Mar 24, 2026

You have probably heard that tirzepatide causes headaches. Maybe you have read the clinical trial data, scrolled through forums, or experienced it firsthand. A dull ache behind the eyes after your weekly injection. A tension that settles across your temples and refuses to leave. The internet is full of people describing these symptoms, and the worry is real.
But here is where it gets strange.
While some people report headaches as a side effect of tirzepatide, a growing body of research suggests that GLP-1 receptor agonists, the very class of drugs tirzepatide belongs to, might actually prevent migraines. Not just reduce them slightly. Prevent them in a meaningful, clinically significant way. One pilot study found that a GLP-1 drug cut monthly headache days nearly in half for chronic migraine sufferers. And the benefit had almost nothing to do with weight loss.
This is the paradox at the heart of tirzepatide and migraines. The same drug that might give you a headache during the first few weeks of treatment could, through entirely different mechanisms, protect your brain from the neuroinflammatory cascade that drives true migraine attacks. GLP-1 receptors sit in brain regions that regulate pain signaling. These drugs reduce CGRP, the neuropeptide that migraine medications like Aimovig specifically target. They lower intracranial pressure. They quiet inflammatory cytokines that amplify pain. The science is early but compelling, and it challenges the simple narrative that tirzepatide causes headaches and nothing more. Understanding the difference between a transient side effect and a chronic neurological condition is essential, and that distinction shapes everything that follows in this guide. SeekPeptides built this resource to help you navigate that complexity with real data, not fear.
What the clinical data actually shows about tirzepatide and headaches
Before diving into the migraine prevention research, we need to be honest about what tirzepatide actually does to people in clinical trials. The SURPASS program, the series of phase 3 trials that led to tirzepatide approval, enrolled thousands of participants across multiple studies. These trials tracked every reported adverse event, and headaches showed up consistently.
But the numbers tell a more nuanced story than the headlines suggest.
Headache rates in SURPASS trials
Across the SURPASS clinical trials, between 4% and 14% of participants reported headaches depending on the dose they received. That is a wide range, and the dose-dependent nature matters. People on lower doses experienced fewer headaches. People on higher doses experienced more. This pattern is consistent with what we see across many GLP-1 receptor agonist side effects, where the body needs time to adjust to a medication that fundamentally alters appetite signaling, gastric emptying, and metabolic function.
Here is what most articles leave out. Headaches were not even listed as a common side effect in the FDA labeling for Zepbound, the weight management version of tirzepatide. The FDA considers something a common side effect when it occurs at notably higher rates in the treatment group compared to placebo. Headaches occur in the general population at remarkably high baseline rates. Many people get headaches regardless of what medication they take. So while the raw numbers show headaches in trial participants, the signal was not strong enough relative to placebo to warrant special labeling.
This does not mean your headache is not real. It absolutely is. But it does mean the relationship between tirzepatide and headaches is more complicated than "drug causes headache."
Why headaches on tirzepatide are not usually migraines
There is a critical distinction that gets lost in online discussions. A headache is not a migraine. They share the feature of head pain, but that is roughly where the similarity ends.
A tension headache feels like a band of pressure around your head. It is uncomfortable. Annoying. But manageable. You can usually keep working, keep functioning, keep living your life with some discomfort. Most headaches reported on tirzepatide fall into this category. Dull, persistent, and usually concentrated in the first few weeks of treatment or after a dose increase.
A true migraine is a different beast entirely. Throbbing, often one-sided pain that can last hours or days. Light sensitivity so intense you need to lie in a dark room. Sound sensitivity. Nausea and sometimes vomiting. Some people experience aura, visual disturbances like flashing lights, zigzag lines, or temporary blind spots that precede the pain. Migraines are neurological events. They involve specific brain pathways, specific neurotransmitters, and specific inflammatory cascades that tension headaches simply do not.
When researchers examined the headache reports from tirzepatide trials more carefully, the vast majority were tension-type headaches. True migraines, the kind with throbbing pain and neurological symptoms, were much less common. This distinction matters enormously because the mechanisms behind each type of headache are completely different, and the potential for GLP-1 drugs to help or harm depends on which type we are discussing.
The dehydration and blood sugar connection
Most headaches that people experience on tirzepatide have straightforward, fixable causes. Two stand out above the rest.
Dehydration is the primary culprit. Tirzepatide reduces appetite significantly. When you eat less, you also tend to drink less, because a substantial portion of daily fluid intake comes from food. Soups, fruits, vegetables, even solid foods contain water that your body relies on. Cut your food intake dramatically and you create a fluid deficit without realizing it. Add to that the fact that some people experience diarrhea on tirzepatide, which accelerates fluid loss, and you have a recipe for dehydration headaches.
Low blood sugar is the second major trigger. Tirzepatide is a dual GIP and GLP-1 receptor agonist. It enhances insulin secretion in response to food. If you skip meals or eat too little, your blood sugar can dip lower than your brain is comfortable with. The brain is exquisitely sensitive to glucose levels. Even modest drops can trigger headaches, dizziness, irritability, and difficulty concentrating. People who are not diabetic rarely think about blood sugar, but on a potent appetite suppressant, it becomes relevant.
These two causes explain why GLP-1 headaches typically resolve within the first few weeks. As people learn to hydrate deliberately, eat regular small meals, and allow their bodies to adjust to the medication, the headaches fade. They are not a sign of neurological damage. They are a sign that your body is adapting to a new metabolic reality, and it needs some support during the transition.
Understanding what to eat on tirzepatide and maintaining adequate hydration are not just comfort measures. They are the foundation of headache prevention during treatment.
The emerging science: how GLP-1 drugs may prevent migraines
Now we arrive at the part of this story that genuinely surprises most people. The very drugs that can cause transient headaches might hold the key to preventing one of the most debilitating neurological conditions on the planet. This is not wishful thinking. It is based on receptor biology, animal studies, and early clinical data that point in a consistent direction.
GLP-1 receptors in the brain
GLP-1 receptors are not just found in the pancreas and gut. They are distributed throughout the central nervous system, with particularly high concentrations in two regions that are deeply relevant to migraine pathophysiology.
The hypothalamus contains a dense population of GLP-1 receptors. This brain region is increasingly recognized as a key player in migraine initiation. Functional imaging studies have shown that the hypothalamus activates before a migraine attack begins, sometimes hours before the pain starts. It is involved in the premonitory phase, that period when people sense that a migraine is coming through subtle changes in mood, energy, appetite, or yawning frequency. When GLP-1 agonists activate receptors in the hypothalamus, they modulate signaling pathways that overlap with migraine circuitry.
The choroid plexus is the other critical location. This structure produces cerebrospinal fluid, the liquid that bathes and cushions the brain. When too much cerebrospinal fluid is produced, intracranial pressure rises. Elevated intracranial pressure is a known headache trigger and is the defining feature of conditions like idiopathic intracranial hypertension. GLP-1 receptors in the choroid plexus appear to regulate fluid production, and activating them may reduce the volume of cerebrospinal fluid being created.
The presence of these receptors is not accidental. The brain uses GLP-1 signaling for purposes that extend far beyond blood sugar regulation. Researchers studying peptides for brain repair have long known that signaling molecules cross the blood-brain barrier and influence neurological function. Tirzepatide, as a dual GIP and GLP-1 agonist, engages these brain receptors every time it is administered. The question is not whether it reaches the brain. It does. The question is what happens when it gets there.
The CGRP connection
If you follow migraine research at all, you have heard of CGRP. Calcitonin gene-related peptide is a 37-amino acid neuropeptide that has become the central target of modern migraine therapy. Drugs like erenumab (Aimovig), fremanezumab (Ajovy), and galcanezumab (Emgality) work by blocking CGRP or its receptor. These medications have transformed migraine treatment for millions of people.
CGRP levels are elevated during migraine attacks. Infusing CGRP into migraine-prone individuals can trigger an attack. The neuropeptide dilates blood vessels in the brain, promotes neurogenic inflammation, and sensitizes pain pathways in the trigeminal system. It is, by all accounts, a key mediator of migraine pain.
Here is where GLP-1 agonists enter the picture. Preclinical research has shown that GLP-1 receptor agonists decrease CGRP expression in chronic migraine models. The mechanism appears to involve modulation of the trigeminal ganglion, the cluster of nerve cells that serves as the relay station for head and face pain. When GLP-1 receptors are activated in this system, CGRP production goes down. Not eliminated. But reduced in a way that could raise the threshold for migraine attacks.
This is remarkable because it means GLP-1 agonists like tirzepatide may work through a mechanism that parallels the most successful class of migraine-specific drugs ever developed. They are not just reducing headaches through some vague anti-inflammatory effect. They are targeting the same molecular pathway that purpose-built migraine drugs target. The implications for people who experience both obesity and chronic migraines are significant, and researchers in brain function optimization are paying close attention.
Neuroinflammation and cytokine reduction
Migraines are increasingly understood as a neuroinflammatory condition. During an attack, the brain releases a cascade of inflammatory molecules that sensitize pain pathways and perpetuate the cycle of pain. Two cytokines in particular, IL-6 and TNF-alpha, have been consistently linked to migraine pathophysiology. They are elevated in the cerebrospinal fluid of chronic migraine patients. They promote neuronal sensitization. They keep the pain going long after the initial trigger has passed.
GLP-1 receptor agonists reduce both IL-6 and TNF-alpha secretion. This has been demonstrated in multiple experimental models, and the anti-inflammatory effect extends beyond the gut and pancreas into the central nervous system. The mechanism involves suppression of NF-kB signaling, one of the master switches of inflammation throughout the body.
For someone with chronic migraines, this means that tirzepatide might be addressing one of the upstream drivers of their condition. Not just blocking pain signals after they start, but reducing the inflammatory environment that makes the brain vulnerable to attacks in the first place. This is the same anti-inflammatory logic that makes GLP-1 agonists interesting for autoimmune conditions and general inflammation management.
The brain does not exist in isolation from the rest of the body. Systemic inflammation drives neuroinflammation. The gut-brain axis carries inflammatory signals in both directions. When a drug like tirzepatide calms inflammatory signaling throughout the body, the brain benefits too. This is not a targeted migraine therapy. It is a systemic intervention that happens to have effects in the exact pathways that drive migraine.
Intracranial pressure reduction
Elevated intracranial pressure causes headaches. This is one of the most straightforward relationships in neurology. When the pressure inside the skull rises, whether from excess cerebrospinal fluid, venous sinus stenosis, or other causes, the result is a headache that can mimic migraine in its severity and characteristics.
GLP-1 receptor agonists reduce intracranial pressure. The evidence for this comes from studies in idiopathic intracranial hypertension, a condition characterized by elevated cerebrospinal fluid pressure without a clear structural cause. The GLP-1 receptors on the choroid plexus, when activated, appear to decrease the rate of cerebrospinal fluid production. Less fluid means lower pressure. Lower pressure means fewer headaches.
But the relevance extends beyond people with diagnosed intracranial hypertension. Some researchers believe that subclinical elevations in intracranial pressure may contribute to migraine in the general population. People who are overweight tend to have higher intracranial pressure, and the relationship between obesity and migraine frequency is well established. If tirzepatide reduces intracranial pressure through direct receptor activation, independent of weight loss, it could lower the migraine threshold for a broad range of people.
This mechanism also explains why some people report that their headaches improve after the first few weeks on tirzepatide, even before significant weight loss occurs. The receptor-mediated effects on cerebrospinal fluid dynamics begin relatively quickly, while meaningful weight loss takes months. It is a temporal pattern that supports a direct neurological effect rather than an indirect one mediated through body weight changes.
The liraglutide migraine pilot study: breakthrough results
The most compelling clinical evidence for GLP-1 agonists in migraine prevention comes from a pilot study published in the journal Headache. While this study used liraglutide rather than tirzepatide, the findings are directly relevant because both drugs activate GLP-1 receptors. And the results were striking enough to generate significant interest in the neurology community.
Study design and population
The study enrolled 31 patients who had two things in common: obesity and chronic migraine. Chronic migraine is defined as 15 or more headache days per month for at least three months. These are not people with occasional headaches. These are people whose lives are shaped by daily or near-daily pain. Many had tried multiple preventive medications. Many had failed standard treatments. They represented a population that is notoriously difficult to help.
Participants received liraglutide, a GLP-1 receptor agonist originally developed for type 2 diabetes and later approved for weight management. The primary interest was in what happened to their migraines, not their weight. This is an important detail because it influenced how the researchers interpreted the results.
Key findings
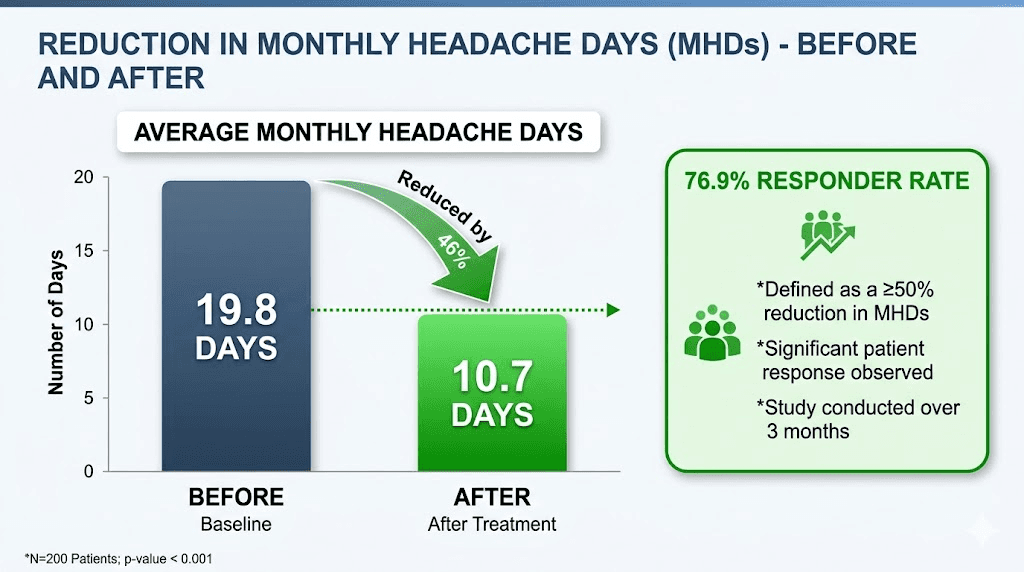
The results were remarkable by any standard in migraine prevention research.
Mean monthly headache days decreased from 19.8 to 10.7. That is a mean difference of 9.1 fewer headache days per month, a reduction that reached statistical significance with a p-value less than 0.001. To put this in perspective, most approved migraine preventive medications reduce monthly headache days by 2 to 4 compared to placebo. A reduction of 9.1 days is extraordinary.
Even more impressive: 76.9% of patients achieved at least a 50% reduction in monthly headache days. In migraine clinical trials, a 50% responder rate is the gold standard endpoint. Most successful migraine drugs achieve 50% responder rates in the range of 40% to 60% of patients. A 76.9% rate, even in a small open-label study, is attention-grabbing.
These numbers are the kind that make neurologists take notice. They are the kind that justify larger, more rigorous studies. And they align perfectly with the mechanistic evidence showing that GLP-1 receptor activation reduces CGRP, lowers neuroinflammation, and decreases intracranial pressure.
Why weight loss was not the driver
Here is the finding that makes the study especially interesting. BMI barely changed during the study period. The mean BMI went from 34.0 to 33.9. That is a trivial change. If the migraine improvement were simply a downstream effect of weight loss, you would expect the BMI change to be substantial and to correlate with the degree of migraine improvement. Neither was true.
This strongly suggests that the migraine benefit was independent of weight loss. The GLP-1 receptor agonist was doing something directly in the nervous system that reduced migraine frequency. The weight-independent mechanisms we discussed earlier, CGRP reduction, neuroinflammation suppression, intracranial pressure reduction, are the most likely explanations.
This has important implications for people taking tirzepatide. Even during the early weeks, before significant weight loss has occurred, the direct neurological effects of GLP-1 receptor activation may already be influencing migraine pathways. People who are interested in how fast tirzepatide works should know that metabolic and neurological effects often precede visible changes on the scale. The weight loss timeline and the neurological benefit timeline may not align at all.
It also matters for people who are at a healthy weight but suffer from migraines. While tirzepatide is currently approved for weight management and type 2 diabetes, the migraine data opens a conversation about potential off-label applications. No one is recommending this yet. But the science is pointing in an intriguing direction.
Tirzepatide for idiopathic intracranial hypertension
Beyond the liraglutide migraine study, there is another line of evidence that connects tirzepatide specifically to headache-related conditions. Research on idiopathic intracranial hypertension, or IIH, has produced some of the strongest data yet on GLP-1 agonists and head pain.
Study results
IIH is a condition where intracranial pressure is elevated without a tumor, infection, or other identifiable cause. It primarily affects women of childbearing age who are overweight. The hallmark symptoms are severe headaches, visual disturbances, and papilledema, which is swelling of the optic disc caused by elevated pressure.
In a study examining tirzepatide for IIH, the results were compelling. At 24 months, there was a 68% reduction in papilledema risk. Visual disturbance risk dropped by 73.9%. These are not small improvements. They represent a fundamental shift in the disease trajectory for a condition that can lead to permanent vision loss if untreated.
The mechanism is straightforward. Tirzepatide activates GLP-1 receptors on the choroid plexus, reducing cerebrospinal fluid production and lowering intracranial pressure. The direct receptor effect, combined with any weight loss that occurs, creates a dual benefit that addresses IIH from two directions simultaneously.
For headache management in IIH, the implications are clear. Lower intracranial pressure means fewer headaches. The severe, daily headaches that characterize IIH often improve in parallel with pressure reduction. People who have experienced these headaches describe them as among the worst they have ever had, sometimes rivaling migraine in their intensity.
Implications for migraine sufferers
You might wonder why IIH research matters if you do not have that specific condition. The answer lies in the overlap between IIH headaches and migraines.
Many IIH patients are initially misdiagnosed with chronic migraine. The headache phenotype can be remarkably similar. Some researchers believe that a spectrum of intracranial pressure dysregulation exists, with IIH at one extreme and subtler pressure-related headaches blending into what gets classified as chronic migraine.
If tirzepatide can reduce intracranial pressure enough to resolve headaches in IIH, it is plausible that it can reduce pressure enough to lower the migraine threshold in people without a formal IIH diagnosis. The choroid plexus GLP-1 receptors do not care about diagnostic labels. They respond to the drug regardless of what the patient chart says.
For people considering tirzepatide who also struggle with migraines, this data is encouraging. It suggests that the headache-causing reputation of GLP-1 drugs may be masking a deeper, more important truth: these drugs might actually help the headaches that matter most. The transient tension headaches of early treatment are a nuisance. A reduction in migraine frequency would be life-changing. Understanding your tirzepatide dosing and working through the initial adjustment period could be the bridge between temporary discomfort and lasting neurological benefit.
When tirzepatide makes migraines worse
Science is never as clean as we want it to be. While the evidence for migraine prevention is promising, there are documented cases where GLP-1 agonists have made migraines worse. Ignoring these cases would be dishonest, and understanding them is essential for anyone with a migraine history who is considering tirzepatide.
The hemiplegic migraine case report
One published case report describes a patient with hemiplegic migraines who experienced daily occurrences during 60 days on a GLP-1 receptor agonist. Hemiplegic migraine is a rare and severe form of migraine that causes temporary paralysis or weakness on one side of the body. It involves specific genetic mutations in ion channels and has a different pathophysiology than typical migraine with or without aura.
Daily hemiplegic migraines for 60 days is a serious adverse event. It suggests that in certain individuals, particularly those with specific migraine subtypes, GLP-1 receptor activation may lower the migraine threshold rather than raise it. The reasons are not fully understood, but they may involve the complex interplay between GLP-1 signaling and the cortical spreading depression that characterizes hemiplegic migraine.
One case report does not establish a pattern. But it does establish a possibility. And for someone with a history of hemiplegic migraine or other severe migraine subtypes, it is information worth discussing with a neurologist before starting tirzepatide.
Risk factors for migraine exacerbation
Beyond the hemiplegic migraine case, several factors can increase the risk of migraines worsening on tirzepatide. These are not guaranteed triggers, but they create conditions where migraines become more likely.
Rapid dose escalation is a significant risk factor. Moving from 2.5 mg to 5 mg to 7.5 mg too quickly does not give the body time to adapt. Each dose increase brings a new wave of metabolic adjustment, and for migraine-prone individuals, these adjustments can trigger attacks. The standard tirzepatide dose chart recommends at least four weeks at each dose level, but migraine-prone patients may benefit from even longer intervals.
Dehydration amplifies migraine risk. We covered this earlier in the context of tension headaches, but dehydration is an even more potent migraine trigger. The brain shrinks slightly when dehydrated, pulling away from the meninges and triggering pain signals. For someone already predisposed to migraines, this mechanical stress can initiate a full attack. Monitoring your fluid intake with the same attention you give to your dietary choices on tirzepatide is not optional for migraine-prone users.
Disrupted sleep patterns can trigger migraines, and some people experience insomnia on tirzepatide. If the medication disrupts your sleep architecture, you lose one of the most important protective factors against migraine attacks. Sleep is when the brain clears metabolic waste, restores neurotransmitter balance, and resets pain thresholds.
Hormonal fluctuations interact with both tirzepatide and migraines. Women who experience menstrual migraines may find that tirzepatide affects their menstrual cycle, and any hormonal disruption can influence migraine patterns. The relationship is bidirectional and complex.
Pre-existing anxiety on tirzepatide can also lower the migraine threshold. Stress and anxiety are among the most commonly reported migraine triggers, and if the medication is causing psychological side effects, migraines may follow.
Warning signs to watch for
Not all headaches on tirzepatide are benign. Certain features should prompt immediate medical attention.
Sudden onset, severe headache. Sometimes called a thunderclap headache, this pattern, where the pain reaches maximum intensity within seconds, can indicate serious conditions like subarachnoid hemorrhage. It is not a tirzepatide side effect. It is a medical emergency.
New neurological symptoms. If you develop weakness on one side, difficulty speaking, vision loss, or confusion along with headache, these could indicate stroke or other serious neurological events. Tirzepatide does not cause these, but they should not be dismissed as drug side effects.
Headaches that progressively worsen over days or weeks without improvement. Tirzepatide headaches typically improve over time. If yours are getting worse, something else may be going on. Headaches accompanied by fever and neck stiffness need urgent evaluation. And headaches that change character dramatically from your baseline, even if you have a history of migraines, deserve medical attention.
The key principle is this: do not assume every headache is a tirzepatide side effect. Most are. But the exceptions matter.
Practical guide: managing headaches and migraines on tirzepatide
Whether you are dealing with the common tension headaches of early treatment or navigating migraines as a pre-existing condition, practical strategies can make a significant difference. These approaches address the most common modifiable triggers and help your body adjust to tirzepatide with minimal neurological disruption.
Hydration protocol
Aim for 8 to 10 glasses of water daily. That is the minimum. If you are active, if you live in a warm climate, if you are experiencing any gastrointestinal side effects like constipation or diarrhea, you may need more.
Spread your water intake throughout the day. Drinking three glasses in the morning and nothing until dinner is not effective hydration. Your body can only absorb a certain amount of water per hour, and excess is simply excreted. Consistent sipping beats periodic gulping.
Add electrolytes. Plain water is not enough if you are eating significantly less food. Sodium, potassium, and magnesium all come from food, and if your food intake has dropped, your electrolyte levels may follow. A pinch of salt in your water, a sugar-free electrolyte mix, or coconut water can help maintain the mineral balance that prevents headaches. This is especially important for people taking supplements alongside tirzepatide.
Track your intake. It sounds tedious, but most people dramatically overestimate how much water they drink. A simple water bottle with time markings, or a phone reminder every hour, can make the difference between adequate hydration and the kind of deficit that triggers headaches.
Blood sugar stabilization
Eat small, frequent meals. Tirzepatide suppresses appetite powerfully, and many people fall into a pattern of eating once or twice a day because they simply are not hungry. This is a recipe for blood sugar instability. Even if you are not hungry, your brain still needs glucose.
Prioritize protein and complex carbohydrates. These foods provide sustained energy release rather than the spike-and-crash pattern of simple sugars. A structured diet plan that emphasizes regular eating intervals can prevent the blood sugar dips that trigger headaches.
Do not skip breakfast. The overnight fast already creates a blood sugar nadir in the early morning. Extending that fast further by skipping breakfast, especially on a drug that enhances insulin sensitivity, is asking for a headache. Even a small meal of 200 to 300 calories can stabilize your blood sugar enough to prevent symptoms.
If you notice headaches consistently occurring at certain times of day, track what you ate and when. You may find a pattern that reveals exactly when your blood sugar is dipping. Adjusting your meal plan around these vulnerable windows can be remarkably effective.
Over-the-counter options
For headaches that do occur despite preventive measures, standard over-the-counter medications are generally safe and effective.
Acetaminophen at 650 to 1000 mg is the first-line option. It does not interact with tirzepatide, does not irritate the stomach (which may already be sensitive from the medication), and provides effective relief for tension headaches. Do not exceed 3000 mg in a 24-hour period, and avoid it if you drink alcohol regularly or have liver concerns.
Ibuprofen at 400 to 600 mg is an alternative when acetaminophen is not sufficient. As an anti-inflammatory, it may be more effective for headaches with an inflammatory component. However, NSAIDs can cause gastrointestinal irritation, and since tirzepatide already affects the GI system, use ibuprofen with food and water.
Avoid overusing either medication. Medication overuse headache, sometimes called rebound headache, is a real phenomenon where taking pain relievers too frequently actually causes more headaches. If you are taking headache medication more than two to three days per week, talk to your healthcare provider about preventive strategies rather than reactive ones.
For true migraines, over-the-counter options may not be sufficient. Triptans and the newer CGRP-targeted acute treatments require a prescription and a discussion with a neurologist who understands both your migraine history and your tirzepatide treatment.
When to adjust your dose
If headaches are persistent and severe, a dose adjustment may be warranted. The standard tirzepatide escalation schedule moves from 2.5 mg to 5 mg after four weeks, then up in 2.5 mg increments at four-week intervals. But this timeline is not carved in stone.
Staying at a lower dose for longer is always an option. If 2.5 mg is producing good results with minimal side effects, there is no rush to increase. Some people find that a microdosing approach provides the benefits they want without the side effect burden of higher doses. The starting dose considerations are especially important for migraine-prone individuals.
Stepping back to a previous dose after a problematic increase is reasonable. If headaches appeared or worsened after going from 5 mg to 7.5 mg, returning to 5 mg for another four to six weeks before attempting the increase again gives your body more time to adapt. Consult your prescriber, but know that this is a common and accepted practice.
Understanding tirzepatide dosage in units helps you make informed decisions about dose adjustments with your healthcare provider.
When to contact a healthcare provider
Contact your prescriber if headaches are severe enough to interfere with daily activities. Contact them if headaches do not improve after the first four to six weeks on a stable dose. Contact them if you experience migraine-specific features, throbbing pain, light or sound sensitivity, nausea, aura, that you did not have before starting tirzepatide.
Contact them urgently if you experience any of the warning signs discussed earlier. Sudden severe headache, new neurological symptoms, progressive worsening, or headaches with fever.
And contact them if you are using headache medication more than two to three days per week. This pattern suggests that the underlying problem needs a different approach, not more reactive treatment. Your provider may recommend preventive migraine medications that work alongside tirzepatide, or they may suggest a different treatment strategy entirely.
Tirzepatide dosing considerations for migraine-prone individuals
Migraine-prone people are not the same as the general population when it comes to medication side effects. Their nervous systems are more reactive. Their thresholds for pain are lower. And their brains respond to metabolic changes with a sensitivity that non-migraineurs do not experience. These differences demand a more thoughtful approach to tirzepatide dosing.
Starting low and going slow
The standard starting dose of tirzepatide is 2.5 mg weekly, with increases at four-week intervals. For migraine-prone individuals, this schedule may still be too aggressive. Consider requesting a slower escalation, spending six to eight weeks at each dose level before increasing. The compound dosage chart can help you understand the available options.
Some practitioners working with compounded tirzepatide have the flexibility to start at doses lower than 2.5 mg. A starting dose of 1 mg or 1.5 mg, while not part of the standard branded protocol, allows the body to acclimate more gradually. This is particularly relevant for people whose migraines are sensitive to metabolic triggers, because the metabolic shifts are proportionally smaller at lower doses.
Document your headache patterns carefully during the first three months. Keep a headache diary that tracks frequency, severity, duration, associated symptoms, and potential triggers. This data is invaluable for your healthcare provider in determining whether dose adjustments are needed and whether your headaches are trending in the right direction. People who track carefully often discover that their headaches peak in weeks two through four of a new dose and then decline, a pattern that would be invisible without systematic recording.
The microdosing approach
Microdosing tirzepatide has gained attention as a strategy for minimizing side effects while still achieving therapeutic benefits. The concept is simple: use a lower dose than the standard protocol and stay there longer, or permanently.
For migraine-prone individuals, microdosing has a specific appeal. Lower doses produce smaller metabolic perturbations. Smaller perturbations mean fewer headache triggers. And if the migraine-preventive effects of GLP-1 receptor activation are present even at lower doses, the net result could be fewer migraines with fewer headache side effects.
The microdosing tirzepatide chart provides detailed information about how to implement this approach. It is not for everyone, and it requires working with a healthcare provider who is open to non-standard dosing strategies. But for the right patient, it can be the difference between tolerating the medication and abandoning it.
People using a compounded tirzepatide dosage calculator have additional flexibility in dialing in precise doses that may not be available with branded products.
Timing your injections
When you take your tirzepatide injection can influence side effect patterns. Some people find that injecting in the evening means they sleep through the peak side effect window. Others prefer morning injections so they can manage any symptoms during waking hours with hydration and food.
For migraine-prone users, the best time to take your GLP-1 shot may depend on your personal migraine patterns. If your migraines tend to occur in the morning, an evening injection that might produce mild symptoms overnight, when you are asleep, could be preferable. If your migraines tend to occur in the evening, a morning injection that produces peak effects during the day might work better.
Consistency matters more than the specific time you choose. Take your injection at the same time each week. This creates a predictable pharmacokinetic pattern that your body can adapt to, rather than a variable one that keeps resetting the adjustment process.
Also consider injection day relative to your schedule. Avoid injecting the night before a day where migraines would be particularly disruptive, like an important work presentation or a long drive. Understanding whether you can take tirzepatide a day early gives you flexibility to manage timing around your life.
Supplements that may help with both migraines and GLP-1 side effects
Several supplements have evidence supporting their use for both migraine prevention and managing the metabolic demands of tirzepatide treatment. This dual benefit makes them particularly valuable for migraine-prone individuals on GLP-1 therapy.
Magnesium
Magnesium is the most well-studied supplement for migraine prevention. The American Academy of Neurology and the American Headache Society have both recognized magnesium as having a probable effect in preventing migraines, based on clinical trial evidence. Magnesium glycinate and magnesium oxide are the most commonly studied forms, with typical preventive doses ranging from 400 to 600 mg daily.
For tirzepatide users, magnesium serves a dual purpose. Beyond migraine prevention, magnesium helps with the constipation that GLP-1 drugs can cause. Magnesium citrate and magnesium oxide have osmotic properties that draw water into the intestines, promoting regular bowel movements. And since reduced food intake on tirzepatide can lower dietary magnesium intake, supplementation addresses a potential deficiency at the same time.
Start with 200 mg daily and increase gradually to avoid gastrointestinal distress. Taking magnesium with food improves absorption and reduces the chance of stomach upset. For migraine prevention specifically, many neurologists recommend the glycinate form, which is better absorbed and less likely to cause digestive issues than oxide.
B vitamins
Riboflavin, or vitamin B2, has strong evidence for migraine prevention. A dose of 400 mg daily has been shown in randomized controlled trials to reduce migraine frequency. The mechanism likely involves mitochondrial energy metabolism, as migraineurs often show impaired mitochondrial function in brain tissue.
Vitamin B12 is relevant for a different reason. Tirzepatide and other GLP-1 agonists can impair B12 absorption over time. Low B12 levels can cause neurological symptoms including headaches, fatigue, and cognitive difficulties. Supplementing with B12, or using a tirzepatide and B12 combination, addresses this potential deficiency proactively.
A B-complex supplement provides both riboflavin and B12, along with other B vitamins that support energy metabolism and neurological function. For tirzepatide users with migraines, this is arguably the most efficient single supplement choice. Methylcobalamin formulations offer superior bioavailability compared to standard cyanocobalamin.
Electrolytes
We touched on electrolytes in the hydration section, but they deserve their own discussion in the supplement context. Sodium, potassium, and magnesium are the three electrolytes most relevant to headache prevention on tirzepatide.
When food intake drops, electrolyte intake drops with it. The body compensates to some extent, but if the deficit is large enough, symptoms appear. Headaches are among the earliest signs of electrolyte imbalance. The mechanism involves changes in cell volume, nerve conduction, and blood vessel tone, all of which influence headache and migraine susceptibility.
A comprehensive electrolyte supplement, taken daily during the adjustment phase and periodically thereafter, can prevent the deficits that trigger headaches. Products designed for fasting or low-carb diets often have the right balance. Avoid products with high sugar content, as these can cause the blood sugar spikes and crashes that trigger their own headaches. The GLP-1 supplement guide covers electrolyte options in detail.
CoQ10 and riboflavin
Coenzyme Q10, at a dose of 100 to 300 mg daily, has shown benefit in migraine prevention trials. Like riboflavin, its mechanism involves mitochondrial energy metabolism. Migraineurs appear to have higher energy demands in certain brain regions, and supporting mitochondrial function helps meet those demands.
The combination of CoQ10 and riboflavin may be more effective than either alone, though this has not been conclusively proven in head-to-head trials. Both are well-tolerated, inexpensive, and available without a prescription. For tirzepatide users, neither supplement has known interactions with GLP-1 therapy, making them safe additions to the regimen.
One practical note: CoQ10 is fat-soluble and absorbs better when taken with a meal containing some fat. Given that tirzepatide users often eat less fat overall, timing CoQ10 supplementation with your largest meal of the day optimizes absorption. Understanding caloric intake on tirzepatide helps you plan when to take fat-soluble supplements for maximum benefit.
Comparing GLP-1 options for migraine-prone users
Not all GLP-1 agonists are identical, and the differences may matter for migraine-prone individuals. While no head-to-head trials have compared GLP-1 drugs specifically for migraine outcomes, we can draw some inferences from their pharmacological profiles and side effect data.
Tirzepatide is a dual GIP and GLP-1 receptor agonist. The GIP component adds metabolic benefits but also adds a variable that does not exist with pure GLP-1 agonists. Whether GIP receptor activation influences migraine pathways is not yet known. The semaglutide versus tirzepatide comparison covers the broader differences between these two drugs.
Semaglutide is a pure GLP-1 agonist. The liraglutide migraine pilot study used another pure GLP-1 agonist, and the results were encouraging. If the migraine benefit comes primarily from GLP-1 receptor activation, then semaglutide should theoretically offer similar benefits. Some people who experience side effects on one GLP-1 drug tolerate a different one better. Switching from tirzepatide to semaglutide is an option if headaches on tirzepatide are problematic.
Newer options like mazdutide, survodutide, and CagriSema are emerging as alternatives. As a triple agonist, retatrutide activates GLP-1, GIP, and glucagon receptors. The additional receptor targets introduce new variables for migraine research that have not been studied at all.
Delivery method also matters. Oral tirzepatide and tirzepatide drops produce different pharmacokinetic profiles than injections. The absorption curve is smoother, which might reduce the metabolic perturbations that trigger headaches. Comparing oral versus injection formats can help migraine-prone users choose the delivery method that minimizes their risk.
The orally disintegrating tablet formulation represents another option with potentially different side effect profiles.
Here is the bottom line on comparisons: no one can tell you definitively which GLP-1 drug is best for migraine-prone individuals. The evidence does not exist yet. What we know is that the class as a whole shows promise for migraine prevention, that individual responses vary enormously, and that having multiple options to try is better than being limited to one.
What the research still does not tell us
Honesty about the limits of current knowledge is not a weakness. It is a strength. And the limits here are significant.
There is no randomized, placebo-controlled trial specifically testing any GLP-1 agonist for migraine prevention. The liraglutide pilot study was open-label and small. Open-label means that both patients and researchers knew what medication was being given, which introduces the possibility of placebo and expectation effects. Small means that the results could be skewed by a few outlier responders. These limitations do not invalidate the findings, but they do mean that the evidence is preliminary rather than definitive.
We do not know the optimal dose for migraine prevention. Is it the same dose needed for weight loss? Lower? Higher? The dose-response relationship for neurological effects may be completely different from the dose-response relationship for metabolic effects. Until dose-finding studies are conducted, we are guessing.
We do not know whether tirzepatide specifically, with its dual GIP and GLP-1 action, offers migraine benefits beyond what pure GLP-1 agonists provide. The GIP component is a wildcard. It might help. It might be neutral. It might complicate things.
We do not know which migraine subtypes respond best. Migraine without aura, migraine with aura, chronic migraine, episodic migraine, vestibular migraine, hemiplegic migraine, these are all distinct conditions with overlapping but different pathophysiology. A drug that helps one subtype might not help another. The case report of hemiplegic migraine worsening on a GLP-1 agonist underscores this point.
We do not know the long-term effects. All the data we have is from relatively short-term studies. Whether the migraine benefits persist over years, whether tolerance develops, whether discontinuation causes rebound migraines, these are all open questions.
And we do not know whether the migraine benefit is specific to people with obesity or extends to normal-weight migraineurs. The pilot study enrolled only obese patients. The weight-independence of the benefit suggests it might help normal-weight people too, but this has not been tested. For people exploring their BMI requirements for GLP-1 eligibility, this distinction matters.
What we do know is that the mechanistic story is coherent. GLP-1 receptors in the brain, CGRP reduction, neuroinflammation suppression, intracranial pressure reduction, these all point in the same direction. The pilot clinical data is consistent with the mechanism. And the signal is strong enough to warrant serious research investment. Randomized controlled trials are being discussed. Some may already be underway. In the meantime, migraine-prone individuals starting tirzepatide should be aware of both the risks and the potential benefits, and they should work with healthcare providers who understand both conditions.
SeekPeptides follows this research closely and updates resources as new evidence emerges, because understanding the full picture matters more than selling a simple narrative.
The lifestyle factors that connect migraines and tirzepatide success
Managing migraines and succeeding on tirzepatide share a surprising amount of common ground. The lifestyle modifications that prevent migraine attacks overlap substantially with the habits that minimize tirzepatide side effects and maximize weight loss outcomes. This convergence is not coincidental. Both conditions respond to metabolic stability, consistent sleep, adequate nutrition, and stress management.
Regular meal timing is critical for both. Migraine specialists have long advised patients to eat at consistent intervals because blood sugar fluctuations are potent migraine triggers. Tirzepatide users need the same consistency to prevent the hypoglycemic headaches discussed earlier and to maintain adequate nutrition during appetite suppression. A structured eating plan serves double duty.
Sleep hygiene matters enormously. Irregular sleep is one of the top migraine triggers. Getting adequate quality sleep protects against both migraines and the fatigue that some people experience on GLP-1 agonists. Aim for seven to nine hours on a consistent schedule, going to bed and waking at the same time even on weekends. If tirzepatide is disrupting your sleep, understanding insomnia patterns with GLP-1 drugs can help you find solutions.
Exercise is beneficial for both conditions but requires balance. Regular moderate exercise reduces migraine frequency. It also supports weight loss and metabolic health during tirzepatide treatment. But overexertion, particularly when dehydrated or underfueled, can trigger migraines. The sweet spot is consistent moderate activity with adequate hydration and nutrition.
Stress management ties everything together. Chronic stress elevates cortisol, increases inflammation, disrupts sleep, triggers migraines, and undermines the metabolic benefits of tirzepatide. Techniques that reduce stress, whether meditation, exercise, therapy, or simply protecting time for rest, support both conditions simultaneously. For those dealing with anxiety and stress management, addressing these underlying factors can improve both migraine outcomes and tirzepatide tolerability.
The gut-brain connection deserves special mention. Tirzepatide fundamentally alters gut function. It slows gastric emptying, changes appetite signaling, and may influence the gut microbiome. The gut and brain communicate bidirectionally through the vagus nerve, immune signaling, and metabolic pathways. Maintaining gut health with adequate fiber and potentially probiotics designed for GLP-1 users may support brain health and migraine resilience through mechanisms we are only beginning to understand. Exploring peptides for gut health may offer additional support for the gut-brain axis during GLP-1 therapy.
Drug interactions to be aware of
Migraine-prone individuals on tirzepatide often take other medications. Understanding potential interactions is essential for safety and effectiveness.
Triptans, the most commonly prescribed acute migraine medications, do not have known direct interactions with tirzepatide. However, some triptans can cause nausea as a side effect, and combining this with tirzepatide nausea can be unpleasant. Taking triptans with food and water, and ensuring your GI system is relatively settled before treating a migraine, can reduce this overlap.
CGRP inhibitors, both the injectable preventive versions and the oral acute treatments, do not interact with tirzepatide pharmacologically. Using both is generally considered safe, and the combination might theoretically be synergistic for migraine prevention, with CGRP inhibitors blocking the receptor directly while tirzepatide reduces CGRP production upstream. No studies have examined this combination specifically, but the mechanistic logic is sound.
Beta-blockers like propranolol, used for migraine prevention, can lower blood sugar and blood pressure. Since tirzepatide also promotes lower blood sugar, the combination requires monitoring for hypoglycemia. The reduced appetite from tirzepatide makes this risk more relevant than it would be otherwise. If you take propranolol for migraines and start tirzepatide, discuss blood sugar monitoring with your provider.
Topiramate, another migraine preventive, causes weight loss as a side effect. Adding tirzepatide could accelerate weight loss beyond what is healthy or intended. Both drugs also reduce appetite. The combination needs careful nutritional monitoring to ensure adequate caloric and nutrient intake.
Thyroid medication is relevant for some migraine patients. Thyroid disorders can contribute to headaches, and if you take levothyroxine alongside tirzepatide, the timing and absorption of your thyroid medication may need adjustment due to tirzepatide effects on gastric emptying.
Always inform both your neurologist and your prescribing physician for tirzepatide about all medications you take. Drug interaction databases are useful but cannot capture every clinical scenario. Personalized guidance from providers who know your full medication list is irreplaceable.
The future of GLP-1 agonists in migraine treatment
The convergence of obesity research and neurology around GLP-1 agonists represents one of the more exciting developments in both fields. The path from here to potential migraine treatment approval is long, but the direction of travel is clear.
Randomized controlled trials are the next step. The pilot data from liraglutide provides the rationale, and the mechanistic evidence supports the biological plausibility. What is needed is a large, well-designed trial that compares a GLP-1 agonist to placebo in migraine patients, stratified by weight status, migraine subtype, and other relevant variables. Such a trial would likely take several years and cost tens of millions of dollars, but the potential payoff, a new treatment option for a condition that affects over a billion people worldwide, justifies the investment.
Tirzepatide specifically is interesting because it is the most effective weight loss drug ever tested in clinical trials, and because its dual mechanism offers additional receptor targets. If migraine benefits prove to be real in rigorous studies, tirzepatide could become a game-changer for the large population of people who suffer from both obesity and migraines, two conditions that exacerbate each other in a vicious cycle.
The research community at SeekPeptides tracks these developments as they unfold, providing updated analysis and practical guidance for people navigating the intersection of peptide therapy and neurological health.
There is also growing interest in whether lower, migraine-specific doses of GLP-1 agonists could provide neurological benefits without the full metabolic effects. If CGRP reduction and neuroinflammation suppression occur at doses lower than those needed for weight loss, a migraine-specific dosing protocol could emerge. This would open GLP-1 agonists to normal-weight migraineurs and reduce the side effect burden for everyone. The concept of microdosing GLP-1 agonists could take on entirely new significance in the migraine context.
For now, what we have is a compelling hypothesis supported by early evidence. People starting tirzepatide who also have migraines should track their headache patterns carefully. The data they generate, the personal experience of whether migraines improve, worsen, or stay the same, contributes to the collective understanding of this emerging therapeutic area.
Reconstitution and injection best practices for migraine-prone users
Proper preparation and injection technique may seem unrelated to migraines, but for sensitive individuals, even minor stressors can contribute to headache risk. Getting the practical aspects of tirzepatide administration right reduces anxiety, ensures accurate dosing, and eliminates avoidable triggers.
If you are using compounded tirzepatide, proper reconstitution is essential. Incorrect reconstitution can lead to inaccurate dosing, which in turn can cause the blood sugar and metabolic fluctuations that trigger headaches. Use the peptide reconstitution calculator to ensure precision.
Injection site matters for comfort and absorption. Injecting into the abdomen is the most common approach, and proper injection technique reduces pain and injection site reactions. Rotating injection sites prevents tissue buildup that can alter absorption patterns. Understanding all available injection sites gives you options.
Using the correct syringe and dosage eliminates one source of dosing error. A comprehensive syringe guide walks you through the selection process. The peptide calculator and semaglutide dosage calculator are additional tools that SeekPeptides provides to help users achieve accurate dosing.
Proper storage preserves medication potency. Understanding how long tirzepatide lasts in the fridge and temperature stability outside refrigeration ensures that you are injecting a fully potent medication. Degraded medication may produce unpredictable pharmacokinetic profiles, and inconsistency is the enemy of migraine management. Knowing refrigeration requirements and expiration timelines protects your investment in both the medication and your health.
For people who experience injection anxiety, the stress of the injection itself can be a headache trigger. Techniques to reduce injection anxiety include icing the site beforehand, using a thin-gauge needle, injecting slowly, and practicing relaxation breathing during the process. Over time, the procedure becomes routine, and the stress response diminishes.
Tracking your response: building your personal data set
The science on tirzepatide and migraines is still being written. But you do not have to wait for large clinical trials to understand how the drug affects your migraines specifically. Building a personal data set is both practically useful and scientifically valuable.
Start tracking before you begin tirzepatide, if possible. One to two months of baseline migraine data, recording frequency, severity, duration, and triggers, provides the comparison point you need to evaluate any change after starting the medication.
After starting tirzepatide, continue tracking with the same level of detail. Record your dose, the day you inject, and any headache or migraine that occurs in the days that follow. Note what you ate, how much you drank, how well you slept, and your stress level. This granular data reveals patterns that aggregate statistics cannot.
Look for trends over months, not days. Migraine patterns are inherently variable. A single bad week does not mean tirzepatide is making your migraines worse, just as a single good week does not mean it is helping. The meaningful signal emerges over eight to twelve weeks at a stable dose.
Share your data with your healthcare providers. A headache specialist or neurologist who sees your tracking data can make much more informed recommendations than one who is relying on your memory of how many migraines you had last month. Memory is notoriously unreliable for headache frequency, with most people underestimating or overestimating by a significant margin.
If you are part of online communities for either tirzepatide users or migraine sufferers, consider sharing your experience. Anecdotal reports from individuals are not clinical evidence, but they contribute to the collective awareness that drives formal research. Every person who reports that their migraines improved on a GLP-1 agonist adds to the signal that researchers use to justify clinical trials.
Special populations and considerations
Certain groups face unique considerations at the intersection of tirzepatide and migraines. Addressing these directly ensures that this guide serves the broadest possible audience.
Women who experience menstrual migraines should know that tirzepatide can alter menstrual patterns. Changes in body fat affect estrogen levels, and estrogen fluctuations are the primary driver of menstrual migraines. If tirzepatide changes your cycle, your migraine pattern may shift in unpredictable ways. This could mean improvement for some women and worsening for others. Understanding how GLP-1 drugs affect your period provides context for these changes.
Women who are pregnant or planning to become pregnant have a particularly complex situation. Tirzepatide is not approved for use during pregnancy. Women who become pregnant on tirzepatide should discontinue the medication. Migraine patterns often change dramatically during pregnancy due to hormonal shifts, and the withdrawal of a GLP-1 agonist adds another variable. Breastfeeding considerations further complicate the picture.
People with a history of autoimmune conditions and migraines represent another special group. Autoimmune diseases often involve neuroinflammation that can drive migraines, and the anti-inflammatory effects of GLP-1 agonists could be particularly beneficial in this context. However, autoimmune patients often take immunosuppressive medications that may interact with GLP-1 therapy in ways that have not been fully studied.
Elderly patients may experience both migraines and conditions for which tirzepatide is beneficial, but they also face higher risks of dehydration, hypoglycemia, and medication interactions. Slower dose titration and more frequent monitoring are advisable.
People taking phentermine alongside tirzepatide face additional headache risk, as phentermine itself can cause headaches. The comparison between phentermine and tirzepatide may help migraine-prone individuals choose the approach with fewer neurological side effects.
Additional considerations for long-term users
For people who have been on tirzepatide for months or longer, the headache landscape changes. The initial adjustment headaches have long since resolved. The question becomes whether the long-term neurological effects of GLP-1 receptor activation are providing ongoing migraine protection.
Some long-term users report a gradual reduction in migraine frequency that they attribute to tirzepatide. These anecdotal reports are consistent with the mechanistic evidence. Chronic GLP-1 receptor activation could produce sustained reductions in CGRP, ongoing anti-inflammatory effects, and persistent intracranial pressure management. If the drug is doing these things continuously, the migraine benefit would be continuous as well.
Others report a plateau effect, where an initial improvement in migraines levels off or reverses. This could reflect tolerance at the receptor level, changes in other migraine triggers, or simply the natural variability of migraine patterns. Understanding why tirzepatide might stop working as expected can help differentiate between tolerance and other factors.
If you stop tirzepatide, there is a question of whether any migraine benefit will persist. GLP-1 withdrawal can bring back appetite and metabolic changes relatively quickly. Whether migraine frequency rebounds as rapidly is unknown. The neuroinflammatory and CGRP changes may resolve more slowly than the metabolic changes, providing a window of continued benefit. Or they may rebound faster. We simply do not have the data to say.
Long-term users should continue monitoring their headache patterns and report any significant changes to their healthcare providers. The relationship between tirzepatide and migraines is not a set-it-and-forget-it situation. It evolves over time and deserves ongoing attention.
Monitoring your metabolic changes alongside headache patterns can reveal correlations that inform treatment decisions. Some people find that as their body composition changes, their migraine patterns shift as well, since adipose tissue produces inflammatory mediators that can influence headache threshold.
The first month on tirzepatide is typically the most challenging for headaches, while the overall timeline for therapeutic effects extends over many months. Patience and systematic tracking are your best tools for understanding your personal response.
Alcohol, caffeine, and other modifiable triggers
Two substances that many people consume daily interact with both tirzepatide and migraine susceptibility: alcohol and caffeine.
Alcohol is a well-established migraine trigger for many people. Red wine is the most commonly cited culprit, but any alcoholic beverage can trigger attacks in susceptible individuals. Tirzepatide alters how the body processes alcohol. Many users report feeling the effects of alcohol much more quickly and intensely. Understanding alcohol use on tirzepatide is important for all users, but migraine-prone individuals have an additional reason to be cautious. The combination of tirzepatide-altered alcohol metabolism and migraine susceptibility creates a higher risk of triggering attacks.
Caffeine has a more complex relationship with migraines. In moderate amounts, it can actually help prevent migraines, which is why it is included in some migraine medications. But caffeine withdrawal is a potent migraine trigger. If tirzepatide reduces your appetite and you find yourself drinking less coffee because you are not eating breakfast, the resulting caffeine withdrawal could trigger migraines. Maintain consistent caffeine intake or taper slowly if you decide to reduce it.
The food guidance for GLP-1 users applies equally to tirzepatide users and should be considered alongside personal migraine trigger lists. Everyone has different food triggers, aged cheeses, processed meats, MSG, artificial sweeteners, and managing these while also following GLP-1 dietary guidelines requires some planning. But the overlap between migraine-friendly eating and tirzepatide-friendly eating is substantial: both favor fresh, whole foods eaten at regular intervals in moderate portions.
The bigger picture: metabolic health and neurological resilience
Stepping back from the specifics, there is a broader theme worth noting. Metabolic health and neurological resilience are deeply connected. Obesity increases migraine risk. Insulin resistance is associated with headache disorders. Systemic inflammation drives both metabolic dysfunction and neurological pain. The conditions that tirzepatide was designed to treat, type 2 diabetes and obesity, share root causes with the conditions it may incidentally help, including migraines.
This is not a coincidence. The body is an integrated system. Metabolic dysfunction creates an inflammatory, insulin-resistant, pressure-elevated environment that the brain cannot escape. Fix the metabolic dysfunction, whether through weight loss, direct receptor effects, or both, and the brain benefits.
The emerging story of GLP-1 agonists and migraines is part of a larger narrative about how metabolic drugs are revealing connections between body systems that were previously studied in isolation. Cardiologists discovered that GLP-1 agonists reduce heart attacks. Nephrologists discovered they protect the kidneys. Hepatologists discovered they improve fatty liver disease. And now neurologists are discovering they may prevent migraines.
For individuals exploring the broader landscape of nootropic peptides and energy-boosting peptides, the GLP-1 story underscores how interconnected metabolic and neurological health truly are. Supporting one system invariably supports the other.
Each discovery reflects the same underlying truth: metabolic health is the foundation on which the rest of the body is built. When that foundation is shaky, everything else, the heart, the kidneys, the liver, the brain, suffers. When that foundation is strengthened, everything else improves. Tirzepatide may not be a migraine drug. But by fixing the metabolic environment that makes migraines more likely, it may accomplish what no targeted migraine therapy has achieved: addressing the root cause rather than the symptom.
Frequently asked questions
Can tirzepatide cause migraines?
Tirzepatide can cause headaches, with 4% to 14% of clinical trial participants reporting them depending on the dose. However, most of these are tension-type headaches, not true migraines. True migraines involving throbbing pain, light sensitivity, nausea, and aura are much less common. The primary causes of headaches on tirzepatide are dehydration and blood sugar fluctuations, both of which are manageable with proper hydration and regular eating. If you experience migraine-specific symptoms for the first time on tirzepatide, consult your healthcare provider, as this warrants evaluation. Most headaches on tirzepatide resolve within the first few weeks of a stable dose.
Do GLP-1 drugs prevent migraines?
Emerging research suggests they might. A pilot study of liraglutide, a GLP-1 receptor agonist, in patients with obesity and chronic migraine found that mean monthly headache days dropped from 19.8 to 10.7, a highly significant reduction. GLP-1 receptor agonists reduce CGRP expression, lower neuroinflammation, and decrease intracranial pressure, all of which are relevant to migraine pathophysiology. However, no large randomized placebo-controlled trial has been completed yet, so the evidence remains preliminary. The mechanistic and early clinical data are promising but not definitive.
Should I stop tirzepatide if I get migraines?
Not necessarily. Headaches on tirzepatide typically resolve within the first few weeks. If you are experiencing new migraines or worsening of existing migraines, first address the common modifiable causes: ensure adequate hydration (8 to 10 glasses daily), eat small frequent meals to stabilize blood sugar, and maintain consistent sleep. If symptoms persist beyond four to six weeks on a stable dose, discuss with your healthcare provider whether a dose reduction or slower titration schedule might help. Stopping the medication should be a collaborative decision with your provider, not a unilateral one based on early side effects that might resolve.
Is the headache from tirzepatide different from a migraine?
Yes, in most cases. The typical tirzepatide headache is bilateral (both sides of the head), mild to moderate in intensity, and has a pressing or tightening quality. This is a tension-type headache. A migraine is usually unilateral (one side), moderate to severe, with a throbbing or pulsating quality. Migraines are often accompanied by nausea, sensitivity to light and sound, and sometimes visual aura. If your headache on tirzepatide has migraine features, it deserves specific attention and management rather than simple over-the-counter treatment. Understanding the full spectrum of GLP-1 headaches helps you identify what you are experiencing.
Can tirzepatide help with chronic migraines?
The evidence is not strong enough to recommend tirzepatide specifically for chronic migraines. However, for people who need tirzepatide for weight management or diabetes and also have chronic migraines, there is reason for cautious optimism. The liraglutide pilot study showed that 76.9% of chronic migraine patients achieved at least a 50% reduction in monthly headache days, and this improvement was independent of weight loss. Tirzepatide activates the same GLP-1 receptors and likely produces similar neurological effects. Discussing this potential benefit with both your neurologist and your metabolic physician is worthwhile.
What supplements help with both migraines and tirzepatide side effects?
Magnesium is the standout dual-purpose supplement. It has established evidence for migraine prevention (400 to 600 mg daily) and helps with the constipation common on GLP-1 drugs. Riboflavin (vitamin B2) at 400 mg daily has proven migraine-preventive effects. Vitamin B12 supports neurological function and addresses potential B12 depletion from GLP-1 therapy. CoQ10 (100 to 300 mg daily) supports mitochondrial energy metabolism relevant to migraine prevention. Electrolyte supplementation prevents the mineral deficits that trigger headaches when food intake is reduced. A comprehensive vitamin guide for GLP-1 users can help you build an effective supplement regimen.
How long do headaches last when starting tirzepatide?
Most headaches resolve within the first two to four weeks on a stable dose. When you increase your dose, headaches may recur temporarily as your body adjusts to the higher level of GLP-1 receptor activation. This is why a slow titration schedule, spending at least four weeks at each dose level, is recommended. Migraine-prone individuals may benefit from even longer intervals of six to eight weeks between dose increases. If headaches persist beyond six weeks on a stable dose, this is atypical and warrants medical evaluation. Understanding the timeline for tirzepatide effects helps set realistic expectations.
Can I take migraine medication with tirzepatide?
Most migraine medications, including triptans, CGRP inhibitors, and common preventive medications, do not have direct pharmacological interactions with tirzepatide. However, tirzepatide slows gastric emptying, which can delay the absorption of oral medications. For acute migraine treatment, where speed of relief matters, this delayed absorption could reduce effectiveness. Nasal spray or injectable migraine medications bypass this issue. Beta-blockers used for migraine prevention can interact with tirzepatide by increasing hypoglycemia risk. Always inform all your healthcare providers about every medication you take. The body aches guide and pain management resources at SeekPeptides cover related topics in detail.
External resources
American Migraine Foundation - Comprehensive patient education on migraine types, treatments, and management strategies
Headache journal: GLP-1 receptor agonists and migraine - Published research on GLP-1 agonists in headache disorders
FDA Drug Safety Communications - Official safety information for tirzepatide and other GLP-1 agonists
International Classification of Headache Disorders - Diagnostic criteria that distinguish migraine subtypes from other headache types
World Health Organization: Headache Disorders - Global perspective on headache burden and classification
The relationship between tirzepatide and migraines defies simple characterization. It is a story of paradox, where a drug that causes headaches might also prevent the worst kind of headache. It is a story of emerging science, where mechanisms discovered in metabolic research are revealing unexpected connections to neurology. And it is a story that is still being written, with crucial chapters missing.
What you can do right now is practical and concrete. If you are starting tirzepatide and have a history of migraines, work with your healthcare providers to develop a monitoring and management plan. Hydrate deliberately. Eat regularly. Start low and go slow with dosing. Track your headache patterns with precision. Take the supplements that have evidence for migraine prevention and GLP-1 support.
And watch the science. The research pipeline is active. Randomized controlled trials will eventually answer the questions that pilot studies and mechanistic evidence can only suggest. When those answers arrive, they may reshape how we think about both metabolic and neurological health.
In case I do not see you, good afternoon, good evening, and good night. May your headaches stay manageable, your migraines stay infrequent, and your protocols stay informed.