Mar 1, 2026

You are about to draw your first dose of tirzepatide. The vial says 2.5 mg. Your syringe measures in milliliters. And right now, staring at that tiny insulin syringe, you have no idea how much liquid to pull.
This is not a small problem.
Drawing the wrong volume means getting the wrong dose. Too little and you waste weeks waiting for results that never come. Too much and you invite nausea, vomiting, and side effects that could have been avoided entirely. The answer to "how many mL is 2.5 mg of tirzepatide" depends on one critical variable that most guides gloss over, and that is the concentration of your specific vial. A 2.5 mg dose from a 5 mg/mL vial requires 0.5 mL. That same 2.5 mg dose from a 10 mg/mL vial requires only 0.25 mL. Get the concentration wrong and every single injection you draw from that vial will be off. This guide breaks down the exact mL volume for 2.5 mg of tirzepatide across every common concentration, covers every syringe type you might use, and walks through the math so you never have to guess. Whether you are working with compounded tirzepatide from a pharmacy or brand-name Mounjaro or Zepbound pens, you will know exactly how much to draw by the time you finish reading. SeekPeptides created this reference because dosing errors are the single most common mistake new users make, and they are completely preventable with the right information.
Why the answer changes based on concentration
Here is the fundamental truth about tirzepatide dosing that trips people up. Milligrams measure the amount of medication. Milliliters measure the volume of liquid. These are not the same thing.
Think of it like salt in water. You can dissolve one teaspoon of salt in a small glass or a large pitcher. The amount of salt is identical. The volume of liquid is completely different. Tirzepatide concentration works the same way.
When a vial reads "10 mg/mL," that means every single milliliter of liquid contains 10 milligrams of tirzepatide. When another vial reads "5 mg/mL," each milliliter holds only 5 milligrams. To get 2.5 mg from the first vial, you need 0.25 mL. To get 2.5 mg from the second, you need twice as much liquid, which is 0.5 mL. Same dose, different volumes. This is why checking your vial label before every injection is not optional. It is the single most important step in the entire dosing process.
Compounded tirzepatide comes in multiple concentrations because different pharmacies prepare it differently. The most common concentrations you will encounter are 5 mg/mL, 10 mg/mL, 15 mg/mL, and 20 mg/mL. Some pharmacies even compound at 25 mg/mL or higher. Each requires a different volume to deliver the same 2.5 mg starting dose, and mixing them up is easier than you think, especially if you switch pharmacies or receive a different batch.
The complete 2.5 mg conversion table
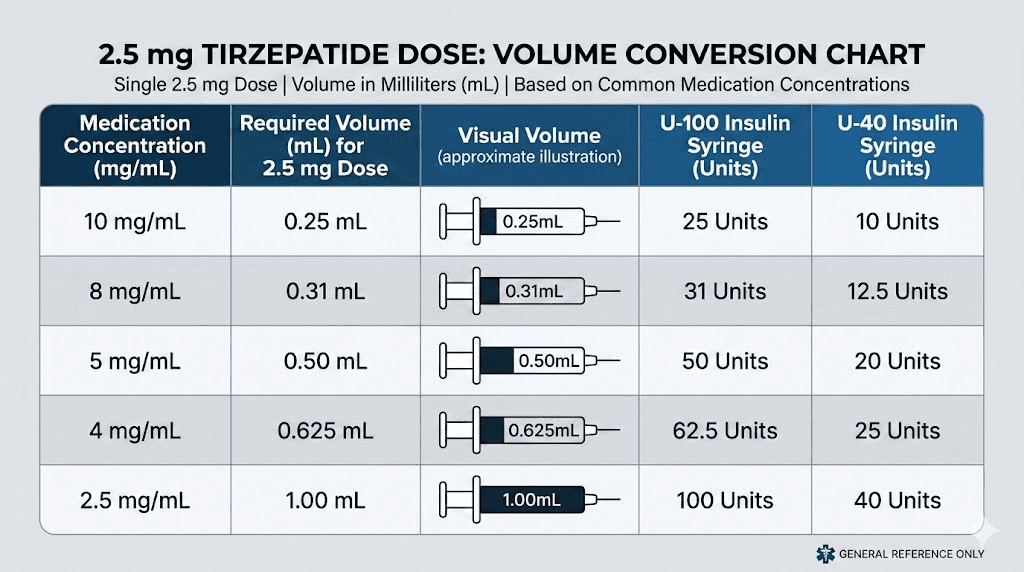
This is the reference table you will want to bookmark. It shows the exact mL volume needed for a 2.5 mg dose of tirzepatide at every standard concentration.
Concentration | Volume for 2.5 mg | Units on insulin syringe | Common vial sizes |
|---|---|---|---|
2.5 mg/0.5 mL | 0.50 mL | 50 units | Brand pens (Mounjaro/Zepbound) |
5 mg/mL | 0.50 mL | 50 units | 10 mg, 15 mg vials |
10 mg/mL | 0.25 mL | 25 units | 30 mg, 60 mg vials |
15 mg/mL | 0.167 mL | ~17 units | 30 mg, 45 mg vials |
20 mg/mL | 0.125 mL | 12.5 units | 60 mg vials |
25 mg/mL | 0.10 mL | 10 units | 50 mg vials |
Notice how dramatically the volume changes. At 5 mg/mL, you draw half a milliliter. At 25 mg/mL, you draw just one-tenth of a milliliter. That is a five-fold difference in volume for the exact same dose. If you used the 5 mg/mL volume with a 25 mg/mL concentration, you would inject 12.5 mg instead of 2.5 mg. That is five times the intended dose. This is exactly why dosage charts in mL must always specify the concentration they are referencing.
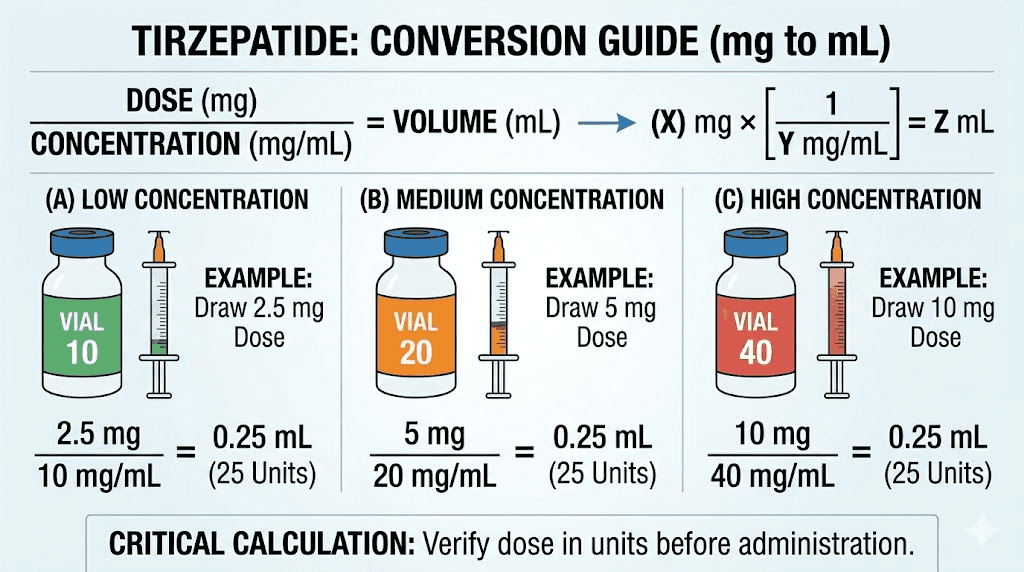
The formula behind every number in that table is simple. Volume in mL equals desired dose in mg divided by concentration in mg per mL. For 2.5 mg at 10 mg/mL, that is 2.5 divided by 10, which equals 0.25 mL. You can use this formula for any dose at any concentration, and our peptide calculator automates this math entirely.
Brand-name pen volumes
If you are using brand-name Mounjaro or Zepbound, the math is already done for you. Each pen delivers a fixed dose at a fixed volume. The 2.5 mg single-dose pens contain 0.5 mL of solution at a concentration of 5 mg/mL. You press the button and the pen delivers the entire contents. No measuring required.
The multi-dose KwikPen format delivers 2.5 mg in 0.6 mL of solution, using a slightly different concentration. These pens are pre-calibrated, so you dial the dose and inject. No syringes, no conversion math, no room for error. But they are significantly more expensive than compounded alternatives, which is why many people transition to vials.
Compounded vial volumes
Compounded tirzepatide is where the conversion math becomes critical. Unlike brand-name pens, compounded vials require you to draw the correct volume manually using an insulin syringe. The concentration varies by pharmacy, and sometimes even between batches from the same pharmacy.
The most popular compounded vial is the 30 mg vial. When reconstituted with 3 mL of bacteriostatic water, this creates a 10 mg/mL concentration. At that concentration, 2.5 mg equals exactly 0.25 mL, which is 25 units on an insulin syringe. Clean math. Easy to draw.
But some pharmacies ship pre-mixed liquid vials at different concentrations. A 60 mg vial in 3 mL gives you 20 mg/mL. Now 2.5 mg is only 0.125 mL, or 12.5 units. That is a tiny volume that demands a precise syringe, and rounding errors become much more significant at smaller volumes.
Understanding insulin syringe units
If you have never used an insulin syringe before, the unit markings can feel confusing. Here is the key relationship you need to memorize. On a standard U-100 insulin syringe, 100 units equals 1 mL. That means 50 units equals 0.5 mL. And 25 units equals 0.25 mL.
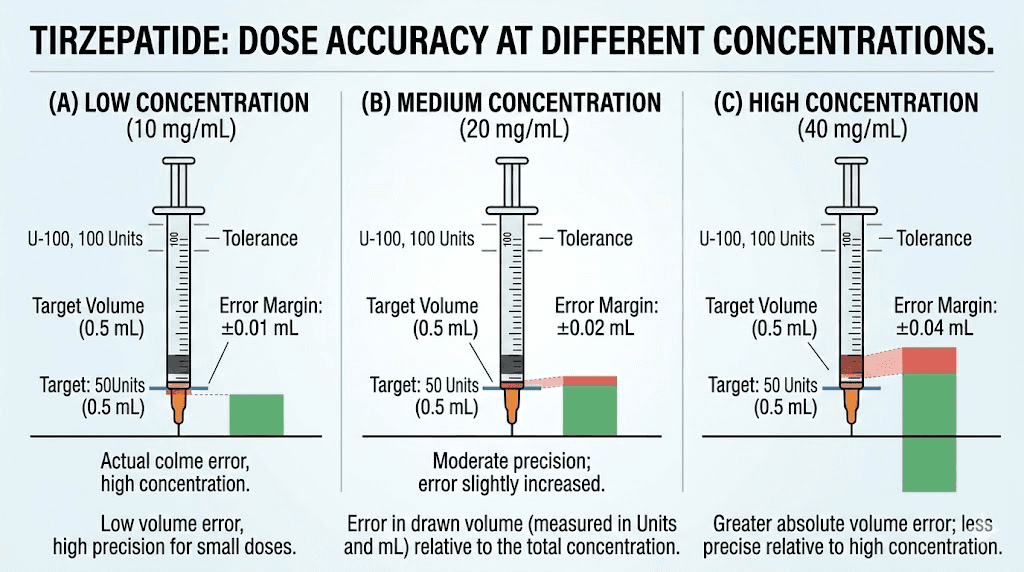
Every line on the syringe represents a specific fraction of a milliliter. On a 1 mL (100-unit) syringe, each small line typically represents 2 units or 0.02 mL. On a 0.5 mL (50-unit) syringe, each small line represents 1 unit or 0.01 mL. On a 0.3 mL (30-unit) syringe, each line represents 0.5 units or 0.005 mL.
For tirzepatide dosing, smaller syringes generally provide better accuracy. When your target volume is 0.25 mL (25 units), a 0.3 mL syringe gives you much finer graduation marks than a full 1 mL syringe. That precision matters because even a small error at these volumes translates to a meaningful dose difference.
Which syringe size to use for 2.5 mg
Your syringe selection should match your target volume. Here is a practical guide.
Concentration | Volume needed | Best syringe size | Why |
|---|---|---|---|
5 mg/mL | 0.50 mL (50 units) | 1 mL or 0.5 mL syringe | Volume fits comfortably |
10 mg/mL | 0.25 mL (25 units) | 0.3 mL (30-unit) syringe | Best precision for this volume |
15 mg/mL | 0.167 mL (~17 units) | 0.3 mL (30-unit) syringe | Fine graduations needed |
20 mg/mL | 0.125 mL (12.5 units) | 0.3 mL (30-unit) syringe | Tiny volume requires precision |
The 0.3 mL (30-unit) syringe with half-unit markings is the gold standard for compounded tirzepatide dosing. Every half-unit line represents 0.005 mL, giving you the precision needed for accurate dosing at higher concentrations. If your pharmacy or supplier offers these, use them. The difference between a 25-unit dose and a 27-unit dose might seem trivial, but over 12 weeks of injections, those small errors compound into meaningful dose variations. For more details on converting 2.5 mg to units, see our dedicated conversion guide.
Reading the syringe correctly
Hold the syringe at eye level with the needle pointing up. The plunger creates a slight curve where the liquid meets the barrel. This curve is called the meniscus. Always read the measurement at the bottom of the meniscus, not the top of the curve. Reading at the top adds approximately 0.5 to 1 unit of error, which at small volumes can shift your dose by 5 to 10 percent.
After drawing your dose, tap the syringe gently to move any air bubbles to the top, then push the plunger up just enough to expel the air without losing liquid. Air bubbles do not cause harm with subcutaneous injections, but they do displace liquid and reduce the actual volume you inject. A large bubble in a 25-unit draw could mean you only deliver 22 or 23 units of actual medication.
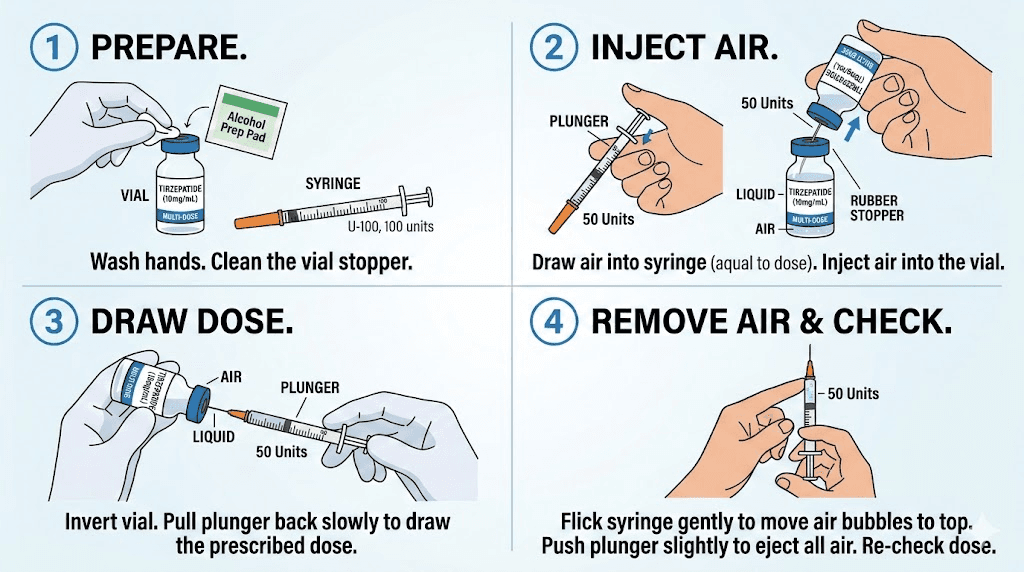
Step-by-step guide to drawing 2.5 mg
Whether this is your first injection or your fiftieth, following a consistent process prevents errors. Here is the exact sequence for drawing 2.5 mg of compounded tirzepatide from a vial.
Before you start
Gather your supplies. You need the tirzepatide vial, an alcohol swab, your insulin syringe, and a sharps container. Check the vial label and confirm the concentration. Write down the target volume. For a 10 mg/mL vial, your target is 0.25 mL or 25 units. For a 5 mg/mL vial, your target is 0.50 mL or 50 units.
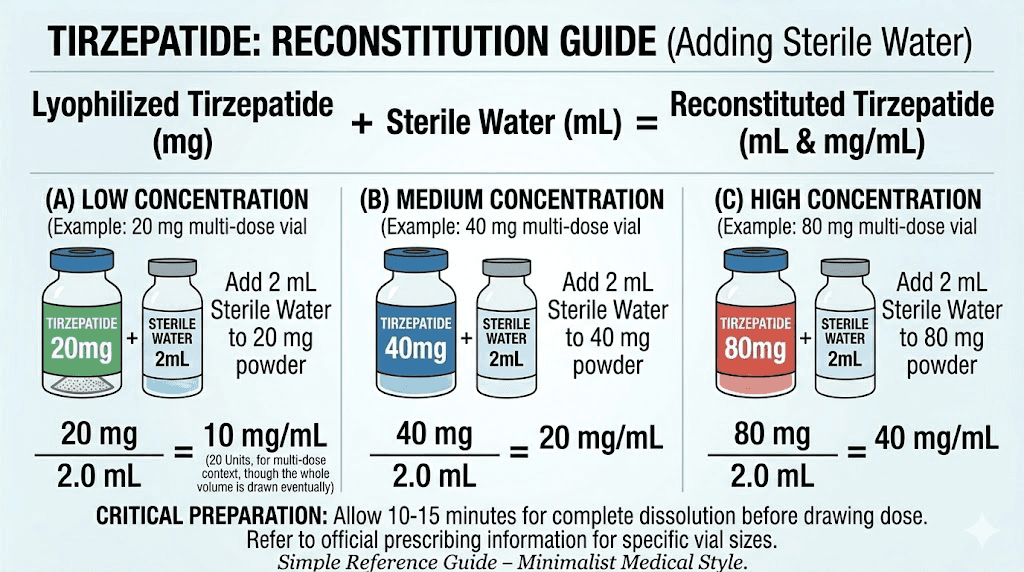
If your vial contains lyophilized (freeze-dried) tirzepatide, you need to reconstitute it first. This means adding bacteriostatic water to the powder to create your injectable solution. The amount of water you add determines the concentration, which determines how much you draw for each dose. Our reconstitution chart PDF covers every vial size.
The drawing process
Clean the top of the vial with an alcohol swab and let it dry for 10 seconds. Pull the plunger on your syringe back to your target volume, filling the barrel with air. Insert the needle through the rubber stopper and push the air into the vial. This equalizes pressure and makes drawing liquid easier.
Flip the vial upside down with the syringe still inserted. Pull the plunger slowly past your target mark. You want to overdraw slightly. Then push the plunger back to exactly your target line, which forces any air bubbles back into the vial. Check for remaining bubbles. Tap them to the top and push them out. Confirm your final volume one last time at eye level.
Remove the needle from the vial. Do not touch the needle to anything. Do not recap it by pushing the cap onto the needle, instead use a one-handed scoop technique if you need to temporarily cap it. Proceed to your injection site immediately.
Common drawing mistakes
The most frequent error is not checking the concentration before drawing. This sounds obvious, but when you are in a routine and have been drawing from the same vial for weeks, it is easy to grab a new vial with a different concentration and draw the same volume out of habit. Always read the label.
The second most common mistake is leaving large air bubbles in the syringe. One bubble that takes up 3 units of space in a 25-unit draw means you are only injecting 22 units of medication. That is a 12 percent reduction in your dose. Over four weeks, you have effectively skipped half a dose without realizing it.
Third, some people push the needle through the stopper at an angle, which can core the rubber and leave small particles in the solution. Insert the needle straight through the center of the stopper at a 90-degree angle. Use a new needle for each draw if possible. If you are drawing multiple doses from the same vial over several weeks, inspect the stopper for signs of coring after each use.
Concentration-specific breakdowns
Each concentration deserves its own detailed explanation because the practical considerations differ significantly. What works perfectly at 5 mg/mL can cause problems at 20 mg/mL, and vice versa.
5 mg/mL concentration
At 5 mg/mL, your 2.5 mg dose requires 0.50 mL, which is 50 units on an insulin syringe. This is the most forgiving concentration for beginners because the volume is large enough to measure accurately with almost any syringe size, including the standard 1 mL syringes that most pharmacies dispense by default.
The downside is that your vial runs out faster. A 10 mg vial at 5 mg/mL contains only 2 mL of solution, giving you four 2.5 mg doses. A 15 mg vial at 5 mg/mL gives you 3 mL and six doses. If you are on a standard escalation schedule starting at 2.5 mg weekly, a 10 mg vial lasts exactly one month.
This concentration commonly comes from pharmacies that prepare tirzepatide for patients on lower doses. It is also the concentration you get if you reconstitute a 10 mg lyophilized vial with 2 mL of bacteriostatic water, or a 15 mg vial with 3 mL.
10 mg/mL concentration
This is the most popular concentration for compounded tirzepatide and the one you will most likely encounter. At 10 mg/mL, 2.5 mg equals 0.25 mL or 25 units. The math is clean, the volume is manageable, and a 30 mg vial gives you twelve 2.5 mg doses, lasting three months at the starting dose.
The standard reconstitution for this concentration is adding 3 mL of bacteriostatic water to a 30 mg vial. This is the setup that most online guides and dosage calculators assume when they list unit conversions. If someone tells you "25 units for your starting dose" without specifying the concentration, they are almost certainly referring to 10 mg/mL.
At this concentration, a 0.3 mL (30-unit) syringe is ideal. The 25-unit mark falls comfortably on the scale, and you have enough resolution between lines to draw with confidence. A 0.5 mL syringe also works well. Avoid using a full 1 mL syringe for this volume because the graduation marks are too far apart for precise measurement at 0.25 mL.
15 mg/mL concentration
At 15 mg/mL, 2.5 mg requires approximately 0.167 mL, which is about 16.7 units. This is where dosing starts to get tricky because 16.7 units does not land cleanly on most syringe markings. You will need to estimate between the 16 and 17 unit lines.
On a 0.3 mL syringe with half-unit markings, you would draw to the line halfway between 16.5 and 17. On a standard syringe with only whole-unit markings, you would draw to between 16 and 17, accepting a small margin of error. This margin is approximately plus or minus 0.3 mg, which is clinically insignificant at the 2.5 mg starting dose but worth being aware of.
This concentration results from adding 2 mL of bacteriostatic water to a 30 mg vial, or 3 mL to a 45 mg vial. Some pharmacies ship pre-mixed liquid at this concentration. It is less common than 10 mg/mL but not unusual.
20 mg/mL concentration
At 20 mg/mL, your 2.5 mg dose is only 0.125 mL, which is 12.5 units. This tiny volume requires the most precise technique of all common concentrations. You are drawing less than one-eighth of a milliliter, where even a one-unit error represents an 8 percent dose change.
Half-unit syringes are not optional at this concentration. They are necessary. Without half-unit markings, you cannot reliably distinguish between 12 and 13 units, which represents the difference between 2.4 mg and 2.6 mg. Some clinicians recommend a different approach entirely at this concentration, which is to reconstitute with more water to reduce the concentration and increase the draw volume.
If you have a 60 mg vial at 20 mg/mL, consider whether the math works better at a lower concentration. Adding bacteriostatic water to dilute from 20 mg/mL to 10 mg/mL would double your draw volume and make dosing significantly easier. Discuss this option with your prescriber.
Brand-name pens versus compounded vials
The volume conversation only matters if you are drawing from a vial. But understanding the difference between delivery methods helps you make an informed decision about which format works best for your situation.
Mounjaro and Zepbound pens
Both Mounjaro (for type 2 diabetes) and Zepbound (for weight management) deliver tirzepatide through pre-filled single-dose pens. The 2.5 mg pen contains 0.5 mL of solution at 5 mg/mL. You uncap the pen, place it against your skin, press the button, and the mechanism delivers the full dose. There is nothing to measure, nothing to calculate, and virtually no room for error.
The advantage is simplicity. The disadvantage is cost. Brand-name tirzepatide without insurance typically runs significantly more per month than compounded alternatives, which is why many people who start on brand-name pens eventually transition to compounded tirzepatide once they are comfortable with the injection process.
If you are currently using pens and considering a switch to vials, the 2.5 mg dose is actually the easiest time to make that transition. The volume is small, the starting dose is low enough that minor measurement variations have minimal clinical impact, and you get to practice drawing technique before moving to higher doses where precision matters more.
Compounded tirzepatide vials
Compounded tirzepatide comes in two main forms. Lyophilized (freeze-dried) powder that you reconstitute yourself, and pre-mixed liquid that is ready to inject. Both ultimately deliver the same medication, but the preparation process differs.
With lyophilized powder, you control the final concentration by choosing how much bacteriostatic water to add. This gives you flexibility. A 10 mg vial can become 5 mg/mL (add 2 mL water), 10 mg/mL (add 1 mL water), or any other concentration you choose. Most people add enough water to create a 10 mg/mL concentration because the resulting volumes are easy to measure accurately.
Pre-mixed liquid vials arrive ready to use. The concentration is fixed by the pharmacy. You need to check the label, identify the mg/mL, and calculate your draw volume accordingly. These are more convenient because you skip the reconstitution step, but you lose the ability to adjust the concentration.
The math behind every conversion
Understanding the formula means you never need to rely on a chart. You can calculate any dose at any concentration in seconds.
The universal formula
Volume (mL) = Dose (mg) / Concentration (mg/mL)
That is the entire equation. Three variables, one division. For 2.5 mg at 10 mg/mL, the calculation is 2.5 divided by 10, which equals 0.25 mL. For 2.5 mg at 5 mg/mL, the calculation is 2.5 divided by 5, which equals 0.50 mL.
To convert mL to insulin syringe units, multiply by 100. So 0.25 mL times 100 equals 25 units. And 0.50 mL times 100 equals 50 units. This works because U-100 insulin syringes have 100 units per milliliter by definition.
Working backwards from units
Sometimes you know the units and need the milligrams. The reverse formula handles that. Dose (mg) = Units / 100 x Concentration (mg/mL). If you drew 25 units from a 10 mg/mL vial, your dose is 25 divided by 100 times 10, which equals 2.5 mg. This is useful for double-checking your work or when someone gives you dosing instructions in units without specifying the dose in milligrams.
For any tirzepatide unit conversion, this formula works regardless of the concentration. And our peptide reconstitution calculator runs these calculations automatically if you prefer to skip the math entirely.
Converting between different concentrations
What if you switch pharmacies and your new vial has a different concentration? You need to recalculate your draw volume. Do not assume the same number of units gives you the same dose.
Example scenario. You were drawing 25 units from a 10 mg/mL vial (2.5 mg). Your new vial is 20 mg/mL. If you draw 25 units from the new vial, you are injecting 5 mg, which is double your intended dose.
The correct calculation for the new vial is 2.5 divided by 20, which equals 0.125 mL or 12.5 units. Every time you receive a new vial, check the concentration, recalculate your volume, and if possible, verify with the tirzepatide conversion chart before your first draw from that vial.
Full dosage escalation in mL
The standard tirzepatide escalation protocol starts at 2.5 mg and increases every four weeks. Seeing the full schedule in mL at your specific concentration helps you plan ahead and know what to expect as your dose increases.
Escalation at 10 mg/mL (most common)
Weeks | Dose | Volume (mL) | Units |
|---|---|---|---|
Weeks 1-4 | 2.5 mg | 0.25 mL | 25 units |
Weeks 5-8 | 5.0 mg | 0.50 mL | 50 units |
Weeks 9-12 | 7.5 mg | 0.75 mL | 75 units |
Weeks 13-16 | 10.0 mg | 1.00 mL | 100 units |
Weeks 17-20 | 12.5 mg | 1.25 mL | N/A (use TB syringe) |
Weeks 21+ | 15.0 mg | 1.50 mL | N/A (use TB syringe) |
Notice that at 10 mg/mL, doses above 10 mg exceed the 1 mL capacity of a standard insulin syringe. At 12.5 mg and 15 mg, you either need to split the injection into two draws or switch to a 3 mL tuberculin (TB) syringe. Some people choose to use a higher concentration vial for these larger doses to keep the volume manageable. A 20 mg/mL concentration brings the 15 mg dose down to 0.75 mL, which fits comfortably in an insulin syringe.
Escalation at 5 mg/mL
Weeks | Dose | Volume (mL) | Units |
|---|---|---|---|
Weeks 1-4 | 2.5 mg | 0.50 mL | 50 units |
Weeks 5-8 | 5.0 mg | 1.00 mL | 100 units |
Weeks 9-12 | 7.5 mg | 1.50 mL | N/A (use TB syringe) |
Weeks 13+ | 10.0 mg | 2.00 mL | N/A (use TB syringe) |
At 5 mg/mL, you outgrow the insulin syringe by week 9. This is one reason why 10 mg/mL is the preferred concentration for most users. It keeps injection volumes manageable through the first several dose escalations. Larger volumes also mean more liquid deposited at the injection site, which can increase discomfort and injection site reactions.
Escalation at 20 mg/mL
Weeks | Dose | Volume (mL) | Units |
|---|---|---|---|
Weeks 1-4 | 2.5 mg | 0.125 mL | 12.5 units |
Weeks 5-8 | 5.0 mg | 0.25 mL | 25 units |
Weeks 9-12 | 7.5 mg | 0.375 mL | 37.5 units |
Weeks 13-16 | 10.0 mg | 0.50 mL | 50 units |
Weeks 17-20 | 12.5 mg | 0.625 mL | 62.5 units |
Weeks 21+ | 15.0 mg | 0.75 mL | 75 units |
The 20 mg/mL concentration keeps every dose within insulin syringe range. Even the maximum 15 mg dose only requires 0.75 mL. The tradeoff is precision at lower doses. That 12.5-unit starting draw is genuinely difficult to measure accurately without half-unit markings on your syringe. If you are using 20 mg/mL, invest in 0.3 mL syringes with half-unit lines. The precision is worth it.
Reconstitution and how it determines your mL
If you are working with lyophilized tirzepatide, the amount of bacteriostatic water you add directly controls how many mL you draw for every dose. This is the step where many dosing errors actually originate, long before the syringe comes into play.
Common vial sizes and water volumes
Vial size | Water added | Final concentration | mL for 2.5 mg |
|---|---|---|---|
5 mg | 1 mL | 5 mg/mL | 0.50 mL |
10 mg | 1 mL | 10 mg/mL | 0.25 mL |
10 mg | 2 mL | 5 mg/mL | 0.50 mL |
15 mg | 1.5 mL | 10 mg/mL | 0.25 mL |
15 mg | 3 mL | 5 mg/mL | 0.50 mL |
30 mg | 3 mL | 10 mg/mL | 0.25 mL |
30 mg | 2 mL | 15 mg/mL | 0.167 mL |
60 mg | 3 mL | 20 mg/mL | 0.125 mL |
60 mg | 6 mL | 10 mg/mL | 0.25 mL |
The sweet spot for most people is creating a 10 mg/mL concentration. This provides clean math for every standard dose, keeps volumes within insulin syringe range through 10 mg, and gives the reconstituted solution enough volume to remain stable for the life of the vial. Adding too little water concentrates the solution and makes accurate dosing harder. Adding too much dilutes it and increases injection volume unnecessarily.
The reconstitution process
Wipe the tops of both the tirzepatide vial and the bacteriostatic water vial with alcohol swabs. Using a fresh syringe (a 3 mL syringe works best for this step), draw your planned volume of bacteriostatic water. Insert the needle into the tirzepatide vial and inject the water slowly along the inside wall of the vial. Do not shoot the water directly into the powder, as this can damage the peptide.
Gently swirl the vial. Do not shake it. Shaking creates air bubbles and can denature the protein. The powder should dissolve within 30 to 60 seconds of gentle swirling. If particles remain after two minutes, continue swirling. The resulting solution should be clear and colorless. If it appears cloudy, contains visible particles that do not dissolve, or has changed color, do not use it.
Label the vial with the date you reconstituted it and the concentration. This prevents confusion later, especially if you have multiple vials. Store the reconstituted vial in the refrigerator at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). Most reconstituted tirzepatide remains stable for 28 to 60 days when properly refrigerated.
What if you do not know your concentration
This situation happens more often than you might think. A vial arrives from the pharmacy without a clear concentration label. Or the label shows the total vial content (30 mg) and the total volume (3 mL) but does not explicitly state the concentration per mL. Or you reconstituted the vial yourself but did not write down how much water you added.
How to determine your concentration
If the vial label shows total mg and total mL, divide the first by the second. A label reading "tirzepatide 30 mg / 3 mL" means 30 divided by 3, which equals 10 mg/mL. A label reading "tirzepatide 60 mg / 6 mL" means 60 divided by 6, which also equals 10 mg/mL.
If you reconstituted the vial yourself and cannot remember the water volume, measure the total liquid in the vial. Draw it all out with a large syringe, note the volume, and divide the total mg by that volume. If you started with a 30 mg vial and measure 3.2 mL of liquid (the extra 0.2 mL comes from the powder displacing some volume), your concentration is approximately 30 divided by 3.2, which is about 9.4 mg/mL. Round to the nearest practical concentration and dose accordingly.
If you truly cannot determine the concentration, do not inject. Contact your pharmacy. Ask them to confirm the concentration. Using an unknown concentration is the single most dangerous dosing error you can make, because you have no way to calculate the correct volume.
Microdosing considerations at 2.5 mg
Some practitioners recommend starting below the standard 2.5 mg dose, particularly for people who are sensitive to GLP-1 medications or have experienced significant side effects with other peptides in this class. This approach, often called microdosing tirzepatide, involves taking half or even a quarter of the 2.5 mg starting dose.
Volumes for sub-2.5 mg doses
Dose | At 5 mg/mL | At 10 mg/mL | At 20 mg/mL |
|---|---|---|---|
0.625 mg (quarter dose) | 0.125 mL (12.5 units) | 0.0625 mL (6.25 units) | 0.03125 mL (~3 units) |
1.0 mg | 0.20 mL (20 units) | 0.10 mL (10 units) | 0.05 mL (5 units) |
1.25 mg (half dose) | 0.25 mL (25 units) | 0.125 mL (12.5 units) | 0.0625 mL (~6 units) |
At these tiny volumes, precision becomes extremely difficult with higher concentrations. If you are microdosing at 1.25 mg with a 20 mg/mL concentration, you need to draw approximately 6 units. That is a razor-thin margin for error. Most clinicians recommend using a 5 mg/mL concentration for microdosing because the larger volumes (25 units for 1.25 mg) are far easier to measure accurately.
Some people also split their tirzepatide dose into two injections per week rather than one. A 2.5 mg weekly dose split into two 1.25 mg doses means injecting twice per week at half the volume. This approach can reduce GI side effects for sensitive individuals, though it has not been studied in clinical trials specifically for tirzepatide.
Injection technique for small volumes
Drawing 0.25 mL or less requires slightly different technique than larger volume injections. The smaller the volume, the more every detail matters.
Injection site selection
The three approved injection sites for tirzepatide are the abdomen, thigh, and upper arm. For the 2.5 mg starting dose, any site works well because the volume is small. Most people start with the abdomen because abdominal injections tend to absorb more consistently and cause less discomfort than thigh injections.
Rotate your injection sites weekly to prevent injection site reactions and lipodystrophy. If you inject in the abdomen this week, switch to the thigh next week, then the upper arm, then back to the abdomen. Also rotate within each area. Do not inject in the exact same spot repeatedly. Space each injection at least one inch from the previous site.
The pinch and inject method
For subcutaneous injection, pinch a fold of skin between your thumb and forefinger. Insert the needle at a 90-degree angle into the pinched skin. Push the plunger slowly and steadily. After the plunger is fully depressed, count to five before withdrawing the needle. This pause allows the small volume of medication to deposit fully into the tissue rather than tracking back along the needle path.
At volumes below 0.25 mL, the injection is so small that you may not even feel the liquid entering. This is normal. Do not assume the injection failed because you did not feel anything. If the plunger went down and the syringe is empty, the dose was delivered.
Dealing with injection site reactions
Some people experience redness, swelling, or itching at the injection site. These reactions are more common at higher doses but can occur at 2.5 mg as well. They typically resolve within a few days. Applying a cold compress after injection can reduce discomfort. If reactions persist or worsen, consult your prescriber.
The volume of liquid injected does affect site reaction severity. Larger volumes create more tissue displacement and higher local drug concentrations, both of which can trigger inflammation. This is another advantage of higher concentration formulations. Injecting 0.25 mL creates less local irritation than injecting 0.50 mL of the same medication.
Storage and its effect on dosing accuracy
Proper storage does not change the concentration, but improper storage can degrade the tirzepatide molecule, reducing its potency. When potency decreases, you are effectively getting less than 2.5 mg even if you draw the correct volume.
Temperature requirements
Reconstituted tirzepatide must stay refrigerated at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). Room temperature exposure degrades the peptide over time. Brief excursions (under two hours) are fine for drawing doses and transporting to your injection site, but leaving the vial on a countertop overnight can reduce potency.
Do not freeze tirzepatide. Freezing can damage the protein structure and render the medication ineffective. If you accidentally freeze your vial, discard it and start fresh. Similarly, heat exposure above 86 degrees Fahrenheit (30 degrees Celsius) for extended periods can degrade the solution. If you are traveling with tirzepatide, use an insulated bag with ice packs to maintain temperature.
Shelf life after reconstitution
Most compounding pharmacies recommend using reconstituted tirzepatide within 28 days, though some studies and pharmacies extend this to 60 days when stored properly. After 28 days, potency may begin to decline even with perfect refrigeration. If you are working through a large vial slowly (a 30 mg vial at 2.5 mg per week lasts 12 weeks), consider dividing the solution into smaller aliquots and storing what you do not need immediately.
Mark the reconstitution date on every vial. It is easy to lose track of time, and injecting from a vial that has been sitting in the fridge for three months means you are likely getting less active medication per dose than the math suggests.
Common questions about 2.5 mg volume
Beyond the basic conversion, several practical questions come up repeatedly when people start their tirzepatide protocol at 2.5 mg.
Can I use a regular syringe instead of an insulin syringe?
Technically yes, but it is not recommended. Standard syringes (like the 3 mL syringes used for reconstitution) have much coarser graduation marks. A 3 mL syringe might have markings every 0.1 mL, which means you cannot distinguish between 0.20 mL and 0.25 mL. That 0.05 mL difference at 10 mg/mL represents 0.5 mg, or a 20 percent dosing error. Insulin syringes are specifically designed for small volume precision and should always be used for dosing.
What if I accidentally draw too much?
If you draw slightly more than your target (say 27 units instead of 25 from a 10 mg/mL vial), push the plunger back to the correct line while the needle is still in the vial. The excess goes back into the vial. If you have already removed the needle from the vial, you can push the excess into a waste container, but this is less precise. Never push excess back through the stopper if the needle has touched anything other than the vial stopper.
Does the dead space in the needle affect my dose?
Yes. Standard insulin syringes have a small amount of "dead space" between the needle hub and the bottom of the barrel. This space holds approximately 0.01 to 0.07 mL of liquid that gets left behind after injection, depending on the needle and syringe design. At small volumes, this can represent a significant percentage of your dose.
Low dead space syringes minimize this issue. They are designed so that less than 0.01 mL remains after injection. If you are dosing at concentrations above 10 mg/mL, where volumes are tiny, low dead space syringes are worth seeking out. For the standard 25-unit draw at 10 mg/mL, standard syringes work fine because the dead space represents only about 2 to 3 percent of the total volume.
Should I warm the vial before drawing?
Some people let their vial sit at room temperature for 15 to 30 minutes before drawing, which slightly reduces the viscosity of the solution and makes drawing easier. This is fine and does not affect the concentration or dosing. Just do not leave the vial out for hours or forget to return it to the refrigerator.
Cold solution can also cause slightly more discomfort at the injection site. Room temperature injections tend to sting less. Either approach is medically acceptable.
Tirzepatide 2.5 mg in the context of the full protocol
The 2.5 mg dose is the starting point, not the destination. Understanding where it fits in the overall tirzepatide protocol helps set realistic expectations.
What 2.5 mg does in your body
At 2.5 mg, tirzepatide activates both GIP and GLP-1 receptors, slowing gastric emptying, reducing appetite, and beginning to improve insulin sensitivity. However, 2.5 mg is considered a sub-therapeutic dose for weight loss. Clinical trials used 2.5 mg as a four-week initiation period to allow the body to adjust before escalating to therapeutic doses.
Most people notice mild appetite suppression at 2.5 mg. Some notice nothing at all. This is expected and does not mean the medication is not working. The 2.5 mg phase is about letting your GI system adapt to the drug before increasing the dose. Side effects at this level are generally mild, though some people do experience fatigue, headaches, or mild GI symptoms even at the starting dose.
When to escalate
The standard protocol calls for increasing to 5.0 mg after four weeks at 2.5 mg. Some practitioners extend the 2.5 mg phase to six or eight weeks if side effects are significant, or if they prefer a more gradual titration. Others skip 2.5 mg entirely if the patient has been on semaglutide previously and is switching to tirzepatide.
The decision to escalate should be based on how you tolerate the current dose, not on a rigid timeline. If 2.5 mg causes persistent nausea or GI distress, staying at the starting dose for an extra week or two is a reasonable approach. Your prescriber should guide this decision based on your individual response. SeekPeptides members access detailed escalation protocols that account for individual tolerance factors, helping researchers optimize their titration schedule for the best balance of results and tolerability.
How long the 2.5 mg phase lasts
At one injection per week, the 2.5 mg phase lasts four weeks. That is four injections total. At 10 mg/mL, you use 1 mL of solution (four draws of 0.25 mL each) during this phase. A 30 mg vial at 10 mg/mL contains 3 mL, so the 2.5 mg phase uses only one-third of a 30 mg vial.
Planning your vial usage across the full escalation helps you order the right amount. A 30 mg vial at 10 mg/mL provides 120 mg-weeks of total capacity (30 mg total). At the standard escalation, the first four weeks use 10 mg (2.5 mg x 4 weeks) and the next four use 20 mg (5 mg x 4 weeks). So one 30 mg vial covers exactly eight weeks of the standard protocol, or the first two dose tiers.
Comparing tirzepatide 2.5 mg to semaglutide volumes
If you have previously used semaglutide, the volume differences are worth noting. Semaglutide and tirzepatide use different concentrations and different dosing scales, so the volumes are not directly comparable even though both are GLP-1 medications.
Side-by-side volume comparison
Medication | Starting dose | Common concentration | Volume | Units |
|---|---|---|---|---|
Tirzepatide | 2.5 mg | 10 mg/mL | 0.25 mL | 25 units |
Semaglutide | 0.25 mg | 5 mg/mL | 0.05 mL | 5 units |
Semaglutide | 0.25 mg | 2.5 mg/mL | 0.10 mL | 10 units |
The tirzepatide starting dose is ten times higher in milligrams than semaglutide, but the actual injection volumes are not ten times larger because the concentrations differ. At typical compounded concentrations, the tirzepatide starting injection (0.25 mL) is about 2.5 to 5 times the volume of the semaglutide starting injection (0.05 to 0.10 mL). This is relevant if you are comparing the two medications or switching between them.
The milligram numbers between tirzepatide and semaglutide are not equivalent. You cannot simply convert 2.5 mg of tirzepatide to a semaglutide dose by ratio. The conversion between the two depends on clinical equivalence, not raw milligrams, and should be determined by your prescriber.
Troubleshooting dosing problems
Even with perfect knowledge of the conversion math, practical problems arise. Here are the most common issues and how to solve them.
The solution will not draw into the syringe
This usually means you forgot to inject air into the vial first. The vacuum inside the sealed vial resists drawing liquid. Solution: remove the syringe, pull the plunger to fill the barrel with air equal to your target volume, reinsert into the vial, inject the air, then draw. If the solution still resists, the needle may be clogged or the stopper has cored. Try a new needle.
Bubbles keep appearing no matter what I do
Some bubbles are inevitable, especially in cold solutions. After drawing your dose, hold the syringe upright and tap the barrel firmly with your fingernail. The bubbles will float to the top near the needle. Push the plunger up gently to expel the air, then adjust back to your target volume. If this draws more air in, repeat the process. Two or three tap-and-push cycles usually clears all significant bubbles.
I cannot see the unit lines clearly
As volumes get smaller, reading fine graduation marks becomes harder, especially in poor lighting. Use a well-lit area with natural light. Hold the syringe at exact eye level. Some people find it helpful to use a magnifying glass for very small volumes. If your eyesight makes this consistently difficult, discuss switching to a lower concentration (which increases the volume and makes measurement easier) with your prescriber.
I am not sure if I injected the full dose
After injecting, check the syringe. The plunger should be fully depressed with no liquid remaining in the barrel. If there is liquid left, you did not inject the complete dose. This can happen if the needle was not fully inserted into the tissue, if you released the skin fold too early (which can pinch the needle and prevent flow), or if the plunger was not pushed down completely.
If some medication remained in the syringe, do not attempt a second injection to make up the difference. Accept the partial dose for this week and aim for the full dose next time. Overcompensating with an additional partial injection introduces more variables than it resolves.
My results seem inconsistent
If your appetite suppression or weight loss results fluctuate from week to week despite consistent dosing, the issue may be measurement variability. Even small differences in draw volume (23 units one week, 27 units the next) create noticeable differences in drug levels. The solution is better technique. Use the smallest syringe that fits your volume, draw in good lighting, read at eye level, and always expel bubbles before injecting.
Other factors that affect results include injection site absorption rates (the abdomen absorbs differently than the thigh), food timing around the injection, and natural variation in GI response. Not every week will feel the same even with perfect dosing.
When to ask your prescriber for help
Some dosing situations require professional guidance. Do not try to figure these out alone.
If you receive a vial with a concentration you have not used before, ask your prescriber or pharmacist to confirm the correct draw volume before your first injection. If you are not seeing expected results despite consistent dosing, a prescriber can help determine whether the issue is dosing, absorption, or expectations. If you experience significant side effects at 2.5 mg, a prescriber can advise on whether to reduce the dose, extend the titration period, or address specific symptoms.
For researchers who want comprehensive protocol support, SeekPeptides provides detailed dosing guides, calculators, and a community of experienced users who have navigated these exact questions. The platform covers everything from reconstitution to escalation schedules to side effect management, giving you the confidence to dose accurately at every stage of your protocol.
Frequently asked questions
Is 2.5 mg of tirzepatide always 0.5 mL?
No. The volume depends entirely on the concentration of your specific vial. At 5 mg/mL, 2.5 mg is 0.50 mL. At 10 mg/mL, it is 0.25 mL. At 20 mg/mL, it is only 0.125 mL. Always check the concentration label on your vial before calculating the volume. See the complete tirzepatide conversion chart for every concentration.
How many units is 2.5 mg of tirzepatide on an insulin syringe?
Again, this depends on concentration. At 10 mg/mL (the most common compounded concentration), 2.5 mg equals 25 units. At 5 mg/mL, it equals 50 units. At 20 mg/mL, it equals 12.5 units. Our detailed guide on how many units is 2.5 mg of tirzepatide covers all scenarios.
Can I draw 2.5 mg from any size vial?
Yes, as long as the vial contains at least 2.5 mg of tirzepatide. A 5 mg vial, 10 mg vial, 30 mg vial, or 60 mg vial can all provide 2.5 mg doses. The difference is how many total doses each vial provides. A 30 mg vial at 10 mg/mL gives twelve 2.5 mg doses, while a 5 mg vial gives only two. Check the compound tirzepatide dosage chart for dose counts by vial size.
What syringe do I need for 2.5 mg of tirzepatide?
A U-100 insulin syringe is recommended for all tirzepatide dosing. For concentrations of 10 mg/mL and above, use a 0.3 mL (30-unit) syringe with half-unit markings for the best precision. For 5 mg/mL concentrations, a 0.5 mL or 1 mL insulin syringe works well. Read our tirzepatide syringe guide for detailed recommendations.
Is 0.25 mL the same as 25 units?
Yes, on a U-100 insulin syringe. The conversion is straightforward because U-100 means 100 units per milliliter. So 0.25 mL times 100 equals 25 units. This applies to all U-100 syringes regardless of their total capacity.
What happens if I inject the wrong volume?
If you inject slightly more or less than intended at the 2.5 mg dose level, the clinical impact is minimal. A difference of 2 to 3 units (0.02 to 0.03 mL) at 10 mg/mL represents approximately 0.2 to 0.3 mg, which is unlikely to produce noticeable differences in efficacy or side effects. However, larger errors, such as drawing from the wrong concentration, can result in significant overdosing or underdosing. Always verify your concentration before drawing.
How do I convert my compounded tirzepatide dose to brand-name pen doses?
Compounded tirzepatide and brand-name tirzepatide contain the same active molecule. If your compounded dose is 2.5 mg, it is equivalent to the Mounjaro or Zepbound 2.5 mg pen. The milligram dose is the same, only the delivery method and cost differ.
Can I reconstitute to get exactly 0.25 mL for 2.5 mg?
To get exactly 0.25 mL for a 2.5 mg dose, you need a 10 mg/mL concentration. For a 30 mg vial, add 3 mL of bacteriostatic water. For a 10 mg vial, add 1 mL. For a 60 mg vial, add 6 mL. The reconstitution guide walks through each vial size in detail.
External resources
For researchers committed to accurate dosing and optimized protocols, SeekPeptides offers the most comprehensive tirzepatide resource available, with personalized protocol builders, dosing calculators, expert-reviewed guides, and a community of thousands navigating their own peptide journeys.
In case I do not see you, good afternoon, good evening, and good night. May your concentrations stay correct, your syringes stay precise, and your doses stay consistent.