Mar 1, 2026
What if the problem is not your dose, but that 60 units means something completely different depending on which vial you are holding?
This is the question that trips up thousands of researchers every single day. They read their prescription. They see 60 units. They draw it up. And they have no idea whether they just pulled 3 mg, 6 mg, 12 mg, or even 24 mg of tirzepatide into that syringe. The number on the barrel stays the same. The medication inside changes dramatically based on one critical variable that most dosing guides barely mention: concentration.
Here is the reality. Sixty units on an insulin syringe always equals 0.6 mL of liquid. That part never changes. But the milligrams of tirzepatide dissolved in that 0.6 mL depend entirely on how concentrated your specific vial is. A 10 mg/mL vial delivers 6 mg in those 60 units. A 20 mg/mL vial delivers 12 mg. Same syringe reading, double the medication. Get this wrong and you are either underdosing by half or overdosing by a factor that could send you to the emergency room with severe nausea, vomiting, and dangerously low blood sugar. This guide breaks down every concentration, every calculation, and every step you need to measure 60 units of tirzepatide safely and accurately.
The quick answer: 60 units of tirzepatide in milligrams
If you need the answer right now, here it is. Sixty units equals 0.6 mL of liquid. The milligrams depend on your vial concentration.
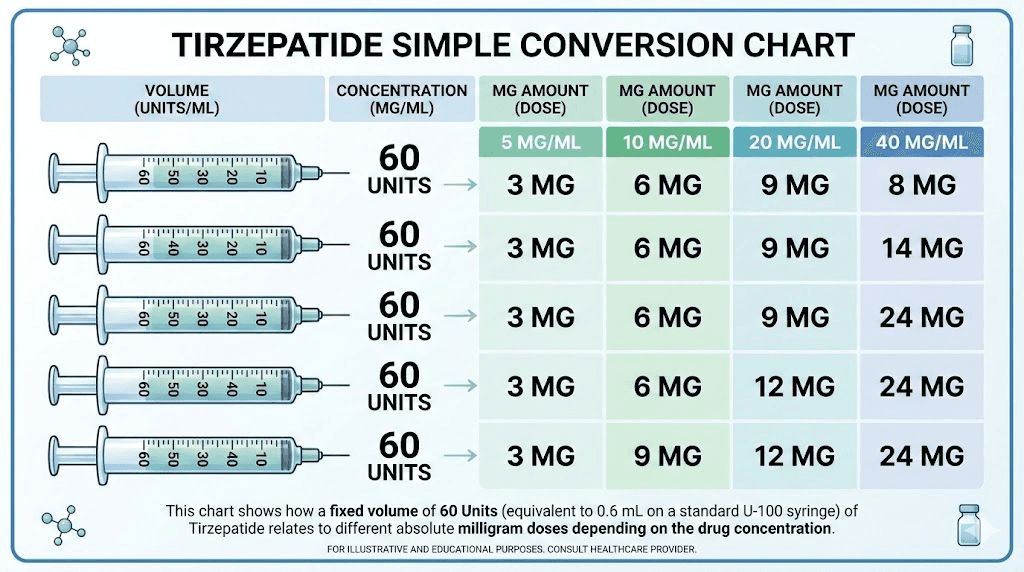
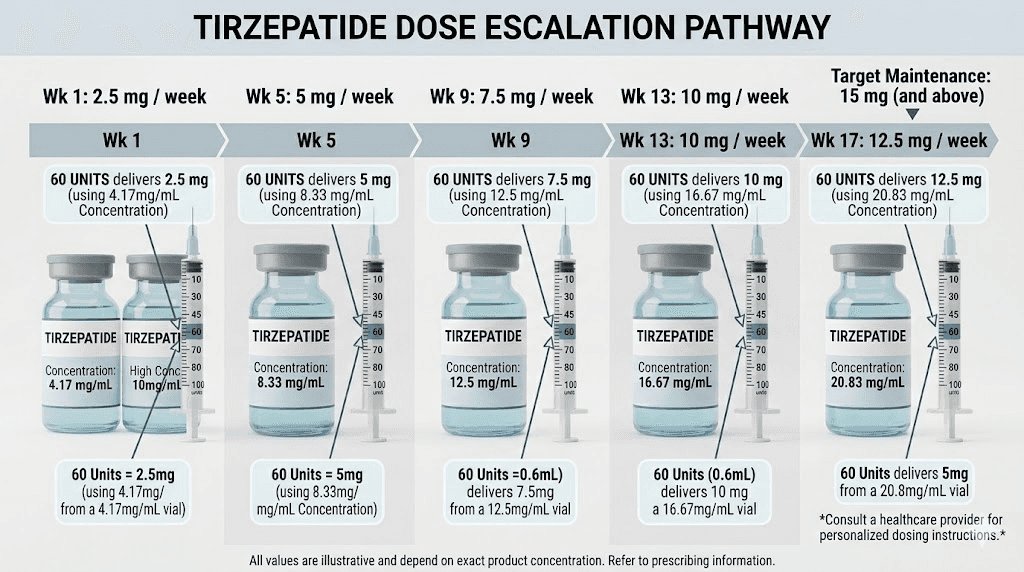
At 5 mg/mL, 60 units equals 3 mg of tirzepatide. At 10 mg/mL, 60 units equals 6 mg. At 15 mg/mL, 60 units equals 9 mg. At 20 mg/mL, 60 units equals 12 mg. At 40 mg/mL, 60 units equals 24 mg. At 60 mg/mL, 60 units equals 36 mg.
That is the short version. But if you are working with compounded tirzepatide, you need to understand why these numbers differ so dramatically, how to verify your own vial concentration, and how to measure with precision every single time. The sections below walk through each concentration in detail, provide complete conversion tables, and cover the most common mistakes researchers make when drawing 60 units from a compounded tirzepatide vial.
Why 60 units does not have one simple answer
Most medications come in a single standard concentration. You open the package, draw the prescribed amount, and inject. Tirzepatide does not work that way, at least not when you are using compounded versions rather than brand-name Mounjaro or Zepbound autoinjectors.
Compounding pharmacies produce tirzepatide in multiple concentrations. Some mix it at 5 mg/mL. Others at 10 mg/mL. Some produce highly concentrated formulations at 20 mg/mL, 40 mg/mL, or even 60 mg/mL. The concentration tells you how many milligrams of tirzepatide are dissolved in every milliliter of liquid. And since insulin syringes measure volume in units (where 100 units equals 1 mL), the milligrams you get from 60 units depends entirely on how dense that liquid is with active medication.
Think of it like coffee.
A regular brew and an espresso both fill a cup. But the espresso packs far more caffeine into the same volume. Similarly, 60 units drawn from a 40 mg/mL vial contains eight times more tirzepatide than 60 units from a 5 mg/mL vial. Same volume. Wildly different potency. This is exactly why understanding your specific tirzepatide concentration matters more than memorizing a single conversion number.
The brand-name difference
Brand-name Mounjaro and Zepbound come in pre-filled autoinjectors. Each pen contains a fixed dose, and the device delivers exactly that amount when you click the button. There are no syringes, no unit markings to interpret, and no concentration math required. The available doses are 2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, and 15 mg. You would never need to draw 60 units from a Mounjaro pen because the delivery mechanism handles everything automatically.
The 60-unit question only applies to researchers working with compounded tirzepatide vials and insulin syringes. If that describes your situation, keep reading. Every detail you need is below.
Understanding units, milligrams, and milliliters
Before diving into specific calculations, you need to understand three measurement terms that get confused constantly. Getting them straight is the foundation of accurate dosing, and most conversion errors trace back to mixing these up.
Units are a measure of volume
On an insulin syringe, units measure how much liquid you are drawing up. They do not measure medication strength. A standard U-100 insulin syringe holds 100 units total, which equals exactly 1 mL (one milliliter) of liquid. So 60 units equals 0.6 mL. Always. Regardless of what medication is inside the vial. Whether that syringe contains saline, tirzepatide, semaglutide, or plain water, 60 units is 0.6 mL of liquid every time.
Milligrams are a measure of medication strength
Milligrams (mg) tell you how much active medication is dissolved in the liquid. This is the number your prescriber cares about. When a protocol says "take 5 mg of tirzepatide," it means 5 milligrams of the active compound, regardless of the volume of liquid that contains it. Two vials can both deliver 5 mg. One might require you to draw 50 units. The other might require only 25 units. The milligrams are the same. The volume differs because the concentrations differ.
Milliliters are the bridge between units and milligrams
Milliliters (mL) measure liquid volume just like units do, but on a different scale. The conversion is straightforward: 100 units equals 1 mL. So 60 units equals 0.6 mL. Once you know the volume in milliliters, you multiply by the concentration (mg/mL) to get your milligrams. This three-step chain, units to mL to mg, is how every tirzepatide syringe dosage calculation works.
Understanding these three terms is not optional. It is the difference between an accurate dose and a potentially dangerous mistake. If you are using compounded tirzepatide with insulin syringes, this knowledge protects you every single time you draw a dose.
The conversion formula every researcher needs
There is one formula that converts any number of units to milligrams for any concentration. Memorize it. Write it on a sticky note. Tape it to your refrigerator where you store your vials.
mg = (units / 100) x concentration (mg/mL)
That is it. Three steps, one multiplication. For 60 units, the math looks like this:
Step 1: Divide 60 units by 100 to get the volume in mL. Result: 0.6 mL.
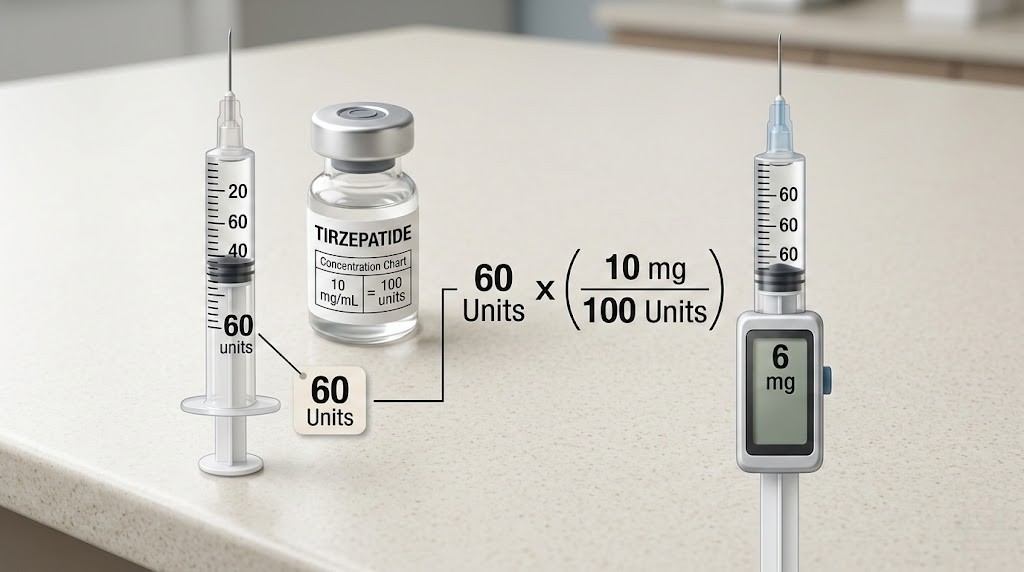
Step 2: Find the concentration printed on your vial label. Example: 10 mg/mL.
Step 3: Multiply 0.6 mL by 10 mg/mL. Result: 6 mg.
This formula works for any unit amount and any concentration. Drawing 20 units from a 10 mg/mL vial? That is 0.2 mL times 10, which equals 2 mg. Drawing 50 units from a 20 mg/mL vial? That is 0.5 mL times 20, which equals 10 mg. The formula never changes. Only the numbers you plug in differ.
You can also work the formula backwards if your prescriber tells you a milligram dose and you need to figure out how many units to draw. The reverse formula is:
units = (mg / concentration) x 100
So if your protocol calls for 6 mg and your vial is 10 mg/mL, you divide 6 by 10 to get 0.6 mL, then multiply by 100 to get 60 units. The dosage calculators on SeekPeptides can do this math automatically, but knowing the manual calculation ensures you can always verify your dose independently.
60 units at every common concentration
Now let us walk through what 60 units actually delivers at each concentration you are likely to encounter. Compounding pharmacies produce tirzepatide at several standard concentrations, and knowing which one you have is the single most important factor in accurate dosing. If you have not already, check your vial label before reading further. The concentration is typically printed as a number followed by mg/mL.
60 units at 5 mg/mL: 3 mg of tirzepatide
At 5 mg/mL, your tirzepatide is relatively dilute. Each milliliter contains 5 mg of active medication. Since 60 units equals 0.6 mL, you multiply 0.6 by 5 to get 3 mg.
This concentration is less common but still produced by some compounding pharmacies. The advantage is that the lower concentration allows for more precise measurement of small doses. The disadvantage is that higher doses require large injection volumes. A 15 mg dose at 5 mg/mL would require 300 units, which is 3 mL, far more than a standard insulin syringe can hold. Most researchers using 5 mg/mL vials stay at lower doses like 2.5 mg (50 units) or 5 mg (100 units), making this concentration best suited for early-stage dosing or microdosing protocols.
At this concentration, 60 units delivers 3 mg, which falls between the 2.5 mg starting dose and the 5 mg second-tier dose in the standard tirzepatide dose escalation schedule. Some researchers use this intermediate dose during transitions between dose levels to minimize gastrointestinal side effects.
60 units at 10 mg/mL: 6 mg of tirzepatide
The 10 mg/mL concentration is the most widely used formulation for compounded tirzepatide. Most compounding pharmacies default to this strength because it hits a sweet spot. Every standard dose from 2.5 mg to 10 mg fits within a single 1 mL insulin syringe, and the unit markings correspond to clean, easy-to-read numbers.
At 10 mg/mL, 60 units delivers exactly 6 mg. The math is simple: 0.6 mL times 10 mg/mL equals 6 mg.
Six milligrams sits between the 5 mg and 7.5 mg dose tiers in the standard escalation protocol. This is not a standard dose level in the FDA-approved dosing schedule, which escalates in 2.5 mg increments (2.5, 5, 7.5, 10, 12.5, 15 mg). However, some prescribers recommend intermediate doses like 6 mg for researchers who respond well to 5 mg but are not yet ready for the full jump to 7.5 mg. This gentler escalation approach can help minimize the nausea and headaches that sometimes accompany dose increases.
If your vial is 10 mg/mL and you are drawing 60 units, confirm with your prescriber that 6 mg is indeed your target dose. A common mistake is confusing 60 units with the 6 mg dose at this concentration, then continuing to draw 60 units after switching to a different concentration vial where 60 units no longer equals 6 mg.
60 units at 15 mg/mL: 9 mg of tirzepatide
Some compounding pharmacies offer a 15 mg/mL concentration. At this strength, 60 units delivers 9 mg of tirzepatide (0.6 mL times 15 mg/mL equals 9 mg).
Nine milligrams is another non-standard dose that falls between the 7.5 mg and 10 mg tiers. Like the 6 mg example above, this intermediate dosing approach is sometimes used by prescribers who prefer smaller incremental increases. The weight loss timeline research from the SURMOUNT clinical trials used 2.5 mg increments every four weeks, but real-world protocols sometimes take smaller steps, especially for researchers who experience significant side effects at standard dose jumps.
The 15 mg/mL concentration is convenient for mid-range doses but can create very small injection volumes at lower doses. A 2.5 mg dose at 15 mg/mL requires only about 17 units (0.17 mL), which is difficult to measure precisely on most insulin syringes. For that reason, many researchers start their tirzepatide journey at lower concentrations and switch to 15 mg/mL only after escalating past the initial doses.
60 units at 20 mg/mL: 12 mg of tirzepatide
At 20 mg/mL, the concentration doubles compared to the standard 10 mg/mL. This means 60 units delivers 12 mg of tirzepatide, twice what the same 60 units would deliver from a 10 mg/mL vial.
This is where concentration differences become genuinely dangerous if you are not paying attention. Imagine you have been drawing 60 units from a 10 mg/mL vial for weeks, getting your comfortable 6 mg dose. Your pharmacy sends a refill at 20 mg/mL. You draw the same 60 units out of habit. Instead of 6 mg, you just injected 12 mg, a dose that is double what your body is accustomed to. The gastrointestinal side effects alone could be severe: intense nausea, vomiting, diarrhea, and abdominal pain that lasts for days.
Twelve milligrams falls between the 10 mg and 12.5 mg standard dose levels. It represents a high therapeutic dose that most researchers reach only after months of careful dose escalation. Never draw this amount unless your prescriber has specifically confirmed 12 mg as your target dose at your current concentration.
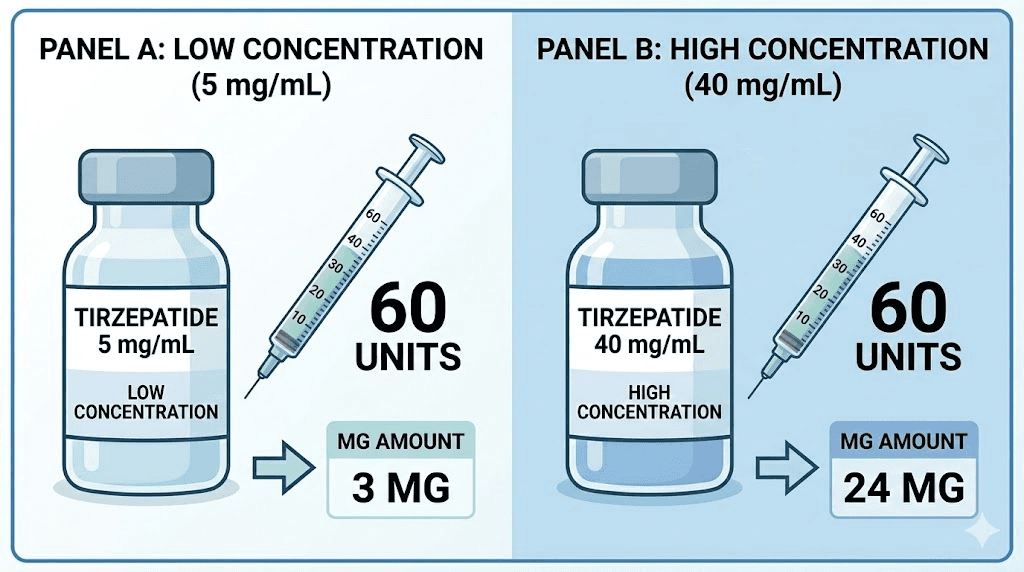
60 units at 40 mg/mL: 24 mg of tirzepatide
High-concentration vials at 40 mg/mL are used by specialized compounding pharmacies, often for researchers on higher maintenance doses who want to minimize injection volume. At this concentration, 60 units delivers a massive 24 mg of tirzepatide.
To put this in perspective, the maximum FDA-approved dose of tirzepatide is 15 mg per week. Twenty-four milligrams exceeds that maximum by 60%. This is not a dose you would ever reach through standard escalation protocols. If you are drawing 60 units from a 40 mg/mL vial, something is almost certainly wrong unless you have a very specific and carefully monitored protocol from your prescriber.
The 40 mg/mL concentration exists primarily so that researchers on the standard 10 mg or 15 mg doses can use smaller injection volumes. At 40 mg/mL, a 10 mg dose requires only 25 units (0.25 mL), and a 15 mg dose requires about 37.5 units (0.375 mL). These smaller volumes can be more comfortable to inject and may reduce injection site reactions.
60 units at 60 mg/mL: 36 mg of tirzepatide
The 60 mg/mL concentration is rare and extremely potent. At this strength, 60 units would deliver 36 mg of tirzepatide, which is more than double the maximum FDA-approved weekly dose. This concentration exists almost exclusively for compounding efficiency and requires extremely careful measurement. A mere 25 units (0.25 mL) from a 60 mg/mL vial delivers 15 mg, the maximum standard dose.
If your vial is 60 mg/mL, you should be working with very small unit amounts. Drawing 60 units from this concentration would be appropriate only under extraordinary circumstances with direct medical supervision. For most researchers, encountering this concentration means adjusting their unit measurements dramatically downward compared to what they were drawing from lower-concentration vials.
Complete 60-unit conversion reference table
Here is every concentration and what 60 units delivers, all in one place. Bookmark this section, screenshot it, or print it and keep it near your supplies. Having a quick reference prevents calculation errors when you are drawing your dose.
Concentration | 60 Units (0.6 mL) | Common for |
|---|---|---|
5 mg/mL | 3 mg | Low-dose protocols, microdosing |
10 mg/mL | 6 mg | Most common, standard compounding |
15 mg/mL | 9 mg | Mid-range compounding |
20 mg/mL | 12 mg | Higher-dose efficiency |
40 mg/mL | 24 mg | Minimal volume protocols |
60 mg/mL | 36 mg | Rare, specialized compounding |
Notice how the milligrams scale directly with concentration. When the concentration doubles, the mg in 60 units doubles. When it quadruples, the mg quadruples. This linear relationship makes the math predictable once you understand the underlying formula, and you can find similar breakdowns for other unit amounts in our complete tirzepatide conversion chart.
For researchers who also work with semaglutide, the same conversion logic applies. The formula is identical, only the concentrations and typical dose ranges differ. You can explore semaglutide unit-to-mg conversions and the semaglutide dosage in units guide for parallel reference tables.
How to read your tirzepatide vial label
Your vial label contains every piece of information you need to calculate your dose. But compounding pharmacy labels vary in format, and the critical details are sometimes buried among other text. Here is exactly what to look for and where to find it.
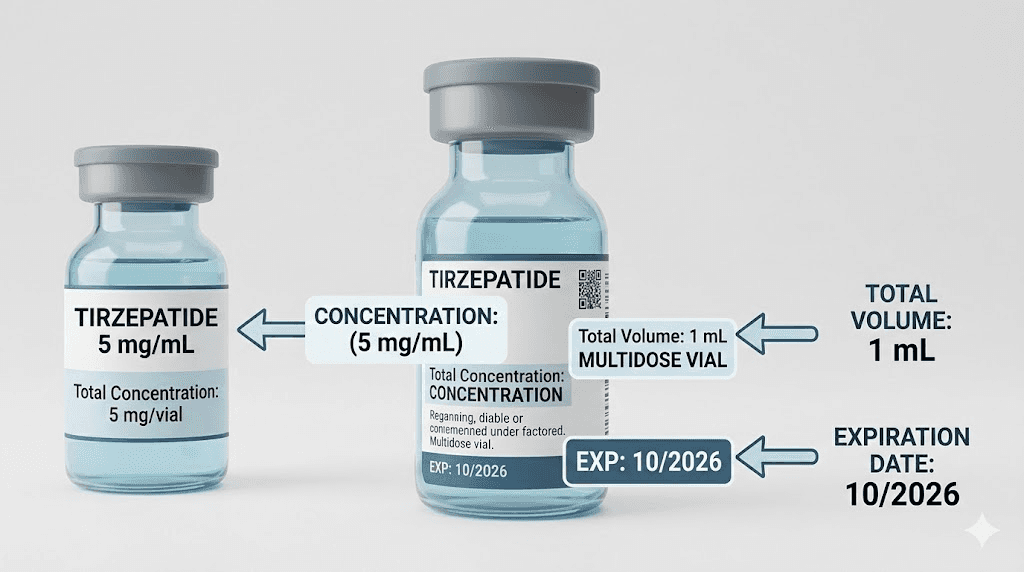
Finding the concentration
The concentration is the most important number on your label. It tells you how many milligrams of tirzepatide are dissolved in each milliliter of liquid. Look for a number followed by "mg/mL" or "mg per mL." Common examples include:
Tirzepatide 10 mg/mL
Tirzepatide 200 mg/10 mL (which equals 20 mg/mL)
Tirzepatide 50 mg/5 mL (which equals 10 mg/mL)
Some labels express concentration as total medication per total volume rather than per-mL. A label reading "50 mg/5 mL" means there are 50 mg total in the entire 5 mL vial, which works out to 10 mg per mL. You need the per-mL number for your unit calculations, so divide the total mg by the total mL if the label gives you the ratio format.
Finding the total vial volume
The total volume tells you how many doses your vial contains. A 5 mL vial at 10 mg/mL contains 50 mg total. If you are taking 6 mg per week (60 units at 10 mg/mL), that vial contains roughly eight weeks of doses. Knowing this helps you plan refills and recognize when your vial is running low, which matters for proper storage timing.
Checking the expiration date
Compounded tirzepatide has a shorter shelf life than many medications. Most compounding pharmacies assign beyond-use dates of 30 to 90 days from compounding, depending on the formulation and storage conditions. Using medication past its expiration date can result in reduced potency, meaning your 60 units might not actually deliver the full expected milligrams of active tirzepatide. Always check this date before drawing a dose.
Verifying the medication name and additives
Some compounded tirzepatide vials include additional ingredients like vitamin B12, glycine, or niacinamide. These additives do not change the tirzepatide concentration or your unit calculations, but you should know what is in your vial. Check that the label matches what your prescriber ordered and what your pharmacy confirmed.
How to read your insulin syringe correctly
Even with the right concentration identified, drawing exactly 60 units requires reading your syringe accurately. This sounds basic. It is not. Parallax errors, air bubbles, and different syringe sizes create measurement mistakes that compound over weeks of dosing.
U-100 insulin syringes explained
The standard insulin syringe used for tirzepatide injections is a U-100 syringe. The "U-100" means the syringe is calibrated so that 100 units equals 1 mL. These syringes come in three common sizes:
0.3 mL syringe (30 units max): Too small for 60 units. Do not use this size.
0.5 mL syringe (50 units max): Also too small for 60 units. Do not use this size.
1 mL syringe (100 units max): This is the correct syringe for drawing 60 units.
Make sure you are using a 1 mL (100-unit) syringe. Using a smaller syringe means you physically cannot draw 60 units, and attempting to force more liquid than the syringe can hold creates a mess and a wasted dose. For complete guidance on choosing the right syringe for your protocol, see our tirzepatide syringe dosage guide.
Reading the markings
On a 1 mL U-100 syringe, the barrel has numbered markings at every 10 units (10, 20, 30, 40, 50, 60, 70, 80, 90, 100). Between each numbered marking, there are smaller lines representing individual units or 2-unit increments, depending on the syringe manufacturer.
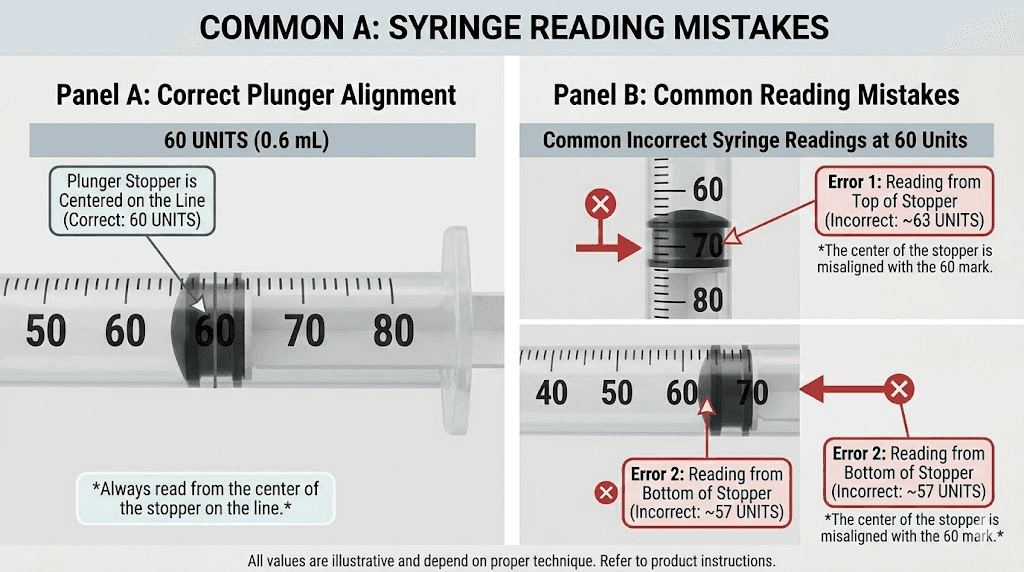
To draw 60 units, you pull the plunger until the top edge of the black rubber stopper aligns with the 60-unit line. Not the bottom edge of the stopper. Not the middle. The top edge. This is the most common source of measurement error, and getting it wrong by even a few units changes your dose by a meaningful amount.
Avoiding parallax errors
Parallax is what happens when you read the syringe from an angle instead of straight on. Looking at the syringe from above makes the liquid level appear higher than it actually is. Looking from below makes it appear lower. Hold the syringe at eye level, perpendicular to your line of sight, and read the top edge of the plunger stopper against the unit markings. This gives you the true volume every time.
Dealing with air bubbles
Air bubbles inside the syringe displace liquid and reduce your actual dose. A large bubble sitting below the medication can make it look like you have drawn 60 units when you have actually drawn only 55 units of liquid plus 5 units of air. Before injecting, hold the syringe needle-up, tap the barrel gently to move bubbles toward the needle, and push the plunger slightly to expel the air. Then verify your 60-unit measurement again, drawing more medication if needed.
For researchers who want a complete walkthrough of the injection process, including syringe preparation, injection technique, and post-injection care, see our guide on how to inject tirzepatide.
Where 60 units falls in the tirzepatide dosing schedule
Understanding the standard tirzepatide escalation protocol helps you verify whether 60 units at your concentration corresponds to an appropriate dose. The FDA-approved dosing schedule for tirzepatide (used in the SURMOUNT and SURPASS clinical trials) follows a gradual escalation over 20 weeks.
The standard dose escalation
Tirzepatide treatment starts at 2.5 mg once weekly for the first four weeks. This initial phase allows your body to adjust to the medication and identify any adverse reactions at the lowest therapeutic dose. After four weeks, the dose increases to 5 mg weekly. From there, it escalates in 2.5 mg increments every four weeks through the available dose levels: 7.5 mg, 10 mg, 12.5 mg, and the maximum of 15 mg.
Here is exactly where 60 units falls at each concentration within this schedule:
Concentration | 60 Units Delivers | Position in Schedule |
|---|---|---|
5 mg/mL | 3 mg | Between starting dose (2.5 mg) and second tier (5 mg) |
10 mg/mL | 6 mg | Between second tier (5 mg) and third tier (7.5 mg) |
15 mg/mL | 9 mg | Between third tier (7.5 mg) and fourth tier (10 mg) |
20 mg/mL | 12 mg | Between fourth tier (10 mg) and fifth tier (12.5 mg) |
40 mg/mL | 24 mg | Above maximum approved dose (15 mg) |
Notice that 60 units rarely lands exactly on a standard dose level. At most concentrations, it delivers an intermediate dose. This is perfectly fine if your prescriber has specifically prescribed that intermediate amount. Many practitioners prefer gradual escalation in smaller increments than the 2.5 mg jumps used in clinical trials, particularly for researchers who experienced significant fatigue or body aches at prior dose increases.
Clinical trial results by dose level
The SURMOUNT-1 trial, published in the New England Journal of Medicine, evaluated tirzepatide for weight management in adults with obesity. Results showed average weight reductions of 16.0% on 5 mg, 21.4% on 10 mg, and 22.5% on 15 mg over 72 weeks. Among participants on the 15 mg dose, 57% achieved 20% or greater weight reduction.
These results inform dosing decisions because they show that higher doses generally produce more weight loss, but the incremental benefit between 10 mg and 15 mg is smaller than between 5 mg and 10 mg. For researchers on intermediate doses like 6 mg (60 units at 10 mg/mL), results will likely fall somewhere between the 5 mg and 10 mg trial outcomes. The timeline for seeing results typically follows a similar pattern regardless of the specific dose within the therapeutic range.
If you are not seeing expected results at your current dose, our guide on tirzepatide not working anymore and why you may not be losing weight on tirzepatide covers the most common reasons and solutions.
Step-by-step guide to drawing 60 units of tirzepatide
Here is the complete process for accurately drawing 60 units from a compounded tirzepatide vial. Follow every step in order. Skipping steps or rushing through the process is how dosing errors happen.
Gather your supplies
You will need your tirzepatide vial, a 1 mL (100-unit) insulin syringe with an attached needle, alcohol swabs, and a sharps container for disposal. Make sure the vial has been removed from refrigeration 15 to 20 minutes before injection. Cold medication can sting more during injection and may be more viscous, making it harder to draw smoothly.
Verify your vial concentration
Before touching the syringe, read the vial label. Confirm the concentration (mg/mL). Run the formula in your head: 60 divided by 100 equals 0.6, times your concentration equals your dose in mg. Does that number match what your prescriber ordered? If yes, proceed. If no, stop and contact your prescriber or pharmacist before drawing any medication.
Clean the vial stopper
Wipe the rubber stopper on top of the vial with an alcohol swab. Let it air dry for a few seconds. This prevents bacteria from being pushed into the vial when you insert the needle. Contamination can compromise the entire vial, wasting every remaining dose and potentially causing injection site infections.
Prepare the syringe
Remove the syringe from its sterile packaging. Pull the plunger back to the 60-unit mark, drawing in 60 units of air. Insert the needle through the rubber stopper into the vial. Push the plunger down to inject the air into the vial. This equalizes pressure inside the vial and makes drawing medication much easier. Without this step, the vacuum inside the vial resists the plunger, making smooth drawing difficult.
Draw the medication
With the needle still in the vial, turn the vial upside down so the needle tip is submerged in the liquid. Slowly pull the plunger back to the 60-unit mark. Watch the medication fill the syringe barrel. If bubbles appear, tap the syringe gently and push them back into the vial, then redraw to the 60-unit line.
Verify the measurement
Remove the syringe from the vial. Hold it at eye level with the needle pointing up. Check that the top edge of the plunger stopper aligns exactly with the 60-unit marking. No air bubbles should sit below the medication. If bubbles are present, tap them upward and push them out through the needle (a tiny drop of medication at the needle tip is normal and expected).
Inject
Clean your injection site with an alcohol swab. Common injection sites include the abdomen (at least two inches from the navel), the front of the thigh, or the back of the upper arm. Pinch a fold of skin, insert the needle at a 90-degree angle, and push the plunger steadily until all medication is delivered. Wait 5 to 10 seconds before withdrawing the needle to ensure the full dose absorbs into the tissue. For detailed injection technique guidance, see our injection guide and GLP-1 injection site recommendations.
Common mistakes when measuring 60 units
These are the errors that trip up both beginners and experienced researchers. Each one can significantly alter your dose, and some can be dangerous.
Mistake 1: not checking the concentration when switching vials
This is the single most dangerous dosing error. You have been drawing 60 units from a 10 mg/mL vial for weeks, getting a comfortable 6 mg dose. Your pharmacy refill arrives. You draw 60 units without reading the label. But this new vial is 20 mg/mL. You just injected 12 mg, double your usual dose. The gastrointestinal consequences of an accidental double dose can be severe and prolonged.
The fix is simple but non-negotiable: read the concentration label every single time you draw from any vial, even if you think it is the same as last time. Especially if you just received a new shipment.
Mistake 2: using the wrong syringe size
A 0.5 mL (50-unit) syringe physically cannot hold 60 units. If you try to draw past the maximum marking, you risk breaking the seal between the plunger and barrel, contaminating the medication, or injecting air into your tissue. Always use a 1 mL (100-unit) syringe when drawing 60 units.
Conversely, using a 1 mL syringe is correct for 60 units, but the markings are more spread out on a 0.5 mL syringe, which offers finer precision for smaller doses. If your dose is under 50 units, a smaller syringe might give you better accuracy. For 60 units specifically, the 1 mL size is your only option.
Mistake 3: reading the wrong edge of the plunger stopper
The plunger stopper is the black rubber piece at the bottom of the plunger inside the barrel. It has a dome shape with a top edge and bottom edge. Always read the measurement from the top edge (the flat part closest to the needle). Reading from the bottom edge or the middle of the dome will give you a false measurement, typically 1 to 2 units off in either direction.
Mistake 4: ignoring air bubbles
Small air bubbles seem harmless. They are not dangerous to inject subcutaneously, but they displace medication. A large bubble in your syringe means you drew less than 60 units of actual medication, even though the plunger sits at the 60-unit line. Always tap out bubbles and verify your measurement after removing them.
Mistake 5: confusing TB syringes with insulin syringes
Tuberculin (TB) syringes measure in milliliters (mL), not units. A TB syringe marked at 0.6 mL delivers the same volume as 60 units on an insulin syringe. But the markings look different, and the scale increments differ. If your prescriber tells you to draw 60 units and you are using a TB syringe, you need to draw to the 0.6 mL mark instead. Confusing these syringe types is a recipe for dosing errors. Our syringe dosage guide explains the differences between syringe types in detail.
Mistake 6: reusing syringes
Insulin syringes are single-use devices. Reusing a syringe dulls the needle (increasing injection pain and tissue damage), introduces bacteria into your vial, and can cause the unit markings to become harder to read as the plunger rubber wears down. Each dose of 60 units should use a fresh, sterile syringe. The cost of a new syringe is trivial compared to the cost of a contaminated vial or an infection.
What to do if you drew the wrong amount
Mistakes happen. Here is how to handle them depending on when you catch the error.
If you catch it before injecting
Good news. Simply push the medication back into the vial and redraw the correct amount. If you drew too much, push the plunger until it reads the correct unit amount, then proceed with your injection. If you drew too little, pull more medication until you reach the correct line. No harm done.
If you already injected the wrong dose
This is more complicated and depends on how far off you were.
Slightly under-dosed (within 10% of target): If you injected 55 units instead of 60 at your concentration, the difference is small enough that it will not meaningfully affect your results for that week. Take your correct dose at the next scheduled injection. Do not try to "make up" the difference by adding extra units next time.
Significantly under-dosed (more than 20% below target): Contact your prescriber. They may advise you to take a supplemental dose, wait until your next scheduled injection, or adjust your schedule. The answer depends on your specific dose level and how much you actually administered.
Over-dosed: This is the more concerning scenario. If you injected significantly more than intended, monitor for side effects. The most common symptoms of excessive tirzepatide include severe nausea, vomiting, diarrhea, abdominal pain, and dizziness. Stay hydrated and contact your prescriber or seek medical attention if symptoms are severe. In rare cases, excessive doses can cause dangerously low blood sugar (hypoglycemia), particularly if combined with other diabetes medications.
The best policy is prevention. Double-check your concentration and your syringe reading before every injection. The ten seconds it takes to verify can prevent hours or days of uncomfortable side effects.
How 60 units compares to other common measurements
Putting 60 units in context helps you understand where this measurement sits relative to other common tirzepatide doses. Here is a comparison at the most popular 10 mg/mL concentration.
Units | Volume (mL) | mg at 10 mg/mL | Standard Dose Tier |
|---|---|---|---|
0.2 mL | 2 mg | Below starting dose | |
0.25 mL | 2.5 mg | Starting dose (Weeks 1-4) | |
0.3 mL | 3 mg | Between tiers 1-2 | |
0.4 mL | 4 mg | Between tiers 1-2 | |
50 units | 0.5 mL | 5 mg | Second tier (Weeks 5-8) |
60 units | 0.6 mL | 6 mg | Between tiers 2-3 |
75 units | 0.75 mL | 7.5 mg | Third tier (Weeks 9-12) |
100 units | 1.0 mL | 10 mg | Fourth tier (Weeks 13-16) |
At 10 mg/mL, 60 units sits comfortably between the 5 mg and 7.5 mg dose tiers. This makes it a natural choice for researchers transitioning between these two levels or for those on a slower escalation schedule who prefer smaller dose increments.
For similar conversion references at different unit amounts, we have comprehensive guides for 50 units, 40 units, 30 units, and 20 units of tirzepatide. Each guide covers the same concentration-dependent math and practical measurement advice specific to that unit amount.
Compounded versus brand-name tirzepatide
Understanding the difference between compounded and brand-name tirzepatide matters for dosing accuracy because the two forms use fundamentally different delivery systems.
Brand-name (Mounjaro and Zepbound)
Mounjaro (for type 2 diabetes) and Zepbound (for weight management) are the brand-name versions of tirzepatide manufactured by Eli Lilly. Both come as pre-filled, single-dose autoinjector pens. You do not draw medication, measure units, or calculate concentrations. Each pen delivers exactly one dose when you click the activation button. The available pen doses are 2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, and 15 mg.
With brand-name pens, the concept of "60 units" does not apply. The pen handles all measurement internally. You simply select the correct dose pen from your prescription and inject.
Compounded tirzepatide
Compounded tirzepatide comes in multi-dose vials and requires manual measurement with insulin syringes. This is where unit-to-mg conversions become essential. Compounded versions are available at various concentrations, and the same unit amount delivers different milligrams depending on the vial you are using.
Compounded tirzepatide has become widely available through compounding pharmacies, often at lower cost than brand-name versions. For researchers comparing their options, our guides on affordable tirzepatide and compounded tirzepatide pricing cover current market conditions. Several pharmacy reviews are also available for specific providers including Empower Pharmacy, ProRx, and Southend Pharmacy.
Compounded formulation variations
Beyond concentration differences, compounded tirzepatide may include additional ingredients. Common additions include vitamin B12 (cyanocobalamin), methylcobalamin, glycine, and niacinamide. These additives serve various purposes, from reducing injection site irritation to supporting metabolic function. However, none of them change the tirzepatide concentration listed on your label. Your 60-unit calculation remains the same regardless of which additives are included in the formulation.
If you are new to compounded tirzepatide and need help with the initial reconstitution process, our reconstitution guide and mixing chart walk through every step. For those who received pre-mixed liquid vials (which most compounding pharmacies now provide), reconstitution is not required and you can draw directly from the vial.
Storage and handling after drawing your dose
Proper storage protects the remaining medication in your vial, ensuring that your next 60-unit draw delivers the same potency as the last one. Degraded tirzepatide can lose effectiveness silently, meaning your 60 units still contains 0.6 mL of liquid but with fewer active milligrams than the label promises.
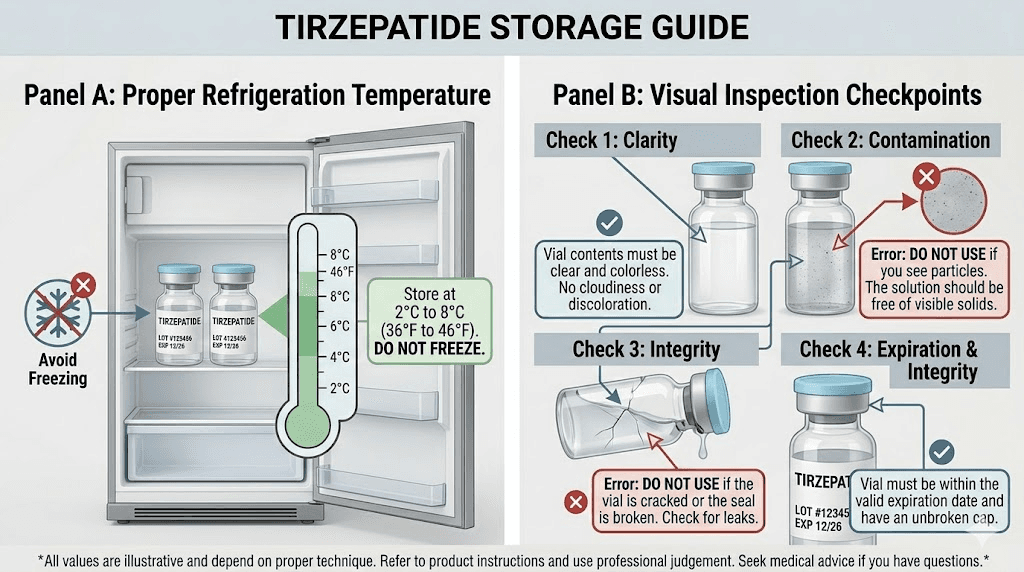
Refrigeration requirements
Most compounded tirzepatide should be stored in the refrigerator at 36 to 46 degrees Fahrenheit (2 to 8 degrees Celsius). After first use (the first time you puncture the vial stopper with a needle), some formulations have a shorter shelf life. Check your pharmacy label for specific storage instructions and beyond-use dating. For complete storage guidance, see our detailed article on tirzepatide refrigeration requirements.
Handling temperature excursions
Life happens. Sometimes a vial gets left out on the counter or sits in a warm delivery box for hours. Brief temperature excursions (a few hours at room temperature) typically do not destroy tirzepatide. However, extended exposure to heat or direct sunlight can degrade the peptide. If your vial has been out of the fridge for more than a few hours, contact your compounding pharmacy for guidance on whether it is still safe to use.
Never freeze tirzepatide
Freezing can damage the peptide structure and alter the concentration in unpredictable ways. If your vial has frozen, do not use it. Contact your pharmacy for a replacement. A compromised vial means your 60-unit dose may contain significantly less active medication than expected, or the medication may have degraded into ineffective fragments.
Inspect before every draw
Before drawing 60 units from your vial, hold it up to the light and inspect the liquid. Tirzepatide solution should be clear and colorless (or very slightly yellow, depending on the formulation). If you see cloudiness, floating particles, discoloration, or anything that looks unusual compared to when you first opened the vial, do not use it. These visual changes can indicate contamination or degradation. Our guide on how long tirzepatide lasts in the fridge provides detailed information on expected shelf life by formulation type.
Converting between syringe types
Not everyone uses U-100 insulin syringes. Some researchers work with tuberculin (TB) syringes, and the markings differ. Here is how 60 units translates across syringe types.
U-100 insulin syringe
As discussed throughout this guide, 60 units on a U-100 insulin syringe equals 0.6 mL. The syringe barrel is marked in units (typically with major lines every 10 units), and 60 units is clearly labeled on 1 mL syringes.
Tuberculin (TB) syringe
TB syringes are marked in milliliters rather than units. To draw the equivalent of 60 units, you would draw to the 0.6 mL mark on a TB syringe. The advantage of TB syringes is that they often have finer graduation marks, allowing for more precise measurement of volumes between major markings. The disadvantage is that your prescriber probably told you "60 units," and you need to remember to convert to 0.6 mL when using a TB syringe.
Quick conversion reference
Insulin Syringe (units) | TB Syringe (mL) | Volume Delivered |
|---|---|---|
10 units | 0.1 mL | Same |
25 units | 0.25 mL | Same |
50 units | 0.5 mL | Same |
60 units | 0.6 mL | Same |
75 units | 0.75 mL | Same |
100 units | 1.0 mL | Same |
The volume is always the same. Only the scale markings on the barrel differ. Whether your syringe says 60 units or 0.6 mL, you are drawing the exact same amount of liquid, and the milligrams of tirzepatide in that liquid still depend on your vial concentration.
Related conversions for other tirzepatide dose amounts
If you are working with tirzepatide, you will likely need to convert other unit amounts as your dose escalates or if your prescriber adjusts your protocol. Here are the most commonly searched conversions with links to our detailed guides for each.
Lower unit amounts
Researchers starting tirzepatide or on lower doses frequently need to convert 20 units to mg (0.2 mL) and 25 units to mg (0.25 mL). At the standard 10 mg/mL concentration, these deliver 2 mg and 2.5 mg respectively. The 2.5 mg dose (25 units at 10 mg/mL) is the standard starting dose for tirzepatide treatment.
As you progress through the escalation schedule, 30 units (3 mg at 10 mg/mL) and 40 units (4 mg at 10 mg/mL) become relevant for researchers on intermediate dose escalation protocols. These amounts are particularly useful for those following a microdosing approach.
Higher unit amounts
After moving past the 60-unit range, researchers often need to convert 50 units (5 mg at 10 mg/mL, a standard dose tier), 75 units (7.5 mg at 10 mg/mL, another standard tier), and 100 units (10 mg at 10 mg/mL, the fourth standard tier). At concentrations above 10 mg/mL, these unit amounts deliver even higher milligram doses.
Converting milligrams to units
Sometimes you need to work in the other direction. Your prescriber says "take 5 mg" and you need to know how many units that is. Our guides for converting specific milligram doses to units cover 2.5 mg to units, 5 mg to units, 7.5 mg to units, 10 mg to units, and 15 mg to units at every common concentration.
Semaglutide versus tirzepatide unit conversions
Many researchers work with both semaglutide and tirzepatide, and the conversion math is identical for both medications. The formula, mg equals units divided by 100 times concentration, works regardless of which GLP-1 receptor agonist is in the vial. The only differences are the typical concentrations available and the standard dose ranges.
Semaglutide vials commonly come in concentrations of 2.5 mg/mL, 5 mg/mL, or 10 mg/mL. The standard dose range is lower than tirzepatide: 0.25 mg to 2.4 mg weekly for weight management. So while the math is the same, the numbers you plug in differ significantly. You can explore semaglutide-specific conversions in our guides for 40 units of semaglutide, 50 units of semaglutide, and our complete semaglutide units-to-mg guide.
For researchers considering switching between these two medications, our semaglutide to tirzepatide conversion chart and dosage comparison chart explain how doses translate between the two drugs. The medications have different side effect profiles as well, which is worth understanding before making any changes. And the broader comparison between these two leading GLP-1 medications is covered in our semaglutide vs tirzepatide comparison page.
Optimizing your tirzepatide results at any dose
Accurate dosing is just one piece of the puzzle. Whether your 60 units delivers 3 mg or 12 mg, the following factors influence how well the medication works.
Timing and consistency
Tirzepatide is administered once weekly. Pick a day and stick with it. Consistency keeps blood levels stable and maximizes the medication appetite-suppressing and glucose-regulating effects. If you need to shift your injection day by a day or two, that is generally fine. For guidance on timing flexibility, see our article on taking tirzepatide a day early and our broader guide on the best time to take your GLP-1 shot.
Diet and nutrition
Tirzepatide suppresses appetite, which means many researchers eat significantly less. This makes food quality more important than ever. Every calorie counts more when you are consuming fewer of them. Prioritize protein (to prevent muscle loss), hydrate aggressively (to avoid constipation), and choose nutrient-dense foods that support your energy and micronutrient needs.
We have comprehensive nutrition guides for researchers on tirzepatide, including what to eat on tirzepatide, foods to avoid, a complete diet plan, and even a downloadable meal plan. These resources help you maximize the benefits of your medication while avoiding nutritional deficiencies that can stall progress.
Supplements that support GLP-1 therapy
Certain supplements can complement tirzepatide therapy. The most commonly recommended include electrolytes, probiotics, fiber supplements, and B vitamins. Many compounded formulations already include B12 or glycine, but additional supplementation may be beneficial depending on your individual needs. Discuss any supplement additions with your prescriber, especially if you are considering combining tirzepatide with other medications like phentermine.
Managing side effects
Side effects are most common during the early weeks of treatment and after dose increases. The most frequently reported include nausea, constipation, diarrhea, headaches, fatigue, and body aches. Most side effects diminish as your body adjusts to each dose level, which is one reason the escalation schedule spans 20 weeks rather than jumping immediately to the target dose.
If you experience persistent or severe side effects, your prescriber may recommend slowing the dose escalation, dropping back to a lower dose temporarily, or trying a formulation with additives like glycine and B12 that can help reduce gastrointestinal symptoms. Do not adjust your dose independently. Always work with your healthcare provider to find the right balance between efficacy and tolerability.
Alternative delivery forms of tirzepatide
While this guide focuses on injectable tirzepatide measured with syringes, it is worth knowing that tirzepatide is available (or becoming available) in other delivery formats that eliminate the need for unit-to-mg conversions entirely.
Oral tirzepatide is in development and early availability, with clinical trials showing promising absorption through the GI tract. The oral versus injection comparison is relevant for researchers who dislike needles or struggle with syringe measurements. Orally disintegrating tablets (ODTs) and sublingual drops are additional formats being explored, each with their own dosing systems that bypass the unit measurement confusion entirely.
For researchers currently using injectable tirzepatide who want to understand all available options, our comparison of tirzepatide tablets versus injections covers the pros, cons, and current availability of each format.
Tirzepatide compared to other GLP-1 medications
Tirzepatide is one of several GLP-1 receptor agonists available for weight management and metabolic health. Understanding where it sits in the broader landscape helps inform your dosing decisions and future protocol planning.
The SURMOUNT-5 trial directly compared tirzepatide to semaglutide, demonstrating superior weight loss outcomes at equivalent therapeutic doses. This trial solidified tirzepatide position as the most effective single-agent GLP-1 therapy currently available for weight management.
Newer medications are also entering the pipeline. Retatrutide is a triple-agonist (GLP-1, GIP, and glucagon receptor) that has shown even more dramatic weight loss results in early trials. Survodutide and CagriSema are other next-generation options in development. For researchers currently on tirzepatide who are curious about these alternatives, understanding your current dosing (including what 60 units means at your concentration) provides the baseline for any future conversion discussions with your prescriber.
SeekPeptides tracks developments across the entire GLP-1 medication landscape. Members get access to protocol comparisons, dosing calculators, and evidence-based guides that cover not just tirzepatide but every emerging option in the weight management peptide space.
Frequently asked questions
Is 60 units of tirzepatide a high dose?
It depends entirely on your vial concentration. At 10 mg/mL (the most common concentration), 60 units delivers 6 mg, which is a moderate dose falling between the second and third tiers of the standard escalation schedule. At 20 mg/mL, the same 60 units delivers 12 mg, which is a high dose near the maximum. Always check your concentration before evaluating whether your dose is high or low.
Can I split 60 units into two injections?
Some researchers prefer splitting their weekly dose into two smaller injections (for example, 30 units twice per week instead of 60 units once per week). While this is not the FDA-approved dosing schedule, some prescribers recommend it to reduce gastrointestinal side effects. Discuss with your prescriber before making any changes to your injection schedule.
What if my syringe does not have a 60-unit marking?
If you are using a 1 mL syringe, it should have markings at every 10 units, with 60 clearly labeled. If your syringe uses 2-unit increments between the major markings, count carefully. If your syringe only goes up to 50 units, you have a 0.5 mL syringe and need to switch to a 1 mL syringe. See our syringe guide for help choosing the right size.
Does the amount of bacteriostatic water I used during reconstitution change what 60 units delivers?
Yes, if you reconstituted lyophilized (freeze-dried) tirzepatide yourself. The amount of bacteriostatic water you add determines the final concentration. For example, adding 2 mL of bacteriostatic water to a 10 mg vial creates a 5 mg/mL solution. Adding only 1 mL creates a 10 mg/mL solution. Different concentrations mean 60 units delivers different milligrams. Our bacteriostatic water mixing guide and reconstitution chart cover every scenario.
Is 60 units the same as 0.6 mL?
Yes. On a U-100 insulin syringe, 60 units equals exactly 0.6 mL. This conversion is always true regardless of what medication is in the syringe or what concentration it is. Units measure volume on insulin syringes. The milligrams are what change based on concentration.
How do I know my exact concentration if the label is unclear?
Call your compounding pharmacy directly. Give them your prescription number or order number and ask them to confirm the tirzepatide concentration in mg/mL. Never guess your concentration. A wrong assumption can lead to a dose that is dramatically higher or lower than intended. If you are working with compounded tirzepatide from any of the major compounding pharmacies, their customer service teams can verify your vial details.
Can I use an insulin pen instead of a syringe for compounded tirzepatide?
No. Insulin pens are designed for specific insulin cartridges and cannot be used with compounded tirzepatide vials. You need either a U-100 insulin syringe or a tuberculin syringe to draw from a vial. The only tirzepatide that comes in a pen format is brand-name Mounjaro or Zepbound, which are pre-filled and do not require any measurement.
How many doses can I get from one vial at 60 units per dose?
Divide your total vial volume by 0.6 mL (60 units). A 5 mL vial yields approximately 8 doses at 60 units each (5 divided by 0.6 equals 8.33). A 3 mL vial yields about 5 doses. A 10 mL vial yields about 16 doses. Account for a small amount of waste (medication that remains in the vial or is lost during air removal), so practical yields may be one dose fewer than the math suggests.
External resources
For researchers serious about optimizing their tirzepatide protocols, SeekPeptides provides the most comprehensive resource available, with evidence-based dosing guides, conversion calculators, and a community of thousands who have navigated these exact questions. Members access detailed protocols, dosing calculators, and expert-reviewed content that covers every aspect of peptide research from first injection to long-term optimization.
In case I do not see you, good afternoon, good evening, and good night. May your concentrations stay verified, your measurements stay precise, and your results stay consistent.