Mar 25, 2026

You noticed it in the shower. A small, firm bump along your neck or under your jaw. Maybe near your armpit. It was not there before. Or maybe it was, and you just never paid attention. But now you are on semaglutide, and every new sensation in your body feels like a signal. A warning. Something worth Googling at 2 AM.
Here is the short answer. Swollen lymph nodes are not listed as a recognized side effect of semaglutide in the prescribing information from the FDA, the EMA, or any major regulatory body. They do not appear in the adverse event data from the STEP clinical trials, the SUSTAIN trials, or the SELECT cardiovascular outcomes trial. That is worth repeating. In clinical studies involving tens of thousands of patients, lymphadenopathy did not emerge as a semaglutide side effect.
But that does not mean your swollen lymph nodes are nothing. It means the cause is almost certainly something else, and some of those causes deserve urgent attention. Especially one that carries an FDA boxed warning on every semaglutide product sold. This guide breaks down what is actually happening when lymph nodes swell during semaglutide treatment, what the science says about GLP-1 receptor agonists and your immune system, which warning signs demand immediate medical evaluation, and when you can reasonably stop worrying. SeekPeptides members frequently ask about unexpected symptoms during peptide protocols, and this is one of the most anxiety-inducing.
What swollen lymph nodes actually mean
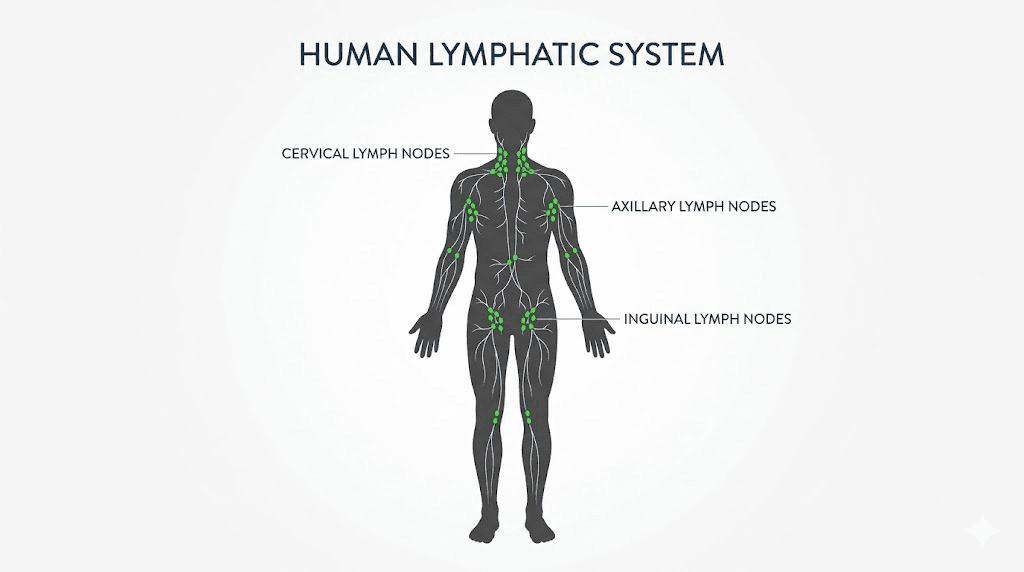
Lymph nodes are small, bean-shaped structures scattered throughout your body. You have roughly 600 of them. They sit along the lymphatic system like checkpoints, filtering lymph fluid and trapping bacteria, viruses, abnormal cells, and other debris your body needs to neutralize. When they swell, it means they are working. Fighting something. Responding to a threat, whether real or perceived.
The medical term is lymphadenopathy. And it is incredibly common. Most adults experience swollen lymph nodes several times per year without ever noticing. The ones you do notice tend to be in predictable locations. Under the jaw. Along the sides of the neck. Behind the ears. In the armpits. In the groin.
Swelling does not equal danger.
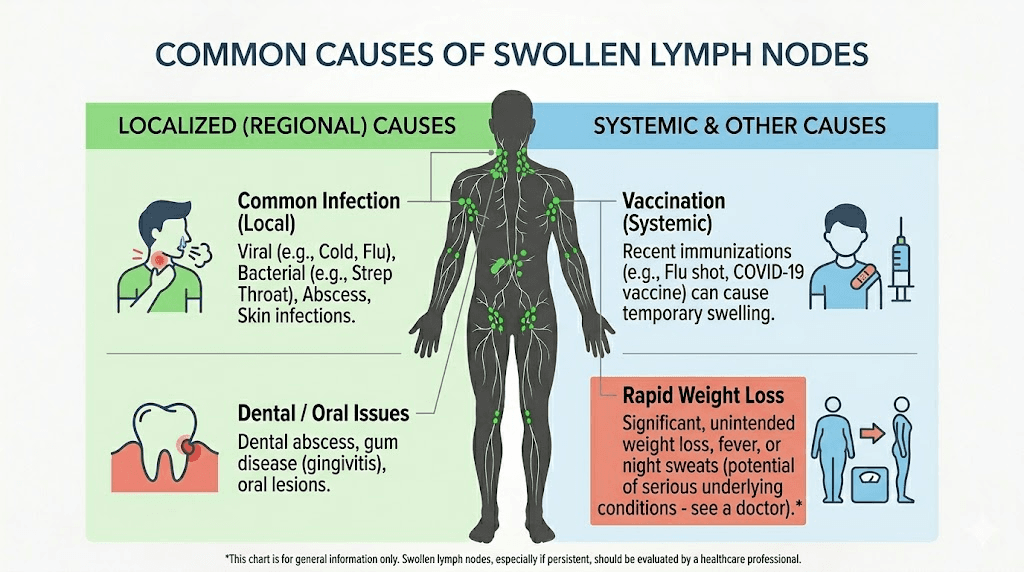
The vast majority of lymphadenopathy is reactive, meaning your immune system is responding to an infection, inflammation, or some other trigger. A cold. A sore throat. A dental infection. A skin wound. Even stress can do it. Reactive lymph nodes are usually soft, mobile, tender to the touch, and they resolve on their own within two to four weeks as the underlying cause clears.
Less commonly, swollen lymph nodes indicate something more serious. Autoimmune conditions. Chronic infections like tuberculosis or HIV. And in rare cases, malignancy. The characteristics that raise concern are hardness, immobility (the node feels fixed to surrounding tissue), painlessness, progressive growth over weeks, and involvement of multiple body regions simultaneously.
Understanding this distinction matters because it separates rational concern from unnecessary panic. When someone on semaglutide discovers a swollen lymph node, the question is not whether semaglutide caused it. The question is what actually did.
What the clinical evidence says about semaglutide and lymph nodes
The evidence is clear, and it is reassuring. Semaglutide does not cause lymphadenopathy based on everything we know from clinical trials and post-marketing surveillance data.
The STEP trial program, which evaluated semaglutide 2.4 mg for weight management, enrolled thousands of participants across multiple studies. STEP 1 alone randomized 1,961 adults. STEP 2 included 1,210 participants with type 2 diabetes. STEP 3 combined semaglutide with intensive behavioral therapy in 611 adults. STEP 4 examined treatment withdrawal in 902 participants. Across all of these trials, swollen lymph nodes did not appear as a treatment-emergent adverse event.
The SUSTAIN trials, which evaluated semaglutide for diabetes management, showed similar results. No lymphadenopathy signal.
The SELECT trial, the landmark cardiovascular outcomes study with over 17,600 participants followed for a mean of 39.8 months, produced the most comprehensive safety dataset for semaglutide available. Lymph node swelling was not identified as an adverse reaction.
This is not a matter of insufficient data. These trials collectively represent tens of thousands of patient-years of semaglutide exposure. If the drug caused meaningful lymphadenopathy, it would have surfaced.
The UK Medicines and Healthcare products Regulatory Agency does not list lymphadenopathy in the Summary of Product Characteristics for semaglutide. Neither does the FDA prescribing information for Ozempic or Wegovy. The European Medicines Agency assessment reports reach the same conclusion.
So if you have swollen lymph nodes while taking semaglutide, the medication is overwhelmingly unlikely to be the cause. But something is causing it. And several possibilities deserve careful investigation.
The thyroid cancer warning you must not ignore
Every box of Ozempic and Wegovy carries an FDA boxed warning, the most serious type of warning the agency issues. It concerns thyroid C-cell tumors.
In rodent studies, semaglutide caused dose-dependent and treatment-duration-dependent increases in the incidence of thyroid C-cell tumors, including medullary thyroid carcinoma. Rats and mice exposed to semaglutide developed these tumors at clinically relevant exposures. The mechanism appears related to GLP-1 receptor activation on thyroid C-cells, which are far more abundant and responsive in rodents than in humans.
The human data is more nuanced. A systematic review published in the International Journal of Clinical Practice found that the incidence of thyroid cancer in semaglutide-treated patients was less than 1%, suggesting no significant elevation of risk in clinical trial populations. However, one epidemiological study found a 58% higher risk of thyroid cancer in patients with type 2 diabetes who took GLP-1 receptor agonists for one to three years, though this study had significant limitations including confounding variables.
Why does this matter for lymph nodes?
Because medullary thyroid carcinoma, the specific cancer type linked to GLP-1 receptor agonist use in animal studies, presents with specific symptoms. And one of them is swollen lymph nodes in the neck.
The classic presentation includes a palpable thyroid nodule or lump in the front of the neck, hoarseness or voice changes, difficulty swallowing, enlarged cervical lymph nodes, and shortness of breath in advanced cases. If you notice swollen lymph nodes specifically in your neck while taking semaglutide, and especially if they are accompanied by any of these other symptoms, you need medical evaluation immediately. Not next week. Now.
This is not alarmism. The absolute risk remains very low based on current human data. But the boxed warning exists for a reason, and neck lymphadenopathy in a semaglutide user warrants thyroid evaluation as a first-line investigation.
Semaglutide is contraindicated in patients with a personal or family history of medullary thyroid carcinoma and in patients with Multiple Endocrine Neoplasia syndrome type 2. If either applies to you, you should not be taking semaglutide at all.
Common reasons lymph nodes swell during semaglutide treatment
Setting the thyroid concern aside, which your doctor can evaluate quickly with a physical exam, blood work, and potentially an ultrasound, there are many mundane explanations for lymphadenopathy that happen to coincide with semaglutide use.
Upper respiratory infections
This is the most common cause of swollen cervical and submandibular lymph nodes in adults. Colds, sinus infections, sore throats, and viral pharyngitis all trigger reactive lymphadenopathy. The nodes swell within days of symptom onset and typically resolve within two to three weeks. If you recently had a runny nose, cough, or sore throat, that is almost certainly your answer.
Dental infections and oral health issues
Cavities, gum disease, tooth abscesses, and recent dental procedures frequently cause swelling in the submandibular and cervical lymph nodes. These infections can smolder for weeks before the lymph node response becomes noticeable. Many people underestimate how profoundly dental health affects their lymphatic system.
Skin infections near the affected area
A cut that got mildly infected. An ingrown hair. A bug bite. A mild case of cellulitis. Any skin infection or inflammation near a lymph node chain can cause those nodes to swell. If you inject semaglutide in your abdomen and notice swollen inguinal lymph nodes (groin area), the injection site itself could be causing mild local inflammation, even without visible injection site reactions.
Injection site reactions
While injection site reactions to semaglutide are relatively uncommon compared to some other GLP-1 receptor agonists, they do occur. Erythema, pain, itching, and rarely, subcutaneous nodules at the injection site have been reported. A case report published in the Journal of the American Pharmacists Association documented injection-site nodules in a 75-year-old patient after dose escalation to 1 mg weekly. The nodules were hard, erythematous, and pruritic, appearing within minutes of injection and resolving within two to four days. While these are not lymph nodes, patients sometimes mistake injection-related bumps for swollen nodes, particularly when injecting near the abdominal region.
Viral infections
Epstein-Barr virus (mononucleosis), cytomegalovirus, HIV, and other viral infections cause widespread lymphadenopathy. These can emerge at any point in life and have nothing to do with medication use. Generalized lymphadenopathy affecting multiple body regions simultaneously should always prompt viral screening.
Autoimmune conditions
Rheumatoid arthritis, systemic lupus erythematosus, Sjogren syndrome, and other autoimmune disorders frequently present with lymphadenopathy. Some of these conditions are associated with obesity and metabolic syndrome, the same conditions that lead people to start semaglutide in the first place. The timing can create a false association.
Recent vaccinations
Vaccines, particularly COVID-19 vaccines and flu shots, commonly cause axillary (armpit) lymphadenopathy on the side of injection. This can persist for weeks, sometimes months. If you received any vaccination recently, that is a likely explanation for armpit lymph node swelling.
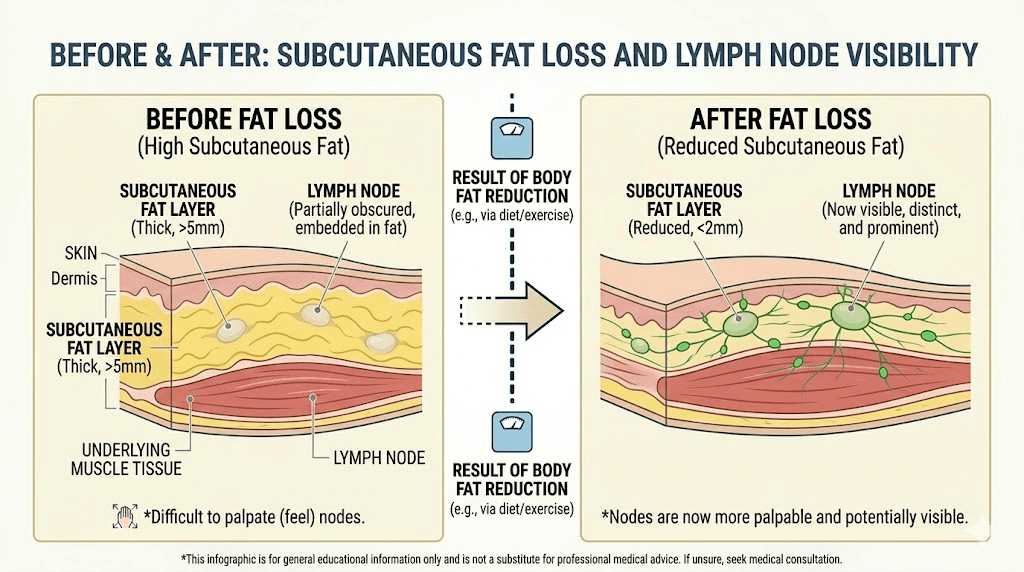
Weight loss itself
This one surprises people. Rapid weight loss, which semaglutide certainly produces, can make previously unnoticeable lymph nodes suddenly palpable. You did not grow new lymph nodes. You lost the subcutaneous fat that was hiding them. Many patients discover lymph nodes they have had for years simply because they can now feel structures beneath thinner skin. This is extremely common and completely benign.
How GLP-1 receptor agonists interact with your immune system
While semaglutide does not cause lymphadenopathy, the relationship between GLP-1 receptor agonists and the immune system is genuinely fascinating. And understanding it helps explain why your lymph nodes are probably fine.
GLP-1 receptors are expressed throughout the body, not just in the pancreas. Research published in Frontiers in Immunology demonstrated that GLP-1 receptors exist on multiple immune cell types, including macrophages, T lymphocytes, natural killer T cells, and intestinal intraepithelial lymphocytes. The expression levels vary significantly by tissue, with lymphoid organs like the spleen, bone marrow, and lymph nodes showing relatively low GLP-1 receptor expression compared to gut-associated immune cells.
What does semaglutide actually do to immune cells? Several things, almost all of them anti-inflammatory.
GLP-1 receptor agonists promote macrophage polarization toward the M2 phenotype. M2 macrophages are anti-inflammatory. They resolve inflammation rather than amplify it. This shift occurs through the PKA/STAT3 signaling pathway and has been documented with multiple GLP-1 receptor agonists including liraglutide and exenatide.
GLP-1 receptor activation also increases regulatory T cell frequency and function. Regulatory T cells are the peacekeepers of the immune system. They suppress excessive immune responses and maintain tolerance. More Tregs with enhanced function means less inflammation, not more.
Research in the Journal of Clinical Investigation showed that GLP-1 based therapies suppress NF-kB signaling, one of the master inflammatory pathways in the body. They reduce pro-inflammatory cytokine production including IL-1 beta, TNF-alpha, and IL-6. They inhibit chemokine-related migration of CD4+ T lymphocytes.
In knockout mouse models where GLP-1 receptors were deleted, researchers observed enhanced infiltration of neutrophils and CD4+ T cells into tissues, along with increased proinflammatory cytokine gene expression in the spleen and lymph nodes. Removing GLP-1 receptor signaling made inflammation worse, not better.
The net effect? Semaglutide is immunomodulatory in a direction that should reduce, not cause, lymph node swelling. If anything, the anti-inflammatory properties of GLP-1 receptor agonists might dampen the lymph node response to minor infections and inflammatory triggers.
A remarkable study published in Frontiers in Pharmacology examined 3,830 breast cancer patients who underwent axillary lymph node dissection. Patients taking GLP-1 receptor agonists were 86% less likely to develop lymphedema compared to non-users. The odds ratio was 0.14 with a p-value less than 0.0001. This protective effect persisted even after controlling for BMI, diabetes status, and other confounders. The researchers attributed the benefit to the combined effects of weight loss, anti-inflammatory action, and potential direct improvement of lymphatic function.
So the science does not support semaglutide causing lymph node problems. It suggests the opposite, that GLP-1 receptor agonists may actually support lymphatic health.
When to see your doctor immediately
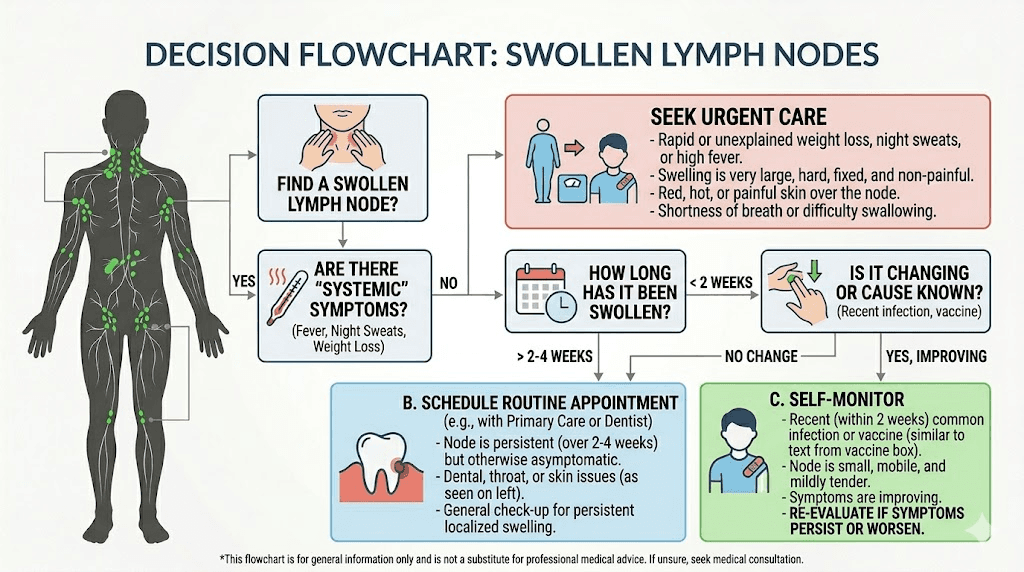
Not all swollen lymph nodes are equal. Some need same-day evaluation. Others can wait for a routine appointment. Here is how to tell the difference.
Seek immediate medical attention if you experience
A lump or swelling in the front of your neck combined with hoarseness, difficulty swallowing, or shortness of breath. These symptoms together warrant urgent thyroid evaluation given the FDA boxed warning on semaglutide products. Do not wait.
Rapidly enlarging lymph nodes anywhere in the body that grow noticeably over days rather than weeks.
Swollen lymph nodes accompanied by high fever, drenching night sweats, or unexplained weight loss beyond what your semaglutide-related weight management explains. This triad, fever, night sweats, unexplained weight loss, is known as B symptoms and warrants prompt hematologic evaluation.
Difficulty breathing or swallowing, regardless of lymph node status. These are emergency symptoms.
Signs of severe allergic reaction including facial swelling, throat tightness, widespread rash, or dizziness and lightheadedness.
See your doctor within a week or two if
Lymph nodes persist beyond three weeks without obvious cause. Most reactive lymphadenopathy from infections resolves within this timeframe.
Nodes feel hard, rubbery, or fixed in place rather than soft and mobile.
Nodes are painless. Counterintuitively, painful lymph nodes are usually less concerning than painless ones. Pain typically indicates an active infection, which is the immune system doing its job. Painless, firm, fixed nodes are more concerning for malignancy.
Nodes appear in the supraclavicular region, just above the collarbones. Supraclavicular lymphadenopathy has a higher association with malignancy than other locations and always warrants investigation. The UK National Institute for Health and Care Excellence recommends an urgent two-week referral pathway for supraclavicular lymphadenopathy.
Nodes are present in multiple unrelated body regions simultaneously, such as neck and groin and armpits, without obvious infectious cause.
Probably nothing to worry about if
The node is small (under 1 cm), soft, mobile, and appeared during or shortly after an obvious infection like a cold or sore throat.
You recently lost significant weight on semaglutide and are now feeling structures you could not feel before.
You received a vaccination in the past few weeks and the swelling is on the same side as the injection.
The node appeared near an area of minor skin irritation, an insect bite, or a healing wound.
What your doctor will do
Knowing what to expect from a medical evaluation reduces anxiety. Here is the typical workup for lymphadenopathy in a patient taking semaglutide.
Physical examination
Your doctor will palpate the swollen nodes, assessing size, consistency, mobility, tenderness, and distribution. They will check for hepatosplenomegaly (enlarged liver or spleen) and examine your thyroid gland. Given your semaglutide use, a careful thyroid and neck examination should be part of every evaluation.
Blood work
A complete blood count with differential can reveal infection, leukemia, or other hematologic abnormalities. Inflammatory markers like C-reactive protein and erythrocyte sedimentation rate help gauge systemic inflammation. Thyroid function tests, including TSH, free T4, and calcitonin (the specific marker for medullary thyroid carcinoma) are particularly relevant for semaglutide users. Liver function tests, viral panels for EBV and CMV, and autoimmune markers may be ordered based on the clinical picture.
Imaging
If physical exam or blood work raises concern, imaging follows. Ultrasound is the first-line imaging study for superficial lymph nodes and is excellent for evaluating thyroid nodules simultaneously. CT scans provide broader assessment of deep lymph node chains. PET scans are reserved for staging known or highly suspected malignancy.
Biopsy
If imaging or clinical features suggest malignancy, a biopsy may be recommended. Fine-needle aspiration is minimally invasive and often diagnostic. Excisional biopsy (complete removal of the node) provides the most definitive diagnosis when needed.
For most semaglutide patients with incidental lymphadenopathy, the workup stops at physical exam and basic blood work. The vast majority of cases have a benign explanation identified quickly.
Should you stop taking semaglutide if you have swollen lymph nodes?
No. Not without medical guidance.
This deserves emphasis because the instinct to stop medication when something feels wrong is powerful. But since semaglutide does not cause lymphadenopathy, stopping it will not resolve the swelling. And abruptly discontinuing semaglutide carries its own consequences, including rebound hunger, potential weight regain, and loss of glycemic control in patients with type 2 diabetes.
UK clinical guidance from the National Health Service specifically states that patients should not discontinue GLP-1 treatment automatically upon discovering swollen lymph nodes. Instead, healthcare providers should evaluate the lymphadenopathy while the patient continues treatment unless there is a specific reason to stop.
The only scenario where stopping semaglutide might be appropriate is if your doctor suspects medullary thyroid carcinoma, in which case discontinuation would be one part of a much larger treatment plan. Or if you are experiencing a severe allergic reaction, which would present with far more than just swollen nodes.
If you are concerned enough to consider stopping, you are concerned enough to see your doctor. Let them make the call based on clinical assessment rather than making changes to your dosing protocol based on anxiety alone.
The weight loss connection most people miss
This section is important because it explains a phenomenon that generates enormous unnecessary worry.
When you lose 15, 20, 30 or more pounds on semaglutide, your body composition changes dramatically. Subcutaneous fat, the layer of fat directly beneath your skin, shrinks. Structures that were previously buried under this fat layer become palpable for the first time.
Lymph nodes are one of those structures.
A lymph node that has been sitting quietly in your neck or armpit for decades, completely normal, completely healthy, suddenly becomes something you can feel with your fingertips. It might feel like a small pea or bean. It moves when you push it. It is not tender. And it terrifies you.
This happens frequently during rapid weight loss. Doctors who treat patients on semaglutide and tirzepatide report fielding these calls regularly. The patient feels a lump, assumes the worst, and comes in panicked. The exam reveals a perfectly normal lymph node that simply became detectable due to fat loss.
How do you distinguish a newly noticeable normal node from a pathologically enlarged one?
Normal lymph nodes that become palpable with weight loss are typically small (under 1 cm), oval-shaped, soft, mobile, non-tender, and located in areas where lymph nodes are normally concentrated (neck, armpits, groin). If this describes what you are feeling, it is very likely nothing more than your body becoming more lean. You can monitor these nodes and mention them at your next regular appointment rather than scheduling an urgent visit.
For SeekPeptides members tracking their body composition changes on GLP-1 protocols, this is one of those facts worth knowing before it happens. Understanding that weight loss reveals previously hidden anatomy prevents a lot of unnecessary panic.
Semaglutide side effects that are actually documented
While lymphadenopathy is not on the list, semaglutide does have a well-characterized side effect profile. Knowing what is actually linked to the medication helps you calibrate your concern appropriately.
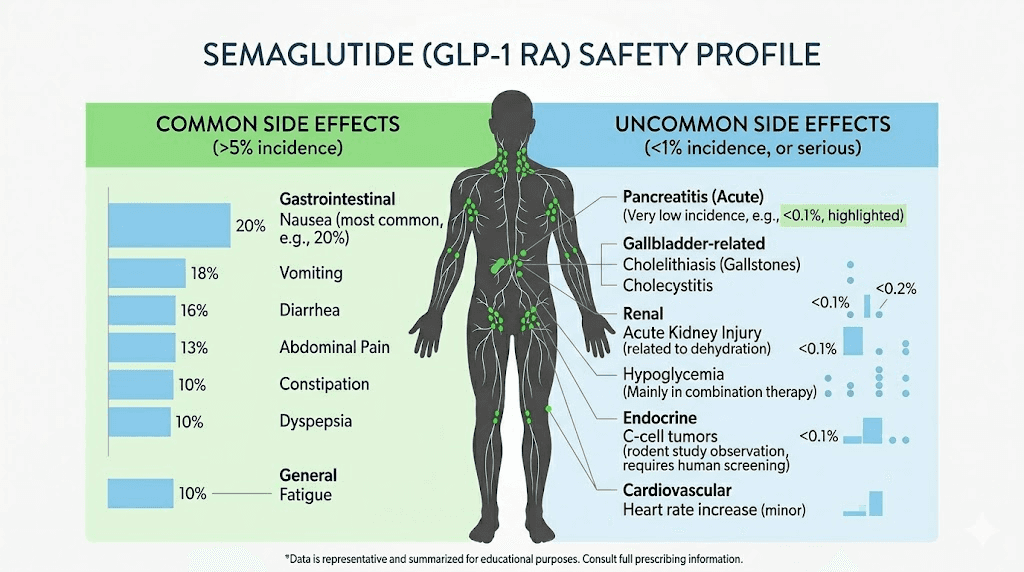
Very common side effects (affecting more than 10% of patients)
Nausea is the most frequently reported side effect, affecting up to 44% of patients in clinical trials. It is typically worst during dose escalation and improves over time. Constipation and diarrhea are common gastrointestinal effects. Vomiting occurs in roughly 24% of patients on the 2.4 mg dose. Abdominal pain and acid reflux round out the gastrointestinal side effects. Fatigue affects a significant proportion of users, particularly early in treatment.
Common side effects (affecting 1-10% of patients)
Dizziness and lightheadedness can occur, particularly with dehydration. Headaches are reported frequently. Sulfur burps and excessive gas bother many patients. Hair thinning, while technically related to rapid weight loss rather than semaglutide directly, is commonly reported. Insomnia and sleep disturbances affect some users.
Serious but uncommon side effects
Pancreatitis is rare but requires immediate medical attention. Symptoms include severe, persistent upper abdominal pain radiating to the back. Gallbladder disease, including gallstones and cholecystitis, occurs at higher rates during rapid weight loss. Kidney problems can develop, particularly from dehydration secondary to gastrointestinal side effects. Rare cardiovascular events have been reported, though the SELECT trial actually showed cardiovascular benefit overall. The thyroid C-cell tumor risk discussed earlier carries the boxed warning.
If you are experiencing side effects from semaglutide, they will almost certainly fall into the gastrointestinal category. Not lymph node swelling.
Lymph nodes by location and what they suggest
Where swollen lymph nodes appear provides diagnostic clues. This reference helps you understand what your doctor is thinking during evaluation.
Cervical (neck) lymph nodes
Swollen nodes along the sides of the neck, under the jaw, or behind the ears most commonly indicate upper respiratory infections, dental problems, or pharyngitis. For semaglutide users specifically, anterior cervical lymphadenopathy (front of the neck) combined with a palpable thyroid nodule warrants thyroid evaluation given the MTC risk. Isolated posterior cervical nodes (back of the neck) are more commonly associated with viral infections like mononucleosis.
Axillary (armpit) lymph nodes
These commonly swell after arm infections, cat scratches, recent vaccinations (especially on the ipsilateral side), breast infections, or skin conditions of the upper extremity. For people injecting semaglutide in the upper arm, mild local inflammation could theoretically trigger nearby axillary node response, though this is not well-documented.
Inguinal (groin) lymph nodes
Groin lymph nodes respond to lower extremity infections, sexually transmitted infections, skin infections on the legs or feet, and urinary tract infections. UTIs can coincide with semaglutide use and might explain inguinal lymphadenopathy. For patients injecting in the abdomen, inguinal node swelling is geographically plausible as a response to injection site inflammation, though again, this link is theoretical.
Supraclavicular (above the collarbones)
These nodes deserve special mention because supraclavicular lymphadenopathy has the highest association with malignancy of any lymph node location. The left supraclavicular node (Virchow node) can indicate abdominal malignancy. The right supraclavicular node may suggest intrathoracic pathology. Any palpable supraclavicular node requires medical evaluation.
Generalized lymphadenopathy (multiple regions)
Involvement of multiple unrelated node groups simultaneously suggests systemic causes: viral infections (HIV, EBV, CMV), autoimmune conditions, certain medications (not semaglutide, but drugs like phenytoin and allopurinol), or lymphoproliferative disorders. Generalized lymphadenopathy always warrants a thorough medical workup.
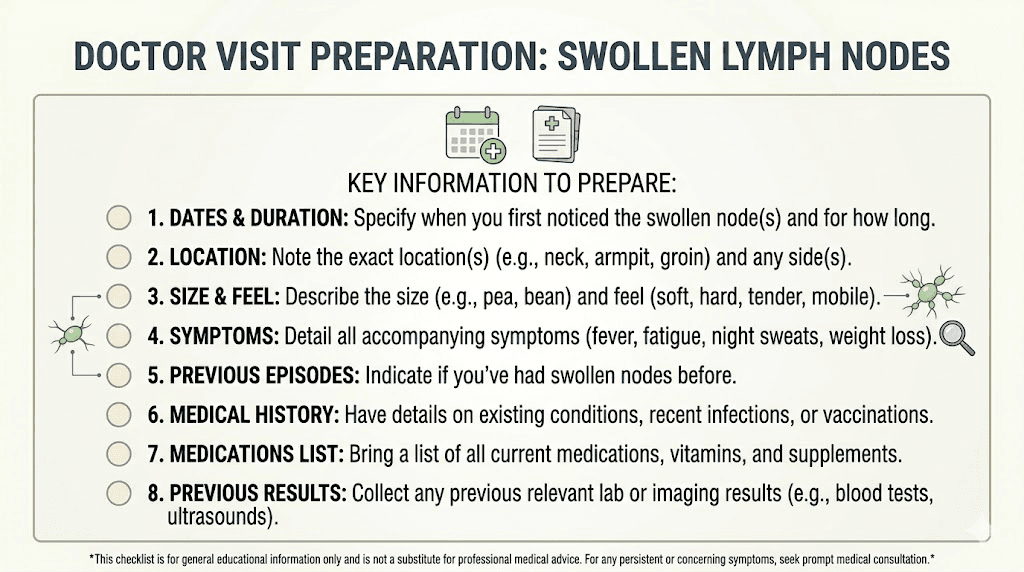
What to tell your doctor
When you visit your doctor about swollen lymph nodes while on semaglutide, providing organized information helps them reach a diagnosis faster. Here is what to communicate.
Tell them exactly which nodes you have noticed and when you first detected them. Describe the size, roughly, using common comparisons: pea, marble, grape. Note whether the nodes are painful or painless, soft or hard, mobile or fixed. Mention any recent infections, dental work, vaccinations, or injuries near the affected area.
Tell them you are taking semaglutide, the dose, and how long you have been on it. Share how much weight you have lost, as this context helps them consider the newly-palpable-normal-node explanation. Mention whether you have noticed any other new symptoms, fever, night sweats, unexplained fatigue, skin changes, or difficulty swallowing.
If you are aware of the thyroid cancer boxed warning on semaglutide and that is driving your concern, say so directly. Your doctor can order calcitonin levels and a thyroid ultrasound to definitively address this worry.
Being specific and organized saves time and reduces the chance of important details being overlooked during a brief appointment.
GLP-1 receptor agonists and lymphatic function: emerging research
An exciting area of emerging research suggests that GLP-1 receptor agonists may actually improve lymphatic function rather than impair it.
The Frontiers in Pharmacology study mentioned earlier found that GLP-1 receptor agonist users were 86% less likely to develop cancer-related lymphedema after axillary lymph node dissection. This dramatic reduction points to direct beneficial effects on the lymphatic system.
The proposed mechanisms include reduced tissue fibrosis through downregulation of NF-kB signaling and decreased TGF-beta1 levels, improved insulin sensitivity (insulin resistance may directly impair lymphatic function), reduced systemic inflammation that would otherwise compromise lymphatic drainage, and weight loss that reduces mechanical compression of lymphatic vessels.
A case report published in the Journal of Cancer Rehabilitation described a breast cancer survivor with established lymphedema who experienced significant improvement after starting a GLP-1 receptor agonist for weight management. While a single case report does not constitute evidence, it aligns with the mechanistic rationale.
Research published in the Journal of Clinical Investigation detailed the broad anti-inflammatory actions of GLP-1 based therapies, noting effects that extend well beyond metabolic benefits. The anti-inflammatory cascade, M2 macrophage polarization, regulatory T cell enhancement, and cytokine suppression, all theoretically support improved lymphatic function.
This research is preliminary. No one should take semaglutide specifically for lymphatic health. But it provides additional reassurance that GLP-1 receptor agonists are lymphatic-friendly compounds, not lymphatic-harmful ones.
For those researching benefits beyond weight loss from GLP-1 receptor agonists, immune modulation and potential lymphatic support represent genuinely promising areas of investigation. SeekPeptides tracks this evolving research and provides members with updates as new findings emerge.
Other medications that actually do cause lymphadenopathy
For context, here are medications with documented lymphadenopathy as a known side effect. Semaglutide is not among them, but this list helps illustrate what drug-induced lymphadenopathy actually looks like.
Phenytoin (Dilantin), an anti-seizure medication, is perhaps the most well-known drug cause of lymphadenopathy. It can cause a syndrome called pseudolymphoma that mimics lymphoma. Allopurinol, used for gout, can trigger a severe hypersensitivity reaction that includes widespread lymphadenopathy, fever, and rash. Carbamazepine, another anti-epileptic, causes lymphadenopathy through similar hypersensitivity mechanisms. Certain antibiotics, including cephalosporins and sulfonamides, can cause serum sickness-like reactions with lymph node swelling. Some antihypertensives, particularly hydralazine, can induce a lupus-like syndrome with lymphadenopathy.
If you take any of these medications alongside semaglutide, they are far more likely culprits for lymph node swelling than your GLP-1 receptor agonist.
Managing anxiety about symptoms while on semaglutide
Starting a new medication heightens body awareness. Every twinge becomes meaningful. Every bump becomes suspicious. This is normal human behavior amplified by the fact that semaglutide has received extraordinary media coverage, much of it focused on potential risks.
The phenomenon even has a name. Nocebo effect. The expectation of side effects can create symptoms or amplify the perception of normal bodily sensations. When you read about semaglutide side effects online, your brain starts looking for them. And a brain looking for problems in the body tends to find them.
This does not mean your lymph nodes are imaginary. They are real. They are swollen, or they are normal and newly palpable. Either way, the sensation is real. But the connection to semaglutide is almost certainly not.
Practical strategies for managing medication-related health anxiety include setting a specific monitoring period. If you notice a swollen lymph node, give it three weeks before escalating. Mark the date. If it persists or grows after three weeks, schedule an appointment. This prevents both ignoring real problems and catastrophizing normal findings.
Keep a simple symptom journal. Note what you find, where, when, and any concurrent events (recent cold, vaccination, dental work). Patterns become clear quickly. Limit your medical Googling. One thorough search is helpful. Repeated searching at midnight creates a spiral. Use evidence-based resources like SeekPeptides, MedlinePlus, or your prescriber for information rather than anonymous forums.
Discuss your concerns with your doctor proactively. Many prescribers provide anticipatory guidance about what symptoms to watch for and what to ignore. Ask for this guidance at your next visit.
The compounded semaglutide consideration
Patients using compounded semaglutide face an additional variable. Compounded formulations may contain different excipients, preservatives, or additives than brand-name Ozempic or Wegovy. Some compounded versions include vitamin B12, glycine, niacinamide, L-carnitine, or other compounds.
While allergic reactions to these additional ingredients are uncommon, they are possible. An allergic response to any injected substance can cause regional lymphadenopathy near the injection site. If you are using compounded semaglutide and notice lymph node swelling near your injection area, mention the specific formulation and its ingredients to your doctor. They may want to consider a trial of brand-name semaglutide to determine whether an excipient in the compound is causing a localized immune response.
This does not change the fundamental conclusion, semaglutide itself does not cause lymphadenopathy, but it adds a variable worth investigating if you are not using a standard FDA-approved formulation.
For guidance on proper reconstitution and handling of semaglutide products, which can affect injection site reactions, see our detailed reconstitution guides.
Comparing lymphadenopathy risk across GLP-1 receptor agonists
If you are concerned about lymph node swelling and considering switching to a different GLP-1 receptor agonist, here is what you should know.
No GLP-1 receptor agonist, whether semaglutide, tirzepatide, liraglutide, exenatide, or dulaglutide, lists lymphadenopathy as a known side effect. The mechanism of action for this entire drug class involves GLP-1 receptor activation, and as we discussed, this activation tends to be anti-inflammatory and immune-modulatory in a lymphatic-friendly direction.
Switching medications to avoid a side effect that does not exist would expose you to the genuine risks of dose transitions and the uncertainty of a new drug without any lymph node benefit. If you are having concerning lymph node symptoms, the answer is medical evaluation, not medication switching.
That said, different GLP-1 receptor agonists do have different injection site reaction profiles. If your lymph node concern is localized near an injection site, and injection site reactions are an issue, switching formulations might be reasonable for that reason. The case report of semaglutide injection-site nodules resolved completely when the patient switched to dulaglutide. But the nodules were injection reactions, not lymphadenopathy.
For a comprehensive comparison of side effect profiles between semaglutide and tirzepatide, see our detailed analysis.
Frequently asked questions
Can semaglutide cause swollen lymph nodes directly?
No. Swollen lymph nodes are not listed as a side effect of semaglutide in any regulatory documentation or clinical trial data. The STEP trials, SUSTAIN trials, and SELECT trial, collectively involving tens of thousands of patients, did not identify lymphadenopathy as a treatment-emergent adverse event. If you have swollen lymph nodes while taking semaglutide, the cause is almost certainly unrelated to the medication.
Should I stop semaglutide if I notice swollen lymph nodes?
No, do not stop semaglutide without medical guidance. Since the medication does not cause lymphadenopathy, stopping it will not resolve the swelling. Instead, see your doctor to identify the actual cause while continuing treatment. The only exception would be if your doctor specifically advises discontinuation based on their clinical assessment.
Can weight loss from semaglutide make lymph nodes more noticeable?
Yes, this is very common. Significant weight loss reduces subcutaneous fat, which can make previously hidden lymph nodes suddenly palpable. These nodes were always there and are completely normal. They are typically small, soft, mobile, and painless. This is a cosmetic finding, not a medical concern.
Does the thyroid cancer warning on semaglutide relate to swollen lymph nodes?
Indirectly, yes. The FDA boxed warning concerns medullary thyroid carcinoma, which can present with neck swelling, a thyroid lump, hoarseness, and cervical lymphadenopathy. While the actual risk in humans appears very low based on current data, any neck swelling combined with these symptoms in a semaglutide user warrants prompt thyroid evaluation including calcitonin levels and ultrasound.
How long should I wait before seeing a doctor about swollen lymph nodes?
For nodes that are soft, mobile, and appeared during an obvious infection, give them three weeks. Most reactive lymphadenopathy resolves in this timeframe. Seek immediate evaluation for hard, fixed, rapidly growing nodes, or nodes accompanied by fever, night sweats, unexplained weight loss, hoarseness, or difficulty swallowing. Supraclavicular nodes at any size warrant prompt evaluation.
Do GLP-1 receptor agonists affect the immune system?
Yes, but in an anti-inflammatory direction. Research shows GLP-1 receptor agonists promote anti-inflammatory macrophage phenotypes, increase regulatory T cell function, suppress NF-kB inflammatory signaling, and reduce pro-inflammatory cytokine production. A study of 3,830 breast cancer patients found GLP-1 receptor agonist users were 86% less likely to develop lymphedema after lymph node surgery, suggesting these medications actually support lymphatic health.
Can injection site reactions from semaglutide be confused with swollen lymph nodes?
Yes. Injection site nodules, while rare with semaglutide, can feel like lumps near the injection area. One case report described hard, erythematous, pruritic nodules appearing within minutes of injection that resolved within two to four days. These are localized inflammatory responses at the injection site, not lymph node enlargement, but patients may confuse the two.
Are compounded semaglutide formulations more likely to cause lymph node swelling?
There is no evidence for this, but compounded formulations may contain additional ingredients that could theoretically cause localized immune responses in sensitive individuals. If you use compounded semaglutide with added ingredients like B12, glycine, or niacinamide, and notice lymph node swelling near your injection site, mention the specific formulation to your doctor.
External resources
GLP-1 Receptor Agonist as a Modulator of Innate Immunity (Frontiers in Immunology)
GLP-1 RAs and Lymphedema Risk Reduction (Frontiers in Pharmacology)
Thyroid Carcinogenic Risk Assessment of Semaglutide (Systematic Review)
For researchers navigating the complexities of GLP-1 receptor agonist protocols, unexpected symptoms can be isolating. SeekPeptides provides evidence-based guidance, comprehensive safety information, and a community of experienced researchers who have encountered these exact concerns. Members access detailed side effect management guides, interaction databases, and protocols built on real-world data from thousands of documented research experiences.
In case I do not see you, good afternoon, good evening, and good night. May your lymph nodes stay quiet, your protocols stay effective, and your health concerns stay answered.