Jan 21, 2026

Tired of conflicting information about testosterone replacement therapy and peptides?
You're not alone. Every day, men search for answers about TRT peptides, trying to understand whether they should use peptides alongside testosterone therapy, instead of it, or as part of a comprehensive hormone optimization strategy. The confusion is understandable. Traditional TRT clinics rarely discuss peptides. Peptide communities often dismiss TRT entirely. And somewhere in between, there's a massive gap in practical, actionable information.
Here's the reality. Both approaches have merit. Both have limitations. And for many men, the optimal path involves understanding how these tools work together rather than viewing them as competing options. The research is increasingly clear that peptides can complement testosterone replacement therapy in ways that address common TRT shortcomings, from testicular atrophy to growth hormone decline to recovery optimization.
This guide covers everything you need to know about the intersection of TRT and peptides. You'll learn which peptides work synergistically with testosterone therapy, which ones offer viable alternatives for men who want to avoid exogenous hormones, and how to build protocols that maximize results while minimizing side effects. Whether you're currently on TRT and looking to enhance your results, considering TRT but worried about side effects, or exploring peptides for testosterone optimization as a standalone approach, this comprehensive resource will help you make informed decisions about your hormone health.
SeekPeptides has become the trusted resource for thousands of men navigating these exact questions, providing evidence-based protocols and practical guidance for peptide research.
Understanding TRT and why peptides matter
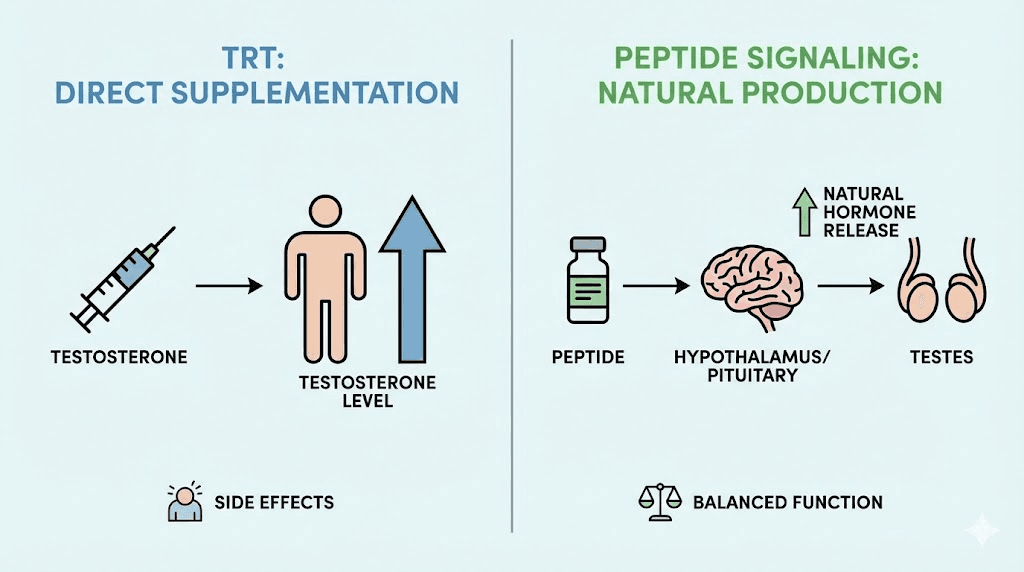
Testosterone replacement therapy involves introducing exogenous testosterone into your body through injections, gels, patches, or pellets. The approach is straightforward. Your testosterone is low. You add testosterone. Levels rise. Symptoms improve.
Simple enough.
But the simplicity masks significant complexity. When you introduce external testosterone, your body's natural production shuts down. The hypothalamic-pituitary-gonadal axis, the feedback loop that regulates hormone production, recognizes the elevated testosterone and stops signaling your testes to produce more. Over time, this can lead to testicular atrophy, fertility concerns, and dependency on continued therapy.
This is where peptides enter the conversation. Unlike testosterone, many peptides work by stimulating your body's own hormone production rather than replacing it. They signal rather than supply. This fundamental difference creates opportunities for men at various stages of their hormone optimization journey, from those looking to avoid TRT entirely to those seeking to mitigate its side effects while maximizing benefits.
TRT basics: what you need to know
Before diving into peptides, let's establish a clear understanding of testosterone replacement therapy. This foundation matters because your decisions about peptides should be informed by how TRT actually works in the body.
How testosterone replacement therapy works
TRT delivers bioidentical or synthetic testosterone directly into your bloodstream. Injectable testosterone cypionate and enanthate remain the most common forms, typically administered every one to two weeks. Topical gels provide daily application options. Patches offer continuous delivery. Pellets, inserted subcutaneously, release testosterone over several months.
Each delivery method has tradeoffs. Injections create peaks and valleys in testosterone levels. Gels require daily application and carry transfer risks. Patches can irritate skin. Pellets require minor surgical procedures. The choice often depends on lifestyle preferences, cost considerations, and individual response patterns.
Within days to weeks of starting TRT, most men notice improvements in energy, mood, libido, and mental clarity. Muscle mass and strength typically increase over months with proper training. Body fat distribution may improve. The effects can be profound for men with genuinely low testosterone.
The downsides of traditional TRT
TRT isn't without consequences. Understanding these helps explain why peptides have become such an important adjunct therapy.
The most significant issue involves natural production shutdown. Your body's testosterone production doesn't just decrease on TRT. It stops almost entirely. The testes, receiving no stimulation from luteinizing hormone, shrink. Fertility plummets. For younger men or those who may want children, this presents a serious concern.
Estrogen conversion can become problematic. Some testosterone converts to estradiol through aromatization, potentially causing water retention, mood changes, and gynecomastia in sensitive individuals. Managing estrogen often requires additional medications.
Hematocrit levels may rise, thickening blood and increasing cardiovascular risks. Regular blood donations or phlebotomy become necessary for some men. Acne, hair loss, and sleep apnea can worsen. The prostate requires monitoring.
Perhaps most concerning for many men: TRT is typically a lifelong commitment. Coming off after extended use means dealing with suppressed natural production, which may never fully recover. The convenience of TRT comes with significant long-term implications that deserve careful consideration.
Who benefits most from TRT
TRT makes the most sense for men with clinically low testosterone, typically below 300 ng/dL, who have clear symptoms and have ruled out treatable causes. Men over 50 with age-related decline often fall into this category. Those with primary hypogonadism, where the testes themselves are damaged, may have no other options.
Younger men with secondary hypogonadism, where the problem lies in signaling rather than testicular function, have more choices. This is precisely where peptides become relevant. If your testes can produce testosterone when properly stimulated, peptides offer a way to restore that signaling without the shutdown associated with exogenous hormones.
Peptides versus TRT: the fundamental differences
The comparison between peptides and TRT isn't straightforward because they operate through entirely different mechanisms. Understanding these differences helps you choose the right approach for your situation.
Mechanism of action
TRT replaces. Peptides signal.
When you inject testosterone, you're adding hormone directly to your system. Your body doesn't need to produce it because you're supplying it externally. This creates immediate, predictable increases in testosterone levels. The results are fast and reliable.
Peptides work upstream. They stimulate your body's own hormone production by acting on the hypothalamus, pituitary, or testes directly. Understanding how peptides work reveals why they can maintain natural function rather than replacing it. Your feedback loops remain intact. Your testes stay active. Your natural rhythms continue.
This distinction matters enormously for fertility, testicular health, and the ability to eventually discontinue therapy.
Speed and magnitude of results
TRT wins on speed. Within one to two weeks, testosterone levels reach optimal ranges. Symptom improvement follows quickly. The results are consistent and dramatic.
Peptides require patience. Studies show 30-60% increases in testosterone over the first few months, but results vary significantly between individuals. Some men respond excellently. Others see modest improvements. The ceiling is typically lower than TRT can achieve.
For severely hypogonadal men, peptides alone may never restore optimal testosterone. For men with mild to moderate decline, peptides can bring levels into healthy ranges while maintaining natural function.
Side effect profiles
TRT side effects stem from supraphysiological testosterone levels and natural production shutdown. Peptide safety profiles differ because they work within your body's natural feedback systems.
Common TRT side effects include testicular atrophy, fertility reduction, elevated hematocrit, estrogen imbalances, and potential cardiovascular concerns. Managing these often requires additional medications and regular monitoring.
Peptide side effects tend to be milder. Injection site reactions, temporary fluid retention, and transient changes in glucose metabolism appear in some users. Because peptides maintain natural feedback loops, the dramatic hormonal disruptions seen with TRT occur less frequently.
Neither approach is inherently safer. Both require medical supervision and regular monitoring. The key difference lies in the types of management required.
Long-term considerations
TRT commits you to ongoing therapy. Stopping after extended use means navigating recovery of suppressed natural production, which may never fully return. Some men require post-TRT therapy with medications like clomiphene to restart natural production, with varying success rates.
Peptides offer more flexibility. Because they maintain natural production, discontinuation doesn't create the same suppression crisis. Your body continues producing testosterone throughout treatment, making transitions smoother.
For younger men, those considering future fertility, or anyone hesitant about lifelong hormone replacement, this flexibility represents a significant advantage.
Peptides that work with TRT
For men already on TRT, peptides offer powerful ways to enhance results, mitigate side effects, and address areas where testosterone alone falls short. This synergistic approach has become increasingly popular as understanding of peptide stacking has grown.
HCG and gonadorelin for testicular maintenance
The most common peptide addition to TRT protocols addresses testicular atrophy and fertility. Human chorionic gonadotropin, technically a hormone rather than a peptide, mimics luteinizing hormone and stimulates the testes to continue producing testosterone internally.
Research demonstrates that adding 250-500 IU of HCG every other day alongside TRT maintains testicular size, function, and sperm production in most men. For those concerned about fertility or simply uncomfortable with testicular shrinkage, HCG has become nearly standard practice.
Gonadorelin offers an alternative when HCG isn't available. As a synthetic form of gonadotropin-releasing hormone, it stimulates the pituitary to release natural LH and FSH. However, its extremely short half-life requires multiple daily injections, making it less convenient than HCG. Some clinics report that gonadorelin doesn't maintain testicular function as reliably as HCG, particularly in men whose natural signaling is already significantly suppressed.
Growth hormone releasing peptides
TRT optimizes testosterone, but growth hormone represents another crucial piece of the hormonal puzzle that declines with age. CJC-1295 combined with Ipamorelin has become the most popular growth hormone secretagogue stack for men on TRT.
The combination works synergistically. CJC-1295 is a growth hormone releasing hormone analog that extends the duration of growth hormone pulses. Ipamorelin is a selective growth hormone secretagogue that triggers GH release without significantly affecting cortisol or other hormones. Together, they enhance natural GH release patterns, closely mimicking the body's rhythms.
Benefits for men on TRT include enhanced fat loss, particularly visceral fat; improved recovery from training; better sleep quality; and potential anti-aging effects on skin, hair, and connective tissue. Many men report that adding these peptides to TRT creates more complete rejuvenation than testosterone alone provides.
Sermorelin offers similar benefits through a slightly different mechanism. As another GHRH analog, it stimulates natural GH release and has been used clinically longer than newer peptides. Its shorter half-life requires more frequent dosing, but some men prefer its established track record.
Tesamorelin deserves special mention for men concerned about abdominal fat. This FDA-approved GHRH analog specifically targets visceral adiposity and has strong clinical data supporting its effectiveness. For men on TRT struggling with midsection fat despite optimized testosterone levels, tesamorelin for visceral fat loss can address what testosterone alone cannot.
Recovery and healing peptides
Men on TRT often train hard, and recovery becomes crucial. The Wolverine stack, combining BPC-157 and TB-500, has gained massive popularity for its recovery-enhancing effects.
BPC-157 is a synthetic peptide derived from a protective protein in gastric juice. Research demonstrates wound healing acceleration, tendon repair enhancement, and gut healing properties. Many men on TRT add BPC-157 specifically for joint and connective tissue support, areas where intense training creates wear that testosterone alone doesn't adequately address.
TB-500 works systemically to enhance cellular regeneration and reduce inflammation. As a synthetic analog of thymosin beta-4, it regulates actin, a protein crucial for cell structure and movement. While BPC-157 works locally at injury sites, TB-500 provides broader systemic support.
Together, these peptides create a comprehensive recovery support system. Typical protocols for the BPC-157 and TB-500 combination run 4-8 weeks, with many men cycling this stack during phases of particularly intense training or when addressing specific injuries.
Libido enhancement
While TRT typically improves libido significantly, some men find that sexual function doesn't optimize as expected. PT-141 addresses this through a completely different mechanism than testosterone or traditional erectile dysfunction medications.
PT-141, also known as bremelanotide, works on melanocortin receptors in the brain rather than on blood vessels like PDE5 inhibitors. This central mechanism can enhance desire, arousal, and sexual satisfaction in ways that complement testosterone's effects on libido.
For men on TRT who have optimized their testosterone but still experience less than ideal sexual function, PT-141 offers an additional tool. PT-141 nasal spray has become a popular delivery method, though injectable forms remain common.
Cognitive and mood support
Some men on TRT seek additional cognitive enhancement beyond what testosterone provides. Semax has gained attention for its nootropic effects, including enhanced memory, focus, and neuroprotection.
As a synthetic analog of ACTH, Semax affects multiple neurotransmitter systems and has been used clinically in Russia for decades. For men seeking cognitive enhancement through peptides, Semax offers benefits distinct from testosterone's mood and cognitive effects.
Peptides as alternatives to TRT
Not every man with suboptimal testosterone needs or wants traditional TRT. Peptides offer alternatives that can restore natural production without the commitment and side effects of exogenous testosterone. For men with secondary hypogonadism, where the problem lies in signaling rather than testicular function, these alternatives can be particularly effective.
Kisspeptin for natural testosterone restoration
Kisspeptin sits at the top of the hormone cascade, acting as the master regulator of reproductive hormone signaling. This hypothalamic neuropeptide signals the pituitary to release gonadotropins, which in turn stimulate testosterone production.
Research demonstrates that kisspeptin-10 potently evokes LH secretion in men, increasing testosterone, LH pulse frequency, and pulse size. Clinical studies show significant testosterone increases within hours of administration, with effects lasting through continuous protocols.
Dosing typically ranges from 100-200mcg administered 2-3 times weekly. However, kisspeptin requires careful management. Chronic continuous administration can lead to receptor downregulation and paradoxical suppression of testosterone. Pulsatile dosing protocols, mimicking natural signaling patterns, appear most effective.
Kisspeptin works best for men whose hypothalamic-pituitary function is intact but understimulated. Those with primary hypogonadism, where the testes themselves are the problem, won't respond adequately.
Enclomiphene for preserving natural production
While not technically a peptide, enclomiphene deserves mention as a powerful tool for natural testosterone restoration that often appears in peptide-based protocols. This selective estrogen receptor modulator blocks estrogen's negative feedback at the pituitary, increasing LH and FSH release.
Studies show dose-dependent testosterone increases with enclomiphene. At 25mg daily, average testosterone rose to 520 ng/dL in hypogonadal men. At 50mg, levels reached nearly 600 ng/dL. Importantly, these increases occurred while maintaining sperm production, unlike TRT.
Typical protocols use 12.5-25mg 3-5 days weekly. Morning dosing aligns with natural testosterone peaks. Many clinics use enclomiphene as a first-line approach for younger men with secondary hypogonadism, reserving TRT for non-responders or those with more severe deficiency.
Enclomiphene combines well with peptides like kisspeptin, working through complementary mechanisms to optimize natural testosterone production without shutdown.
Growth hormone secretagogues for overall hormone optimization
While not directly boosting testosterone, growth hormone secretagogues create an overall hormonal environment that supports testosterone optimization. Improved sleep from peptides like DSIP enhances natural testosterone production. Better body composition from GH peptides reduces estrogen conversion. Enhanced recovery supports training adaptations that elevate testosterone naturally.
For men with mildly low testosterone, addressing growth hormone deficiency and sleep quality through peptides can sometimes normalize testosterone without direct intervention. This holistic approach appeals to those seeking minimal intervention strategies.
Building your TRT peptide protocol
Designing an effective protocol requires understanding your goals, current hormone status, and how different peptides interact. This section provides frameworks for common scenarios, though individual optimization always requires working with knowledgeable healthcare providers.
Protocol for TRT enhancement
Men already on testosterone replacement therapy often build peptide stacks to address specific limitations. A comprehensive TRT enhancement protocol might include:
Testicular maintenance: HCG 250-500 IU three times weekly or gonadorelin if HCG unavailable. This preserves testicular function, supports fertility, and may enhance estrogen metabolism by maintaining intratesticular testosterone production.
Growth hormone support: CJC-1295 without DAC at 100mcg combined with Ipamorelin at 100-200mcg, administered nightly before bed. This timing leverages natural GH release patterns during sleep. Some protocols use five days on, two days off to prevent receptor desensitization.
Recovery support: BPC-157 at 250-500mcg daily during training intensification or injury recovery phases. TB-500 at 2-5mg weekly for systemic support. These can be cycled as needed rather than run continuously.
Optional additions: Tesamorelin for stubborn visceral fat. PT-141 as needed for libido optimization. Selank or Semax for cognitive enhancement.
Protocol for TRT alternative
Men seeking to optimize testosterone without exogenous hormones need protocols that stimulate natural production through multiple pathways. A natural testosterone restoration protocol might include:
HPG axis stimulation: Kisspeptin-10 at 100-200mcg administered 2-3 times weekly, timed to avoid desensitization. Alternatively, enclomiphene at 12.5-25mg 3-5 mornings weekly.
Growth hormone optimization: Sermorelin or CJC-1295/Ipamorelin combination to enhance overall hormonal environment and improve body composition, sleep, and recovery.
Sleep and stress support: DSIP for sleep optimization if needed, given testosterone's production during deep sleep. Peptides for stress management can also support natural testosterone by reducing cortisol interference.
This approach requires more patience than TRT. Results develop over months rather than weeks. Regular blood work guides adjustments. For many men with secondary hypogonadism, this approach successfully restores optimal testosterone while maintaining natural function and fertility.
Protocol for transition off TRT
Some men on TRT decide to attempt discontinuation, whether for fertility, personal preference, or other reasons. Peptides can support this transition, though success depends heavily on how long TRT was used and individual recovery capacity.
Initial phase: While still on reduced TRT dose, begin HCG to stimulate testicular function. Add kisspeptin or enclomiphene to activate the HPG axis.
Transition phase: Gradually taper TRT while increasing peptide support. Monitor testosterone levels carefully during this period.
Post-TRT phase: Continue kisspeptin or enclomiphene to maintain stimulation. Support with GH peptides for overall hormonal environment. Expect 3-6 months for full recovery assessment.
Not all men successfully transition off TRT, particularly after prolonged use. Working with experienced practitioners who can adjust protocols based on response is essential.
Specific peptides for testosterone optimization
Understanding each peptide's mechanism, benefits, and practical considerations helps you make informed decisions about your protocol. Here's comprehensive coverage of the key players in testosterone optimization.
Kisspeptin
Kisspeptin is encoded by the KISS1 gene and acts as the primary hypothalamic regulator of GnRH secretion. Different forms exist, including kisspeptin-10, -13, -14, and -54, with kisspeptin-10 being most commonly used due to its potency and manageable dosing.
Research shows that IV bolus of kisspeptin-10 elevates LH and FSH at doses as low as 0.3-1.0 nmol/kg. Continuous infusions increase testosterone, LH pulse frequency, and pulse size. This makes kisspeptin among the most directly testosterone-relevant peptides available.
Practical dosing for subcutaneous use typically ranges from 100-200mcg administered 2-3 times weekly. Daily continuous use risks receptor desensitization and paradoxical suppression. Pulsatile protocols better mimic natural physiology.
Kisspeptin works best for men with functional testes and suboptimal hypothalamic signaling. Those with primary hypogonadism or severely damaged HPG axes respond poorly.
Growth hormone peptides
The relationship between growth hormone and testosterone is complex but important. While GH doesn't directly increase testosterone, optimizing growth hormone creates conditions that support testosterone optimization through improved body composition, sleep quality, and recovery.
Sermorelin stimulates GH release through GHRH receptor activation. Clinical use spans decades, providing substantial safety data. Typical dosing runs 200-500mcg at bedtime. Its shorter half-life means less sustained elevation but more natural pulsatile patterns.
CJC-1295 offers similar GHRH-type stimulation with modified duration. The version without DAC (drug affinity complex) provides 30-minute half-life, while the DAC version extends this significantly. For testosterone optimization purposes, the no-DAC version paired with Ipamorelin remains most popular.
Ipamorelin selectively stimulates GH release without significantly affecting cortisol or prolactin. This selectivity makes it particularly useful for testosterone optimization, as elevated cortisol and prolactin both suppress testosterone production.
MOTS-c deserves mention as a mitochondrial-derived peptide that affects metabolic function. While not directly GH-releasing, its effects on insulin sensitivity and body composition indirectly support testosterone optimization.
Healing and recovery peptides
The best peptides for injury recovery complement testosterone optimization by supporting the intense training that naturally elevates testosterone and maintaining the physical function that hormone optimization enables.
BPC-157 demonstrates remarkable wound healing properties in research. Derived from gastric juice proteins, it promotes angiogenesis, nitric oxide production, and collagen formation. For men pushing physical limits, BPC-157 addresses the connective tissue stress that testosterone alone doesn't adequately support.
Standard BPC-157 dosing runs 200-500mcg daily, with some protocols using local injections near injury sites for targeted effects. Systemic administration works as well, though potentially with less localized benefit.
TB-500 works through different mechanisms, regulating actin to enhance cellular migration to injury sites. Its systemic effects make it valuable for overall recovery support rather than targeted healing. Weekly doses of 2-5mg are typical during recovery phases.
Peptides for tendon repair become increasingly important as men age and accumulated stress catches up with connective tissues. The combination of TRT's anabolic effects with healing peptides' regenerative properties creates comprehensive support for active men.
Cognitive and sleep peptides
Testosterone production occurs primarily during sleep, making sleep quality directly relevant to hormone optimization. DSIP dosing protocols can enhance deep sleep patterns, supporting natural testosterone production.
Delta sleep inducing peptide works on multiple neurotransmitter systems to normalize sleep architecture. For men with disrupted sleep patterns affecting testosterone, DSIP offers targeted support without the dependency risks of pharmaceutical sleep aids.
Semax provides nootropic effects through ACTH fragment activity. Enhanced cognition, memory, and neuroprotection complement the cognitive benefits of testosterone optimization. For men experiencing brain fog as a low testosterone symptom, Semax can accelerate improvements.
Pinealon supports circadian rhythm regulation and sleep quality through its effects on the pineal gland. Normal circadian function is essential for optimal testosterone production.
Dosing and administration
Proper peptide dosing requires understanding reconstitution, calculation, and administration techniques. Errors in any of these areas can compromise results or safety.
Reconstitution basics
Most peptides arrive as lyophilized powder requiring reconstitution with bacteriostatic water before use. The reconstitution process directly affects peptide stability and dosing accuracy.
Use bacteriostatic water rather than sterile water for peptides you'll use over multiple days. The benzyl alcohol preservative in bacteriostatic water prevents bacterial growth. Sterile water contains no preservative and should only be used for single-use preparations.
The peptide reconstitution calculator simplifies dosing math. For example, adding 2mL of bacteriostatic water to a 5mg vial creates a concentration of 2.5mg per mL, or 250mcg per 0.1mL (10 units on an insulin syringe).
When adding water to peptide vials, direct the stream against the glass wall rather than directly onto the powder. Swirl gently rather than shaking to dissolve. Aggressive mixing can damage peptide structures.
Storage requirements
Unreconstituted peptides remain stable at room temperature for short periods but benefit from refrigeration. Understanding peptide stability at room temperature helps with travel and storage decisions.
Once reconstituted, peptides require refrigeration. Most maintain potency for 3-4 weeks refrigerated. Reconstituted peptide shelf life varies by specific compound, with some remaining stable longer than others.
Never freeze reconstituted peptides. The expansion and contraction can damage structures. Unreconstituted peptides can be frozen for long-term storage if needed.
Protect peptides from light exposure, which can degrade certain compounds. Store vials in their original boxes or wrap in foil if exposed to light regularly.
Injection technique
Subcutaneous injection remains the standard administration route for most peptides. Using insulin syringes simplifies dosing and reduces discomfort.
Common injection sites include abdominal fat, upper thighs, and the fatty area behind the arms. Rotate sites to prevent localized issues. Clean sites with alcohol before injection.
Some peptides, particularly BPC-157, can be injected locally near injury sites for enhanced targeted effects. This subcutaneous injection places the peptide closer to the treatment area.
Nasal administration works for certain peptides. Nasal spray peptide delivery offers convenience for peptides like Semax and PT-141, though absorption varies between individuals.
Timing considerations
Peptide timing can significantly affect results. Growth hormone peptides work best administered before bed, leveraging natural nighttime GH release. Taking them with food reduces effectiveness due to insulin interference.
Kisspeptin timing should mimic natural pulsatile patterns. Morning administration aligns with typical testosterone rhythms. Avoiding daily continuous use prevents desensitization.
BPC-157 and TB-500 can be administered at any time, though consistent timing helps establish routine. Splitting BPC-157 doses between morning and evening may enhance effects for some.
PT-141 should be administered 30-60 minutes before anticipated sexual activity. Effects last several hours, and some men experience nausea if doses are too high or taken too frequently.
What results to expect and when
Setting realistic expectations prevents disappointment and helps you evaluate whether your protocol is working. Understanding peptide result timelines is essential for protocol assessment.
Timeline for TRT with peptide enhancement
For men adding peptides to existing TRT, the TRT benefits are already established. Peptide additions create layered improvements over time.
HCG effects on testicular volume become noticeable within 2-4 weeks. Men often report return of testicular fullness within the first month of adding HCG to TRT.
Growth hormone peptide effects develop gradually. Sleep improvements often appear within the first week. Body composition changes, enhanced recovery, and skin improvements typically emerge over 8-12 weeks. Maximum benefits may require 4-6 months of consistent use.
Recovery peptide effects vary by application. For acute injuries, many men notice accelerated healing within 2-4 weeks. Chronic issues may require longer protocols.
Timeline for peptide alternatives to TRT
Men using peptides instead of TRT need more patience. Natural testosterone restoration through peptides typically shows:
Kisspeptin effects on testosterone can be rapid, with studies showing increases within hours of administration. However, sustainable optimization through pulsatile protocols develops over weeks to months.
Enclomiphene typically normalizes testosterone within 2-4 weeks of consistent use. Maximum effects may require 6-8 weeks.
Overall symptom improvement from peptide-based testosterone optimization often parallels blood work changes, though some men report feeling better before labs show significant changes, and vice versa.
Tracking progress
Regular blood work guides protocol adjustments. For testosterone optimization, key markers include total testosterone, free testosterone, LH, FSH, estradiol, and SHBG.
For growth hormone peptides, IGF-1 serves as a proxy for GH status, as direct GH measurement is impractical due to pulsatile release patterns.
Beyond blood work, track subjective markers: energy, libido, mood, sleep quality, recovery from training, body composition changes. Peptide transformation stories often emphasize these quality-of-life improvements as much as lab values.
Safety considerations and side effects
Both TRT and peptides require respect for potential risks. Understanding peptide safety enables informed decisions about risk management.
Common side effects
TRT side effects are well documented: testicular atrophy, elevated hematocrit, estrogen imbalances, potential cardiovascular effects, skin changes, and mood alterations. Most are manageable with proper monitoring and adjunct therapies.
Peptide side effects tend to be milder but vary by compound. Common issues include:
Injection site reactions: redness, itching, or mild pain at injection sites. These typically resolve with proper rotation and technique.
Water retention: GH peptides can cause temporary fluid retention, particularly in the hands and feet. This usually stabilizes as the body adjusts.
Glucose effects: GH peptides may affect insulin sensitivity in both directions, requiring attention from those with metabolic concerns.
Nausea: PT-141 commonly causes nausea, particularly at higher doses. Starting low and titrating up minimizes this issue.
Fatigue or flushing: Some peptides cause temporary fatigue or flushing that resolves as tolerance develops.
Serious considerations
Long-term safety data for many peptides remains limited. Most were never intended for chronic human use, and understanding of long-term effects continues developing.
Cancer concerns exist theoretically for growth-promoting peptides, though direct evidence is lacking. Men with history of hormone-sensitive cancers should exercise particular caution and involve oncologists in decisions.
Cardiovascular effects require monitoring, particularly when combining multiple growth-promoting agents. Regular health screenings should continue regardless of peptide use.
Quality and purity concerns affect the peptide market. Without FDA regulation, peptide quality varies significantly between sources. Third-party testing provides some assurance, but users assume inherent risks with unregulated products.
Contraindications
Certain conditions warrant avoiding specific peptides or requiring careful medical supervision:
Active malignancies contraindicate growth-promoting peptides. Even with cancer in remission, growth factors theoretically could stimulate dormant cells.
Cardiovascular disease requires careful monitoring with TRT and GH peptides, which can affect fluid balance and metabolic parameters.
Diabetes or significant insulin resistance requires attention when using GH peptides due to their effects on glucose metabolism.
Fertility concerns should guide peptide selection. While some peptides preserve fertility better than TRT, effects vary, and men actively trying to conceive need careful protocol design.
Working with healthcare providers
Ideal management involves practitioners experienced with both TRT and peptides. Unfortunately, few physicians have deep expertise in both areas.
TRT clinics increasingly offer peptides but may lack sophisticated understanding of optimal combinations and timing. Peptide-focused practitioners may not fully appreciate TRT integration.
Finding practitioners who understand peptide therapy clinics and TRT integration improves outcomes. Bringing research and asking informed questions helps establish collaborative relationships.
Regular monitoring through blood work, health screenings, and symptom tracking remains essential regardless of practitioner involvement. Your engagement in your own health optimization matters most.
Cost considerations
The financial aspects of TRT and peptide protocols deserve honest assessment. Understanding peptide therapy costs helps with planning and decision-making.
TRT costs
Traditional TRT through clinics typically runs $100-300 monthly, including testosterone, supplies, and basic monitoring. More comprehensive clinic programs with frequent labs and consultations can exceed $400-500 monthly.
Insurance may cover TRT for diagnosed hypogonadism, significantly reducing out-of-pocket costs. Coverage varies dramatically between plans and requires documented medical necessity.
Self-managed TRT with prescriptions from regular physicians can cost $40-100 monthly for testosterone cypionate, plus supplies and lab work.
Peptide costs
Peptides are typically not covered by insurance and must be paid out of pocket. Costs vary significantly by compound and source:
HCG: $60-100 monthly for typical dosing
CJC-1295/Ipamorelin combination: $100-200 monthly
Sermorelin: $100-200 monthly
BPC-157: $50-150 monthly depending on dose
TB-500: $80-150 monthly
Kisspeptin: $100-200 monthly
Comprehensive peptide protocols combining multiple compounds can reach $300-500 monthly or more. Costs add quickly when stacking multiple peptides.
Value considerations
Cost-per-benefit analysis helps prioritize spending. HCG for testicular maintenance on TRT offers clear value given the alternative of atrophy. Growth hormone peptides provide benefits difficult to achieve otherwise but at significant cost.
Recovery peptides may be worth cycling strategically rather than running continuously. Using them during training intensification or injury recovery maximizes value.
Kisspeptin and enclomiphene for natural testosterone restoration can be more economical long-term than lifetime TRT, though initial costs may be similar.
Comparing approaches: TRT, peptides, or both
The right approach depends entirely on individual circumstances. Here's how different scenarios typically align with different strategies.
TRT alone makes sense when
Testosterone is severely deficient, below 200-250 ng/dL, with clear hypogonadal symptoms. Natural production is unlikely to restore adequate levels.
Age exceeds 50-55 with progressive decline. Natural production capacity diminishes, reducing peptide effectiveness.
Fertility is not a concern. Men who have completed family building or chosen not to have children face fewer downsides from TRT.
Rapid symptom relief is needed. TRT delivers faster, more reliable results than peptide alternatives.
Peptides alone make sense when
Testosterone is mildly to moderately low, 300-450 ng/dL, with preserved testicular function.
Age is under 40-45 with secondary hypogonadism. Natural production capacity remains, and peptides can effectively stimulate it.
Fertility preservation matters. Peptides maintain or enhance fertility rather than suppressing it.
Avoiding lifelong commitment appeals. Peptides offer more flexibility in discontinuation.
Combination approaches make sense when
TRT is necessary but side effect mitigation is important. Adding HCG and other peptides addresses TRT limitations.
Optimizing beyond testosterone matters. GH peptides, recovery peptides, and cognitive peptides enhance TRT benefits.
Transitioning off TRT is desired. Peptides can support recovery of natural production.
Comprehensive hormone optimization is the goal. Maximum results often require multiple tools working synergistically.
Common mistakes to avoid
Understanding common peptide mistakes helps you avoid problems that derail results.
Starting too many peptides at once
The temptation to add everything simultaneously makes troubleshooting impossible. If you experience side effects or don't see results, you can't identify which compound is responsible.
Start with one or two peptides. Establish baseline response. Add additional compounds gradually, noting effects with each addition.
Ignoring quality concerns
The peptide market includes legitimate research companies and questionable operations. Compromised quality means compromised results at best and health risks at worst.
Use established sources with third-party testing. Reviewing peptide vendors before purchasing protects your investment and health.
Neglecting foundational factors
Peptides and TRT can't overcome terrible diet, inadequate sleep, excessive stress, or sedentary lifestyle. These fundamentals affect hormone optimization regardless of what you're taking.
Address lifestyle factors alongside any hormone protocol.
The combination creates multiplicative rather than additive benefits.
Skipping blood work
Subjective improvement matters, but blood work reveals what's actually happening hormonally. Regular testing guides adjustments and identifies issues early.
Test before starting any protocol. Test 4-6 weeks after changes. Test periodically for ongoing management.
Unrealistic expectations
Peptides aren't magic. TRT isn't magic. Both require time, consistency, and complementary lifestyle factors to deliver results.
Expect gradual improvement rather than overnight transformation. Trust the process while remaining attentive to whether things are moving in the right direction.
Frequently asked questions
Can I take testosterone and peptides at the same time?
Yes, many men successfully combine TRT with various peptides. Common additions include HCG for testicular maintenance, CJC-1295 with Ipamorelin for growth hormone support, and BPC-157 for recovery. Working with practitioners experienced in both TRT and peptides optimizes these combinations.
Will peptides replace TRT for low testosterone?
For some men, yes. Those with secondary hypogonadism where signaling is impaired but testicular function remains intact often respond well to peptides like kisspeptin or SERMs like enclomiphene. Men with severely low testosterone or primary hypogonadism typically need TRT because their testes can't adequately respond to stimulation.
What's the best peptide for testosterone?
Kisspeptin directly stimulates LH release and testosterone production, making it the most testosterone-specific peptide.
However, optimal peptide selection depends on your specific situation, existing hormone levels, and goals. Growth hormone peptides indirectly support testosterone through improved body composition and sleep.
Do peptides cause testosterone shutdown like TRT?
No. Peptides that stimulate natural testosterone production work through your body's feedback systems rather than replacing hormones directly. This maintains natural production capacity and avoids the shutdown associated with exogenous testosterone. However, some peptides require pulsatile dosing to avoid receptor desensitization.
How long do TRT peptide benefits last?
Benefits persist as long as you continue the protocol. For peptides maintaining testicular function on TRT, discontinuation leads to gradual atrophy resumption. For peptides stimulating natural testosterone, effects may persist longer as they support rather than replace natural function. Individual variation is significant.
Are TRT peptides safe?
When used properly with medical supervision, most peptides have acceptable safety profiles. However, long-term data remains limited for many compounds. Regular monitoring through blood work and health assessments helps identify issues early. Understanding the full safety picture enables informed decisions.
What peptides help with TRT side effects?
HCG addresses testicular atrophy and fertility concerns. GH peptides may help with body composition when TRT doesn't fully address fat distribution. DSIP can improve sleep if TRT disrupts sleep patterns. KPV may help with inflammation. Protocol customization based on specific side effects optimizes results.
How much do TRT peptide protocols cost?
Costs vary widely based on compounds used and sources. TRT alone runs $100-300 monthly through clinics. Adding peptides can increase costs by $100-500 monthly depending on how many compounds you use. Detailed cost breakdowns help with budgeting.
External resources
Kisspeptin-10 Is a Potent Stimulator of LH and Increases Pulse Frequency in Men - PubMed Central
Enclomiphene Citrate for the Treatment of Secondary Male Hypogonadism - PubMed Central
For researchers serious about optimizing their testosterone and hormone protocols, SeekPeptides provides the most comprehensive peptide resource available, with evidence-based guides, proven protocols, and a community of thousands who've navigated these exact questions.
In case I don't see you, good afternoon, good evening, and good night. May your testosterone stay optimal, your recovery stay swift, and your protocols stay effective.