Feb 4, 2026

What if the needle is not the only option?
That question changes everything. For years, the peptide world revolved around one delivery method: subcutaneous injection. Syringes, alcohol swabs, vial reconstitution, the whole ritual. And it works. Nobody disputes that. But it also creates a barrier, one that keeps thousands of people from ever starting a peptide protocol in the first place. Fear of needles. Inconvenience during travel. The daily hassle of drawing up precise doses from a vial. These are real obstacles, and they push people away from compounds that could genuinely improve their health. The entire world of peptide applications becomes inaccessible to people who simply refuse to inject.
Sublingual peptides offer a different path.
Place a tablet, troche, or liquid drop under your tongue. Hold it there. Let the thin, blood-vessel-rich tissue beneath your tongue absorb the peptide directly into your bloodstream. No needles. No reconstitution. No refrigerated vials clinking around in your travel bag. The sublingual route bypasses the digestive system entirely, which means the peptide avoids the brutal gastrointestinal environment that destroys most oral peptides before they ever reach circulation. This is not some futuristic concept. Compounding pharmacies already produce sublingual formulations for peptides like sermorelin, BPC-157, PT-141, and dozens of bioregulator peptides from the Khavinson research lineage. The science supporting sublingual delivery has advanced dramatically, with novel formulations now achieving bioavailability levels that rival subcutaneous injection in certain peptide categories. Understanding which peptides absorb well sublingually, which do not, and how to optimize your technique can mean the difference between wasting product and getting genuine therapeutic benefit. That is exactly what this guide covers, from the molecular science of sublingual absorption to practical step-by-step protocols you can follow today. Whether you are a seasoned researcher exploring injection alternatives or someone just getting started with peptides, the information here will reshape how you think about peptide delivery.
What are sublingual peptides?
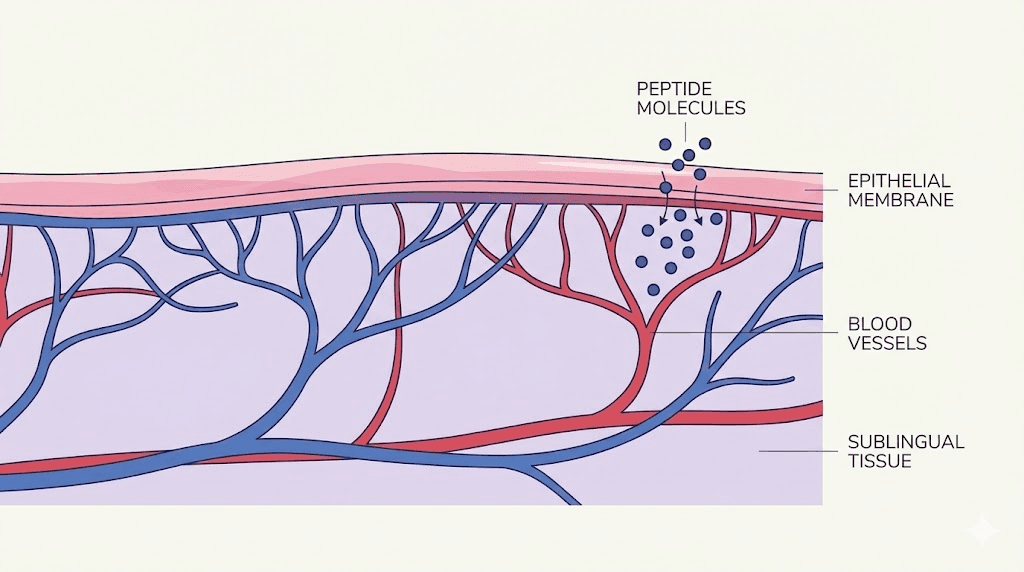
Sublingual peptides are peptide compounds designed to be absorbed through the mucous membrane under the tongue. The word "sublingual" comes from the Latin sub (under) and lingua (tongue). Rather than swallowing a capsule or injecting into subcutaneous tissue, you place the peptide formulation beneath your tongue and allow it to dissolve. The rich network of blood vessels in this region carries the peptide directly into systemic circulation.
This matters more than most people realize.
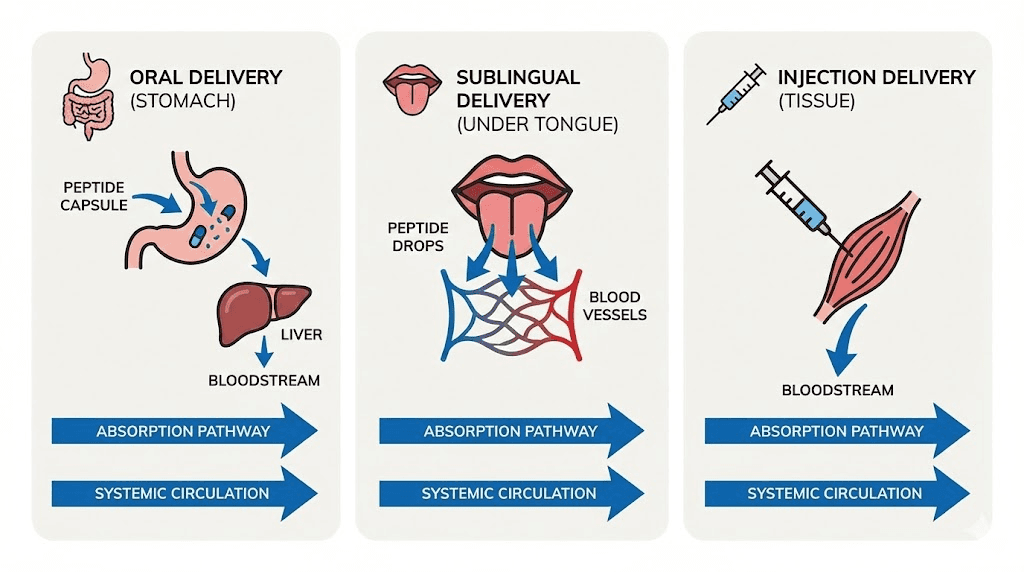
When you swallow a peptide in capsule form, it faces a gauntlet of destruction. Stomach acid with a pH between 1 and 3 attacks the peptide bonds. Proteolytic enzymes like pepsin, trypsin, and chymotrypsin break the amino acid chains into fragments. Whatever survives the stomach and small intestine then passes through the liver via first-pass metabolism, where additional enzymes further reduce what reaches your bloodstream. The result? Oral bioavailability for most peptides hovers around 1 to 2 percent. That means if you swallow a 500 mcg peptide capsule, roughly 5 to 10 mcg actually reaches circulation. The rest is destroyed. Understanding injectable versus oral peptides makes this contrast painfully clear, and the peptide formula guide explains how molecular structure influences this destruction.
Sublingual delivery sidesteps most of that destruction.
The anatomy of the sublingual region
The floor of the mouth contains some of the thinnest, most permeable tissue in the entire oral cavity. The sublingual epithelium measures just 100 to 200 micrometers thick, compared to 500 to 600 micrometers for the buccal mucosa lining the inner cheeks. This thinness is not a weakness. It is a feature. Thinner tissue means shorter diffusion distance for peptide molecules trying to reach the capillaries underneath.
Beneath that thin epithelium sits a dense network of blood vessels, including the sublingual artery and its branches. These capillaries connect to the sublingual vein, which drains into the internal jugular vein, feeding directly into systemic circulation. The peptide bypasses the portal vein entirely. It never touches the liver on its first pass. This is the key advantage, and it is why sublingual delivery can achieve bioavailability rates dramatically higher than oral swallowing.
The sublingual mucosa is also non-keratinized, unlike the hard palate or gums. Keratinized tissue has an extra protective layer that makes absorption more difficult. The non-keratinized sublingual membrane allows for easier passive diffusion of molecules, making it the preferred site for rapid-absorption drug delivery across many pharmaceutical applications, not just peptides. If you are exploring what peptides actually are and how they work in the body, understanding delivery routes is foundational knowledge.
How sublingual peptides differ from oral and injectable forms
Three delivery routes. Three completely different experiences. And three vastly different absorption profiles.
Oral peptides, whether in capsule or tablet form, must survive the entire gastrointestinal tract. Most do not. The few that do, like certain peptide capsules, rely on protective coatings, permeation enhancers, or the unusual gastric stability of specific peptides like BPC-157. Even then, systemic bioavailability rarely exceeds single-digit percentages for most compounds.
Injectable peptides, delivered subcutaneously or intramuscularly, bypass digestion entirely. They enter the bloodstream or local tissue directly. Bioavailability often approaches 100 percent for subcutaneous delivery, which is why injections remain the gold standard for peptide administration. Our complete list of injectable peptides covers the full range of compounds commonly delivered this way.
Sublingual peptides sit between these two extremes. They bypass the stomach and liver but must still cross the sublingual epithelial membrane. Bioavailability varies enormously depending on the peptide, the formulation, and the technique, ranging from 15 percent for some compounds to over 70 percent for others. The convenience factor is significant. No needles, no reconstitution, no special storage requirements for many formulations. For people who need peptide reconstitution knowledge, must figure out which water to mix with peptides, and need to learn proper injection technique just to get started with injectables, sublingual options simplify the entire process.
How sublingual peptide delivery works
The science behind sublingual absorption is elegant in its simplicity, yet the details matter enormously for practical results. A peptide placed under the tongue does not simply "soak in" through random chance. Specific biophysical mechanisms govern whether a given peptide molecule crosses the sublingual membrane, how quickly it does so, and how much actually reaches the bloodstream intact.
Passive diffusion: the primary absorption mechanism
Unlike the small intestine, which has specialized transporter proteins that actively shuttle certain molecules across the gut wall, the sublingual mucosa relies almost entirely on passive diffusion. There are no known carrier-mediated transport mechanisms for peptides in the oral mucosa. The peptide molecule must cross the epithelial barrier on its own, driven by the concentration gradient between the high-concentration peptide solution under your tongue and the lower concentration in the capillary blood flowing beneath the epithelium.
Two pathways exist for this crossing.
The paracellular route takes the peptide between the epithelial cells, squeezing through the narrow spaces where cells meet. This pathway is limited by tight junctions and by organized lipid barriers in the superficial layers of the epithelium. Small, hydrophilic peptides tend to favor this route, but the barriers are real. For many larger peptides, paracellular transport is minimal.
The transcellular route takes the peptide directly through the epithelial cells. This requires the peptide to cross two cell membranes, the apical membrane facing the mouth and the basolateral membrane facing the blood vessels. Lipophilic molecules cross more easily here, which is one reason why certain peptide modifications, like adding fatty acid chains, can boost sublingual absorption. This is the same principle that governs how different peptide formulas behave in various delivery contexts.
Bypassing first-pass metabolism
This is the sublingual advantage that matters most.
When you swallow anything, it travels through the stomach, into the small intestine, gets absorbed into the portal vein, and flows directly to the liver before reaching systemic circulation. The liver is packed with metabolic enzymes, cytochrome P450 enzymes in particular, that chemically modify and break down compounds. For peptides, this first-pass effect is devastating. Most peptide chains are efficiently cleaved by hepatic enzymes, reducing bioavailability to near zero for many compounds.
Sublingual absorption routes blood flow through the sublingual veins into the internal jugular vein and then directly into the heart for systemic distribution. The liver is bypassed entirely on the first pass. The peptide enters general circulation intact, or at least as intact as it was when it crossed the sublingual membrane. This single advantage explains why sublingual bioavailability can be 10 to 50 times higher than oral bioavailability for the same peptide at the same dose. Researchers studying peptide safety should note that this also means sublingual peptides may produce faster and stronger systemic effects than oral versions.
The role of molecular weight
Not all peptides are created equal when it comes to sublingual absorption. Molecular weight is the single most important predictor of whether a peptide will cross the sublingual membrane effectively.
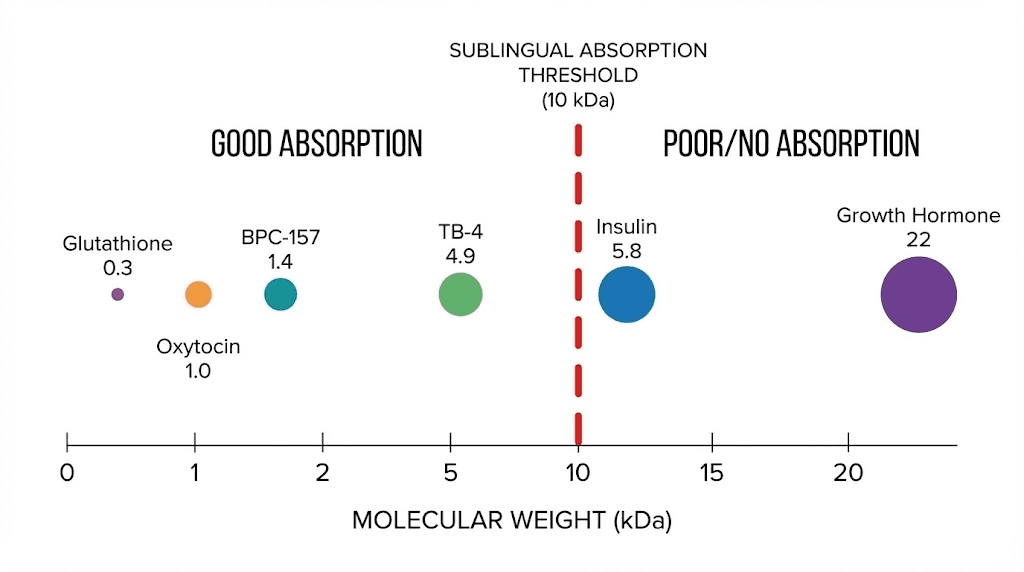
Research on porcine sublingual mucosa demonstrates that passive permeability drops sharply as molecular weight increases. The practical cutoff for effective passive sublingual absorption sits around 10 kDa (10,000 Daltons) for unenhanced formulations. Below this threshold, many peptides can achieve meaningful sublingual bioavailability. Above it, absorption becomes negligible without permeation enhancement technologies.
To put this in perspective, BPC-157 has a molecular weight of approximately 1,419 Daltons. Sermorelin sits around 3,358 Daltons. Both fall well below the 10 kDa threshold. Growth hormone, at roughly 22,124 Daltons, exceeds it. This is why you see sublingual formulations for smaller peptides but rarely for larger proteins. The molecular weight cutoff is not absolute, as molecular structure, charge, and lipophilicity also play roles, but it is the most reliable general predictor. Our guide to biomimetic peptides explores how peptide structure influences biological activity across different delivery methods.
Factors that influence sublingual absorption rate
Beyond molecular weight, several factors determine how effectively a peptide absorbs sublingually. Lipophilicity matters. More lipophilic peptides cross cell membranes more easily, favoring transcellular transport. Molecular charge influences interaction with the negatively charged mucus layer and cell surfaces. The pH of the formulation affects ionization state, which in turn affects membrane permeability. Concentration gradient drives the diffusion rate, so higher initial concentrations at the absorption site generally produce faster uptake.
Formulation design plays a critical role too. Mucoadhesive polymers keep the peptide in contact with the sublingual membrane longer, increasing absorption time. Permeation enhancers like bile salts, chitosan, or fatty acid conjugates can temporarily increase membrane permeability. The physical form of the delivery vehicle, whether it is a troche, liquid drop, dissolving strip, or gel, affects how long the peptide stays in the sublingual space before salivary washout carries it away. These are not minor details. They can mean the difference between 5 percent and 35 percent bioavailability for the same peptide compound.
Sublingual versus injectable versus oral peptides
Choosing a delivery method is not just about convenience. It is about matching the delivery route to the peptide, the therapeutic goal, and the practical realities of your daily life. Each route has genuine advantages and real limitations. Understanding the tradeoffs allows you to make an informed decision rather than defaulting to whatever seems easiest or most familiar.
Head-to-head comparison
Factor | Sublingual | Injectable (subcutaneous) | Oral (capsule/tablet) |
|---|---|---|---|
Bioavailability | 15-75% (varies by peptide) | 80-100% | 1-5% (most peptides) |
Onset of action | 15-30 minutes | 15-45 minutes | 30-90 minutes |
Ease of use | Very easy | Moderate (requires training) | Very easy |
Pain/discomfort | None | Mild (injection site) | None |
First-pass metabolism | Bypassed | Bypassed | Not bypassed |
Preparation needed | Minimal | Reconstitution required | None |
Dose consistency | Moderate (technique dependent) | High | Low (GI variable) |
Travel friendly | Very | Less (needles, cold chain) | Very |
Best peptide candidates | Small peptides under 10 kDa | All peptides | GI-stable peptides only |
Cost per effective dose | Moderate | Lower (less waste) | Higher (low absorption) |
The comparison page on injectable versus oral peptides breaks down these differences in even greater detail. For sublingual delivery, the key insight is this: it occupies a genuine middle ground. Not as efficient as injection, but far more efficient than oral swallowing for most peptides. And dramatically more convenient than injection for daily-use protocols.
When sublingual makes the most sense
Sublingual delivery shines in specific scenarios. If you have a genuine needle phobia, sublingual formulations allow access to peptide protocols that would otherwise be off-limits. If you travel frequently and cannot maintain cold chain storage for reconstituted injectable peptides, shelf-stable sublingual troches solve that problem. If your protocol involves a peptide with reasonable sublingual bioavailability, like BPC-157 or bioregulator peptides, you may not need injections at all.
Daily-use peptides, whether targeting energy and focus or menopause support, benefit most from sublingual convenience. Injecting once daily is manageable. Injecting twice or three times daily, as some protocols require, becomes burdensome. Sublingual administration takes 30 to 120 seconds of hold time. No preparation. No cleanup. This matters for long-term compliance, and compliance is the single biggest predictor of whether a peptide protocol actually delivers results. Our guide on how long peptides take to work emphasizes that consistency over weeks is essential.
When injection is still the better choice
For larger peptides above 10 kDa, injection remains necessary. Growth hormone secretagogues like CJC-1295 DAC, growth hormone itself, and most antibody fragments simply cannot achieve therapeutic blood levels through sublingual absorption alone. When precise dosing is critical, such as with semaglutide or tirzepatide for metabolic conditions, the predictability of subcutaneous injection is important. For localized effects, like injecting BPC-157 near an injury site for targeted tissue repair, sublingual delivery cannot replicate the local tissue concentrations that direct injection provides.
The honest truth? Most experienced researchers use both delivery methods. Many follow a peptide stacking approach that combines routes for different compounds. Sublingual for convenience-focused daily protocols. Injection for maximum potency and localized applications. The choice is not either/or. It is about matching the right tool to the right job.
Which peptides work best sublingually
Not every peptide belongs under your tongue. Some absorb beautifully through the sublingual membrane. Others barely cross at all. The difference comes down to molecular characteristics, inherent stability, and how well a given peptide interacts with the sublingual tissue environment. Here are the peptides with the strongest evidence for sublingual effectiveness.
BPC-157: the standout sublingual candidate
BPC-157 is arguably the best peptide candidate for sublingual delivery that exists. At just 15 amino acids and a molecular weight of approximately 1,419 Daltons, it falls well within the sublingual absorption window. But what makes BPC-157 truly exceptional is its gastric stability. Unlike virtually every other peptide, BPC-157 remains stable in human gastric juice for over 24 hours. It does not require carrier molecules or protective formulations to survive the oral environment. This inherent stability extends to the sublingual space, where salivary enzymes pose far less threat to BPC-157 than they do to most peptides.
Sublingual BPC-157 bioavailability is estimated at approximately 70 to 75 percent, which is extraordinary for a peptide delivered through any non-injection route. Oral capsule bioavailability sits lower, around 50 to 60 percent, still remarkable compared to the 1 to 2 percent typical of most oral peptides. Animal studies have demonstrated that oral and sublingual BPC-157 produces comparable healing effects to injectable administration for gastrointestinal applications. One study found that BPC-157 administered orally through drinking water produced substantial improvements in biomechanical, histological, and functional recovery of injured ligaments over a 90-day period, regardless of administration method.
For gut health applications specifically, sublingual BPC-157 may actually be preferable to injection. The peptide makes initial contact with oral and upper GI tissues as residual amounts are swallowed, providing both systemic absorption and local gastrointestinal effects. Our complete BPC-157 guide covers all administration methods, and the BPC-157 dosage calculator can help determine appropriate amounts regardless of delivery route. Research on how to take BPC-157 increasingly acknowledges sublingual delivery as a legitimate option, especially the oral supplement approach that many people find accessible.
Bioregulator peptides: designed for sublingual use
The Khavinson bioregulator peptides represent an entire class of compounds specifically formulated for sublingual delivery. These are short-chain peptides, typically just 2 to 4 amino acids in length, with molecular weights well under 1,000 Daltons. Their small size makes sublingual absorption highly efficient.
Vladimir Khavinson developed over 60 peptide bioregulators based on decades of research in Russia, with six gaining pharmaceutical approval. The "Lingual" product line delivers these bioregulators in sublingual form, with the same active ingredient doses as their capsule counterparts. Sublingual absorption provides faster onset and higher bioavailability compared to oral capsules. Key sublingual bioregulator formulations include Cerluten for brain tissue support, Visoluten for retinal health, Glandokort for adrenal function, Libidon for prostate tissue, and Zhenoluten for ovarian health. Our comprehensive guide on bioregulator peptides and the Khavinson peptides overview cover these compounds in detail.
Long-term research on bioregulator peptides has shown remarkable results, with animal studies demonstrating a 20 to 40 percent increase in mean lifespan and human studies reporting improved physiological function over 6 to 12 year observation periods. Whether delivered orally or sublingually, these tiny peptides reach their target tissues and influence gene expression, a process explored in depth in our how peptides work guide. The sublingual route simply gets them there faster. Anyone interested in longevity peptides or epitalon should understand how sublingual delivery fits into the broader bioregulator peptide landscape.
Sermorelin: a popular sublingual formulation
Sermorelin, a growth hormone releasing hormone analog with 29 amino acids and a molecular weight of approximately 3,358 Daltons, is one of the most commonly prescribed sublingual peptide troches. Compounding pharmacies, as discussed in our peptide therapy online guide, routinely produce sermorelin troches in 600 mcg and 1,000 mcg strengths, typically dosed five nights per week at bedtime to align with the natural nocturnal growth hormone pulse.
Sublingual sermorelin bioavailability falls in the 15 to 30 percent range, which is lower than injection but still clinically meaningful at appropriate doses. Because bioavailability is lower, sublingual troches often require higher nominal doses compared to injectable protocols. A typical injectable sermorelin dose of 200 to 500 mcg might translate to a 500 to 1,000 mcg sublingual troche to achieve comparable growth hormone stimulation. The benefits of sermorelin remain consistent across delivery methods, though the magnitude may differ. Users tracking sermorelin before and after results should account for the delivery method when evaluating outcomes. For men considering combination protocols, the sermorelin-ipamorelin blend is sometimes available in sublingual formulations as well. Those looking to compare growth hormone secretagogues should also review the ipamorelin benefits profile and the broader ipamorelin side effects overview.
PT-141 (bremelanotide): effective in sublingual form
PT-141, or bremelanotide, is a melanocortin receptor agonist used for sexual dysfunction. It works through the central nervous system rather than the vascular system, which distinguishes it from PDE-5 inhibitors. PT-141 is available in sublingual strip and troche formulations, and the sublingual route is gaining popularity because it avoids the injection-site reactions (nausea, flushing) that can accompany subcutaneous administration.
Sublingual PT-141 troches typically take effect within 30 to 60 minutes, compared to 45 to 60 minutes for injection. The slightly faster onset makes sense given the direct-to-bloodstream absorption pathway. For men and women alike, PT-141 is considered one of the best peptides for women and men when it comes to sexual health. Our guides on how to use PT-141, PT-141 nasal spray, and best peptides for libido provide broader context on this compound across all delivery methods.
Oxytocin: a well-studied sublingual candidate
Oxytocin, the nine-amino-acid neuropeptide hormone produced in the hypothalamus, cannot survive oral administration. The peptide is rapidly destroyed in the GI tract. However, sublingual delivery provides a viable alternative to nasal spray or injection. Compounding pharmacies produce sublingual oxytocin in liquid drops, troches, and fast-dissolving tablets, typically in the 10 to 100 IU range.
Research shows that sublingual oxytocin effectively influences social cognition and attention, though bioavailability is lower than intranasal or intravenous delivery. Clinical applications include pain management, lactation support, sexual function enhancement, and psychiatric conditions. The sublingual route may produce different central nervous system effects compared to intranasal delivery because of the different absorption pathway, a distinction relevant to those studying brain repair peptides. It is worth noting that research into peptides for hormone balance has explored oxytocin mechanisms extensively. For people exploring peptides for mood support or anxiety management, sublingual oxytocin represents an accessible option worth discussing with a healthcare provider.
Other peptides with sublingual potential
Several additional peptides show promise for sublingual delivery. Semax and Selank, both small neuropeptides, are traditionally delivered intranasally but have structural characteristics, small molecular weight, relative stability, that support sublingual absorption. Our guides on Semax dosage and Selank dosage discuss delivery options for these nootropic peptides. The pinealon bioregulator peptide, used for sleep and circadian rhythm support alongside DSIP, is another candidate with a molecular weight small enough for sublingual absorption. Many of the best peptides for brain function fall within the molecular weight range that supports this delivery route.
Which peptides do not work well sublingually
Just as some peptides are excellent sublingual candidates, others are poor choices for this delivery method. Understanding why certain peptides fail sublingually is just as important as knowing which ones succeed. It prevents wasted product and unmet expectations.
The molecular weight barrier
The 10 kDa threshold is not an arbitrary number. Research on porcine sublingual mucosa shows that passive permeability drops sharply and becomes negligible for molecules above this size. The sublingual epithelium simply cannot accommodate the passage of larger molecules through either paracellular or transcellular routes without assistance from permeation enhancers.
Growth hormone (22 kDa), insulin (5.8 kDa but with poor sublingual permeability due to structure), and most antibody fragments (25-50 kDa) fall into this category. While novel permeation enhancers like protamine derivatives have enabled sublingual absorption of proteins up to 150 kDa in mouse models, these technologies are not yet available in commercial peptide formulations. For now, if you are using larger peptides, injection remains the standard.
Peptides that degrade too quickly in saliva
Saliva contains peptidases and other enzymes that, while less aggressive than gastric enzymes, still degrade susceptible peptides. The sublingual space is not enzyme-free. Peptides with particularly vulnerable amino acid sequences, especially those containing arginine or lysine residues at cleavage-susceptible positions, may be broken down before absorption occurs. This is one reason why formulation matters so much, a concept explored more broadly in our guide on lyophilized versus liquid peptides. Enzyme inhibitors incorporated into sublingual formulations can protect vulnerable peptides during the absorption window.
Highly hydrophilic large peptides
Large peptides that are both hydrophilic and high molecular weight face a double barrier. Their hydrophilicity prevents efficient transcellular transport (crossing through cell membranes), while their size prevents efficient paracellular transport (passing between cells). These peptides are essentially locked out of both absorption pathways. CJC-1295, most growth hormone secretagogues, and GHRP-6 fall into categories where sublingual delivery is not practical with current technology.
When higher doses cannot compensate
Some people assume that you can overcome poor sublingual bioavailability by simply using a higher dose. This logic has limits. If a peptide has 2 percent sublingual bioavailability, achieving a therapeutic dose of 200 mcg in circulation would require placing 10,000 mcg under the tongue. Beyond the cost implications, such large doses can overwhelm the sublingual space, trigger excessive salivary production, and result in most of the product being swallowed rather than absorbed sublingually. There is a practical ceiling to how much peptide the sublingual tissue can absorb in a single administration, and for poorly-absorbed compounds, that ceiling falls below therapeutic thresholds. Using the peptide calculator to determine bioavailability-adjusted dosing can clarify when sublingual delivery is not viable for a particular compound.
How to take sublingual peptides properly
Technique matters. The difference between correct and incorrect sublingual administration can mean a twofold or threefold difference in actual absorption. Most people who report that sublingual peptides "do not work" are making technique errors that dramatically reduce bioavailability. Follow this protocol precisely.
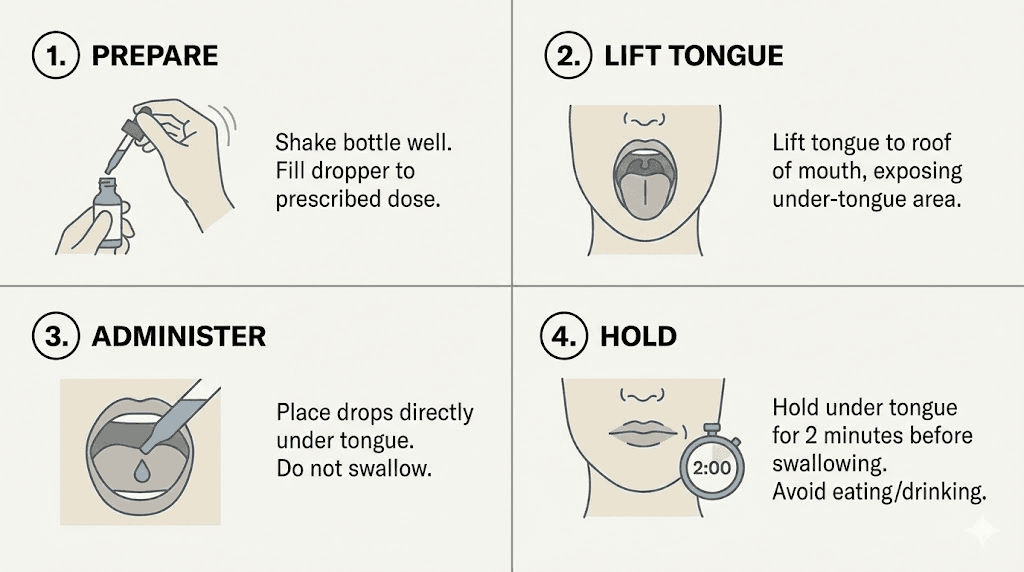
Step-by-step sublingual administration technique
Step 1: Prepare the oral environment. Do not eat or drink anything for 15 to 30 minutes before administration. Food particles, beverages, and excess saliva in the mouth reduce absorption by diluting the peptide and coating the sublingual membrane. If your mouth feels dry, good. A slightly dry mouth produces less salivary washout.
Step 2: Place the peptide correctly. Lift your tongue. Place the troche, drop, or strip directly on the floor of your mouth, centered beneath the tongue. The target area is the sublingual frenulum, where the tissue is thinnest and most vascular. Do not place it on top of the tongue, against the inner cheek, or between the gum and lip. Those are buccal or oral mucosal sites, not sublingual. They have thicker tissue and lower permeability.
Step 3: Hold without swallowing. This is where most people fail. Keep the peptide under your tongue and resist the urge to swallow saliva. Every swallow of saliva carries dissolved peptide away from the absorption site and into the stomach, where it faces the same degradation as an oral dose. Hold time varies by formulation. Liquid drops require 30 to 60 seconds. Troches need 15 to 30 minutes to fully dissolve. Dissolving strips fall in between, typically 2 to 5 minutes.
Step 4: Minimize saliva production. Try to relax. Anxiety or anticipation increases salivary flow. Breathe through your nose. Do not talk. Some people find that tilting the head slightly forward helps prevent involuntary swallowing. If using a troche, you can shift its position occasionally, rotating between the left sublingual space, right sublingual space, and center, to maximize mucosal contact area.
Step 5: Wait after administration. After the peptide has dissolved and been held for the appropriate duration, wait at least 15 minutes before eating, drinking, or brushing your teeth. Residual peptide may still be absorbing through the sublingual tissue, and food or drink can interrupt this process. For researchers tracking detailed peptide dosing protocols, noting the exact hold time and post-administration fasting window can help optimize results over time.
Timing optimization
When you take sublingual peptides relative to meals and daily activities affects absorption significantly. Most protocols recommend morning administration on an empty stomach or evening administration at least two hours after dinner. The stomach-empty window ensures minimal salivary enzyme activation from recent food, as eating stimulates digestive enzyme production throughout the oral cavity.
For growth hormone secretagogues like sublingual sermorelin, bedtime administration aligns with the natural nocturnal GH pulse. Take the troche 30 minutes before sleep, after brushing teeth (to remove food residue but not immediately before, as toothpaste chemicals can irritate the sublingual membrane). For BPC-157 targeting gut health, some practitioners suggest splitting the dose between morning and evening to maintain more consistent peptide levels. Our peptide cycle planning guide covers timing strategies across various protocols. Understanding how to calculate peptide dosages becomes especially important with sublingual delivery, where bioavailability adjustments are necessary.
Technique tips that most guides miss
A hot drink 10 to 15 minutes before administration increases blood flow to the sublingual region, which can enhance absorption rate. This is why some practitioners recommend a cup of warm water (not hot tea or coffee, which leave residue) before using sublingual troches.
Dry the sublingual area gently with a clean tissue before placing the peptide. This removes the existing saliva layer that sits between the peptide and the mucosal membrane, allowing more direct contact.
If using liquid drops, hold the dropper close to the sublingual tissue and release the drops directly onto the membrane. Do not let drops fall onto the tongue surface itself. The top of the tongue has different tissue characteristics and absorbs less efficiently.
Consider your oral health. Mouth ulcers, cuts, or inflamed gums can actually increase absorption, sometimes unpredictably, by exposing deeper tissue layers. Healthy oral mucosa provides the most consistent absorption profile. Anyone exploring common peptide mistakes should add sublingual technique errors to their awareness list. The peptide strength protocol framework also applies to sublingual dosing consistency.
Sublingual peptide forms and formulations
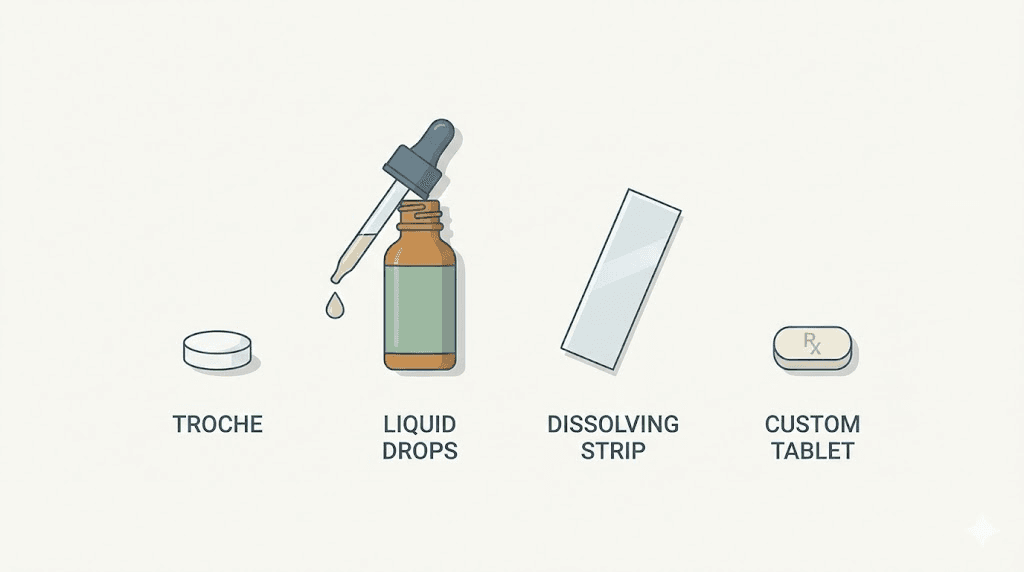
Sublingual peptides come in multiple physical forms, and each form has distinct advantages and limitations. The formulation type you choose affects dissolution time, absorption efficiency, stability, portability, and ease of use. Understanding the differences helps you select the right product for your specific protocol.
Troches (lozenges)
Troches are the most common sublingual peptide formulation. These are small, flavored lozenges typically produced by compounding pharmacies to a specific peptide concentration. A troche is placed under the tongue or between the cheek and gum and allowed to dissolve slowly over 15 to 30 minutes.
The slow dissolution is both an advantage and a challenge. Extended contact time with the sublingual membrane maximizes absorption opportunity. However, the prolonged dissolution also means more time for salivary washout to dilute the peptide. Well-formulated troches incorporate mucoadhesive polymers that help the troche stick to the mucosal surface, resisting salivary displacement. Common troche bases include polyethylene glycol, fatty acid bases, and silicone-based compounds, each with different dissolution profiles.
Sermorelin troches (600-1,000 mcg), PT-141 troches, semaglutide troches, and testosterone troches are among the most commonly prescribed sublingual troche formulations. The troche format allows precise dosing since each troche contains a known amount of peptide. They are shelf-stable at room temperature for short periods, though most compounding pharmacies recommend refrigeration for peptide troches.
Sublingual drops and liquids
Liquid sublingual formulations deliver the peptide in a dissolved solution, typically with a calibrated dropper or spray mechanism. Drops provide rapid dissolution since the peptide is already in solution, eliminating the 15 to 30 minute wait for troche dissolution. Hold time is shorter, typically 30 to 120 seconds, because the liquid contacts the sublingual membrane immediately.
The downside? Liquids are harder to hold in place. They spread across the oral cavity, mix with saliva, and are easily swallowed accidentally. The effective contact time with the sublingual membrane is shorter, which can reduce total absorption despite the faster initial dissolution. Liquid formulations also tend to have shorter shelf lives once opened, as the peptide in solution is more susceptible to degradation than in solid form. Storage guidelines for reconstituted and liquid peptides, covered in our storage after reconstitution guide, apply to sublingual liquids as well.
Dissolving strips and films
Thin film strips represent a newer delivery technology that combines advantages of both troches and liquids. A thin, polymer-based film embedded with peptide is placed on the sublingual tissue, where it adheres and dissolves over 2 to 5 minutes. The film format provides excellent mucosal contact, controlled release kinetics, and minimal salivary dilution.
Mucoadhesive films are particularly promising for peptide delivery. Research on chitosan-coated nanoparticle films has demonstrated enhanced mucoadhesion, improved epithelial uptake, and prolonged plasma exposure compared to liquid formulations. PT-141 sublingual strips are one commercially available example of this technology. Nanofiber mat delivery systems represent the cutting edge, with studies showing that these mats significantly enhance mucosal permeability by increasing local drug concentration and providing close, sustained contact with the mucosa.
Compounded custom formulations
Compounding pharmacies can create customized sublingual formulations tailored to specific peptides and patient needs. These formulations may include permeation enhancers, enzyme inhibitors, mucoadhesive agents, and flavoring to improve the absorption profile and patient experience. Custom formulations allow for combination products, such as a single troche containing both BPC-157 and TB-500 for researchers following a BPC-157 and TB-500 stacking protocol.
The quality of compounding matters enormously. Not all compounding pharmacies have the expertise or equipment to produce effective sublingual peptide formulations. Factors like particle size, polymer selection, dissolution rate, and permeation enhancer concentration all affect the final product performance. Our guide on peptide testing labs covers how to verify product quality, and understanding the difference between research and pharmaceutical grade peptides helps set appropriate expectations.
Bioavailability comparison data
Numbers tell the real story. Vague claims about sublingual peptides being "better absorbed" than oral peptides mean nothing without specific bioavailability data. Here is what the research actually shows.
Bioavailability by peptide and delivery route
Peptide | Sublingual bioavailability | Oral bioavailability | Injectable bioavailability | Molecular weight |
|---|---|---|---|---|
BPC-157 | 70-75% | 50-60% (gastric stable) | ~100% (SC) | 1,419 Da |
Bioregulator peptides | 40-60% (estimated) | 20-40% (estimated) | N/A (typically oral/SL) | 200-500 Da |
Sermorelin | 15-30% | Less than 5% | ~90% (SC) | 3,358 Da |
PT-141 | 15-25% (estimated) | Less than 5% | ~90% (SC) | 1,025 Da |
Oxytocin | 10-20% | Less than 1% | ~100% (IV) | 1,007 Da |
Desmopressin | 3-5% | 0.08-0.16% | ~100% (IV) | 1,069 Da |
Insulin | 1-2% (unenhanced) | Less than 1% | ~100% (SC) | 5,808 Da |
Semaglutide (enhanced) | Comparable to SC (novel enhancers) | 0.4-1% (Rybelsus formulation) | ~90% (SC) | 4,114 Da |
Several patterns emerge from this data. First, sublingual bioavailability consistently exceeds oral bioavailability, often by an order of magnitude. The peptide dosage chart typically references injectable values, so adjustments are needed for sublingual dosing. Second, smaller peptides generally achieve higher sublingual bioavailability.
Third, BPC-157 is a genuine outlier, its gastric stability gives it unusually high absorption across all oral routes. And fourth, novel permeation enhancer technologies are closing the gap between sublingual and injectable delivery for some peptides, including semaglutide, a compound with enormous clinical relevance as detailed in our semaglutide versus tirzepatide comparison.
What the 36.2 percent versus 24.8 percent study means
One frequently cited study found that sublingual delivery achieved bioavailability rates of 36.2 percent compared to 24.8 percent for oral administration of the same compound. This roughly 46 percent improvement from switching from oral swallowing to sublingual holding demonstrates the significance of bypassing first-pass metabolism and reducing gastrointestinal degradation. However, this study used a specific peptide formulation, and results vary across different compounds. The takeaway is not that every peptide achieves 36 percent sublingual bioavailability. The takeaway is that the sublingual route consistently outperforms oral swallowing, and the margin is clinically meaningful.
Novel delivery systems pushing the boundaries
Cutting-edge research is dramatically improving sublingual peptide absorption. Lipid-conjugated protamine peptides, developed as permeation enhancers, have enabled sublingual delivery of proteins with molecular weights from 22 to 150 kDa in mouse models, with effects comparable to subcutaneous injection. These enhancers work by forming nanopores on cell surfaces, temporarily increasing transcellular permeability without damaging the tissue.
Chitosan-coated liposomes carrying peptide payloads have shown enhanced mucoadhesion and epithelial uptake, with prolonged plasma exposure compared to unformulated sublingual solutions. PEGylated nanofiber assemblies using low-molecular-weight PEG (optimally 2,000 to 3,000 Daltons) decrease interactions with mucin and promote longer residence time at the sublingual site. Two-layer jelly formulations that control dissolution rate to keep the peptide in the sublingual region longer have shown improved urinary excretion of model drugs, indicating greater systemic absorption.
The peptide therapeutics market, valued at approximately 46 to 53 billion dollars and projected to reach 80 to 100 billion dollars within the next decade, is driving enormous investment in oral and sublingual delivery technologies. The parenteral (injection) segment currently dominates at roughly 85 percent of revenue, but the oral segment is projected to grow fastest. This investment trajectory means sublingual peptide technology will continue to improve rapidly. For researchers following peptide regulation developments, delivery method innovations will increasingly influence regulatory pathways and commercial availability.
Benefits of sublingual peptide delivery
The advantages of sublingual delivery extend beyond simply avoiding needles. Each benefit has practical implications for protocol adherence, cost-effectiveness, and therapeutic outcomes.
No needles, no injection anxiety
Needle phobia affects an estimated 20 to 25 percent of adults. For these individuals, injectable peptides are not merely inconvenient; they are psychologically inaccessible. Sublingual delivery eliminates this barrier entirely. No needles, no alcohol swabs, no injection site rotation, no disposal of sharps. The entire administration process involves placing something under your tongue. This accessibility opens peptide protocols to a significantly larger population. People who have avoided peptide therapy because of needle aversion, including those curious about peptides for muscle growth or anti-aging protocols, now have a viable path forward.
Rapid onset of action
Because the sublingual mucosa delivers peptides directly into the bloodstream, as explained in our how peptides work overview, onset of action is typically faster than oral administration and comparable to subcutaneous injection for some compounds. Sublingual formulations often produce detectable blood levels within 15 to 30 minutes, compared to 30 to 90 minutes for oral capsules that must transit the GI tract. For peptides where timing matters, such as PT-141 taken before sexual activity or sermorelin taken before sleep, this rapid onset provides practical advantage.
Improved compliance and protocol adherence
The single greatest threat to any peptide protocol is inconsistent use. People skip doses. They forget their morning injection. They travel without their reconstituted vials. Sublingual peptides dramatically reduce these compliance barriers. A troche can be taken anywhere, any time, without preparation or cleanup. There is no need for bacteriostatic water, mixing protocols, or water-to-peptide calculations. The simplicity translates directly into better adherence, and better adherence translates into better results.
Travel convenience
Traveling with injectable peptides requires cold chain management, needle disposal planning, and often explanations to security personnel or customs agents. Sublingual troches and strips look like ordinary lozenges or breath strips. They do not require refrigeration during short trips. They pass through airport security without questions. For frequent travelers, this convenience factor alone can justify choosing sublingual over injectable delivery for appropriate peptides. Our guides on peptide stability at room temperature and lyophilized versus liquid peptides provide relevant context for travel planning.
Dual local and systemic effects
An underappreciated advantage of sublingual peptide delivery is the potential for dual-action effects. When you hold BPC-157 under your tongue, the peptide contacts oral and upper GI mucosal tissue directly while also absorbing into systemic circulation. For gut health applications, this means the peptide works both locally on the oral and esophageal mucosa and systemically through blood-delivered distribution to the gastrointestinal tract. This dual mechanism may explain why some researchers report that sublingual BPC-157 is as effective as injection for GI conditions, as documented in our peptides for gut health resource.
Reduced injection site reactions
Subcutaneous peptide injections can cause injection site reactions including redness, swelling, itching, lipodystrophy (fat tissue changes) at the injection site, and rarely, infection. Those comparing the safest peptides for muscle growth should consider delivery method as part of the safety equation. Sublingual delivery eliminates all injection-site adverse effects. For people using peptides long-term, the cumulative impact of avoiding daily injection site trauma is meaningful, both cosmetically and for tissue health at injection sites.
Limitations and challenges of sublingual peptide delivery
No delivery method is perfect. Sublingual peptide delivery has genuine limitations that must be acknowledged and managed. Pretending otherwise leads to disappointment and wasted resources.
Salivary washout
Continuous saliva production is the primary enemy of sublingual absorption. The average person produces 0.5 to 1.5 liters of saliva per day, with flow rates that vary based on hydration status, time of day, and stimulation from food or flavored formulations. Each swallow of saliva carries dissolved peptide away from the sublingual membrane and into the stomach. Ironically, flavored troches, while more palatable, stimulate greater salivary flow, which can reduce absorption efficiency. This is why unflavored or minimally flavored formulations may actually perform better despite the less pleasant experience.
Dose limitations
The sublingual space is physically small. You can only fit so much peptide formulation under your tongue. For peptides with low sublingual bioavailability, the amount of product needed to achieve therapeutic blood levels may exceed what can practically be administered sublingually in a single dose. This is why some sublingual protocols require multiple daily administrations rather than a single dose, increasing complexity and reducing the convenience advantage.
Absorption variability
Sublingual absorption is more variable between individuals and between doses than injectable delivery. Factors like mucosal health, saliva volume, technique consistency, oral pH, and recent food intake all influence absorption. Two people taking the same sublingual troche can achieve meaningfully different blood levels. Even the same person may absorb different amounts on different days. This variability makes precise dose-response optimization harder than with injection, where absorption is highly predictable. The peptide cost calculator should account for this variability when comparing the true cost-effectiveness of sublingual versus injectable protocols.
Limited peptide candidates
The molecular weight cutoff and stability requirements mean that only a subset of therapeutic peptides can be delivered sublingually with current technology. Many of the most popular research peptides, including growth hormone secretagogues, ipamorelin combinations, and longer-chain compounds, remain injection-only for practical purposes. This limits the range of protocols that can be conducted entirely via sublingual delivery. A look at our complete peptide list reveals how many compounds still require injection for practical use. Those comparing options between peptides and steroids or peptides and TRT should factor delivery convenience into their decision-making process.
Quality control concerns
Most sublingual peptide formulations come from compounding pharmacies rather than FDA-approved manufacturers. Compounded medications do not undergo the same rigorous testing for bioequivalence, stability, and potency as commercially manufactured pharmaceuticals. Understanding the research versus pharmaceutical grade distinction is critical here, and navigating the grey market peptide landscape requires extra caution for sublingual products. The quality of a sublingual peptide troche depends entirely on the compounding pharmacy producing it, and quality varies widely. Verifying purity through independent testing labs and choosing reputable peptide vendors becomes even more important for sublingual formulations, where compounding quality directly affects absorption.
Common mistakes with sublingual peptides and how to fix them
Most sublingual peptide failures are user error, not product failures. These are the mistakes researchers make most often, along with the fixes.
Mistake 1: swallowing too early
This is the number one error. People place a troche under their tongue and swallow normally within the first minute, sending the peptide straight to the stomach. The fix is simple but requires discipline. Hold the troche for its full dissolution time, typically 15 to 30 minutes. Resist every urge to swallow. Let saliva pool under your tongue if necessary. Tilt your head slightly forward. Some practitioners recommend lightly biting the tip of the tongue as a reminder not to swallow. The first few times feel awkward. It becomes habitual within a week.
Mistake 2: eating or drinking too close to dosing
Eating within 15 minutes before or after sublingual administration dramatically reduces absorption. Food particles coat the sublingual membrane, creating a physical barrier. Beverages dilute the peptide concentration at the absorption site. Even water can wash the peptide away from the mucosal surface. The fix: maintain a strict 15 to 30 minute food and drink window on both sides of administration. Set a timer if necessary.
Mistake 3: incorrect placement
Placing the troche on top of the tongue, between the teeth, or against the hard palate misses the optimal absorption zone entirely. The sublingual frenulum area, the thin, vascular tissue connecting the underside of the tongue to the floor of the mouth, is the target. Placing the formulation against the inner cheek (buccal placement) is second-best but has thicker tissue and lower absorption rate. The fix: use a mirror the first few times. Lift your tongue. Place the troche or drops directly on the floor of the mouth beneath the tongue. Confirm placement visually until it becomes habit.
Mistake 4: using the wrong peptide sublingually
Attempting sublingual delivery with a peptide that has poor sublingual absorption wastes product and money. If you are using a peptide above 10 kDa without permeation enhancers, sublingual delivery is unlikely to provide therapeutic benefit. The fix: verify that your specific peptide has documented sublingual bioavailability before choosing this route. Check molecular weight. Check stability data. If the data does not support sublingual delivery, use injection or nasal spray instead.
Mistake 5: inconsistent technique
Sublingual absorption is technique-dependent. Doing it correctly on Monday but carelessly on Wednesday produces erratic blood levels and unreliable results. The fix: develop a consistent ritual. Same time of day. Same preparation steps. Same hold duration. Same post-dose fasting period. Consistency eliminates the variability that makes sublingual protocols unreliable for some users. People who follow our peptide cycle planning recommendations know that protocol consistency drives outcomes regardless of delivery method.
Mistake 6: storing sublingual formulations improperly
Peptide troches left in a hot car, exposed to direct sunlight, or stored in a humid bathroom cabinet degrade faster than most people expect. The fix: follow storage instructions precisely. Most sublingual peptide formulations should be refrigerated. If room temperature storage is acceptable for short periods, keep them in a cool, dry, dark location. Our guides on peptide storage, fridge storage duration, and peptide expiration apply to sublingual formulations just as much as injectable ones.
Mistake 7: expecting injectable-equivalent results at the same dose
A 200 mcg sublingual troche does not deliver the same systemic peptide level as a 200 mcg subcutaneous injection. With sublingual bioavailability ranging from 15 to 75 percent depending on the peptide, the effective dose reaching circulation is significantly lower. The fix: work with your healthcare provider or use bioavailability-adjusted dosing. If a peptide has approximately 30 percent sublingual bioavailability, you need roughly three times the injectable dose to achieve comparable blood levels. The peptide calculator and dosage calculation guide help with these conversions.
Sublingual peptides for specific health goals
Different health objectives call for different sublingual peptide strategies. The delivery route interacts with the therapeutic goal in ways that matter for practical protocol design.
Sublingual peptides for gut health
Gut health is perhaps the strongest use case for sublingual peptide delivery, specifically with BPC-157. The sublingual route provides dual benefits: systemic absorption through the bloodstream plus direct mucosal contact with the upper GI tract as residual amounts are swallowed. BPC-157 sublingual formulations are widely used for conditions involving the esophagus, stomach, and upper intestinal tract, where the peptide contacts tissue directly before systemic distribution.
Research confirms that BPC-157 delivered orally produces comparable healing effects to injection for gastrointestinal applications. Studies have shown efficacy against NSAID-induced GI toxicity, ulcer healing, and intestinal inflammation when administered through drinking water, which is essentially an oral/sublingual hybrid delivery. For comprehensive coverage of this topic, see our main peptides for gut health page and the detailed gut health peptides article. The KPV peptide, another small anti-inflammatory compound, also shows sublingual potential for gut-related applications, with dosing guidance available in our dedicated guide. More broadly, inflammation-targeting peptides represent a growing area for sublingual research.
Sublingual peptides for brain health and cognitive function
Small neuropeptides with sublingual potential include Semax, Selank, pinealon, and various Khavinson bioregulator peptides targeting brain tissue. The sublingual route for neuropeptides offers an interesting advantage: the sublingual venous drainage connects to the internal jugular vein, which supplies the brain relatively directly compared to peripheral venous return from injection sites in the abdomen or thigh.
Bioregulator peptides like Cerluten, specifically designed for brain tissue support, are available in sublingual formulations and are used in longevity-focused protocols. The best peptides for brain function guide covers these compounds in detail, alongside nootropic peptides like Cerebrolysin and BDNF-related peptides. For those researching peptides for brain repair or neuropathy treatment, sublingual delivery of appropriate small peptides offers a convenient, consistent administration route.
Sublingual peptides for immune support
Thymic peptides and immune-modulating bioregulators are excellent candidates for sublingual delivery given their small molecular sizes. Thymalin, a bioregulator peptide extracted from thymus tissue, has demonstrated immune-enhancing effects in long-term studies. Our guides on thymalin benefits, best immune system peptides, and peptides for autoimmune conditions provide broader context. For people managing allergies or seeking consistent immune modulation, daily sublingual dosing offers practical advantages over injection-based protocols.
Sublingual peptides for anti-aging and longevity
The bioregulator peptide approach to longevity was built on sublingual and oral delivery. Khavinson bioregulators, with decades of research behind them, are designed to be taken as capsules or sublingual formulations. Epitalon, one of the most studied longevity peptides, is a four-amino-acid compound (molecular weight ~390 Da) that falls easily within the sublingual absorption range. Our comprehensive guides on epitalon, longevity peptides, and peptides for anti-aging cover the full range of compounds in this category. The mitochondrial-targeted SS-31 peptide and the exercise mimetic MOTS-c are additional longevity compounds where delivery route research continues to evolve.
Sublingual peptides for sexual health
PT-141 sublingual troches and strips represent one of the most successful commercial applications of sublingual peptide delivery. The convenience of placing a dissolving strip under the tongue 30 to 60 minutes before sexual activity, without needing to prepare an injection, has made sublingual PT-141 popular among both men and women. Our guides on PT-141 usage, nasal spray alternatives, and libido peptides compare delivery methods for this application. Combined oxytocin-tadalafil sublingual tablets also exist as compounded formulations for sexual health.
Sublingual peptides for pain and injury recovery
BPC-157 sublingual formulations for injury recovery are common, though the evidence for systemic (sublingual/oral) BPC-157 is strongest for GI-tract injuries and generalized healing rather than targeted local tissue repair. Researchers dealing with back pain or general pain have options with both routes. For localized injuries, many researchers still prefer injection near the injury site. However, for people who cannot or will not inject, sublingual BPC-157 provides a meaningful alternative. Combined with TB-500, which has different delivery requirements, a comprehensive healing protocol might use sublingual BPC-157 alongside injectable TB-500. Our guides on injury recovery peptides, joint pain peptides, tendon repair, bone healing, and shoulder pain peptides discuss when different delivery routes are appropriate for recovery goals.
Sublingual peptides for weight management
Compounded semaglutide sublingual troches have emerged as an alternative to the injectable formulation (Ozempic/Wegovy) and the oral tablet (Rybelsus). While the FDA-approved oral semaglutide uses a specialized SNAC absorption enhancer, compounded sublingual versions attempt to achieve therapeutic levels through mucosal absorption. The best peptides for weight loss and fat loss peptide guides cover the full range of weight management compounds. For those comparing options, our peptides for fat loss resource and cagrilintide guide provide additional context. The weight loss peptide category, including tesofensine and related compounds, represents one of the fastest-growing applications for sublingual peptide delivery. Athletes exploring peptides for athletic performance and fast injury healing are also increasingly interested in sublingual options that simplify daily protocols.
Storage and handling of sublingual peptide products
Proper storage is not optional. Peptides degrade. Heat, light, moisture, and time are enemies of peptide stability, and sublingual formulations are no exception. In some ways, they are more vulnerable than lyophilized powders because they are already in a dissolved or semi-dissolved state within the troche matrix.
Temperature requirements
Most sublingual peptide troches should be refrigerated at 2 to 8 degrees Celsius (36 to 46 degrees Fahrenheit). Some formulations are stable at room temperature for limited periods, typically days to weeks, which provides a travel window. However, extended room temperature storage, especially above 25 degrees Celsius, accelerates peptide degradation. Never leave sublingual formulations in a hot car, near a window, or in a bathroom medicine cabinet where steam and heat from showers create an unstable environment.
Liquid sublingual formulations are typically less stable than troches and should always be refrigerated once opened. Unopened vials may have longer shelf lives depending on the formulation. Check the compounding pharmacy documentation for specific stability data. Our complete peptide storage guide provides temperature-specific recommendations across all peptide forms.
Moisture and humidity control
Peptides are hygroscopic. They absorb moisture from the air. For sublingual troches, this is particularly problematic because absorbed moisture can initiate the dissolution process prematurely, causing the troche to become sticky, soft, or crumbly before use. Store troches in airtight containers with desiccant packets. When removing a troche from the container, handle it with dry hands. Do not leave the container open longer than necessary. If you see visible moisture inside the container, replace the desiccant and inspect the troches for degradation. The principles from our guide on peptide shelf life in powder form apply to the solid peptide content within sublingual formulations.
Light protection
Some peptides are photosensitive and degrade when exposed to UV or visible light. Amber glass containers or opaque packaging protects against light-induced degradation. Even if the formulation is not known to be photosensitive, storing sublingual peptides away from direct light is a conservative best practice that costs nothing and protects potency. Our detailed guide on peptide stability at room temperature covers degradation factors for all peptide forms.
Shelf life expectations
Compounding pharmacies typically assign beyond-use dates of 30 to 90 days for peptide troches, depending on the specific formulation and storage conditions. This is shorter than the multi-year stability of lyophilized peptide powders stored at minus 20 degrees Celsius. Plan your purchase quantities accordingly. Buying a six-month supply of sublingual troches with a 60-day beyond-use date means losing product to expiration. Our guide on reconstituted peptide shelf life discusses similar time-limited stability considerations.
Handling best practices
Handle sublingual formulations with clean, dry hands. Do not break or cut troches unless specifically instructed by the prescribing provider, as this disrupts the formulation matrix and can alter dissolution and absorption characteristics. For liquid formulations, use the provided dropper and close the bottle immediately after use. Do not introduce foreign objects or contaminants into liquid peptide bottles. Avoid transferring peptides between containers, as each transfer introduces contamination and degradation risk.
Building a sublingual peptide protocol
Putting the pieces together. Knowing the science is one thing. Designing a practical, effective sublingual peptide protocol is another. Here is how to structure a sublingual-focused protocol from start to finish.
Protocol design: matching peptides to goals
Start with your health objective. Identify which peptides support that goal. Then filter for sublingual viability. Not every peptide you want to use will work sublingually, and forcing a poorly absorbed peptide into sublingual delivery wastes money and undermines results. Consult our peptide stacks guide and peptide stack calculator for combination protocol design. The question of how many peptides you can take at once applies to sublingual protocols just as it does to injectable ones, though the practical limit may be lower given the physical constraints of the sublingual space.
Sample sublingual protocol: gut healing focus
Goal: GI tract repair and inflammation reduction
Primary peptide: BPC-157 sublingual liquid, 500 mcg twice daily
Morning dose: 500 mcg sublingual drops on empty stomach, hold 60 seconds
Evening dose: 500 mcg sublingual drops 2 hours after dinner, hold 60 seconds
15-minute food/drink buffer before and after each dose
Duration: 4 to 8 weeks
Expected timeline: Initial improvements around days 7 to 10. Significant healing by weeks 4 to 6. This aligns with timelines described in our peptide results timeline guide. Monitoring progress using the framework from our before and after results article helps track effectiveness.
Sample sublingual protocol: longevity and anti-aging
Goal: Cellular health optimization and geroprotection
Primary peptides: Khavinson bioregulator peptides in sublingual form
Morning: Cerluten (brain) sublingual, 1 dose
Evening: Epitalon complex sublingual, 1 dose
10-day protocol cycles with breaks as per Khavinson methodology
Duration: 10-day cycles, repeated 2 to 3 times per year
This cyclic approach is consistent with the bioregulator peptide philosophy detailed in our bioregulator guide and peptide cycling guide.
Combining sublingual and injectable delivery
Many researchers use sublingual and injectable delivery together in the same protocol. This is not only acceptable but often optimal. For example, a recovery-focused protocol might combine sublingual BPC-157 (for convenience and GI-tract benefits) with injectable TB-500 (which requires injection for adequate bioavailability) and potentially injectable GHK-Cu for tissue repair. The BPC-157 versus TB-500 comparison helps understand when each compound is best suited to different delivery methods.
The key is to choose the delivery method based on each individual peptide rather than applying one method uniformly. Use sublingual for peptides that absorb well this way. Use injection for peptides that require it. Use nasal sprays for neuropeptides where that route is optimal. The Wolverine peptide nasal spray and Wolverine stack guides illustrate how different delivery methods combine in a single protocol.
Cost considerations
Sublingual formulations often have a higher per-dose cost than raw lyophilized peptide powder. You are paying for the compounding work, the formulation excipients, and the convenience. However, the effective cost comparison must account for bioavailability. If a sublingual peptide has 30 percent bioavailability and injection has 100 percent, you need approximately 3.3 times more peptide mass for the same effect. Factor in the cost of syringes, bacteriostatic water, alcohol swabs, and sharps disposal for injectable protocols. Our peptide therapy cost guide and general peptide cost overview provide frameworks for realistic cost comparison across delivery methods. The peptide cost calculator can help model these tradeoffs quantitatively.
The future of sublingual peptide delivery
Sublingual peptide technology is advancing rapidly. The current generation of troches and drops works well for small peptides, but emerging technologies promise to extend sublingual delivery to compounds that are currently injection-only.
Protamine-derived permeation enhancers represent one of the most exciting developments. By forming transient nanopores on epithelial cell surfaces, these enhancers have enabled sublingual absorption of proteins up to 150 kDa in animal models, with effects comparable to subcutaneous injection. If this technology translates to commercial formulations, it could make growth hormone, insulin, and dozens of other therapeutic proteins available through sublingual delivery.
Mucoadhesive nanofiber mats, chitosan-coated liposomes, and PEGylated nanofiber assemblies are moving from laboratory research into preclinical development. These formulations address the core challenges of salivary washout, limited residence time, and epithelial permeability that currently limit sublingual peptide absorption.
The trend is clear. The oral delivery segment of the peptide therapeutics market is projected to grow faster than any other delivery route over the coming decade. Investment in non-injectable delivery technologies is accelerating. Within a few years, sublingual formulations for many peptides that currently require injection will likely become available. This democratization of peptide access will bring these compounds to people who never would have started an injection-based protocol. For anyone tracking developments in online peptide therapy or peptide legality, delivery innovation is reshaping the entire landscape.
SeekPeptides has built the most comprehensive resource available for understanding peptide delivery methods, from injection protocols to sublingual techniques to nasal spray delivery. As sublingual technology evolves, members access updated protocols, bioavailability data, and expert guidance for optimizing every delivery route. For researchers exploring sublingual peptides alongside injectable and oral options, SeekPeptides provides the evidence-based framework to make informed decisions about which delivery method matches each peptide and each health goal.
Frequently asked questions
How long should you hold a sublingual peptide under your tongue?
Hold time depends on the formulation. Liquid drops require 30 to 120 seconds. Troches need 15 to 30 minutes to dissolve fully. Dissolving strips typically take 2 to 5 minutes. The critical rule is to avoid swallowing during the hold period, as this removes the peptide from the absorption site. After the peptide has fully dissolved, wait an additional 15 minutes before eating or drinking. Consistency in hold time is one of the most important factors for reliable sublingual absorption, as explained in our peptide dosing guide.
Are sublingual peptides as effective as injections?
It depends on the peptide. BPC-157 achieves 70 to 75 percent sublingual bioavailability, making it nearly as effective as injection for many applications. Bioregulator peptides are specifically designed for oral and sublingual delivery. However, larger peptides like growth hormone secretagogues achieve only 15 to 30 percent sublingual bioavailability, requiring significantly higher doses to approach injectable effectiveness. For localized injury treatment, injection near the injury site provides benefits that systemic sublingual delivery cannot replicate. The injectable versus oral comparison provides a detailed framework for evaluating delivery methods by compound.
Can you take BPC-157 sublingually?
Yes. BPC-157 is one of the best sublingual peptide candidates because of its small molecular weight (1,419 Da) and exceptional stability in the oral environment. Sublingual BPC-157 achieves approximately 70 to 75 percent bioavailability. It is especially effective for gastrointestinal applications, where the peptide provides both systemic and local mucosal effects. Our complete BPC-157 guide and 5mg dosing guide cover sublingual protocols alongside injectable options.
What is a peptide troche?
A peptide troche (pronounced "tro-key") is a small, medicated lozenge formulated by a compounding pharmacy to contain a specific peptide at a precise dose. It is placed under the tongue or between the cheek and gum, where it dissolves slowly over 15 to 30 minutes, allowing the peptide to absorb through the oral mucosa into the bloodstream. Troches bypass the digestive system, providing higher bioavailability than capsules for most peptides.
Do sublingual peptides need to be refrigerated?
Most sublingual peptide troches should be refrigerated at 2 to 8 degrees Celsius for optimal stability. Some formulations tolerate room temperature storage for short periods, typically up to a few weeks, which provides a travel window. Liquid sublingual formulations should always be refrigerated after opening. Always check the specific storage instructions from your compounding pharmacy, as stability varies by formulation. Our peptide storage guide covers temperature requirements across all peptide forms.
Which peptides cannot be taken sublingually?
Peptides above approximately 10 kDa molecular weight generally cannot achieve therapeutic blood levels through sublingual delivery without permeation enhancers. This includes growth hormone, most antibody fragments, and larger peptide hormones. Peptides that are rapidly degraded by salivary enzymes are also poor sublingual candidates. For these compounds, subcutaneous injection remains the appropriate delivery method. Understanding the complete range of options, from our complete peptide list, helps match each compound to its optimal delivery route.
Can you combine multiple sublingual peptides in one dose?
Some compounding pharmacies produce combination sublingual formulations containing two or more peptides in a single troche. This is practical when the peptides are compatible and the combined volume fits the sublingual space. However, combining too many peptides can increase troche size beyond what dissolves effectively under the tongue, and interactions between peptides or excipients can affect stability and absorption. Our guides on peptide stacking and taking multiple peptides apply to sublingual protocols with the additional consideration of physical space limitations.
How do sublingual peptides compare to nasal spray peptides?
Both sublingual and nasal spray delivery bypass first-pass metabolism and provide faster onset than oral capsules. Nasal delivery has higher bioavailability for some peptides, particularly neuropeptides like Semax and Selank, due to the nasal mucosa direct proximity to the brain and rich vascularization. Sublingual delivery is generally more convenient and less technique-sensitive than nasal sprays. The choice often depends on the specific peptide and therapeutic target. Our nasal spray peptides guide provides a detailed comparison.
Are sublingual peptides safe?
Sublingual delivery itself is a well-established pharmaceutical route used for many medications, including nitroglycerin, certain vitamins, and hormone preparations. Checking whether peptides show up on drug tests is relevant regardless of delivery route. The safety profile of sublingual peptides depends primarily on the specific peptide being administered rather than the delivery route. Side effects are generally milder than injectable administration because there are no injection-site reactions. Mild mouth irritation is possible with some formulations. As with all peptide use, working with a knowledgeable healthcare provider and sourcing from reputable compounding pharmacies is essential. Our peptide safety guide covers risk management across all delivery methods.
How much do sublingual peptide troches cost?
Sublingual peptide troche costs vary widely depending on the specific peptide, dose, quantity, and compounding pharmacy. Generally, troches cost more per dose than raw peptide powder reconstituted for injection because of the compounding labor and specialized excipients. However, when you factor in the cost of injection supplies, bacteriostatic water, and the time spent preparing each injection, the total cost difference narrows. For detailed cost analysis, see our peptide therapy cost guide and use the peptide cost calculator.
External resources
Development of new sublingual formulation for transmucosal delivery of peptides (PubMed)
Systemic delivery of proteins using novel peptides via the sublingual route (ScienceDirect)
Approaches for enhancing oral bioavailability of peptides and proteins (PMC)
For researchers serious about optimizing their peptide protocols across every delivery method, SeekPeptides offers the most comprehensive resource available. Members access evidence-based guides covering sublingual, injectable, nasal, and oral delivery, along with personalized protocol builders, bioavailability-adjusted dosing calculators, and a community of experienced researchers who have navigated these exact decisions. Whether you are transitioning from injection to sublingual delivery, designing a mixed-route protocol, or exploring peptides for the first time, SeekPeptides provides the framework you need to make informed, confident choices.
In case I do not see you, good afternoon, good evening, and good night. May your sublingual absorption stay efficient, your peptide protocols stay consistent, and your health goals stay within reach.