutide. It comes as a tablet, not a liquid, but many people search for "GLP-1 oral liquid" when they actually mean any oral GLP-1 formulation. Rybelsus uses a special absorption enhancer called SNAC (sodium N-[8-(2-hydroxybenzoyl)amino]caprylate) that protects semaglutide from stomach acid and helps it cross the gastric lining. This is a once-daily medication. No exceptions.
The Wegovy pill formulation also entered the market for weight management. Same active ingredient, different dose range. Still once daily. The key thing to understand about GLP-1 medications like these is that the tablet form requires strict empty-stomach protocols because food destroys absorption almost completely.
Compounded sublingual GLP-1 drops
This is where most of the confusion lives. Compounded sublingual drops are liquid formulations of semaglutide or tirzepatide prepared by compounding pharmacies. You place them under your tongue, hold them there, and the medication absorbs through the mucous membranes in your mouth. These are not FDA-approved as sublingual formulations, though the active ingredients themselves have FDA approval in other delivery forms.
The dosing frequency for sublingual drops is typically once daily. Some providers allow patients to move to three times per week once they reach a steady state. But the starting protocol is almost always daily. Sublingual semaglutide and sublingual peptides in general rely on consistent daily exposure to build and maintain therapeutic blood levels.
GLP-1 six-in-one oral liquid products
Some products marketed as "GLP-1 oral liquid" combine multiple ingredients. The GLP-1 six-in-one oral liquid is one example that has gained attention. These combination products typically include a GLP-1 receptor agonist alongside herbal ingredients, vitamins, or other compounds. Their dosing schedules vary by manufacturer and should always follow the specific product label.
Understanding how peptides work at the molecular level helps explain why different formulations require different frequencies. The half-life of the active ingredient, the absorption pathway, and the bioavailability all play roles in determining how often you need to dose.
How often to take FDA-approved oral GLP-1 tablets
Once a day. That is the answer for every FDA-approved oral GLP-1 tablet currently on the market. But the details around that daily dose matter enormously for effectiveness.
Rybelsus (oral semaglutide) dosing frequency
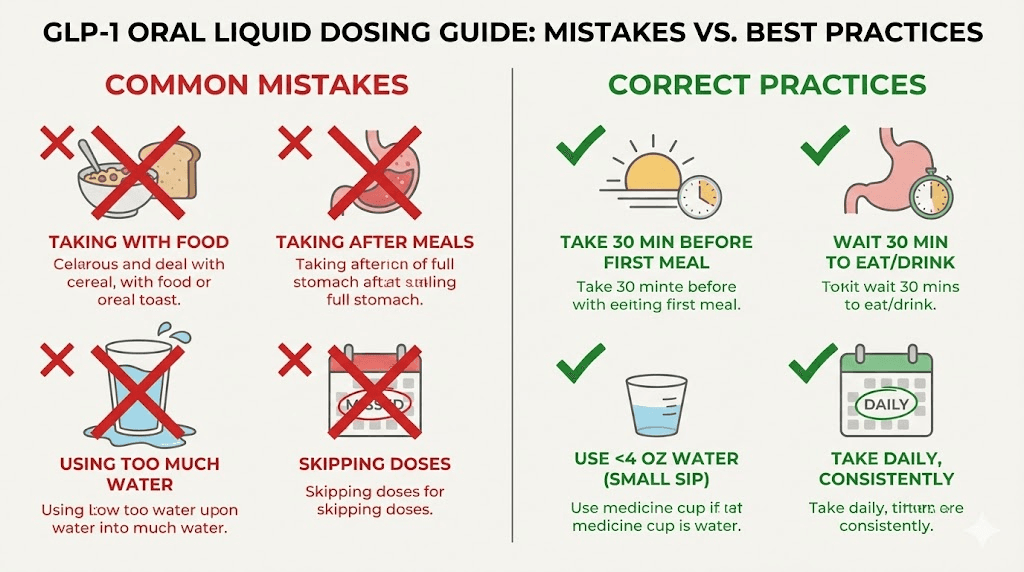
Rybelsus is taken once daily, every single day, at the same time. The manufacturer is explicit about this. You take one tablet in the morning, at least 30 minutes before your first food, beverage, or other oral medication. You swallow it with no more than 4 ounces of plain water. Not coffee. Not juice. Not sparkling water. Plain water only.
Why the strict rules? Because oral semaglutide has a bioavailability of roughly 0.4% to 1%. That means your body absorbs less than 1% of what you swallow. Food reduces that number even further, potentially cutting absorption by more than 50%. The SNAC absorption enhancer in each tablet needs an empty stomach to work properly. If you eat too soon or drink too much liquid, the protective mechanism fails and you waste your dose.
The best time of day to take semaglutide is first thing in the morning for most people. This gives the medication a clear window on an empty stomach and allows the 30-minute waiting period to pass before breakfast. Some people set an alarm 30 minutes before their usual wake time, take the tablet, then go back to sleep until their normal alarm. Creative. Effective.
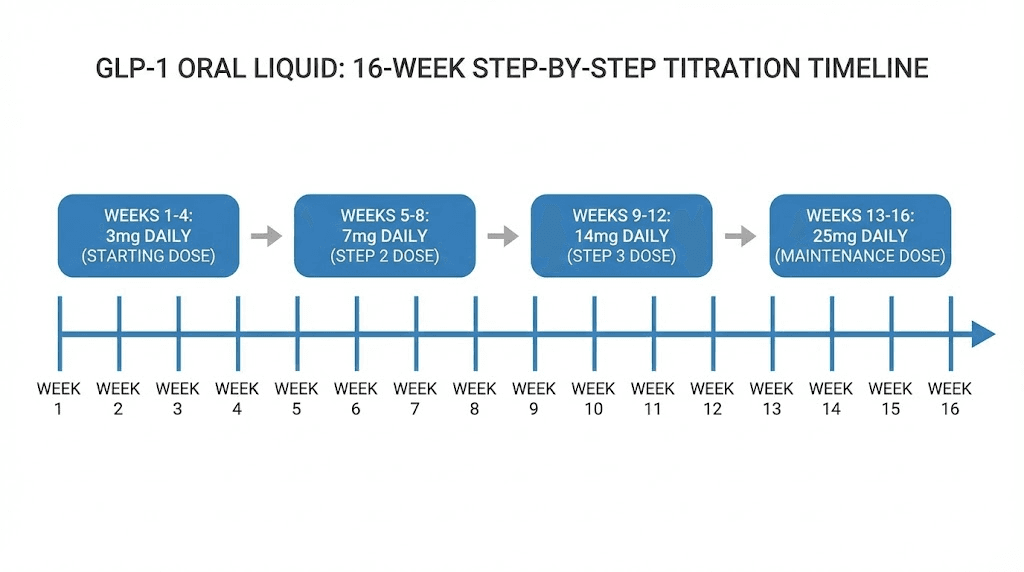
The semaglutide dosage for Rybelsus follows a specific titration. You start at 3 mg daily for 30 days. Then you increase to 7 mg daily. If needed and tolerated, you can go up to 14 mg daily. Each step lasts at least 30 days. Rushing the titration leads to worse nausea and higher dropout rates.
Wegovy pill dosing frequency
The Wegovy oral formulation follows the same once-daily rule. The difference is the dose range. Wegovy pills start at 1.5 mg once daily for 30 days, then escalate in monthly steps. The target maintenance dose can reach up to 25 mg once daily, which is significantly higher than Rybelsus because the pill formulation was designed specifically for the weight management indication.
Same empty-stomach rules apply. Same 30-minute waiting period. Same plain-water-only requirement. Understanding how long it takes for semaglutide to suppress appetite helps set realistic expectations during the early titration phase when you are still on lower doses.
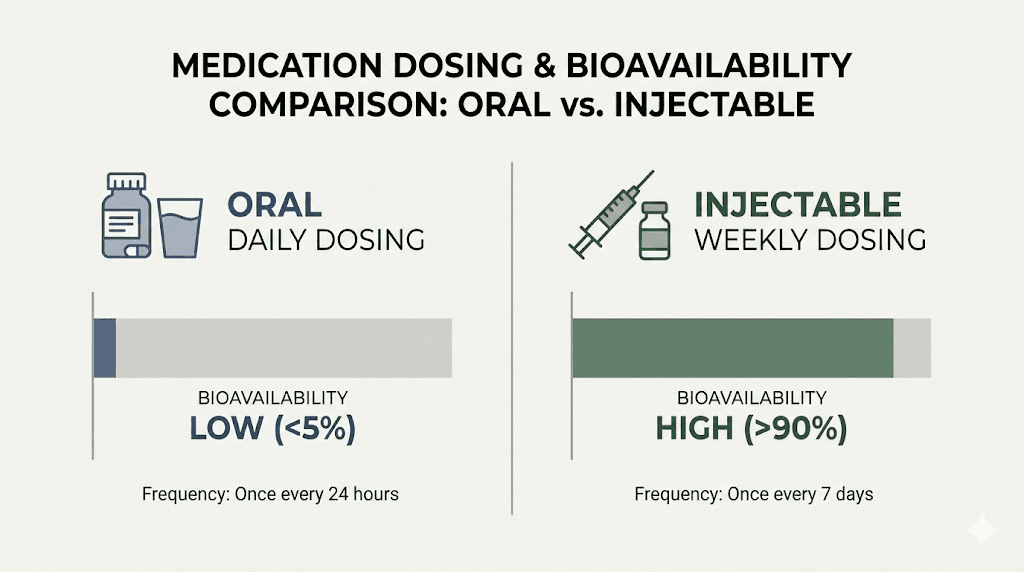
Why daily dosing matters for oral formulations
Injectable semaglutide (Ozempic, Wegovy injection) is dosed once weekly. So why is oral semaglutide daily? It comes down to pharmacokinetics. The injectable form delivers semaglutide directly into subcutaneous tissue, where it absorbs slowly and maintains steady blood levels for seven days. The oral form, with its extremely low bioavailability, cannot achieve the same sustained release. Daily dosing compensates by providing frequent small amounts that accumulate to therapeutic levels over time.
It takes approximately 4 to 5 weeks of consistent daily dosing to reach steady-state blood levels. This is why semaglutide does not work instantly. You need that accumulation period. Missing days during the first month is especially damaging because you never build up to the concentration needed for meaningful appetite suppression and metabolic effects. The full timeline for semaglutide results typically spans 8 to 12 weeks before significant changes become visible.
Compounded sublingual GLP-1 drops dosing frequency
This is the section most people are actually searching for. Compounded sublingual drops have become increasingly popular as an alternative to injections. The dosing frequency depends on your specific prescription, but standard protocols follow predictable patterns.
Standard daily dosing protocol
Most compounding pharmacies and prescribing providers recommend once-daily dosing for sublingual GLP-1 drops. You measure your prescribed dose using the oral syringe provided, place the liquid under your tongue, hold it there for 1 to 2 minutes minimum (some providers recommend up to 5 minutes), then swish and swallow.
The daily protocol works because sublingual absorption, while better than swallowing a tablet through the stomach, still has significant variability. Daily dosing creates the most consistent blood levels. The complete sublingual semaglutide guide covers the specific steps for proper administration in detail.
Here is what a typical daily protocol looks like:
Month 1: 0.25 mL once daily (equivalent to the lowest starting dose)
Month 2: 0.5 mL once daily (intermediate dose)
Month 3+: 0.75 mL to 1.0 mL once daily (maintenance dose)
The exact volumes depend on the concentration your pharmacy uses. Compounding pharmacies label drops by concentration (strength per mL) and volume, not always by milligrams. Your provider should specify both the volume to measure and the corresponding milligram dose. Using a semaglutide dosage calculator can help verify your measurements are correct.
Three times weekly protocol
Some providers transition patients to three times per week dosing once they reach steady state, which typically occurs around weeks 5 to 6. This reduced frequency can work for patients who have achieved their target blood levels and want less frequent administration.
Three things must be true before switching to this reduced frequency. First, you must have completed at least 5 to 6 weeks of daily dosing. Second, you must be seeing therapeutic effects like appetite suppression and weight changes. Third, your provider must specifically approve the transition. Do not reduce frequency on your own.
The logic behind three times weekly dosing relates to semaglutide half-life. Once blood levels reach steady state through daily dosing, the long half-life of semaglutide (approximately 7 days) means levels do not drop dramatically between doses. However, research on this specific protocol for sublingual formulations remains limited compared to injectable data.
Tirzepatide sublingual drops frequency
Tirzepatide drops follow a similar once-daily protocol during the initial phases. Because tirzepatide is a dual GIP/GLP-1 receptor agonist, its pharmacokinetic profile differs slightly from pure GLP-1 agonists. The tirzepatide oral vs injection comparison shows meaningful differences in absorption patterns.
For compounded tirzepatide sublingual liquid, the starting frequency is once daily. The compounded tirzepatide dosage calculator can help determine proper volumes based on your prescribed concentration. The tirzepatide sublingual dosage chart provides visual reference for titration steps.
The complete titration schedule for oral GLP-1 liquid
Titration is the process of gradually increasing your dose over time. Every GLP-1 oral liquid formulation requires titration. Nobody starts at the full dose. Rushing it leads to severe gastrointestinal side effects that make people quit before the medication has a chance to work.
Week-by-week titration for sublingual semaglutide drops
The following schedule represents a common compounded sublingual semaglutide titration. Your provider may adjust this based on your tolerance, weight, and treatment goals. Always follow your specific prescription over any general guide.
Weeks 1 through 4 (initiation phase): Starting dose once daily. This is the lowest available concentration. The goal is not weight loss yet. The goal is getting your body accustomed to the medication. Expect minimal appetite changes. Some people feel slight nausea. Others feel nothing at all. Both responses are normal. The question of whether semaglutide suppresses appetite immediately is one that many people ask during this phase, and the answer is usually no.
Weeks 5 through 8 (first escalation): Dose increases to the next level, still once daily. This is when most people first notice appetite changes. Portions shrink naturally. Cravings fade. Some experience semaglutide burping or mild nausea during the first few days after the increase. These side effects typically resolve within 3 to 5 days.
Weeks 9 through 12 (second escalation): Another dose increase, still once daily. Weight loss usually becomes measurable at this stage. The one-month results on semaglutide vary widely, but by week 12 most people have established a clear downward trend on the scale. If you are not seeing results by this point, it is time to evaluate your protocol with your provider. Understanding why you might not be losing weight on semaglutide can help identify what needs adjustment.
Weeks 13 through 16 (maintenance evaluation): If the current dose is producing results, you stay here. If not, another escalation may be appropriate. Some patients reach their optimal dose at the second level. Others need the third or fourth tier. There is no single correct maintenance dose. The right dose is the one that produces consistent results with tolerable side effects.
Titration for compounded tirzepatide drops
Tirzepatide titration follows a similar gradual approach. The tirzepatide dosage breakdown shows how units translate to milligrams at each level. For sublingual drops specifically, concentrations vary by pharmacy, so volume measurements will differ.
A standard compounded tirzepatide titration might look like:
Month 1: 2.5 mg equivalent once daily
Month 2: 5 mg equivalent once daily
Month 3: 7.5 mg equivalent once daily
Month 4+: 10 mg or higher as prescribed
The tirzepatide dosing for weight loss follows established clinical trial protocols adapted for the sublingual route. Remember that sublingual bioavailability differs from injectable bioavailability, which is why your provider may prescribe different absolute doses than what you see in injection dosing charts.
Why you should never skip titration steps
The temptation to jump to higher doses is real. Especially when the first few weeks produce no noticeable effects. Resist this urge completely.
Skipping titration steps increases the risk of severe nausea, vomiting, diarrhea, and constipation. These are the side effects that cause people to abandon treatment entirely. Studies on injectable semaglutide show that faster titration leads to significantly higher rates of treatment discontinuation. The same principle applies to oral and sublingual formulations.
Your GI tract needs time to adjust. GLP-1 receptor agonists slow gastric emptying, meaning food stays in your stomach longer. When you escalate too fast, the slowing effect becomes so pronounced that it causes significant discomfort. Gradual increases let your body adapt incrementally. The constipation treatment strategies for tirzepatide work much better when titration is done properly from the start.
Best time of day to take GLP-1 oral liquid
Morning. For the vast majority of people, morning dosing produces the best results with the fewest complications. But the specifics depend on your formulation type.
Morning dosing for tablets (Rybelsus, Wegovy pill)
FDA-approved oral semaglutide tablets must be taken on an empty stomach. This essentially forces morning dosing for most people. The optimal timing for semaglutide is immediately upon waking, before anything else enters your mouth. Set the tablet and a small glass of water on your nightstand. Wake up, take it, start your morning routine, eat breakfast 30 minutes later.
Why morning specifically? Three reasons. First, you have the longest natural fasting period overnight, guaranteeing an empty stomach. Second, the appetite-suppressing effects kick in during the day when you need them most for managing food choices. Third, taking it at a consistent time each day is easiest when you anchor it to your wake-up routine.
Morning dosing for sublingual drops
Sublingual drops do not have the same strict empty-stomach requirement as tablets because the medication absorbs through oral mucous membranes rather than through the stomach lining. However, most providers still recommend morning dosing, ideally 30 minutes before eating.
The reason relates to oral cavity preparation. When you first wake up, your mouth has had hours without food, drink, or brushing. The mucous membranes are relatively clean and receptive. Some providers recommend a specific preparation protocol: floss, brush your teeth gently, then rinse with warm water before applying the drops. This clears debris from the sublingual area and may improve absorption. After placing the drops, wait at least 30 minutes before eating, drinking, or brushing your teeth.
If morning dosing does not work with your schedule, evening dosing is an acceptable alternative. The critical factor is consistency. Taking your drops at the same time every day is more important than which specific time you choose. The best time to take GLP-1 is ultimately the time you can maintain consistently.
Evening dosing considerations
Some people prefer evening dosing because morning nausea is a common side effect during the first weeks. Taking the dose before bed means you sleep through the worst of the nausea. Others find that evening dosing helps control nighttime snacking, which is a significant calorie source for many people.
The downside of evening dosing for sublingual drops is that you have likely eaten and consumed beverages throughout the day. Residue in your mouth may affect absorption. If you choose evening dosing, wait at least 2 hours after your last meal and rinse your mouth with water before administering the drops.
How to take GLP-1 oral liquid for maximum absorption
The difference between mediocre and excellent results often comes down to absorption technique. Two people can take the exact same dose of the exact same product and get wildly different blood levels based purely on how they administer it.
Sublingual drop administration technique
Step one is measuring accurately. Use the oral syringe provided by your pharmacy. Do not estimate. Do not use kitchen spoons. Do not use different measuring devices. Precision matters when you are working with formulations where small volume changes equal significant dose changes.
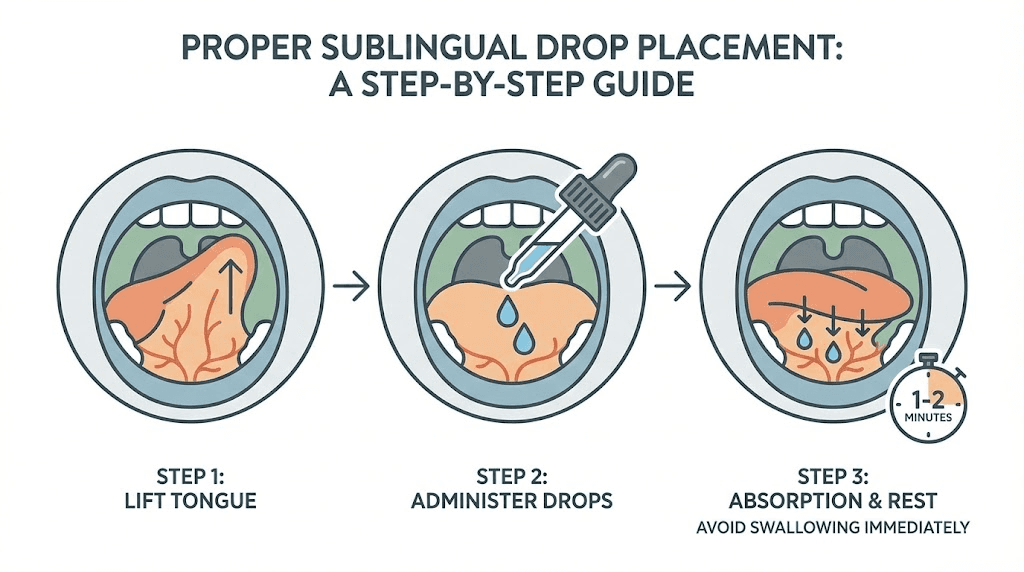
Step two is placement. Lift your tongue. Place the drops directly into the sublingual pocket, the area under the tongue where you can see veins. This area has thin tissue and rich blood supply. The medication enters your bloodstream through these membranes directly, bypassing the digestive system entirely.
Step three is patience. Hold the liquid under your tongue for at least 2 minutes. Five minutes is better. Some providers recommend keeping it in your mouth as long as possible. Do not talk. Do not swallow. Let the medication sit and absorb. You will feel the liquid under your tongue. That is normal. After your hold time is complete, swish the remaining liquid around your mouth before swallowing. The inside of your cheeks also have permeable mucous membranes that can absorb the medication.
Step four is the waiting period. After swallowing, wait at least 30 minutes before eating or drinking anything. This gives any medication still coating your oral tissues time to absorb fully. If you can still taste the flavor (many compounded drops have a spearmint or peppermint taste), there is still active medication in your mouth being absorbed. Wait until the flavor is completely gone.
Factors that reduce absorption
Several common mistakes can dramatically reduce how much medication actually reaches your bloodstream. Eating or drinking too soon after dosing is the most common one. Food particles and liquids wash away the medication before it can absorb. Even water can dilute the concentration against your mucous membranes.
Brushing your teeth immediately before or after dosing is another mistake. Brushing creates micro-abrasions in your gums and oral tissue. While some providers recommend brushing before dosing to prepare the mucosa, aggressive brushing can actually cause bleeding or irritation that changes absorption patterns. If you brush before dosing, do it gently and wait a few minutes for any irritation to settle.
Smoking, using mouthwash with alcohol, or consuming hot beverages shortly before dosing can all affect the oral mucosa. Alcohol-based mouthwash dries out the tissues. Hot liquids can cause temporary inflammation. Smoking reduces blood flow to oral tissues. All of these factors decrease absorption efficiency.
The injectable vs oral peptides comparison explains why bioavailability matters so much. Injectable semaglutide achieves roughly 89% bioavailability. Oral tablet semaglutide achieves about 0.4% to 1%. Sublingual delivery falls somewhere between these extremes. Recent animal studies suggest sublingual semaglutide may achieve significantly higher bioavailability than oral tablet forms, but human data remains limited.
What happens when you miss a dose
You will miss a dose eventually. Life happens. Travel, busy mornings, forgetfulness. The key is knowing exactly what to do when it happens so you do not make the situation worse.
Missed daily dose protocol
For daily oral GLP-1 formulations, both tablets and sublingual drops, the rule is simple. Skip the missed dose. Take your next dose at the normal scheduled time the following day. Do not double up. Do not take an extra dose later in the day. Do not try to "make up" for the missed dose.
Doubling your dose will not speed up results. What it will do is spike your blood levels temporarily, causing a surge of side effects like nausea, vomiting, and severe gastrointestinal discomfort. The dizziness some people experience on semaglutide can become severe with accidental double dosing.
Multiple missed days
Missing one day is no big deal. The long half-life of semaglutide means blood levels barely drop from a single missed dose once you have reached steady state. But what about multiple consecutive days?
If you miss 2 to 3 days, resume your normal daily dose. You may notice reduced appetite suppression during the gap, but blood levels will rebuild quickly once you resume. If you miss more than a week, contact your provider. Extended gaps in dosing may require restarting the titration process, especially if you experience side effects when you resume. The semaglutide withdrawal symptoms some people report are actually the return of normal appetite signals after the medication wears off.
For gaps of two weeks or more, many providers recommend restarting from the initial dose and titrating up again. This is not because the medication becomes dangerous at your previous dose. It is because your body has lost its adaptation to the GI-slowing effects, and jumping back to a full dose will likely cause the same nausea you experienced at the start.
Setting up reminders
The best missed-dose strategy is preventing missed doses in the first place. Phone alarms work. Pill organizer systems work. Habit stacking, where you attach the dose to an existing daily habit like making coffee, works particularly well. The GLP-1 companion tools available can help track your dosing consistency over time.
Daily dosing vs three times weekly dosing
The question of whether you can reduce from daily to three times per week comes up frequently with sublingual GLP-1 drops. Some providers offer this option. Others do not. Understanding the science helps you make an informed decision with your prescriber.
The case for daily dosing
Daily dosing provides the most consistent blood levels. Each day you add a small amount to the circulating semaglutide in your system. Over time, this creates a steady concentration that keeps appetite suppression constant. There are no "off days" where the medication effect diminishes. For people in active weight loss phases, daily dosing maximizes the therapeutic benefit.
Daily dosing also makes it easier to remember. Same time, same routine, every day. There is no confusion about which days are dose days. The typical treatment duration for semaglutide spans months or even years, so building a sustainable daily habit matters for long-term adherence.
The case for three times weekly dosing
Once you reach steady state (typically after 5 to 6 weeks of daily dosing), blood levels of semaglutide remain relatively stable even with less frequent dosing. The medication half-life of approximately 7 days means it takes a full week for blood levels to drop by half after stopping completely. Three doses per week can theoretically maintain adequate levels.
Reduced frequency may also reduce side effects for some people. Less frequent dosing means less frequent GI stimulation, which can help with constipation, nausea, and bloating that some patients experience throughout treatment. It also costs less if you are paying out of pocket, since each bottle lasts longer.
However, the evidence base for three times weekly sublingual dosing is thin compared to the robust clinical trial data supporting daily oral and weekly injectable protocols. This is an area where the practice has outpaced the research. Discuss the tradeoffs honestly with your provider.
Which frequency is right for you
If you are in the first 3 months of treatment, stick with daily dosing. Do not reduce frequency until you have established steady-state blood levels and confirmed the medication is working.
If you are past the initial phase, have reached your target weight or a stable maintenance phase, and want to reduce frequency, discuss it with your provider. They may recommend a trial period where you switch to three times weekly while monitoring your weight and appetite patterns. If weight starts creeping back up or appetite suppression weakens, return to daily dosing.
The semaglutide plateau phenomenon affects some patients regardless of dosing frequency. If you hit a plateau on three times weekly dosing, returning to daily dosing is a reasonable first step before escalating the dose.
Adjusting your frequency over time
GLP-1 treatment is not static. What works in month one may not be optimal in month six. Understanding when and how to adjust frequency helps you get the most from long-term treatment.
During active weight loss
During the active weight loss phase, daily dosing at your prescribed level is standard. Do not reduce frequency while you are actively trying to lose weight. The goal is maximum consistent therapeutic effect. Tirzepatide typically takes several weeks to show full effects, and semaglutide follows a similar timeline. Patience combined with consistent daily dosing produces the best outcomes.
The first four weeks often produce minimal weight loss. This is normal. The medication is building to therapeutic levels in your blood. Real results start appearing in months 2 through 4 for most people. The before and after results on tirzepatide and before and after results on semaglutide both show this delayed onset followed by accelerating progress.
During weight maintenance
Once you reach your target weight, the question of maintenance dosing becomes critical. Some providers reduce the dose while maintaining daily frequency. Others maintain the dose but reduce frequency. And some keep everything the same.
Research suggests that stopping GLP-1 medications entirely leads to weight regain in the majority of patients. The withdrawal pattern typically involves gradual return of appetite over 2 to 4 weeks, followed by weight regain over the subsequent months. Maintaining some level of medication, even at reduced frequency, may help prevent this rebound.
When to discuss changes with your provider
Contact your provider about dosing frequency if any of these apply:
You have been on the same dose and frequency for 3+ months with no weight change
Side effects are persistent and significantly affecting quality of life
You want to transition from daily to less frequent dosing
You have reached your weight loss goal and want to discuss maintenance
You are switching between different GLP-1 formulations
The process of switching between GLP-1 medications involves careful dose conversion and may require restarting titration. The semaglutide to tirzepatide conversion chart provides guidance on equivalent doses across different medications.
Oral GLP-1 liquid vs injectable GLP-1 medications
Understanding how oral liquid GLP-1 compares to injectable forms helps explain why dosing frequencies differ and helps you evaluate which option fits your lifestyle best.
Dosing frequency comparison
The frequency differences are dramatic:
Oral semaglutide tablets: Once daily
Sublingual semaglutide drops: Once daily (potentially three times weekly at maintenance)
Injectable semaglutide (Ozempic/Wegovy): Once weekly
Injectable tirzepatide (Mounjaro/Zepbound): Once weekly
Injectable liraglutide (Saxenda): Once daily
The semaglutide vs tirzepatide comparison covers effectiveness differences between these two primary GLP-1 medications regardless of delivery method. The side effect profiles also differ between oral and injectable forms.
Bioavailability and why it matters for frequency
Injectable semaglutide achieves approximately 89% bioavailability. Almost everything you inject gets into your bloodstream. This is why a single weekly injection of 0.5 mg to 2.4 mg maintains therapeutic levels for a full seven days.
Oral semaglutide tablets achieve roughly 0.4% to 1% bioavailability. For every 14 mg tablet you swallow, your body absorbs approximately 0.06 mg to 0.14 mg. This is why you need to take it daily, because each individual dose delivers so little medication that frequent dosing is necessary to maintain adequate blood levels.
Sublingual drops fall between these two extremes. Animal studies suggest sublingual bioavailability may be significantly higher than oral tablet bioavailability. One rat study found sublingual semaglutide achieved a 5-fold higher blood concentration compared to oral administration at the same dose. Human data is still limited, but the improved bioavailability helps explain why some patients can eventually reduce to three times weekly dosing.
Convenience trade-offs
Weekly injections are the most convenient from a frequency standpoint. Once per week, done. But many people dislike needles, which is where oral options become attractive. The GLP-1 injection guide and best injection sites for GLP-1 can help make injections less intimidating for those considering the switch, but the reality is that some people will always prefer an oral option regardless of convenience differences.
Daily sublingual drops add about 5 minutes to your morning routine. That is the hold time plus waiting before eating. For many people, this is a small price to pay for avoiding needles entirely. The oral vs injection comparison for tirzepatide breaks down these trade-offs in more detail.
Side effects and how dosing frequency affects them
The frequency at which you take GLP-1 oral liquid directly influences which side effects you experience and how severe they are. Understanding this relationship gives you more control over your treatment comfort.
Common side effects with daily oral dosing
Nausea is the most reported side effect. It affects roughly 15% to 20% of people on oral semaglutide. With sublingual drops, the nausea rate may differ because the medication enters the bloodstream through a different pathway. Nausea typically peaks during the first week of a new dose and fades over the following 7 to 10 days. If fatigue accompanies your semaglutide use, it usually follows the same pattern, peaking early and resolving as your body adjusts.
Constipation is the second most common issue. GLP-1 receptor agonists slow gastric motility, which means food moves through your digestive tract more slowly. Daily dosing means continuous slowing effect. The semaglutide constipation treatment guide covers effective management strategies including fiber supplementation, hydration, and when to consider medication adjustments.
Headaches occur in about 10% to 15% of users, most commonly during the first two weeks. Insomnia is less common but does affect some people, particularly with evening dosing. GLP-1 fatigue can persist longer than other side effects for some individuals.
How titration speed affects side effects
Faster titration equals worse side effects. Period.
Clinical trials consistently show that patients who escalate doses more slowly report milder and shorter-duration side effects. The standard 4-week intervals between dose increases exist specifically to minimize GI disruption. Providers who push faster titration may get patients to therapeutic doses sooner, but they also lose more patients to intolerable side effects.
If you experience significant nausea or other GI problems at a new dose, you have two options. First, stay at the current dose for an additional 2 to 4 weeks before attempting to increase again. Second, drop back to the previous dose for 1 to 2 weeks, then re-attempt the increase. Both approaches are preferable to pushing through severe symptoms.
Managing side effects without changing frequency
Before reducing dosing frequency to manage side effects, try these adjustments first:
For nausea: Eat smaller meals more frequently throughout the day. Avoid fatty, greasy, or heavily seasoned foods. Ginger tea or ginger supplements can help. The recommended foods while on semaglutide and foods to avoid on tirzepatide provide specific dietary guidance.
For constipation: Increase water intake to 80+ ounces daily. Add 25 to 30 grams of fiber per day. Magnesium citrate supplements can help. Regular physical activity stimulates bowel motility. The tirzepatide constipation strategies apply equally to semaglutide users.
For fatigue: Ensure adequate protein intake (0.7 to 1.0 grams per pound of body weight daily). Low protein intake on GLP-1 medications causes muscle loss, which worsens fatigue. Protein shakes designed for GLP-1 users can help meet targets when appetite is suppressed. The relationship between semaglutide and energy levels often improves once nutrition is optimized.
A thoughtful diet plan while on semaglutide or tirzepatide diet plan makes a substantial difference in side effect management. The specific foods that work best on tirzepatide tend to be high-protein, moderate-fiber options that digest easily.
Supplements that pair well with tirzepatide include B12, magnesium, and fiber. For those on semaglutide formulations containing added vitamins, the semaglutide with B12 combination and semaglutide with glycine offer potential advantages. Similarly, tirzepatide glycine combinations and tirzepatide with B12 are popular compounded options.
Storage and handling for GLP-1 oral liquid
Proper storage directly affects potency. Take your medication at the perfect frequency with flawless technique, but store it wrong and you are dosing yourself with degraded product that will not deliver full results.
Sublingual drop storage requirements
Most compounded sublingual GLP-1 drops require refrigeration. Store them in the refrigerator at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). Do not freeze them. Freezing permanently damages the peptide structure and renders the medication ineffective. The refrigeration requirements for compounded semaglutide are strict for a reason.
Once opened, most compounded sublingual formulations remain stable for 28 to 90 days in the refrigerator, depending on the pharmacy and formulation. Check your specific prescription label for the exact beyond-use date. The shelf life of compounded semaglutide in the fridge varies by formulation and concentration.
For tablet formulations like Rybelsus, storage is simpler. Room temperature, 68 to 77 degrees Fahrenheit (20 to 25 degrees Celsius), in the original bottle. Keep it away from moisture and humidity. Do not transfer tablets to a pill organizer, as moisture exposure degrades the SNAC protective coating.
Travel considerations
Traveling with GLP-1 oral liquid requires planning. If your drops need refrigeration, you need a travel cooler or insulated bag with ice packs. The semaglutide travel guide covers everything from TSA regulations to keeping your medication at proper temperature during flights and hotel stays.
Short periods outside refrigeration (a few hours) are generally acceptable, but extended exposure to heat degrades the medication. The consequences of semaglutide getting warm include reduced potency and potentially altered side effect profiles. Do not leave your medication in a hot car, near a window with direct sunlight, or in checked luggage during air travel (cargo holds can reach extreme temperatures).
Understanding how long semaglutide remains good under various conditions helps you make informed decisions about whether a dose is still viable after temperature excursions. When in doubt, contact your pharmacy. The question of whether you can use expired semaglutide comes up frequently, and the answer is generally no, you should not risk it.
Common mistakes that reduce GLP-1 oral liquid effectiveness
Knowing the right dosing frequency is only half the battle. Avoiding the mistakes that undermine your protocol is equally important. These are the errors that SeekPeptides sees researchers ask about most frequently.
Mistake 1: inconsistent timing
Taking your dose at 7 AM one day, noon the next, and 10 PM the day after creates blood level fluctuations that reduce effectiveness and worsen side effects. Pick a time. Stick to it. Consistency within a 1-hour window each day is the target. Your body establishes metabolic rhythms around consistent medication timing, and disrupting those rhythms undermines the steady-state blood levels you worked weeks to build.
Mistake 2: eating or drinking too soon
The 30-minute fasting window after dosing exists for a reason. For tablets, food reduces absorption by more than 50%. For sublingual drops, eating or drinking washes medication off the mucosal surfaces before absorption is complete. Some people think "close enough" is fine. It is not. Set a timer. Wait the full 30 minutes. Every time.
Mistake 3: not holding sublingual drops long enough
The minimum hold time is 2 minutes. Many people rush this. They place the drops, hold for 30 seconds, and swallow. This drastically reduces sublingual absorption and forces most of the medication through the GI tract, where bioavailability plummets. Think of the hold time as the most important 2 to 5 minutes of your entire dosing routine. If you can hold longer, do it.
Mistake 4: storing medication improperly
Leaving compounded drops on the counter instead of in the fridge. Freezing them accidentally. Exposing them to direct sunlight. All of these degrade the active ingredient. You might be taking the right dose at the right frequency but getting subtherapeutic blood levels because half the semaglutide or tirzepatide has degraded. The peptide storage guide covers best practices for maintaining potency.
Mistake 5: self-adjusting frequency without provider guidance
Reducing from daily to every other day because you "feel fine" or increasing to twice daily because you want faster results. Both are problematic. GLP-1 dosing is calibrated carefully. The dose and frequency work together as a system. Changing one without professional guidance can lead to either subtherapeutic levels (wasting medication and money) or supratherapeutic levels (unnecessary side effects and potential complications).
Mistake 6: giving up during the first month
Many people expect immediate results. When the first 2 to 4 weeks produce minimal changes, they assume the medication is not working and stop. But the first month is the building phase. Blood levels are accumulating. Your body is adjusting. Results typically start between weeks 4 and 8. The timeline for GLP-1 to start working is longer than most people expect. Staying consistent with daily dosing through this period is essential.
Microdosing GLP-1 oral liquid
Microdosing GLP-1 has gained attention as an approach for people who want the metabolic benefits at lower side effect levels. The microdosing tirzepatide chart shows how small doses compare to standard protocols.
What microdosing means for oral GLP-1
Microdosing typically involves taking a dose below the standard starting level, often daily, to achieve subtle appetite modulation without the gastrointestinal side effects that come with standard dosing. For sublingual semaglutide drops, this might mean taking half the standard starting dose once daily.
The frequency for microdosing is still daily in most protocols. The reduced dose, not the reduced frequency, is what defines microdosing. Some practitioners have explored microdosing GLP-1 for autoimmune conditions, where the anti-inflammatory properties of GLP-1 receptor activation are the primary goal rather than weight loss.
Who microdosing may benefit
People who experience intolerable side effects even at the lowest standard dose may benefit from starting even lower. Those who are sensitive to medications in general often do better with a microdose approach. And individuals using GLP-1 for reasons beyond weight loss, such as metabolic health optimization or inflammatory conditions, may not need full therapeutic doses.
The microdose tirzepatide schedule provides a framework for how these lower-dose protocols progress over time. The general peptide dosing guide from SeekPeptides covers principles that apply across all peptide medications including GLP-1 formulations.
Special populations and frequency considerations
Not everyone follows the standard dosing frequency. Certain populations require modified approaches based on their specific circumstances.
People on thyroid medications
If you take levothyroxine (Synthroid, Levoxyl) or other thyroid medications, timing becomes complicated. Both oral semaglutide and thyroid medications need to be taken on an empty stomach. The standard recommendation is to take your thyroid medication first, wait at least 30 to 60 minutes, then take your GLP-1 oral liquid, then wait another 30 minutes before eating.
For sublingual GLP-1 drops, the interaction may be less of a concern since the medication absorbs through the mouth rather than the stomach. However, discuss this specific scenario with your provider to establish a timing protocol that works for both medications.
People with gastroparesis
GLP-1 medications slow gastric emptying. People who already have slow gastric emptying (gastroparesis) need extra caution. The frequency may remain daily, but the dose titration often proceeds much more slowly, with longer intervals between increases. Some providers extend titration intervals to 6 to 8 weeks per dose level instead of the standard 4 weeks.
People taking other medications
GLP-1 oral liquid, particularly tablets that pass through the stomach, can affect the absorption of other oral medications. The slowed gastric emptying means other pills may take longer to reach the small intestine where they absorb. This is particularly relevant for medications with narrow therapeutic windows like blood thinners, seizure medications, and certain antibiotics.
People who combine GLP-1 medications with other weight management compounds should be especially careful about frequency and timing. The question of combining phentermine with semaglutide and the phentermine vs semaglutide comparison address these interaction concerns directly. Understanding whether you can drink alcohol on semaglutide is another common frequency-adjacent question, since alcohol timing relative to doses matters.
Pregnancy and breastfeeding
GLP-1 medications should be discontinued before pregnancy. The frequency question becomes "zero doses" once pregnancy is planned or confirmed. The GLP-1 and breastfeeding guide covers the nuances of this topic, but the general recommendation is to stop GLP-1 treatment at least 2 months before attempting conception due to the long half-life.
Comparing oral GLP-1 frequency with newer formulations
The GLP-1 landscape is evolving rapidly. New formulations and delivery methods are changing the frequency conversation.
GLP-1 patches
The Onmorlo GLP-1 patch system represents a completely different approach to dosing frequency. Transdermal patches deliver medication continuously through the skin, potentially eliminating the need for daily oral dosing entirely. While still emerging, this technology could eventually offer weekly or even less frequent application schedules.
Next-generation oral GLP-1 medications
Orforglipron is a non-peptide oral GLP-1 receptor agonist in late-stage clinical trials. Unlike semaglutide tablets that require the SNAC enhancer, orforglipron has much higher oral bioavailability as a small molecule. The orforglipron vs tirzepatide comparison discusses how this new medication may change the oral GLP-1 landscape. Current trial protocols use once-daily dosing, but the improved bioavailability could theoretically support less frequent administration in the future.
Combination therapies
Newer combination treatments like CagriSema (cagrilintide plus semaglutide) are being studied as weekly injections. The cagrilintide and semaglutide combination shows enhanced weight loss compared to either drug alone. As these combinations move toward approval, oral formulations may follow. The amylin receptor agonist class, which includes cagrilintide, adds a second mechanism of action that strengthens the weight loss effect.
The GLP-3 peptide research and triple-agonist medications like retatrutide point to a future where multiple receptor targets are activated simultaneously. How these next-generation treatments will be formulated for oral delivery, and what dosing frequencies they will require, remains an active area of research. The mazdutide comparison shows another dual-agonist approaching the market.
Tracking your dosing and results
Consistent dosing frequency only matters if you can verify it is actually working. Tracking both adherence and outcomes gives you data to optimize your protocol.
What to track daily
At minimum, record your daily dose time, dose amount, and any side effects. Many people use a simple spreadsheet or a medication tracking app. The GLP-1 plotter tool can help visualize your dosing patterns over time.
Recording what you eat and your hunger levels throughout the day provides valuable data for your provider appointments. If your daily dosing is not producing adequate appetite suppression, this food diary becomes the evidence that supports a dose increase. Conversely, if you are experiencing severe appetite loss and eating too little, the diary helps identify that problem early.
Weekly measurements
Weigh yourself once per week, same day, same time, same conditions (morning, after using the bathroom, before eating). Daily weight fluctuates too much to be useful. Weekly trends reveal the true trajectory. The tirzepatide weight loss timeline shows typical weekly patterns you can compare against your own data.
Monthly check-ins
Every 4 weeks, assess whether your current frequency and dose are optimal. Are you losing weight at a reasonable rate (1 to 2 pounds per week is typical)? Are side effects manageable? Are you adhering to the daily schedule consistently? If any answer is no, discuss adjustments with your provider.
SeekPeptides members access comprehensive tracking tools, protocol databases, and community insights that help optimize GLP-1 treatment from the first dose through long-term maintenance. The combination of proper dosing frequency, careful tracking, and evidence-based adjustments produces the best outcomes.
Frequently asked questions
Can you take GLP-1 oral liquid twice a day?
No. Standard protocols for all GLP-1 oral liquid formulations call for once-daily dosing. Taking it twice daily without provider direction could cause excessive gastrointestinal side effects including severe nausea and vomiting. If your current daily dose is not effective, the solution is a dose increase at your next titration step, not doubling the frequency.
How long does it take for GLP-1 oral liquid to start working?
Most people notice initial appetite changes within 2 to 4 weeks of consistent daily dosing. Significant weight loss typically becomes measurable between weeks 8 and 12. The full timeline for GLP-1 to start working depends on your specific formulation, dose, and individual metabolism. Steady-state blood levels require approximately 5 to 6 weeks of daily dosing to establish.
What happens if you take GLP-1 oral liquid with food?
For tablets like Rybelsus, food reduces absorption by more than 50%, essentially wasting the dose. For sublingual drops, eating immediately after dosing washes medication off the oral mucosa before absorption is complete. Always wait at least 30 minutes after dosing before consuming any food or beverages. Following proper dietary guidelines while on semaglutide enhances overall results.
Can you switch from daily oral to weekly injectable GLP-1?
Yes, many patients transition from oral to injectable formulations. The switch requires your provider to calculate equivalent doses and may involve a brief titration period on the injectable form. The semaglutide dosage chart and tirzepatide dosage chart help visualize dose equivalencies across formulations.
Is daily oral dosing as effective as weekly injections?
Clinical studies show comparable effectiveness in blood sugar control and weight loss between daily oral and weekly injectable semaglutide when doses are optimized. However, some meta-analyses suggest injectable semaglutide may produce slightly greater weight loss overall. The oral vs injection effectiveness comparison covers the evidence for tirzepatide specifically.
Can you take GLP-1 oral liquid every other day?
Every other day dosing is not a standard recommended protocol. While the long half-life of semaglutide theoretically supports less frequent dosing, clinical data supports either daily oral or weekly injectable schedules. If cost is a factor driving interest in alternate-day dosing, discuss options with your provider rather than self-adjusting. The affordable tirzepatide options and cost-effective compounded tirzepatide may offer better alternatives than reducing frequency.
Do you need to take GLP-1 oral liquid on an empty stomach?
For tablets (Rybelsus), absolutely yes. Empty stomach with only plain water. For sublingual drops, an empty stomach is recommended but less critical since the medication absorbs through the mouth, not the stomach. However, an empty mouth is essential. No food residue, no beverages coating the mucosa. The cleaner your oral cavity, the better the sublingual absorption.
How long do you stay on GLP-1 oral liquid?
Treatment duration varies by individual goals and response. Many people take GLP-1 medications for 12 months or longer. Some transition to maintenance dosing indefinitely. The typical duration for semaglutide treatment depends on weight loss goals, maintenance needs, and ongoing medical supervision. Stopping abruptly often leads to weight regain, so work with your provider on a gradual plan if discontinuation is the goal.
External resources
For researchers serious about optimizing their GLP-1 protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, dosing tools, and a community of thousands who have navigated these exact dosing frequency questions.
In case I do not see you, good afternoon, good evening, and good night. May your doses stay consistent, your absorption stay optimal, and your results stay on track.