Mar 25, 2026

You finally started semaglutide. The appetite suppression kicked in. The scale started moving. Everything felt like it was working. Then the constipation hit. And it did not just hit once. It settled in like a stubborn houseguest, refusing to leave, making everything uncomfortable, turning what should have been a positive experience into a daily frustration that nobody warned you about.
You are not alone. Not even close. Clinical trial data from the STEP studies show that constipation affects roughly 24% of semaglutide users, compared to just 11% in the placebo group. That is nearly one in four people dealing with this exact problem. And the real-world numbers might be even higher, since clinical trials tend to underreport side effects that participants consider embarrassing or manageable on their own.
So here is the question everyone types into Google at 2 AM while sitting uncomfortably on the couch: can you take a laxative while on semaglutide? The short answer is yes. The longer answer involves understanding which laxatives work best, which ones to avoid, how timing matters, and why the underlying mechanism of semaglutide side effects makes constipation almost predictable once you understand the pharmacology. This guide covers every laxative option, natural alternatives, specific dosages, timing protocols, and the warning signs that mean you need to call a doctor instead of reaching for another dose of MiraLAX.
SeekPeptides members have access to comprehensive side effect management guides that go beyond what most resources cover, including personalized protocols for handling semaglutide side effects at every dose level.
Why semaglutide causes constipation in the first place
Understanding why semaglutide causes constipation is not just academic curiosity. It directly affects which laxative you should choose and how you should use it. The mechanism matters because it tells you whether you are dealing with a temporary adjustment or something that needs ongoing management.
Semaglutide is a GLP-1 receptor agonist. It mimics a hormone your body naturally produces in the gut after eating. One of its primary effects is slowing gastric emptying, which means food stays in your stomach longer. This is actually the mechanism behind appetite suppression. When your stomach empties slowly, you feel full longer, eat less, and lose weight.
But that same slowing does not stop at the stomach.
The entire gastrointestinal tract slows down. Intestinal motility decreases. Peristalsis, the wave-like contractions that push food through your digestive system, becomes sluggish. When transit time increases, your colon absorbs more water from the stool. The result is harder, drier stool that moves through the intestines at a crawl.
Research published in the journal Obesity analyzed pooled data from STEP trials 1 through 3 and found that semaglutide users experienced constipation for a median duration of 47 days. Nearly seven weeks of constipation. That is not a minor inconvenience. That is a quality-of-life issue that deserves a real solution, not just the advice to "drink more water" that most doctors offer in a 15-minute appointment.
The severity typically follows a pattern. Constipation is worst during the dose escalation phase, when your body is adjusting to increasing amounts of the medication. Many people notice improvement once they reach their maintenance dose, but for some, it persists throughout the entire course of treatment. Understanding your own pattern helps you decide whether you need a short-term solution or a longer-term management strategy.
The dose-response relationship
Higher doses of semaglutide generally produce more constipation. This makes intuitive sense because greater GLP-1 receptor activation means more pronounced slowing of gut motility. If you are on the standard escalation schedule, you might notice constipation worsening each time you increase your dose.
The 2.4mg weekly dose used for weight management (Wegovy) tends to cause more GI side effects than the 1mg dose used for diabetes (Ozempic). This is simply because more medication means more receptor activation, which means more slowing of the gut. Your semaglutide dosage directly influences how aggressively you need to manage constipation.
Some researchers have found that splitting semaglutide doses can reduce the peak concentration and potentially decrease side effect intensity, though this approach should only be considered under medical guidance.
Why some people get hit harder than others
Not everyone on semaglutide develops constipation. About 76% of users in clinical trials did not report it at all. Several factors influence your risk.
Pre-existing gut motility issues matter. If you tended toward constipation before starting semaglutide, the medication will almost certainly make it worse. People with thyroid conditions, particularly hypothyroidism, are already predisposed to slow gut transit and should plan for constipation management from day one.
Diet plays a significant role. Many semaglutide users dramatically reduce their caloric intake because of appetite suppression. Less food means less bulk moving through the intestines, which means less stimulation of peristalsis. If you are eating 800 calories a day instead of your previous 2,000, your colon simply has less to work with.
Hydration status amplifies the problem. Semaglutide can cause dizziness and reduced thirst signals. Many users forget to drink adequate water because they are not feeling hungry or thirsty. Dehydration on top of slowed motility is a recipe for severe constipation.
Activity level contributes too. Physical movement stimulates gut motility. If semaglutide-related fatigue has reduced your exercise routine, that further compounds the problem.
The definitive answer: yes, you can take laxatives with semaglutide
Let us address the core question directly. Yes, you can take laxatives while on semaglutide. There are no known contraindications between semaglutide and any major class of laxatives. No clinical studies have identified dangerous interactions. No prescribing information for semaglutide warns against laxative use.
However, there is one important nuance that most sources gloss over.
Laxatives can potentially affect the absorption of oral medications by speeding up intestinal transit. For injectable semaglutide (Ozempic, Wegovy), this is essentially a non-issue because the medication is absorbed through subcutaneous tissue, not the GI tract. Your laxative has no pathway to interfere with absorption of an injected drug.
For oral semaglutide (Rybelsus), the picture is slightly more complicated. Oral semaglutide is absorbed primarily through the stomach lining, not the intestines, which makes it somewhat unique among oral medications. Stimulant laxatives that dramatically speed intestinal transit are unlikely to significantly affect stomach absorption. That said, if you are taking oral semaglutide, spacing your laxative dose at least 30 minutes after taking your semaglutide is a reasonable precaution.
The bottom line: injectable semaglutide users can take laxatives freely. Oral semaglutide users should maintain reasonable timing separation. Neither group needs to worry about dangerous interactions.
Best laxatives for semaglutide constipation: a complete breakdown
Not all laxatives are created equal, and some are significantly better suited for GLP-1-related constipation than others. Here is a detailed breakdown of every major category, ranked by how well they address the specific type of constipation semaglutide causes.
Osmotic laxatives: the gold standard
Osmotic laxatives work by drawing water into the intestines, which softens stool and increases its volume. This directly counteracts the dehydration effect that semaglutide creates in the colon. They are considered the first-line treatment for GLP-1-related constipation by most gastroenterologists.
Polyethylene Glycol 3350 (MiraLAX)
MiraLAX is the single best laxative for semaglutide users. Period. It has no known interactions with semaglutide, minimal systemic absorption (meaning it stays in the gut and does not enter your bloodstream in meaningful amounts), and produces gentle, predictable results without cramping or urgency.
The standard dose is 17 grams (one capful) mixed into 4 to 8 ounces of any beverage, taken once daily. Effects typically appear within 1 to 3 days. Unlike stimulant laxatives, MiraLAX does not cause dependency even with extended use, which matters because your semaglutide-related constipation might persist for weeks or months.
For semaglutide users specifically, consider this protocol:
Mild constipation (skipping 1-2 days): 17g once daily until regular, then as needed
Moderate constipation (skipping 3-4 days): 17g daily for one week, then reassess
Severe constipation (5+ days without a bowel movement): 17g twice daily for 2-3 days, then step down to once daily
MiraLAX can be taken at any time of day, with or without food. Many semaglutide users find that taking it in the morning with their first beverage creates the most consistent results.
Lactulose
Lactulose is a prescription osmotic laxative that works similarly to MiraLAX but through a slightly different mechanism. It is a synthetic sugar that gut bacteria ferment, producing acids that draw water into the colon. The typical dose is 15 to 30ml daily.
The downside of lactulose is bloating and gas. Because it relies on bacterial fermentation, it can cause significant bloating, which many semaglutide users are already dealing with. For most people, MiraLAX is the better choice. Lactulose makes sense primarily for people who cannot tolerate PEG 3350 or who need a prescription option for insurance coverage.
Magnesium-based osmotic laxatives
Magnesium citrate and magnesium hydroxide (Milk of Magnesia) are osmotic laxatives that also provide supplemental magnesium. They work faster than MiraLAX, sometimes within hours, which makes them better for acute episodes but potentially too aggressive for daily use.
Magnesium citrate dosing for constipation: 200 to 400mg daily, taken at bedtime. Start at the lower end and increase as needed.
Magnesium oxide at 400mg before bed is another option that works well as both a laxative and a general supplement. Many semaglutide users are deficient in electrolytes including magnesium, so this approach serves double duty.
Important caution: people with kidney problems should not use magnesium laxatives without medical supervision, as impaired kidneys cannot efficiently clear excess magnesium from the blood.
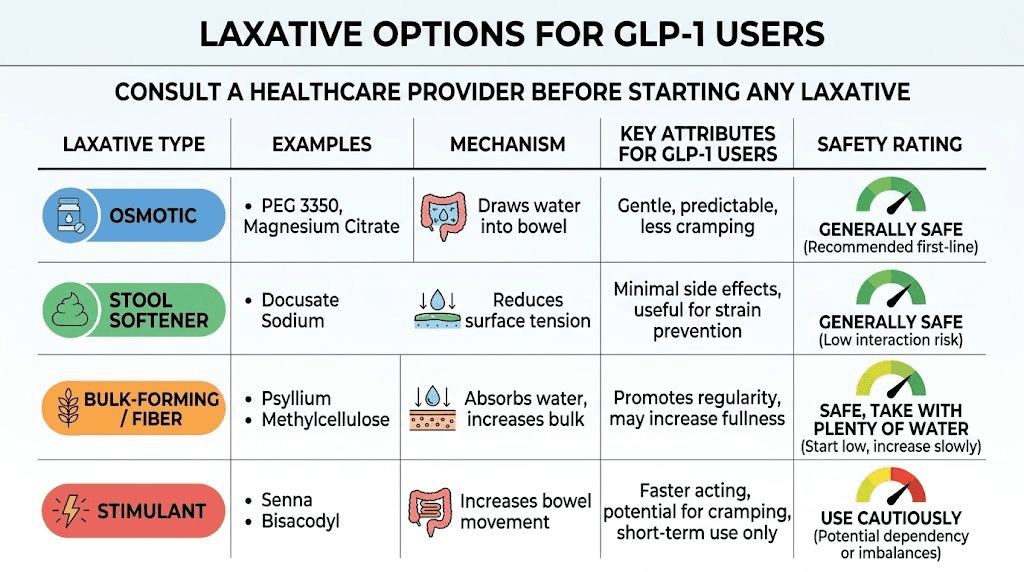
Stool softeners: gentle but limited
Stool softeners work by allowing water and fats to penetrate the stool, making it softer and easier to pass. They do not actively draw water into the intestines or stimulate contractions.
Docusate Sodium (Colace)
Colace is the most common stool softener. The typical dose is 100 to 300mg daily, usually taken at bedtime. It is extremely gentle and has virtually no side effects.
The problem with Colace for semaglutide users is effectiveness. Multiple studies have shown that docusate sodium is only marginally better than placebo for treating established constipation. It works best as a preventive measure rather than a treatment. If you already have hard, dry stool sitting in your colon, Colace alone is probably not going to resolve the situation.
Where Colace shines is in combination therapy. Taking Colace daily as a preventive alongside MiraLAX as needed for breakthrough constipation is a strategy that many experienced semaglutide users find effective. The softener keeps things from getting too hard while the osmotic agent handles the volume and moisture when needed.
Stimulant laxatives: use with caution
Stimulant laxatives work by directly stimulating the nerves in the colon wall, causing contractions that push stool through. They are the most powerful over-the-counter option but come with important caveats for semaglutide users.
Bisacodyl (Dulcolax)
Dulcolax tablets or suppositories produce a bowel movement within 6 to 12 hours (tablets) or 15 to 60 minutes (suppositories). The standard dose is 5 to 10mg orally or one suppository rectally.
For semaglutide users, stimulant laxatives should be reserved for acute situations when you have not had a bowel movement in several days and osmotic laxatives have not worked. They should not be used daily because regular stimulant laxative use can lead to dependence, where the colon loses its ability to contract without pharmaceutical stimulation.
Senna (Senokot)
Senna is a plant-based stimulant laxative available over the counter. The typical dose is 15 to 30mg of sennosides at bedtime, with effects occurring the next morning. Like bisacodyl, senna is effective but should be limited to short-term or occasional use.
The combination of senna with docusate (sold as Senokot-S) provides both stimulation and softening, which can be particularly helpful for semaglutide users experiencing hard, difficult-to-pass stool.
A reasonable protocol for semaglutide users: if MiraLAX has not produced a bowel movement in 3 days, add a single dose of senna or bisacodyl. If that does not work within 24 hours, contact your healthcare provider.
Bulk-forming laxatives: proceed with caution
Bulk-forming laxatives like psyllium (Metamucil) and methylcellulose (Citrucel) work by absorbing water in the intestine and forming a gel-like mass that adds bulk to stool and stimulates peristalsis.
Here is where it gets tricky for semaglutide users. Bulk-forming laxatives require adequate hydration to work properly. If you take Metamucil without drinking enough water, it can actually make constipation worse by creating a dense, hard mass in your already sluggish intestines. Given that many semaglutide users are already dehydrated, fiber supplements need to be used carefully.
If you do use a bulk-forming laxative, follow these rules:
Drink at least 8 ounces of water with each dose
Drink an additional 8 ounces within the next hour
Start with half the recommended dose and increase gradually
If constipation worsens or you develop bloating, stop and switch to an osmotic laxative
Bulk-forming laxatives work best as a long-term preventive strategy rather than a treatment for acute constipation. They take 1 to 3 days to produce effects and are most effective when used consistently.
Prescription options for severe cases
When over-the-counter laxatives are not enough, several prescription medications can help.
Lubiprostone (Amitiza) is a chloride channel activator that increases intestinal fluid secretion. It is FDA-approved for chronic idiopathic constipation and can be used alongside semaglutide. The typical dose is 24mcg twice daily with food and water.
Linaclotide (Linzess) is a guanylate cyclase-C agonist that increases intestinal fluid secretion and accelerates transit. It is particularly useful for people who also experience abdominal pain with their constipation. The dose ranges from 72 to 290mcg daily, taken on an empty stomach at least 30 minutes before breakfast.
Prucalopride (Motegrity) is a serotonin 5-HT4 receptor agonist that stimulates colonic motility. It works through a completely different pathway than semaglutide and can be particularly effective for GLP-1-related constipation because it directly addresses the motility issue rather than just adding moisture. The standard dose is 2mg daily.
These prescription options require a conversation with your doctor, but they are worth knowing about if over-the-counter options fail. Many GI specialists are familiar with the specific pattern of constipation that GLP-1 medications cause and can tailor prescription therapy accordingly.
Laxative comparison chart for semaglutide users
Laxative Type | Example | How It Works | Onset | Best For | Daily Use Safe? | Rating |
|---|---|---|---|---|---|---|
Osmotic | MiraLAX | Draws water into colon | 1-3 days | First-line treatment | Yes | 9/10 |
Osmotic | Magnesium citrate | Draws water + adds magnesium | 30 min - 6 hrs | Acute episodes | With caution | 8/10 |
Stool softener | Colace | Allows water into stool | 1-3 days | Prevention | Yes | 6/10 |
Stimulant | Dulcolax/Senna | Stimulates colon contractions | 6-12 hours | Acute relief only | No | 7/10 |
Bulk-forming | Metamucil | Adds fiber bulk | 1-3 days | Long-term prevention | Yes (with water) | 5/10 |
Prescription | Linzess/Motegrity | Increases fluid/motility | Varies | Severe/chronic cases | Yes | 9/10 |
Optimal timing: when to take laxatives relative to your semaglutide dose
Timing matters more than most people realize, especially during the first few weeks of treatment when side effects are most intense.
For injectable semaglutide (Ozempic, Wegovy, compounded formulations): since the medication is injected subcutaneously, there is no interaction with anything in your GI tract. You can take laxatives at any time relative to your injection. The injection day itself often brings a temporary increase in GI side effects, so many users find it helpful to take their osmotic laxative the evening before their injection day as a preventive measure.
For oral semaglutide (Rybelsus): take your semaglutide first thing in the morning on an empty stomach with no more than 4 ounces of water, as directed. Wait at least 30 minutes before taking anything else, including laxatives. This ensures maximum absorption of the medication before introducing anything that might speed intestinal transit.
A practical daily schedule for semaglutide users managing constipation:
Morning (upon waking): Oral semaglutide if applicable, with 4oz water
30 minutes later: MiraLAX mixed into morning beverage, plus 8oz water
With breakfast: Fiber-rich foods, additional water
Midday: Colace 100mg if using as preventive
Evening: Magnesium oxide 400mg at bedtime (optional, if additional support needed)
This staggered approach ensures your semaglutide absorbs fully while providing consistent constipation management throughout the day.
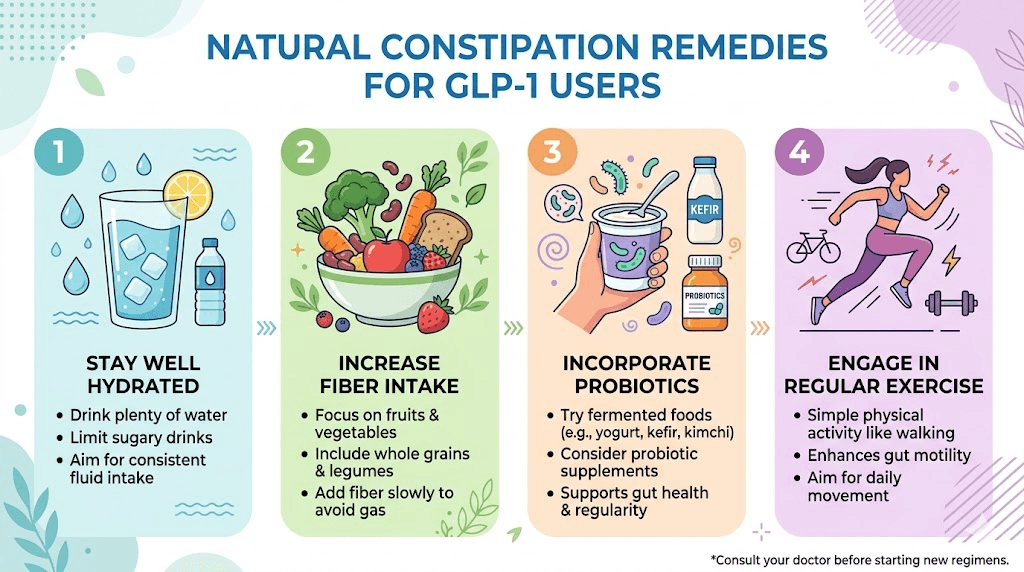
Natural alternatives and lifestyle strategies that actually work
Not everyone wants to take a pharmaceutical laxative, and that is completely understandable. The good news is that several natural strategies can be remarkably effective for semaglutide-related constipation, either alone or in combination with occasional laxative use.
Hydration: the foundation everything else builds on
This sounds basic because it is. But most semaglutide users are not drinking enough water, and the deficit is larger than they think.
Semaglutide reduces appetite and thirst signals. You are eating less food (which contains water) and feeling less compelled to drink. Meanwhile, your slowed GI tract is absorbing more water from stool. The math does not work in your favor unless you consciously increase your fluid intake.
The minimum target for semaglutide users is 64 ounces (eight 8-ounce glasses) of water daily. Many experts recommend 80 to 100 ounces for people on GLP-1 medications, especially those experiencing constipation. The right electrolyte balance also matters, as plain water without electrolytes can actually worsen hydration at the cellular level.
Practical hydration tips that work for people with suppressed appetite:
Keep a 32oz water bottle and refill it 2-3 times daily
Set phone reminders every 2 hours to drink
Add lemon, cucumber, or a splash of juice for flavor if plain water is unappealing
Herbal teas count toward your total (peppermint and ginger teas also soothe the GI tract)
Eat water-rich foods: cucumber, watermelon, oranges, celery, zucchini
Fiber intake: get it right or make things worse
Fiber is a double-edged sword for semaglutide users. The right amount improves constipation significantly. Too much, or the wrong type, or not enough water with it, makes everything worse.
The target is 25 to 30 grams of fiber daily. Most Americans get about 15 grams. If you are eating significantly less food due to semaglutide appetite suppression, you might be getting even less than that.
There are two types of fiber that matter here:
Soluble fiber dissolves in water and forms a gel. It softens stool and is generally well-tolerated. Good sources include oats, chia seeds, flaxseed, beans, apples, and psyllium husk. This is the type most semaglutide users should focus on.
Insoluble fiber does not dissolve in water and adds bulk. Sources include whole wheat, vegetables, and bran. While important for overall health, insoluble fiber can worsen bloating in people with slowed gut motility. Increase it gradually.
The key rule: increase fiber slowly. Adding 15 grams of fiber overnight to a system that is already moving slowly will cause gas, bloating, and potentially worsened constipation. Add 5 grams per day for a week, assess tolerance, then increase by another 5 grams if needed. Always pair fiber increases with proportional water increases.
The best foods to eat while on semaglutide tend to be naturally high in fiber while being easy on the stomach. Prioritizing these foods helps with constipation while supporting your overall nutrition plan.
Probiotics: gut bacteria matter
The bacteria in your gut play a role in motility and stool consistency. Semaglutide can alter the gut microbiome by changing the environment bacteria live in, particularly through changes in pH, transit time, and nutrient availability.
The best probiotics for semaglutide users include strains specifically studied for constipation relief: Bifidobacterium lactis, Lactobacillus rhamnosus, and Bifidobacterium longum. These strains have demonstrated the ability to increase stool frequency and improve consistency in clinical studies.
Fermented foods provide natural probiotics and are often easier to tolerate than supplements for people with GI sensitivity. Yogurt, kefir, sauerkraut, kimchi, and miso are all excellent options. The Pendulum GLP-1 probiotic was specifically designed for people on GLP-1 medications and contains strains that support GLP-1 production and gut health simultaneously.
Physical activity: get moving to get things moving
Exercise stimulates intestinal motility through direct mechanical stimulation and through activation of the enteric nervous system. Walking is surprisingly effective. A 20 to 30 minute walk after meals can significantly improve constipation in semaglutide users.
The challenge is that GLP-1 fatigue can make exercise feel impossible. Start small. Even a 10-minute walk is better than nothing. Yoga and stretching, particularly poses that compress and release the abdomen, can also stimulate gut motility. The key is consistency rather than intensity.
Some specific movements that target constipation:
Abdominal massage: Using moderate pressure, massage your abdomen in a clockwise direction (following the path of the colon) for 5 to 10 minutes
Deep squatting: The squat position straightens the anorectal angle, making elimination easier
Twisting yoga poses: Seated spinal twists compress the abdominal organs and can stimulate peristalsis
Walking immediately after meals: Takes advantage of the gastrocolic reflex
If you are struggling with weight loss on semaglutide without exercise, know that even light movement for digestive health can make your overall experience significantly more comfortable.
Magnesium supplementation: the underrated solution
Magnesium deserves its own section because it addresses multiple problems simultaneously for semaglutide users.
First, it functions as a gentle osmotic laxative. Magnesium draws water into the intestines, softening stool and increasing motility.
Second, many people on calorie-restricted diets are magnesium deficient. Inadequate magnesium intake can itself contribute to constipation, muscle cramps, poor sleep, and leg cramps that some semaglutide users experience.
Third, magnesium glycinate or magnesium threonate can improve sleep quality. Better sleep supports healthy gut motility. It is a virtuous cycle.
The best forms of magnesium for semaglutide-related constipation:
Magnesium oxide: Strongest laxative effect. 400mg at bedtime. Poorly absorbed systemically, which means more stays in the gut to draw water.
Magnesium citrate: Moderate laxative effect. 200-400mg daily. Better absorbed than oxide, so it doubles as a supplement.
Magnesium glycinate: Mild laxative effect. 200-400mg at bedtime. Best for people who also want the calming and sleep benefits.
A practical approach: start with magnesium citrate 200mg at bedtime. If constipation persists, increase to 400mg. If you need more aggressive relief, switch to magnesium oxide 400mg. If loose stools develop at any point, reduce the dose. Finding your personal sweet spot usually takes about a week of experimentation.
Coffee: the unexpected constipation tool
Coffee stimulates colonic motility. Research shows that caffeinated coffee increases colon contractions within minutes of consumption. This effect is independent of caffeine, as decaffeinated coffee also stimulates motility (though to a lesser degree).
For semaglutide users who can tolerate coffee without worsening acid reflux or nausea, a cup of warm coffee in the morning can be an effective natural laxative. The warmth of the liquid adds to the stimulatory effect. Drinking coffee about 30 minutes after waking, ideally following any oral medications, can kickstart the gastrocolic reflex and promote a morning bowel movement.
Specific foods that help
Certain foods have natural laxative properties that can complement your constipation management strategy. Incorporating these into your semaglutide diet can make a real difference.
Prunes and prune juice: Contain sorbitol, a natural osmotic laxative, plus fiber. Two to three prunes daily or 4 ounces of prune juice is a gentle starting point.
Kiwifruit: Studies show that eating two kiwis daily significantly increases bowel movement frequency. Kiwis contain actinidin, an enzyme that improves GI motility.
Ground flaxseed: One to two tablespoons of ground flaxseed added to yogurt or smoothies provides both soluble and insoluble fiber plus healthy fats that lubricate the intestinal lining.
Olive oil: One tablespoon of extra virgin olive oil on an empty stomach in the morning can lubricate the intestinal walls and stimulate bile production, which has a mild laxative effect.
Chia seeds: When soaked in liquid, chia seeds form a gel that adds moisture and bulk to stool. Start with one tablespoon in 8 ounces of water and drink before it fully gels.
Understanding what foods to avoid on semaglutide is equally important. Highly processed foods, excessive dairy, red meat, and refined carbohydrates can all worsen constipation.
Week-by-week constipation management protocol for new semaglutide users
Starting semaglutide with a proactive constipation management plan is far better than waiting for problems to develop and then scrambling for solutions. Here is a protocol designed specifically for new users based on the typical semaglutide timeline.
Before starting semaglutide (preparation week)
Begin increasing your fiber intake by 5 grams per day above your current level. Start drinking 80 ounces of water daily. Purchase MiraLAX and magnesium citrate to have on hand. Begin a daily probiotic. Establish a baseline understanding of your normal bowel habits so you can recognize changes quickly.
Weeks 1-4 (initial dose, 0.25mg)
This is the lowest dose, and many people experience minimal constipation here. Continue your increased fiber and hydration. Monitor bowel movements. If you notice any slowing, begin MiraLAX 17g daily. Add magnesium citrate 200mg at bedtime if needed. This is also when you will experience other first-week side effects like nausea, which may actually promote looser stools in some people.
Weeks 5-8 (dose increase to 0.5mg)
Constipation often worsens with the first dose increase. If you were not taking MiraLAX previously, start now. Increase magnesium to 400mg if 200mg was not sufficient. Add a daily walk of at least 20 minutes. Pay close attention to hydration as appetite suppression intensifies and food intake decreases. The appetite suppression timeline typically accelerates during this phase, which means less food bulk moving through the intestines.
Weeks 9-12 (dose increase to 1mg)
Another potential worsening point. If MiraLAX alone is not sufficient, add Colace 100mg daily as a preventive. Consider the prune protocol (2-3 prunes or 4oz prune juice daily). If you have gone more than 4 days without a bowel movement despite these measures, use a single dose of senna or bisacodyl as rescue therapy, then contact your healthcare provider.
Weeks 13-16 (dose increase to 1.7mg)
By this point, you should have a clear picture of your constipation pattern and what works for you. Most people have found their personal management protocol. Continue all effective strategies. If constipation remains severe despite comprehensive management, discuss prescription options (Linzess, Motegrity) with your doctor. This is also a good time to reassess whether your dosage is appropriate or if adjustments might help.
Weeks 17+ (maintenance dose, 2.4mg)
Many users report that constipation stabilizes or even improves slightly once they reach the maintenance dose and their body has had time to adapt. Continue your management protocol but reassess periodically. Some people find they can reduce laxative use over time as their GI system adjusts. Others need ongoing support for the duration of treatment.
This week-by-week approach aligns with the typical semaglutide timeline for weight loss effects, so you can anticipate constipation challenges at each escalation point.
When laxatives are not enough: warning signs that need medical attention
Most semaglutide-related constipation is manageable with the strategies above. But there are situations where constipation becomes a medical concern that requires professional intervention. Knowing these warning signs could prevent a serious complication.
Red flags requiring immediate medical attention
No bowel movement for 7 or more days despite laxative use. This suggests a potential mechanical or functional obstruction that simple laxatives cannot resolve.
Severe abdominal pain that does not respond to position changes or over-the-counter pain relief. This could indicate a bowel obstruction (ileus), which was added to the Ozempic label as a recognized side effect in September 2023. Bowel obstruction is a medical emergency.
Inability to pass gas. The inability to pass flatus, combined with constipation and abdominal distension, is a classic sign of bowel obstruction. This requires emergency evaluation.
Persistent vomiting combined with constipation. Nausea and occasional vomiting are common semaglutide side effects, but persistent vomiting that prevents you from keeping down fluids, especially combined with constipation, needs urgent assessment.
Rectal bleeding. Small amounts of bright red blood after straining are usually from hemorrhoids or anal fissures, which are common with chronic constipation. However, any rectal bleeding should be discussed with a healthcare provider, and significant bleeding requires immediate evaluation.
Signs of dehydration: dark urine, dizziness when standing, dry mouth, rapid heartbeat. Severe constipation combined with the reduced fluid intake common in semaglutide users can lead to dehydration that requires medical attention. These symptoms can overlap with other semaglutide side effects like lightheadedness, so do not dismiss them.
When to talk to your prescriber (non-emergency but important)
Schedule a conversation with your prescriber if:
Constipation persists for more than 2 weeks despite consistent use of osmotic laxatives
You are using stimulant laxatives more than twice per week
Constipation is significantly affecting your quality of life or your willingness to continue semaglutide
You develop new symptoms like severe bloating, painful cramping, or a feeling of incomplete evacuation
Over-the-counter options are not providing adequate relief and you want to explore prescription alternatives
Your prescriber may consider adjusting your dose, slowing the escalation schedule, or adding a prescription motility agent. In rare cases, switching to tirzepatide may result in different GI side effect profiles, though constipation is common with all GLP-1 medications.
Compounded semaglutide and constipation: is there a difference?
Many users take compounded semaglutide rather than brand-name Ozempic or Wegovy. The constipation mechanism is identical because the active ingredient is the same. However, compounded formulations sometimes include additional ingredients that may affect GI symptoms.
Some compounded semaglutide products include vitamin B12, glycine, or L-carnitine. These additives do not directly affect constipation, but glycine has mild gut-calming properties that some users report as beneficial for overall GI comfort. The semaglutide glycine B12 blend is a popular formulation that provides additional nutritional support without worsening constipation.
If you are experiencing constipation with compounded semaglutide, the same laxative and lifestyle strategies apply. The compounding pharmacy and formulation do not change the fundamental GLP-1 mechanism that causes slowed gut motility. Whether you are getting your medication from Empower Pharmacy, Olympia Pharmacy, or any other source, the constipation management approach remains the same.
What can differ with compounded formulations is concentration and dosing precision. If you suspect your constipation is worse because your actual dose is higher than intended, verify your calculations using a semaglutide dosage calculator and confirm your reconstitution method is correct.
Drug interactions to be aware of
While laxatives themselves do not interact dangerously with semaglutide, it is worth understanding how semaglutide affects the absorption of other medications you might be taking alongside both your GLP-1 and your laxative.
Semaglutide slows gastric emptying, which can delay the absorption of oral medications. Research published in Clinical Pharmacokinetics examined semaglutide interactions with metformin, warfarin, atorvastatin, and digoxin. The findings showed that while peak blood levels (Cmax) of co-administered drugs were sometimes reduced or delayed, the total amount absorbed (AUC) generally remained unchanged. This means semaglutide might make other drugs take longer to kick in, but it does not significantly reduce how much gets absorbed overall.
If you are taking medications with a narrow therapeutic index (like warfarin, certain anti-seizure medications, or thyroid hormones like levothyroxine), adding a stimulant laxative that dramatically speeds transit could theoretically affect absorption. This is another reason why osmotic laxatives like MiraLAX are preferred, as they work gently without dramatically altering transit speed.
If you are also taking metformin with semaglutide, note that metformin itself can cause diarrhea. The opposing GI effects of metformin (loosening) and semaglutide (tightening) sometimes balance each other out. If you are on both medications and still constipated, you may need laxative support despite the metformin.
For people exploring combinations like berberine and semaglutide or phentermine and semaglutide, each additional medication adds complexity to the GI picture. Always discuss your full medication list, including over-the-counter laxatives, with your prescriber.
The constipation and weight loss connection
Here is something that frustrates semaglutide users more than the constipation itself: the effect on the scale.
When you are constipated, stool accumulates in your colon. This stool has weight, typically 1 to 5 pounds depending on the degree of constipation. If you have been constipated for several days, the scale might show a "stall" or even a weight increase that has nothing to do with fat gain. For people tracking their semaglutide progress week by week, this can be deeply discouraging.
After a successful bowel movement (or a few), the scale can drop dramatically. This is not real weight loss in the sense that you burned fat overnight. It is simply the removal of accumulated stool. But it can create a confusing pattern where the scale seems to stall for a week, then suddenly drops 3 to 4 pounds.
If you are in a semaglutide plateau or feeling like you are not losing weight on semaglutide, check your bowel habits before assuming the medication has stopped working. Resolving constipation often resolves the apparent plateau.
For accurate weight tracking while managing constipation, consider:
Weighing yourself at the same time each day, after your morning bathroom routine
Looking at weekly averages rather than daily numbers
Using monitoring tools that track trends rather than individual data points
Not interpreting a 2-3 day stall as evidence of medication failure
Understanding this connection helps you maintain perspective during the inevitable ups and downs of the semaglutide weight loss journey.
Constipation across different GLP-1 medications
Semaglutide is not the only GLP-1 that causes constipation. Understanding how constipation compares across different medications can help you and your prescriber make informed decisions if constipation is severely impacting your quality of life.
The side effect comparison between semaglutide and tirzepatide shows that both medications cause constipation at similar rates, though individual experiences vary. Tirzepatide, which is a dual GIP/GLP-1 receptor agonist, causes constipation in approximately 6 to 12% of users in clinical trials (lower than semaglutide at 24%), but tirzepatide constipation can be equally persistent in those affected.
If you are considering a switch, the transition between these medications should be discussed with your prescriber. Switching solely because of constipation may or may not resolve the issue, since the fundamental GLP-1 mechanism is present in both drugs.
Newer GLP-1 medications in development, including retatrutide and survodutide, also report GI side effects including constipation in clinical trials. This appears to be a class-wide effect of GLP-1 receptor activation rather than something unique to semaglutide.
For a comprehensive comparison of how different GLP-1 medications stack up against each other, including side effect profiles, the complete comparison guide covers each medication in detail.
Long-term laxative use on semaglutide: is it safe?
Many semaglutide users worry about taking laxatives for months or even years. The concern is reasonable. Here is what the evidence says about long-term safety of different laxative types.
Osmotic laxatives (MiraLAX): long-term safety is well established
Polyethylene glycol 3350 has been studied in long-term use (6 months to 2 years) and shows an excellent safety profile. It does not cause electrolyte imbalances at standard doses, does not lead to dependency, and does not damage the colon lining. For most semaglutide users, daily MiraLAX use for the duration of treatment is medically acceptable.
Magnesium: safe with monitoring
Long-term magnesium supplementation is generally safe for people with normal kidney function. However, chronic high-dose magnesium can accumulate in people with kidney impairment. If you plan to use magnesium as an ongoing constipation management tool, periodic blood work to check magnesium levels and kidney function is prudent.
Stool softeners: safe for extended use
Docusate sodium has no known long-term safety concerns. The main issue is diminishing effectiveness over time rather than safety problems.
Stimulant laxatives: not recommended for long-term use
This is the category with legitimate concerns. Regular use of stimulant laxatives (bisacodyl, senna) for more than 1 to 2 weeks can lead to:
Melanosis coli: Dark pigmentation of the colon lining. This is generally harmless and reversible but indicates chronic stimulant use.
Tolerance: The colon may require increasing doses to achieve the same effect.
Dependence: In severe cases, the colon may lose its ability to contract normally without stimulant assistance.
If you find yourself needing stimulant laxatives more than twice per week for several consecutive weeks, talk to your doctor about switching to a prescription motility agent like prucalopride, which does not carry the same dependency risk.
The psychological impact of chronic constipation on GLP-1 therapy
This topic rarely gets addressed, but it matters. Chronic constipation on semaglutide affects more than your gut. It affects your willingness to continue treatment.
Semaglutide-related GI side effects are the primary reason people discontinue the medication. In clinical trials, approximately 7% of participants on semaglutide 2.4mg discontinued due to GI adverse events. In real-world use, the number is likely higher because people outside of clinical trials have less support and less motivation to push through discomfort.
If constipation is making you consider stopping semaglutide, know that aggressive constipation management is almost always a better option than discontinuation, especially if the medication is otherwise working well for you. The withdrawal effects and weight regain after stopping are significant concerns that should factor into any decision to discontinue.
SeekPeptides members access detailed side effect management protocols, community support from others navigating the same challenges, and expert guidance on optimizing their GLP-1 experience. Managing constipation effectively is a key part of long-term success with any GLP-1 medication.
Special considerations for different populations
Women on semaglutide
Women may experience constipation fluctuations tied to their menstrual cycle. Progesterone, which rises during the luteal phase, slows gut motility. Combined with semaglutide-induced slowing, the premenstrual period can bring significantly worsened constipation. Women who notice this pattern should consider increasing their laxative dose during the second half of their cycle.
Additionally, semaglutide can affect menstrual cycles in various ways. Changes in cycle regularity, combined with constipation fluctuations, can make symptom management more complex. Tracking both bowel habits and cycle days can help identify patterns.
For women who are breastfeeding, laxative safety becomes an additional consideration. Most osmotic laxatives like MiraLAX are considered safe during breastfeeding because they are not significantly absorbed systemically. However, always verify with your prescriber, especially since semaglutide itself has limited safety data for breastfeeding.
Older adults
Older adults on semaglutide face compounded constipation risk because gut motility naturally decreases with age. This population may need more aggressive management from the outset and should be monitored more closely for dehydration and electrolyte imbalances. Magnesium-based laxatives require particular caution in older adults with declining kidney function.
People with thyroid conditions
Hypothyroidism slows gut motility independently of semaglutide. People with Hashimoto thyroiditis or hypothyroidism on semaglutide should anticipate more severe constipation and begin proactive management from their first dose. Ensuring thyroid hormones are optimally dosed can help mitigate this compounding effect.
People taking other constipation-causing medications
Several common medications also cause constipation: opioids, calcium channel blockers, iron supplements, certain antidepressants, and anticholinergic medications. If you take any of these alongside semaglutide, the constipation burden is additive. Discuss your full medication list with your prescriber to identify all contributing factors.
Frequently asked questions
Can I take MiraLAX every day while on semaglutide?
Yes. MiraLAX (polyethylene glycol 3350) is safe for daily use and does not cause dependence. Many semaglutide users take it daily throughout their treatment. The standard dose is 17 grams once daily, and it has no known interactions with semaglutide.
Will a laxative reduce how well semaglutide works?
For injectable semaglutide (Ozempic, Wegovy), no. The medication is absorbed through subcutaneous injection, so nothing in your GI tract can affect it. For oral semaglutide (Rybelsus), taking laxatives at least 30 minutes after your morning dose minimizes any theoretical absorption concern.
How long will semaglutide constipation last?
Clinical data shows a median duration of 47 days, but individual experiences vary widely. Some people experience constipation only during dose escalation phases, while others deal with it throughout treatment. Proactive management typically reduces severity even when it does not eliminate constipation entirely.
Is it safe to take Dulcolax with semaglutide?
Yes, but only for short-term or occasional use. Bisacodyl (Dulcolax) is a stimulant laxative that should not be used daily. Reserve it for acute situations when osmotic laxatives have not worked after 3 or more days. If you need stimulant laxatives regularly, talk to your doctor about prescription alternatives.
Can constipation on semaglutide be dangerous?
In most cases, semaglutide constipation is uncomfortable but not dangerous. However, severe or prolonged constipation can lead to fecal impaction or, in rare cases, bowel obstruction (ileus). The FDA added ileus as a recognized side effect of Ozempic in 2023. Seek immediate medical care if you experience severe abdominal pain, inability to pass gas, or persistent vomiting combined with constipation.
Should I take a laxative before I start semaglutide?
Not necessarily before, but at the same time is reasonable. Many experienced practitioners recommend starting MiraLAX or magnesium citrate on the same day you begin semaglutide, especially if you have a history of constipation. Proactive management prevents the problem from developing rather than treating it after the fact.
Does compounded semaglutide cause more constipation than brand-name?
The active ingredient is the same, so the constipation mechanism is identical. Some compounded semaglutide formulations include additives like glycine or B12 that may have mild GI benefits, but the constipation rates are fundamentally comparable.
What about fiber supplements versus laxatives?
The best fiber supplements for GLP-1 users can help prevent constipation, but they are not as effective as osmotic laxatives for treating established constipation. The ideal approach combines a fiber supplement for prevention with MiraLAX as needed for breakthrough episodes. Always take fiber with plenty of water to avoid worsening the problem.
Building your personal constipation management plan
Everyone responds differently to semaglutide, and your optimal constipation management plan will be unique to you. Here is a framework for building and refining your approach.
Step 1: establish your baseline
Before starting or during the first week of semaglutide, note your typical bowel frequency, stool consistency, and any existing digestive issues. This baseline helps you recognize when things change and how significantly.
Step 2: implement foundation strategies
Start with hydration (80+ ounces daily), gradual fiber increase (target 25-30 grams), daily movement (20+ minutes walking), and a probiotic supplement. These four pillars address the most common underlying causes and cost almost nothing.
Step 3: add first-line laxative support as needed
When lifestyle strategies alone are not sufficient, add MiraLAX 17g daily and/or magnesium citrate 200-400mg at bedtime. These osmotic agents directly counter the water absorption that makes semaglutide constipation so stubborn.
Step 4: layer additional support if needed
Add Colace 100mg daily as a stool softener. Incorporate specific constipation-fighting foods (prunes, kiwi, ground flaxseed). Try abdominal massage and squatting position for elimination.
Step 5: rescue therapy for acute episodes
If you have not had a bowel movement in 4+ days despite the measures above, use a single dose of senna or bisacodyl. A glycerin suppository can provide faster relief for stool that is in the rectum but difficult to pass. If rescue therapy is needed more than twice in a month, escalate to your prescriber.
Step 6: consider prescription options
For persistent, severe constipation that does not respond adequately to the above steps, prescription motility agents like prucalopride (Motegrity) or secretagogues like linaclotide (Linzess) can provide significant relief. These medications work through different mechanisms than over-the-counter options and can be used safely alongside semaglutide.
For researchers serious about optimizing their peptide protocols, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, detailed side effect management protocols, and a community of thousands who have navigated these exact challenges. Managing constipation is just one piece of the puzzle, and having access to SeekPeptides expert guidance can make the difference between a frustrating experience and a successful one.
External resources
PMC: Gastrointestinal tolerability of semaglutide 2.4mg in STEP trials
PMC: Clinical recommendations for GI adverse events with GLP-1 receptor agonists
PMC: Potentially serious adverse effects of GLP-1 receptor agonists
PMC: Drug interactions between GLP-1 receptor agonists and oral medications
In case I do not see you, good afternoon, good evening, and good night. May your bowel movements stay regular, your hydration stay consistent, and your semaglutide journey stay on track.