Apr 2, 2026

The alarm starts the same way for almost everyone. You step out of the shower, glance down, and notice more hair than usual circling the drain. Maybe it collects on your pillow. Maybe your ponytail feels thinner between your fingers. And because you recently started tirzepatide, you draw the obvious conclusion.
That conclusion is wrong. Or at least, it is incomplete in ways that matter enormously for what you do next.
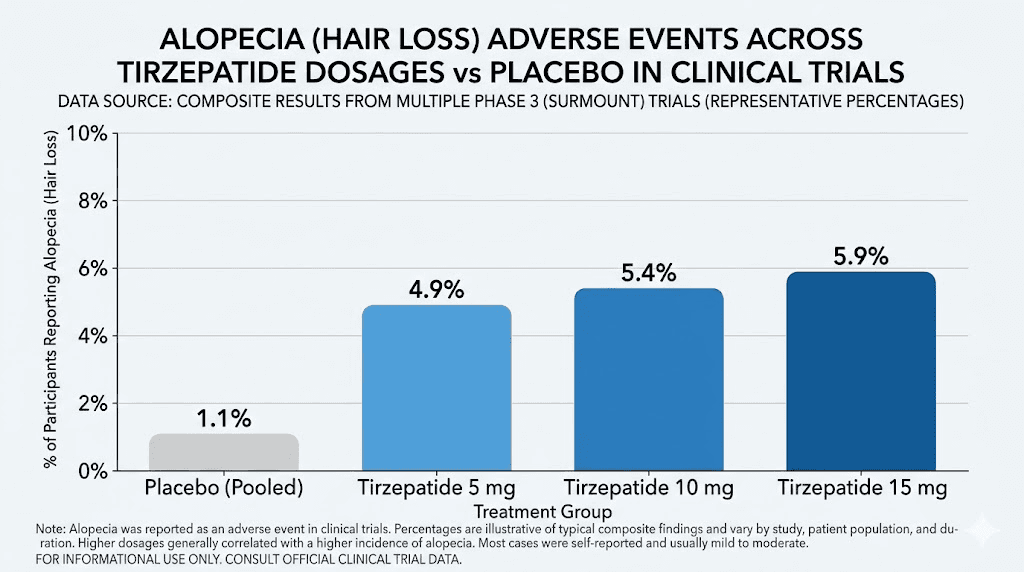
Clinical trial data from the SURMOUNT studies shows that roughly 4% to 5% of people taking tirzepatide report increased hair shedding, compared with just 1% in the placebo group. Those numbers are real. The shedding is real. But the mechanism behind it tells a completely different story than most people assume, and understanding that mechanism is the difference between panicking unnecessarily and taking targeted action that actually works.
Here is what the research shows. Tirzepatide does not attack hair follicles. It does not disrupt the hair growth cycle through any direct pharmacological action. What it does, remarkably well, is cause rapid weight loss. And rapid weight loss, regardless of how it happens, triggers a well-documented condition called telogen effluvium. This is the same temporary shedding that follows crash diets, bariatric surgery, severe illness, or any major metabolic shift. The drug gets blamed. The weight loss is the actual trigger. This guide covers what clinical trials reveal, why it happens, who faces the highest risk, exactly when hair grows back, and the specific steps that prevent or minimize shedding while you continue your tirzepatide weight loss journey.
What clinical trials actually reveal about tirzepatide and hair loss
The most robust data comes from the SURMOUNT clinical trial program, which enrolled thousands of participants across multiple studies evaluating tirzepatide for weight management. In these trials, the medication was marketed under the brand name Zepbound for obesity and Mounjaro for type 2 diabetes. The hair loss findings emerged as a secondary observation, not a primary endpoint, but the numbers paint a clear picture.
Across the SURMOUNT trials, alopecia was reported in approximately 4% to 5% of participants receiving tirzepatide. The placebo group reported hair loss at roughly 1%. That gap, about 3 to 4 percentage points, is statistically meaningful but requires context to interpret properly.
The gender breakdown matters significantly. Women experienced hair shedding at rates up to 7.1%, while men reported it at less than 1%. This disparity is not unique to tirzepatide. It mirrors patterns seen with every weight loss intervention, from semaglutide side effect profiles to bariatric surgery outcomes. Women appear more susceptible to telogen effluvium triggered by rapid metabolic changes, likely due to hormonal interactions between weight loss, estrogen fluctuations, and the hair growth cycle.
A 2025 systematic review published in Cureus analyzed five studies encompassing 2,905 adult patients using GLP-1 receptor agonists. The findings were surprisingly contradictory. Three of the five studies reported significant hair improvement and regrowth following tirzepatide treatment. Two studies reported hair loss as an adverse event. This split reveals something important: the relationship between tirzepatide and hair is not one-directional.
The pharmacovigilance data provides additional granularity. Tirzepatide carries a reporting odds ratio (ROR) of 1.73 for alopecia events, while semaglutide shows a ROR of 1.42. These numbers indicate a slightly elevated signal compared to baseline, but they do not establish direct causation. They indicate association, which is a crucial distinction when you are trying to decide whether to continue or adjust your tirzepatide dosing protocol.
Perhaps the most telling statistic: patients who lost more than 20% of their total body weight experienced alopecia at a rate of 5.3%, while those who lost less than 20% reported it at just 2.5%. The severity of hair loss correlated with the speed and magnitude of weight reduction, not with medication dosage per se. Someone on a microdose tirzepatide protocol losing weight gradually would face substantially lower risk than someone on the maximum dose experiencing rapid, dramatic weight loss.
One more critical detail from the trials: not a single participant discontinued tirzepatide due to hair loss. Zero. The shedding, while distressing, was not severe enough to outweigh the metabolic benefits of continued treatment. This tells us something about severity. We are talking about diffuse thinning and increased shedding, not bald patches or permanent hair loss.
Understanding telogen effluvium and why weight loss triggers it
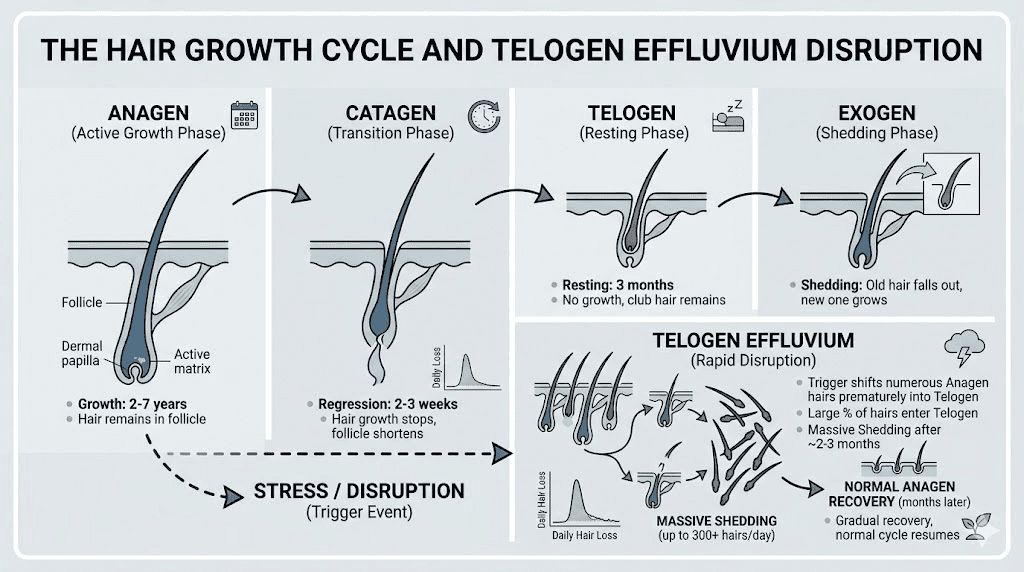
To understand why your hair falls out during tirzepatide treatment, you need to understand the hair growth cycle itself. Every hair on your head cycles through four distinct phases, and the transition between these phases explains everything about medication-related shedding.
The anagen phase is the active growth period. It lasts two to seven years. During this phase, cells in the hair follicle divide rapidly, building the hair shaft from the root upward. At any given time, roughly 85% to 90% of the hair on your scalp is in this growth phase. This is the phase you want to protect.
The catagen phase is a short transitional period lasting about two weeks. The hair follicle shrinks. Blood supply reduces. The hair detaches from its nutritional source but remains physically anchored in the scalp.
The telogen phase is the resting period. It lasts approximately three months. The old hair sits dormant while a new hair begins forming underneath. Under normal conditions, only 10% to 15% of your hair is in this resting phase at any point.
Then comes the exogen phase. The old hair falls out. The new hair pushes through. You lose 50 to 100 hairs daily through this natural cycle. You do not notice it because new growth replaces what sheds.
Telogen effluvium disrupts this balance. When your body experiences a significant physiological stressor, it shifts resources away from non-essential functions. Hair growth, biologically speaking, is non-essential. The body redirects protein, iron, zinc, and energy toward vital organs and metabolic processes. In response, a disproportionate number of follicles prematurely enter the telogen resting phase. Instead of the normal 10% to 15%, telogen effluvium can push 25% to 30% or more of your hair into the resting phase simultaneously.
Three months later, all those resting hairs fall out at once. This is why tirzepatide users typically notice increased shedding around months three to six of treatment, not immediately. The trigger happened months before the shedding became visible. The delay confuses people. They assume the current dose or recent change caused it, when the actual trigger was the rapid weight loss that began weeks or months earlier.
Rapid weight loss is one of the most well-documented triggers of telogen effluvium. It happens after GLP-1 fat loss treatment, after bariatric surgery, after crash diets, after severe caloric restriction of any kind. The mechanism is identical regardless of the method. Your body interprets rapid weight reduction as a physiological emergency and deprioritizes hair growth in favor of survival functions.
This is not a flaw in tirzepatide. This is your body doing exactly what evolution designed it to do when it detects a sudden change in energy balance. Understanding this distinction changes the entire conversation about what to do about it.
People experiencing fatigue on semaglutide or tiredness on tirzepatide are observing the same fundamental process. The body is conserving energy during a period of caloric deficit, and hair growth is one of the first non-essential processes to get deprioritized.
Why tirzepatide itself is not directly damaging your hair follicles
This distinction matters for practical reasons, not just academic ones. If tirzepatide directly damaged hair follicles through its pharmacological mechanism, your options would be limited. You would face a choice between hair and weight loss benefits. But that is not what the evidence shows.
Tirzepatide is a dual GIP/GLP-1 receptor agonist. It activates receptors in the gut, pancreas, and brain to regulate appetite, insulin secretion, and glucose metabolism. These receptor pathways have no known direct effect on hair follicle cycling. The drug does not interfere with keratin production. It does not alter DHT levels through its primary mechanism. It does not reduce blood flow to the scalp.
What tirzepatide does do, and does remarkably well, is reduce appetite and increase satiety. People eat significantly less. Caloric intake drops substantially. The body enters a sustained energy deficit. Weight comes off quickly, particularly in the first several months of treatment when tirzepatide starts working at its most effective.
This rapid energy deficit creates multiple hair-hostile conditions simultaneously.
First, total caloric intake drops. Hair follicles require energy to maintain the rapid cell division of the anagen growth phase. When calories decrease sharply, less energy reaches the follicles.
Second, protein intake often decreases. Many tirzepatide users struggle to eat adequate portions, and protein is frequently the macronutrient that suffers most. Hair is made primarily of keratin, a protein. Without sufficient dietary protein, the raw building blocks for hair production become scarce. This is why guides on what to eat on tirzepatide emphasize protein-first eating strategies.
Third, micronutrient absorption can decrease. Reduced food intake means reduced intake of iron, zinc, vitamin D, biotin, and other nutrients critical to hair health. Some tirzepatide users experience gastrointestinal changes that further impact nutrient absorption.
Fourth, hormonal shifts accompany rapid fat loss. Fat tissue is metabolically active and produces hormones including estrogen. Rapid reduction in fat mass alters hormonal balance, which can influence the hair growth cycle independently of nutritional factors. Women who notice changes in their menstrual cycle on tirzepatide are observing these same hormonal shifts.
The evidence supporting this indirect mechanism is strong. Hair loss rates correlate with magnitude of weight loss, not with medication dose. They correlate with speed of weight loss, not with duration of treatment. And they occur with every weight loss method, not uniquely with tirzepatide.
This means the problem is solvable without stopping medication. You can address the nutritional deficits. You can moderate the speed of weight loss. You can support hair follicles through targeted supplementation. The drug is not the enemy. The caloric deficit and nutritional gaps are the targets.
The surprising case where tirzepatide actually improved hair growth
Not all the research points in one direction. A case report published in JAAD Case Reports in 2024 documented something unexpected: a patient whose hair significantly improved on tirzepatide.
The patient was a 57-year-old male with androgenic alopecia, the most common form of pattern hair loss in men. He also had insulin resistance, with an insulin resistance score of 3.2 (normal is below 2.0), elevated fasting insulin at 13.1 (normal range 5 to 12), and elevated C-peptide at 2.14 (normal 0.8 to 1.8). His BMI was 33.45.
He began tirzepatide at 2.5 mg weekly for three months, increased to 5 mg weekly for six months, and then moved to 7.5 mg weekly. After one year of treatment, he lost 30 pounds. But the hair results were the headline. Significant improvements in hair density were documented at six months and continued through the twelve-month follow-up. Clinical photographs showed visible regrowth in areas of previous thinning.
His metabolic markers normalized. Fasting insulin dropped from 13.1 to 8. C-peptide fell from 2.14 to 1.67. His insulin resistance score improved from 3.2 to 1.7, within normal limits.
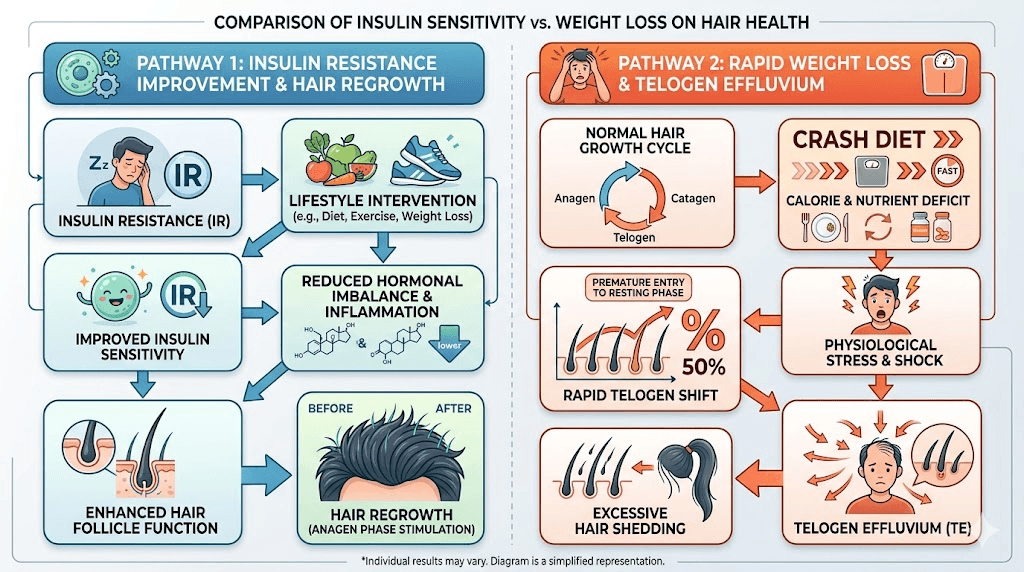
The proposed mechanism is fascinating. Insulin resistance increases the conversion of testosterone to dihydrotestosterone (DHT), the hormone primarily responsible for androgenic hair loss. By resolving insulin resistance, tirzepatide reduced DHT production. Additionally, insulin resistance causes microvascular insufficiency, reducing blood flow to hair follicles. Improved insulin sensitivity restored proper blood supply to the scalp, supporting follicle health and reversing miniaturization.
This single case does not override the clinical trial data showing increased shedding in some users. But it demonstrates that the relationship between tirzepatide and hair is genuinely complex. For people whose hair loss is driven by insulin resistance and metabolic dysfunction, tirzepatide may actually help rather than harm. For people whose hair loss is driven by rapid weight reduction and nutritional deficiency, the approach needs to focus on slowing the pace and filling nutritional gaps.
The systematic review confirmed this duality. Three of five analyzed studies reported hair improvement. Two reported hair loss. The outcome depends heavily on the individual starting point, the mechanism driving their hair loss, and how well their nutrition supports hair growth during treatment. People exploring whether tirzepatide increases metabolism are seeing one piece of this metabolic puzzle. The hair story is another piece of the same metabolic transformation.
Risk factors that increase hair shedding on tirzepatide
Not everyone on tirzepatide experiences hair loss. Understanding the risk factors helps you assess your personal likelihood and take preventive action before shedding begins. The clinical data identifies several clear predictors.
Speed of weight loss
This is the single biggest predictor. People who lose weight rapidly face substantially higher risk than those who lose gradually. The clinical data shows a clear threshold: losing more than 20% of total body weight correlates with a 5.3% alopecia incidence, compared with 2.5% for those losing less than 20%. Losing more than one to two pounds per week consistently also increases risk.
If your tirzepatide weight loss timeline shows dramatic early results, that rapid initial phase is when the telogen effluvium trigger occurs. The shedding will appear two to four months later.
Gender
Women face significantly higher risk. The clinical trial data shows 7.1% of women experienced hair shedding compared with less than 1% of men. Hormonal fluctuations related to fat loss, combined with the effects of changing estrogen levels on the hair cycle, create additional vulnerability. Women who also experience menstrual changes on tirzepatide may be at even higher risk because the hormonal shifts are more pronounced.
Inadequate protein intake
Protein is the raw material for hair production. Hair is approximately 95% keratin, a protein. When tirzepatide suppresses appetite, many users struggle to consume adequate protein. The recommended minimum during active weight loss on GLP-1 medications is 0.8 to 1.2 grams per kilogram of body weight daily, and some experts recommend even higher intake to preserve both muscle and hair.
Guides on tirzepatide diet planning and foods to avoid on tirzepatide can help structure meals that prioritize protein despite reduced overall appetite. The caloric targets for tirzepatide users should account for adequate protein allocation.
Pre-existing nutrient deficiencies
If you entered tirzepatide treatment with low iron, low ferritin, low vitamin D, or low zinc, you face compounded risk. These nutrients are essential for hair follicle function. Weight loss depletes them further. Low ferritin is particularly well-documented as an independent cause of telogen effluvium, and it is common in women of reproductive age even before starting any weight loss medication.
High starting dose or rapid titration
Starting on a higher dose or escalating too quickly can accelerate weight loss beyond what the body can adapt to smoothly. The standard tirzepatide starting dose protocol begins at 2.5 mg weekly for four weeks specifically to allow gradual adaptation. Skipping titration steps or increasing doses ahead of schedule amplifies the metabolic stress that triggers telogen effluvium.
History of telogen effluvium
If you have experienced stress-related hair shedding before, whether from illness, surgery, pregnancy, or a previous diet, your follicles may be more susceptible to future episodes. This does not mean you will definitely experience it again, but it increases the probability and suggests extra precaution.
Concurrent stressors
Telogen effluvium responds to cumulative physiological stress. If you are dealing with sleep disruption from tirzepatide, high emotional stress, illness, or other physical stressors alongside rapid weight loss, the combined burden on your body increases the likelihood and severity of hair shedding. Managing overall stress load, including addressing anxiety that sometimes accompanies tirzepatide, contributes to better outcomes for hair retention.
The complete timeline of hair shedding and regrowth on tirzepatide
Understanding the timeline removes much of the fear. When you know what to expect and when to expect it, the experience shifts from alarming to manageable.
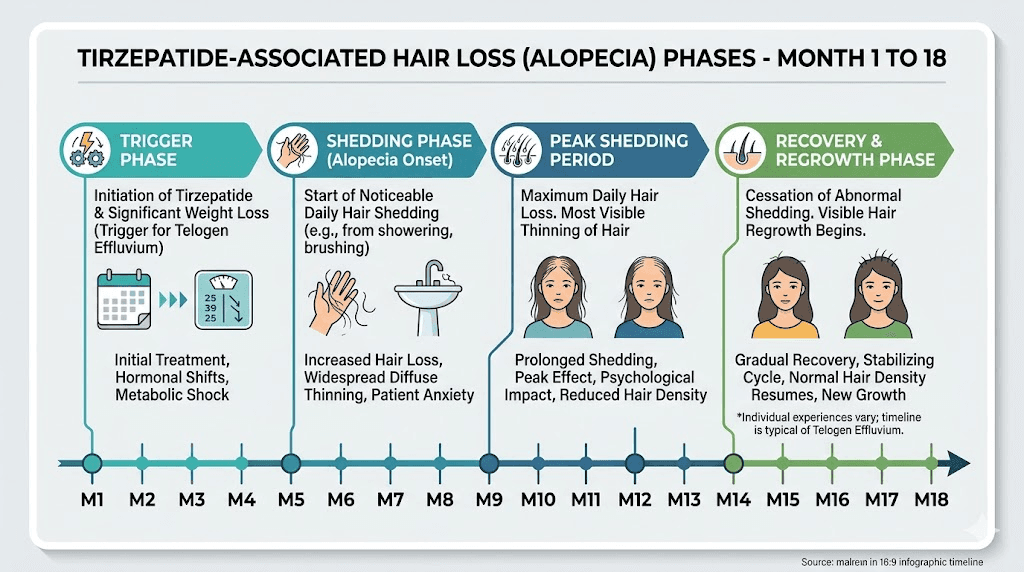
Months 1 to 2: the silent trigger phase
During the first weeks of tirzepatide treatment, the metabolic shift begins. Appetite decreases. Caloric intake drops. Weight starts coming off, sometimes rapidly. You feel the initial effects of your first tirzepatide dose. Your body registers this as a significant change in energy balance.
During this period, your hair looks completely normal. Nothing visible is happening on your scalp. But beneath the surface, follicles are beginning to respond to the metabolic shift. A higher-than-normal percentage of hairs are transitioning from the anagen growth phase into the telogen resting phase.
You will not notice this. Nobody does. The trigger is invisible.
Months 3 to 4: shedding becomes noticeable
This is when most people first notice increased hair loss. The telogen hairs that entered the resting phase two to three months ago begin falling out as new hairs push through underneath. Instead of the normal 50 to 100 hairs per day, you may lose 200 to 300 or more.
The shedding is diffuse. It comes from all over the scalp, not in patches. You notice it in the shower, on your pillow, in your hairbrush, on your clothes. The volume of loose hair is startling and causes many people to assume something is seriously wrong.
This is the phase where people typically search for answers and consider stopping their medication. This is also, ironically, the worst time to make that decision, because the shedding was triggered months ago and stopping the medication now will not stop the current shedding cycle.
Month 5: peak shedding
For most people, hair loss peaks around month five of treatment. The maximum number of follicles that shifted into telogen are now releasing their resting hairs simultaneously. This is typically the most distressing phase.
The hair may visibly thin. Ponytails feel smaller. Parts look wider. The good news: you have already passed the worst point. From here, new growth is actively pushing through, even though the shedding has not fully stopped yet.
Months 6 to 9: transition and regrowth begins
As your body adapts to its new weight and the rate of weight loss slows, the telogen effluvium resolves. Fewer follicles are being pushed into the resting phase. The ones that already shed are cycling back into the anagen growth phase.
You will notice short new hairs growing in, sometimes called "baby hairs" along the hairline and part. These new hairs look wispy and different from the surrounding longer hair, but they are signs of active recovery.
During this phase, continuing to optimize nutrition is critical. The new growth needs adequate protein, iron, and other nutrients to produce strong, healthy hair shafts. People working on maintaining weight loss after tirzepatide should keep nutrition high even as the weight stabilizes.
Months 9 to 18: full recovery
Complete recovery from telogen effluvium typically takes 9 to 18 months from the point where weight stabilizes. Hair grows approximately half an inch per month, so regaining several inches of length takes time even after the follicles are actively growing again.
By 12 months post-stabilization, most people report their hair has returned to its pre-treatment thickness and volume. Some report that their hair is actually healthier than before, potentially due to improved nutrition habits developed during treatment and the metabolic benefits of reduced body weight on overall circulation and hormone balance.
How to prevent hair loss while taking tirzepatide
Prevention is more effective than treatment. If you are starting tirzepatide or are in the early weeks of treatment, these strategies can significantly reduce the risk and severity of hair shedding. If shedding has already begun, these same approaches will support faster recovery.
Prioritize protein at every meal
This is the single most impactful dietary change. Aim for 0.8 to 1.2 grams of protein per kilogram of body weight daily, minimum. Some hair loss specialists recommend 1.2 to 1.5 grams per kilogram during active weight loss on GLP-1 medications.
Protein-first eating is essential. When your appetite is suppressed by tirzepatide, you may only manage small portions. Make every bite count by starting each meal with protein. Lean poultry, fish, eggs, Greek yogurt, cottage cheese, and legumes are excellent sources. Protein shakes can help when solid food feels challenging.
The tirzepatide meal planning guide provides structured approaches to meeting protein targets despite reduced appetite. Understanding which foods to avoid also helps by eliminating items that fill you up without providing adequate nutrition.
Moderate the pace of weight loss
If possible, aim for a steady loss of one to two pounds per week rather than dramatic rapid drops. This may mean working with your provider to titrate doses more slowly or staying at a lower dose longer before increasing.
The standard starting dose protocol begins at 2.5 mg for a reason. Some people benefit from extending each dose level beyond the minimum four weeks before escalating. The microdosing tirzepatide approach is another strategy that can slow the rate of weight loss while still achieving meaningful results over time.
Losing 50 pounds over 12 months is far less stressful on hair follicles than losing 50 pounds over 5 months, even though the end result is identical.
Get baseline blood work before starting
Before your first tirzepatide injection, request a comprehensive metabolic panel that includes ferritin, iron, vitamin D, zinc, and thyroid function. These are the nutrients and hormones most closely linked to hair health. Knowing your baseline allows you to identify and correct deficiencies before they compound with weight-loss-related stress.
Ferritin deserves special attention. It is the storage form of iron and is one of the most common deficiencies linked to telogen effluvium. A ferritin level below 30 ng/mL increases hair loss risk, and many dermatologists recommend levels above 50 to 70 ng/mL for optimal hair health. Standard lab reference ranges often list anything above 12 as "normal," which is misleadingly low for hair purposes.
Eat nutrient-dense foods consistently
Even when appetite is suppressed, focus on nutrient density over volume. Every calorie should carry maximum nutritional value. This means prioritizing whole foods over processed options and choosing meals that pack protein, iron, zinc, and vitamins into small portions.
The GLP-1 breakfast ideas guide and GLP-1 recipes for weight loss provide specific meal suggestions designed for people with reduced appetite. Eggs, leafy greens, fatty fish, nuts, seeds, and lean meats should feature prominently in your rotation.
Stay hydrated
Dehydration stresses the body and can contribute to telogen effluvium independently. Tirzepatide can cause gastrointestinal changes that increase fluid loss. Aim for at least 64 ounces of water daily, more if you are physically active or experiencing digestive side effects like diarrhea.
Manage stress proactively
Psychological stress is an independent telogen effluvium trigger. Combined with the physiological stress of weight loss, it creates a compounding effect. Prioritize sleep quality, particularly if tirzepatide affects your sleep patterns. Exercise regularly but moderately. Practice stress management techniques that work for you.
Do not skip meals
Even when you are not hungry, try to eat structured meals at regular intervals. Going extended periods without eating creates cortisol spikes that further stress the body and hair follicles. Small, protein-rich meals spread throughout the day are better than sporadic eating patterns.
Consider a gentle scalp massage routine
While the evidence is limited, some studies suggest that regular scalp massage increases blood flow to hair follicles and may support growth. Spending five minutes daily gently massaging your scalp with your fingertips is low risk and may provide modest benefit. Do not use harsh brushing or tight hairstyles during the shedding phase, as mechanical stress on already-vulnerable follicles can worsen the situation.
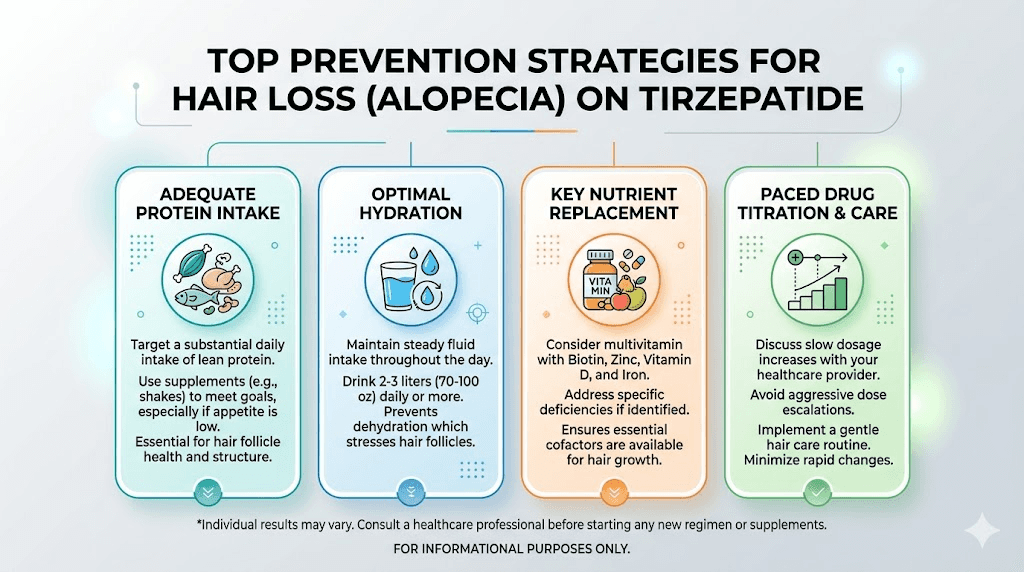
Supplements and nutrients that actually support hair during tirzepatide treatment
The supplement industry makes enormous claims about hair growth products. Most of those claims collapse under scrutiny. Here is what the evidence actually supports, and what is wasted money.
Iron and ferritin: the most important nutrient
Low ferritin is the single most correctable cause of telogen effluvium. Multiple dermatology studies confirm that ferritin levels below 30 ng/mL significantly increase hair shedding risk, and optimal levels for hair health are 50 to 70 ng/mL or higher.
If your blood work shows low ferritin, supplementation can make a meaningful difference. Iron bisglycinate is generally better tolerated than ferrous sulfate and has good absorption. Take iron with vitamin C to enhance absorption, and avoid taking it with calcium, coffee, or tea, which reduce absorption.
Do not supplement iron without testing first. Iron overload is dangerous. This is a supplement that requires blood work before and during use. The supplements to take with tirzepatide guide provides broader context on nutritional support during treatment.
Vitamin D: commonly deficient, genuinely important
Vitamin D receptors are present on hair follicles, and deficiency is associated with telogen effluvium and alopecia areata. Vitamin D deficiency is extremely common, affecting an estimated 40% to 60% of the general population, and weight loss can further deplete stores since vitamin D is stored in fat tissue that is being reduced.
If your levels are below 30 ng/mL, supplementation with 2,000 to 5,000 IU daily (depending on the degree of deficiency) is generally recommended. Retesting after three months helps verify you have reached adequate levels.
Zinc: underrated for hair health
Zinc plays a direct role in hair follicle function and protein synthesis. Deficiency causes telogen effluvium and can also cause hair to become brittle and break easily. Weight loss and reduced food intake make zinc deficiency more likely.
If testing reveals low zinc levels, supplementation with 15 to 30 mg daily can help. Zinc competes with copper for absorption, so prolonged zinc supplementation should include a small amount of copper (1 to 2 mg) to prevent secondary copper deficiency.
Biotin: the overhyped supplement
Biotin is the most marketed hair supplement, and the evidence for it is weak unless you are actually biotin deficient. Multiple dermatology reviews and placebo-controlled trials show no benefit for biotin supplementation in people with normal biotin levels.
True biotin deficiency is rare in people eating a varied diet, even a reduced-calorie one. Additionally, and this is important, biotin supplementation at doses exceeding 5,000 mcg daily can interfere with blood tests, producing false results for thyroid function, cardiac troponin, and other critical lab values. If you do take biotin, stop it at least 48 hours before any blood work.
The bottom line on biotin: test first, supplement only if deficient, and use modest doses. The mega-dose biotin supplements marketed for hair growth are generally not supported by evidence.
Omega-3 fatty acids: supportive evidence
Fish oil and omega-3 supplements have some evidence supporting their role in hair health. A French study found that women supplementing with omega-3 and omega-6 fatty acids showed improved hair density after six months compared with placebo. The anti-inflammatory properties of omega-3s may help reduce inflammation around hair follicles that contributes to shedding.
Fish, walnuts, flaxseeds, and chia seeds are dietary sources. If supplementing, 1,000 to 2,000 mg of combined EPA and DHA daily is a reasonable amount. People interested in tirzepatide and B12 combinations or tirzepatide glycine B12 compounds should note that B12 deficiency itself can contribute to hair issues, making compounded formulations potentially beneficial for multiple reasons.
Collagen peptides: emerging evidence
Collagen peptide supplementation has generated interest for hair support. Collagen provides amino acids (particularly proline and glycine) that serve as building blocks for keratin production. Some preliminary studies suggest that collagen supplementation may support hair thickness, though the research is still early.
Doses of 5 to 15 grams daily of hydrolyzed collagen peptides are commonly used. This also provides additional protein, which helps address the protein gap that many tirzepatide users experience. Those using tirzepatide with glycine formulations are already getting one of the key amino acids found in collagen.
What to skip
Avoid expensive "hair growth" supplements that combine dozens of ingredients at sub-therapeutic doses. They typically contain small amounts of many things rather than meaningful amounts of the nutrients that actually matter. Focus your budget on testing for deficiencies and supplementing specifically what your body needs.
Topical treatments like minoxidil are sometimes suggested for telogen effluvium, but they work through a different mechanism (prolonging anagen phase) and their benefit for telogen effluvium specifically, as opposed to androgenic alopecia, is less established. Discuss with a dermatologist before starting topical treatments.
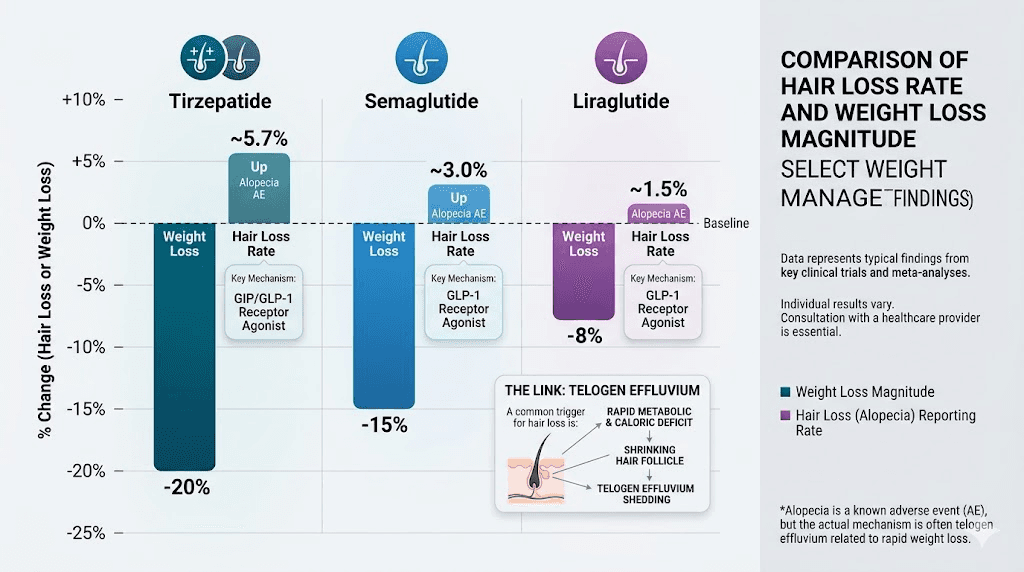
Comparing hair loss rates across GLP-1 medications
If hair loss concerns are influencing your choice of GLP-1 medication, understanding how different options compare is useful. However, the comparison reveals more about weight loss efficacy than about drug-specific hair effects.
The pharmacovigilance data shows slightly different reporting odds ratios for alopecia across GLP-1 receptor agonists:
Tirzepatide: ROR of 1.73 (95% CI: 1.42-2.09)
Semaglutide: ROR of 1.42 (95% CI: 1.3-1.55)
Liraglutide: Lower reporting rates, but also less dramatic weight loss
The pattern is telling. Tirzepatide produces the most dramatic weight loss results of the three, and it has the highest hair loss association. Semaglutide produces slightly less dramatic weight loss, and it has a slightly lower hair loss association. Liraglutide produces the least weight loss, and it has the lowest association.
This dose-response relationship between weight loss magnitude and hair shedding further supports the conclusion that weight loss, not the specific medication, drives the hair loss. Our comprehensive comparison of semaglutide versus tirzepatide side effects explores this relationship in detail across multiple side effect categories.
For people considering switching medications specifically to reduce hair loss risk, the data suggests that switching from tirzepatide to semaglutide might slightly reduce the rate of weight loss and therefore the hair loss trigger. However, the nutritional strategies outlined above are likely more effective than switching medications, because they address the root cause directly.
The three-way comparison between semaglutide, tirzepatide, and retatrutide provides additional context. Retatrutide, a newer triple receptor agonist, produces even more dramatic weight loss than tirzepatide in clinical trials, and hair loss on retatrutide follows the same pattern, correlating with weight loss magnitude rather than drug mechanism. Our broader guide on GLP-1 and hair loss covers this topic across all medication classes.
Some people explore alternatives to tirzepatide for various reasons including side effect profiles. The key insight for hair loss specifically is that any effective weight loss treatment carries similar risk, because the trigger is the weight loss itself, not the tool used to achieve it.
Newer delivery methods like tirzepatide oral drops or orally disintegrating tablets do not change the hair loss equation. The route of administration does not affect the weight loss mechanism that triggers telogen effluvium.
When hair loss on tirzepatide signals something more serious
While telogen effluvium from weight loss is by far the most common cause of hair shedding on tirzepatide, other conditions can cause or worsen hair loss. Knowing when to seek medical evaluation prevents dismissing something that needs attention.
Thyroid dysfunction
Both hypothyroidism and hyperthyroidism cause hair loss. Weight changes can sometimes unmask or worsen underlying thyroid conditions. If your hair loss is accompanied by extreme fatigue beyond what normal tirzepatide fatigue would explain, feeling unusually cold (beyond typical cold sensitivity on tirzepatide), or significant mood changes, request thyroid testing including TSH, free T3, and free T4.
Iron deficiency anemia
Beyond low ferritin, actual iron deficiency anemia causes more severe and persistent hair loss. Symptoms include extreme fatigue, shortness of breath, pale skin, and brittle nails in addition to hair shedding. A complete blood count and iron panel can identify this quickly.
Autoimmune conditions
Alopecia areata, an autoimmune condition, causes patchy hair loss rather than the diffuse thinning of telogen effluvium. If you notice distinct round bald patches rather than general thinning, this is not telogen effluvium and requires dermatological evaluation. People with Hashimoto thyroiditis using GLP-1 medications should be particularly aware of autoimmune-related hair changes.
Androgenic alopecia acceleration
For people with a genetic predisposition to pattern hair loss, the hormonal shifts accompanying weight loss can sometimes accelerate androgenic alopecia. This type of loss follows specific patterns: receding hairline and crown thinning in men, widening part and diffuse thinning in women. Unlike telogen effluvium, androgenic alopecia does not fully self-resolve and may benefit from specific treatments like minoxidil or finasteride.
When to see a doctor
Seek medical evaluation if:
Hair loss persists beyond 9 to 12 months after weight stabilization
You notice patchy bald spots rather than diffuse thinning
Hair loss is accompanied by scalp pain, itching, or redness
You have additional symptoms suggesting thyroid or nutritional issues
The severity is extreme, with visible scalp showing through
Hair loss began before starting tirzepatide or weight loss
A dermatologist can perform a pull test, examine the scalp with dermoscopy, and order targeted blood work to distinguish telogen effluvium from other causes. Early evaluation leads to better outcomes for conditions that require specific treatment.
Practical strategies people use to cope while hair regrows
The emotional impact of hair loss should not be minimized. Even when you understand the science and know it is temporary, watching your hair thin is distressing. Here are practical approaches people use while waiting for regrowth.
Gentle hair care adjustments
Switch to a gentle, sulfate-free shampoo. Avoid heat styling tools as much as possible. Let hair air dry when you can. These changes do not prevent telogen effluvium, but they reduce mechanical breakage that makes thinning look worse than it is.
Loose hairstyles reduce traction on vulnerable follicles. Tight ponytails, braids, and buns pull on hair that is already in a fragile resting phase and can cause additional loss through traction alopecia on top of the telogen effluvium.
Volumizing products
Volumizing shampoos, root-lifting sprays, and dry shampoo can create the appearance of fuller hair while you wait for regrowth. These cosmetic solutions do not affect the hair growth cycle but can significantly improve how your hair looks and feels during the thinning phase.
Strategic haircuts
A shorter hairstyle can actually make thinning less noticeable. Long, thin hair makes the scalp more visible, while a well-layered shorter cut creates the illusion of volume. A stylist experienced with thinning hair can recommend cuts that maximize the appearance of fullness.
Scalp concealers
Keratin hair fibers (brands like Toppik or Caboki) are finely ground keratin particles that cling to existing hair and create the appearance of thicker, fuller coverage. They wash out with shampoo and are cosmetically effective for many people dealing with temporary thinning.
Tracking progress
Take monthly photos of your part line and hairline under consistent lighting. When you see your hair every day, gradual improvement is hard to notice. Monthly comparison photos provide concrete evidence that regrowth is happening, even when day-to-day it feels like nothing is changing.
Many people find it helpful to track their overall progress alongside their weight loss journey. Documenting tirzepatide before and after results including hair changes provides a complete picture of the treatment experience.
How peptides may support hair during GLP-1 treatment
For people exploring peptide-based approaches to hair support alongside their tirzepatide protocol, several peptides have demonstrated hair-related benefits in research settings.
GHK-Cu (copper peptide) is one of the most studied peptides for hair applications. Research shows it can increase hair follicle size, stimulate hair growth, and reduce hair loss by promoting blood flow to the scalp and supporting collagen production around follicles. Our GHK-Cu peptide for hair guide covers the research and protocols in detail. The broader category of copper peptides for hair growth includes several related compounds worth exploring.
PTD-DBM is a newer peptide showing promise in hair loss research. It works through a different mechanism than GHK-Cu, targeting the Wnt signaling pathway that governs hair follicle development and cycling. Early studies suggest it may help stimulate dormant follicles to re-enter the growth phase. The PTD-DBM peptide hair growth guide provides current research details.
The complete overview of peptides for hair loss and peptides for hair growth covers additional compounds being studied for these applications. SeekPeptides provides comprehensive resources on peptide protocols for members looking to support multiple health goals simultaneously.
It is worth noting that peptide-based hair support and GLP-1 therapy can coexist. The mechanisms do not conflict. Someone using tirzepatide for metabolic benefits while using topical copper peptides for scalp support is addressing two different systems through two different pathways.
Frequently asked questions
Does tirzepatide directly cause hair loss?
No. Tirzepatide does not directly damage hair follicles or disrupt the hair growth cycle through its pharmacological mechanism. The hair shedding observed in clinical trials is telogen effluvium triggered by rapid weight loss, not by the medication itself. The same shedding occurs with any rapid weight loss method including bariatric surgery and crash dieting.
How common is hair loss on tirzepatide?
Clinical trials report alopecia in 4% to 5% of tirzepatide users compared with 1% in the placebo group. Women are more affected at approximately 7.1% compared with less than 1% of men. Importantly, no clinical trial participants stopped treatment due to hair loss, indicating the severity is generally mild to moderate.
When does hair loss start on tirzepatide?
Most people notice increased shedding around months 3 to 4 of treatment. This delay occurs because telogen effluvium has a built-in lag: the trigger (rapid weight loss) shifts follicles into the resting phase, and the actual shedding does not become visible until 2 to 4 months later when those resting hairs are released.
Is tirzepatide hair loss permanent?
No. Telogen effluvium is fully reversible. Hair typically begins regrowing once the body adapts to its new weight and nutritional intake stabilizes. Most people see significant recovery within 3 to 6 months after their weight stabilizes, with complete recovery taking 9 to 18 months. The GLP-1 hair loss guide covers recovery timelines across all medications.
Should I stop taking tirzepatide if my hair is falling out?
Stopping tirzepatide will not immediately stop the current shedding cycle because the trigger occurred months ago. The decision to continue or stop should weigh the metabolic benefits against the temporary cosmetic concern. Nutritional optimization, slower weight loss pacing, and supplementation of documented deficiencies are generally more effective approaches than discontinuation. Discuss with your healthcare provider before making changes to your tirzepatide dosing.
What supplements help with hair loss on tirzepatide?
The most evidence-backed approach is testing for and correcting specific deficiencies. Ferritin (iron storage), vitamin D, and zinc are the most commonly deficient nutrients that affect hair. Adequate protein intake (0.8 to 1.2 g per kg body weight daily) is critical. High-dose biotin is not recommended unless you are genuinely biotin deficient. See our guide on supplements to take with tirzepatide for comprehensive recommendations.
Does microdosing tirzepatide reduce hair loss risk?
Potentially, yes. Because hair loss correlates with speed and magnitude of weight loss rather than medication dose per se, a microdosing tirzepatide approach that produces slower, more gradual weight loss may reduce the severity of telogen effluvium. The trade-off is slower progress toward weight loss goals.
Can tirzepatide actually help hair grow?
In some cases, yes. A published case report documented significant hair density improvement in a patient with insulin resistance-driven androgenic alopecia after tirzepatide treatment. By normalizing insulin levels and reducing DHT production, tirzepatide improved the conditions that were causing hair loss. This effect appears most relevant for people whose hair loss involves metabolic dysfunction rather than nutritional deficiency.
External resources
Hair Loss Associated With GLP-1 Receptor Agonist Use: A Systematic Review (Cureus, 2025)
Telogen Effluvium Associated With Weight Loss: A Retrospective Study (PMC, 2024)
For researchers serious about optimizing their peptide protocols and managing side effects effectively, SeekPeptides offers the most comprehensive resource available, with evidence-based guides, proven protocols, and a community of thousands who have navigated these exact questions.
In case I do not see you, good afternoon, good evening, and good night. May your follicles stay active, your nutrients stay balanced, and your regrowth stay strong.