Jan 8, 2026

Taking semaglutide or Ozempic creates a unique challenge for anyone dealing with injuries, slow recovery, or concerns about muscle loss during rapid weight loss. The GLP-1 revolution has transformed weight management, but many users discover that losing 15-20% of body weight comes with unintended consequences, including loss of lean muscle mass that can reach 25-40% of total weight lost. For those experiencing nagging injuries, slow wound healing, or wanting to preserve hard-earned muscle while on GLP-1 therapy, healing peptides like BPC-157 and TB-500, along with growth hormone secretagogues like Ipamorelin, offer potential solutions worth exploring with medical supervision. This guide covers which peptides researchers combine with Ozempic, the science behind each combination, safety considerations, proper protocols, and how SeekPeptides can help you navigate this increasingly common scenario.
The Ozempic healing challenge
Semaglutide works remarkably well for weight loss. Too well, some might argue. The rapid reduction in body weight that makes GLP-1 agonists so effective also creates challenges that healing peptides may help address.
Why healing becomes harder on GLP-1s
Several factors contribute to healing challenges while taking Ozempic or similar medications:
Reduced caloric intake: GLP-1 agonists dramatically decrease appetite. While this drives weight loss, it also means less nutritional building blocks available for tissue repair. Protein intake often drops significantly, and protein provides the amino acids essential for healing.
Muscle loss concerns: Research shows that roughly one-quarter to one-third of weight lost on GLP-1 agonists comes from lean body mass rather than fat. This muscle loss, sometimes called "Ozempic face" or "Ozempic body," represents more than cosmetic concerns. Muscle tissue plays crucial roles in metabolic health, physical function, and recovery capacity.
Rapid metabolic changes: The speed of weight loss on semaglutide often outpaces the body's ability to adapt. When weight comes off quickly, there's less opportunity to preserve and rebuild muscle tissue.
Connective tissue stress: Rapid weight loss can stress joints, tendons, and ligaments as they adapt to different mechanical loads. Some users report new joint pain or aggravation of existing issues.
These factors don't mean Ozempic prevents healing entirely. But they do create an environment where additional support may prove valuable.
Common scenarios requiring healing support
Several situations prompt people on GLP-1 therapy to explore healing peptides:
Pre-existing injuries: Many people start Ozempic while already dealing with chronic injuries, whether joint pain, tendonitis, or other issues that excess weight may have caused or worsened.
New injuries from increased activity: Weight loss often motivates increased physical activity. This is positive, but new exercise habits can lead to overuse injuries, especially when the body is simultaneously adapting to weight changes.
Post-surgical recovery: Some undergo procedures like skin removal surgery after major weight loss. Optimizing healing during recovery becomes a priority.
Muscle preservation goals: Athletes, fitness enthusiasts, or anyone wanting to maintain strength while losing fat may seek peptides that support lean mass.
General wellness optimization: Some simply want to support their body's overall recovery capacity during a period of significant metabolic change.
Healing peptides compatible with Ozempic
Several peptides have gained attention for their potential to support healing while taking GLP-1 agonists. Understanding each option helps inform discussions with healthcare providers.
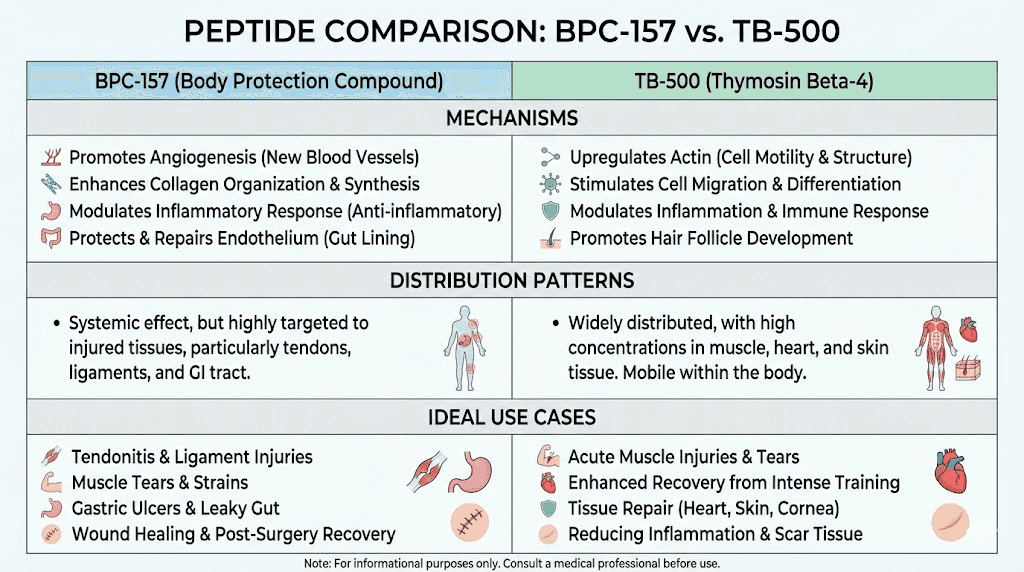
BPC-157: The tissue repair peptide
BPC-157 (Body Protection Compound-157) represents the most widely discussed healing peptide. Originally isolated from human gastric juice, this 15-amino-acid peptide has demonstrated remarkable tissue repair properties in animal studies.
Why it pairs well with Ozempic:
BPC-157's mechanisms don't interfere with GLP-1 signaling. The peptide works through different pathways, primarily promoting angiogenesis (new blood vessel formation), modulating growth factors, and supporting tissue regeneration. This mechanistic independence suggests the compounds can work simultaneously without competing or conflicting.
Interestingly, BPC-157 may support gut health, which aligns well with the GI-focused mechanism of GLP-1 agonists. Some researchers speculate it could help with the nausea and digestive discomfort some experience on semaglutide, though this remains theoretical.
What it targets:
BPC-157 has shown benefits for tendon injuries, ligament damage, muscle tears, and general wound healing in preclinical research. The peptides for tendon repair guide covers these applications in detail.
For someone on Ozempic dealing with joint pain, chronic tendonitis, or recovering from injury, BPC-157 offers a targeted healing mechanism that doesn't depend on the pathways semaglutide affects.
Typical protocols:
Research protocols typically use 250-500mcg of BPC-157 once or twice daily. Some prefer injecting near the injury site for localized effects, while others use subcutaneous abdominal injections for systemic distribution. The BPC-157 dosage calculator helps determine appropriate amounts.
Protocol length varies based on injury severity. Minor issues might respond within 2-4 weeks. Chronic conditions often require 6-12 weeks. Some cycle the peptide with periodic breaks.
TB-500: Systemic healing support
TB-500 (Thymosin Beta-4) offers complementary healing mechanisms to BPC-157. This peptide, found naturally in almost all human cells, plays fundamental roles in tissue repair and regeneration.
Why it pairs well with Ozempic:
TB-500 works through actin regulation and cellular signaling pathways unrelated to GLP-1 receptors. Like BPC-157, its mechanisms operate independently of semaglutide's appetite and glucose effects.
TB-500's smaller molecular weight allows it to distribute more systemically compared to BPC-157's more localized action when injected near injuries. This makes TB-500 particularly relevant for people with multiple issues or seeking general recovery support.
What it targets:
TB-500 promotes healing across multiple tissue types, including muscle, tendons, ligaments, and even cardiac tissue. It reduces inflammation, enhances cell migration to injury sites, and supports tissue remodeling.
For Ozempic users experiencing widespread joint discomfort, multiple minor injuries, or general recovery challenges, TB-500's systemic distribution may prove advantageous.
Typical protocols:
Standard research protocols use 2-2.5mg of TB-500 twice weekly during an initial loading phase, typically lasting 4-6 weeks. Maintenance dosing drops to once weekly or less. The TB-500 dosage calculator assists with protocol planning.
BPC-157 + TB-500: The healing stack
Many researchers combine BPC-157 and TB-500 for synergistic healing effects. The rationale involves their complementary mechanisms:
BPC-157 provides targeted, local healing support with strong effects on angiogenesis and growth factor signaling. TB-500 offers systemic distribution and broad tissue support through different cellular pathways.
Together, they may provide both localized and systemic healing enhancement. For someone on Ozempic dealing with healing challenges, this combination addresses the issue from multiple angles.
Standard stacking protocols run both peptides simultaneously at their typical individual dosages. Some prefer different injection sites, using BPC-157 near specific injuries and TB-500 subcutaneously in the abdomen.
The peptide stack calculator helps design combination protocols safely.
Muscle preservation peptides with Ozempic
Beyond injury healing, preserving lean muscle mass represents a major concern for Ozempic users. Growth hormone secretagogues offer potential solutions.
The muscle loss problem explained
GLP-1 agonist weight loss typically includes significant lean mass reduction. Studies suggest 25-40% of weight lost may come from muscle rather than fat. This happens for several reasons:
Caloric deficit magnitude: The dramatic appetite suppression from semaglutide creates substantial caloric deficits. While this drives fat loss, the body also catabolizes muscle for energy when deficits become too large.
Protein intake reduction: Many Ozempic users struggle to consume adequate protein due to reduced appetite. Without sufficient amino acids, the body cannot maintain or build muscle tissue.
Activity changes: Some experience fatigue or reduced energy on GLP-1s, leading to less physical activity and resistance training that would otherwise preserve muscle.
Metabolic adaptations: Rapid weight loss triggers metabolic adaptations including reduced muscle protein synthesis rates.
The consequences extend beyond aesthetics. Lost muscle reduces metabolic rate, making weight regain more likely. It impairs physical function and independence, particularly concerning for older adults. It also affects overall health, as muscle tissue plays important roles in glucose metabolism and hormonal balance.
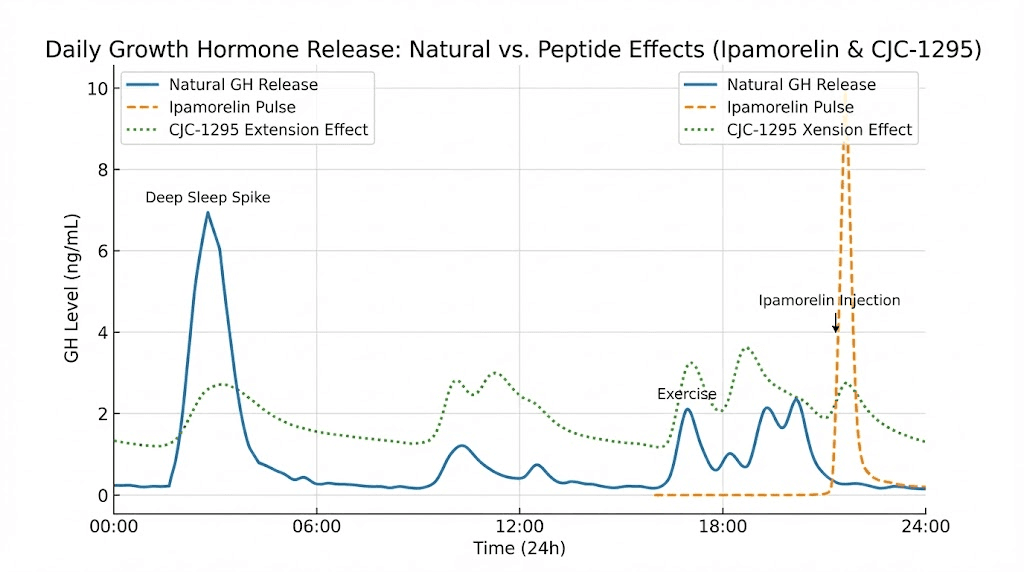
Ipamorelin: The clean GH releaser
Ipamorelin stimulates natural growth hormone release without many side effects associated with other secretagogues. This makes it particularly relevant for Ozempic users seeking muscle preservation.
Why it pairs well with Ozempic:
Ipamorelin works through ghrelin receptors in the pituitary, triggering growth hormone release. This mechanism operates entirely independently of GLP-1 pathways. The peptides don't compete or interfere with each other.
More importantly, Ipamorelin doesn't significantly affect appetite, cortisol, or prolactin, unlike some other GH secretagogues. This matters because Ozempic users don't need additional appetite stimulation, and hormonal disruptions could complicate their protocol.
Benefits for Ozempic users:
Growth hormone supports multiple processes relevant to GLP-1 therapy:
Muscle protein synthesis: GH stimulates muscle building and repair, potentially counteracting the catabolic effects of severe caloric restriction.
Fat metabolism: GH enhances lipolysis (fat breakdown), potentially complementing semaglutide's weight loss effects while shifting the ratio toward fat loss rather than muscle loss.
Connective tissue support: GH promotes collagen synthesis, supporting tendons, ligaments, and skin health during rapid body composition changes.
Sleep quality: Many report improved deep sleep on Ipamorelin, which is when the body does most of its repair and recovery.
Typical protocols:
Research protocols commonly use 200-300mcg of Ipamorelin, typically administered before bed to align with natural GH release patterns. Some use twice daily dosing. Cycles often run 8-12 weeks with breaks between.
CJC-1295: Extended GH support
CJC-1295 often pairs with Ipamorelin for enhanced growth hormone support. While Ipamorelin triggers acute GH pulses, CJC-1295 extends the duration of release.
Why it pairs well with Ozempic:
CJC-1295 works through growth hormone releasing hormone (GHRH) receptors, again operating independently of GLP-1 pathways. The combination with Ipamorelin creates sustained, physiologically-relevant GH elevation.
Benefits for muscle preservation:
The CJC-1295/Ipamorelin combination is often called the "gold standard" for body recomposition, promoting muscle growth while encouraging fat loss. For Ozempic users, this directly addresses the concern about losing lean mass alongside fat.
Dr. Chakravarthy explains the synergy: "CJC-1295 provides steady GH release, while Ipamorelin triggers short pulses. Together, they promote recovery, improved sleep, fat loss, and lean muscle development, without overstimulating cortisol or prolactin."
Typical protocols:
The combination typically uses CJC-1295 (100-300mcg) with Ipamorelin (200-300mcg), often administered together before bed. The CJC-1295 dosage calculator helps determine appropriate amounts.
Creating a comprehensive Ozempic support stack
Combining healing and muscle preservation peptides creates a comprehensive support strategy for Ozempic users. Understanding how to structure such protocols helps optimize outcomes.
The complete stack approach
A comprehensive peptide stack for someone on semaglutide might include:
For healing support:
BPC-157 (250-500mcg daily) for targeted tissue repair, particularly if dealing with specific injuries. TB-500 (2mg twice weekly) for systemic healing and inflammation support.
For muscle preservation:
Ipamorelin (200-300mcg before bed) for growth hormone support. CJC-1295 (100-300mcg before bed) for extended GH release.
Timing considerations:
BPC-157 can be administered at any time, though some prefer splitting into morning and evening doses. TB-500 is typically twice weekly, often on non-consecutive days.
GH secretagogues work best on an empty stomach, ideally 2-3 hours after eating and 30 minutes before sleep. This aligns with natural GH release patterns during deep sleep.
Ozempic itself is typically once weekly, so it doesn't create daily timing conflicts with other peptides.
Simplified stacks
Not everyone needs a comprehensive four-peptide stack. Simpler approaches may suffice depending on goals:
Healing focus only:
BPC-157 alone for specific injuries, or BPC-157 + TB-500 for more comprehensive healing support.
Muscle preservation focus only:
Ipamorelin alone for clean GH support, or Ipamorelin + CJC-1295 for enhanced effects.
Balanced approach:
BPC-157 + Ipamorelin combines one healing peptide with one GH secretagogue, addressing both concerns without complexity.
The peptide stacks guide explores combination strategies in greater depth.
What about collagen peptides?
Oral collagen peptides represent a different category entirely. These are dietary supplements rather than research peptides, and they're readily available without the regulatory complexity of injectable peptides.
Collagen peptides may support skin elasticity, joint health, and connective tissue during weight loss. For Ozempic users concerned about loose skin or joint discomfort, collagen supplementation offers a simple, accessible option that complements other approaches.
However, oral collagen works differently than injectable healing peptides. It provides amino acid building blocks for the body's own collagen synthesis rather than directly triggering repair mechanisms like BPC-157 or TB-500.
Safety considerations for peptide combinations
Combining peptides with Ozempic requires careful attention to safety. While these compounds work through different mechanisms, combining multiple substances always warrants caution.
The regulatory reality
Important context: Most peptides discussed here lack FDA approval for the purposes people use them for. BPC-157 was placed on the FDA's Category 2 bulk drug substance list, meaning it cannot be compounded by commercial pharmaceutical companies. BPC-157's regulatory status continues evolving.
Ozempic itself is FDA-approved for diabetes and (as Wegovy) for weight loss. But combining it with unapproved research peptides means entering territory without formal safety data on the combinations.
This regulatory reality doesn't mean the combinations are dangerous. It means there's limited formal evidence on safety, and caution is warranted.
Known and theoretical concerns
BPC-157 considerations:
BPC-157 promotes angiogenesis (new blood vessel formation), which supports healing but raises theoretical concerns for anyone with cancer or precancerous conditions. New blood vessel growth could theoretically support tumor growth. No human evidence confirms this risk, but the mechanism warrants awareness.
TB-500 considerations:
Animal studies found TB-500 could accelerate dormant tumor growth and affect immune responses. Again, human data is limited, but those with cancer history should exercise particular caution.
GH secretagogue considerations:
Growth hormone elevation can affect blood sugar regulation. Since Ozempic is often prescribed for diabetes or prediabetes, adding compounds that influence glucose metabolism requires monitoring. GH typically raises blood sugar acutely, potentially counteracting some of semaglutide's glucose-lowering effects.
Long-term GH elevation also carries theoretical cancer concerns, as GH and IGF-1 can promote cell growth. Moderate, physiological elevation from secretagogues differs from supraphysiological HGH doses, but the theoretical concern exists.
Peptide safety and risks covers these considerations comprehensively.
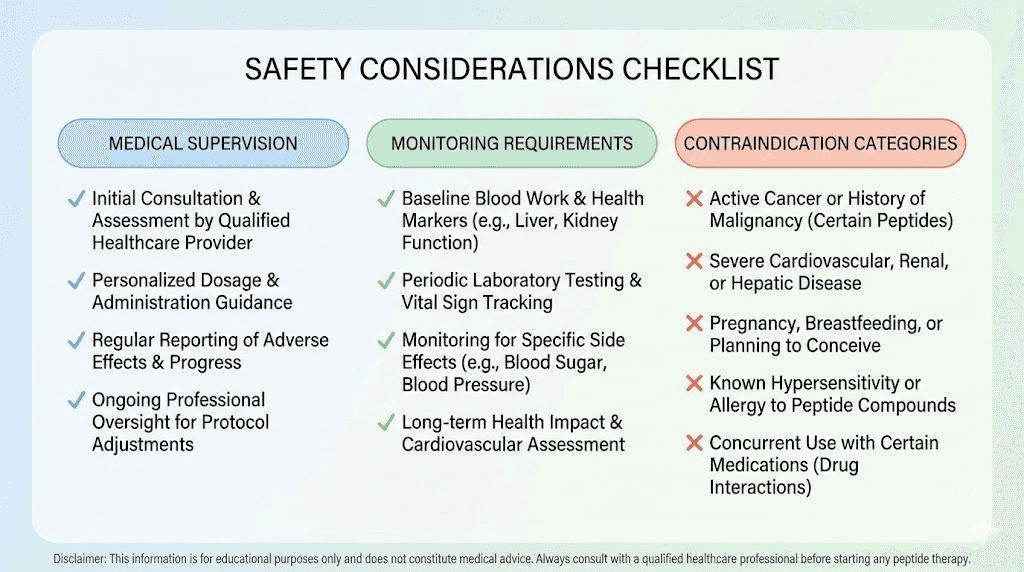
Medical supervision is essential
Given the combination of an FDA-approved medication (Ozempic) with research peptides, medical supervision becomes particularly important. A qualified provider can:
Assess baseline health: Bloodwork before starting peptides establishes baseline hormone levels, liver function, kidney function, and other relevant markers.
Monitor for interactions: While peptides and GLP-1s work through different mechanisms, individual responses vary. Professional monitoring catches problems early.
Adjust protocols: Dosing may need adjustment based on response, side effects, or changes in the primary Ozempic protocol.
Ensure quality: Medical channels often provide access to higher-quality peptides than research chemical markets.
Peptide therapy clinics specialize in these protocols. Many now offer telemedicine consultations, expanding access. SeekPeptides helps connect users with appropriate resources and education.
Practical protocols for Ozempic users
Implementing peptide protocols alongside Ozempic requires attention to practical details. Proper handling, timing, and administration affect outcomes.
Reconstitution and storage
Most peptides arrive as lyophilized (freeze-dried) powders requiring reconstitution before use. Key considerations:
Bacteriostatic water is the standard diluent for injectable peptides. It contains a preservative that prevents bacterial growth, allowing multi-use from a single vial.
The peptide reconstitution calculator determines how much water to add for desired concentrations. Getting this right affects dosing accuracy.
After reconstitution, peptides require refrigeration. Reconstituted peptide stability varies, but most remain potent for 3-4 weeks when properly stored.
Ozempic comes pre-mixed in an injection pen, requiring refrigeration but no reconstitution. Its storage requirements don't conflict with peptide storage.
Injection protocols
Peptide injection technique is straightforward once learned. Subcutaneous injection (into fat tissue) is standard for most peptides.
Ozempic is also subcutaneous, typically injected in the thigh, abdomen, or upper arm. Using different sites for Ozempic and other peptides is practical, preventing any confusion and allowing site rotation.
For BPC-157 targeting specific injuries, some prefer injecting near the injury site. This doesn't affect Ozempic administration, which occurs in standard subcutaneous locations.
Timing around meals
Meal timing matters for GH secretagogues but not significantly for healing peptides or Ozempic:
Ipamorelin/CJC-1295: Best on an empty stomach. Food, especially carbohydrates and fats, can blunt growth hormone release. Most protocols recommend 2-3 hours after eating, with sleep following within 30-60 minutes.
BPC-157: No significant meal timing requirements. Can be taken with or without food.
TB-500: No significant meal timing requirements.
Ozempic: Administered once weekly, on any day, with or without meals. No timing conflicts with peptides.
Cycling strategies
Peptide cycling prevents receptor desensitization and maintains effectiveness. Common approaches:
Healing peptides: BPC-157 and TB-500 are often run for 6-12 week cycles, with 2-4 week breaks between. Some use 5-days-on, 2-days-off protocols within cycles.
GH secretagogues: Ipamorelin and CJC-1295 cycles typically run 8-12 weeks, followed by 4-week breaks. Some maintain them longer under medical supervision.
Ozempic: Unlike peptides, GLP-1 agonists are typically continuous therapy rather than cycled. Stopping semaglutide often leads to weight regain, so most use it long-term under medical supervision.
This means peptide cycling occurs around continuous Ozempic use. The peptides come and go while the GLP-1 therapy continues.
Optimizing results while on GLP-1 therapy
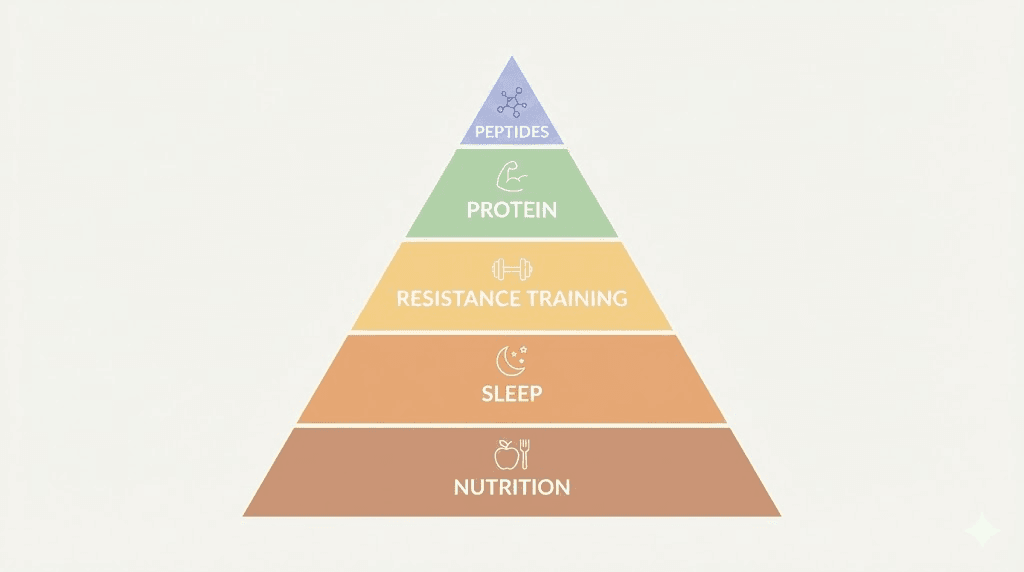
Peptides alone won't maximize outcomes. Lifestyle factors profoundly influence healing, muscle preservation, and overall results on Ozempic.
Protein intake: The critical factor
Adequate protein intake may be the single most important factor for preserving muscle on GLP-1 therapy. Recommendations typically suggest 1.0-1.6 grams of protein per kilogram of body weight daily, with higher amounts for those actively trying to preserve or build muscle.
The challenge: Ozempic dramatically reduces appetite, making adequate protein consumption difficult. Strategies include:
Prioritizing protein: When eating capacity is limited, prioritize protein-rich foods before other macronutrients.
Protein supplementation: Shakes and supplements help reach targets when whole food intake is limited.
Spreading intake: Multiple smaller protein portions throughout the day may be easier than large meals.
Timing around training: For those exercising, protein around workouts supports muscle protein synthesis.
Resistance training: Non-negotiable for muscle
Peptides can support muscle preservation, but they can't replace resistance training. Exercise provides the stimulus that tells the body to maintain muscle tissue rather than catabolizing it.
Recommendations for Ozempic users:
Frequency: At minimum, 2-3 resistance training sessions weekly.
Intensity: Moderate to challenging weights that fatigue muscles within 8-12 repetitions.
Progression: Gradually increasing weight or difficulty over time.
Compound movements: Exercises that work multiple muscle groups maximize efficiency.
Peptides for muscle growth complement this training but don't replace it.
Sleep and recovery
Growth hormone releases primarily during deep sleep. This makes sleep quality particularly relevant for anyone using GH secretagogues like Ipamorelin and CJC-1295.
Optimizing sleep while on Ozempic and peptides:
Consistent schedule: Regular sleep and wake times support circadian rhythm and GH release patterns.
GH secretagogue timing: Administering Ipamorelin/CJC-1295 shortly before bed aligns with natural GH peaks during early sleep.
Sleep environment: Dark, cool, quiet environments promote deeper sleep phases when GH release peaks.
Avoiding late eating: Empty stomach optimizes GH secretagogue effects, and late eating can disrupt sleep quality.
Hydration and micronutrients
Reduced food intake on Ozempic can create micronutrient deficiencies. Key nutrients for healing and muscle health include:
Vitamin D: Supports muscle function and immune health.
Zinc: Essential for tissue repair and protein synthesis.
Magnesium: Supports muscle function and sleep quality.
B vitamins: Support energy metabolism and protein utilization.
A comprehensive multivitamin and targeted supplementation may help address gaps from reduced food intake.
Monitoring and measuring results
Tracking outcomes helps optimize protocols and confirm that peptide additions are providing value.
Body composition metrics
For muscle preservation, body composition matters more than weight alone. Tracking methods include:
DEXA scans: The gold standard for measuring fat mass versus lean mass. Periodic scans (every 2-3 months) track body composition changes during Ozempic therapy.
Bioelectrical impedance: Less accurate than DEXA but more accessible. Many scales include this feature.
Circumference measurements: Waist, hip, arm, and thigh measurements track where changes occur.
Strength metrics: If strength is maintained or increasing despite weight loss, muscle preservation is likely successful.
Healing indicators
For injury healing, tracking is more subjective but still valuable:
Pain levels: Rating pain on a 1-10 scale before, during, and after peptide protocols.
Function: Tracking what activities are possible, what range of motion exists, what limitations persist.
Recovery time: Noting how quickly soreness resolves after activity.
Imaging: For significant injuries, follow-up imaging can document structural changes.
Peptide before and after tracking helps document progress objectively.
Blood work monitoring
Periodic blood work helps ensure safety and optimize protocols:
IGF-1: Reflects growth hormone status. Helps confirm GH secretagogues are working and levels aren't excessive.
Glucose and HbA1c: Monitors blood sugar, particularly important given Ozempic's diabetes-related uses and GH's glucose-raising effects.
Liver and kidney function: General safety monitoring when using multiple compounds.
Hormone panels: Tracks testosterone, thyroid, and other hormones that can shift with body composition changes.
Common questions about peptides and Ozempic
Can BPC-157 help with Ozempic side effects?
Some theorize that BPC-157's gut-protective properties might help with gastrointestinal side effects common on GLP-1 agonists. The peptide was originally isolated from gastric juice and demonstrates protective effects on digestive tissue in animal studies.
However, no formal research examines this specific application. The theory is plausible given BPC-157's mechanisms, but remains unproven. Those experiencing significant GI side effects should first discuss dosage adjustment and standard management strategies with their prescribing provider.
Will GH secretagogues interfere with Ozempic's weight loss effects?
Growth hormone secretagogues shouldn't interfere with semaglutide's primary mechanisms. GLP-1 agonists work through GLP-1 receptors affecting appetite and glucose metabolism. GH secretagogues work through ghrelin and GHRH receptors affecting growth hormone release.
GH itself is actually lipolytic, meaning it promotes fat breakdown. This could theoretically complement rather than counteract weight loss. The goal of adding GH secretagogues is shifting the weight loss composition toward fat loss and away from muscle loss, not preventing weight loss.
That said, individual responses vary, and monitoring results helps ensure the combination works as intended.
How long should I wait after starting Ozempic to add peptides?
No formal guidance exists. Reasonable approaches include:
Stabilization approach: Wait until Ozempic dose is titrated to maintenance level and side effects have stabilized, typically 4-8 weeks. This allows attributing any new effects to the peptides rather than ongoing Ozempic adjustment.
Concurrent approach: Some add healing peptides immediately if dealing with active injuries, reasoning that healing support is needed now.
Delayed approach: Add muscle preservation peptides after several months when muscle loss becomes apparent on body composition testing.
Medical supervision helps determine the most appropriate timing for individual situations.
Are there peptides I should avoid while on Ozempic?
No peptides are specifically contraindicated with semaglutide based on mechanism conflicts. However, certain peptide categories warrant extra consideration:
Appetite-stimulating peptides: GHRP-6 and similar secretagogues that increase hunger might counteract Ozempic's appetite suppression. Ipamorelin is preferred partly because it doesn't significantly affect appetite.
Glucose-affecting peptides: GH secretagogues can raise blood sugar. For diabetic Ozempic users specifically, close glucose monitoring is warranted when adding these compounds.
Untested combinations: Novel or less-researched peptides lack even the limited safety information available for established compounds. Sticking to well-known options like BPC-157, TB-500, and Ipamorelin is more conservative.
Sourcing quality peptides
Product quality matters significantly for peptide outcomes. The unregulated research chemical market varies enormously in reliability.
Quality indicators
Third-party testing: Reputable vendors provide independent laboratory analysis verifying peptide identity and purity. The testing documentation guide explains how to interpret these results.
Certificate of Analysis: Each batch should have documentation of testing results, including purity percentage and absence of contaminants.
Proper packaging: Lyophilized peptides should arrive in sealed vials with appropriate labeling, stored and shipped with temperature controls when needed.
Vendor reputation: Community feedback from experienced users helps identify reliable sources. Peptide vendor reviews compile this information.
Research vs pharmaceutical grade
Research vs pharmaceutical peptides differ in regulatory oversight and quality assurance. Pharmaceutical-grade peptides come from licensed facilities with strict quality controls. Research-grade peptides vary more in quality.
For Ozempic users adding peptides, the quality consideration becomes particularly important. You're combining regulated medication with unregulated compounds, and poor-quality peptides could introduce unknown variables.
Medical channels often provide access to higher-quality peptides, which is another reason professional supervision makes sense for these combinations.
Alternative approaches to consider
Peptides aren't the only option for addressing healing and muscle preservation while on Ozempic. Alternative approaches deserve consideration.
Adjusting Ozempic dosing
Some providers reduce semaglutide dosing when muscle loss becomes concerning. Lower doses may still provide appetite suppression and weight loss while allowing more food intake and potentially less muscle catabolism.
This approach trades some weight loss speed for better body composition. The semaglutide dosage calculator helps understand different dosing levels.
Tirzepatide as an alternative
Tirzepatide (Mounjaro, Zepbound) is a dual GIP/GLP-1 agonist that some research suggests may preserve muscle better than semaglutide. Early data showed potentially better body composition outcomes, though more research is needed.
Switching GLP-1 medications is a conversation for your prescribing provider, but tirzepatide represents an option worth discussing if muscle preservation is a primary concern.
Creatine supplementation
Creatine is one of the most researched and effective supplements for muscle preservation and performance. It requires no injection, has excellent safety data, and is widely available.
For Ozempic users not ready to explore peptides, creatine supplementation combined with resistance training offers an accessible starting point for muscle preservation.
Physical therapy for injuries
Peptides may accelerate healing, but they don't replace proper rehabilitation. Physical therapy addresses movement patterns, strengthens supporting structures, and guides progressive loading during recovery.
The best outcomes likely combine appropriate rehabilitation with peptide support when needed, not peptides alone.
Helpful resources
These foundational tools and guides support peptide education and protocol planning:
May your healing stay accelerated, your muscle stay preserved, and your weight loss journey stay successful. Join SeekPeptides.