Feb 3, 2026

Of all the growth hormone secretagogues that have shaped peptide research over the past three decades, GHRP-6 remains the most polarizing. Some researchers swear by it. Others abandoned it years ago for newer alternatives. And the truth about this hexapeptide sits somewhere between the enthusiastic claims and the cautious dismissals, buried in decades of clinical data that most guides never bother to read.
GHRP-6, or Growth Hormone Releasing Peptide-6, was one of the first synthetic peptides developed specifically to trigger natural growth hormone release from the pituitary gland. It does not supply exogenous growth hormone. Instead, it convinces your body to produce more of its own. That distinction matters enormously for understanding both its benefits and its limitations. The peptide works through a mechanism entirely separate from traditional HGH therapy, binding to the ghrelin receptor (GHS-R1a) and activating intracellular calcium signaling rather than the cAMP pathway used by GHRH.
But GHRP-6 is not clean. Not selective. Not without consequences.
It raises cortisol. It raises prolactin. And it triggers appetite stimulation so intense that experienced researchers describe it as agonizing hunger within 20 minutes of injection. These are not minor footnotes. They are central to understanding when GHRP-6 makes sense and when a different secretagogue serves the research protocol better.
This guide covers everything researchers need to know about GHRP-6: its mechanism at the cellular level, evidence-backed dosing protocols, a direct comparison against ipamorelin and GHRP-2, real side effect management strategies, and stacking approaches that amplify its effects while minimizing its drawbacks. SeekPeptides has compiled the research so you do not have to piece together contradictory forum posts and vendor marketing pages. The data is here. All of it.
What is GHRP-6 and how does it work?
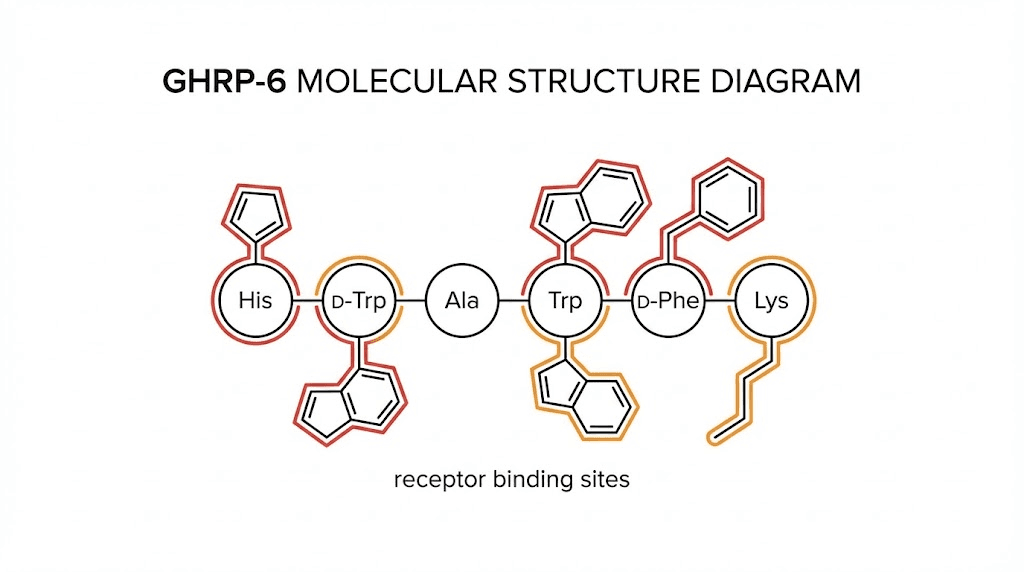
GHRP-6, formally known as Growth Hormone Releasing Hexapeptide, is a synthetic six-amino-acid peptide with the sequence His-DTrp-Ala-Trp-DPhe-Lys-NH2. It appeared as the first in-line synthetic peptide that specifically triggered growth hormone release in a dose-dependent manner, both in cell cultures and in living organisms. Its molecular mass is 873 Daltons, making it a small, stable compound that researchers have studied extensively since the early 1980s.
Small peptide. Massive impact.
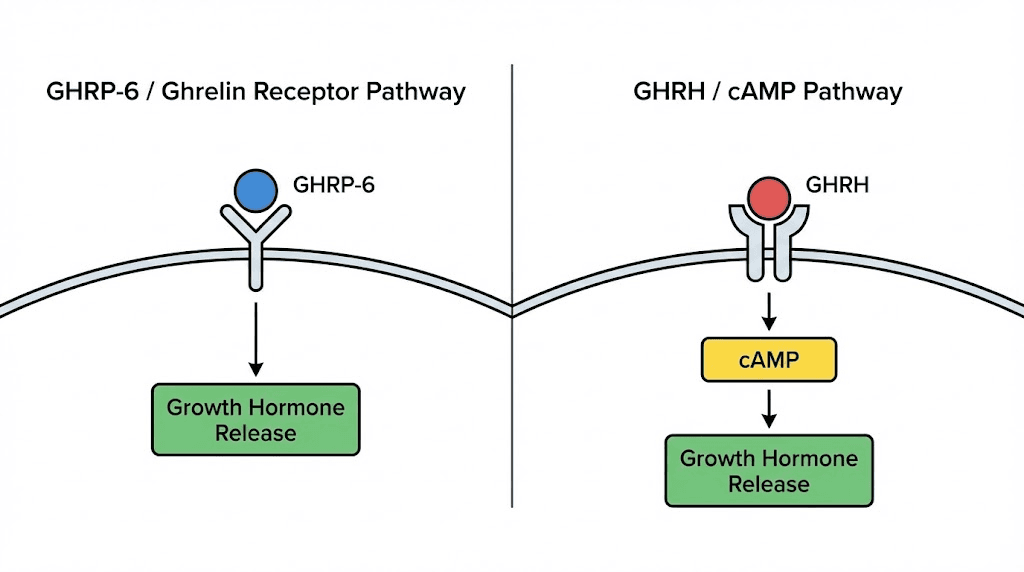
The way GHRP-6 triggers growth hormone release is fundamentally different from GHRH-based peptides like CJC-1295. GHRH works through cAMP-dependent signaling. GHRP-6 does not. Instead, it activates the GH secretagogue receptor 1a (GHSR1a), the same receptor that the natural hormone ghrelin binds to. This activation triggers protein kinase C (PKC) and mobilizes intracellular calcium reserves through the inositol trisphosphate/diacylglycerol pathway. The result is a powerful, pulsatile burst of growth hormone from the anterior pituitary.
Research on human pituitary somatotroph cells demonstrated that GHRP-6 produces potent effects on membrane phosphatidylinositol turnover. This is the second messenger system that leads to PKC activation and calcium mobilization. It is a completely separate signaling cascade from the one GHRH uses, which is precisely why combining the two produces synergistic rather than additive effects on growth hormone output.
GHRP-6 also binds to the ectodomain of CD36, a receptor involved in fatty acid uptake, angiogenesis, and immune function. This dual-receptor activity partly explains the peptide broad pharmacological profile that extends well beyond simple GH secretion into cardioprotection, cytoprotection, and tissue repair.
The hypothalamic connection
GHRP-6 does not act exclusively at the pituitary level. Research has confirmed a dual mechanism involving both the pituitary gland and the hypothalamus. Studies using GHRH antagonists showed that blocking hypothalamic GHRH largely eliminated the growth hormone response to GHRP-6. This means that while GHRP-6 can directly stimulate pituitary somatotrophs, it requires endogenous GHRH for maximal effect.
This finding has practical implications. It means GHRP-6 works best when the hypothalamic-pituitary axis is intact and functional. Patients with hypothalamopituitary disconnection showed complete blockade of the GHRP-6 response, confirming the importance of the hypothalamic pathway. For most researchers with normal pituitary function, this is not a concern. But it explains why GHRP-6 results can vary significantly between individuals, because the health of the entire GH axis matters, not just the pituitary response.
GHRP-6 also functions as a functional somatostatin antagonist at the pituitary level. Somatostatin normally puts the brakes on growth hormone release. GHRP-6 partially overrides that brake, allowing GH pulses to occur even during periods when somatostatin tone would normally suppress them. This is one reason GHRP-6 remains effective even in aging populations where somatostatin activity tends to increase.
Why GHRP-6 is different from HGH injections
Direct HGH injections supply exogenous growth hormone. The body receives a flat dose, processes it, and the negative feedback loop eventually suppresses endogenous production. Over time, the pituitary produces less GH on its own because it no longer needs to.
GHRP-6 takes the opposite approach. It stimulates the pituitary to release its own stored GH in natural, pulsatile bursts. The negative feedback mechanisms stay more balanced because the body is still controlling the process. The amplitude increases, but the rhythm remains physiological. This distinction matters for long-term research protocols where maintaining endogenous GH production is important.
Understanding what peptides are and how they signal at the receptor level helps researchers appreciate why GHRP-6 produces different outcomes than direct GH replacement. The pulsatile pattern of release, the preservation of feedback loops, and the activation of multiple receptor systems all contribute to a pharmacological profile that cannot be replicated by simply injecting recombinant growth hormone.
GHRP-6 benefits backed by research
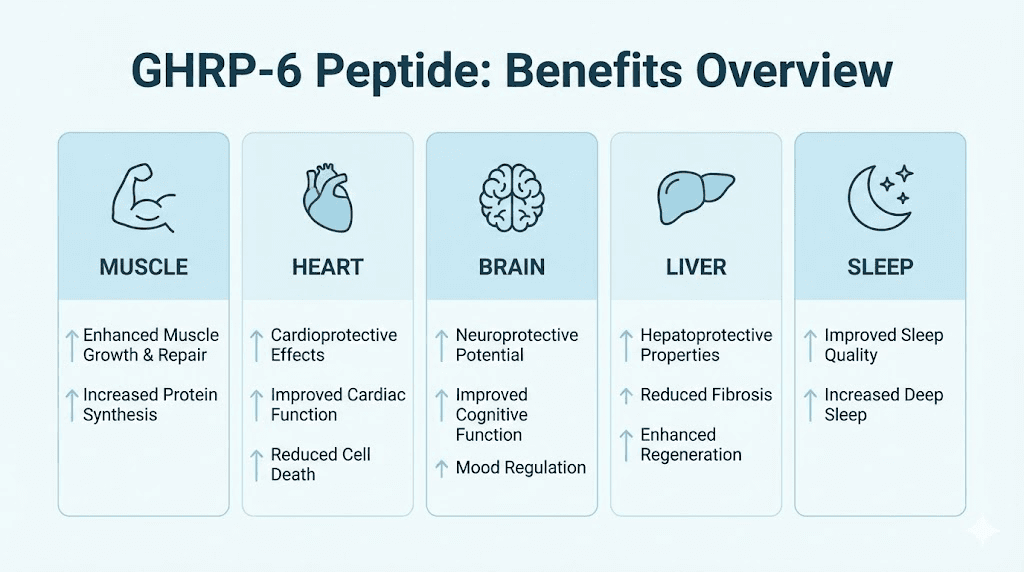
The benefits of GHRP-6 extend far beyond simple growth hormone elevation. Over three decades of research have revealed a pharmacological profile that includes cardioprotection, neuroprotection, tissue repair, metabolic modulation, and immune support. Here is what the evidence actually shows.
Growth hormone and IGF-1 elevation
The primary and most well-documented benefit of GHRP-6 is its ability to stimulate robust growth hormone release. Clinical studies in normal subjects showed GH secretion of 1434.8 plus or minus 393.0 after GHRP-6 administration alone, compared to 483.7 plus or minus 99.2 after GHRH alone. When combined with GHRH, the result was a striking synergistic response of 3771.5 plus or minus 399.6, roughly 2.6 times higher than GHRP-6 alone.
This elevated GH triggers the liver to secrete IGF-1 (Insulin-like Growth Factor 1), a hormone that drives many of the downstream effects associated with growth hormone therapy. IGF-1 improves the body ability to build lean muscle tissue, metabolize stored fat, and accelerate tissue repair. The elevation is dose-dependent up to a saturation point, which research places at approximately 1 mcg per kilogram of body weight per injection.
One critical finding: aging does not significantly blunt the GHRP-6 response. A study published in the Journal of Clinical Endocrinology found that GH responses to GHRP-6 are much greater than to GHRH in late adulthood. The researchers concluded that impaired GH secretion in aging is a functional and potentially reversible state, not a permanent decline. This makes GHRP-6 particularly interesting for longevity-focused research.
Muscle growth and protein synthesis
The GH and IGF-1 elevation from GHRP-6 directly supports lean muscle protein synthesis and muscle fiber repair. A study testing a newly synthesized GHRP-6-biotin conjugate on cultured myoblasts confirmed that the peptide induced expression of myogenic proteins and elevated IGF-1 levels at the cellular level.
For researchers interested in body composition, GHRP-6 occupies a unique niche. The GH pulses it produces support both anabolic (muscle-building) and lipolytic (fat-burning) processes simultaneously. A study in normal mice showed significant differences in body composition, muscle growth, glucose metabolism, memory, and cardiac function in the mice administered GHRP-6 compared to controls.
The appetite stimulation that comes with GHRP-6 can actually be an advantage during muscle building phases. Researchers who struggle to maintain caloric surplus find that GHRP-6 induced hunger makes it significantly easier to consume the surplus calories needed for growth. This is why many experienced researchers specifically choose GHRP-6 over more selective alternatives during bulking protocols.
Cardioprotective effects
Perhaps the most exciting area of GHRP-6 research is its cardioprotective properties. The evidence here is substantial and growing. GHRP-6 has proved to prevent and attenuate cardiac cell death and left ventricular failure in multiple experimental scenarios.
A 2024 study published in Frontiers in Pharmacology examined GHRP-6 ability to protect against doxorubicin-induced cardiotoxicity (doxorubicin is a chemotherapy drug notorious for damaging the heart). The results were remarkable. GHRP-6 administration prevented myocardial fiber consumption and ventricular dilation, effectively preserving left ventricular systolic function. Mechanistically, GHRP-6 sustained cellular antioxidant defense, upregulated the prosurvival gene Bcl-2, and preserved cardiomyocyte mitochondrial integrity.
The cardioprotective effects operate through the CD36 receptor, which is broadly expressed throughout the cardiovascular system.
This is separate from the GH-releasing activity. GHRP-6 demonstrated safety when administered alongside metoprolol, a beta-blocker, with no pharmacological interaction detected. This dual-receptor pharmacology, GH release through GHSR1a and cardioprotection through CD36, gives GHRP-6 a therapeutic profile that newer, more selective secretagogues like ipamorelin do not possess.
Cytoprotective and anti-fibrotic properties
GHRP-6 belongs to a class of peptides that have demonstrated cytoprotective effects, meaning they protect cells from damage and death across multiple organ systems. The evidence spans liver protection, kidney protection, and systemic anti-fibrotic activity.
In hepatoprotection studies, GHRP-6 administration attenuated the effects of lipopolysaccharide (LPS) on circulating levels of transaminases, nitrites/nitrates, and TNF-alpha. The molecular mechanism involves the PI3K/AKT1 pathway, a major cell survival signaling cascade. The exogenous administration of GHRP-6 appeared to exert a potent hepatoprotective role by attenuating the inflammatory response orchestrated by liver-resident macrophages.
The anti-fibrotic properties extend beyond single organs. GHRP-6 has demonstrated the ability to reduce fibrotic tissue formation in cardiac, hepatic, and other tissue models. For researchers studying tissue repair and regeneration, this anti-fibrotic activity is particularly relevant because fibrosis (excessive scar tissue formation) is often the limiting factor in functional recovery.
Neuroprotective potential
Researchers have opened unprecedented avenues by combining GHRP-6 with Epidermal Growth Factor (EGF) as a therapeutic approach for neurological conditions. In animal models, this combination has been used to study damage amelioration in multiple sclerosis, peripheral axonal pathology, and brain ischemia. The combined action produced better outcomes in both clinical and pathological measurements than either compound alone.
The memory improvements observed in the mouse study mentioned earlier add another dimension to GHRP-6 neuroprotective profile. For researchers interested in cognitive enhancement peptides, GHRP-6 combination protocols represent an area of active investigation that extends well beyond what the single-peptide studies would suggest.
Sleep quality improvement
Growth hormone is intimately linked to sleep architecture, with the largest natural GH pulse occurring during deep slow-wave sleep. GHRP-6 administered before bed amplifies this natural pulse, and many users report improved sleep quality, deeper sleep, and more vivid dreams.
This connection between GH secretagogues and sleep optimization makes evening dosing particularly strategic.
One caveat: GHRP-6 has been associated with reduction of the slow-wave sleep phase at higher doses in some research. This appears to be dose-dependent, with moderate doses enhancing sleep quality while excessive doses may paradoxically impair deep sleep architecture. Finding the right dose is essential, which brings us to protocols.
GHRP-6 dosage protocols and administration
Getting GHRP-6 dosing right requires understanding the saturation dose concept, timing windows, and the relationship between dose and side effects. Too little produces minimal GH elevation. Too much does not increase GH further but does amplify cortisol, prolactin, and appetite side effects. The sweet spot is well-defined by research.
The saturation dose principle
Research has established that the optimal single dose of GHRP-6 is approximately 1 mcg per kilogram of body weight. For an 80 kg individual, that is 80 mcg per injection. Decreased doses produce less significant increases in growth hormone concentration. But here is the key finding: exceeding the saturation dose does not produce proportionally higher GH secretion. You hit a ceiling.
In practical terms, this means doses of 100 mcg per injection represent the efficiency sweet spot for most individuals. One study found that 300 mcg per day produced greater total GH increases than 100 mcg per day. Other research found that 50-100 mcg per day was effective, with higher doses showing diminishing returns on GH but increasing returns on side effects.
The SeekPeptides peptide calculator can help determine exact dosing based on body weight and vial concentration.
Standard dosing protocol
Goal: Maximize GH pulses while keeping side effects manageable
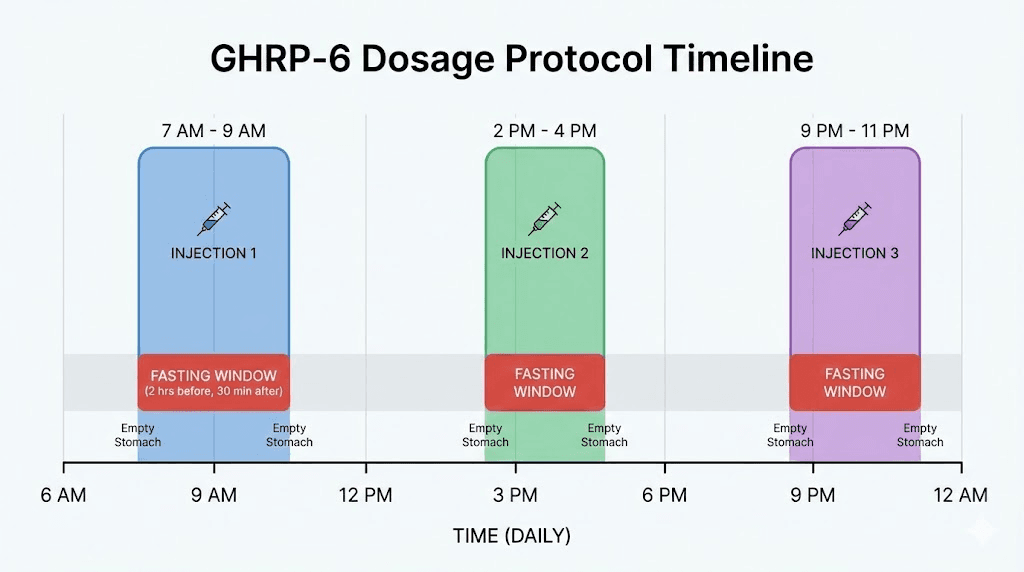
Dose: 100 mcg per injection, 2-3 times daily
Timing:
Dose 1: Immediately upon waking (fasted)
Dose 2: Immediately post-workout
Dose 3: 30 minutes before bed
Administration route: Subcutaneous injection (preferred) or intramuscular. Most researchers prefer subcutaneous for convenience and consistency. Intramuscular results in slightly quicker absorption but no meaningful difference in total GH release.
Cycle length: 8-12 weeks, though some protocols extend to 16 weeks
The spacing between doses matters. At least 3 hours between injections is required to allow the pituitary to restore its GH reserves. Injecting more frequently than every 3 hours produces diminishing returns because the somatotroph cells have not had time to resynthesize and store growth hormone for the next pulse.
Conservative protocol for beginners
Goal: Assess tolerance and response before committing to full dosing
Week 1: 50 mcg once daily (before bed, fasted)
Week 2: 100 mcg once daily (before bed, fasted)
Week 3-4: 100 mcg twice daily (morning and bedtime, both fasted)
Week 5 onward: 100 mcg three times daily (if tolerated)
This graduated approach allows researchers to assess their individual response to the appetite stimulation and any cortisol or prolactin-related effects before committing to full dosing. Some individuals are more sensitive to GHRP-6 hunger effects than others, and discovering this at 50 mcg is far more manageable than discovering it at 300 mcg.
Advanced bulking protocol
Goal: Maximum GH output and appetite stimulation for muscle gain
Dose: 100-200 mcg per injection, 3 times daily
Combined with: Mod GRF 1-29 at 100 mcg per injection (same timing)
Timing:
Dose 1: Upon waking (fasted, 30 minutes before eating)
Dose 2: Post-workout (wait at least 30 minutes after last meal)
Dose 3: Before bed (at least 2 hours after last meal)
Cycle length: 12-16 weeks
The combination with Mod GRF 1-29 (CJC-1295 without DAC) is where GHRP-6 truly shines. The synergistic effect between the two pathways produces GH output significantly higher than either peptide alone. Clinical data shows the combination produces approximately 2.6 times the GH release of GHRP-6 alone. We will cover stacking in detail later in this guide.
The fasting requirement
This cannot be overstated. GHRP-6 must be administered on an empty stomach. Elevated blood glucose or insulin levels significantly blunt the GH response. Dietary fats and carbohydrates consumed around the administration window reduce GH release substantially.
The practical guideline: wait at least 30 minutes after injection before eating, and ensure at least 2 hours have passed since your last meal before injecting. This fasting requirement is one of the more demanding aspects of GHRP-6 protocols, particularly given that the peptide itself triggers intense hunger within 20-30 minutes of injection. Researchers who can tolerate that hunger window and wait before eating will see significantly better GH response than those who eat immediately.
For those who find the fasting window challenging, using a structured peptide dosing schedule helps maintain consistency. Planning meals around injection windows rather than the other way around makes the protocol sustainable over multi-week cycles.
Reconstitution and storage
GHRP-6 typically comes as a lyophilized (freeze-dried) powder in 5 mg or 10 mg vials. Reconstitution follows standard peptide preparation:
1. Use bacteriostatic water (not sterile water, which lacks the preservative needed for multi-use vials)
2. Add water slowly, directing the stream against the vial wall, not directly onto the powder
3. Gently swirl to dissolve. Never shake.
4. For a 5 mg vial reconstituted with 2.5 mL of bacteriostatic water, each 0.05 mL (5 units on an insulin syringe) equals 100 mcg
Store reconstituted GHRP-6 in the refrigerator at 2-8 degrees Celsius. Properly stored, reconstituted GHRP-6 remains stable for approximately 4-6 weeks in the fridge. Unreconstituted lyophilized powder can be stored at room temperature for short periods or in the refrigerator/freezer for extended shelf life. The peptide reconstitution calculator can help determine exact water volumes for your target concentration.
GHRP-6 side effects and how to manage them
GHRP-6 is not a clean peptide. That is not a criticism. It is a factual assessment of its selectivity profile. Understanding the side effects, their mechanisms, and management strategies separates informed research from guesswork.
Appetite stimulation (the big one)
GHRP-6 triggers appetite stimulation so intense that it stands alone among growth hormone secretagogues. No other peptide in this class produces anything comparable. The mechanism is direct: GHRP-6 binds to the ghrelin receptor, and ghrelin is the hunger hormone. Within 20-30 minutes of injection, most researchers experience what can only be described as urgent, sometimes agonizing hunger.
This is not subtle. This is not a gentle increase in appetite. This is a primal, immediate need to eat that can derail dietary plans if researchers are unprepared for it.
Management strategies:
Schedule injections around planned meal times so the hunger aligns with eating
Prepare meals in advance so you are not making impulsive food choices while ravenously hungry
Start with lower doses (50-100 mcg) to assess individual sensitivity before increasing
For cutting phases, consider switching to ipamorelin which produces minimal appetite stimulation
Some researchers embrace this side effect. During bulking phases where caloric surplus is the goal, GHRP-6 induced hunger makes it significantly easier to consume 4,000-5,000 calories daily. The appetite effect is a bug for cutting. It is a feature for gaining.
Cortisol elevation
GHRP-6 increases ACTH (adrenocorticotropic hormone) and subsequently cortisol levels. Cortisol is a stress hormone that, when chronically elevated, promotes fat storage (particularly visceral fat), breaks down muscle tissue, impairs sleep, and suppresses immune function. Research confirms that GHRP-6 produces a mild but measurable increase in cortisol with each injection.
The dose-response relationship matters here. Studies showed that at doses of 100 mcg or less, cortisol increases were minimal. Higher doses amplify the cortisol response without proportionally increasing GH output. This is one of the strongest arguments for staying at or near the 100 mcg per injection saturation dose rather than escalating higher.
Management strategies:
Keep individual doses at 100 mcg or below
Limit total daily GHRP-6 exposure to 300 mcg
Prioritize the bedtime dose (cortisol is naturally lowest at night)
Monitor for signs of cortisol excess: disrupted sleep, increased abdominal fat, mood changes
Consider cycling 8 weeks on, 4 weeks off to prevent cumulative cortisol effects
Prolactin elevation
GHRP-6 can increase prolactin secretion, though the clinical significance varies by dose and individual sensitivity. At 100 mcg or less, prolactin increases are generally minimal and clinically insignificant. At higher doses, some individuals, particularly those predisposed to prolactin sensitivity, may experience symptoms including mood changes, sexual dysfunction, and in rare cases, mild gynecomastia.
Management strategies:
Keep doses at 100 mcg per injection
If prolactin-related symptoms emerge, vitamin B6 (P-5-P form, 50-100 mg daily) can help
More significant prolactin elevation may require pharmaceutical management with a healthcare provider
Consider switching to ipamorelin, which does not significantly elevate prolactin at any dose
Water retention and joint effects
The elevated GH levels produced by GHRP-6 can cause fluid retention, manifesting as bloating, puffiness (particularly in the face and extremities), and joint stiffness. This is not unique to GHRP-6. It occurs with any GH-elevating compound. The retained water can put pressure on neurovascular structures, leading to numbness and tingling in the extremities, and in some cases, symptoms resembling carpal tunnel syndrome.
These effects are dose-dependent and typically reversible upon dose reduction or cessation.
Management strategies:
Stay well-hydrated (counterintuitive but effective, as proper hydration helps regulate fluid balance)
Monitor sodium intake
If numbness or tingling develops, reduce the dose
Joint stiffness typically resolves within 1-2 weeks of starting the protocol as the body adjusts
Blood glucose effects
GHRP-6 can influence glucose metabolism and insulin sensitivity. Growth hormone itself is a counter-regulatory hormone that opposes insulin action, and GHRP-6 induced GH elevation can increase fasting blood glucose. Some users report pseudoglycemia, a condition characterized by dizziness, weakness, slight limb tremor, and hunger that occurs even when blood glucose is technically normal. The body perceives a rapid shift in glucose utilization as hypoglycemia even when actual blood sugar levels are adequate.
Long-term effects on insulin sensitivity remain under investigation. Researchers with pre-existing insulin resistance or metabolic concerns should exercise caution and monitor blood glucose throughout the protocol.
Head rush and injection site reactions
Many GHRP-6 users report a characteristic head rush feeling accompanied by tingling and a pins-and-needles sensation in the extremities shortly after injection. This typically lasts 5-15 minutes and is considered a normal physiological response rather than a concerning side effect. Injection site reactions (redness, mild swelling) are common with subcutaneous peptide administration and are not specific to GHRP-6.
For proper peptide injection technique and site rotation strategies, a structured approach helps minimize local reactions over long protocols.
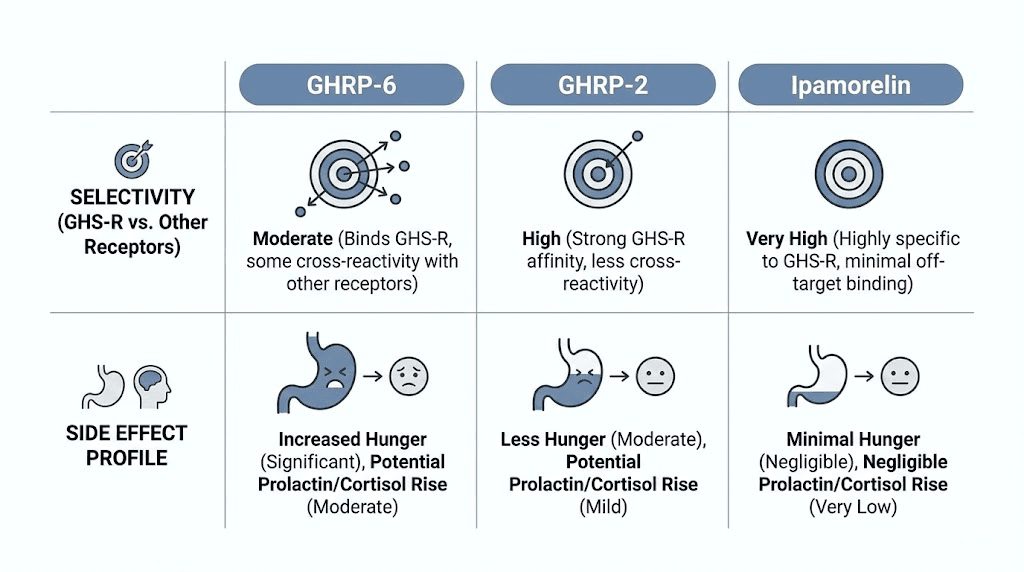
GHRP-6 vs GHRP-2 vs ipamorelin: which secretagogue is right for your protocol?
This is the question every researcher eventually faces. Three growth hormone releasing peptides, three generations, three different selectivity profiles. The choice matters more than most guides acknowledge.
GHRP-6: the first generation powerhouse
GHRP-6 was the first synthetic GHRP developed for GH-releasing activity. It is potent, well-studied, and effective. But it is not selective. Along with strong GH release, it produces significant appetite stimulation through ghrelin receptor activation, mild to moderate cortisol and prolactin elevation, and the most intense hunger response of any peptide in this class.
Best suited for:
Bulking and mass-gaining phases where appetite stimulation is beneficial
Researchers who need robust GH pulses and can manage the side effect profile
Protocols where cardioprotective benefits are desirable (GHRP-6 unique CD36 activity)
Budget-conscious protocols (GHRP-6 is typically the least expensive option)
GHRP-2: the refined second generation
GHRP-2 was developed specifically to improve upon GHRP-6 limitations. It produces slightly stronger GH release (research suggests it is the most potent of the three for raw GH output) with less appetite stimulation, reduced cortisol elevation, and lower prolactin increases compared to GHRP-6.
Best suited for:
Researchers who want strong GH release with fewer side effects than GHRP-6
Protocols where moderate appetite control is needed
Recomposition phases (simultaneous fat loss and muscle gain)
Ipamorelin: the selective third generation
Ipamorelin represents the most selective GHRP available. Research published in the Journal of Endocrinology demonstrated that while GHRP-6 and GHRP-2 both increased ACTH and cortisol, ipamorelin did not produce ACTH or cortisol levels significantly different from those observed following GHRH stimulation alone. It produces GH release comparable to GHRP-6 in potency but without the appetite stimulation, cortisol elevation, or prolactin increase.
Best suited for:
Cutting and fat loss phases where appetite control matters
Long-term protocols where hormonal cleanliness is prioritized
Researchers sensitive to cortisol or prolactin elevation
Female researchers who want to avoid prolactin-related effects
Head-to-head comparison table
Factor | GHRP-6 | GHRP-2 | Ipamorelin |
|---|---|---|---|
GH release potency | Strong | Strongest | Comparable to GHRP-6 |
Appetite stimulation | Very strong | Mild | Minimal |
Cortisol increase | Yes (moderate) | Yes (mild) | No significant increase |
Prolactin increase | Yes (moderate) | Yes (mild) | No significant increase |
Selectivity | Low | Moderate | Highest |
Cardioprotection | Strong (CD36) | Limited | Limited |
Best phase | Bulking | Recomp | Cutting/long-term |
Cost | Lowest | Moderate | Moderate |
The honest assessment: ipamorelin is the better choice for most research protocols. It matches GHRP-6 GH output without the appetite, cortisol, and prolactin baggage. GHRP-6 earns its place in protocols where the appetite stimulation is specifically desired (bulking), where cardioprotective benefits are prioritized, or where budget is the primary constraint.
For a broader comparison of growth hormone peptide strategies, the peptide stacking guide covers how different secretagogues combine with GHRH analogues for optimal results.
Stacking GHRP-6 with GHRH peptides for maximum effect
GHRP-6 alone produces meaningful GH elevation. GHRP-6 combined with a GHRH analogue produces GH elevation that is dramatically, synergistically greater than either compound alone. This is not marketing. This is validated clinical data.
The science behind the synergy
GHRP-6 and GHRH peptides work through completely different receptor systems and intracellular pathways. GHRP-6 activates GHSR1a using calcium-dependent PKC signaling. GHRH activates GHRH receptors using cAMP-dependent PKA signaling. When both pathways fire simultaneously, the pituitary somatotrophs release GH in quantities that far exceed the sum of what each peptide would produce individually.
The clinical numbers tell the story clearly. In normal subjects:
GHRH alone: GH secretion of 483.7
GHRP-6 alone: GH secretion of 1434.8
GHRH plus GHRP-6: GH secretion of 3771.5
The combined output is not 1918.5 (the additive sum). It is 3771.5, nearly double the additive prediction. That is true pharmacological synergy. And it happens because two independent signaling cascades are converging on the same cellular output.
GHRP-6 plus Mod GRF 1-29 (CJC-1295 without DAC)
This is the most common and well-validated GHRP-6 stack. Mod GRF 1-29, also known as CJC-1295 without DAC, is a synthetic analogue of GHRH with four amino acid substitutions that make it resistant to enzymatic degradation while maintaining a short half-life suitable for pulsatile dosing.
Protocol:
GHRP-6: 100 mcg per injection
Mod GRF 1-29: 100 mcg per injection
Frequency: 2-3 times daily (same timing, mixed in the same syringe or injected sequentially)
Timing: Upon waking (fasted), post-workout, and before bed (fasted)
Cycle length: 12-16 weeks
The short half-life of Mod GRF 1-29 (without DAC) matches GHRP-6 pulsatile release profile. Both peptides act quickly, produce a GH pulse, and clear the system before the next dose. This maintains the natural pulsatile pattern that the hypothalamic-pituitary axis expects, reducing the risk of desensitization.
GHRP-6 plus CJC-1295 with DAC
CJC-1295 with DAC (Drug Affinity Complex) has a much longer half-life, lasting days rather than minutes. This means it provides a sustained elevation of baseline GH rather than sharp pulses. Some researchers combine it with GHRP-6 to get both elevated baseline GH (from the DAC version) and sharp pulsatile bursts (from GHRP-6).
This combination is more aggressive and less physiological than the Mod GRF 1-29 stack. The sustained GH elevation from DAC can increase side effects including water retention and insulin resistance. Most experienced researchers prefer the Mod GRF 1-29 approach for its cleaner, more controllable profile.
Multi-peptide stacking considerations
Some advanced protocols combine GHRP-6 with other peptides beyond GHRH analogues. Common additions include:
BPC-157 for injury healing: The GH elevation from GHRP-6 complements BPC-157 direct tissue repair mechanisms. This stack is popular among researchers dealing with tendon injuries and joint problems.
TB-500 for systemic healing: TB-500 and GHRP-6 work through entirely different mechanisms, making them complementary. The BPC-157 and TB-500 stacking guide provides detailed protocols for combining healing peptides.
IGF-1 LR3 for direct anabolic effects: Some protocols add IGF-1 LR3 to capitalize on both the endogenous IGF-1 elevation from GHRP-6 and the exogenous IGF-1 from direct administration. This is an advanced approach with significant complexity. Understanding how many peptides can be safely combined requires careful protocol design.
The peptide stack calculator on SeekPeptides can help plan multi-peptide protocols with appropriate timing and dosing.
GHRP-6 for specific research goals
Different research objectives call for different GHRP-6 approaches. Here are targeted protocols based on specific goals.
Muscle growth and body composition
GHRP-6 supports muscle growth through elevated GH and IGF-1 levels. The appetite stimulation makes it particularly suitable for caloric surplus phases. Researchers targeting lean mass gains typically combine GHRP-6 with resistance training protocols and adequate protein intake (1.6-2.2 g per kg body weight).
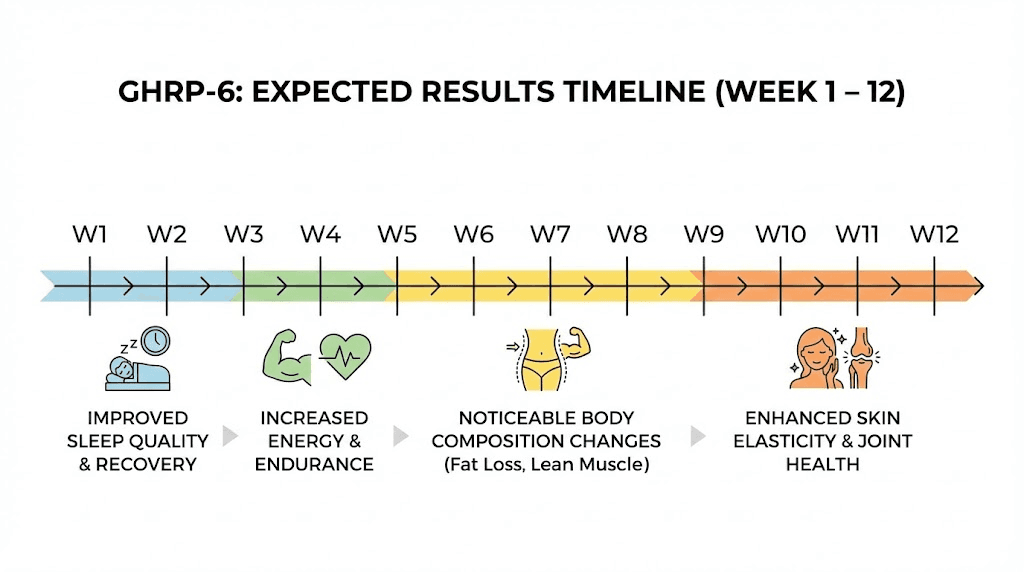
Expected timeline:
Week 1-2: Improved sleep quality, increased appetite, possible water retention
Week 3-4: Improved recovery between training sessions, subtle body composition changes
Week 6-8: Noticeable improvements in lean mass and strength when combined with training
Week 8-12: Full body composition effects become apparent
For those comparing peptide approaches to anabolic steroids, GH secretagogues like GHRP-6 work through fundamentally different mechanisms. They do not suppress testosterone production or carry the same androgenic risks. The trade-off is that the anabolic effect is more subtle and takes longer to manifest.
Fat loss and metabolic optimization
Growth hormone is a potent lipolytic hormone, meaning it promotes the breakdown of stored fat for energy. GHRP-6 induced GH pulses enhance lipolysis, particularly when timed with fasting periods. The morning (fasted) injection capitalizes on the overnight fast, and the pre-bed injection extends the GH elevation through the natural nocturnal GH pulse.
The challenge: GHRP-6 appetite stimulation works directly against fat loss protocols. The intense hunger it produces can lead to overeating, negating the metabolic benefits of elevated GH. Researchers focused primarily on fat burning typically achieve better results with ipamorelin or AOD-9604, which provide GH-related fat metabolism benefits without the hunger drive.
If GHRP-6 is used during a fat loss phase, strict meal planning and preparation become non-negotiable. Having pre-measured, calorie-appropriate meals ready to consume within the eating window after injection prevents impulsive overconsumption.
Recovery and injury healing
Elevated GH and IGF-1 accelerate tissue repair processes throughout the body. GHRP-6 combined with dedicated healing peptides like BPC-157 and TB-500 creates a multi-pathway approach to recovery. The GH elevation supports systemic healing factors while the targeted peptides work on specific tissue repair mechanisms.
For shoulder injuries, back pain, and bone healing, the combination of GHRP-6 systemic GH elevation with localized peptide therapy has generated significant interest among researchers.
Anti-aging and longevity
Growth hormone declines with age. This decline is called somatopause, and it contributes to many age-related changes: loss of muscle mass, increased body fat, decreased bone density, impaired cognitive function, reduced skin elasticity, and weakened immune response. GHRP-6 research in aging populations has produced encouraging results.
The aging study showed that GH responses to GHRP-6 are well-preserved into late adulthood, and the combination of GHRP-6 plus GHRH maintained full synergistic activity. The researchers explicitly stated that impaired GH secretion in aging is a functional and potentially reversible state. This is a significant finding for longevity-focused peptide research.
The anti-aging peptide landscape extends well beyond GH secretagogues. Combining GHRP-6 with epitalon (telomerase activation), bioregulator peptides (organ-specific rejuvenation), and SS-31 (mitochondrial support) represents the frontier of multi-target anti-aging protocol design.
Cardiac research applications
GHRP-6 unique cardioprotective properties through CD36 receptor activation make it the only GH secretagogue with direct cardiovascular applications. The 2024 doxorubicin study demonstrated preservation of left ventricular function, mitochondrial integrity, and anti-fibrotic activity. For researchers studying cardiac peptides, GHRP-6 occupies a unique position that neither GHRP-2 nor ipamorelin can replicate.
The clinical safety data showing no interaction between GHRP-6 and metoprolol is also significant. It suggests that GHRP-6 could potentially be combined with standard cardiovascular medications without pharmacological interference, though any such combination would require proper medical supervision.
Practical GHRP-6 cycle planning
Running an effective GHRP-6 cycle requires more than just injecting at the right times. Proper cycle planning accounts for desensitization, protocol cycling, monitoring, and exit strategy.
Cycle duration and desensitization
The pituitary gland can develop reduced sensitivity to repeated GHRP-6 stimulation over time. This desensitization is more theoretical than dramatically demonstrated in research, but most experienced practitioners recommend cycling to maintain optimal responsiveness.
Standard cycle structure:
On cycle: 8-12 weeks of daily dosing
Off cycle: 4 weeks without GHRP-6 (Mod GRF 1-29 can be continued during off-cycle if desired)
Repeat
Some researchers run longer cycles of 16-20 weeks, particularly when GHRP-6 is part of a structured peptide cycle. The key monitoring point is whether the side effects (particularly the head rush and hunger response) remain consistent. If they diminish noticeably, the pituitary may be desensitizing, and a break is warranted.
What to monitor during the cycle
Smart researchers track objective markers, not just subjective feelings.
Body composition: Regular measurements (weight, body fat percentage, waist circumference) provide objective feedback. Photos under consistent lighting conditions are more reliable than scale weight alone, as GHRP-6 water retention can mask fat loss and muscle gain on the scale.
Sleep quality: GH secretagogues should improve deep sleep. If sleep quality deteriorates, dose timing or total daily dose may need adjustment.
Appetite patterns: The hunger response should remain consistent throughout the cycle. Diminishing appetite stimulation may indicate developing desensitization.
Injection site reactions: Monitor for any developing sensitivity at injection sites. Proper injection technique and site rotation minimize this risk.
Blood work (if accessible): Pre-cycle and mid-cycle blood panels can reveal changes in IGF-1 levels, fasting glucose, and prolactin. These provide the most objective assessment of both efficacy and side effect burden.
Post-cycle considerations
Unlike anabolic steroids or direct HGH injections, GHRP-6 does not require a complex post-cycle therapy (PCT). The peptide stimulates endogenous GH production rather than suppressing it, so the hypothalamic-pituitary axis is not shut down in the way it would be with exogenous hormone administration.
When stopping GHRP-6:
GH levels will return to baseline within days of cessation
Water retention will resolve within 1-2 weeks
Appetite will return to pre-cycle levels quickly (often within 48-72 hours)
Any improvements in body composition achieved during the cycle can be maintained with proper training and nutrition
The peptides versus steroids comparison covers the fundamental differences in how these two approaches affect the endocrine system and recovery requirements.
GHRP-6 and the broader growth hormone secretagogue landscape
GHRP-6 does not exist in isolation. It is one member of a growing family of compounds that influence GH secretion through various mechanisms. Understanding where GHRP-6 fits in this landscape helps researchers make informed decisions.
The GHRP family tree
The GH secretagogue research program that produced GHRP-6 also spawned several related compounds:
GHRP-1: The earliest compound in the series. Less studied and less commonly available than GHRP-6.
GHRP-6: The first widely studied and commercially available GHRP. Strong GH release, strong appetite stimulation, moderate cortisol and prolactin elevation.
GHRP-2: Second generation. Slightly stronger GH release than GHRP-6 with reduced (but not eliminated) side effects.
Hexarelin: The most potent GHRP for raw GH release but also the most likely to cause desensitization. Some researchers report that hexarelin GH response diminishes significantly within 2-4 weeks of daily use.
Ipamorelin: Third generation, most selective. Comparable GH release to GHRP-6 without the cortisol, prolactin, or appetite effects. The current gold standard for clean GH secretagogue research.
Non-peptide GH secretagogues
The ghrelin receptor can also be activated by non-peptide compounds. Ibutamoren (MK-677) is an oral GH secretagogue that activates the same GHSR1a receptor as GHRP-6. It offers the convenience of oral dosing but shares many of GHRP-6 drawbacks including appetite stimulation and cortisol/prolactin elevation. For researchers comparing peptides versus SARMs and other research compounds, understanding these mechanistic overlaps matters.
Where GHRP-6 still wins
Despite being a first-generation compound, GHRP-6 retains several unique advantages:
1. Cardioprotection: The CD36-mediated cardioprotective effects are unique to GHRP-6 among the commonly available secretagogues. No other GHRP has demonstrated comparable cardiac benefits.
2. Cost: GHRP-6 remains the most affordable GH secretagogue, making it accessible for researchers on limited budgets.
3. Research depth: With over 30 years of published research, GHRP-6 has the most extensive evidence base of any GH secretagogue. This matters for researchers who prioritize data over novelty.
4. Appetite utility: For mass-gaining protocols, the appetite stimulation is genuinely useful. No other legal compound produces such reliable, intense appetite enhancement.
5. Combination synergies: The combination of GHRP-6 with EGF for neurological applications is unique and has no equivalent with other secretagogues.
Frequently asked questions
How quickly does GHRP-6 start working?
GHRP-6 produces measurable GH elevation within 15-30 minutes of subcutaneous injection. Appetite stimulation occurs within 20-30 minutes. Subjective effects like improved sleep quality may be noticed within the first few days. Body composition changes require 4-8 weeks of consistent use to become noticeable. Full effects on lean mass and recovery typically manifest over 8-12 weeks.
Can GHRP-6 be taken orally?
While GHRP-6 has shown some oral bioavailability in research (it is described as effective when orally administered in early studies), subcutaneous injection remains the standard administration route. Oral bioavailability is significantly lower than injection, requiring much higher doses to achieve comparable GH release. Nasal spray and oral capsule formulations are areas of ongoing research but not yet standard practice for GHRP-6.
Does GHRP-6 show up on drug tests?
GH secretagogues including GHRP-6 are prohibited by WADA (World Anti-Doping Agency) in competitive sports. Detection methods have improved significantly, and metabolites can be identified in urine samples. For researchers concerned about testing implications, the peptide drug testing guide provides detailed information on detection windows and testing methods.
Is GHRP-6 legal?
GHRP-6 is available for purchase as a research chemical in many jurisdictions. It is not FDA-approved for human therapeutic use. Peptide legality varies by country and intended use. The current regulatory landscape for peptides is evolving rapidly, and researchers should verify compliance with local regulations before acquiring or using any research peptide.
Can GHRP-6 be combined with BPC-157 and TB-500?
Yes. GHRP-6 works through GH secretion pathways while BPC-157 and TB-500 work through direct tissue repair mechanisms. There are no known negative interactions. The BPC-157 plus TB-500 stacking guide covers how to integrate healing peptides with GH secretagogues effectively.
What happens if you eat right after injecting GHRP-6?
Eating immediately after GHRP-6 injection, particularly foods containing carbohydrates or fats, significantly blunts the GH response. The insulin spike from food intake counteracts the GH-releasing signal. For optimal results, wait at least 30 minutes after injection before eating. This is challenging given the intense hunger GHRP-6 produces, but the difference in GH output is substantial.
How does GHRP-6 compare to direct HGH therapy?
Direct HGH therapy supplies exogenous growth hormone. GHRP-6 stimulates endogenous production. HGH provides predictable, controllable doses. GHRP-6 maintains pulsatile release patterns and preserves feedback loops. HGH is significantly more expensive. GHRP-6 is more affordable but less controllable in terms of exact GH output. Both approaches have valid applications depending on the research context.
Should I use GHRP-6 or ipamorelin?
For most research purposes, ipamorelin is the better choice due to its comparable GH release with significantly fewer side effects. Choose GHRP-6 specifically when you want the appetite stimulation (bulking), need the cardioprotective benefits (CD36 activation), or are working within a limited budget. For cutting, recomposition, or long-term protocols, ipamorelin provides a cleaner experience.
Does GHRP-6 affect thyroid function?
Research in patients with hypothyroidism showed that thyroid hormones modulate GH release induced by GHRP-6. Patients with untreated primary hypothyroidism showed blunted GH responses to both GHRH and GHRP-6, though the mechanism differed between the two. This suggests that thyroid function should be optimized before starting GHRP-6 to ensure maximal GH response. Researchers with known thyroid issues should address those first.
How should GHRP-6 be stored?
Unreconstituted GHRP-6 powder should be stored in a cool, dry place. Refrigeration or freezer storage extends shelf life. Once reconstituted with bacteriostatic water, store in the refrigerator at 2-8 degrees Celsius and use within 4-6 weeks. Never freeze reconstituted peptides. The peptide storage guide covers proper handling for all peptide formats.
For researchers serious about optimizing their growth hormone protocols, SeekPeptides provides the most comprehensive resource available, with evidence-based guides, dosing calculators, and a community of researchers who have navigated these exact questions. The peptide calculator handles the math. The protocol guides handle the strategy. And the getting started guide makes the first steps straightforward.
External resources
PMC: Synthetic GHRPs historical appraisal of cytoprotective effects
PubMed: GHRP-6 requires endogenous GHRH for maximal GH stimulation
Frontiers in Pharmacology: GHRP-6 prevents doxorubicin-induced cardiotoxicity
In case I do not see you, good afternoon, good evening, and good night. May your GH pulses stay strong, your pituitary stay responsive, and your protocols stay consistent.