Feb 2, 2026

Why bone loss accelerates faster than most people realize
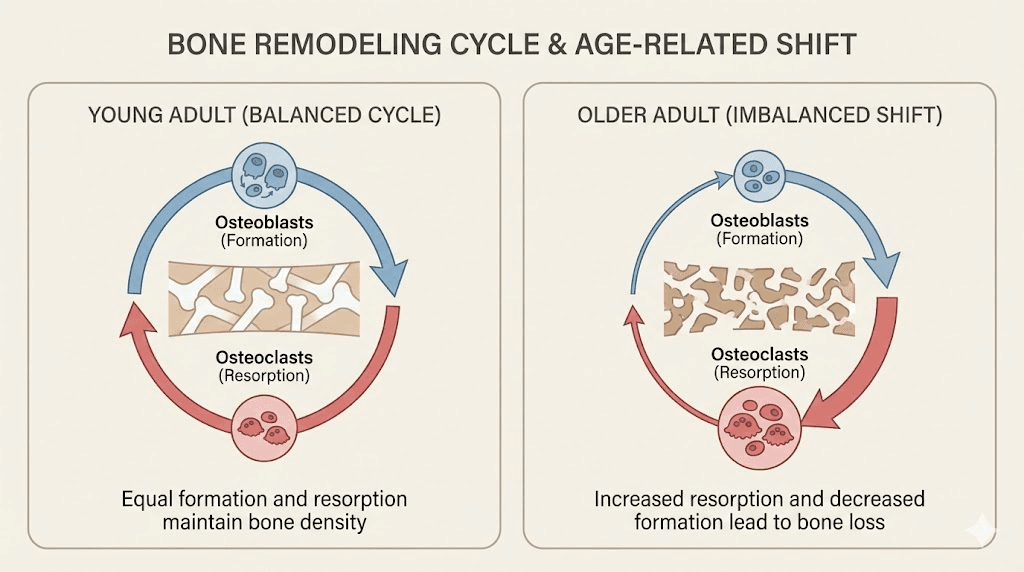
Your skeleton is not static. It is a living organ, constantly breaking down old bone and building new tissue in a process called remodeling. Every ten years, your body essentially replaces its entire skeleton. But here is the problem.
After age 30, the balance shifts. Bone resorption begins outpacing bone formation. Slowly at first. Then faster.
By the time a DEXA scan reveals osteopenia or osteoporosis, years of silent bone loss have already occurred. The World Health Organization estimates that osteoporosis affects over 200 million people worldwide, and osteoporotic fractures happen every three seconds. Hip fractures alone carry a 20% mortality rate within the first year. These are not abstract statistics. They represent real consequences of a skeletal system that has been quietly deteriorating for decades.
Standard treatments focus primarily on slowing bone breakdown. Bisphosphonates, denosumab, and calcium supplementation all target the resorption side of the equation. But what about actually building new bone? What about stimulating the osteoblasts, the cells responsible for bone formation, to work harder and faster? This is where peptide research has opened genuinely exciting possibilities.
Several peptides have demonstrated the ability to influence bone metabolism through multiple pathways, from direct osteoblast stimulation to inflammatory pathway modulation and tissue repair acceleration. Some are already FDA-approved medications. Others remain in the preclinical research phase with promising animal data. And a few, like collagen peptides, have solid randomized controlled trial evidence in humans showing measurable improvements in bone mineral density.
This guide covers every peptide with meaningful research connections to bone health, osteoporosis prevention, and skeletal regeneration. Not vague claims. Specific mechanisms, study data, dosage protocols from research, and practical considerations that SeekPeptides members use to make informed decisions about their bone health strategies.
Understanding bone metabolism and where peptides fit in
Before examining specific peptides, understanding bone metabolism provides critical context for how these compounds actually work. Bone remodeling involves two cell types in constant communication. Osteoblasts build new bone. Osteoclasts break down old bone. In healthy adults, these processes remain balanced.
The signaling system controlling this balance is remarkably complex.
The RANK/RANKL/OPG pathway serves as the primary regulatory mechanism. RANKL (receptor activator of nuclear factor kappa-B ligand) stimulates osteoclast formation and activity. OPG (osteoprotegerin) acts as a decoy receptor, binding RANKL and preventing it from activating osteoclasts. When RANKL dominates, bone resorption increases. When OPG dominates, bone formation gets the upper hand.
Estrogen plays a major protective role. It suppresses RANKL production while boosting OPG levels. This is precisely why postmenopausal women face dramatically accelerated bone loss. The sudden drop in estrogen tips the RANKL/OPG ratio decisively toward resorption. Within the first five to seven years after menopause, women can lose up to 20% of their bone density.
Peptides influence this system at multiple points. Some directly stimulate osteoblast activity. Others inhibit osteoclast formation. A few do both simultaneously. And certain peptides enhance the production of type I collagen, the protein that forms approximately 90% of bone organic matrix and provides the scaffold for mineral deposition. Understanding these mechanisms helps explain why different peptides may benefit different aspects of bone health, and why combining approaches might prove more effective than any single intervention.
The mechanisms through which peptides operate are diverse. Some bind directly to cell surface receptors on osteoblasts. Others modulate inflammatory pathways that indirectly affect bone turnover. A few work through growth factor stimulation, triggering cascades that ultimately result in increased bone formation. Each mechanism offers distinct advantages and limitations, which is why researchers are increasingly interested in peptide stacking strategies that target multiple pathways simultaneously.
Teriparatide: the gold standard peptide for osteoporosis
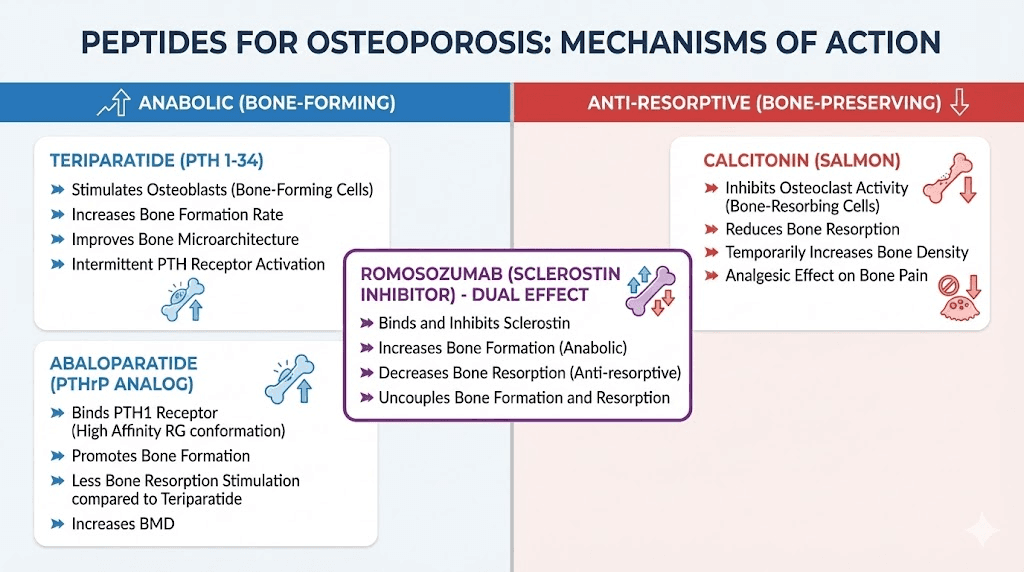
Teriparatide deserves first mention because it is the most well-established peptide therapy for osteoporosis, with FDA approval since 2002 and extensive clinical trial data. Sold under the brand name Forteo, teriparatide consists of the first 34 amino acids of parathyroid hormone (PTH). It represents the first approved anabolic therapy for osteoporosis, meaning it actually builds new bone rather than simply slowing bone loss.
The mechanism is fascinating. Continuous exposure to PTH causes bone loss, which is exactly what happens in hyperparathyroidism. But intermittent, pulsed exposure to low-dose PTH does the opposite. It preferentially stimulates osteoblast activity over osteoclast activity. This is called the anabolic window, and teriparatide exploits it through once-daily subcutaneous injections that create brief, controlled spikes of PTH activity.
At the molecular level, teriparatide binds to PTH type 1 receptors on osteoblasts and osteocytes. This activates PKA and PKC-dependent signaling pathways. It upregulates transcription of pro-osteoblastogenic growth factors including insulin-like growth factor 1 (IGF-1) and fibroblast growth factor 2 (FGF-2). The result is increased bone formation on both trabecular and cortical bone surfaces.
Clinical efficacy data
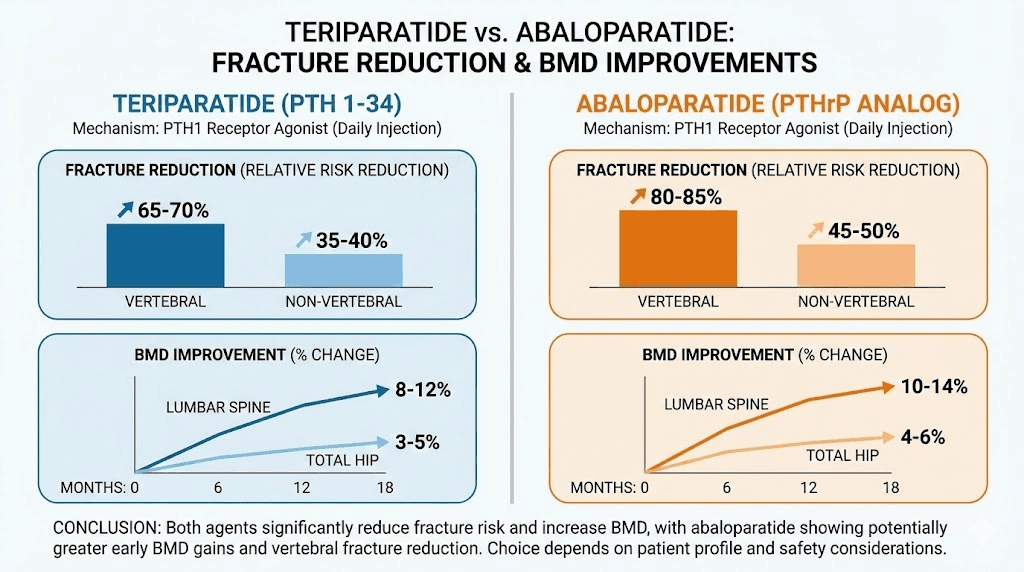
The numbers are compelling. In the pivotal Fracture Prevention Trial, teriparatide at 20 mcg daily reduced vertebral fracture risk by 65% and nonvertebral fracture risk by 35% over approximately 20 months. Lumbar spine bone mineral density increased by roughly 8% after one year. In patients with glucocorticoid-induced osteoporosis, which is notoriously difficult to treat, teriparatide produced a 7.2% increase in lumbar spine BMD, 3.6% at the total hip, and 3.7% at the femoral neck.
These results exceed what most antiresorptive medications achieve.
Dosage and administration
The standard dose is 20 mcg injected subcutaneously once daily. Peak serum concentrations occur about 30 minutes after injection and decline to undetectable levels within three hours. Treatment duration is limited to two years, both because of regulatory guidelines related to an osteosarcoma signal in rat studies (which has not been observed in humans, and the original black box warning has been removed) and because efficacy tends to plateau.
A critical consideration: bone loss can be rapid after discontinuing teriparatide. Follow-up therapy with an antiresorptive agent like a bisphosphonate or denosumab is typically recommended to consolidate gains. This sequential approach, using teriparatide first to build bone and then switching to an antiresorptive to maintain it, has become the preferred treatment strategy for severe osteoporosis.
For those researching peptide dosing protocols, teriparatide offers a clear example of how administration timing fundamentally changes a peptide biological effect. The difference between anabolic and catabolic PTH activity comes down entirely to pulsed versus continuous exposure, a principle that applies to several other peptide compounds as well. SeekPeptides members can access detailed protocol guides that explain these timing principles across various peptide categories.
Abaloparatide: the next-generation PTH analog
Abaloparatide (brand name Tymlos) represents an evolution of the teriparatide concept. Rather than being a fragment of PTH itself, abaloparatide is a synthetic analog of PTHrP (parathyroid hormone-related protein), specifically the 1-34 amino acid region. This distinction matters because PTHrP activates the same receptor but with a different binding profile that may offer clinical advantages.
The key difference lies in receptor selectivity. Abaloparatide preferentially binds to the RG conformation of the PTH1 receptor, which is associated with transient signaling. This produces a strong anabolic bone-building response while causing less bone resorption and less hypercalcemia compared to teriparatide. In simple terms, abaloparatide may offer a more favorable ratio of bone building to bone breakdown.
The ACTIVE trial results
In the landmark ACTIVE trial, abaloparatide achieved remarkable outcomes. An 86% reduction in risk of new vertebral fractures. A 43% decrease in risk of nonvertebral fractures. These numbers were achieved in postmenopausal women with osteoporosis over an 18-month treatment period. The vertebral fracture risk reduction was numerically superior to teriparatide in a head-to-head comparison arm of the same trial, though the study was not specifically powered for that comparison.
Bone mineral density increases were also substantial. Lumbar spine BMD increased by approximately 11% over 18 months. Total hip BMD increased by about 4%. These gains were rapid, with significant improvements detectable as early as six months.
Practical considerations
Abaloparatide is administered as an 80 mcg subcutaneous injection once daily. Like teriparatide, treatment duration is limited to two years. The same principle of sequential therapy applies: follow-up with an antiresorptive agent is essential to maintain bone density gains. Side effects are similar to teriparatide but with reportedly lower rates of hypercalcemia and nausea.
For researchers comparing peptide treatment options, the teriparatide versus abaloparatide decision typically comes down to tolerability, insurance coverage, and individual response patterns. Both represent the most validated peptide-based approaches to actively building bone in osteoporosis.
BPC-157 and bone healing: what the research actually shows
Body protection compound-157 (BPC-157) is a 15-amino-acid peptide sequence derived from human gastric juice that has generated significant interest in the bone healing research community. Unlike teriparatide and abaloparatide, BPC-157 is not an approved medication. It remains a research compound. But the preclinical evidence for its effects on bone is worth understanding in detail.
The landmark study was published in the journal Bone by Sebecic and colleagues in 1999. Researchers created segmental bone defects in rabbits, essentially removing a section of bone to create a gap that would not heal on its own. BPC-157 was administered continuously via percutaneous intramuscular injection directly into the bone defect site.
The results were striking.
Within six weeks, BPC-157-treated rabbits showed complete bony continuity across the defect site. All control animals remained unhealed. After just two weeks, BPC-157-treated animals showed callus formation twice as large as controls. Radiographic assessment, microphotodensitometry, and quantitative histomorphometry all confirmed that BPC-157 effects were comparable to local application of bone marrow or autologous cortical bone graft, which are gold-standard treatments for segmental bone defects.
How BPC-157 promotes bone healing
BPC-157 appears to promote bone healing through several interconnected mechanisms. First, it stimulates angiogenesis within bone tissue. New blood vessel formation is critical for bone healing because osteoblasts need oxygen and nutrient delivery to build new bone matrix. BPC-157 enhances VEGFR2-NO signaling, which promotes vascular tube formation and endothelial cell migration.
Second, BPC-157 activates the ERK1/2 (extracellular signal-regulated kinase) pathway in a dose-dependent manner. This pathway drives cellular proliferation and migration, essential processes for bone defect repair. Third, and perhaps most relevant to osteoporosis specifically, BPC-157 promotes osteogenesis and accelerates bone healing under compromised conditions, including delayed union and avascular osteonecrosis.
A 2025 systematic review published in HSS Journal evaluated 36 studies from 1993 to 2024. The review confirmed that BPC-157 promotes healing by boosting growth factors and reducing inflammation. It has improved outcomes in muscle, tendon, ligament, and bone injury models in animals. However, only one human study was identified, involving 12 people with chronic knee pain, where 7 of 12 experienced relief lasting over six months after a single BPC-157 injection.
Relevance to osteoporosis
The connection between BPC-157 and osteoporosis is indirect but logical. Osteoporotic bone heals more slowly after fractures because the compromised microarchitecture impairs normal repair mechanisms. BPC-157 capacity to accelerate healing under exactly these compromised conditions suggests potential utility for osteoporotic fracture recovery. Additionally, the peptide origin in gastric juice is relevant because gastrectomy (stomach removal) is known to cause osteoporosis, suggesting that gastric peptides may play a natural role in bone metabolism.
The BPC-157 versus TB-500 comparison is relevant here because both peptides have bone healing research, and some researchers explore stacking both compounds for enhanced tissue repair. Whether this translates to meaningful benefits for osteoporosis specifically remains to be determined in clinical trials.
Preclinical safety data has been encouraging. BPC-157 showed no mutagenic or genotoxic effects in Ames tests, chromosomal aberration assays, or micronucleus assays. But it is important to note that no clinical safety data exists, and the safety profile of research peptides in general requires careful consideration. For those researching BPC-157 administration protocols, understanding these limitations is essential.
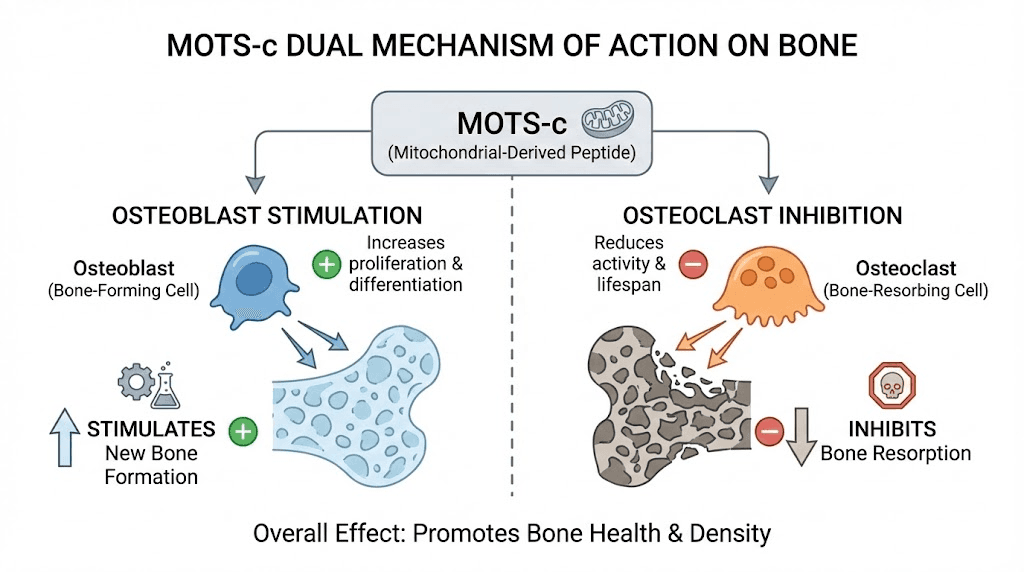
MOTS-c: the mitochondrial peptide with bone-protective effects
MOTS-c (mitochondrial open reading frame of the 12S rRNA type-c) is a 16-amino-acid peptide discovered in 2015. It is encoded by mitochondrial DNA, making it one of only a handful of known mitochondria-derived peptides. What makes MOTS-c particularly interesting for osteoporosis research is that it appears to affect both sides of the bone remodeling equation, promoting bone formation while simultaneously inhibiting bone breakdown.
The decline of MOTS-c with age parallels the decline in bone density. In human plasma, MOTS-c levels decrease significantly as people get older. This correlation has led researchers to investigate whether restoring MOTS-c levels could help counteract age-related bone loss.
Effects on osteoblasts and bone formation
MOTS-c promotes osteoblast proliferation, differentiation, and mineralization through the TGF-beta/Smad signaling pathway.
Specifically, it upregulates TGF-beta1, TGF-beta2, and Smad7 expression. This promotes the synthesis of type I collagen, the primary structural protein in bone matrix. In cell culture studies, MOTS-c treatment remarkably stimulated the formation of calcified nodules in bone marrow stem cells (BMSCs). When researchers knocked down TGF-beta1, the osteogenic effects of MOTS-c were reversed, confirming this pathway as the primary mechanism.
Effects on osteoclasts and bone resorption
On the other side of the equation, MOTS-c inhibits osteoclast differentiation through AMPK-dependent suppression of RANKL signaling. MOTS-c increases phosphorylated AMPK levels, which blocks the osteoclastogenesis cascade. When researchers used compound C (an AMPK inhibitor), the anti-osteoclast effects of MOTS-c were partially abolished, confirming the AMPK pathway as the key mechanism.
MOTS-c also increases the OPG/RANKL ratio in osteoblasts. Since OPG acts as a decoy receptor that prevents RANKL from activating osteoclasts, a higher OPG/RANKL ratio translates to less bone resorption. This dual action, boosting formation while reducing breakdown, makes MOTS-c a particularly attractive candidate for osteoporosis research.
Animal model evidence
In ovariectomized mice (the standard animal model for postmenopausal osteoporosis), MOTS-c injection at 5 mg/kg daily for 12 weeks significantly alleviated bone loss as measured by micro-CT. The treatment prevented the dramatic bone density decline that normally follows estrogen withdrawal in this model. Separate studies showed that MOTS-c injection into areas with implanted UHMWPE (ultra-high molecular weight polyethylene) particles prevented significant bone mass loss and reversed existing bone loss.
The exercise connection
One of the most intriguing aspects of MOTS-c research is its connection to exercise. When healthy young men exercised on a stationary bicycle, skeletal muscle MOTS-c levels increased nearly 12-fold. Plasma levels also rose approximately 50%. This suggests that some of the well-documented bone-protective benefits of exercise may be mediated, at least partially, through MOTS-c release. For those interested in MOTS-c benefits beyond bone health, the peptide also shows effects on metabolic function and energy metabolism.
Researchers interested in MOTS-c should review the side effect profile carefully. While animal studies have been encouraging, human clinical trials have not yet been completed for osteoporosis specifically.
AOD-9604: the growth hormone fragment with bone effects
AOD-9604 is a 16-amino-acid synthetic peptide fragment derived from the C-terminal domain of human growth hormone (amino acids 176-191). It was originally developed in the 1990s by Professor Frank Ng at Monash University as a potential anti-obesity drug. The goal was to isolate the fat-burning effects of growth hormone without its proliferative side effects. But subsequent research revealed that AOD-9604 also influences bone and cartilage metabolism.
AOD-9604 activates both the IGF-1 pathway and direct cellular pathways associated with growth hormone. Since IGF-1 is a critical mediator of bone formation, this mechanism provides a plausible basis for the observed bone effects.
Unlike full-length growth hormone, AOD-9604 is only an 8% fragment of the GH molecule, which means it lacks many of the concerning side effects associated with growth hormone therapy, including diabetogenic effects and organ enlargement.
Bone and cartilage research
Research has shown that AOD-9604 supports repair and regeneration of both cartilage and bone. In a rabbit model of osteoarthritis, researchers compared AOD-9604 alone, hyaluronic acid (HA) alone, and AOD-9604 combined with HA against saline controls. The results were revealing. The saline group showed the worst cartilage degeneration. AOD-9604 alone and HA alone both improved outcomes. But the combination of AOD-9604 plus HA was significantly better than either treatment alone, producing less cartilage damage and shorter duration of lameness.
For osteoporosis specifically, AOD-9604 may have positive effects on bone mineral density. The mechanism appears to involve IGF-1-mediated stimulation of osteoblast activity. However, it is important to note that despite completing six human clinical trials involving over 900 participants for its primary obesity indication, AOD-9604 failed to achieve statistical significance in its largest Phase IIb trial. The safety profile was favorable with minimal adverse effects, but the peptide lacks regulatory approval from any major health authority.
For those researching the complete AOD-9604 profile, understanding both its dosage protocols and side effect considerations is essential before forming conclusions about its role in bone health strategies.
GHK-Cu: copper peptide effects on bone formation
GHK-Cu (glycyl-L-histidyl-L-lysine copper complex) is a naturally occurring tripeptide first isolated from human plasma. While most people know GHK-Cu for its skin regeneration properties, the peptide also has documented effects on bone formation that deserve attention in the osteoporosis discussion.
In human plasma, GHK-Cu levels are approximately 200 ng/ml at age 20 but drop to around 80 ng/ml by age 60. This 60% decline parallels the age-related decline in bone density, collagen production, and tissue repair capacity. While correlation does not prove causation, the timing is suggestive.
Osteoblast stimulation and bone growth
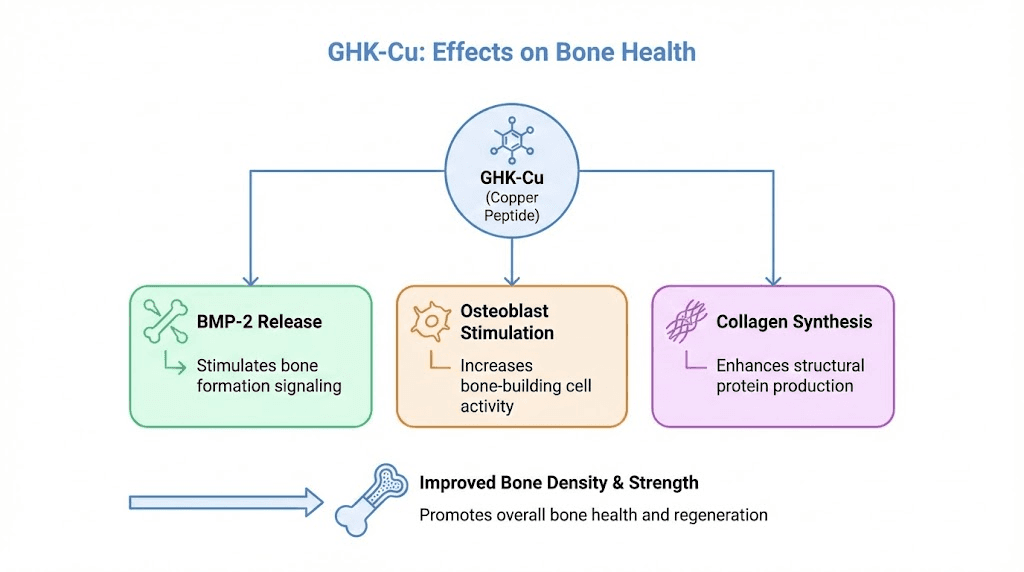
GHK-Cu increases growth of human marrow stromal cells and enhances attachment of osteoblastic cells. These are direct effects on the cell populations responsible for building new bone. At the molecular level, GHK-Cu stimulates release of bone morphogenetic protein 2 (BMP-2), one of the most important signaling molecules in bone formation and osteoblast differentiation.
In rat studies with experimental bone fractures, GHK at 0.5 mcg/kg combined with other peptides (dalargin and thymogen) produced a marked increase in reparative osteogenesis within 10 days. The combination of peptides was more potent than any individual peptide, suggesting synergistic effects on bone healing. This aligns with the broader principle that targeting multiple pathways simultaneously often produces better outcomes than single-pathway approaches.
Collagen and bone matrix support
GHK-Cu promotes collagen synthesis, which is directly relevant to bone health because type I collagen forms the organic scaffold of bone. Without adequate collagen production, mineral deposition lacks its structural framework. The peptide also stimulates VEGF (vascular endothelial growth factor), which promotes blood vessel formation essential for nutrient delivery to bone tissue.
Advanced research using 3D-printed silk-based scaffolds coated with GHK-Cu for controlled release has shown promise for vascularized bone regeneration. The released GHK-Cu promoted bone marrow stem cell proliferation, induced neovascularization, and facilitated macrophage polarization toward the M2 (anti-inflammatory, pro-repair) phenotype. While these are highly specialized research applications, they demonstrate the breadth of GHK-Cu bone-related effects.
For those already using GHK-Cu for skin health and curious about its broader effects, understanding the proper dosing protocols and administration methods is important. The differences between GHK-Cu and other copper peptide forms may also influence which compound is most appropriate for specific research goals.
Collagen peptides: the oral supplement with clinical evidence
Among all the peptides discussed in this guide, collagen peptides have the strongest human clinical trial evidence for directly improving bone mineral density. This is notable because collagen peptides are available as oral supplements, making them the most accessible option on this list. They do not require injections, prescriptions, or complex protocols.
Type I collagen constitutes approximately 90% of the organic matrix of bone. As people age, collagen production decreases by roughly 1% to 1.5% per year. This decline directly affects bone quality because the collagen scaffold provides the framework for mineral deposition. Without adequate collagen, even sufficient calcium and vitamin D cannot maintain optimal bone structure.
The randomized controlled trial evidence
A landmark randomized, placebo-controlled trial enrolled 131 postmenopausal women with age-related BMD decline. Participants received either 5 grams of specific collagen peptides (SCP) or placebo daily for 12 months. The collagen peptide group showed significant increases in bone mineral density at the lumbar spine and femoral neck. Blood levels of P1NP (procollagen type I N-terminal propeptide), a marker of bone formation, also increased significantly, while markers of bone degradation decreased.
A follow-up study tracked 31 participants from the original trial for four years of continuous collagen peptide supplementation. The results were even more impressive. Bone mineral density significantly increased over the four-year period. No fractures occurred during the entire study duration. Taking into account the expected BMD loss in postmenopausal women, the improvement in spine and femoral neck BMD was approximately 7% relative to predicted decline, representing a pronounced, clinically relevant effect.
A recent meta-analysis confirmed these findings across multiple studies, concluding that collagen peptide supplementation, especially when combined with calcium and vitamin D, significantly enhances bone mineral density. The effects were greatest at the spine and femoral neck, with moderate to large standardized mean differences across studies.
How collagen peptides improve bone
Bioactive collagen peptides work through several mechanisms. They stimulate osteoblasts to produce essential collagen and other structural proteins. They function as biological signals, promoting collagen synthesis while inhibiting collagen degradation in the extracellular matrix. They also modulate bone remodeling by reducing osteoclast activity, effectively slowing bone breakdown while enhancing bone formation.
In animal studies, ingestion of collagen peptides prevented bone loss and improved bone microarchitecture in chronologically aged mice. The improvements included increased trabecular bone volume, trabecular number, and trabecular thickness, along with decreased trabecular separation. These structural improvements translate to stronger, more fracture-resistant bone.
Practical protocol for collagen peptides
Based on the clinical trial data, the effective dose is 5 grams of specific bioactive collagen peptides daily. Consistency matters more than timing. The trials used daily supplementation without interruption for 12 months minimum, with the four-year follow-up showing continued improvement. For best results, combine with adequate calcium intake (1,000-1,200 mg daily) and vitamin D (600-800 IU daily, or as guided by blood levels).
Collagen peptide supplements are generally well tolerated. They are available as powders, capsules, and liquid formulations. The marine collagen peptide and bovine collagen peptide options both contain type I collagen, which is the relevant form for bone health. For those wondering about collagen peptides in the context of their broader health routine, guides on bone broth versus collagen peptides, whether collagen counts as protein, and collagen and fasting compatibility provide additional context.
Calcitonin: the bone-protective peptide hormone
Calcitonin is a 32-amino-acid peptide hormone naturally secreted by parafollicular cells (C cells) in the thyroid gland. It has been used therapeutically for osteoporosis for decades, though its role has diminished somewhat with the advent of more potent antiresorptive agents. Still, understanding calcitonin provides important context for how peptide hormones regulate bone metabolism.
The primary mechanism is straightforward. Calcitonin binds to calcitonin receptors on osteoclasts, directly inhibiting their bone-resorbing activity. This reduces the rate of bone breakdown. Calcitonin also enhances production of vitamin D-activating enzymes, which improves calcium absorption and promotes bone mineralization. The net effect is increased calcium retention and improved bone density.
Salmon calcitonin (sold as Miacalcin and Fortical) is the most commonly used form because it is approximately 40 to 50 times more potent than human calcitonin. It is available as a nasal spray (200 IU daily) or subcutaneous injection (100 IU daily). The nasal spray form gained popularity for its convenience, though its efficacy is modest compared to bisphosphonates and the newer anabolic agents.
Clinical data shows that salmon calcitonin can reduce vertebral fracture risk and modestly improve lumbar spine BMD. It also provides analgesic effects for acute vertebral fractures, making it useful in the immediate post-fracture period. However, long-term safety concerns about a potential association with malignancy have led to restrictions on prolonged use in some countries.
For researchers exploring the intersection of nasal spray peptide delivery and bone health, calcitonin represents one of the earliest examples of intranasal peptide therapy. Its relatively mild side effect profile and analgesic properties make it a useful option in specific clinical scenarios, even if it is no longer considered first-line therapy for most osteoporosis patients.
CGRP: calcitonin gene-related peptide and bone density
Calcitonin gene-related peptide (CGRP) is derived from the same gene as calcitonin but through alternative splicing. It is a 37-amino-acid neuropeptide found throughout the nervous system, including in sensory nerve fibers that innervate bone tissue. While CGRP is most known clinically as a target for migraine treatment (anti-CGRP antibodies are major migraine drugs), its role in bone metabolism is increasingly recognized.
CGRP stimulates the proliferation and differentiation of osteoprogenitor cells while reducing their apoptosis. In practical terms, it helps create more bone-building cells and keeps them alive longer. CGRP levels increase in patients with fractures, suggesting it plays an important role during the inflammatory phase of bone healing.
Transgenic mice engineered to overexpress CGRP showed high trabecular bone density and bone volume, associated with increased bone formation rate. This genetic evidence strongly supports a direct role for CGRP in maintaining bone density. Conversely, CGRP knockout mice show reduced bone mass.
The clinical implications are complex. Anti-CGRP therapies for migraine could theoretically impair bone health, though this has not been clearly demonstrated in clinical trials. On the positive side, understanding CGRP role in bone metabolism opens possibilities for targeted approaches that could selectively enhance its bone-protective effects without triggering unwanted vascular effects.
For those interested in how peptide research connects different physiological systems, CGRP illustrates a fascinating principle. A single peptide can have profoundly different effects in different tissues, which is why understanding peptide formulation and targeting is so critical for therapeutic applications.
PEPITEM: the emerging peptide therapy for bone loss
PEPITEM (Peptide Inhibitor of Trans-Endothelial Migration) represents one of the newest and most exciting developments in peptide-based bone therapy. First identified in 2015 by University of Birmingham researchers, PEPITEM is a naturally occurring peptide whose role in bone remodeling has only recently been recognized.
The latest research from teams at the University of Birmingham and University of Oxford, funded by the Medical Research Council, demonstrated that PEPITEM regulates bone remodeling in ways that could have major therapeutic implications. Increasing PEPITEM levels in young, healthy bones stimulated bone mineralization and produced increases in bone strength and density comparable to current standard-of-care drugs.
Perhaps more importantly for osteoporosis patients, researchers showed that administering additional PEPITEM in animal models of menopause-induced bone loss limited the bone density decline and improved overall bone density. This directly addresses the most common trigger for osteoporosis in humans.
The potential advantage of PEPITEM over existing therapies is its safety profile. Current anabolic agents like teriparatide are limited to two years of use. Romosozumab (an anti-sclerostin antibody that promotes bone formation) has been associated with cardiovascular events. PEPITEM, as a naturally occurring peptide, could potentially offer a longer treatment window with fewer safety concerns, though clinical trials in humans are needed to confirm this.
This is early-stage research, and PEPITEM is not yet available for clinical use. But for those following the latest peptide developments, PEPITEM is worth watching closely. It represents a fundamentally different approach to bone loss, one that works with the body natural regulatory mechanisms rather than introducing an exogenous signal.
Growth hormone releasing peptides and bone health
Growth hormone (GH) is a major regulator of bone metabolism. It directly stimulates osteoblast activity and enhances production of insulin-like growth factor-1 (IGF-1), which mediates many of GH bone-building effects. GH secretion declines with age, which is one reason why bone density decreases in older adults. This decline has led researchers to investigate whether growth hormone releasing peptides (GHRPs) could indirectly support bone health by restoring more youthful GH levels.
Several GHRPs have been studied in the context of bone metabolism. CJC-1295, a growth hormone releasing hormone (GHRH) analog, stimulates pulsatile GH release that mimics natural secretion patterns. Ipamorelin, a selective growth hormone secretagogue, increases GH without significantly raising cortisol or prolactin. The sermorelin-ipamorelin combination has gained attention for its synergistic effects on GH release.
The rationale for using GHRPs in bone health is indirect but scientifically grounded. By increasing endogenous GH production, these peptides boost IGF-1 levels, which then stimulates osteoblast proliferation and differentiation. IGF-1 also promotes calcium absorption in the gut and phosphate reabsorption in the kidneys, both of which support bone mineralization.
However, the evidence for GHRPs specifically improving bone density in osteoporosis is limited. Most studies focus on GH replacement therapy rather than GHRP-mediated GH stimulation. The theoretical framework is sound, and GHRPs like CJC-1295 do produce meaningful increases in GH and IGF-1, but direct bone density outcomes from GHRP use have not been well-established in clinical trials.
For those exploring sermorelin or hexarelin for other purposes, the potential bone health benefits represent a secondary consideration rather than a primary indication. The SeekPeptides peptide calculator can help determine appropriate dosing based on individual parameters.
The 11R-VIVIT peptide: targeting the NFAT pathway
The 11R-VIVIT peptide is lesser known but deserves mention for its specific mechanism relevant to osteoporosis. This peptide inhibits the calcineurin/NFAT (nuclear factor of activated T cells) signaling pathway, which plays a crucial role in osteoclast differentiation.
The NFAT pathway is activated during osteoclastogenesis. When RANKL binds to RANK on osteoclast precursors, it triggers a signaling cascade that ultimately activates NFATc1, a transcription factor essential for osteoclast formation and function. By blocking this pathway, 11R-VIVIT prevents the formation of mature, bone-resorbing osteoclasts.
Animal studies have demonstrated that 11R-VIVIT can reduce bone loss in osteoporosis models. The specificity of its mechanism is both an advantage and a limitation. On one hand, targeting NFAT provides a clean, well-defined approach to reducing bone resorption. On the other hand, NFAT signaling is involved in immune function and other physiological processes, raising questions about potential off-target effects.
This peptide remains firmly in the research phase. No human trials have been conducted for osteoporosis. But its inclusion in the literature alongside BPC-157, AOD-9604, and MOTS-c reflects the growing interest in peptide-based approaches to bone health that go beyond the established PTH analogs.
TB-500 and bone repair
Thymosin beta-4 (TB-500) is a 43-amino-acid peptide involved in cell migration, blood vessel formation, and tissue repair. While most TB-500 research focuses on soft tissue healing, some evidence suggests effects on bone repair as well.
TB-500 promotes angiogenesis and reduces inflammation, both of which are critical for bone healing. Adequate blood supply is essential for delivering osteoblast precursors, nutrients, and oxygen to fracture sites. Inflammation, while necessary in the early phases of bone healing, becomes counterproductive if it persists. TB-500 ability to modulate both processes makes it a theoretical candidate for supporting bone repair.
The peptide has been recognized alongside BPC-157 and AOD-9604 as one of the key peptides with potential benefits for bone and joint health. Administration methods include subcutaneous injection, and the compound is being studied in clinical trials for various tissue repair applications.
For osteoporosis specifically, TB-500 evidence is limited compared to the other peptides discussed in this guide. Its primary value may be in accelerating fracture healing rather than preventing bone loss. Those interested in TB-500 protocols should note that the TB-500 dosage calculator can help determine appropriate research amounts.
Comparing peptide approaches for bone health
With so many peptide options, understanding how they compare helps clarify which approaches have the strongest evidence and which mechanisms they target.
Peptide | Evidence level | Primary mechanism | Administration | Regulatory status | Best for |
|---|---|---|---|---|---|
Teriparatide | Strong (RCTs) | Osteoblast stimulation via PTH1R | SC injection 20 mcg/day | FDA approved | Severe osteoporosis |
Abaloparatide | Strong (RCTs) | Osteoblast stimulation via PTH1R | SC injection 80 mcg/day | FDA approved | Postmenopausal osteoporosis |
Collagen peptides | Moderate (RCTs) | Osteoblast stimulation + matrix support | Oral 5 g/day | Supplement | BMD maintenance/improvement |
Calcitonin | Moderate (RCTs) | Osteoclast inhibition | Nasal spray or SC injection | FDA approved | Acute vertebral fractures |
BPC-157 | Preclinical | Angiogenesis + osteogenesis | SC injection | Research only | Fracture healing research |
MOTS-c | Preclinical | Dual: osteoblast promotion + osteoclast inhibition | SC injection | Research only | Age-related bone loss research |
AOD-9604 | Preclinical | IGF-1 pathway activation | SC injection | Research only | Cartilage/bone repair research |
GHK-Cu | Preclinical | BMP-2 release + collagen synthesis | SC injection or topical | Research only | Bone formation research |
PEPITEM | Preclinical | Bone remodeling regulation | Injection | Research only | Early intervention research |
The evidence hierarchy is clear. Teriparatide and abaloparatide sit at the top with robust clinical trial data and regulatory approval. Collagen peptides occupy a middle ground, with good RCT evidence but as a supplement rather than a pharmaceutical. The remaining peptides show promise in preclinical research but lack the human data needed to make definitive recommendations.
For those navigating these options, SeekPeptides provides comprehensive protocol guides and evidence-based comparisons that help researchers understand the strengths and limitations of each approach. The complete peptide database includes detailed information on mechanisms, dosing, and research status for hundreds of peptides.
Practical considerations for bone health peptide protocols
Understanding the research is one thing. Applying it practically is another. Several factors affect how peptides perform in the context of bone health, and overlooking these can mean the difference between meaningful results and wasted effort.
The importance of baseline assessment
Before starting any bone health protocol, a baseline DEXA scan provides essential data. DEXA measures bone mineral density at the lumbar spine and hip, producing T-scores that classify bone health as normal (T-score above -1.0), osteopenic (T-score between -1.0 and -2.5), or osteoporotic (T-score below -2.5). Without baseline data, there is no way to objectively measure whether any intervention is working.
Blood markers add additional information. P1NP (a formation marker), CTX (a resorption marker), vitamin D levels, calcium, and PTH all provide context about the current state of bone metabolism. These can be repeated at intervals to track biochemical changes before structural changes become visible on DEXA, which typically takes 12-24 months.
Foundational nutrition cannot be skipped
No peptide will compensate for inadequate calcium, vitamin D, protein, or other essential nutrients. The clinical trial on collagen peptides specifically combined supplementation with adequate calcium and vitamin D. Teriparatide and abaloparatide prescribing information recommends concurrent calcium and vitamin D supplementation.
Key nutritional targets for bone health include calcium (1,000-1,200 mg daily from food and supplements combined), vitamin D (aim for blood levels of 30-50 ng/ml, often requiring 1,000-4,000 IU daily depending on baseline), protein (at least 1.0 g/kg body weight daily, with higher intakes supporting bone health in older adults), magnesium, vitamin K2, and boron. These are not optional additions. They form the foundation upon which any peptide intervention operates.
Exercise as a peptide amplifier
Weight-bearing exercise and resistance training are the most well-proven non-pharmacological interventions for bone density. They also create the mechanical stimulus that drives bone remodeling. Importantly, as the MOTS-c research demonstrated, exercise itself triggers peptide release that supports bone health.
Combining exercise with peptide protocols creates a synergistic effect. Exercise provides the mechanical signal that tells bones they need to be stronger. Peptides provide the biological tools (growth factors, collagen building blocks, osteoblast stimulators) to execute that remodeling more effectively. Neither is maximally effective alone.
Monitoring and adjusting
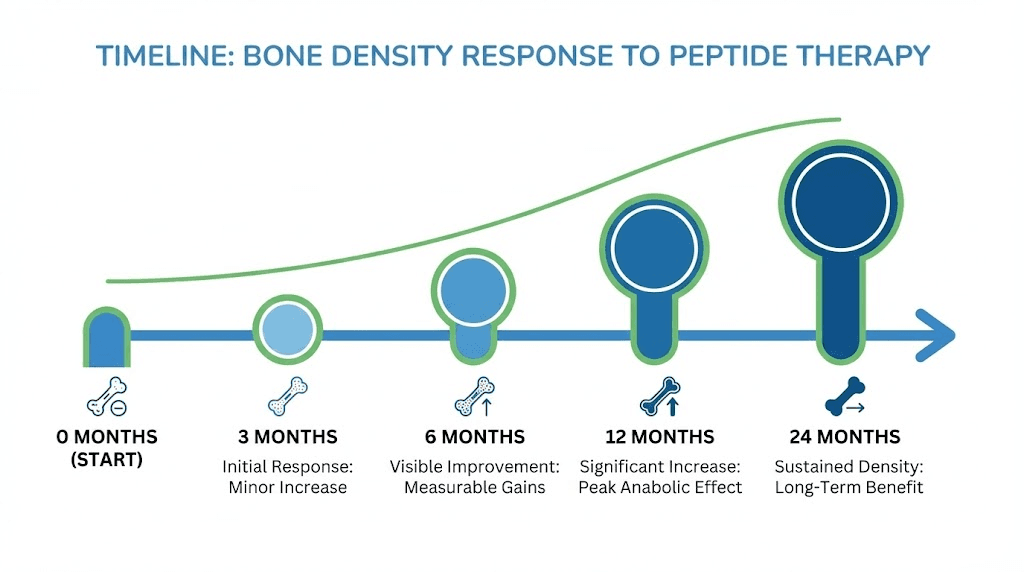
Bone responds slowly. Changes in bone mineral density typically require 6-12 months to become detectable on DEXA scans. Blood markers can show changes sooner, within 3-6 months, providing early signals about whether a protocol is moving bone metabolism in the right direction. For those using before-and-after tracking methods, patience and consistent protocol adherence are essential.
Researchers should track not just bone-specific markers but also overall health indicators. Proper peptide storage and correct reconstitution techniques are fundamental to getting reliable results. Using degraded or improperly prepared peptides will produce unreliable outcomes regardless of the protocol design. The peptide reconstitution calculator helps ensure accurate preparation every time.
Risk factors and who benefits most from peptide approaches
Osteoporosis is not a uniform condition. Understanding specific risk factors helps determine which peptide approaches might be most relevant for different populations.
Postmenopausal women
The largest at-risk group. Estrogen withdrawal triggers rapid bone loss through increased RANKL and decreased OPG. Teriparatide and abaloparatide have their strongest evidence in this population. Collagen peptides also showed their most dramatic results in postmenopausal women. MOTS-c animal studies specifically modeled menopause-induced bone loss. For women navigating the broader challenges of menopause and peptide options, understanding the bone health dimension adds an important layer to the decision-making process. Younger postmenopausal women may also benefit from exploring perimenopause-specific peptide approaches.
Men with low testosterone
Male osteoporosis is underdiagnosed and undertreated. Testosterone plays a protective role in bone metabolism similar to estrogen. Men with hypogonadal osteoporosis are specifically indicated for teriparatide treatment. Those researching peptides for testosterone support should understand that maintaining adequate testosterone levels is independently important for bone health. The testosterone-peptide connection extends beyond muscle and libido to include critical skeletal effects.
Glucocorticoid-induced osteoporosis
Chronic steroid use devastates bone. Prednisone and similar medications suppress osteoblast function, increase osteoclast activity, and reduce calcium absorption. Teriparatide is specifically approved for this indication and shows strong efficacy, with 7.2% BMD improvement at the lumbar spine. Patients on long-term steroids should discuss bone-protective strategies with their physicians.
Age-related bone loss in both sexes
Even without hormonal triggers, aging reduces bone density. Growth hormone decline, decreased physical activity, reduced nutrient absorption, and declining collagen production all contribute. Collagen peptide supplementation addresses the collagen component directly. GHRPs address the growth hormone component indirectly. And longevity-focused peptide strategies increasingly incorporate bone health as a key consideration. Women over 40 and those approaching their senior years face compounding risk factors that make early intervention particularly valuable.
Athletes and active individuals with stress fractures
High-impact activities can paradoxically lead to stress fractures, especially in female athletes with relative energy deficiency (RED-S). BPC-157 and TB-500 research on fracture healing is most relevant to this population. For athletes exploring injury recovery peptides, understanding the bone-specific evidence helps distinguish between compounds that primarily heal soft tissue and those with documented effects on bone.
Combining peptides with conventional osteoporosis treatment
An important consideration is how research peptides relate to conventional osteoporosis medications. This is not an either/or proposition for most people. Sequential and combination approaches often produce better outcomes than single-agent therapy.
The established treatment paradigm now favors starting with anabolic therapy (teriparatide or abaloparatide) and then switching to an antiresorptive (bisphosphonate or denosumab) to maintain gains. This "build then maintain" approach leverages the strengths of each medication class.
Collagen peptides can be added to virtually any treatment regimen as a supplement. There are no known interactions with bisphosphonates, denosumab, teriparatide, or abaloparatide. The collagen peptide studies explicitly noted that supplementation should complement, not replace, standard treatments.
Research peptides like BPC-157, MOTS-c, and AOD-9604 exist in a different category. They are not approved medications and should not be substituted for proven treatments. Some researchers explore them as adjunctive or complementary approaches, but this requires careful consideration and ideally medical supervision. The regulatory landscape around peptide prescribing varies by jurisdiction and continues to evolve.
Weight-bearing exercise, adequate nutrition, fall prevention strategies, and regular monitoring remain the cornerstones of any bone health program. Peptides, whether approved medications or research compounds, work best when layered on top of these fundamentals rather than as replacements for them.
The future of peptide therapy for osteoporosis
The pipeline of peptide-based bone therapies continues to expand. PEPITEM represents a new class of naturally occurring peptides that may offer safer, longer-duration treatment options. Researchers are exploring novel PTH analogs with improved anabolic-to-catabolic ratios. Combination peptide therapies targeting multiple bone metabolism pathways simultaneously are under investigation.
Bone tissue engineering incorporating peptides like GHK-Cu into biocompatible scaffolds offers possibilities for treating severe bone defects that currently require surgical grafting. 3D-printed scaffolds with controlled peptide release represent the cutting edge of regenerative medicine for skeletal applications.
The exercise-MOTS-c connection opens an entirely new avenue of research. If specific exercise protocols can optimize mitochondrial peptide release for bone health, this could lead to precision exercise prescriptions tailored to individual bone metabolism profiles.
For researchers and patients alike, staying informed about these developments is essential. SeekPeptides members receive regular updates on emerging peptide research, including bone-specific developments, protocol updates, and new safety data as it becomes available. The platform comprehensive educational resources help members navigate the growing complexity of peptide science with confidence.
Safety considerations specific to bone health peptides
Each category of bone health peptide carries distinct safety considerations that researchers must understand.
FDA-approved peptides (teriparatide, abaloparatide, calcitonin)
These have the most well-characterized safety profiles. Teriparatide common side effects include nausea, headache, dizziness, and leg cramps. The theoretical osteosarcoma risk from rat studies has not materialized in human use. Abaloparatide has a similar profile with potentially less hypercalcemia. Calcitonin (salmon) is well tolerated but has raised concerns about long-term malignancy risk in some analyses. All three require medical supervision and prescriptions.
Collagen peptides
The safest option on this list. Collagen peptides are generally recognized as safe (GRAS) food ingredients. Side effects in clinical trials were minimal and comparable to placebo. They can be taken long-term without the safety concerns associated with pharmaceutical agents. However, individuals with fish or shellfish allergies should exercise caution with marine collagen sources.
Research peptides (BPC-157, MOTS-c, AOD-9604, GHK-Cu, TB-500)
These carry the most uncertainty. While preclinical safety data is generally encouraging (BPC-157 showed no genotoxicity, AOD-9604 was well tolerated in 900+ trial participants), clinical safety data specific to bone applications is lacking. Manufacturing quality is a significant concern with unregulated sources. Third-party testing and proper vial assessment are essential considerations for anyone working with research peptides. Vendor quality directly impacts both safety and efficacy of any research protocol.
Regardless of which approach is being considered, working with knowledgeable healthcare providers who understand both conventional osteoporosis treatment and peptide research is strongly recommended. The peptide therapy landscape is complex, and finding qualified practitioners can make a significant difference in safety and outcomes.
Frequently asked questions
What is the best peptide for osteoporosis?
Teriparatide (Forteo) has the strongest clinical evidence for treating osteoporosis, with a 65% reduction in vertebral fracture risk and significant BMD improvements. For those seeking a supplement approach, collagen peptides at 5 grams daily have shown meaningful BMD improvements in randomized controlled trials. The "best" choice depends on severity, as severe osteoporosis typically requires injectable peptide therapy under medical supervision.
Can collagen peptides reverse osteoporosis?
Clinical trials show that 5 grams of specific collagen peptides daily can significantly increase bone mineral density at the lumbar spine and femoral neck in postmenopausal women. A four-year follow-up study showed continued improvements and no fractures. However, "reversing" osteoporosis is not a realistic claim, as these should be considered complementary to conventional treatment rather than standalone therapy. They work best combined with calcium, vitamin D, and other evidence-based approaches.
Is BPC-157 good for bone healing?
In animal studies, BPC-157 produced complete healing of segmental bone defects within six weeks while controls remained unhealed. It showed results comparable to bone marrow grafts. However, only one human study exists (for knee pain, not bone healing specifically). BPC-157 remains a research compound without regulatory approval. The preclinical data is promising but insufficient for clinical recommendations. More information about BPC-157 research is available for those wanting to explore the full evidence base.
How long does it take for peptide therapy to improve bone density?
Blood markers of bone formation can improve within 3-6 months. Measurable changes in bone mineral density on DEXA scans typically require 12-24 months. Teriparatide shows approximately 8% lumbar spine BMD improvement after one year. Collagen peptides showed significant improvements at 12 months with continued gains at four years. Patience and consistent protocol adherence are essential.
Can I use peptides alongside bisphosphonates for osteoporosis?
Collagen peptides can be safely combined with bisphosphonates. However, teriparatide and abaloparatide are typically used sequentially with bisphosphonates rather than concurrently. The recommended approach is to use anabolic therapy first (to build bone) then switch to antiresorptive therapy (to maintain gains). Always discuss treatment combinations with a healthcare provider familiar with peptide interaction considerations.
Does MOTS-c help with osteoporosis?
In animal models, MOTS-c significantly reduced bone loss in ovariectomized mice (mimicking menopause) through dual mechanisms: promoting osteoblast differentiation and inhibiting osteoclast formation. Exercise naturally increases MOTS-c levels by up to 12-fold in muscle tissue. However, no human clinical trials for osteoporosis have been completed. The research is promising but still preclinical. For the full MOTS-c evidence review, see our comprehensive guide.
Are peptides safe for long-term use in bone health?
FDA-approved peptides have established safety profiles: teriparatide and abaloparatide are limited to two years of use. Collagen peptides have been studied for up to four years with no safety concerns. Research peptides lack long-term human safety data for bone applications. Each category carries different risk levels, which is why understanding the full safety landscape is critical before starting any protocol.
What peptides do for bone that bisphosphonates cannot?
Bisphosphonates only prevent bone loss by inhibiting osteoclasts. Anabolic peptides like teriparatide and abaloparatide actually build new bone by stimulating osteoblasts. This is a fundamental difference. Antiresorptive drugs preserve what you have. Anabolic peptides add to it. For severe osteoporosis where BMD is very low, building new bone is often more important than simply preventing further loss.
External resources
For researchers committed to understanding and optimizing bone health through evidence-based approaches, SeekPeptides offers the most comprehensive resource available. Members access detailed protocols, dosing calculators, safety databases, and a community of experienced researchers who have navigated these exact questions. Whether the goal is fracture prevention, bone density improvement, or understanding the latest peptide science, the platform provides the tools and knowledge to make informed decisions.
In case I do not see you, good afternoon, good evening, and good night. Join SeekPeptides.