Jan 9, 2026

Clinical evidence for peptide-based approaches to erectile dysfunction reveals mechanisms fundamentally different from conventional pharmaceutical interventions like sildenafil or tadalafil. Where traditional PDE5 inhibitors work downstream, blocking the enzyme that breaks down cyclic GMP to maintain erections once arousal occurs, specific peptides target the upstream neurological and vascular pathways that initiate and sustain sexual function. PT-141, the most extensively studied peptide for erectile dysfunction, activates melanocortin receptors in the hypothalamus to create genuine desire and arousal, not merely the mechanical capacity for erection.
BPC-157 supports the vascular infrastructure through nitric oxide modulation, while kisspeptin addresses hormonal dysfunction at the hypothalamic level. The research encompasses compounds working through central nervous system activation, vascular enhancement, tissue regeneration, and hormonal optimization, each addressing different etiologies of erectile dysfunction that pharmaceutical approaches often miss.
SeekPeptides provides comprehensive resources for understanding these mechanisms and developing personalized approaches.
For you, this guide examines every peptide with documented relevance to erectile function, analyzing molecular pathways, reviewing available research, detailing practical protocols, comparing effectiveness across different presentations, and helping you understand which compounds address specific underlying causes of dysfunction.
Understanding erectile dysfunction: why peptides offer unique advantages
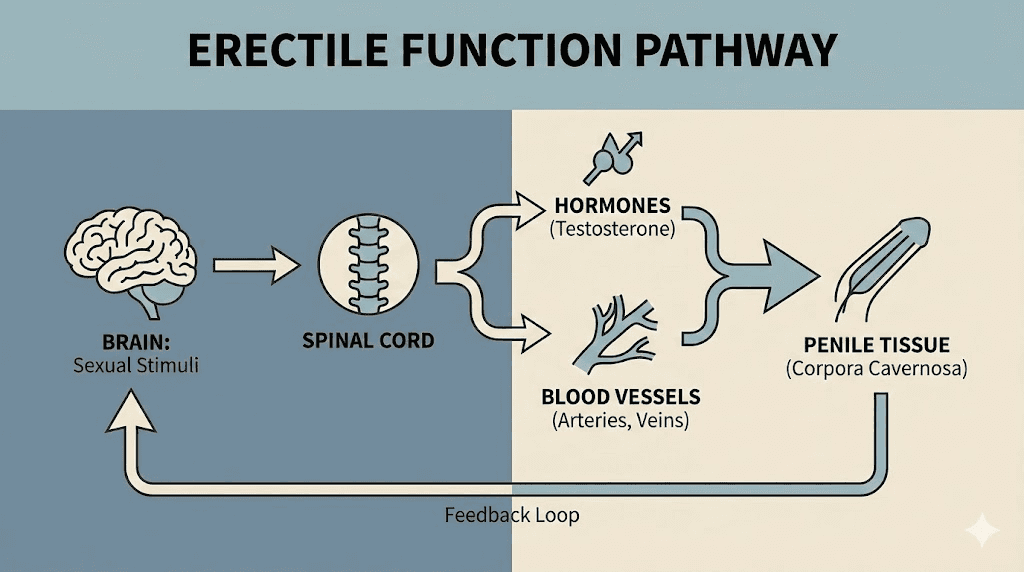
Erectile function represents one of the most complex physiological processes in the male body. It requires precise coordination between neurological signaling, hormonal balance, vascular function, and tissue health. When any component fails, the entire system suffers.
Most men think erectile dysfunction means blood flow problems. This oversimplification leads to overreliance on PDE5 inhibitors that address only one piece of a multifactorial puzzle.
The complete erectile response involves five interconnected systems. Neurological initiation begins in the brain, where arousal triggers descending signals through the spinal cord to the erectile tissue. Hormonal regulation through testosterone, dopamine, and other signaling molecules modulates libido and responsiveness. Vascular function enables blood to flow into and remain within the corpora cavernosa. Nitric oxide production relaxes smooth muscle to allow engorgement. Tissue integrity maintains the structural capacity for tumescence and rigidity.
Traditional ED medications target only the vascular component. They inhibit phosphodiesterase type 5, the enzyme that degrades cyclic GMP, thereby prolonging smooth muscle relaxation once the erectile cascade has already begun. But they cannot initiate desire. They cannot address low libido. They cannot repair damaged vascular tissue or correct hormonal imbalances.
This is where peptides demonstrate their unique value.
PT-141 works directly in the brain, activating the melanocortin system that generates sexual desire. It creates arousal rather than merely enabling mechanical function. BPC-157 enhances nitric oxide production and promotes vascular healing at the tissue level. Kisspeptin stimulates the hypothalamic-pituitary-gonadal axis to optimize testosterone production. TB-500 promotes angiogenesis, potentially improving blood flow capacity over time.
Understanding how peptides work reveals why they offer advantages for men whose ED stems from causes beyond simple vascular insufficiency. Rather than forcing a response through enzyme inhibition, peptides address root causes across multiple physiological systems.
Categorizing erectile dysfunction by etiology
Different causes of ED respond to different interventions. Understanding the underlying etiology guides peptide selection.
Neurogenic ED stems from disrupted nerve signaling. Spinal cord injuries, multiple sclerosis, diabetic neuropathy, and prostate surgery can damage the nerves controlling erection. These men often have intact vascular systems but cannot initiate or maintain the neurological cascade. PT-141's central mechanism may benefit this population by activating alternative arousal pathways.
Vasculogenic ED involves impaired blood flow. Atherosclerosis, hypertension, diabetes, and cardiovascular disease damage blood vessels throughout the body, including those supplying the penis. BPC-157 and TB-500 may support vascular repair and function in these cases.
Hormonal ED results from testosterone deficiency, elevated prolactin, thyroid dysfunction, or disrupted hypothalamic signaling. Kisspeptin and growth hormone secretagogues like ipamorelin address hormonal causes at the regulatory level.
Psychogenic ED originates from anxiety, depression, stress, or relationship issues. The neurological arousal pathways remain intact but are suppressed by psychological factors. PT-141's central activation may help override inhibitory signals.
Mixed etiology combines multiple factors. Most men with ED actually have contributions from several categories. This reality makes multi-target approaches particularly valuable.
The complete guide to peptides for men provides additional context for understanding how different compounds address male health concerns.
PT-141 (Bremelanotide): the central arousal activator
PT-141 stands alone as the only peptide with direct, documented effects on sexual arousal through central nervous system activation. Unlike every other intervention for ED, PT-141 creates desire rather than merely enabling mechanical response.
This makes it fundamentally different from Viagra, Cialis, or any vascular-targeting compound.
Mechanism of action
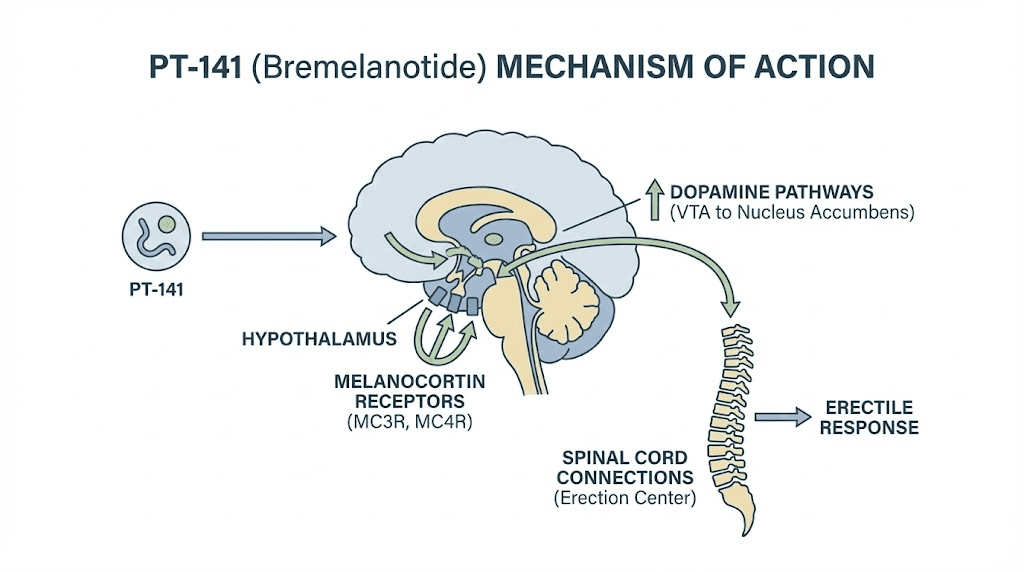
PT-141 is a synthetic peptide derived from Melanotan II, specifically designed to activate melanocortin receptors MC3R and MC4R in the hypothalamus. These receptors regulate sexual behavior, appetite, and energy homeostasis.
When PT-141 binds to hypothalamic melanocortin receptors, it triggers a cascade of downstream effects. Dopamine release increases in brain regions associated with sexual motivation and reward. Descending neural pathways activate, sending pro-erectile signals through the spinal cord. Sensitivity to sexual stimuli heightens. The psychological experience of desire intensifies.
This represents true arousal induction, not the permissive vascular effects of PDE5 inhibitors.
Research published in the Journal of Sexual Medicine demonstrated that PT-141 improved erectile function in men who had failed to respond to sildenafil. The peptide worked where conventional medication could not, precisely because it targeted a different mechanism entirely.
Understanding peptide mechanisms helps explain why PT-141 succeeds in cases where vascular interventions fail. The compound addresses neurological and psychological barriers to arousal that blood flow enhancement cannot overcome.
Clinical evidence for PT-141
PT-141 has progressed through rigorous clinical trials, eventually receiving FDA approval as Vyleesi for hypoactive sexual desire disorder in women. The research in men, though less publicized, proves equally compelling.
Phase II trials in men with erectile dysfunction showed statistically significant improvements in erectile function scores compared to placebo. Subjects reported enhanced desire, improved arousal, and greater satisfaction with sexual encounters. Importantly, these benefits appeared in men with various ED etiologies, suggesting broad applicability.
A study specifically examining PT-141 in sildenafil non-responders found that the peptide improved erectile function in approximately 70% of subjects who had failed conventional treatment. This finding has profound implications for men who have exhausted pharmaceutical options.
The onset of effects typically occurs within 30-60 minutes of administration. Duration extends 6-12 hours for many users. Unlike PDE5 inhibitors, PT-141 does not require sexual stimulation to produce some initial effects, though optimal response still involves appropriate context.
For detailed administration guidance, consult the PT-141 usage guide and nasal spray instructions.
PT-141 dosing protocols
Research protocols typically examine PT-141 in the 1-2mg range for subcutaneous administration. The PT-141 nasal spray for men offers an alternative delivery method with different absorption characteristics.
Starting protocol: Begin with 0.5-1mg subcutaneously to assess tolerance. Nausea represents the most common side effect and appears dose-dependent. Lower initial doses allow adaptation while still producing effects.
Standard protocol: 1.5-2mg subcutaneously, administered 30-60 minutes before anticipated sexual activity. Most research suggests limiting use to no more than 8 doses per month to maintain receptor sensitivity.
Nasal administration: Intranasal delivery offers convenience but may produce more variable absorption. Dosing typically ranges from 1-2mg delivered intranasally. The nasal spray peptides guide covers administration techniques.
Proper reconstitution ensures accurate dosing. The peptide reconstitution calculator helps determine appropriate bacteriostatic water volumes for your specific vial concentration.
The peptide calculator assists with precise dose measurement from reconstituted solutions.
Side effects and safety considerations
PT-141 demonstrates a distinct side effect profile compared to PDE5 inhibitors. Nausea occurs commonly, particularly at higher doses or initial exposures. Most users report adaptation over subsequent doses. Flushing affects some individuals, typically mild and transient. Headache occurs occasionally but generally less frequently than with sildenafil.
Blood pressure changes represent a theoretical concern given the peptide's central effects, though clinical data shows minimal cardiovascular impact at standard doses. Men with uncontrolled hypertension or cardiovascular disease should exercise appropriate caution.
The peptide safety and risks guide provides comprehensive information on minimizing adverse effects and identifying contraindications.
Melanotan II: the multifunctional melanocortin agonist
Melanotan II is the parent compound from which PT-141 was derived. It activates a broader spectrum of melanocortin receptors, producing effects on both sexual function and skin pigmentation.
Many men discovered Melanotan II's sexual effects while using it for tanning purposes. The spontaneous erections and enhanced libido proved powerful enough that researchers isolated the specific active region, eventually developing PT-141 for more targeted sexual applications.
Broader melanocortin activation
Melanotan II activates five melanocortin receptor subtypes with varying affinity. MC1R activation stimulates melanin production, producing the tanning effect. MC3R and MC4R activation generates sexual and appetite-modulating effects. MC2R relates to adrenal function. MC5R influences exocrine gland activity.
This broad activation profile means Melanotan II produces multiple simultaneous effects. Users experience enhanced pigmentation, reduced appetite, increased libido, and improved erectile function. For some, this multifunctionality represents a feature. For others pursuing only sexual benefits, the tanning and appetite effects are unwanted.
Sexual function research
Early Melanotan II research documented spontaneous erections in a significant percentage of male subjects, occurring even without sexual stimulation. This finding prompted further investigation into the compound's sexual applications.
Studies showed improved erectile function in men with ED, enhanced libido regardless of baseline desire levels, and increased sexual satisfaction. The effects appeared more pronounced than those seen with PDE5 inhibitors alone, likely because Melanotan II addresses central arousal rather than peripheral vascular function.
The compound demonstrated effectiveness across various ED etiologies, including cases with psychological components that typically respond poorly to conventional medications.
Comparing Melanotan II and PT-141
Melanotan II advantages: Potentially longer-lasting sexual effects due to broader receptor activation. Additional tanning benefits for those who desire them. Lower cost per dose in most markets. Established user experience base from tanning communities.
PT-141 advantages: More selective for sexual function receptors. No unwanted tanning or pigmentation changes. Cleaner side effect profile focused on sexual applications. FDA-approved formulation available. More predictable effects without confounding receptor activation.
For men pursuing purely erectile benefits without pigmentation changes, PT-141 represents the more targeted option. For those who appreciate multiple melanocortin effects, Melanotan II offers broader utility.
Melanotan II protocols
Melanotan II protocols typically involve loading and maintenance phases due to the tanning component.
Loading phase: 0.25-0.5mg daily subcutaneously for 2-4 weeks. This establishes baseline melanin stimulation and allows assessment of sexual effects.
Maintenance phase: 0.5-1mg 2-3 times weekly to maintain effects. Some users reduce to once weekly depending on individual response.
Sexual-focused protocol: For those primarily interested in erectile effects, 0.5-1mg administered 2-4 hours before anticipated activity. Effects may last 24-48 hours.
The peptide dosing guide provides additional context for establishing individual protocols.
BPC-157: vascular foundation for erectile health
BPC-157 approaches erectile function from an entirely different angle than melanocortin agonists. Rather than targeting central arousal, this gastric pentadecapeptide supports the vascular infrastructure that enables erection.
The connection is straightforward: erection requires blood flow. Damaged blood vessels, impaired nitric oxide signaling, or compromised endothelial function all limit erectile capacity regardless of desire or neurological function.
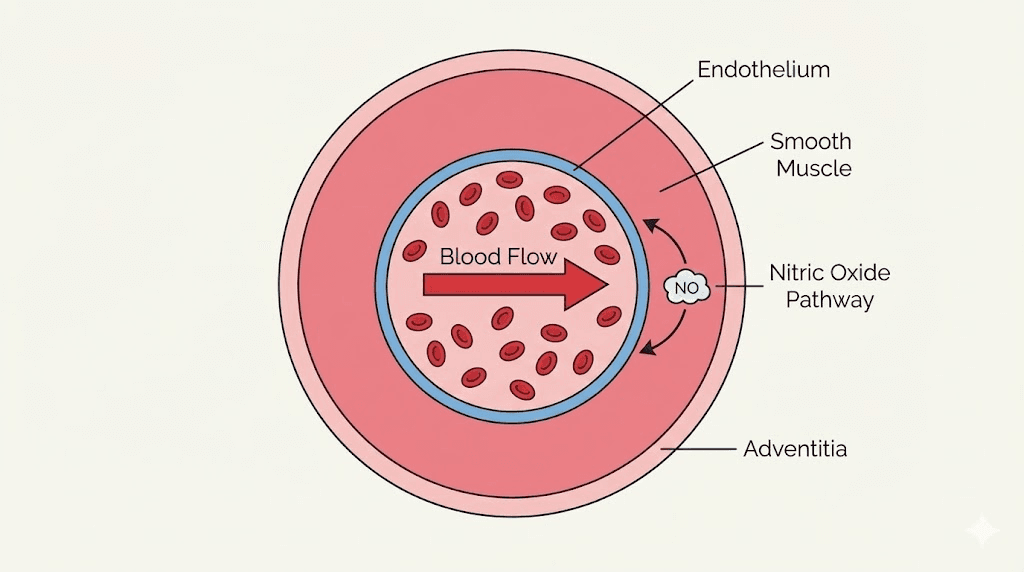
Nitric oxide modulation
Nitric oxide serves as the primary molecular trigger for erection. When arousal occurs, nerve terminals and endothelial cells release NO, which activates guanylate cyclase, increases cyclic GMP, relaxes smooth muscle, and allows blood to engorge the corpora cavernosa.
Research demonstrates that BPC-157 influences multiple points in the NO pathway. The peptide enhances NO production through endothelial nitric oxide synthase activation. It protects the endothelium from damage that impairs NO release. It counteracts the effects of NO-blocking agents in research models.
A study examining BPC-157 in L-NAME-treated animals, where NO production was pharmacologically blocked, found that the peptide partially restored normal function. This suggests BPC-157 may support NO signaling even in compromised vascular environments.
For men whose ED stems from vascular insufficiency, endothelial dysfunction, or impaired NO signaling, BPC-157 addresses causative factors rather than merely overriding symptoms.
Vascular healing properties
Beyond acute NO modulation, BPC-157 demonstrates remarkable vascular healing capabilities. Research shows the peptide accelerates blood vessel repair following injury. It promotes angiogenesis, the formation of new blood vessels. It protects vessels from oxidative stress and inflammatory damage.
These properties have implications for men with vascular ED. Rather than simply enhancing function in damaged tissue, BPC-157 may support actual repair and regeneration of the vascular infrastructure.
Studies examining BPC-157 in various vascular injury models consistently show improved healing, reduced fibrosis, and better functional outcomes compared to controls. The peptide appears to coordinate multiple repair mechanisms simultaneously.
Understanding what BPC-157 is and how to take it provides foundational knowledge for erectile health applications.
BPC-157 protocols for erectile support
BPC-157 protocols for erectile support emphasize consistent dosing to support ongoing vascular function and healing rather than acute pre-activity administration.
Standard protocol: 250-500mcg daily, administered subcutaneously. Many users split into twice-daily doses for more sustained levels. The BPC-157 dosage calculator helps determine precise quantities.
Vascular focus protocol: 500mcg twice daily for enhanced vascular support. This higher dosing approach may benefit men with significant endothelial dysfunction.
Duration: Most protocols run 4-8 weeks. BPC-157 does not appear to require cycling in the same way hormone-affecting peptides might. Longer-term use seems well-tolerated based on available data.
The BPC-157 5mg dosing guide provides detailed instructions for common vial sizes.
For comparison with other healing peptides, review BPC-157 vs TB-500 and explore BPC-157 alternatives.
Combining BPC-157 with PT-141
The combination of BPC-157 and PT-141 addresses both vascular function and central arousal, potentially offering synergistic benefits for erectile dysfunction.
BPC-157 provides the vascular foundation, supporting blood vessel health, NO signaling, and tissue repair. PT-141 activates the neurological arousal pathways that initiate the erectile response. Together, they address both the supply side (vascular capacity) and the demand side (central drive) of erectile function.
This combination approach may particularly benefit men with mixed-etiology ED where both vascular and psychological/neurological factors contribute.
The peptide stack calculator helps plan combination protocols. Additional information on stacking strategies appears in the peptide stacks guide and how many peptides you can take at once.
Kisspeptin: hormonal gateway to sexual function
Kisspeptin controls the master switch of the reproductive hormone cascade. This neuropeptide initiates the entire hypothalamic-pituitary-gonadal axis, making it relevant for ED with hormonal etiology.
When kisspeptin neurons in the hypothalamus fire, they trigger GnRH release. GnRH stimulates the pituitary to release LH and FSH. LH stimulates the testes to produce testosterone. Dysfunction anywhere in this cascade impairs sexual function.
The HPG axis and erectile function
Testosterone plays multifaceted roles in erectile function. It modulates libido through central effects. It supports nitric oxide production in erectile tissue. It maintains the structural integrity of the corpora cavernosa. It influences neurotransmitter systems involved in arousal.
Men with hypogonadism frequently experience erectile dysfunction alongside reduced libido. Testosterone replacement therapy often improves erectile function in these cases, demonstrating the hormone's essential role.
Kisspeptin represents an upstream approach to testosterone optimization. Rather than replacing testosterone exogenously, kisspeptin stimulates endogenous production through natural regulatory pathways.
Research on kisspeptin and sexual function
Clinical studies have examined kisspeptin administration in various male populations. Research in The Journal of Clinical Investigation found that kisspeptin enhanced LH pulsatility and testosterone levels in healthy men. Studies in hypogonadotropic hypogonadism showed restoration of normal pulsatile hormone release.
Particularly relevant for erectile function, research published in JCI Insight demonstrated that kisspeptin enhanced brain activity in regions associated with sexual arousal and romantic attraction. Subjects showed increased penile tumescence in response to erotic stimuli following kisspeptin administration.
These findings suggest kisspeptin affects sexual function through both hormonal optimization and direct central effects on arousal circuitry.
When kisspeptin makes sense
Kisspeptin research is most relevant for ED with hormonal components. Men with low testosterone, particularly when accompanied by low or inappropriately normal LH, may benefit from kisspeptin-mediated HPG axis stimulation.
Specific situations where kisspeptin may apply include secondary hypogonadism with hypothalamic dysfunction, age-related testosterone decline, metabolic syndrome-associated hormonal disruption, and recovery from exogenous testosterone use.
For ED with purely vascular or psychological etiology and normal hormonal status, kisspeptin may offer less direct benefit. However, even eugonadal men may experience enhanced sexual response through kisspeptin's central effects.
The interplay between hormonal optimization and sexual function connects to broader topics covered in the testosterone boosters vs peptides comparison.
TB-500: angiogenesis and vascular support
TB-500 (Thymosin Beta-4) is primarily recognized for tissue repair applications, but its effects on blood vessel formation and cardiovascular function make it relevant for erectile health.
Angiogenesis, the formation of new blood vessels, represents a fundamental mechanism for improving blood flow capacity. TB-500 potently promotes this process.
Angiogenic mechanisms
TB-500 upregulates actin, a protein essential for cell migration and blood vessel formation. When endothelial cells need to form new capillaries, they require actin to migrate into new territory. Research shows TB-500 significantly enhances this process.
Studies demonstrate that TB-500 promotes endothelial cell migration and proliferation. It supports the formation of functional new blood vessels in tissue with compromised circulation. It enhances tissue perfusion in areas previously limited by vascular insufficiency.
For erectile function, better blood vessel networks mean improved capacity for the blood flow that produces erection. This represents a structural improvement rather than merely a functional enhancement.
The TB-500 benefits overview covers applications across multiple tissue types.
Cardiovascular implications
Research on TB-500 and cardiac function reveals broader cardiovascular benefits. Studies show improved cardiac efficiency under stress. Enhanced blood vessel formation in damaged tissue. Reduced inflammation that impairs vascular function. Support for overall cardiovascular health.
Since ED often shares etiology with cardiovascular disease, compounds supporting cardiovascular health may indirectly benefit erectile function. The endothelial dysfunction underlying coronary artery disease frequently manifests as ED years before cardiac symptoms appear.
TB-500's systemic vascular benefits may therefore support erectile function as part of broader cardiovascular improvement.
TB-500 protocols
Loading phase: 2-2.5mg twice weekly for 4-6 weeks. This establishes tissue levels and initiates angiogenic processes.
Maintenance phase: 2-2.5mg once weekly or every 10-14 days. Maintains benefits without requiring continuous high-dose administration.
The TB-500 dosage calculator assists with precise dose determination.
For comprehensive comparison, review the BPC-157 vs TB-500 analysis and consider TB-500 alternatives.
Combining TB-500 with BPC-157
TB-500 and BPC-157 work through complementary mechanisms, making them a popular combination for vascular support.
TB-500 promotes systemic angiogenesis and tissue repair. BPC-157 provides more targeted effects on nitric oxide signaling and localized healing. Together, they address vascular health from multiple angles.
For erectile function specifically, this combination may support both the structural capacity for blood flow (TB-500) and the functional signaling that triggers vasodilation (BPC-157).
Learn more about combination approaches in the peptide stacks guide.
GHK-Cu: tissue regeneration and vascular health
GHK-Cu (Glycyl-L-Histidyl-L-Lysine Copper Complex) influences over 4,000 human genes. While not specific to sexual function, its effects on tissue health, vascular function, and systemic regeneration have implications for erectile capacity.
Gene expression and tissue maintenance
Research on GHK-Cu's gene expression profile reveals widespread effects relevant to erectile tissue. Enhanced collagen synthesis and remodeling supports structural integrity. Improved blood vessel health and function maintains vascular capacity. Anti-inflammatory effects protect tissue from damage. Antioxidant effects prevent cellular dysfunction. Support for nerve function and repair may benefit neurogenic components of erection.
For erectile function specifically, healthy tissue in the corpora cavernosa means better response to arousal signals and more efficient blood filling. The structural proteins, blood vessels, nerves, and smooth muscle all require ongoing maintenance that GHK-Cu may support.
The GHK-Cu complete guide covers mechanisms and applications in detail.
The copper connection
Copper is essential for multiple processes relevant to vascular and tissue health. Collagen and elastin synthesis depends on copper-containing lysyl oxidase. Connective tissue cross-linking requires copper. Superoxide dismutase, a critical antioxidant enzyme, contains copper. Various processes affecting vascular health involve copper-dependent enzymes.
GHK-Cu delivers copper in a bioavailable form directly to tissues. This may support vascular and erectile tissue maintenance in ways that dietary copper cannot replicate.
For dosing guidance, review the GHK-Cu 50mg dosage guide and how long GHK-Cu lasts.
GHK-Cu protocols for vascular support
Systemic protocol: 200-500mcg daily subcutaneously for general tissue and vascular support.
Duration: Protocols typically run 4-8 weeks. Some users employ ongoing maintenance dosing at reduced frequency.
GHK-Cu is best viewed as a supportive compound for overall tissue health rather than a primary intervention targeting erectile function specifically. Combined with more directly acting peptides like PT-141 or BPC-157, it may enhance outcomes by supporting the tissue foundation.
Growth hormone secretagogues: hormonal optimization
Growth hormone secretagogues influence sexual function through multiple hormonal pathways. While not directly targeting erection, their effects on body composition, energy, recovery, and overall hormonal milieu may support erectile health.
GH/IGF-1 axis and sexual function
Growth hormone and IGF-1 have documented effects on sexual health. GH supports lean body mass and reduces visceral fat, improving metabolic health that influences hormonal balance. IGF-1 promotes tissue health and may support erectile tissue maintenance. The GH axis interacts with the HPG axis, with adequate growth hormone supporting testosterone production.
Men with growth hormone deficiency frequently experience reduced libido and erectile dysfunction. GH replacement often improves sexual function in these cases.
Ipamorelin
Ipamorelin offers clean GH stimulation with minimal effects on cortisol, prolactin, or appetite. This selective profile makes it attractive for those seeking GH benefits without confounding hormonal effects.
For erectile function, ipamorelin may support improved body composition, enhanced recovery, better sleep quality affecting hormonal output, and maintenance of lean tissue mass. These indirect benefits contribute to overall hormonal health that underlies sexual function.
The ipamorelin vs CJC-1295 comparison details differences between secretagogue options.
CJC-1295
CJC-1295 extends GH release duration, providing more sustained elevation compared to pulse-type secretagogues. The CJC-1295 dosage calculator helps determine appropriate protocols.
Sustained GH elevation may support continuous lipolytic effects reducing visceral fat. Prolonged anabolic signaling supports tissue health. Extended recovery benefits improve training response. Maintained metabolic rate supports hormonal balance.
Many protocols combine CJC-1295 with ipamorelin for synergistic GH elevation through complementary mechanisms.
Hexarelin's unique cardiac effects
Hexarelin demonstrates cardioprotective properties independent of GH release. Research has identified hexarelin receptors directly on cardiac tissue, suggesting effects on heart function regardless of GH levels.
Studies show hexarelin protects cardiomyocytes from damage. It improves cardiac contractility. It enhances coronary blood flow. These cardiovascular effects may indirectly benefit erectile function given the shared vascular etiology between heart disease and ED.
Peptide comparison for erectile dysfunction
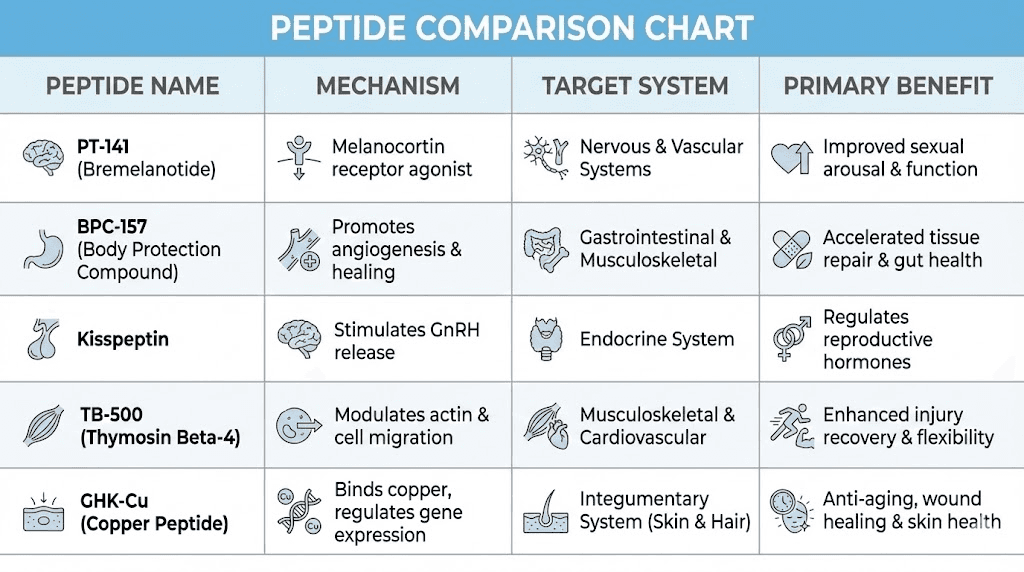
Understanding how different peptides compare helps guide selection based on individual presentation.
Peptide | Primary Mechanism | Target System | Best For | Onset | Duration |
|---|---|---|---|---|---|
PT-141 | Melanocortin activation | Central nervous system | Low desire, psychogenic ED | 30-60 min | 6-12 hours |
Melanotan II | Broad melanocortin | CNS + pigmentation | ED + tanning desired | 2-4 hours | 24-48 hours |
BPC-157 | NO modulation, healing | Vascular system | Vascular ED, endothelial dysfunction | Days-weeks | Ongoing |
Kisspeptin | HPG axis stimulation | Hormonal | Low testosterone, hormonal ED | Hours | Variable |
TB-500 | Angiogenesis | Vascular system | Chronic vascular insufficiency | Weeks | Long-term |
GHK-Cu | Gene expression, tissue | Systemic | Tissue maintenance, anti-aging | Weeks | Long-term |
Ipamorelin | GH release | Hormonal/metabolic | Body composition, energy | Weeks | Ongoing |
This comparison reveals that different peptides address different aspects of erectile function. Optimal selection depends on underlying etiology.
For more peptide comparisons, explore the peptides vs steroids comparison and peptides vs SARMs analysis.
Protocols for different ED presentations
Matching peptide selection and protocols to specific ED presentations optimizes outcomes. These protocols represent starting points based on available research, requiring individual adjustment.
Protocol 1: low desire with intact vascular function
Primary presentation: Reduced libido, decreased interest in sex, but ability to achieve erection when sufficiently aroused. Often psychological component present.
Primary compound: PT-141
Protocol: 1.5-2mg subcutaneously 30-60 minutes before anticipated activity. Limit to 8 doses monthly.
Supporting compound: Consider kisspeptin if hormonal optimization desired.
Expected timeline: Acute effects within 30-60 minutes. No cumulative protocol needed for PT-141 specifically.
Success indicators: Increased spontaneous sexual thoughts, enhanced response to sexual stimuli, improved arousal with appropriate context.
Protocol 2: vascular insufficiency
Primary presentation: Difficulty achieving or maintaining erection despite adequate desire. Often history of cardiovascular risk factors, diabetes, or documented vascular disease.
Primary compound: BPC-157
Protocol: 500mcg twice daily subcutaneously for 8-12 weeks.
Supporting compounds: TB-500 2.5mg twice weekly for enhanced angiogenic support. GHK-Cu 200mcg daily for tissue maintenance.
Expected timeline: Gradual improvement over 4-8 weeks as vascular function enhances. Not an acute intervention.
Success indicators: Improved morning erections, better erectile rigidity, enhanced response to PDE5 inhibitors if used concurrently.
Use the BPC-157 calculator and TB-500 calculator for precise dosing.
Protocol 3: hormonal dysfunction
Primary presentation: Low testosterone with accompanying symptoms including reduced libido, fatigue, and erectile dysfunction. Laboratory confirmation of hypogonadism.
Primary compound: Kisspeptin (if hypothalamic/pituitary dysfunction) or GH secretagogues (if broader hormonal optimization desired)
Kisspeptin protocol: Variable based on specific presentation. Acute dosing for LH stimulation assessment, or repeated administration for ongoing HPG support.
GH secretagogue protocol: Ipamorelin 200-300mcg plus CJC-1295 100mcg before bed, 5 days weekly.
Expected timeline: Hormonal changes measurable within 2-4 weeks. Symptomatic improvement may require 4-8 weeks.
Success indicators: Improved libido, better morning erections, laboratory confirmation of testosterone increase.
Protocol 4: mixed etiology comprehensive approach
Primary presentation: Multiple contributing factors including reduced desire, vascular compromise, and suboptimal hormones. Most common real-world scenario.
Compound combination:
- PT-141: 1.5mg as needed for acute arousal enhancement
- BPC-157: 500mcg daily for vascular support
- Ipamorelin: 200mcg before bed for hormonal optimization
Duration: BPC-157 and ipamorelin ongoing for 8-12 weeks. PT-141 as needed throughout.
Expected timeline: PT-141 effects acute. Vascular and hormonal improvements gradual over weeks.
Success indicators: Improved desire, better erectile function, enhanced response when combining with PT-141, overall vitality improvement.
Review the peptide cycle planning guide for structuring extended protocols.
Stacking strategies for erectile dysfunction
Strategic peptide combinations address multiple aspects of erectile function simultaneously. Understanding synergies optimizes stack design.
The comprehensive stack
PT-141 + BPC-157 + Ipamorelin
This combination addresses central arousal (PT-141), vascular function (BPC-157), and hormonal optimization (ipamorelin). It represents the most comprehensive peptide approach to erectile dysfunction.
Rationale: PT-141 provides acute arousal enhancement for on-demand use. BPC-157 builds vascular capacity over time. Ipamorelin supports overall hormonal milieu and body composition.
Implementation: Run BPC-157 and ipamorelin daily as foundational compounds. Add PT-141 as needed for specific occasions.
The vascular repair stack
BPC-157 + TB-500 + GHK-Cu
This combination prioritizes vascular health and tissue repair. It suits men with significant vascular ED who require infrastructure restoration rather than acute enhancement.
Rationale: BPC-157 modulates NO and promotes localized healing. TB-500 drives systemic angiogenesis. GHK-Cu supports tissue maintenance and gene expression favoring repair.
Implementation: BPC-157 500mcg twice daily. TB-500 2.5mg twice weekly during loading, then weekly. GHK-Cu 200mcg daily.
Duration: 8-12 weeks minimum to allow vascular remodeling.
The hormonal optimization stack
Kisspeptin + Ipamorelin + CJC-1295
This combination targets hormonal causes of ED through multiple axes. It suits men with documented hormonal dysfunction contributing to erectile problems.
Rationale: Kisspeptin stimulates endogenous testosterone production through HPG axis activation. GH secretagogues support overall hormonal health, body composition, and the interplay between GH and reproductive axes.
The peptide stack calculator helps plan multi-compound protocols. Additional guidance appears in how many peptides you can take at once.
Practical considerations for peptide therapy
Successful peptide use requires attention to practical details beyond compound selection.
Reconstitution and storage
Most peptides arrive as lyophilized powder requiring reconstitution with bacteriostatic water before use.
The reconstitution calculator determines appropriate water volumes for your vial concentration. The water for peptides guide explains different diluent options.
Once reconstituted, store peptides refrigerated at 2-8°C. Most reconstituted peptides remain stable for 4-6 weeks under proper storage. Review how long reconstituted peptides last in the fridge and peptide storage best practices.
Unreconstituted lyophilized peptides have longer stability. Do peptides expire covers shelf life considerations.
Administration techniques
Subcutaneous injection represents the most common administration route for most erectile dysfunction peptides. The peptide injections guide covers proper technique.
PT-141 and some other peptides also come in nasal spray formulations offering convenience but potentially variable absorption.
Review the list of injectable peptides and compare with injectable vs oral peptides.
Dosing precision
Accurate dosing ensures consistent results. The peptide calculator converts between concentration, volume, and dose. The peptide dosage calculation guide explains the mathematics.
Reference the peptide dosage chart for common compounds and ranges.
Timing considerations
Different peptides have different optimal timing. PT-141 requires 30-60 minutes before anticipated activity. GH secretagogues work best administered fasted, often before bed. BPC-157 and TB-500 can be administered at convenient times as they build cumulative effects.
Understanding how long peptides take to work sets appropriate expectations.
Sourcing quality peptides
Peptide quality varies significantly between vendors. Impure or degraded products produce unreliable results and potential safety concerns.
Review the best peptide vendors analysis for sourcing guidance. Consider research vs pharmaceutical peptides differences.
SeekPeptides provides resources for evaluating vendor quality and making informed purchasing decisions.
Safety and risk considerations
Any compounds affecting sexual function require careful safety consideration. Understanding risks enables informed decision-making.
General peptide safety
Peptides as a class demonstrate favorable safety profiles compared to small molecule pharmaceuticals. As protein fragments, they're metabolized through normal amino acid pathways without accumulating toxic metabolites.
However, specific risks exist for specific compounds. The peptide safety and risks guide provides comprehensive coverage.
Common considerations include injection site reactions, which are typically mild and transient. Allergic reactions are rare but possible. Individual compound-specific effects vary.
PT-141 specific considerations
PT-141's most common side effect is nausea, occurring in approximately 40% of users at standard doses. Nausea is typically mild and transient, often resolving within 1-2 hours. Starting with lower doses allows tolerance development.
Flushing affects some users. Blood pressure changes are possible given central mechanism, requiring caution in those with cardiovascular conditions.
Priapism, while theoretically possible with any pro-erectile compound, appears rare with PT-141. Standard medical advice applies: seek immediate attention for erections lasting more than 4 hours.
Melanocortin agonist considerations
Both PT-141 and Melanotan II affect melanocortin receptors. Monitoring for changes in moles or nevi is prudent, as melanocortin signaling relates to melanocyte activity. Any concerning skin changes warrant dermatological evaluation.
Interactions with ED medications
PT-141 works through different mechanisms than PDE5 inhibitors, potentially allowing combination use. However, combining multiple pro-erectile compounds increases priapism risk. Conservative approaches suggest using one or the other rather than both simultaneously.
BPC-157 and other vascular peptides should not produce concerning interactions with standard ED medications, as they support function through complementary rather than additive mechanisms.
Contraindications
Absolute contraindications vary by compound but generally include uncontrolled hypertension for melanocortin agonists, history of priapism for any pro-erectile compounds, and hormone-sensitive conditions for kisspeptin.
Always review individual compound contraindications before use. Consult healthcare providers for personalized guidance, particularly with pre-existing conditions.
Frequently asked questions
What is the most effective peptide for erectile dysfunction?
PT-141 (Bremelanotide) demonstrates the most direct effects on erectile function through central nervous system activation. It works differently from all other interventions by creating desire rather than merely enabling mechanical response. For men who have failed PDE5 inhibitors, PT-141 offers an alternative mechanism. However, the most effective peptide depends on underlying etiology, with BPC-157 better suiting vascular causes.
Can peptides work when Viagra fails?
Yes. PT-141 specifically demonstrated effectiveness in men who failed to respond to sildenafil in clinical trials. This success stems from PT-141's different mechanism, targeting central arousal rather than peripheral vascular function. Men whose ED has psychological, neurological, or desire-related components may respond to PT-141 despite PDE5 inhibitor failure.
How quickly do ED peptides work?
PT-141 produces effects within 30-60 minutes of administration, similar to PDE5 inhibitors. BPC-157, TB-500, and other vascular peptides work over weeks to months, building improvements through tissue repair rather than acute enhancement. Kisspeptin and GH secretagogues also require weeks for hormonal optimization. Review peptide onset timing for detailed timelines.
Are peptides for ED legal?
Peptide legality varies by jurisdiction and intended use. PT-141 has FDA approval for female hypoactive sexual desire disorder, making pharmaceutical formulations legally available. Research peptides exist in a different regulatory category. The are peptides legal guide covers regulatory nuances.
Can you combine ED peptides with each other?
Yes. Different peptides address different mechanisms, making combination approaches rational. PT-141 for central arousal combines logically with BPC-157 for vascular support. Review stacking limits and use the stack calculator for planning.
Do ED peptides have long-term effects?
PT-141 and Melanotan II produce acute effects without demonstrated long-term changes to erectile function. BPC-157 and TB-500 may produce lasting improvements through vascular repair, potentially maintaining benefits after cessation. Hormonal peptides like kisspeptin affect endogenous hormone production, which may have sustained effects depending on underlying physiology.
What are the side effects of PT-141?
Nausea is most common, affecting approximately 40% of users. Flushing, headache, and fatigue occur less frequently. Starting with lower doses reduces nausea risk. Side effects typically decrease with subsequent doses. Blood pressure monitoring is prudent for those with cardiovascular conditions. Review the safety guide for comprehensive information.
How SeekPeptides supports sexual health optimization
SeekPeptides provides the best resources for understanding and implementing peptide approaches to erectile dysfunction and broader sexual health.
The peptide calculator ensures accurate dosing for all compounds discussed in this guide. The reconstitution calculator simplifies preparation of lyophilized peptides.
Specialized calculators including the BPC-157 calculator, TB-500 calculator, and CJC-1295 calculator support protocol planning for specific compounds.
The peptide stack calculator helps design combination protocols addressing multiple aspects of erectile function simultaneously.
SeekPeptides remains committed to providing evidence-based guidance for peptide therapy applications, including sexual health optimization.
Helpful resources
In case I don't see you, good afternoon, good evening, and good night. May your desire stay strong, your vascular function stay optimal, and your peptide protocols stay effective. Join SeekPeptides.